Embed Size (px)
Citation preview

www.saferhealthcarenow.ca
A Novel Tool to Assess the Quality of Admission MedRec Processes
Jennifer TurpleISMP Canada
Alex TiteuSafer Healthcare Now! Central Measurement
(Patient Safety Metrics)

www.saferhealthcarenow.ca
Objectives
• To briefly describe the need for improved quality of admission MedRec processes.
• To introduce the use of a tool which allow teams to collect patient level data on specific admission MedRec quality determinants (for acute care and long‐term care based MedRec).
• To demonstrate how this data can be easily submitted and analyzed through the Patient Safety Metrics system.

www.saferhealthcarenow.ca
Presence of an Admission MedRec /BPMHform on chart
Are the processes “behind the form” of good quality?

www.saferhealthcarenow.ca
At the monthly management meeting of a large urban hospital, the head of patient safety announces: “We had a critical incident last week. A
patient was readmitted two days after discharge with severe hypoglycemia. The treating team discharged the patient on a new insulin regimen without realizing that the patient also had insulin 30/70 at home. The patient continued to take both her previous regimen as well as the new one, and was found unresponsive by her husband. She’s in ICU and will probably have permanent neurological deficits.” After various sighs and exclamations from the executives around the table, the chief medical officer asks incredulously, “Why didn’t this get picked up by medication reconciliation?” Before anyone can answer, the executive adds: “We had that other case six months ago in which a patient was discharged without
restarting his Coumadin, and he ended up having a stroke. We implemented medication reconciliation a year ago. Why is this still
happening?”
Reference: Fernandes et al., Healthcare Quarterly, 2012

www.saferhealthcarenow.ca
Why focus on Admission?

www.saferhealthcarenow.ca
Quality Admission MedRec Process(es):
Allows for the effective, reliable, and timely completion of each of these steps:
– STEP 1‐ COLLECT
Use a systematic approach/process to collect a BPMH
– STEP 2‐ COMPARE
Compare the BPMH (as collected) with the admission orders (to identify differences)
– STEP 3‐ CORRECT
As needed, resolve unaccounted for differences between the BPMH and the admission orders

www.saferhealthcarenow.ca
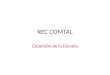
STEP 2‐COMPARE
STEP 3‐CORRECT
Each circle represents a unique process
STEP 1‐COLLECT
Admission Medication Reconciliation
This process can decrease
specific, clinically
meaningful, and
preventableadverse drug
events.

www.saferhealthcarenow.ca
STEP 1‐Collect
A Best Possible Medication History (BPMH) is a medication history created using:1) A systematic process of interviewing the patient
or their caregiver
2) A review of at least one other reliable source of information to obtain and verify all of a patient’s medication use (prescribed and non‐prescribed)
3) Complete documentation of all the medications including name, dose, route and frequency
BPMH is a snapshot of a patient’s actual medication use, which may be different than what is
contained in their records!

www.saferhealthcarenow.ca
Quality BPMH Collection
• 2012 publication from an organization who had “implemented” MedRec, compared medication histories completed in the usual process of medication reconciliation to an independent investigators compiled medication list.
• Primary outcome: Percentage of medication histories accurately completed. Accuracy was defined as complete matching of medication name, dose, route and frequency of the two lists.
• Secondary outcomes: Rate of Omissions, Commissions, and consistency of allergy information.
Reference: Miller et al., Hosp Pharm, 2012

www.saferhealthcarenow.ca
Quality BPMH Collection
• Results– Of the 114 audits, the percentage of accurate medication histories was 13%

www.saferhealthcarenow.ca

www.saferhealthcarenow.ca
Challenges
http://www.youtube.com/watch?v=spqrcu4Wspc

www.saferhealthcarenow.ca
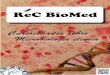
STEP 2‐ Compare
• The process of comparing the BPMH to admission orders generally occurs in one of two ways/through two models:
• This comparison takes place to identify differences (or discrepancies)
Decision to admit
BPMH Collected
TIME
Admission Orders Written
Admission Orders Written
BPMH Collected

www.saferhealthcarenow.ca
Challenges
• Proactive model– Embeds the “compare” step
into the process of writing admission orders
– This allows for explicit ordering (communication) of each medication in the BPMH
• Retroactive model – Perceived as “extra work” as
it is not embedded into a pre‐existing workflow
– The “compare” step is more challenging in that the prescribers intentions may not be obviously stated in the admission orders/chart
ECASA 325 mg po dailyMetoprolol 50 mg po bid
Bradycardia
Admission Orders BPMH
ECASA 325 mg po daily Metoprolol 50 mg po bidECASA 325 mg po daily
?? Simvastatin 40 mg daily

www.saferhealthcarenow.ca
STEP 3‐ Correct
• When discrepancies are identified, there is a process to ensure that these are resolved with the prescriber (or designate).

www.saferhealthcarenow.ca
How often are we doing everything right?

www.saferhealthcarenow.ca
The Tool
Please refer to the tab at the top of the WebEx screen, to view/print an
example of the audit tool

www.saferhealthcarenow.ca
Overview
The tool:
• Allows acute care and long term care organizations to qualify and quantify how they are performing the basics tenets of the admission MedRec process. Aggregated data can be helpful in identifying specific areas in need of process improvement.
• Is in a format that allows for patient level data collection, completed via a retrospective chart review (i.e. time point after admission MedRec process should have taken place)
• Decreases data collection/submission “burden” through use of optical marker recognition technology– Results are collated and presented within minutes in the
Patient Safety Metrics System

www.saferhealthcarenow.ca
Use of the Tool• The sample size, sampling strategy, selection of the area to audit and the frequency of the audits are at the discretion of the end‐users.
Note: SHN! recommends 10‐20 charts monthly. IHI recommends a sampling strategy of a monthly random sample of 20 patient records from patients with a minimum two day length of stay for a similar
measure.
• The ability to complete the tool is strongly dependant on organizational chart documentation practices specific to MedRec tasks.

www.saferhealthcarenow.ca
Use of the Tool
• Ideally an auditor(s) should:– be someone familiar with the admission MedRec process(es), forms used and overall chart layout
– not audit their own work
– have some training or guidance provided (to ensure consistency in application of org‐specific criteria)

www.saferhealthcarenow.ca
Identify the admission “route”
The criteria for a “yes” response to this question is up to the end users to determine. The aggregated data from this column may be
used as a measure of “Percent (%) Reconciled at Admission”.
Components of the Tool
When interpreting this result, consider the sampling strategy used. Comparing the results of this measure against other units/orgs, should be done cautiously.

www.saferhealthcarenow.ca
COLLECT CORRECTCOMPARE
Components of the Tool• The remaining sections of the tool are designed to identify if specific
objectives have been met at each of the 3 steps in the overall admission MedRec process. When combined, these objectives provide a sense of the overall quality of the process from start to finish.

www.saferhealthcarenow.ca
Step 1‐Collect
Components of this section are based on key principles of collecting and documenting a BPMH including:
– Medication information source utilization (C)
– Patient involvement/interview to confirm actual medication use (D)
– Completeness of the medication information for each medication (E)

www.saferhealthcarenow.ca
Medication Info Source (C)• “YES” when auditor identifies use of any one of the
following sources:• Electronic provincial medication/community pharmacy record • Medication vials or pill‐packs/community pharmacy records • Patient’s own medication list (hand‐written or electronic) • Home care reconciled medication list• Previous admission records/discharge summary • Prescriber referral/consultation notes • Ambulatory clinic medication records For patients admitted directly from a setting where medications have been
administered directly to the patient:• Most current Medication Administration Record (MAR) • Best Possible Medication Discharge Plan (BPMDP)
• “No” when auditor does not identify use of any of these• “Unclear” if the chart documentation does not allow the
auditor to respond confidently “yes/no”

www.saferhealthcarenow.ca
Actual Med Use/Patient or Caregiver Interview (D)
• “YES” if there has been verification of medication use through patient or caregiver interview (OR if the source includes a MAR or BPMDP for those coming from structured care settings)
• “NO” if there has not been verification through an interview
• “Unable to perform” if the interview was not possible due to patient specific factors (e.g. non‐verbal patient, unable to contact a caregiver)
• “Unclear” if the chart documentation does not allow you to respond confidently “yes/no”

www.saferhealthcarenow.ca
Complete components for each medication listed in BPMH and Orders (E)
• “YES” if all applicable medication order components are provided (i.e. drug name, dose ± strength, route and frequency)
• “NO” if there is missing components in the medication order
Note: End users may wish to code medication informationlisted using unapproved abbreviations as “NO”

www.saferhealthcarenow.ca
STEP 2‐ Compare (F)
• In this section, auditors are asked to assess whether all of the medications, as listed in the BPMH, have been accounted for in the admission orders.

www.saferhealthcarenow.ca
Compare (F)
• “YES” if in the previously conducted process of comparing admission orders to BPMH (as collected), all medications are accounted for
• “NO” if there are any differences that are unaccounted forbetween the BPMH (as collected) and the admission orders
An “unaccounted‐for” difference could include the lack of:‐an explicit admission order to either discontinue/ hold/change/continue a medication listed in the BPMH
OR‐a clear* clinical reason/documentation for the difference (e.g. stopping warfarin in a patient admitted with an acute bleed). * The definition of “clear” is at the discretion of end users and should incorporate some clinical judgement.
No reference to unintentional or intentional. Quantity or type of difference is not captured.

www.saferhealthcarenow.ca
Rationale (G)
• “YES/not applicable” if all BPMH medications that have been discontinued or held in the admission orders include documentation on a rationale for this action OR if there are no BPMH medications discontinued or held
• “NO” if there are any BPMH medications that are discontinued or held in the admission orders that lack an accompanying rationale for this action
• “Unclear” if the chart documentation does not allow you to respond confidently “yes/no”

www.saferhealthcarenow.ca
STEP 3 ‐ Correct (H)
• Auditor is looking for evidence/chart documentation that any
identified differences have been resolved.
•“YES” if adequate evidence (documentation such as progress note or
prescriber order) is identified to support the resolution of any identified differences between the BPMH and the Admission
Orders•“NO” if there are outstanding differences that do not appear to have been resolved.•“Unclear” if the chart documentation does
not allow you to respond confidently “yes/no”

www.saferhealthcarenow.ca
Patient Safety Metrics
Alex Titeu

www.saferhealthcarenow.ca
• Patient Safety Metrics - Introduction– Features– Worksheets vs. Data Collection Forms (DCF)
• MedRec Quality Assessment DCF– Contact Information, Unit and Patient Sample, Date– How to fill-out the information and fax the form
• Patient Safety Metrics - Demo– How to enroll in MedRec-Acute and MedRec-LTC Intervention– How to add and generate the forms– How to view data and run reports
Agenda

www.saferhealthcarenow.ca
Features:• Cloud-based data collection and reporting tool• Available in English and French• User friendly and simple to navigate • Accessible from website with login details• Tracks >100 process and outcome measures over 14 interventions• Provides real time reporting.• Reduces burden of data collection, entry and analysis• Roll Up or Drill Down Reports (i.e. Unit National) with
automated Run Charts• Capacity to customize measures and reports
Patient Safety Metrics - Introduction

www.saferhealthcarenow.ca
• Measurement Worksheets– Aggregate data - monthly – Numerator and Denominator
• Data Collection Forms (DCF)– Patient-level data (de-identified) - daily– Multiple data elements – Print form Collect data Fax form – Automatic roll-up to Measurement Worksheets
Worksheets vs Data Collection Forms

www.saferhealthcarenow.ca
MedRec Quality Assessment DCF
35

www.saferhealthcarenow.ca
• Fill in bubble completely (Sharpie is best)• Do not colour outside the line • Do not fold the form• Fax form in FINE RESOLUTION (setting on fax machine)• Do NOT use a cover sheet• No extra markings on form• To void fill in the VOID bubble• Do not spill anything on the form
Data Collection Forms - BEWARE!

www.saferhealthcarenow.ca
• DCF - MedRec-Acute QA - Patient Data (Form Format)– Report by individual patients (No QA score)
• DCF - MedRec-Acute QA - Patient QA Score– Report by individual patients
• DCF - MedRec-Acute QA - Monthly Form QA Score– Aggregate report by patient population
• DCF - MedRec-Acute QA - Monthly Overall QA Score– Overall organization score
Data Collection Forms - Reports
37

www.saferhealthcarenow.ca
Live Demo
Patient Safety Metricshttps://shn.med.utoronto.ca/metrics/login.aspx
38
Central Measurement TeamVirginia Flintoft & Alexandru [email protected]

www.saferhealthcarenow.ca
Questions?
39

www.saferhealthcarenow.ca
Jennifer Turple
ISMP Canada
www.ismp‐canada.org
1‐866‐544‐7672 ext. 255
JTurple@ismp‐canada.org
Patient Safety Metrics
https://shn.med.utoronto.ca/metrics/login.aspx
CPSI Central Measurement Team
Virginia Flintoft ‐ 416‐946‐8350
Alexandru Titeu ‐ 416‐946‐3103
Thank you! Please complete our POLL