Embed Size (px)
Citation preview
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
Palliative RVOT Palliative RVOT proceduresprocedures
양 지 혁성균관의대 삼성서울병원
흉부외과학교실
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
Palliative RVOT procedures
Pulmonary Valvotomy/valvectomyTransannular patch enlargementRV-PA conduit interposition
Right heart obstructive lesion
Pulmonary atresia (PA) Pulmonary stenosis (PS)
intact ventricular septum
Intact ventricular septum
With VSD TOF
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
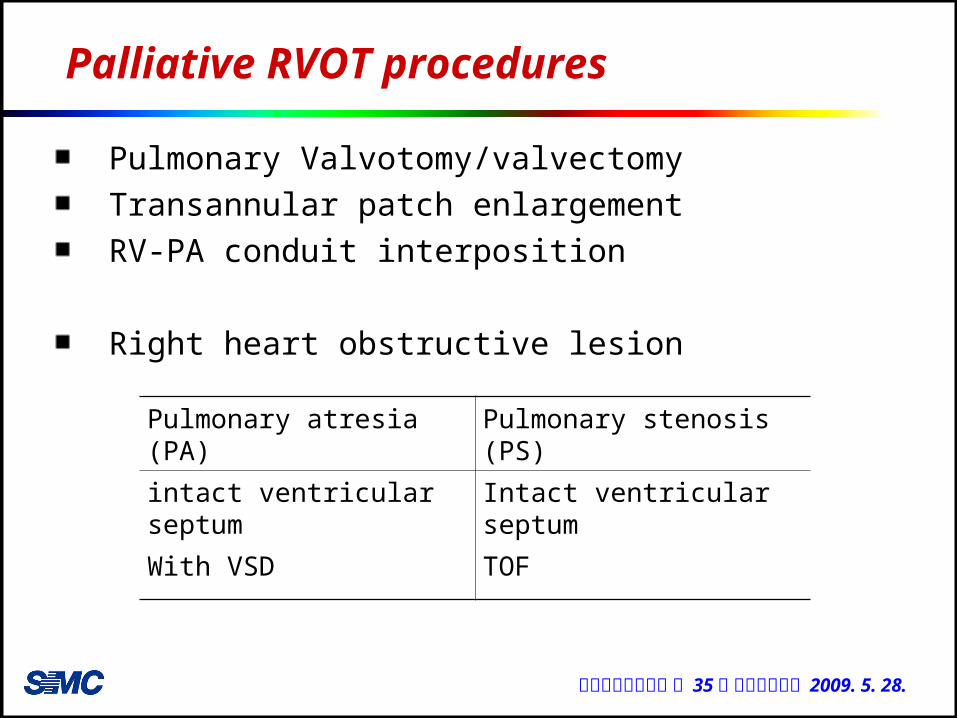
Pulmonary valvotomy / valvectomy
Closed pulmonary valvotomy (Brock procedure)
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
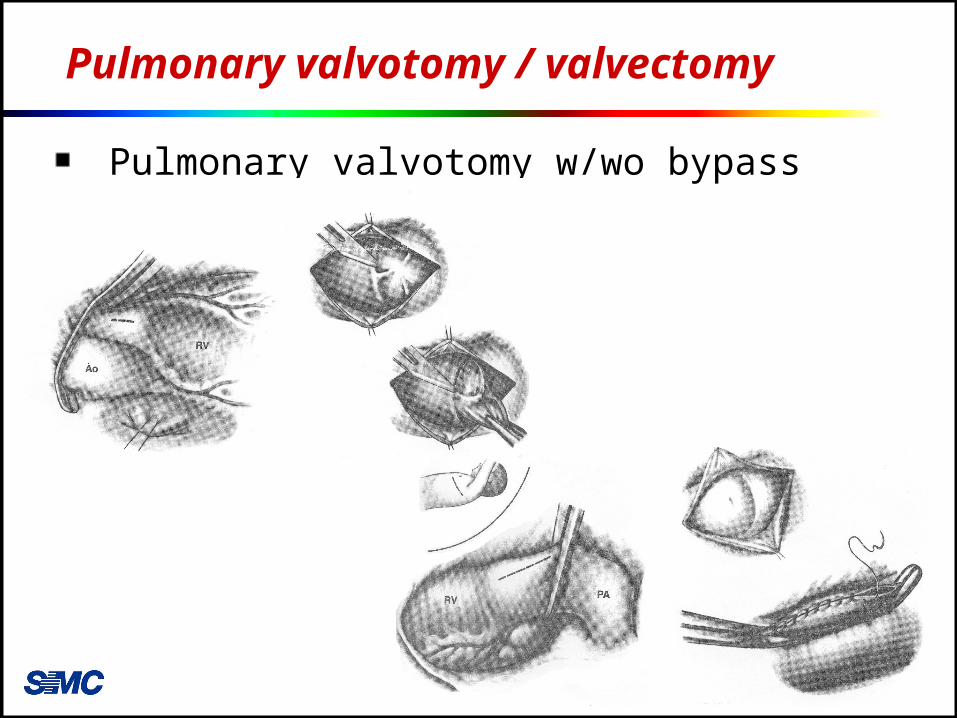
Pulmonary valvotomy / valvectomy
Pulmonary valvotomy w/wo bypass
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
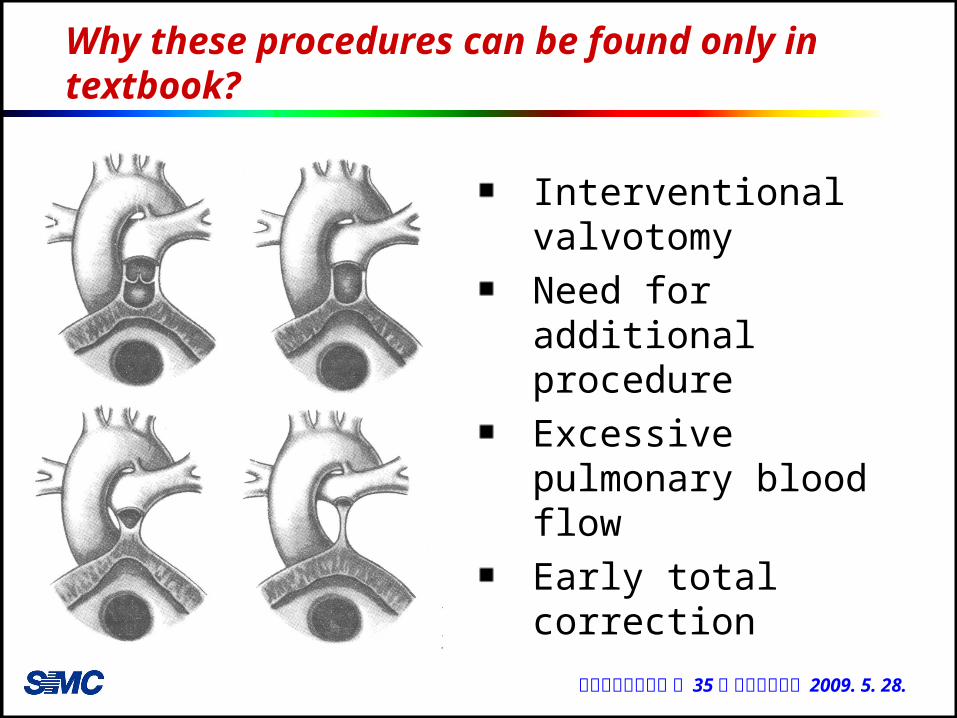
Why these procedures can be found only in textbook?
Interventional valvotomyNeed for additional procedureExcessive pulmonary blood flowEarly total correction
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
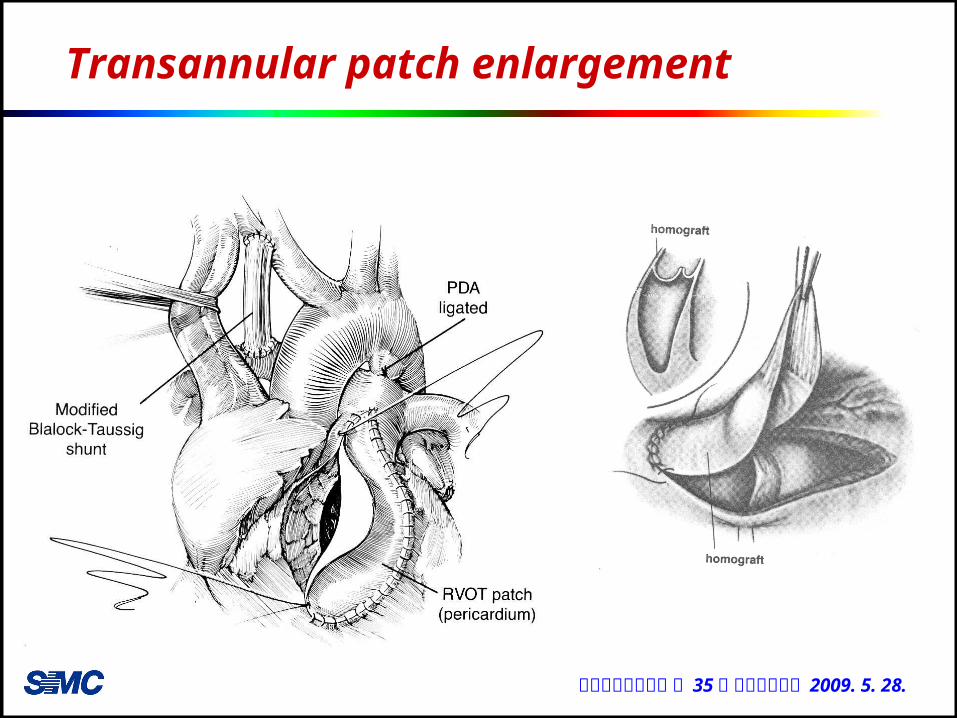
Transannular patch enlargement
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
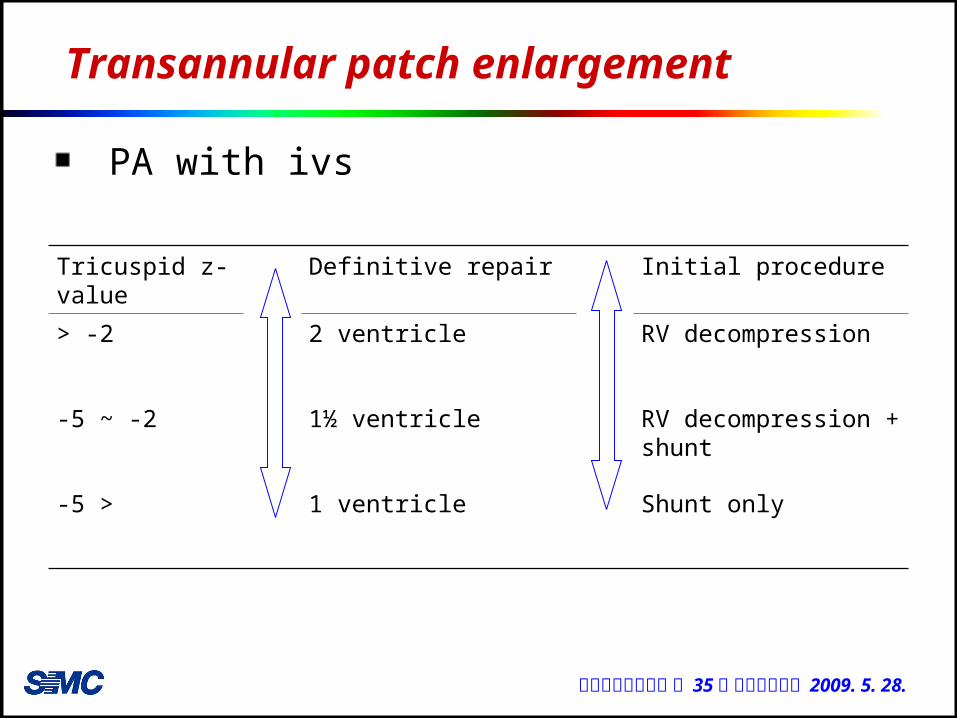
Transannular patch enlargement
PA with ivs
Tricuspid z-value
Definitive repair Initial procedure
> -2 2 ventricle RV decompression
-5 ~ -2 1½ ventricle RV decompression + shunt
-5 > 1 ventricle Shunt only
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
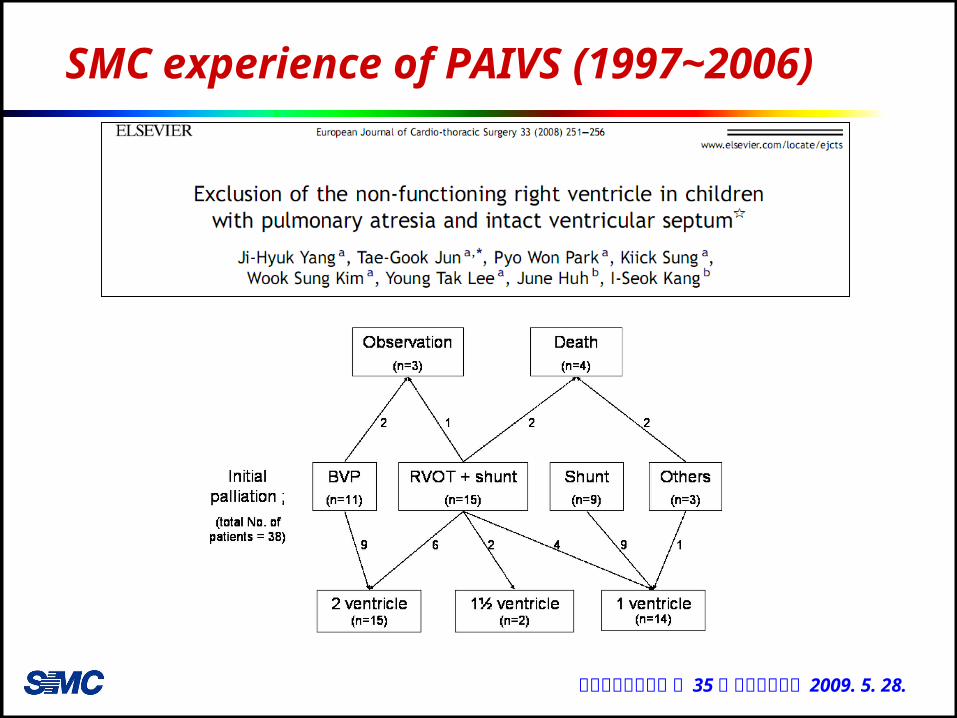
SMC experience of PAIVS (1997~2006)
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
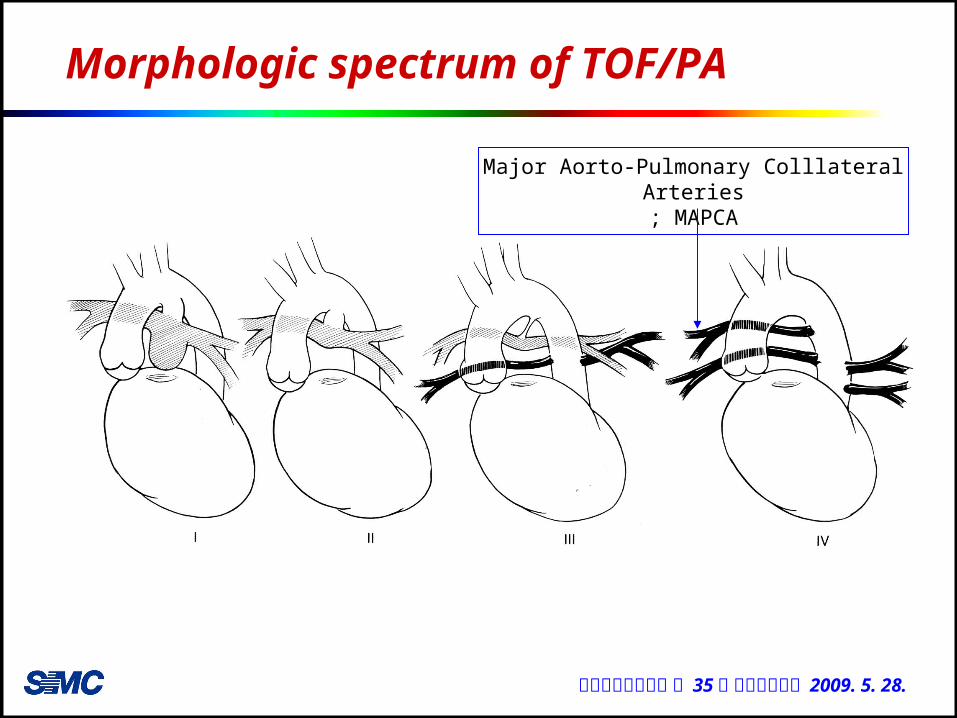
Morphologic spectrum of TOF/PA
Major Aorto-Pulmonary Colllateral Arteries; MAPCA
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
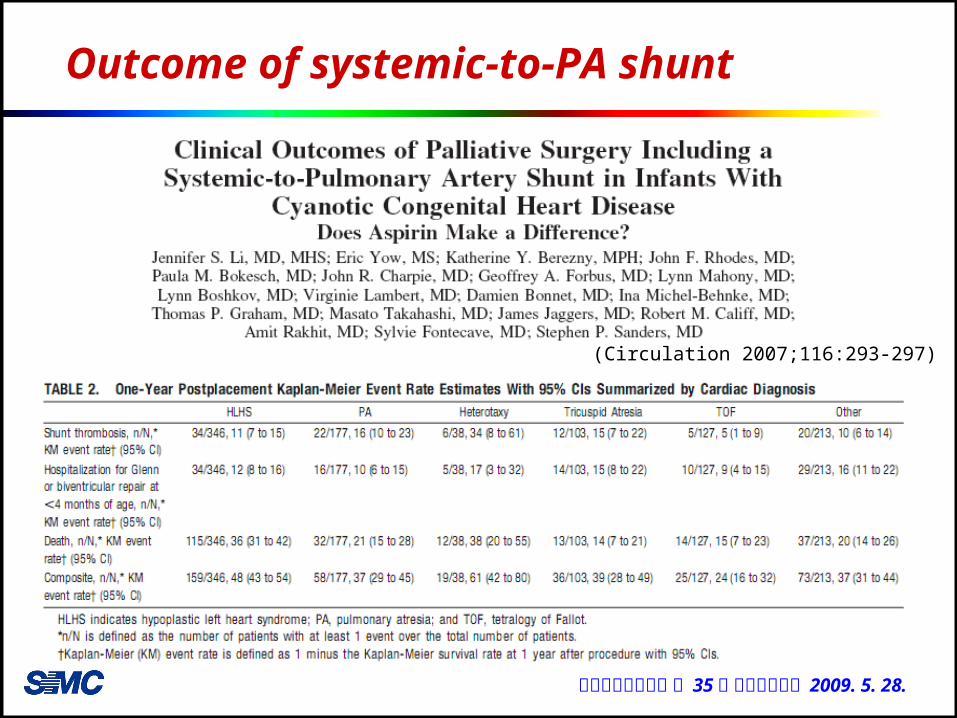
Outcome of systemic-to-PA shunt
(Circulation 2007;116:293-297)
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
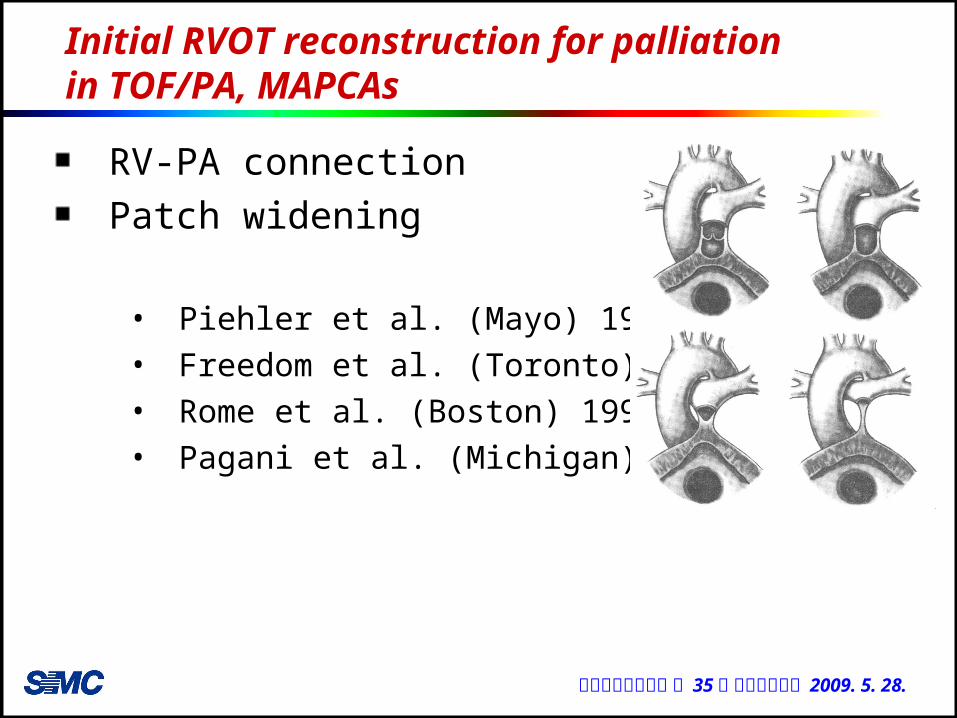
Initial RVOT reconstruction for palliation in TOF/PA, MAPCAs
RV-PA connectionPatch widening
• Piehler et al. (Mayo) 1980• Freedom et al. (Toronto) 1983• Rome et al. (Boston) 1993• Pagani et al. (Michigan) 1995

대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
Rationale for initial RV-PA connection
↑ PA size and angiogenesis of distal microvessels, especially early in lifeNonconfluence in the presence of PA is low (3 ~ 16%)Significant arborization abnormality in the setting of centrally confluent arteries is low
• 80% of patients with confluent central PA have pulmonary blood flow to 15 or more pulmonary segments
• 11.8 segments received blood flow from central PA5.1 segments from aortopulmonary collateral arteries only0.64 segments from a dual source.
Allows access to pulmonary arteries • balloon dilation of peripheral stenotic vessels• precise identification of native pulmonary artery
segmental distribution
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
Advantage of RV-PA connection
LV volume overload
Pulsatile blood flow to enhance PA
growth
Branch PA distortion, pleural adhesion→ easier staged procedures (unifocalization)
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
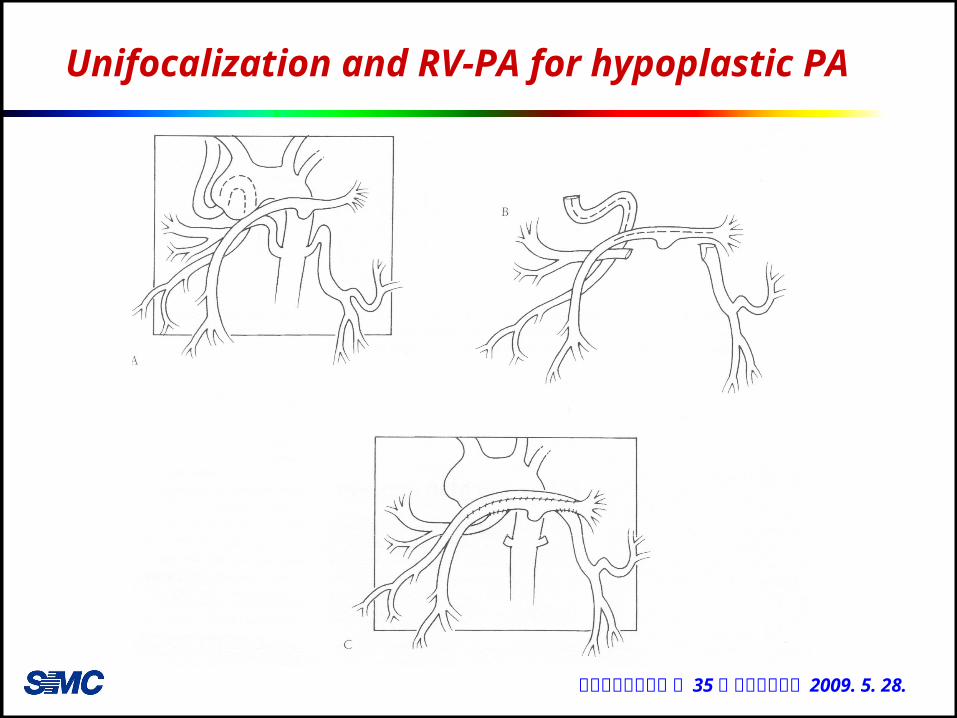
RV-PA connection for hypoplastic PA
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
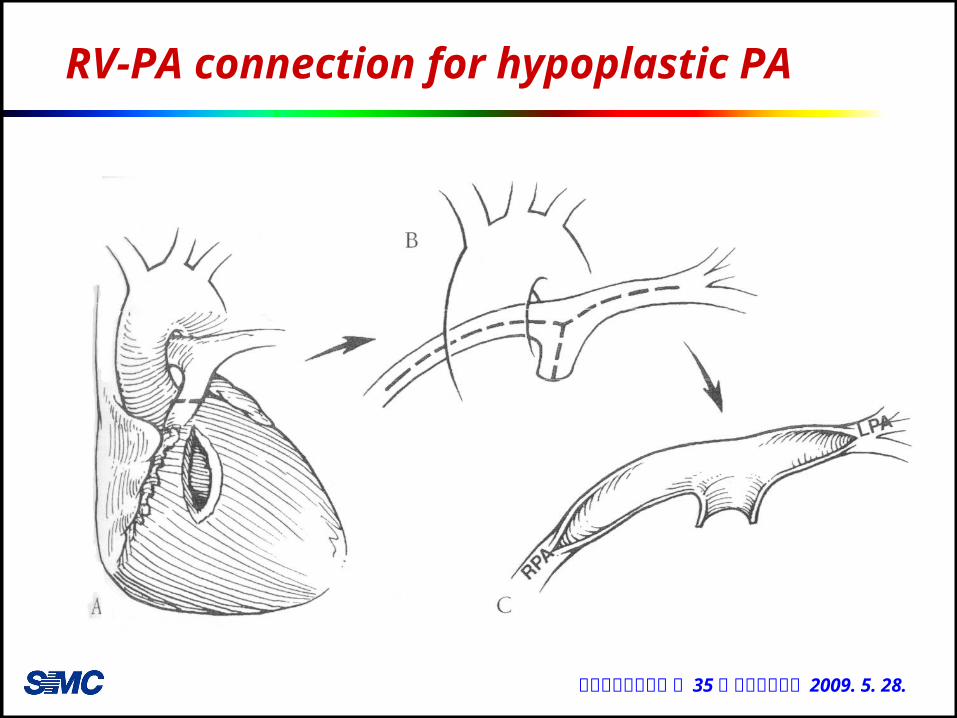
RV-PA connection for hypoplastic PA
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
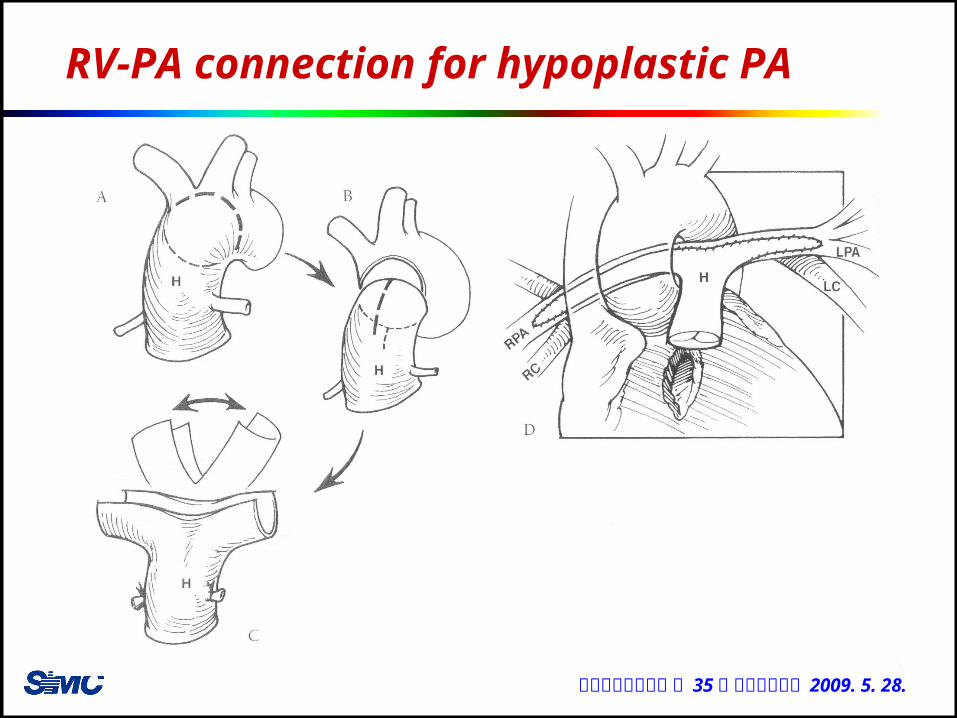
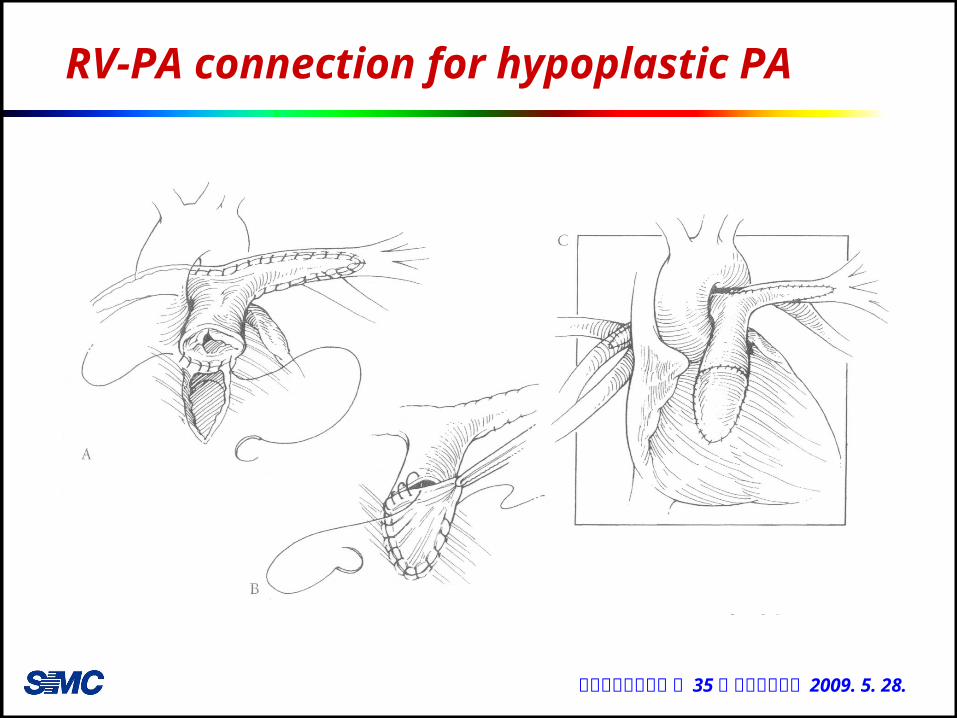
RV-PA connection for hypoplastic PA
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
Unifocalization and RV-PA for hypoplastic PA
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
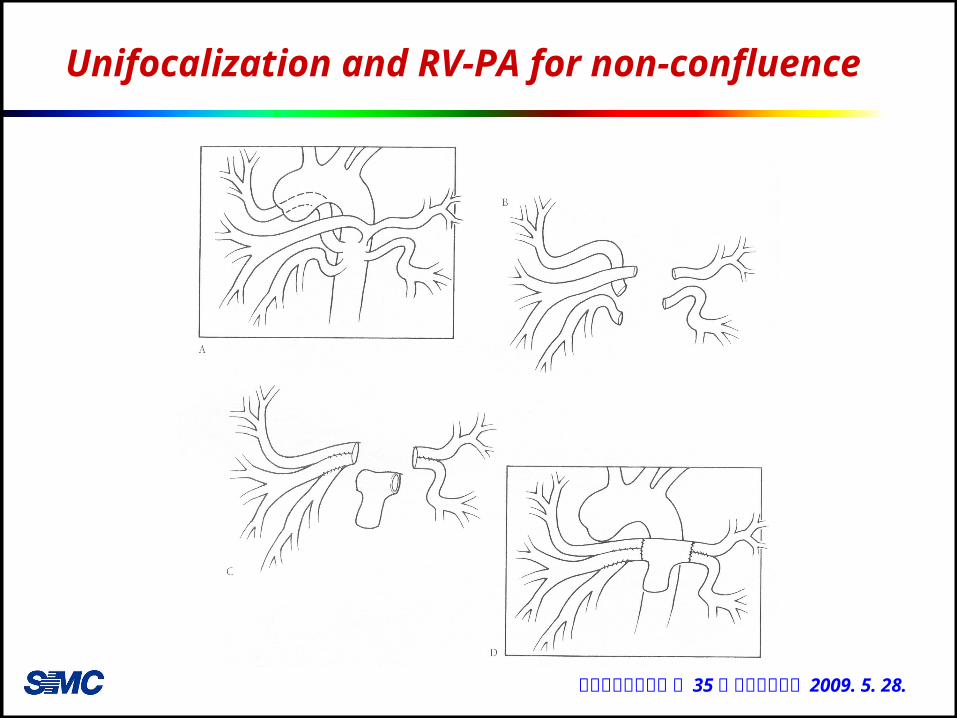
Unifocalization and RV-PA for non-confluence
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
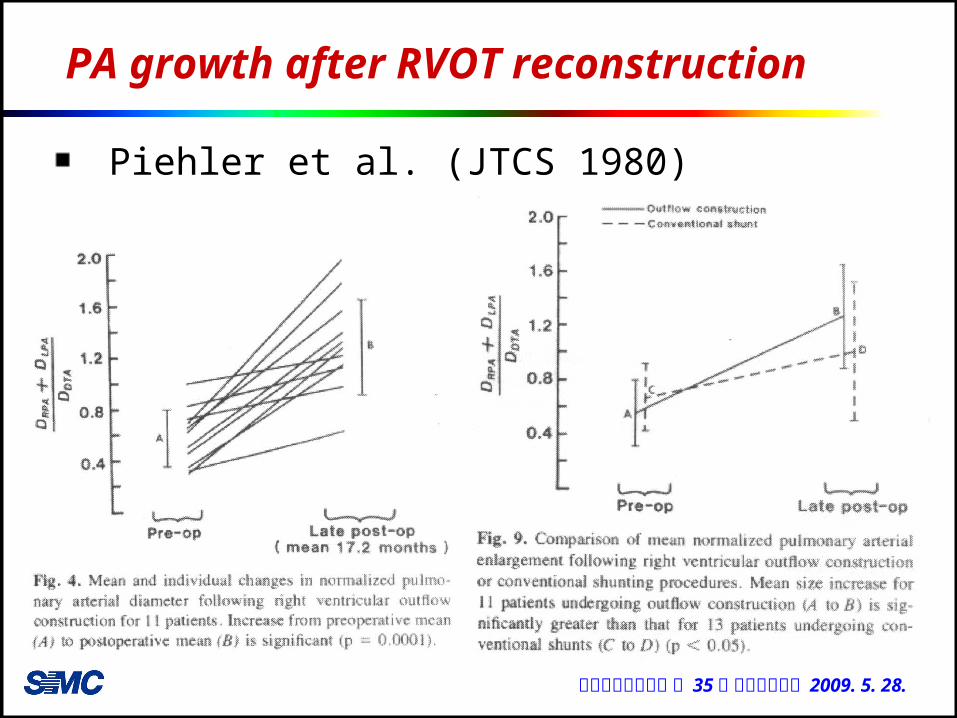
PA growth after RVOT reconstruction
Piehler et al. (JTCS 1980)
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
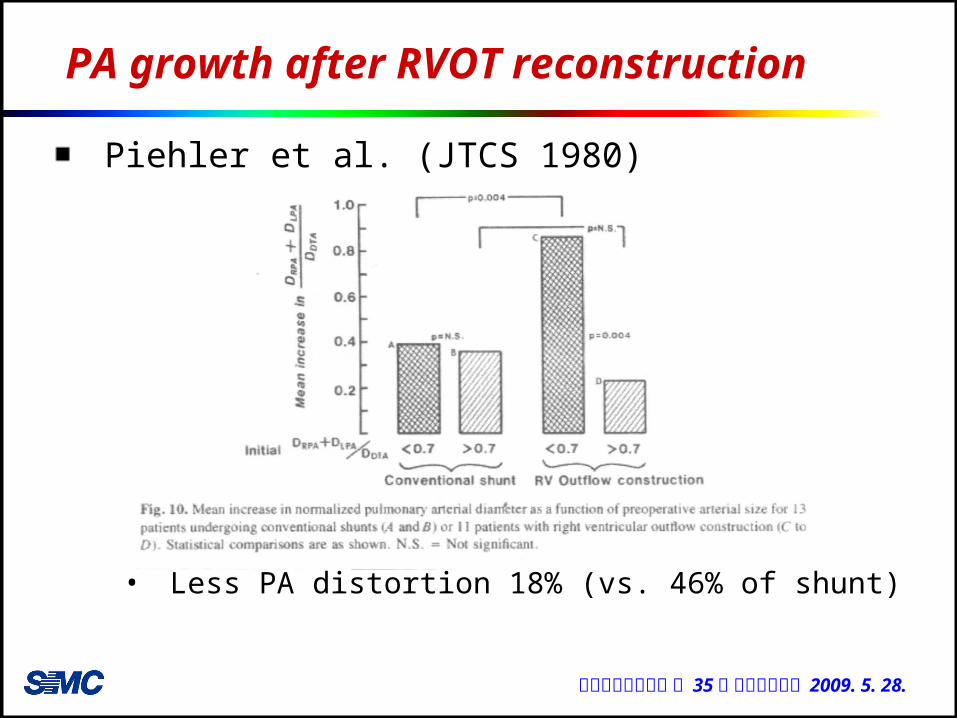
PA growth after RVOT reconstruction
Piehler et al. (JTCS 1980)
• Less PA distortion 18% (vs. 46% of shunt)
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
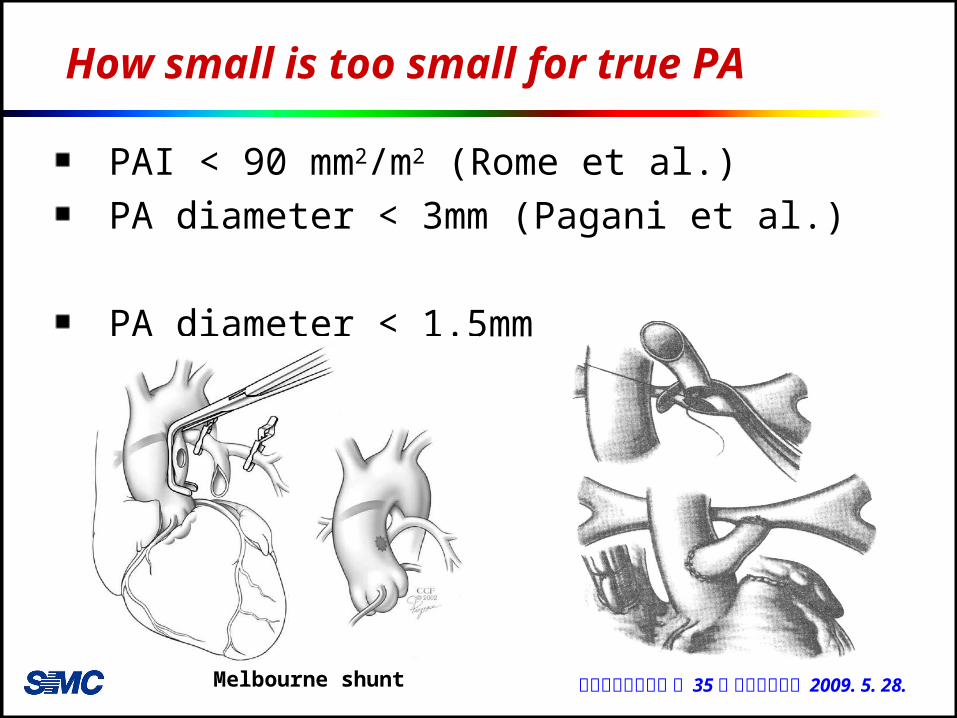
How small is too small for true PA
PAI < 90 mm2/m2 (Rome et al.) PA diameter < 3mm (Pagani et al.)
PA diameter < 1.5mm
Melbourne shunt
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
Selection of Conduit - material
Valved homograft• Advantage
↓ regurgitation → more growth ?↓ bleeding↓ pseudointimal formation
• DisadvantageAneurysmal changeShortage of supply
Valveless conduit (Goretex)• Advantage
Less energy loss
• DisadvantageUnable to maintain distal diastolic PA pressure
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
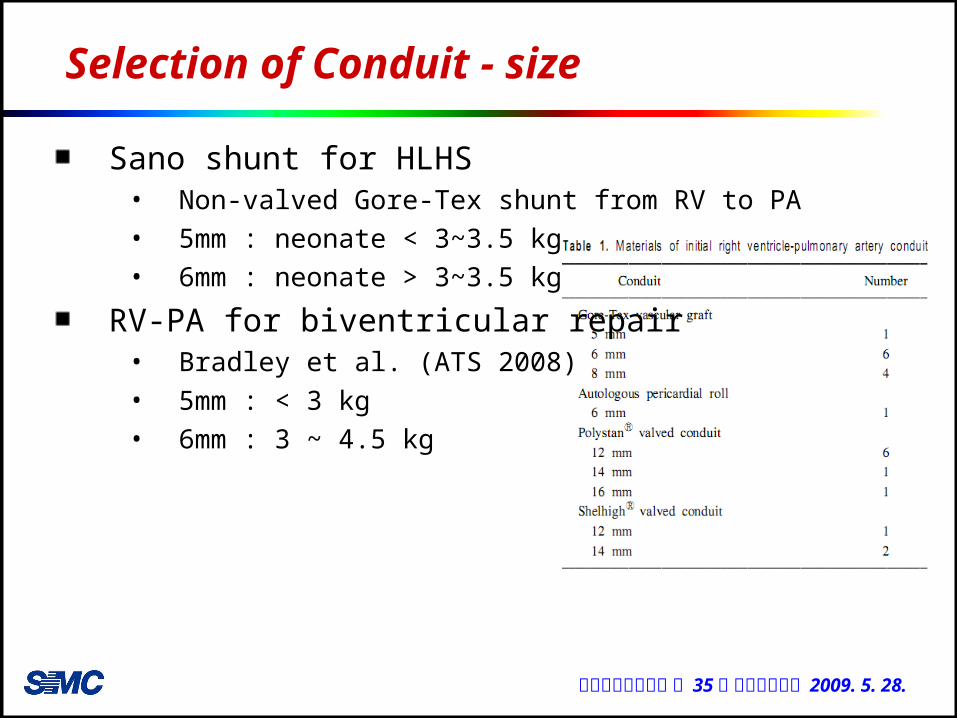
Selection of Conduit - size
Sano shunt for HLHS• Non-valved Gore-Tex shunt from RV to PA • 5mm : neonate < 3~3.5 kg• 6mm : neonate > 3~3.5 kg
RV-PA for biventricular repair• Bradley et al. (ATS 2008)• 5mm : < 3 kg• 6mm : 3 ~ 4.5 kg
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
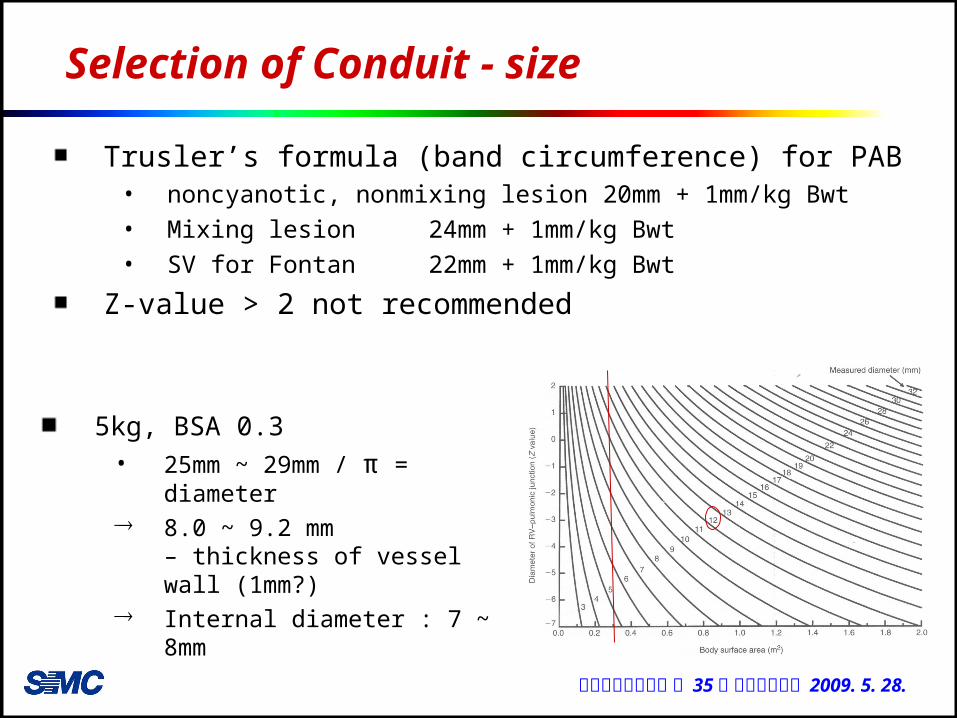
Selection of Conduit - size
5kg, BSA 0.3 • 25mm ~ 29mm / π =
diameter 8.0 ~ 9.2 mm
– thickness of vessel wall (1mm?)
Internal diameter : 7 ~ 8mm
Trusler’s formula (band circumference) for PAB• noncyanotic, nonmixing lesion 20mm + 1mm/kg Bwt• Mixing lesion 24mm + 1mm/kg Bwt• SV for Fontan 22mm + 1mm/kg Bwt
Z-value > 2 not recommended
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
Predictors of successful definitive repair
PAI > 150 mm2/m2
Total neopulmonary artery index (TNPAI) > 200mm2/m2
Qp/Qs > 1.5
pRV/LV < 0.8
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
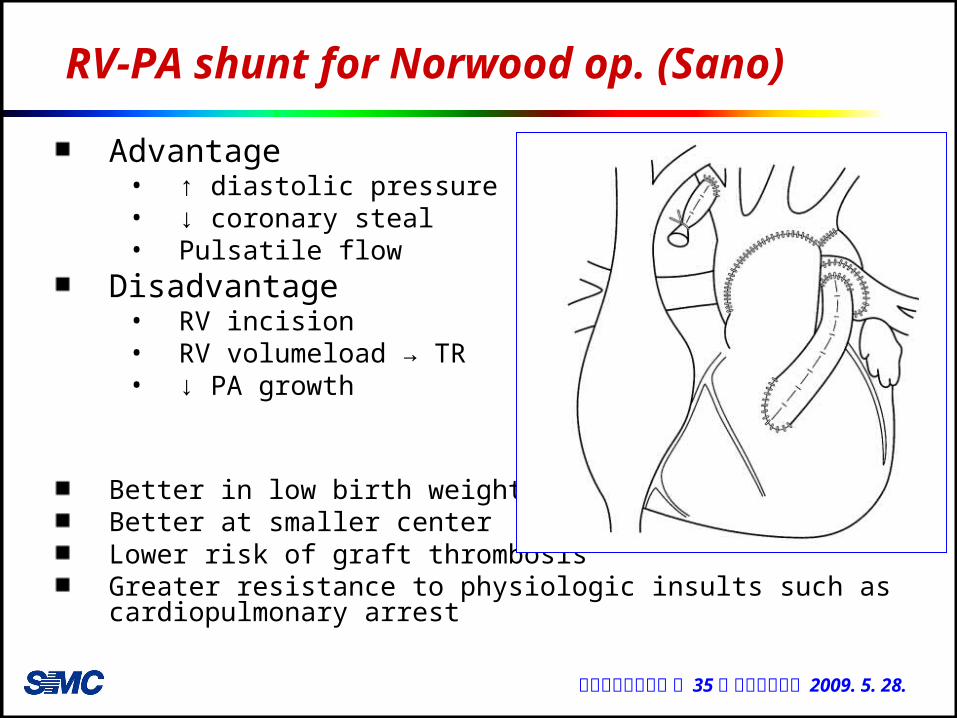
RV-PA shunt for Norwood op. (Sano)
Advantage• ↑ diastolic pressure• ↓ coronary steal• Pulsatile flow
Disadvantage• RV incision• RV volumeload → TR• ↓ PA growth
Better in low birth weight babiesBetter at smaller centerLower risk of graft thrombosisGreater resistance to physiologic insults such as cardiopulmonary arrest
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
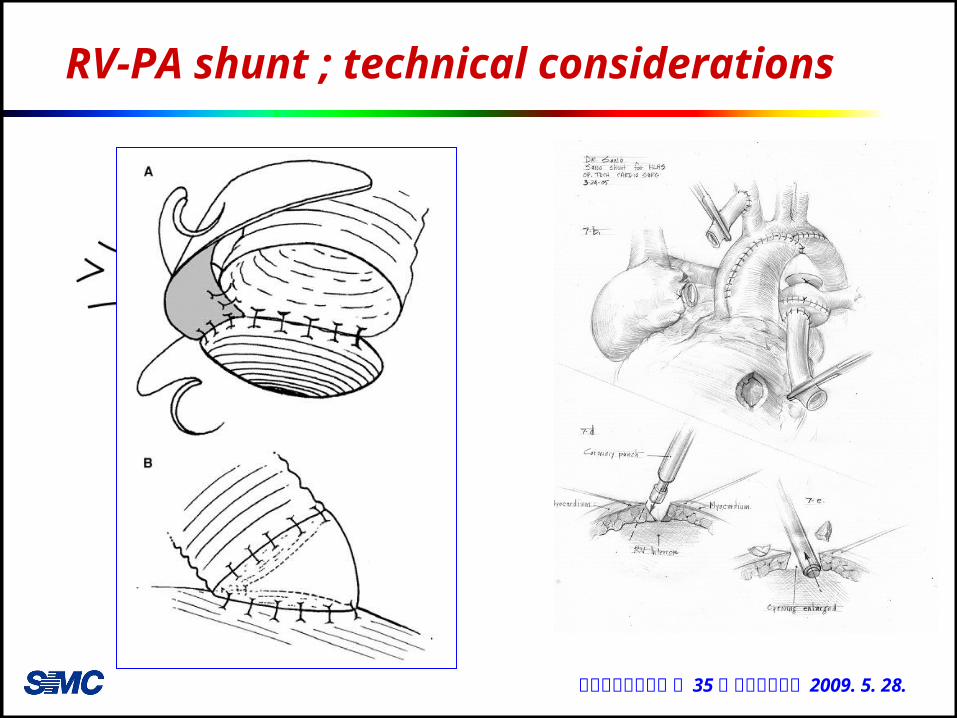
RV-PA shunt ; technical considerations
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
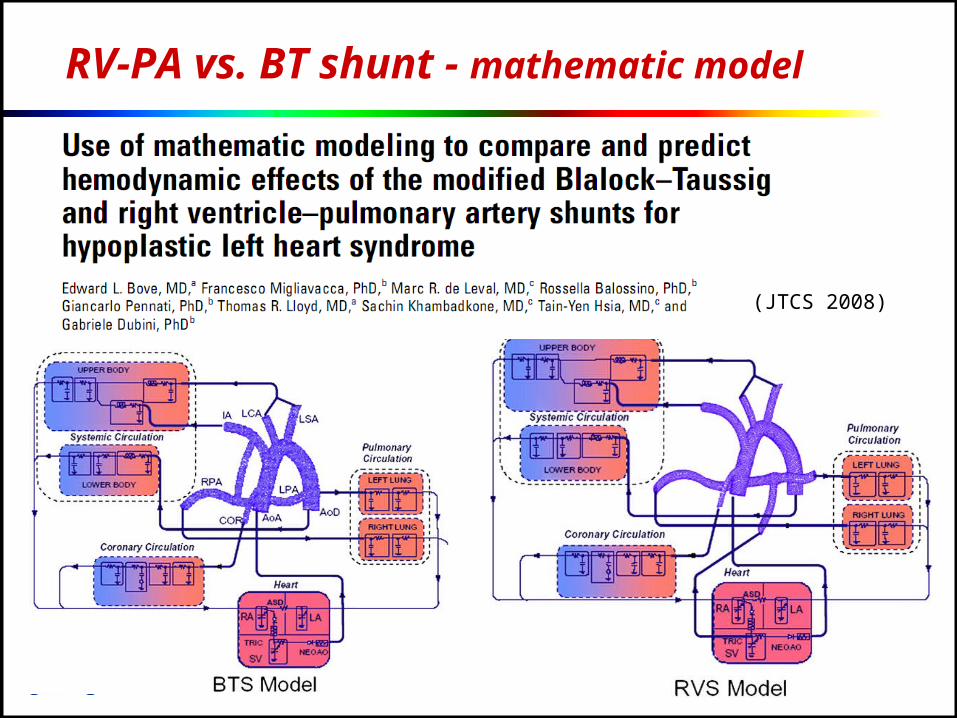
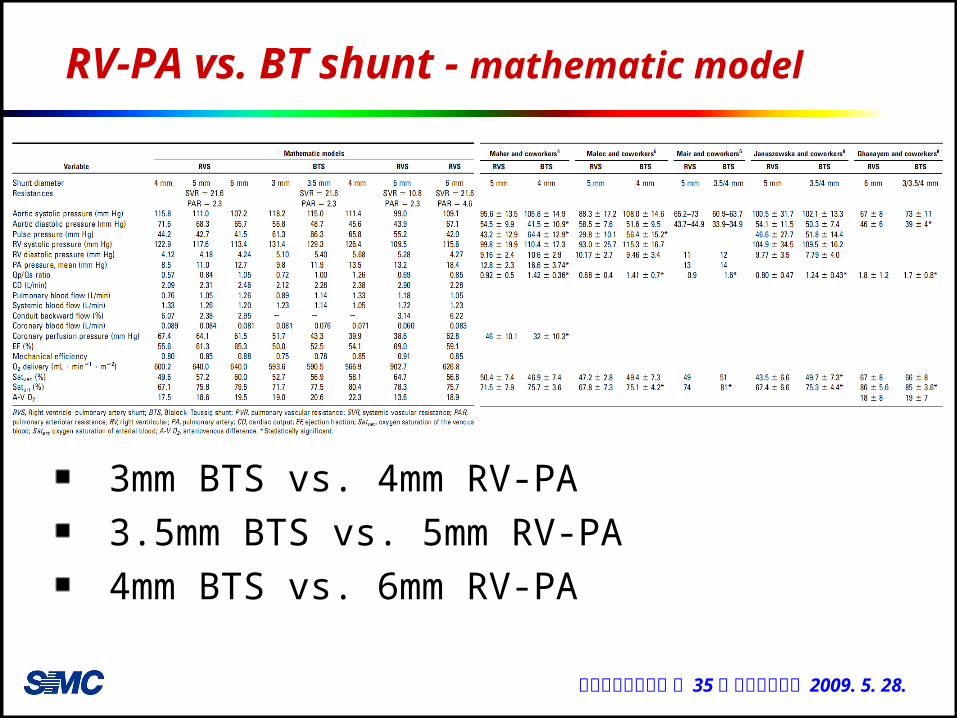
RV-PA vs. BT shunt - mathematic model
(JTCS 2008)
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
RV-PA vs. BT shunt - mathematic model
3mm BTS vs. 4mm RV-PA3.5mm BTS vs. 5mm RV-PA4mm BTS vs. 6mm RV-PA
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
RV-PA vs. BT shunt - mathematic model
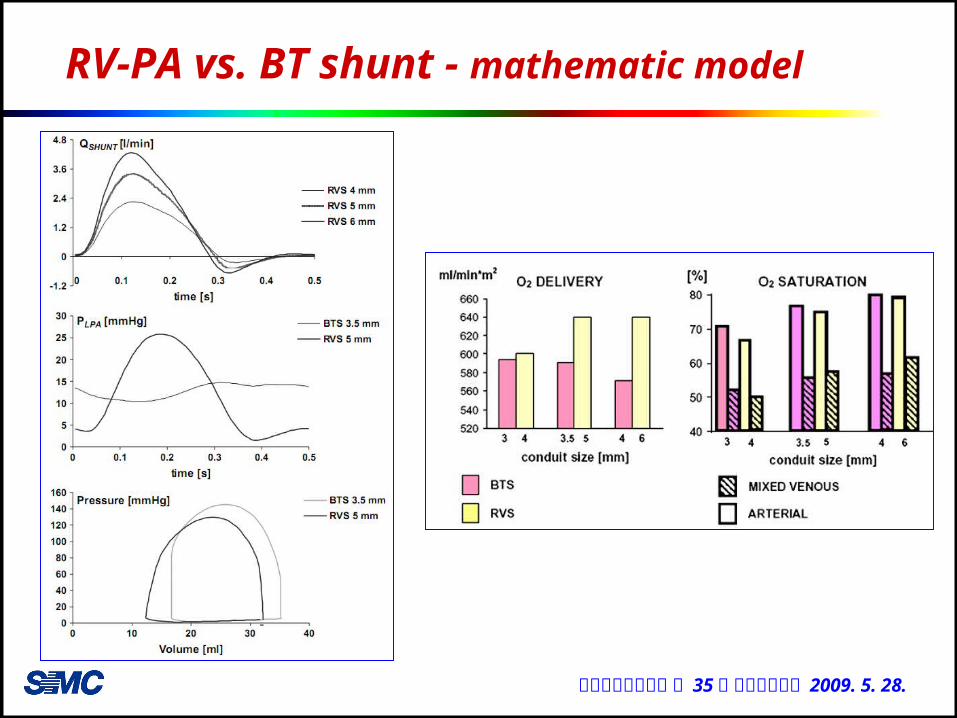
RV-PA model exhibited, at similar SaO2
• lower pulse pressure • lower Qp/Qs ratio• lower PAP• lower RV systolic and diastolic pressure• higher coronary perfusion pressure• higher O2 delivery• higher ventricular performance
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
RV-PA vs. BT shunt - mathematic model
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
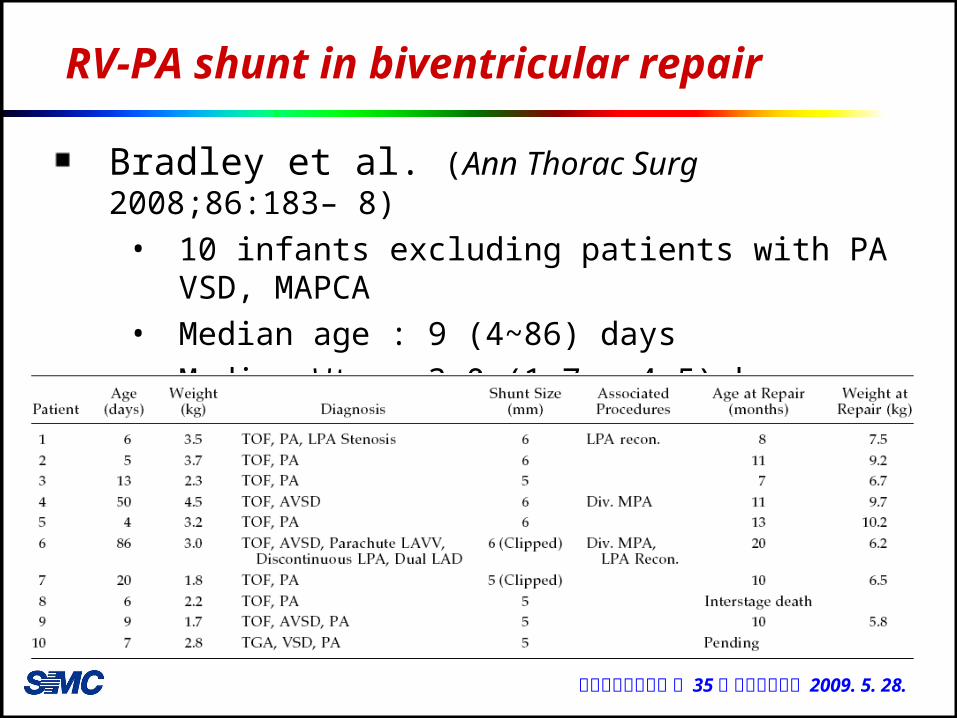
RV-PA shunt in biventricular repair
Bradley et al. (Ann Thorac Surg 2008;86:183– 8)• 10 infants excluding patients with PA VSD,
MAPCA• Median age : 9 (4~86) days• Median Wt. : 3.0 (1.7 ~ 4.5) kg• Non-valved Gore-Tex shunt from RV to PA
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
RV-PA shunt in biventricular repair
No hospital deaths1 reoperation
• Revision of shunt d/t distal anastomosis stenosis SpO2 at the discharge : 94 ± 4 %
2 patients with a clipped shunt underwent successful balloon dilation (6 Mo after RV-PA)
Biventricular repair • 8 patients• interval : median 10 (6~17) months• SpO2 : 86 ± 1• Conduit diameter : 14 ~ 16 mm• No early or late deaths
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
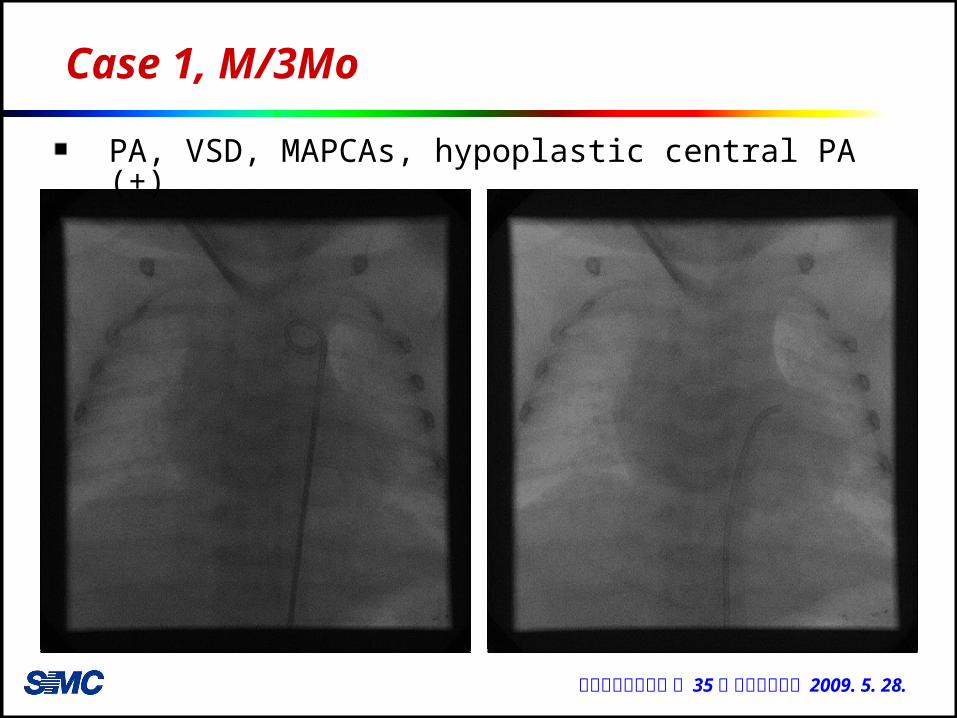
Case 1, M/3Mo
PA, VSD, MAPCAs, hypoplastic central PA (+)
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
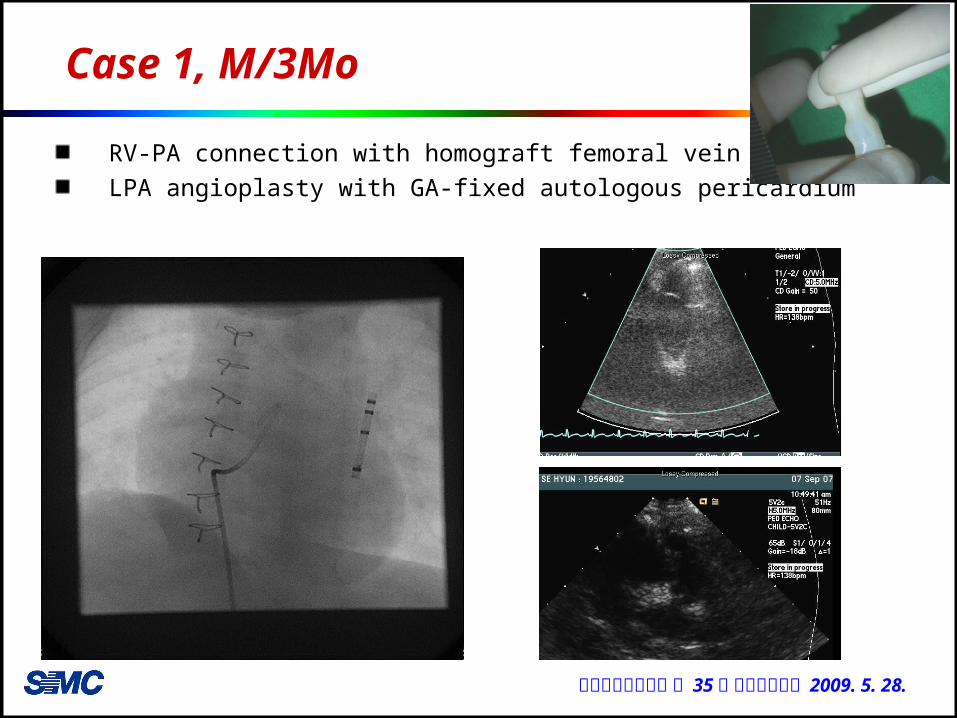
Case 1, M/3Mo
RV-PA connection with homograft femoral vein 7mmLPA angioplasty with GA-fixed autologous pericardium
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
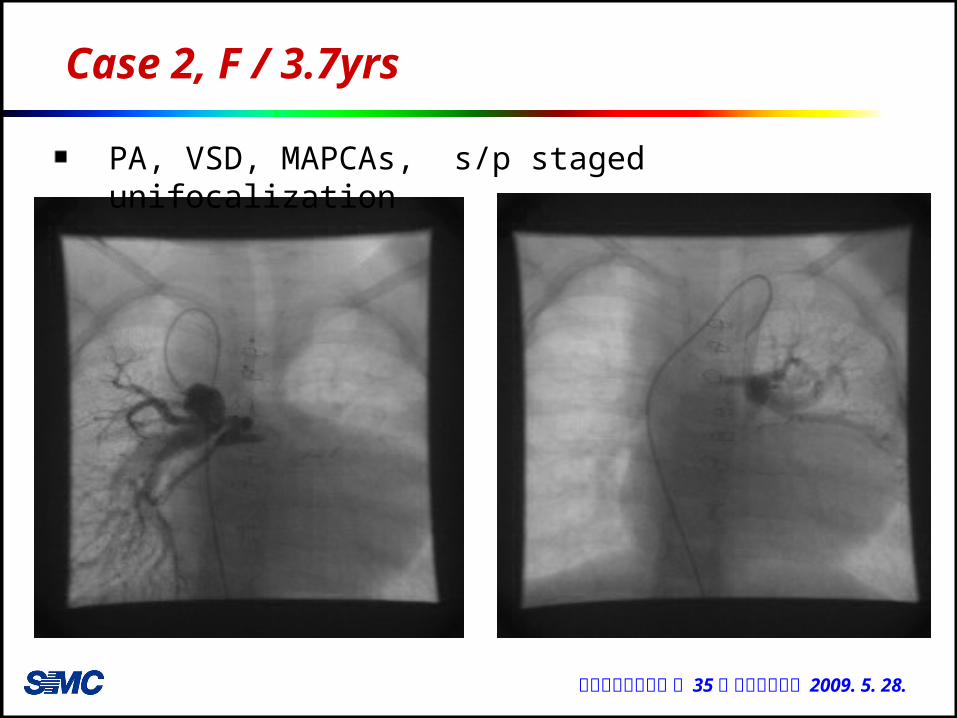
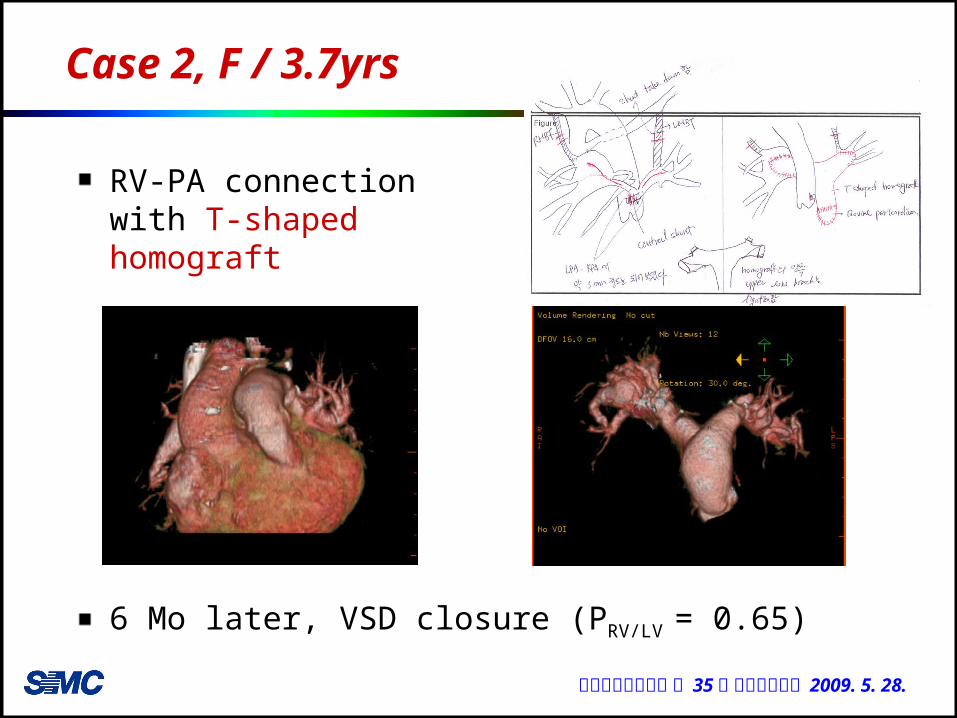
Case 2, F / 3.7yrs
PA, VSD, MAPCAs, s/p staged unifocalization
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
Case 2, F / 3.7yrs
6 Mo later, VSD closure (PRV/LV = 0.65)
RV-PA connection with T-shaped homograft
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
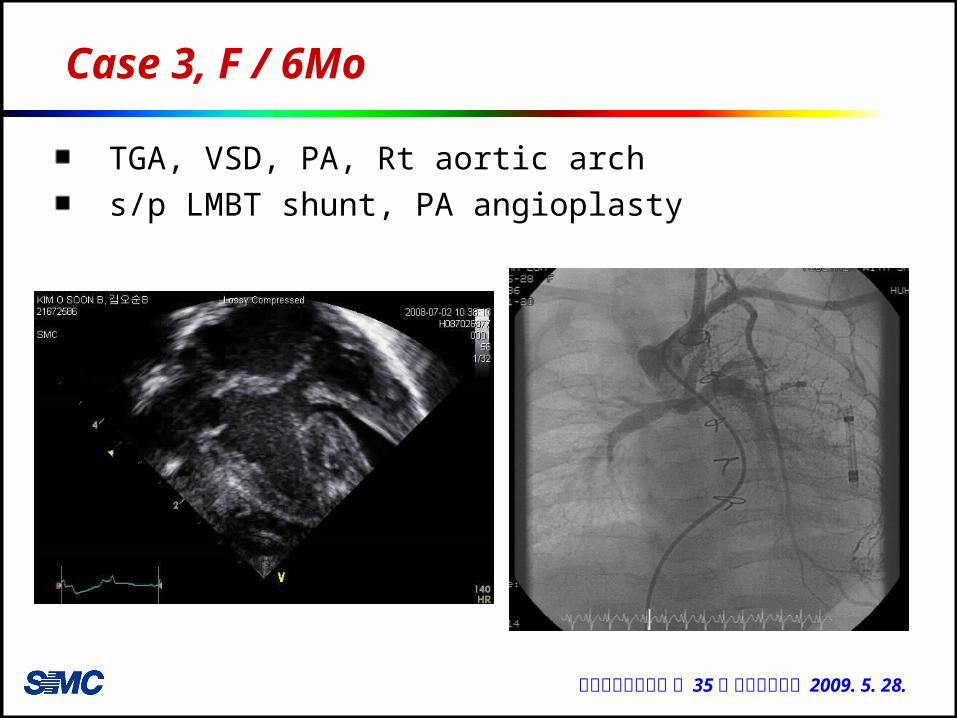
Case 3, F / 6Mo
TGA, VSD, PA, Rt aortic archs/p LMBT shunt, PA angioplasty
대한흉부외과학회 제 35 차 춘계학술대회 2009. 5. 28.
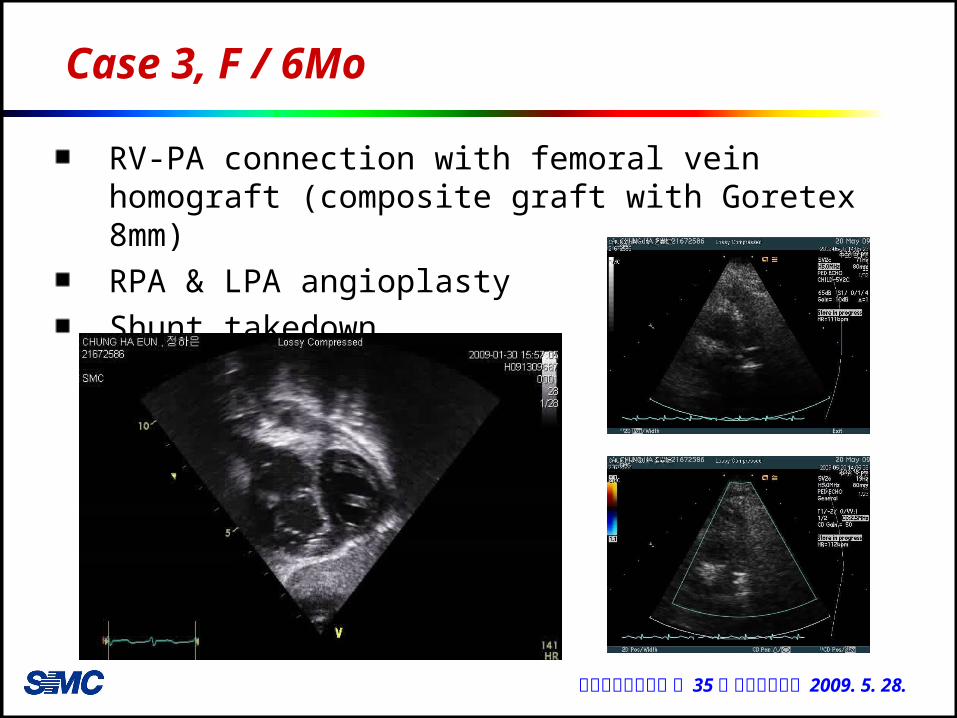
Case 3, F / 6Mo
RV-PA connection with femoral vein homograft (composite graft with Goretex 8mm)RPA & LPA angioplastyShunt takedown