Embed Size (px)
Citation preview

02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 1
รศ.พญ.สวุชิา อศิราดิสยักลุ แกว้ศิริหน่วยโสตวทิยา โสตประสาทวทิยาและการสื�อความหมาย
ภาควชิาโสต ศอ นาสกิวทิยาคณะแพทยศาสตร ์มหาวทิยาลยัเชียงใหม่
กระบวนวิชา พ.คพ.510 (331510) โสต ศอ นาสกิวิทยา
1ปีการศึกษา 2561s u w i c h a . k a e w s i r i @ c m u . a c . t h
2
วตัถปุระสงค์ เพื�อใหน้ักศึกษาสามารถ 1. มีความรู ้ความเขา้ใจเกี�ยวกบัสาเหต ุพยาธิกาํเนิด พยาธิสรรีวิทยา และพยาธิสภาพ ตลอดจนหลกัการวินิจฉยัสาเหต ุของการเกดิโรคของหชูั�นในและระบบทรงตวัในหชูั�นใน2. มีความรู ้ความเขา้ใจเกี�ยวกบักลไกการเกดิโรค สามารถใหก้ารวินิจฉยัแยกโรค และรูห้ลกัในการดูแลรกัษาผูป่้วยโรคของหชูั�นในและระบบทรงตวัในหชูั�นในเบื�องตน้ แกไ้ขปญัหาเฉพาะหนา้และตดัสนิใจสง่ผูป่้วยต่อไปยงัผูเ้ชี�ยวชาญไดอ้ย่างเหมาะสม 3. สามารถใหก้ารวินิจฉยัแยกโรค และรูห้ลกัในการดูแลรกัษาผูป่้วยโรคของหชูั�นในและระบบทรงตวัในหชูั�นในเบื�องตน้และตดัสนิใจสง่ผูป่้วยต่อไปยงัผูเ้ชี�ยวชาญได้อย่างเหมาะสม4. สามารถแปลผล audiogram ไดด้ว้ยตนเองอย่างถกูตอ้ง ออกเอกสารรบัรองความพกิาร โดยพจิารณาจากความบกพร่องทางการไดย้ินหรอืสื�อความหมายได้
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 2
3
Topic outline
Anatomy and physiology of the inner ear
& the vestibular system
Approach to the patient with vertigo
and hearing loss
Otoneurological examinations
Diseases of the inner ear & the vestibular system
Investigations in SNHL & vertigo
Rehabilitation: hearing & vestibular
SuwichaENT, CMU
Anatomy and physiology of inner ear, hearing &
balance system
4
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 3
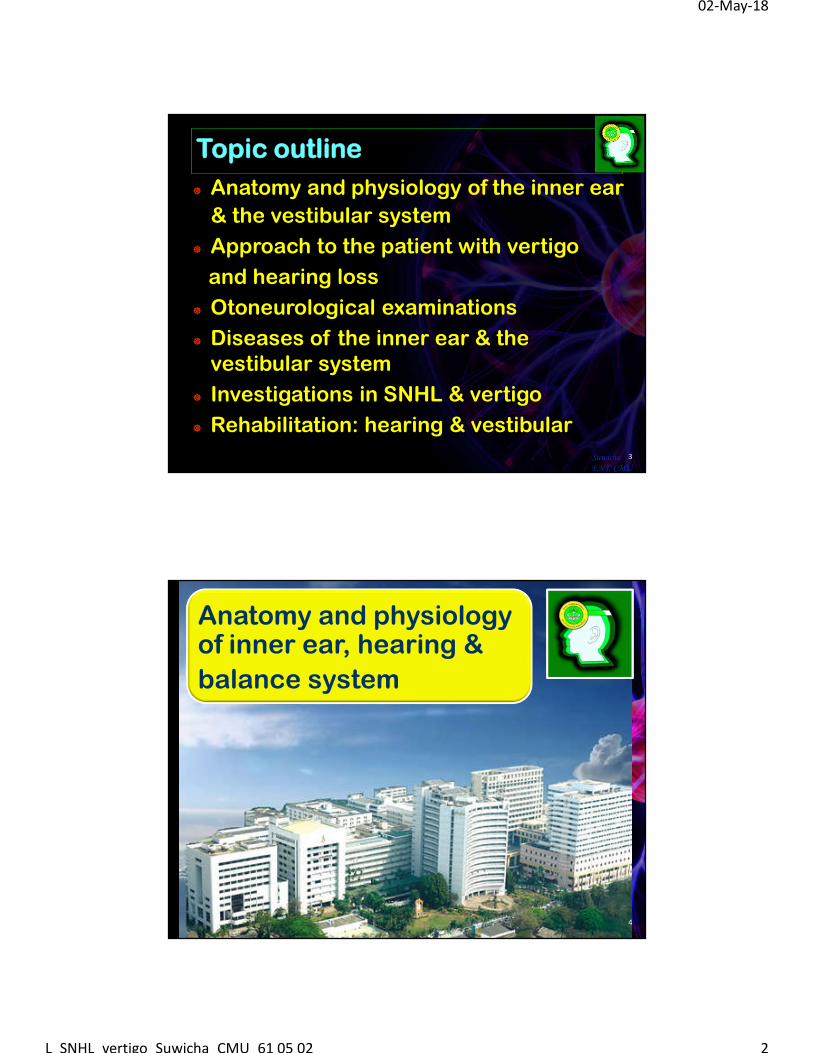
The ear: 3 parts
5SuwichaENT, CMU
หชูั�นนอก หชูั�นกลางหชูั�นใน
http://www.vestibular.org/images/ear_diagram_lg.gif
vertigo
SNHL
Vertigo = illusory sensation of motion
Hearing: auditory pathway
6SuwichaENT, CMU
http://www.musicearth.name/wp-content/uploads/2011/02/afferent-auditory-pathways.jpghttp://www.musicearth.name/wp-content/uploads/2011/02/efferent-auditory-pathways.jpg
Peripheral/cochlea
Central/retrocochlear
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 4
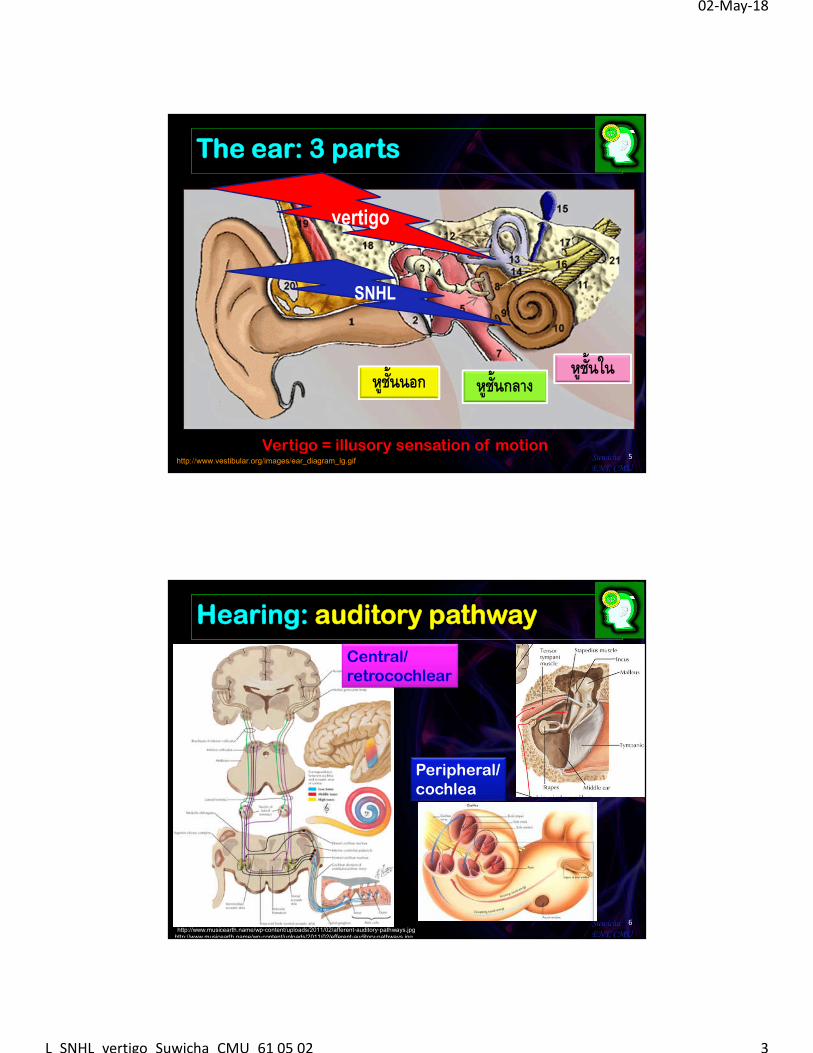
Hearing: Cochlea
7SuwichaENT, CMU
http://2.bp.blogspot.com/-endMCu_scPc/TpG7pQIXVwI/AAAAAAAAAME/NbdmBbPJ0R0/s1600/Cochlea_cross_section.jpghttps://forum.facmedicine.com/threads/histology-of-the-ear-explained.25373/
Hair cells Depolarization Nerve conduction
organ of corti
Scala media
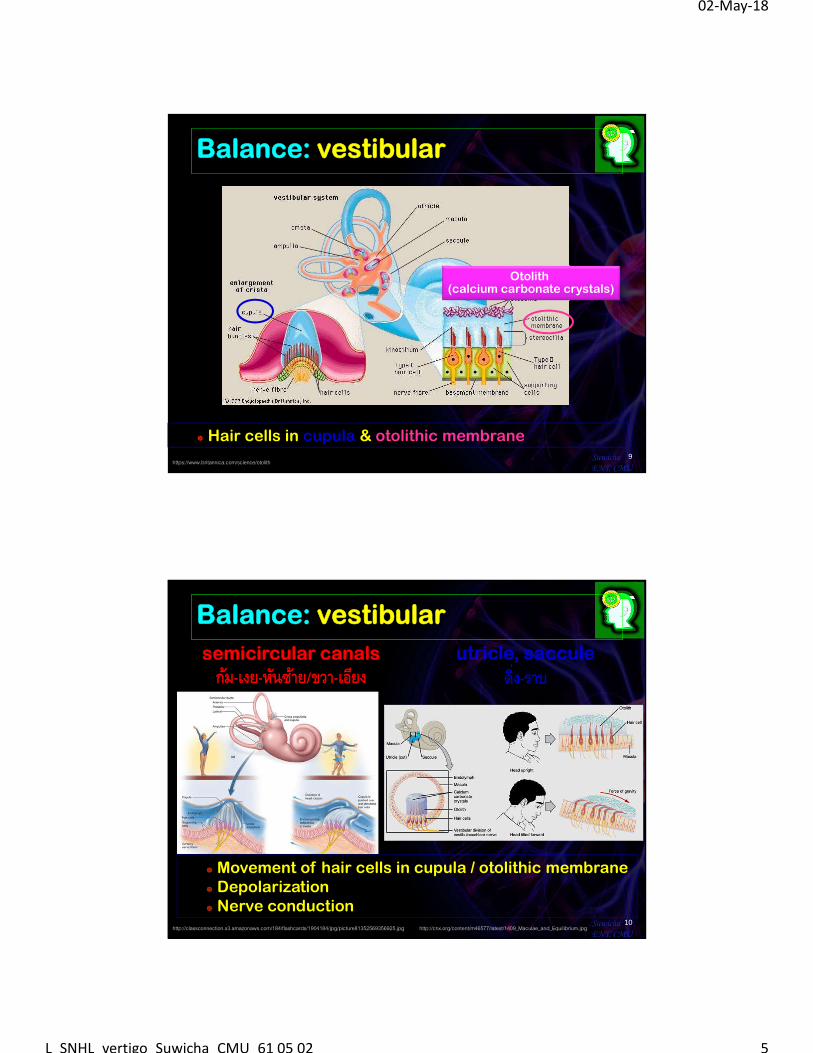
8
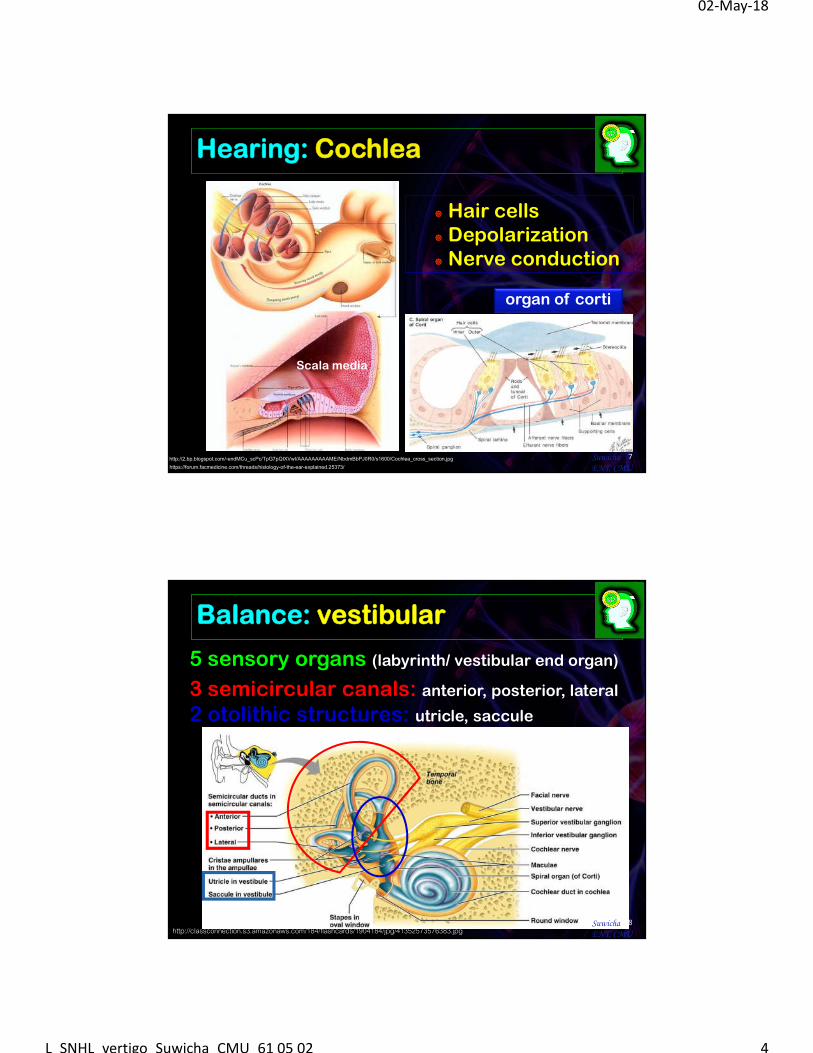
Balance: vestibular
5 sensory organs (labyrinth/ vestibular end organ)
http://classconnection.s3.amazonaws.com/184/flashcards/1904184/jpg/41352573576383.jpg SuwichaENT, CMU
3 semicircular canals: anterior, posterior, lateral
2 otolithic structures: utricle, saccule
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 5
9https://www.britannica.com/science/otolith
SuwichaENT, CMU
Hair cells in cupula & otolithic membrane
Balance: vestibular
Otolith (calcium carbonate crystals)
10http://classconnection.s3.amazonaws.com/184/flashcards/1904184/jpg/picture81352569356925.jpg http://cnx.org/content/m46577/latest/1409_Maculae_and_Equilibrium.jpg
SuwichaENT, CMU
Movement of hair cells in cupula / otolithic membrane Depolarization Nerve conduction
semicircular canals
กม้-เงย-หนัซา้ย/ขวา-เอยีงutricle, saccule
ดิ�ง-ราบ
Balance: vestibular
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 6
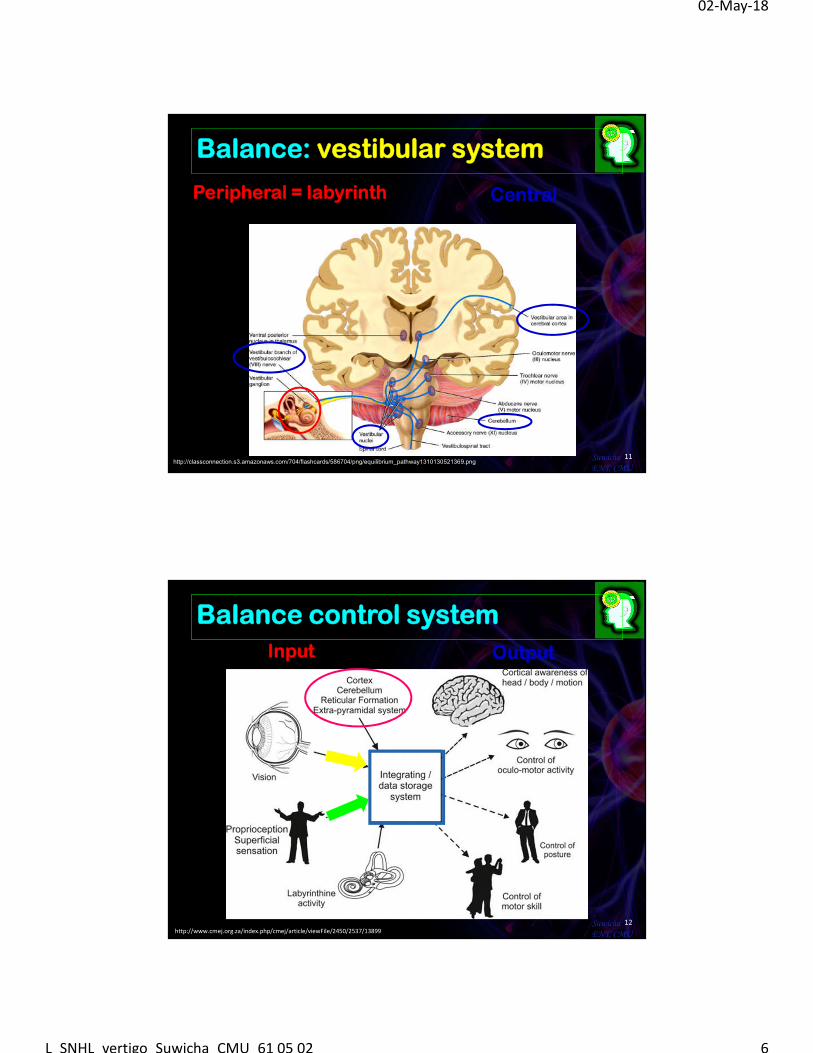
11SuwichaENT, CMU
Peripheral = labyrinth Central
Balance: vestibular system
http://classconnection.s3.amazonaws.com/704/flashcards/586704/png/equilibrium_pathway1310130521369.png
12SuwichaENT, CMU
Input Output
Balance control system
http://www.cmej.org.za/index.php/cmej/article/viewFile/2450/2537/13899
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 7
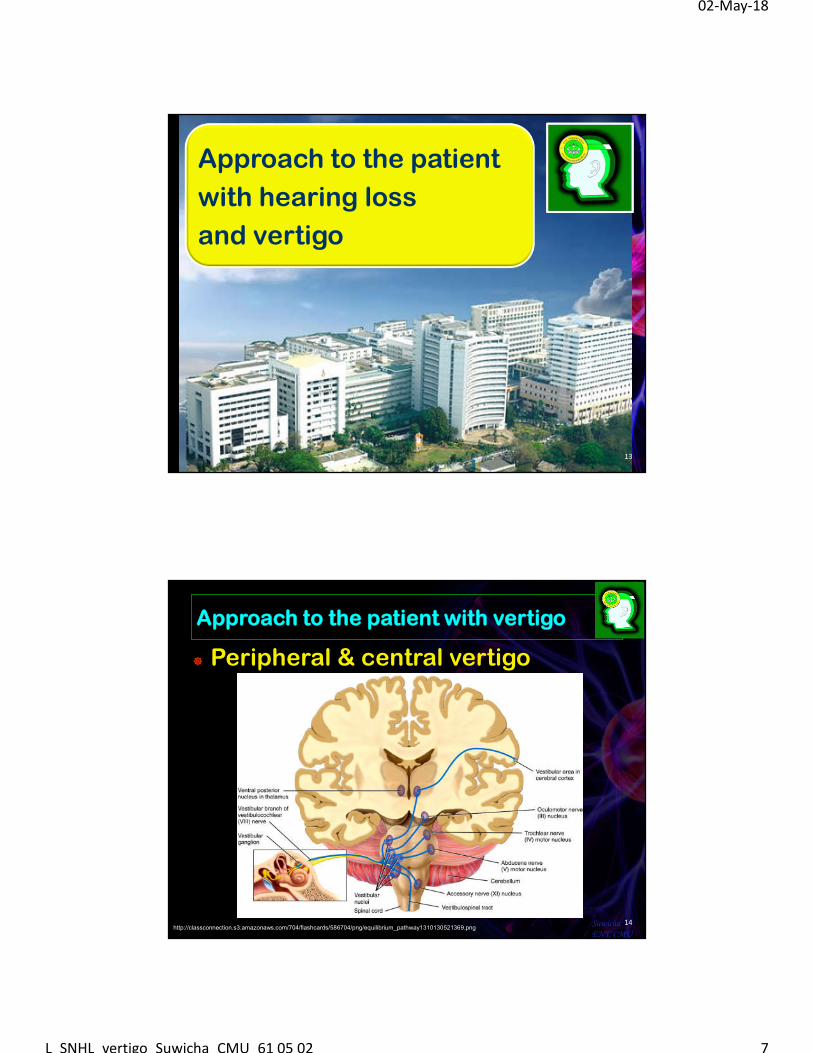
Approach to the patient
with hearing loss
and vertigo
13
Approach to the patient with vertigo
Peripheral & central vertigo
14SuwichaENT, CMU
http://classconnection.s3.amazonaws.com/704/flashcards/586704/png/equilibrium_pathway1310130521369.png
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 8
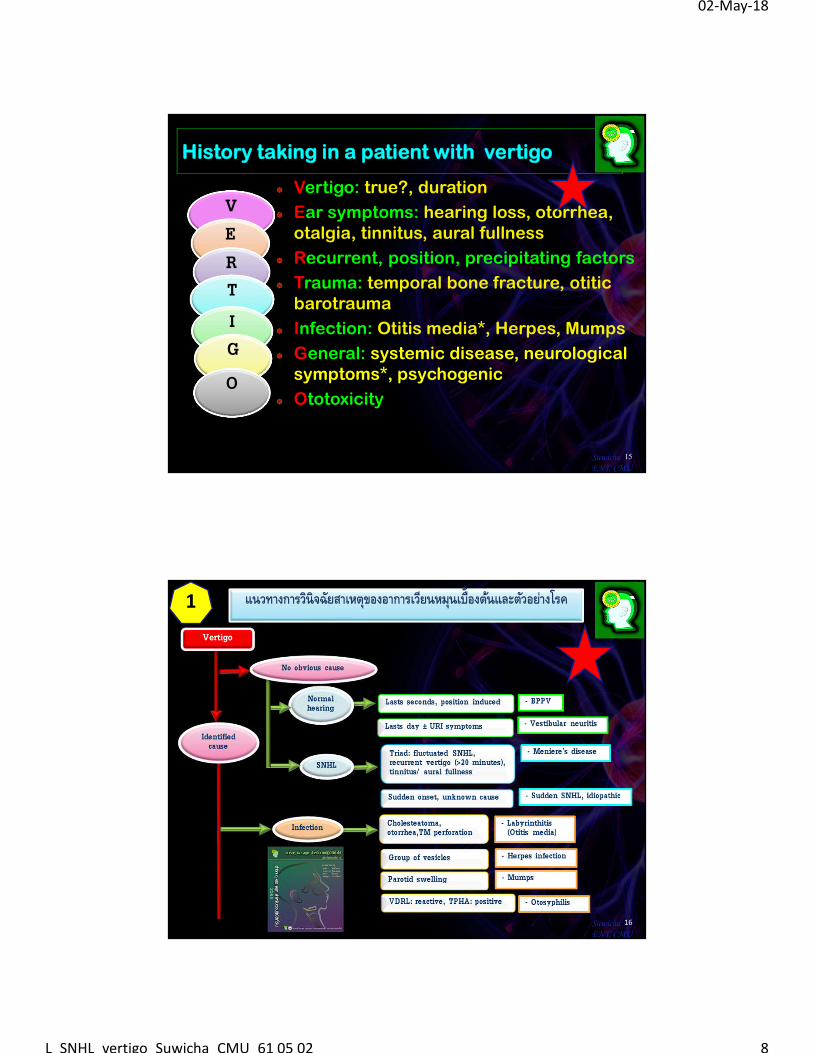
V
History taking in a patient with vertigo
Vertigo: true?, duration
Ear symptoms: hearing loss, otorrhea, otalgia, tinnitus, aural fullness
Recurrent, position, precipitating factors
Trauma: temporal bone fracture, otiticbarotrauma
Infection: Otitis media*, Herpes, Mumps
General: systemic disease, neurological symptoms*, psychogenic
Ototoxicity
15SuwichaENT, CMU
ERTIG
O
16SuwichaENT, CMU
1 แนวทางการวนิิจฉยัสาเหตขุองอาการเวยีนหมนุเบื�องตน้และตวัอยา่งโรค
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 9
1717SuwichaENT, CMU
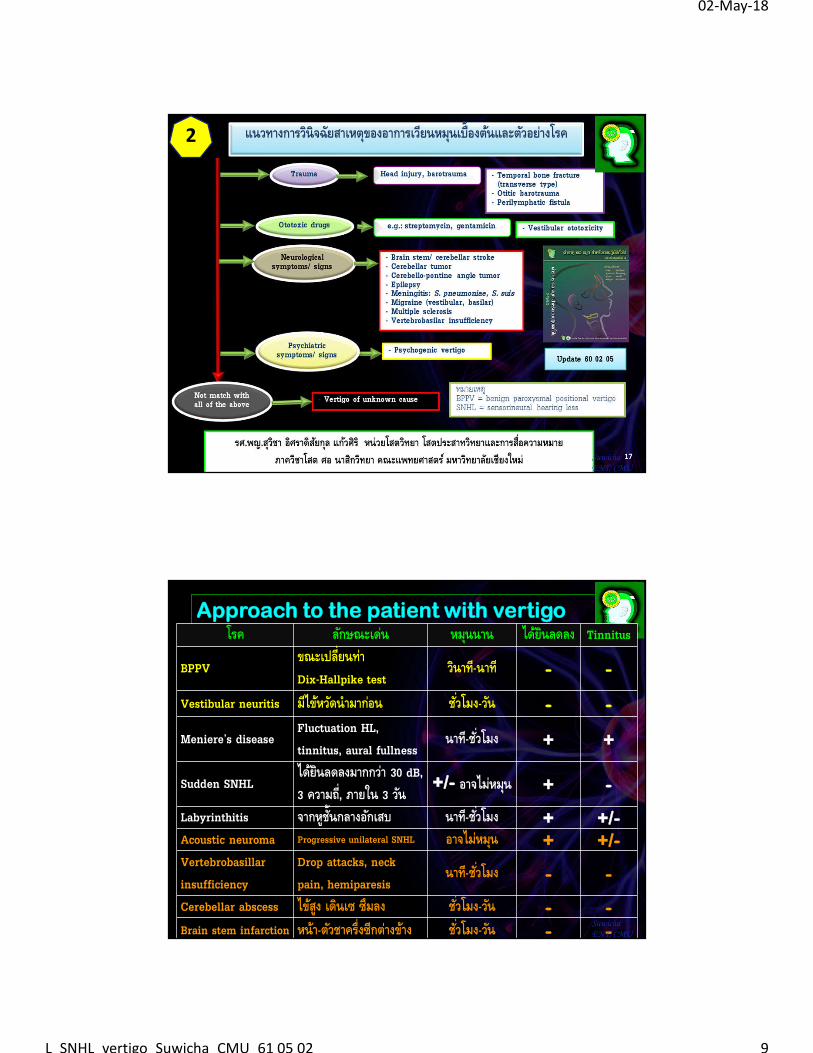
2 แนวทางการวนิิจฉยัสาเหตขุองอาการเวยีนหมนุเบื�องตน้และตวัอยา่งโรค
Approach to the patient with vertigoโรค ลกัษณะเด่น หมนุนาน ไดย้นิลดลง Tinnitus
BPPVขณะเปลี�ยนทา่ Dix-Hallpike test
วนิาท-ีนาที - -
Vestibular neuritis มีไขห้วดันํามากอ่น ชั �วโมง-วนั - -
Meniere’s diseaseFluctuation HL, tinnitus, aural fullness
นาท-ีชั �วโมง + +
Sudden SNHLไดย้นิลดลงมากกวา่ 30 dB, 3 ความถี�, ภายใน 3 วนั
+/- อาจไม่หมนุ + -
Labyrinthitis จากหูชั�นกลางอกัเสบ นาท-ีชั �วโมง + +/-Acoustic neuroma Progressive unilateral SNHL อาจไม่หมนุ + +/-Vertebrobasillarinsufficiency
Drop attacks, neck pain, hemiparesis
นาท-ีชั �วโมง - -
Cerebellar abscess ไขสู้ง เดินเซ ซึมลง ชั �วโมง-วนั - -Brain stem infarction หนา้-ตวัชาครึ�งซีกตา่งขา้ง ชั �วโมง-วนั - -
SuwichaENT, CMU
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 10
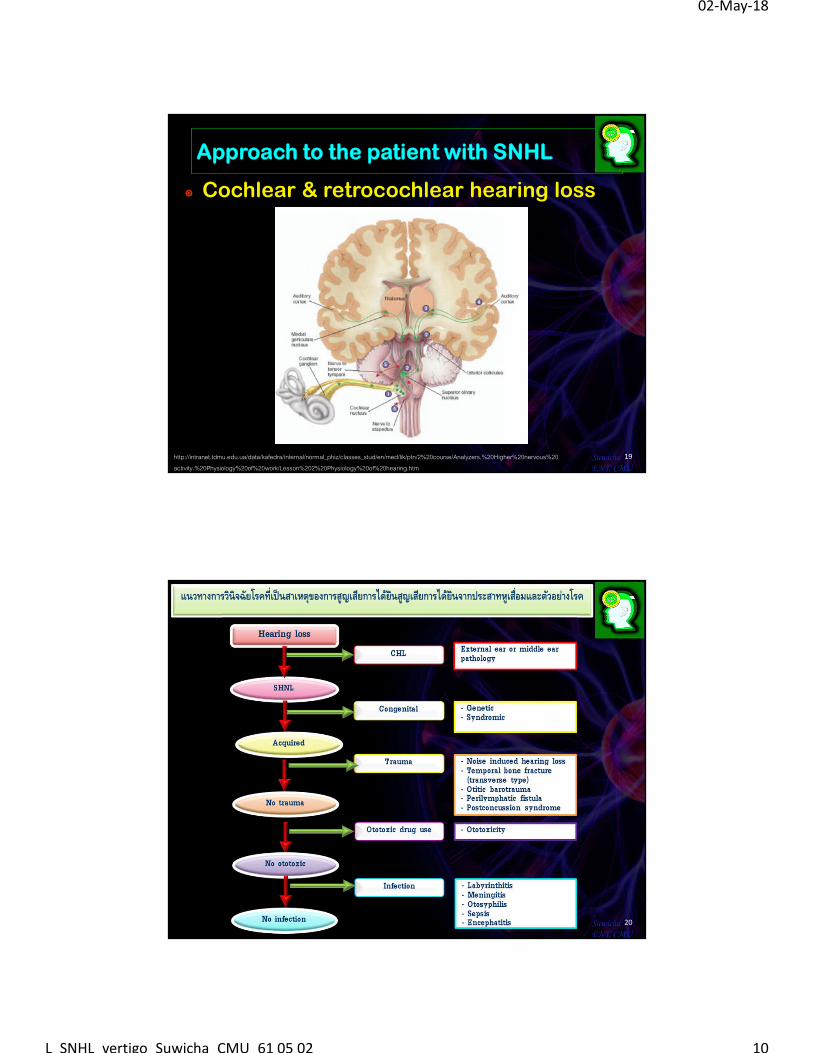
Approach to the patient with SNHL
Cochlear & retrocochlear hearing loss
19SuwichaENT, CMU
http://intranet.tdmu.edu.ua/data/kafedra/internal/normal_phiz/classes_stud/en/med/lik/ptn/2%20course/Analyzers.%20Higher%20nervous%20activity.%20Physiology%20of%20work/Lesson%202%20Physiology%20of%20hearing.htm
20SuwichaENT, CMU
แนวทางการวินิจฉัยโรคที�เป็นสาเหตขุองการสูญเสยีการไดย้นิสูญเสยีการไดย้นิจากประสาทหูเสื�อมและตวัอยา่งโรค
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 11
21SuwichaENT, CMU
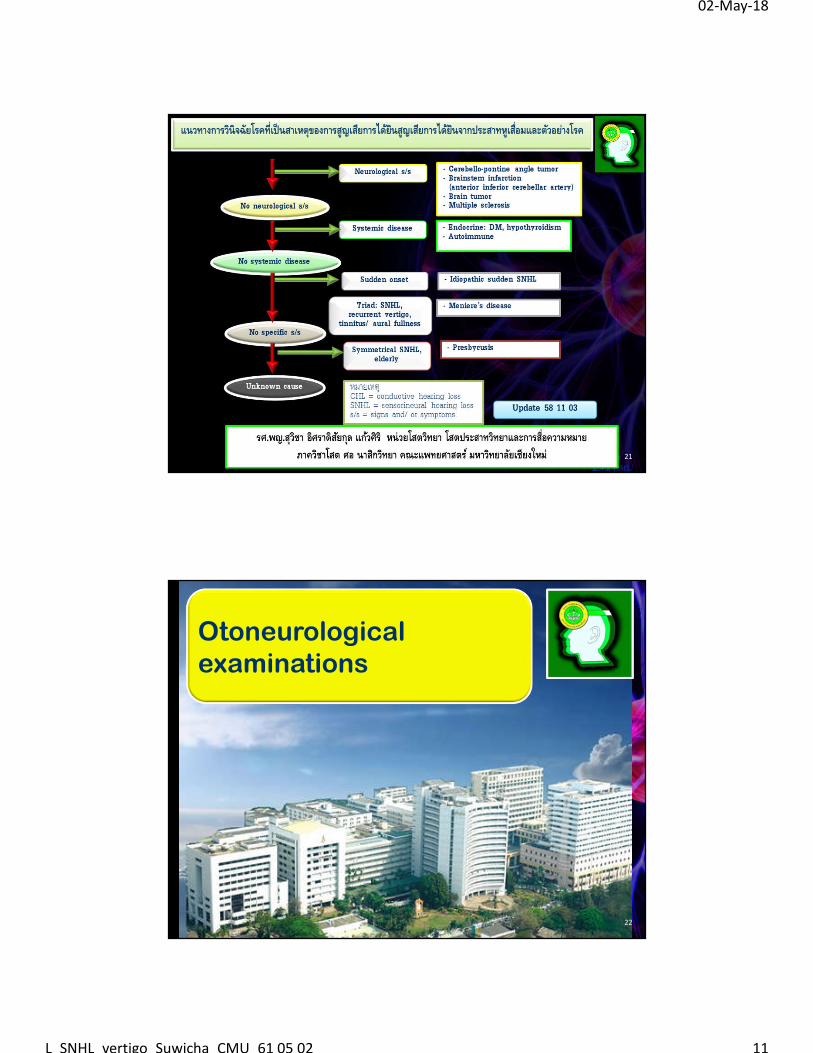
แนวทางการวินิจฉัยโรคที�เป็นสาเหตขุองการสูญเสยีการไดย้นิสูญเสยีการไดย้นิจากประสาทหูเสื�อมและตวัอยา่งโรค
Otoneurologicalexaminations
22
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 12
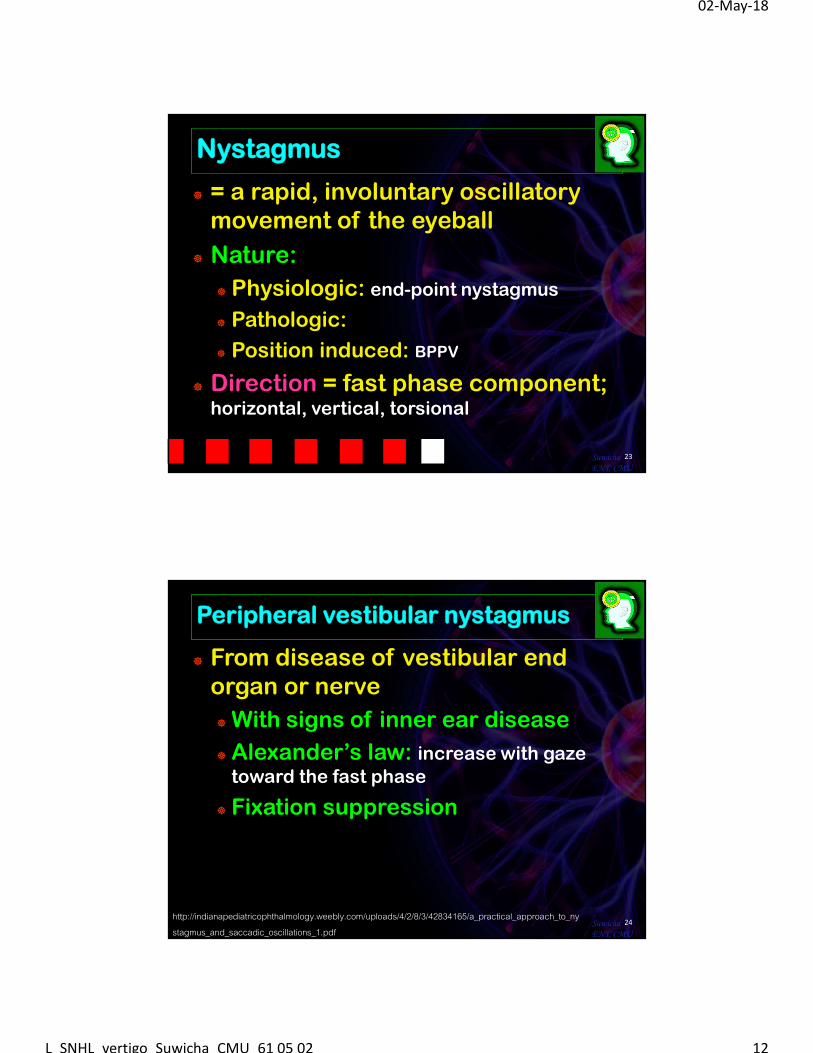
Nystagmus
= a rapid, involuntary oscillatory movement of the eyeball
Nature:
Physiologic: end-point nystagmus
Pathologic:
Position induced: BPPV
Direction = fast phase component; horizontal, vertical, torsional
23SuwichaENT, CMU
Peripheral vestibular nystagmus
From disease of vestibular end organ or nerve
With signs of inner ear disease
Alexander’s law: increase with gaze toward the fast phase
Fixation suppression
24SuwichaENT, CMU
http://indianapediatricophthalmology.weebly.com/uploads/4/2/8/3/42834165/a_practical_approach_to_nystagmus_and_saccadic_oscillations_1.pdf
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 13
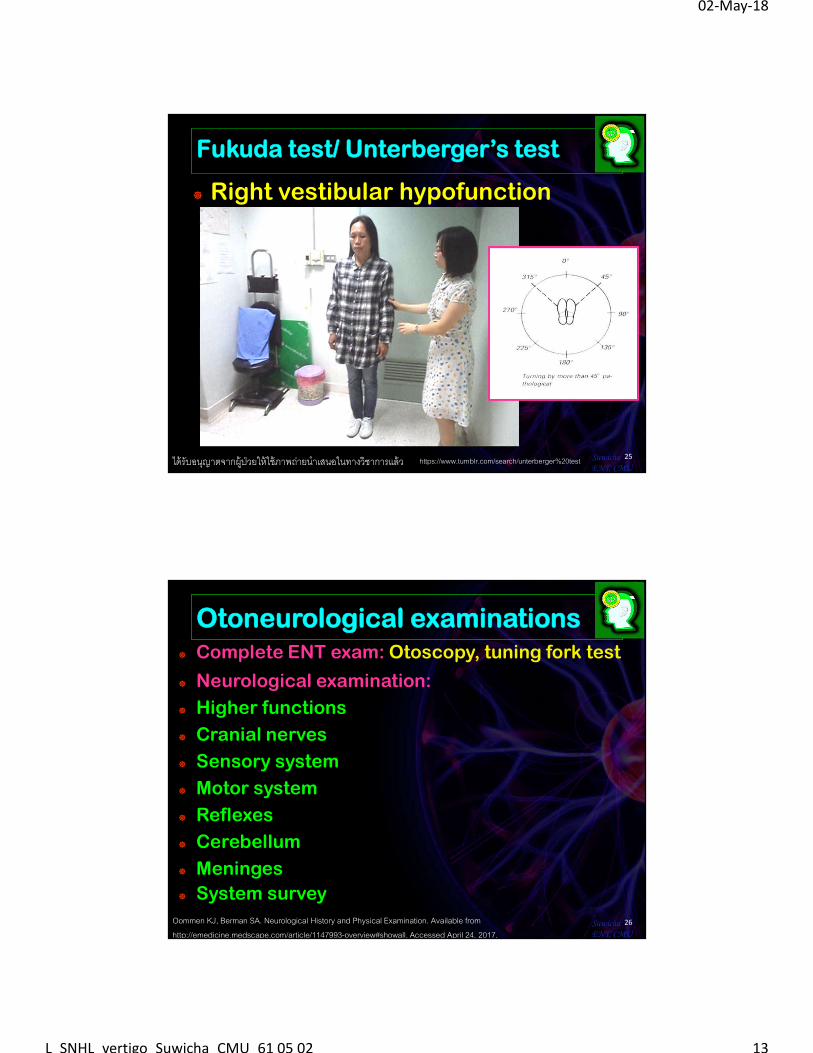
Fukuda test/ Unterberger’s test
Right vestibular hypofunction
25SuwichaENT, CMU
ได้รับอนญุาตจากผู้ ป่วยให้ใช้ภาพถ่ายนําเสนอในทางวิชาการแล้ว https://www.tumblr.com/search/unterberger%20test
Otoneurological examinations Complete ENT exam: Otoscopy, tuning fork test
Neurological examination:
Higher functions
Cranial nerves
Sensory system
Motor system
Reflexes
Cerebellum
Meninges
System survey
26SuwichaENT, CMU
Oommen KJ, Berman SA. Neurological History and Physical Examination. Available from http://emedicine.medscape.com/article/1147993-overview#showall. Accessed April 24, 2017.
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 14
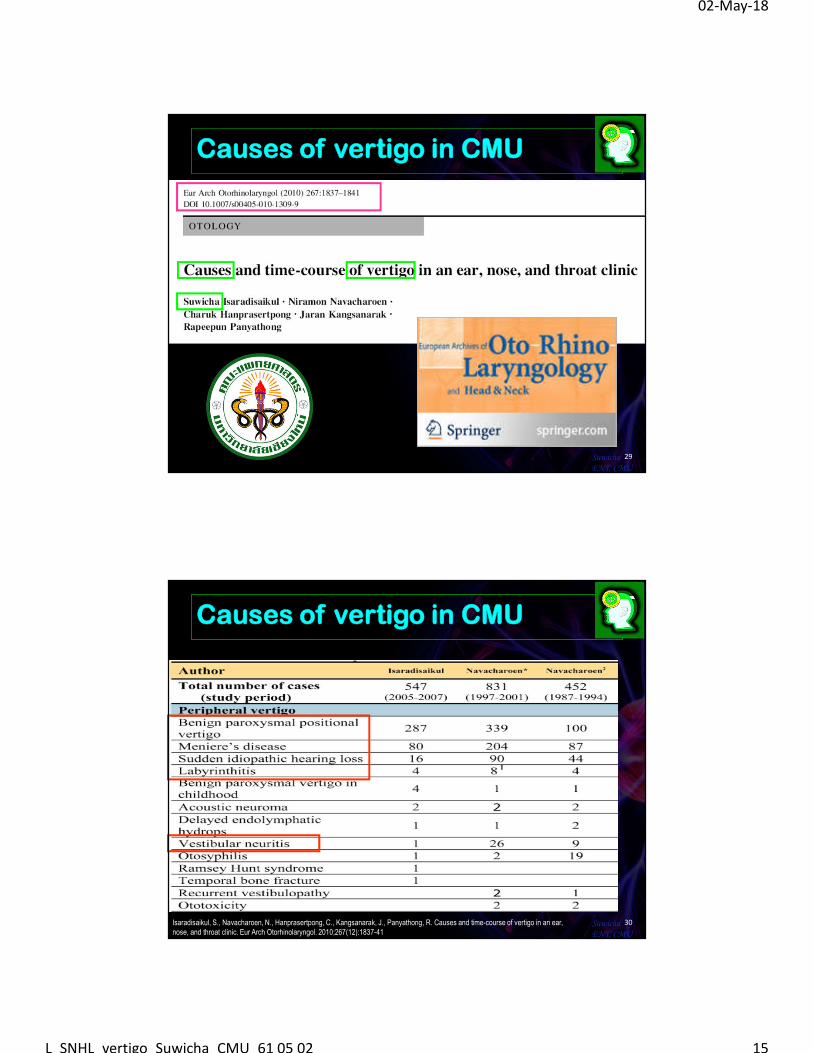
Otoneurological examinations Vestibuloocular pathway:
nystagmus
head thrust test
head shaking test: 2 Hz, 20 seconds
Vestibulospinal pathway:
Romberg, sharpened/Tandem Romberg test
Tandem walk
Fukuda test (Unterberger’s test)
Specific test:
Positioning test: Dix-Hallpike test, supine roll test
27SuwichaENT, CMU
http://www.physio-pedia.com/Romberg_Test#The_Sharpened_or_Tandem_Romberg_test
Diseases of the inner ear & the vestibular system
28
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 15
Causes of vertigo in CMU
29SuwichaENT, CMU
Causes of vertigo in CMU
30SuwichaENT, CMU
Isaradisaikul, S., Navacharoen, N., Hanprasertpong, C., Kangsanarak, J., Panyathong, R. Causes and time-course of vertigo in an ear, nose, and throat clinic. Eur Arch Otorhinolaryngol. 2010;267(12):1837-41
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 16
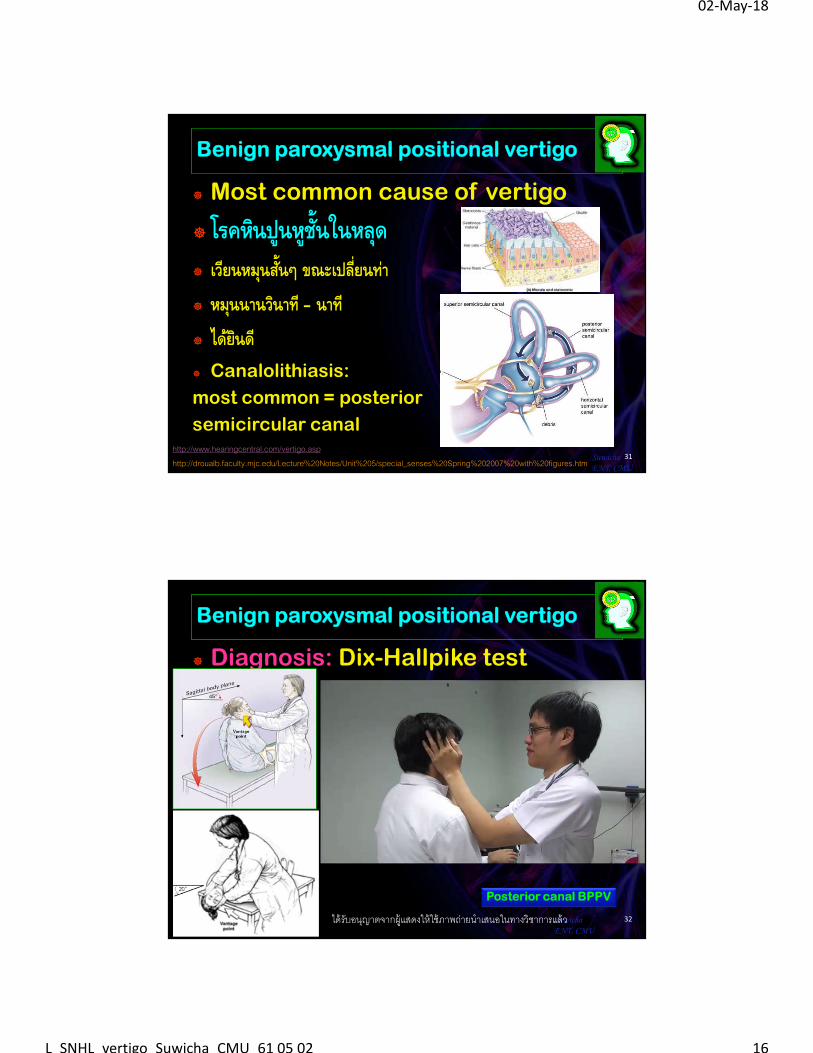
Benign paroxysmal positional vertigo
Most common cause of vertigo
โรคหนิปูนหชูั�นในหลดุ เวยีนหมนุส ั�นๆ ขณะเปลี�ยนท่า
หมนุนานวนิาท ี– นาที
ไดย้นิดี
Canalolithiasis:
most common = posterior
semicircular canal
31SuwichaENT, CMU
http://www.hearingcentral.com/vertigo.asphttp://droualb.faculty.mjc.edu/Lecture%20Notes/Unit%205/special_senses%20Spring%202007%20with%20figures.htm
Benign paroxysmal positional vertigo
Diagnosis: Dix-Hallpike test
32SuwichaENT, CMU
Posterior canal BPPV
ได้รับอนญุาตจากผู้แสดงให้ใช้ภาพถ่ายนําเสนอในทางวิชาการแล้ว
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 17
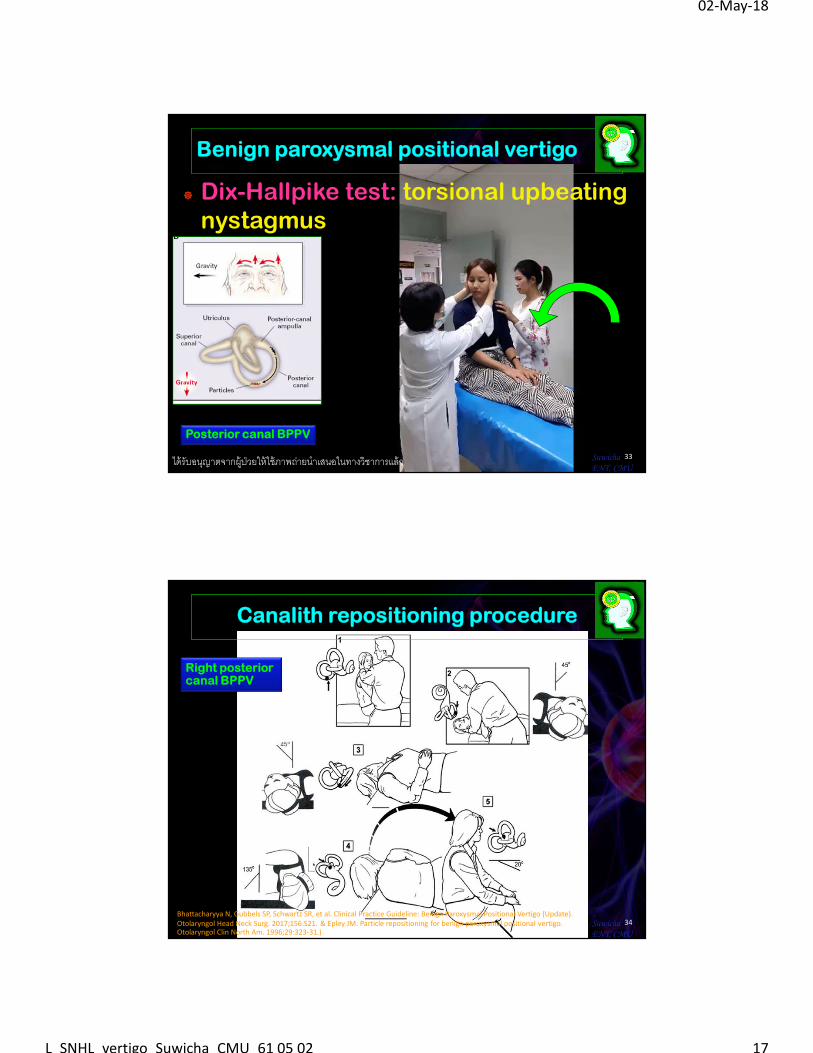
Dix-Hallpike test: torsional upbeatingnystagmus
Benign paroxysmal positional vertigo
33SuwichaENT, CMU
ได้รับอนญุาตจากผู้ ป่วยให้ใช้ภาพถ่ายนําเสนอในทางวิชาการแล้ว
Posterior canal BPPV
Canalith repositioning procedure
34SuwichaENT, CMU
Right posterior canal BPPV
Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol Head Neck Surg. 2017;156:S21. & Epley JM. Particle repositioning for benign paroxysmal positional vertigo. Otolaryngol Clin North Am. 1996;29:323-31.)
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 18
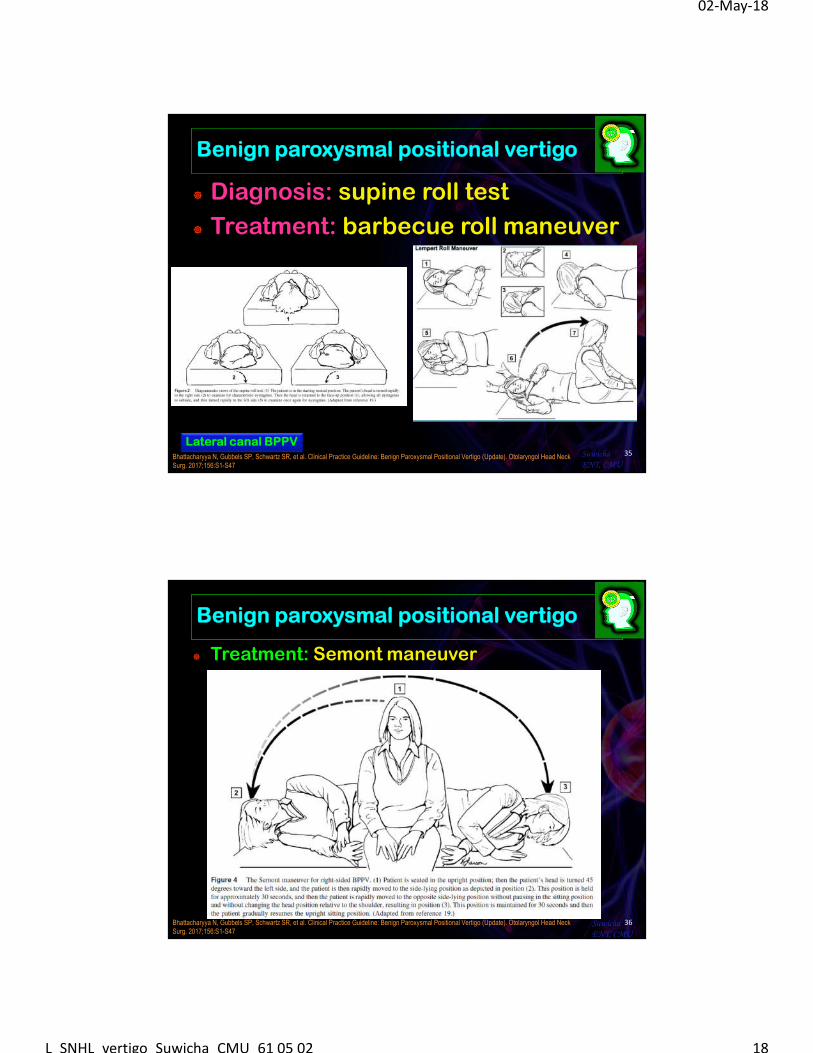
Benign paroxysmal positional vertigo
Diagnosis: supine roll test
Treatment: barbecue roll maneuver
35SuwichaENT, CMU
Lateral canal BPPVBhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol Head Neck Surg. 2017;156:S1-S47
Benign paroxysmal positional vertigo
Treatment: Semont maneuver
36SuwichaENT, CMU
Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol Head Neck Surg. 2017;156:S1-S47
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 19
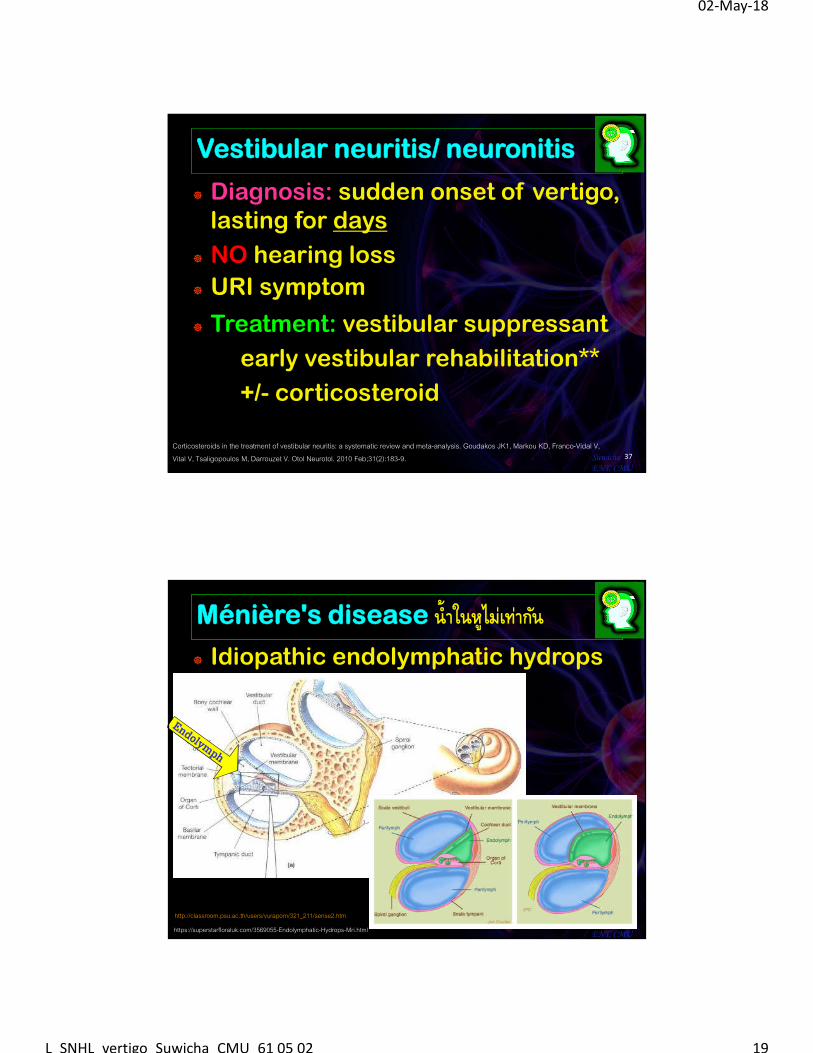
Vestibular neuritis/ neuronitis
Diagnosis: sudden onset of vertigo, lasting for days
NO hearing loss
URI symptom
Treatment: vestibular suppressant
early vestibular rehabilitation**
+/- corticosteroid
37SuwichaENT, CMU
Corticosteroids in the treatment of vestibular neuritis: a systematic review and meta-analysis. Goudakos JK1, Markou KD, Franco-Vidal V, Vital V, Tsaligopoulos M, Darrouzet V. Otol Neurotol. 2010 Feb;31(2):183-9.
Ménière's disease นํ�าในหไูม่เท่ากนั
Idiopathic endolymphatic hydrops
38SuwichaENT, CMU
http://classroom.psu.ac.th/users/vuraporn/321_211/sense2.htm
https://superstarfloraluk.com/3569055-Endolymphatic-Hydrops-Mri.html
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 20
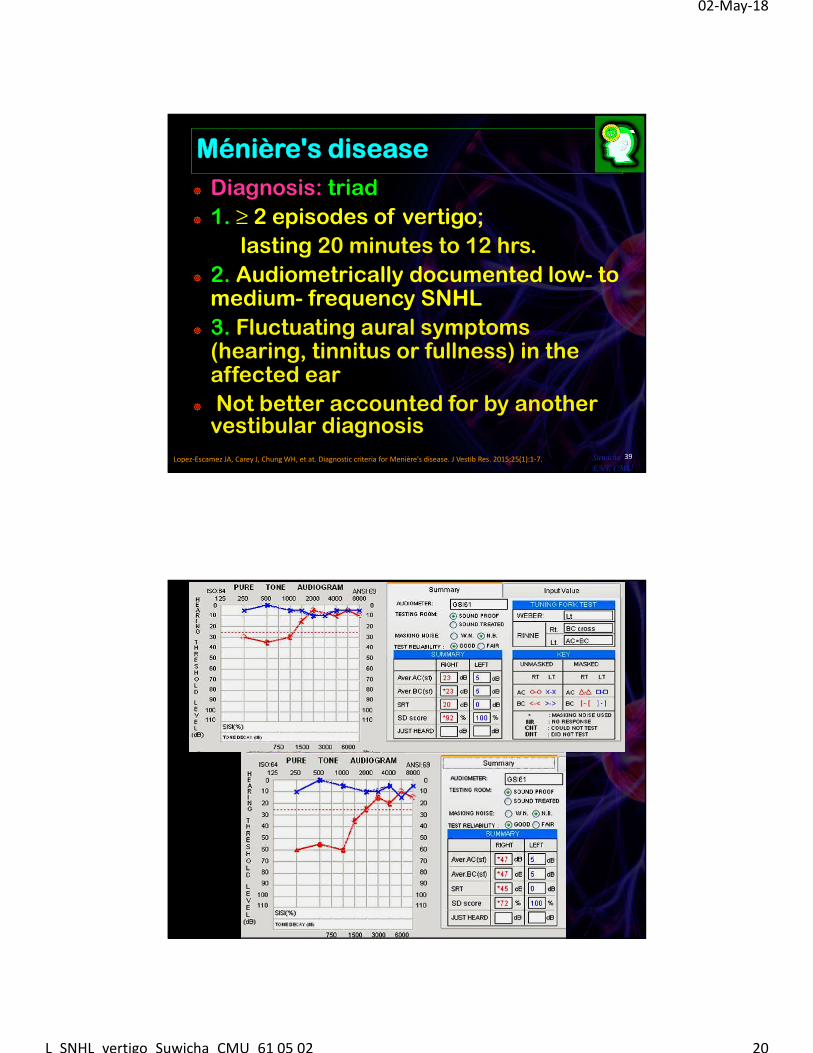
Ménière's disease
Diagnosis: triad
1. ≥ 2 episodes of vertigo;
lasting 20 minutes to 12 hrs.
2. Audiometrically documented low- to medium- frequency SNHL
3. Fluctuating aural symptoms (hearing, tinnitus or fullness) in the affected ear
Not better accounted for by another vestibular diagnosis
39SuwichaENT, CMU
Lopez-Escamez JA, Carey J, Chung WH, et at. Diagnostic criteria for Menière's disease. J Vestib Res. 2015;25(1):1-7.
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 21
Ménière's disease
Treatment:
Salt restriction & diuretics
Vasodilator: betahistine
Symptomatic: Antivertiginous, antiemetics, sedatives, antidepressants, and psychiatric treatment
Intratympanic injection: gentamicin, dexamethasone
Surgery: endolymphatic sac shunt, vestibular nerve
section, labyrintectomy
41SuwichaENT, CMU
Crane BT, Minor LB. Peripheral vestibular disorders. In: Flint PW, Haughey BH, Lund VJ, Niparko JK, Robbins TK, Thomas RJ, Lesperance MM. Cummings Otolaryngology: Head and Neck Surgery. 6th edition. Philadelphia: Elsevier, Saunders; 2015. p.2548-2566.
Sudden SNHL
Rule of 3
Sudden onset of hearing loss < 3 days
Audiogram: PTA > 30 dBHL, 3 freq.
40% with vertigo
Most common = idiopathic
**Need to identify causes if: with neurologic symptoms, both ears, recurrent hearing loss
42SuwichaENT, CMU
Stachler RJ, Chandrasekhar SS, Archer SM, et al. Clinical practice guideline: sudden hearing loss. Otolaryngol Head Neck Surg. 2012;146(3 Suppl):S1-35.
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 22
Idiopathic sudden SNHL
Possible etiologies: viral infection, vascular
impairment, inner ear/ CNS pathology, autoimmune
Diagnosis: audiogram, VDRL, TPHA, ABR, etc.
Treatment: No concensus,
1st do no harm
1/3-2/3 spontaneous improvement
Oral corticosteroid 1 mg/kg/d 7-14 days
Intratympanic steroid injection
Hyperbaric oxygen43Suwicha
ENT, CMUStachler RJ, Chandrasekhar SS, Archer SM, et al. Clinical practice guideline: sudden hearing loss. Otolaryngol Head Neck Surg. 2012;146(3 Suppl):S1-35.
Labyrinthitis: หชูั�นในอกัเสบ
Virus: mumps, herpes zoster
Bacteria: otitis media**
postmeningitis deafness
Fungus
Treponema: otosyphilis
Diagnosis: SNHL, vertigo, specific signs & symptoms
Treatment: specific disease44Suwicha
ENT, CMU
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 23
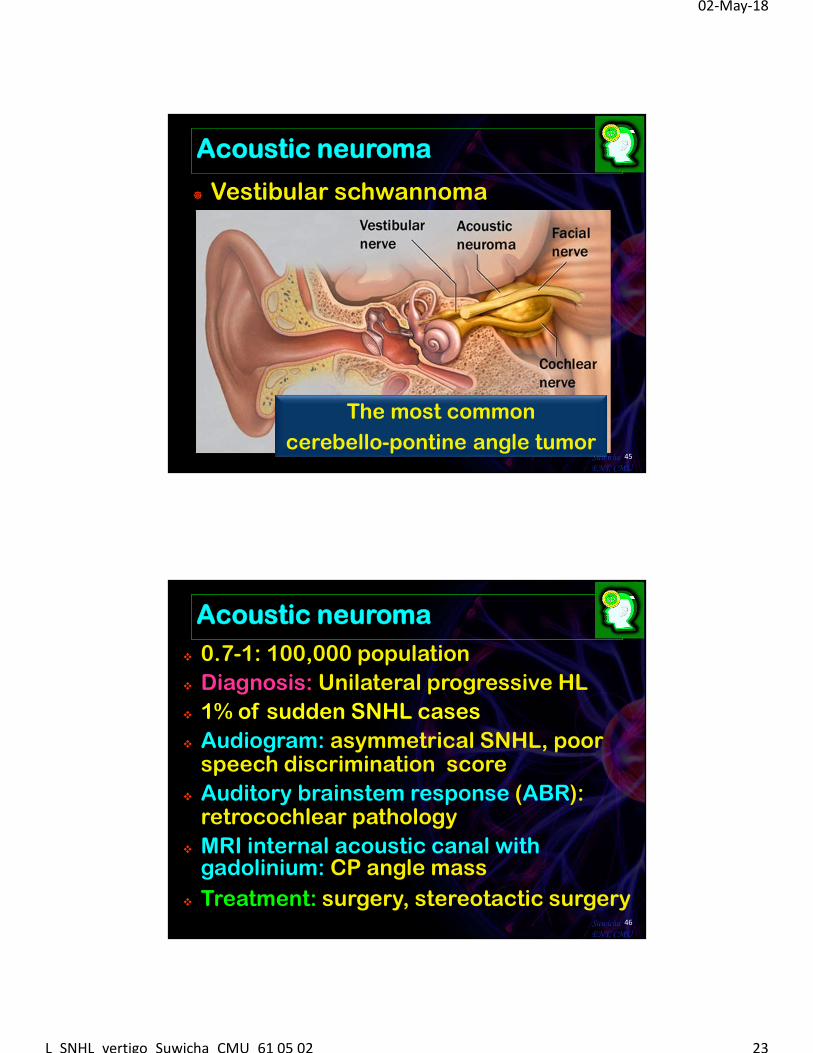
Acoustic neuroma
Vestibular schwannoma
45SuwichaENT, CMU
The most common
cerebello-pontine angle tumor
Acoustic neuroma
0.7-1: 100,000 population
Diagnosis: Unilateral progressive HL
1% of sudden SNHL cases
Audiogram: asymmetrical SNHL, poor speech discrimination score
Auditory brainstem response (ABR): retrocochlear pathology
MRI internal acoustic canal with gadolinium: CP angle mass
Treatment: surgery, stereotactic surgery46Suwicha
ENT, CMU
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 24
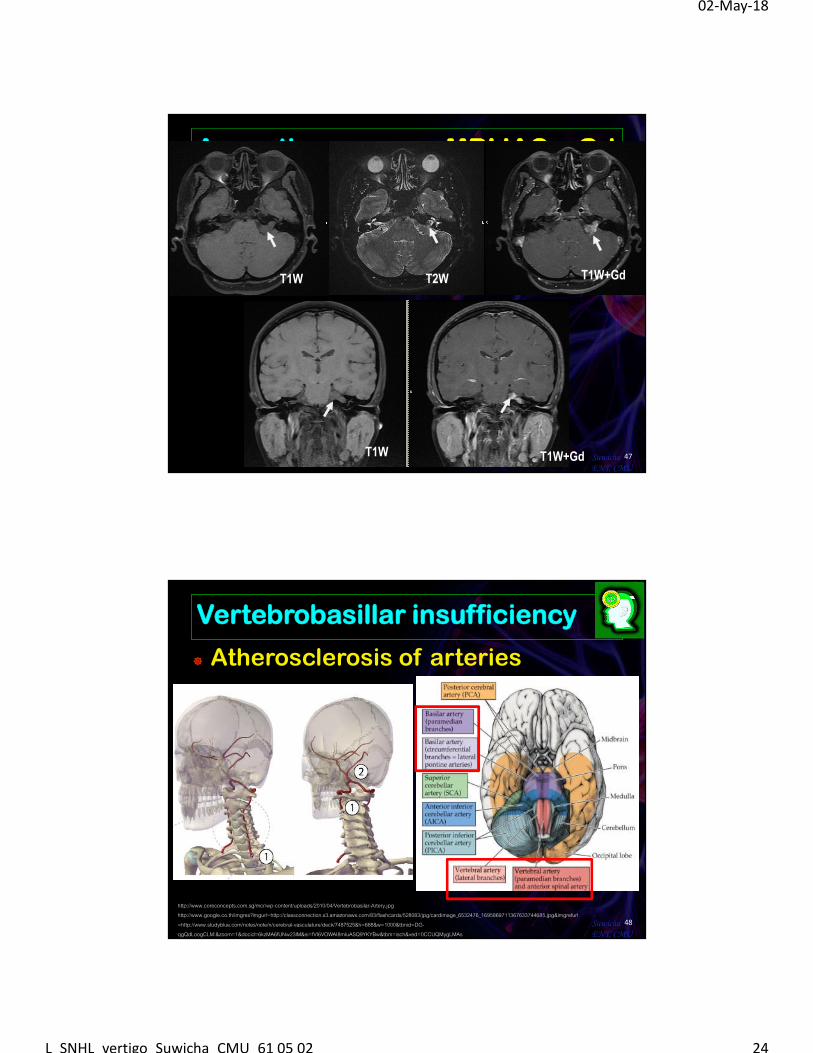
Acoustic neuroma; MRI IAC + Gd
47SuwichaENT, CMU
T1W T2W T1W+Gd
T1W T1W+Gd
Vertebrobasillar insufficiency
Atherosclerosis of arteries
48SuwichaENT, CMU
http://www.coreconcepts.com.sg/mcr/wp-content/uploads/2010/04/Vertebrobasilar-Artery.jpghttp://www.google.co.th/imgres?imgurl=http://classconnection.s3.amazonaws.com/83/flashcards/528083/jpg/cardimage_6532476_1695869711367633744685.jpg&imgrefurl=http://www.studyblue.com/notes/note/n/cerebral-vasculature/deck/7487525&h=688&w=1000&tbnid=DG-qgQdLoogCLM:&zoom=1&docid=6kzMA6fUNw23lM&ei=fVI6VOWAI8mIuASQ9YKYBw&tbm=isch&ved=0CCUQMygLMAs
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 25
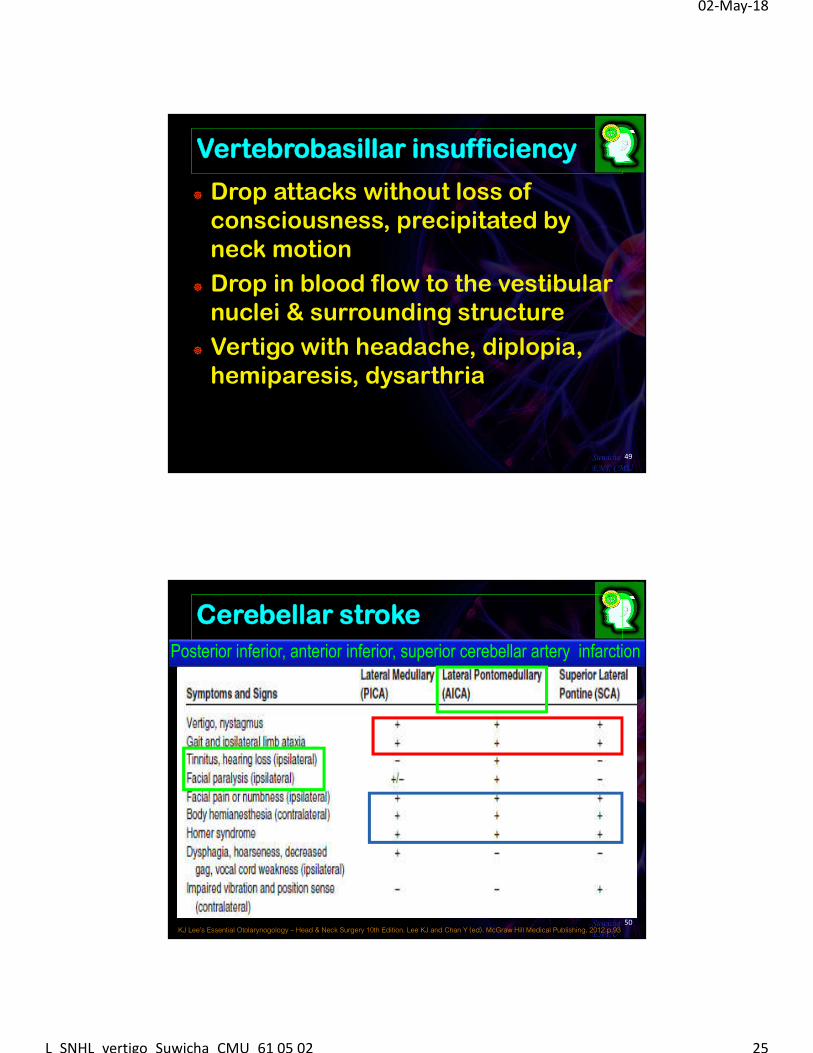
Vertebrobasillar insufficiency
Drop attacks without loss of consciousness, precipitated by neck motion
Drop in blood flow to the vestibular nuclei & surrounding structure
Vertigo with headache, diplopia, hemiparesis, dysarthria
49SuwichaENT, CMU
50SuwichaENT,UKJ Lee’s Essential Otolarynogology – Head & Neck Surgery 10th Edition. Lee KJ and Chan Y (ed). McGraw Hill Medical Publishing. 2012 p.93
Cerebellar stroke
Posterior inferior, anterior inferior, superior cerebellar artery infarction
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 26
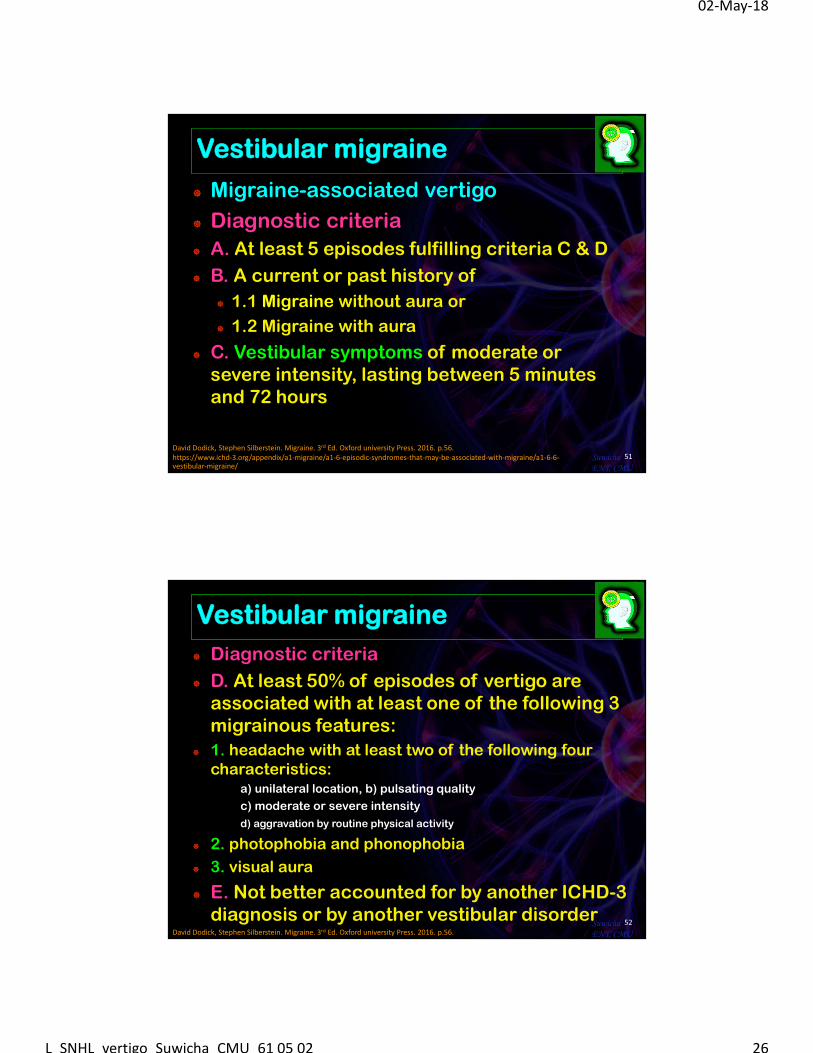
Vestibular migraine
Migraine-associated vertigo
Diagnostic criteria
A. At least 5 episodes fulfilling criteria C & D
B. A current or past history of
1.1 Migraine without aura or
1.2 Migraine with aura
C. Vestibular symptoms of moderate or severe intensity, lasting between 5 minutes and 72 hours
51SuwichaENT, CMU
David Dodick, Stephen Silberstein. Migraine. 3rd Ed. Oxford university Press. 2016. p.56.https://www.ichd-3.org/appendix/a1-migraine/a1-6-episodic-syndromes-that-may-be-associated-with-migraine/a1-6-6-vestibular-migraine/
Vestibular migraine
Diagnostic criteria
D. At least 50% of episodes of vertigo are associated with at least one of the following 3 migrainous features:
1. headache with at least two of the following four characteristics:
a) unilateral location, b) pulsating quality
c) moderate or severe intensity
d) aggravation by routine physical activity
2. photophobia and phonophobia
3. visual aura
E. Not better accounted for by another ICHD-3 diagnosis or by another vestibular disorder
52SuwichaENT, CMUDavid Dodick, Stephen Silberstein. Migraine. 3rd Ed. Oxford university Press. 2016. p.56.
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 27
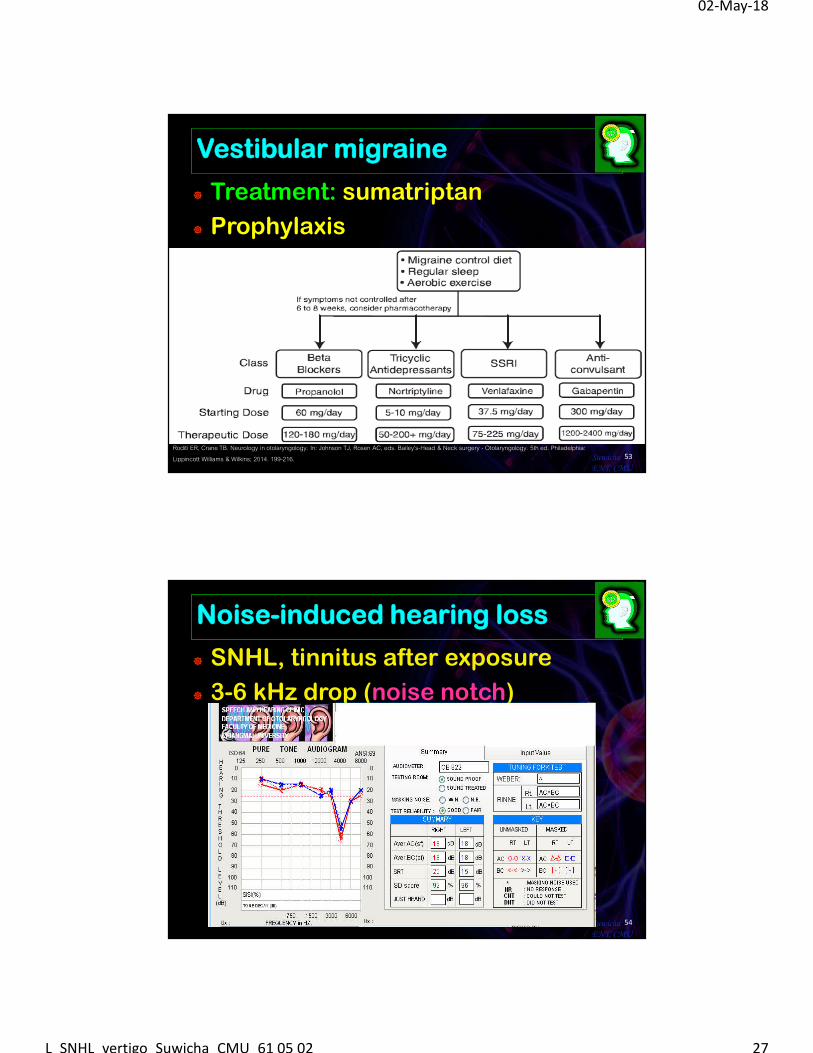
Vestibular migraine
Treatment: sumatriptan
Prophylaxis
53SuwichaENT, CMU
Roditi ER, Crane TB. Neurology in otolaryngology. In: Johnson TJ, Rosen AC, eds. Bailey's-Head & Neck surgery - Otolaryngology. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2014. 199-216.
Noise-induced hearing loss
SNHL, tinnitus after exposure
3-6 kHz drop (noise notch)
54SuwichaENT, CMU
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 28
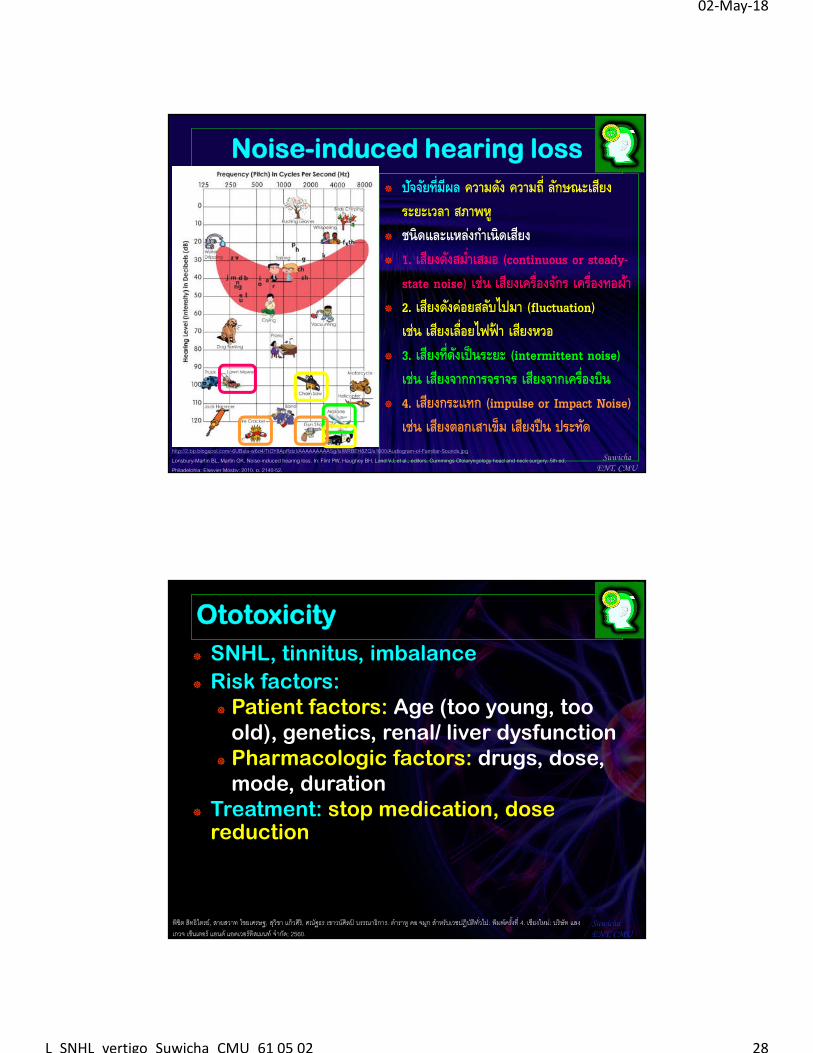
Noise-induced hearing loss
ปจัจยัที�มีผล ความดงั ความถี� ลกัษณะเสยีง ระยะเวลา สภาพหู
ชนิดและแหลง่กาํเนิดเสยีง 1. เสยีงดงัสมํ �าเสมอ (continuous or steady-
state noise) เช่น เสยีงเครื�องจกัร เครื�องทอผา้ 2. เสยีงดงัค่อยสลบัไปมา (fluctuation)
เช่น เสยีงเลื�อยไฟฟ้า เสยีงหวอ 3. เสยีงที�ดงัเป็นระยะ (intermittent noise)
เช่น เสยีงจากการจราจร เสยีงจากเครื�องบิน 4. เสยีงกระแทก (impulse or Impact Noise)
เช่น เสยีงตอกเสาเข็ม เสยีงปืน ประทดั
SuwichaENT, CMU
http://2.bp.blogspot.com/-6UBsla-w6d4/TtOY8ApRdzI/AAAAAAAAASg/lsIWRBEH8ZQ/s1600/Audiogram-of-Familiar-Sounds.jpgLonsbury-Martin BL, Martin GK. Noise-induced hearing loss. In: Flint PW, Haughey BH, Lund VJ, et al., editors. Cummings Otolaryngology head and neck surgery. 5th ed. Philadelphia: Elsevier Mosby; 2010. p. 2140-52.
SNHL, tinnitus, imbalance
Risk factors: Patient factors: Age (too young, too
old), genetics, renal/ liver dysfunction Pharmacologic factors: drugs, dose,
mode, duration Treatment: stop medication, dose
reduction
SuwichaENT, CMU
พิชิต สทิธิไตรย์, สายสวาท ไชยเศรษฐ, สวุิชา แก้วศิริ, ศณฐัธร เชาวน์ศิลป์ บรรณาธิการ. ตําราห ูคอ จมกู สาํหรับเวชปฏิบตัิทั�วไป. พิมพ์ครั �งที� 4. เชียงใหม:่ บริษัท แลงเกวจ เซ็นเตอร์ แอนด์ แอดเวอร์ทิสเมนท์ จํากดั; 2560.
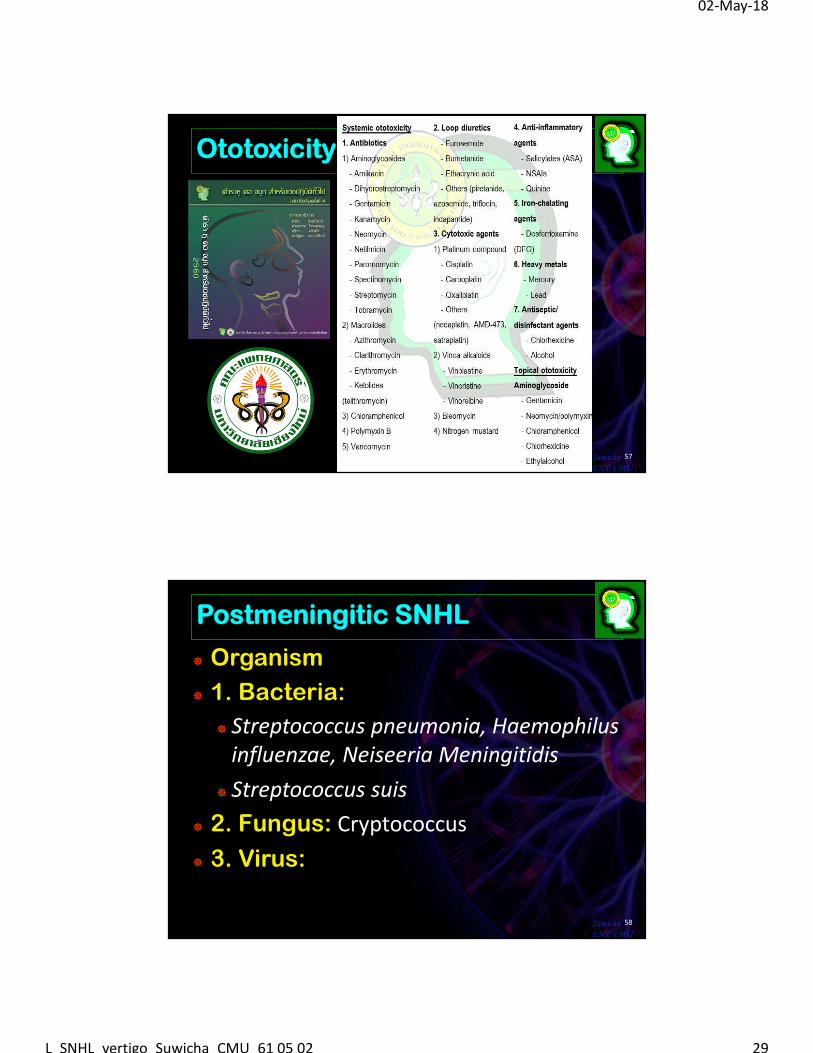
Ototoxicity
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 29
Ototoxicity
57SuwichaENT, CMU
Postmeningitic SNHL
Organism
1. Bacteria:
Streptococcus pneumonia, Haemophilusinfluenzae, Neiseeria Meningitidis
Streptococcus suis
2. Fungus: Cryptococcus
3. Virus:
58SuwichaENT, CMU
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 30
Postmeningitic SNHL
Mechanism of hearing loss
1. Inflammatory labyrinthitis
2. Cochlear/ labyrithitis ossificans, fibrosis
3. Hemorrhage in cochlear duct
4. Septicemia: septic emboli
5. Neuritis
6. Central auditory pathway/ hydrocephalus
59SuwichaENT, CMU
พชิิต สทิธไิตรย์, สายสวาท ไชยเศรษฐ, สวุชิา แก้วศิริ, ศณฐัธร เชาวน์ศิลป์ บรรณาธิการ. ตําราห ูคอ จมูก สําหรับเวชปฏิบตัิทั�วไป. พมิพ์ครั �งที� 4. เชียงใหม่: บริษัท แลงเกวจ เซน็เตอร์ แอนด์ แอดเวอร์ทสิเมนท ์จํากดั; 2560.
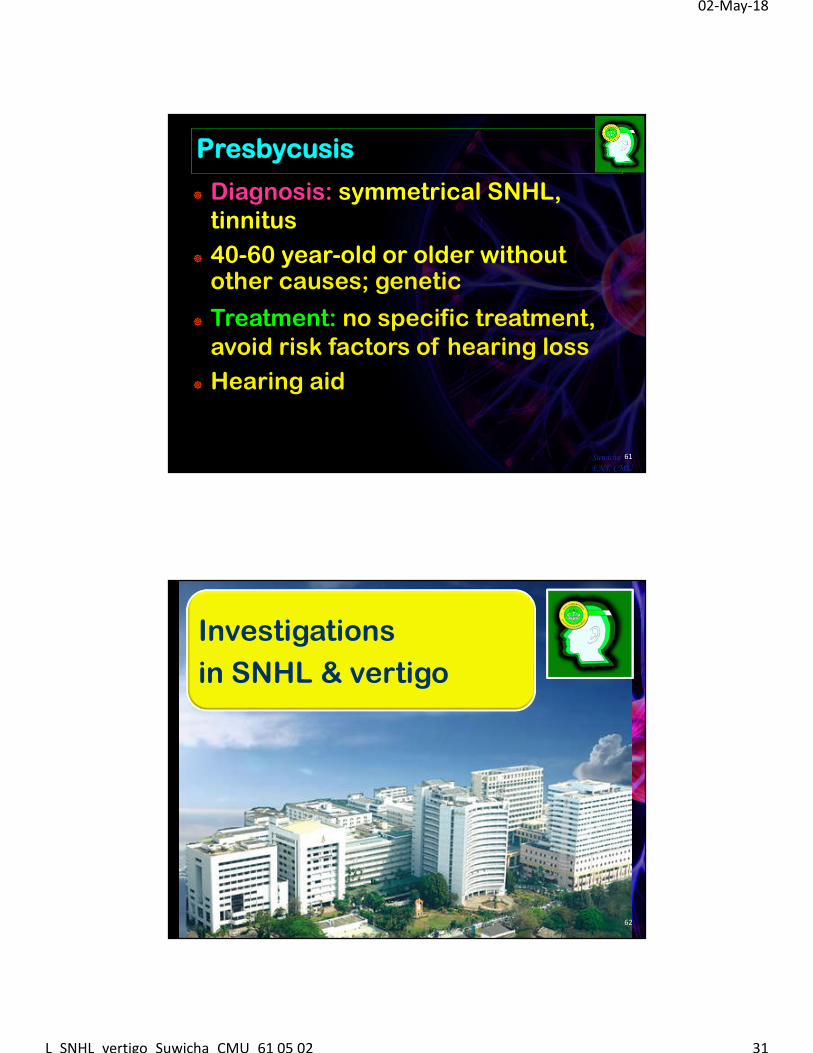
Presbycusis
Bilateral progressive SHNL
60SuwichaENT, CMU
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 31
Presbycusis
Diagnosis: symmetrical SNHL, tinnitus
40-60 year-old or older withoutother causes; genetic
Treatment: no specific treatment, avoid risk factors of hearing loss
Hearing aid
61SuwichaENT, CMU
Investigations
in SNHL & vertigo
62
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 32
Investigations in SNHL & vertigo
Hearing test: Audiogram, Auditory brainstem response (ABR)
Radiological test: MRI of the IAC/ brain, CT temporal bone
Blood test: VDRL, TPHA, thyroid function test
Vestibular function test: Dix-Hallpike test, Lab
63SuwichaENT, CMU
แปลผล Audiogram
Normal hearing
1. Sensorineural hearing loss
2. Conductive hearing loss
3. Mixed hearing loss
4. Central hearing loss
5. Functional hearing loss
64SuwichaENT, CMU
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 33
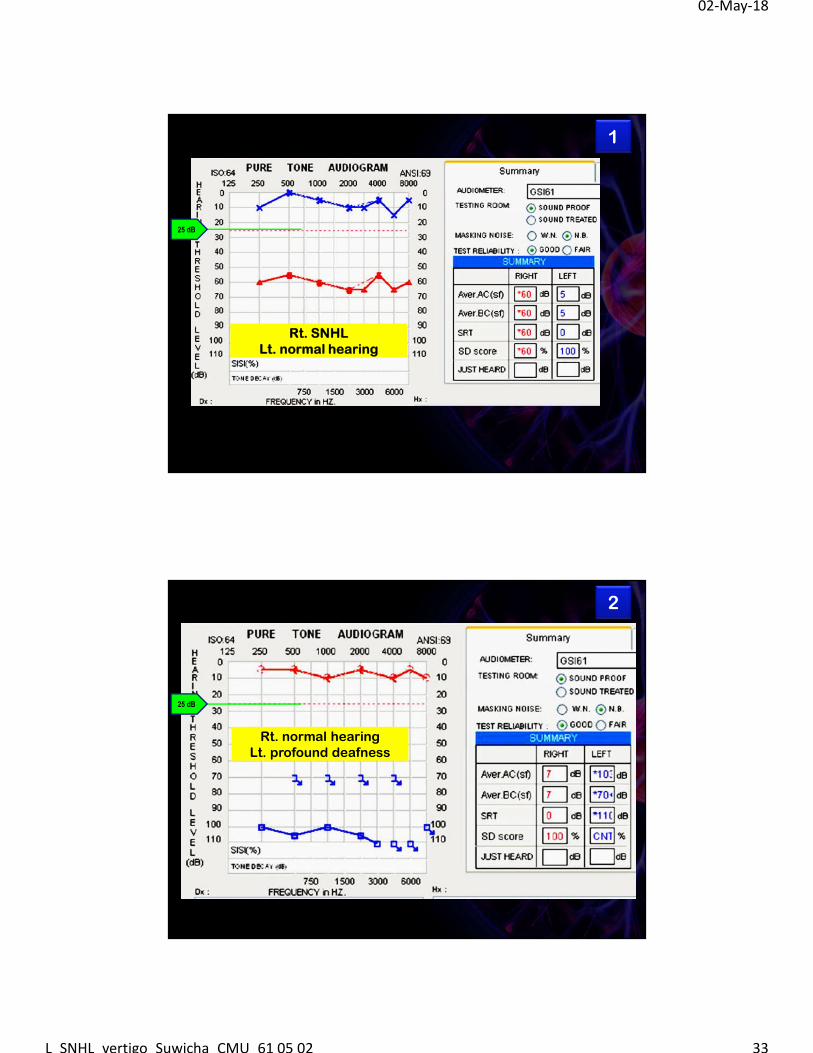
1
Rt. SNHLLt. normal hearing
25 dB
2
Rt. normal hearing Lt. profound deafness
25 dB
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 34
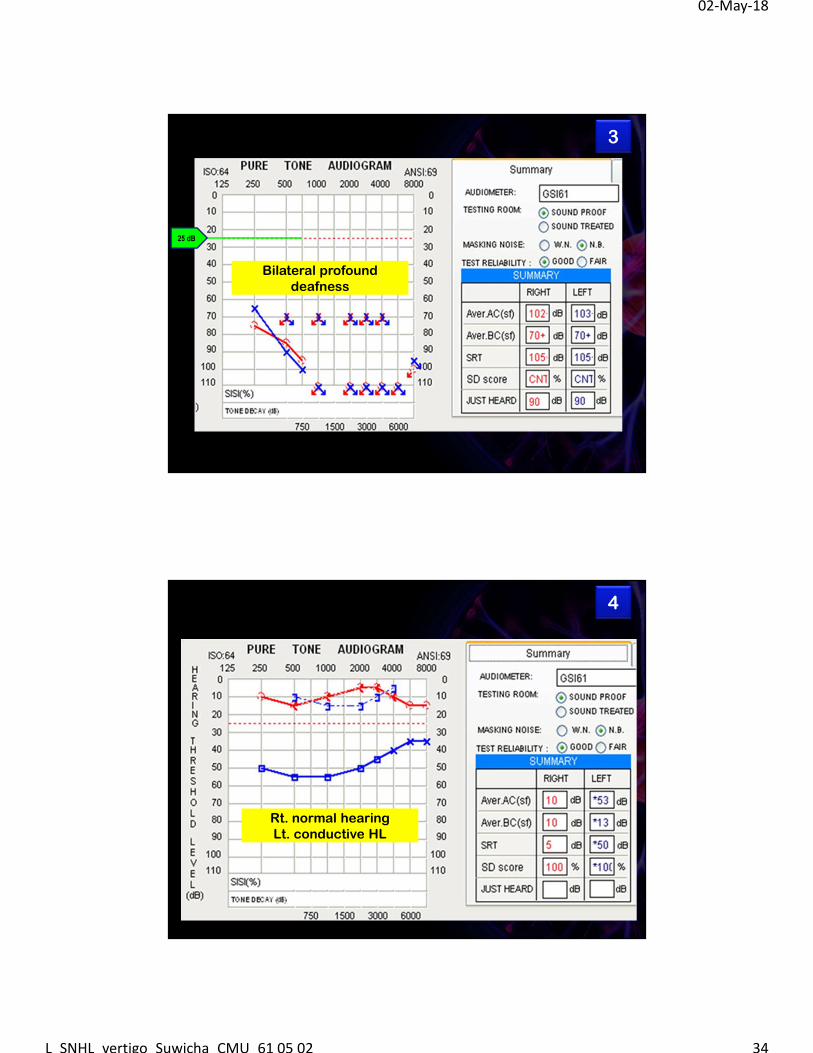
3
Bilateral profound deafness
25 dB
4
Rt. normal hearing Lt. conductive HL
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 35
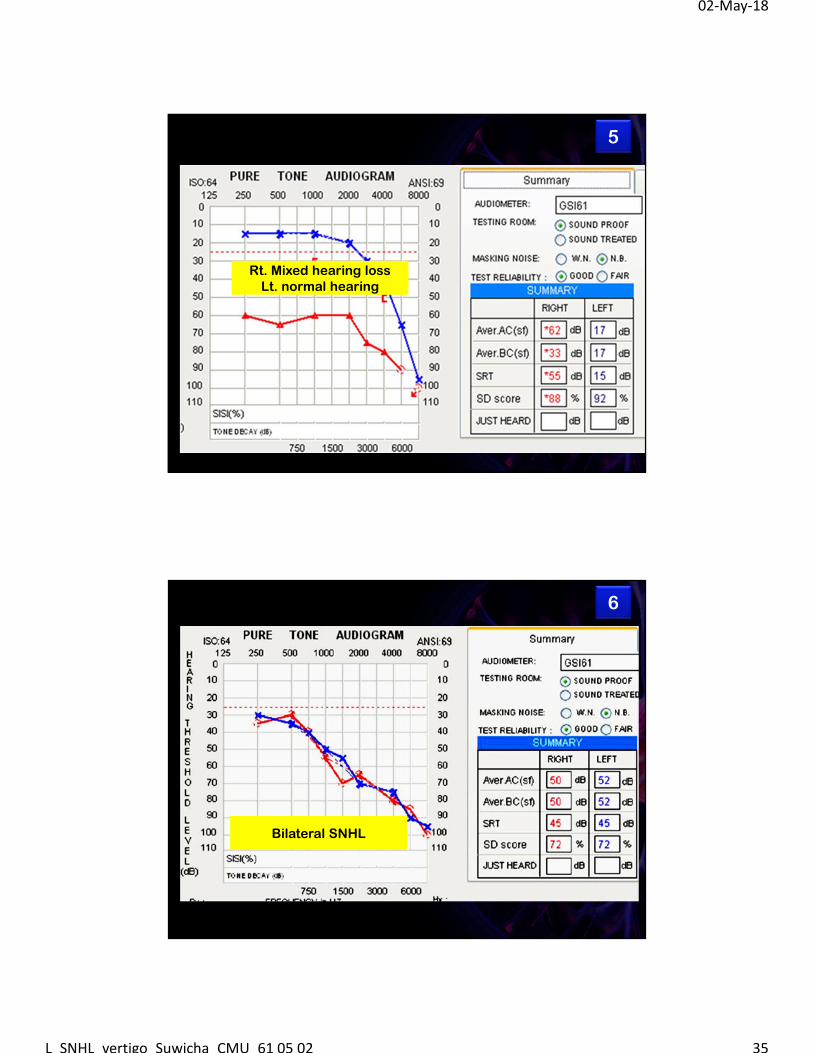
5
Rt. Mixed hearing lossLt. normal hearing
6
Bilateral SNHL
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 36
SuwichaENT, CMU
http://2.bp.blogspot.com/-6UBsla-w6d4/TtOY8ApRdzI/AAAAAAAAASg/lsIWRBEH8ZQ/s1600/Audiogram-of-Familiar-Sounds.jpgวาสนา วะสนีนท์ การฟื�นฟสูมรรถภาพการได้ยิน ใน: พิชิต สทิธิไตรย์, สายสวาท ไชยเศรษฐ, สวุิชา อิศราดิสยักลุ, บรรณาธิการ. ตําราห ูคอ จมกู สาํหรับเวชปฏิบตัิทั�วไป ภาควิชาโสต ศอ นาสกิวิทยา คณะแพทยศาสตร์ มหาวิทยาลยัเชียงใหม.่ Trick think; 2554. หน้า 291-304.http://www.oshthai.org/upload/file_linkitem/20110629093435_2.pdf
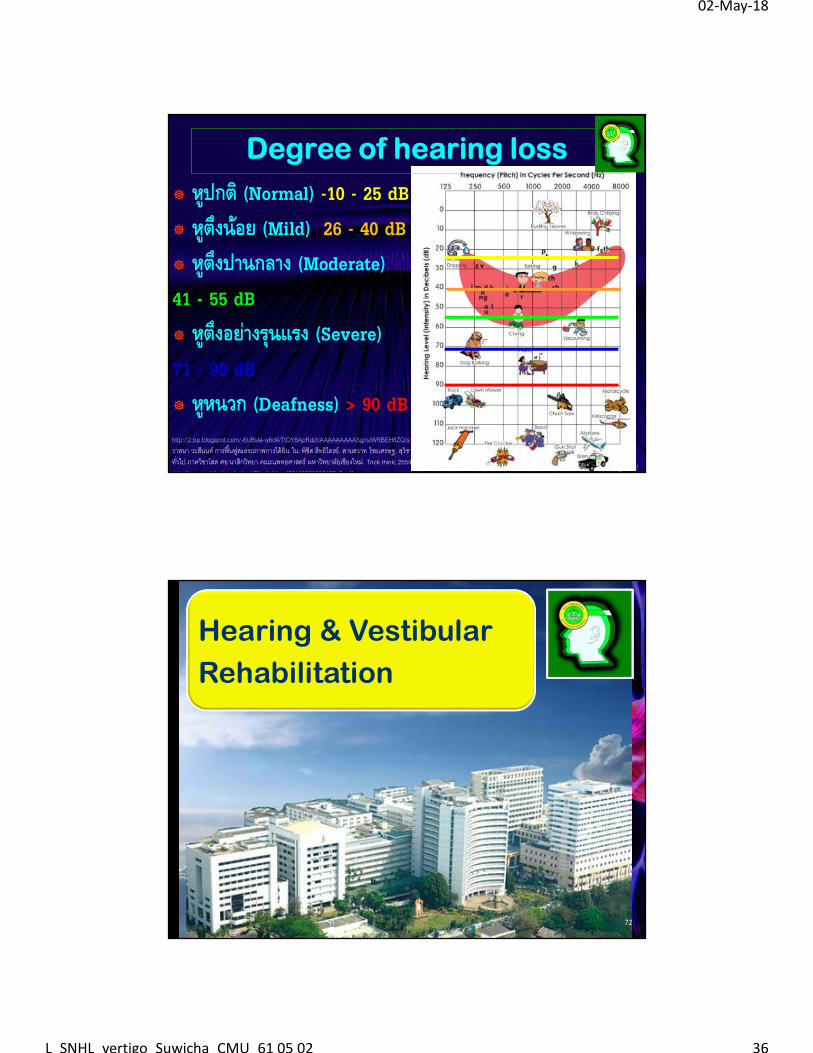
หูปกติ (Normal) -10 - 25 dB หูตึงนอ้ย (Mild) 26 - 40 dB หูตึงปานกลาง (Moderate) 41 - 55 dB หูตึงอย่างรุนแรง (Severe) 71 - 90 dB หูหนวก (Deafness) > 90 dB
Degree of hearing loss
Hearing & Vestibular
Rehabilitation
72
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 37
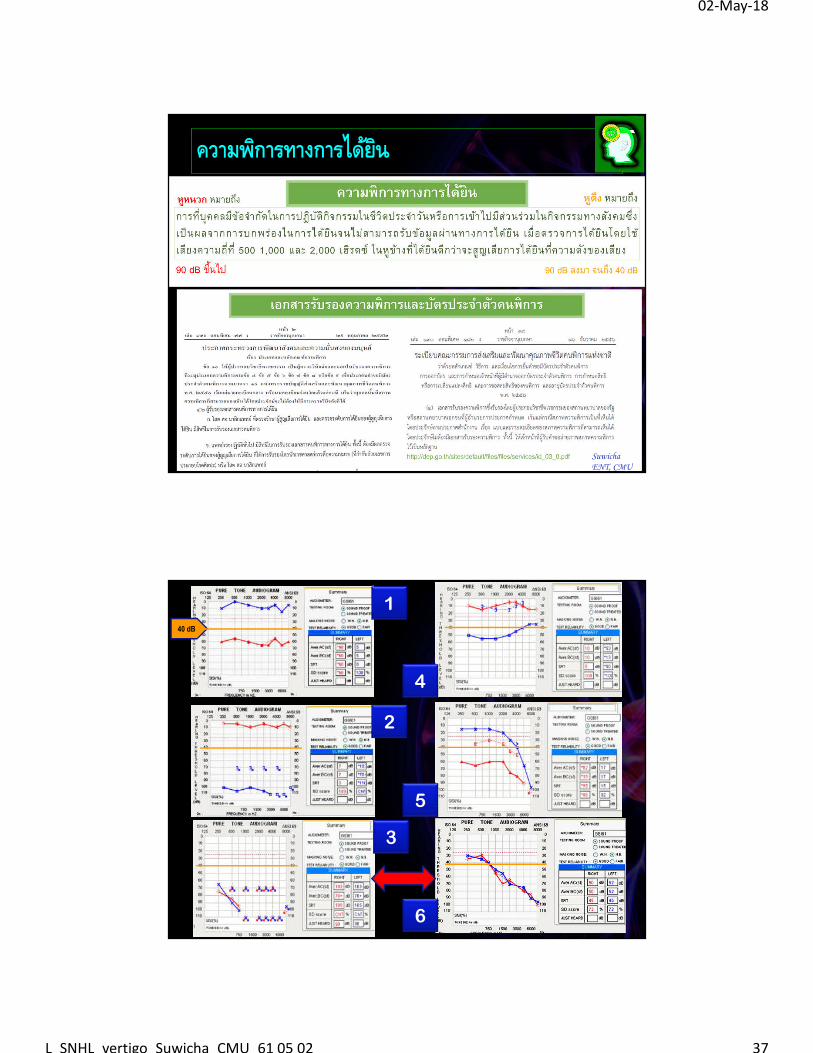
ความพกิารทางการไดย้นิ
73SuwichaENT, CMU
1
2
3
4
5
6
40 dB
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 38
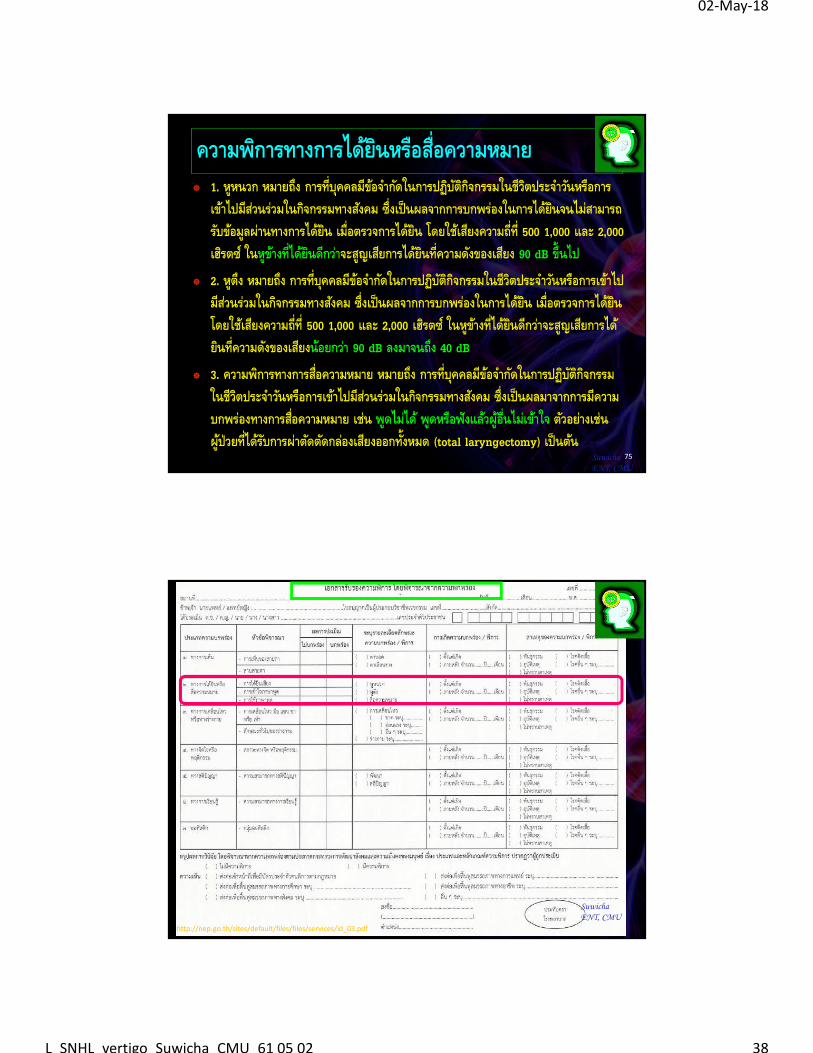
ความพกิารทางการไดย้นิหรอืสื�อความหมาย 1. หูหนวก หมายถงึ การที�บคุคลมีขอ้จาํกดัในการปฏบิตักิจิกรรมในชีวติประจาํวนัหรือการ
เขา้ไปมีสว่นร่วมในกจิกรรมทางสงัคม ซึ�งเป็นผลจากการบกพร่องในการไดย้นิจนไม่สามารถรบัขอ้มูลผ่านทางการไดย้นิ เมื�อตรวจการไดย้นิ โดยใชเ้สยีงความถี�ที� 500 1,000 และ 2,000 เฮริตซ ์ในหูขา้งที�ไดย้นิดีกวา่จะสูญเสยีการไดย้นิที�ความดงัของเสยีง 90 dB ขึ�นไป
2. หูตงึ หมายถงึ การที�บคุคลมีขอ้จาํกดัในการปฏบิตักิจิกรรมในชีวติประจาํวนัหรือการเขา้ไปมีสว่นร่วมในกจิกรรมทางสงัคม ซึ�งเป็นผลจากการบกพร่องในการไดย้นิ เมื�อตรวจการไดย้นิ โดยใชเ้สยีงความถี�ที� 500 1,000 และ 2,000 เฮริตซ ์ในหูขา้งที�ไดย้นิดีกวา่จะสูญเสยีการได้ยนิที�ความดงัของเสยีงนอ้ยกวา่ 90 dB ลงมาจนถงึ 40 dB
3. ความพกิารทางการสื�อความหมาย หมายถงึ การที�บคุคลมีขอ้จาํกดัในการปฏบิตักิจิกรรมในชีวติประจาํวนัหรือการเขา้ไปมีสว่นร่วมในกจิกรรมทางสงัคม ซึ�งเป็นผลมาจากการมีความบกพร่องทางการสื�อความหมาย เช่น พูดไม่ได ้พูดหรือฟังแลว้ผูอ้ื�นไม่เขา้ใจ ตวัอยา่งเช่น ผูป่้วยที�ไดร้บัการผ่าตดัตดักลอ่งเสยีงออกทั�งหมด (total laryngectomy) เป็นตน้
75SuwichaENT, CMU
SuwichaENT, CMU
http://nep.go.th/sites/default/files/files/services/id_03.pdf
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 39
77SuwichaENT, CMUhttp://www.nhso.go.th/FrontEnd/page-contentdetail.aspx?CatID=NDI=
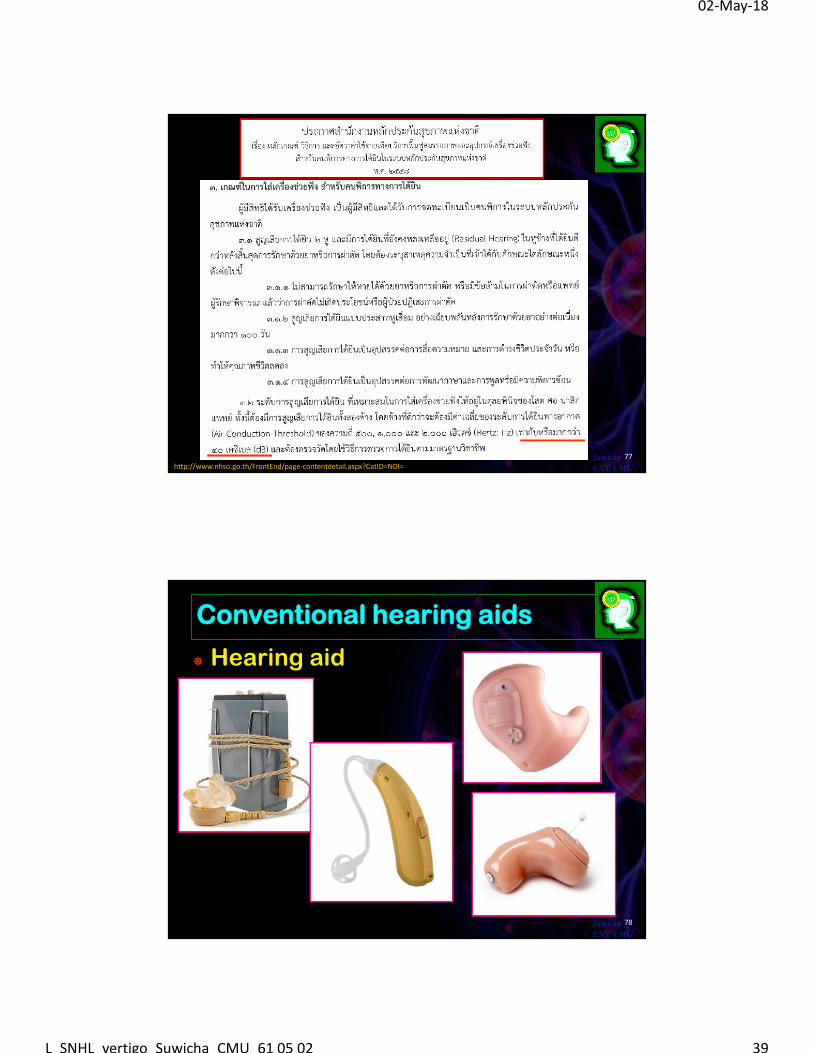
Conventional hearing aids
Hearing aid
78SuwichaENT, CMU
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 40
Conventional hearing aids
79SuwichaENT, CMU
ศณฐัธร เชาวน์ศิลป์ การฟื�นฟกูารได้ยิน ใน: พิชิต สทิธิไตรย์, สายสวาท ไชยเศรษฐ, สวุิชา แก้วศิริ, ศณฐัธร เชาวน์ศิลป์ บรรณาธิการ. ตําราห ูคอ จมกู สาํหรับเวชปฏิบตัิทั�วไป. พิมพ์ครั �งที� 4. เชียงใหม:่ บริษัท แลงเกวจ เซ็นเตอร์ แอนด์ แอดเวอร์ทิสเมนท์ จํากดั; 2560.
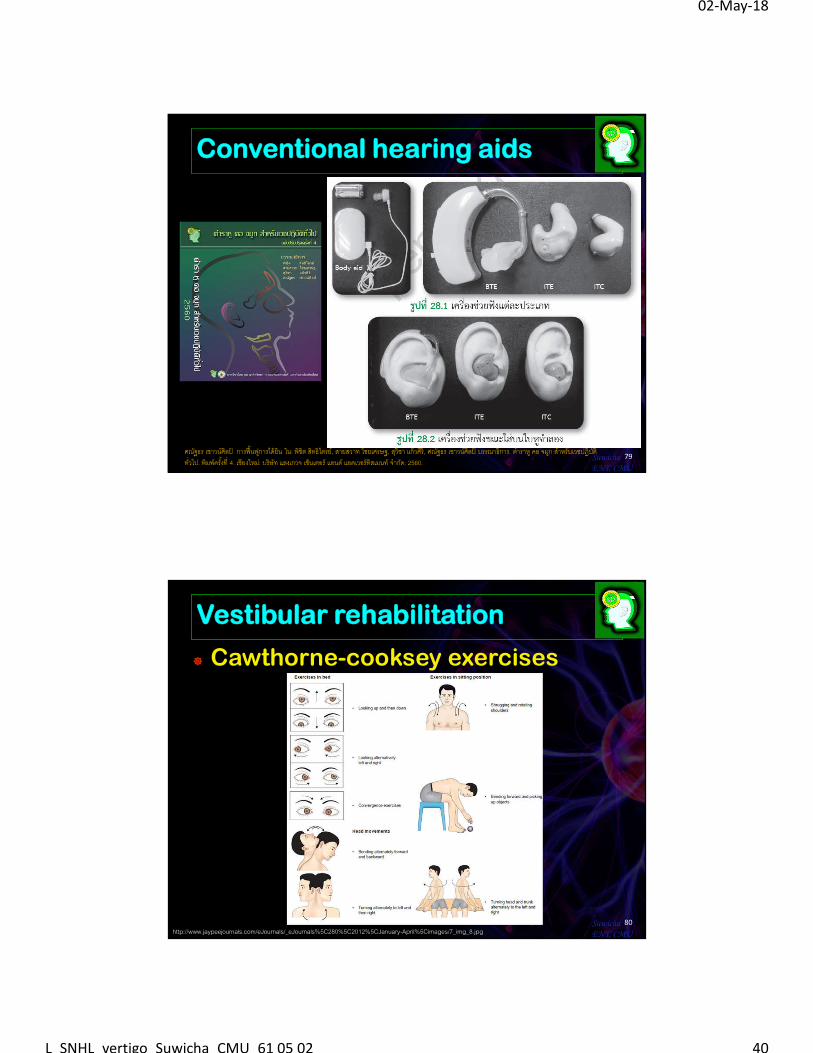
Vestibular rehabilitation
Cawthorne-cooksey exercises
80SuwichaENT, CMUhttp://www.jaypeejournals.com/eJournals/_eJournals%5C280%5C2012%5CJanuary-April%5Cimages/7_img_8.jpg
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 41
Vestibular rehabilitation
Exercises & sports
81SuwichaENT, CMU
Antivertigo medications-1
กลุม่ยา ยา ขนาดยาที�ใช ้(ในผูใ้หญ่)1. Vestibular suppressant1.1. Antihistamine
Dimenhydrinate (Dramamine®, Navamin® 50 มก., amp 50 มก./มล.)
1-2 เมด็ orally prn vertigo ทกุ 4-6 ชม. หรือ tid-qid, 50 มก. IV หรือ IM ทกุ 6-8 ชม.
Meclizine (Antivert®12.5, 25 มก.)25 มก. รบัประทาน 1 to 4 ครั�ง/วนั หรือ 50 มก. orally 2 ครั�ง/วนั
1.2. Anticholinergics Scopolamine (Transderm-Scop®
Transdermal patch 1.5 มก.) 1.5 มก. แปะหลงัหู ทกุ 3 วนั1.3. Antidopaminergics (anti-emetics)
Promethazine HCl (Phenergan®50 มก./ 2 มล.) 25-50 มก. IVหรือ IM ทกุ 4-6 ชม. Prochlorperazine(Stemitil®5 มก.) 5 มก. orally tidHaloperidol (Haldol®, Halomed®0.5, 2, 5 มก., 5 มก./ มล.)
0.5-5 มก. orally bid หรือ tid2-5 มก. IM ทกุ 4-8 ชม.
Metoclopramide (Plasil®, Nausil®10 มก., 5 มก./ มล.)
10 มก. orally tid หรือ qid, ac10-20 มก. IV หรือ IM
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 42
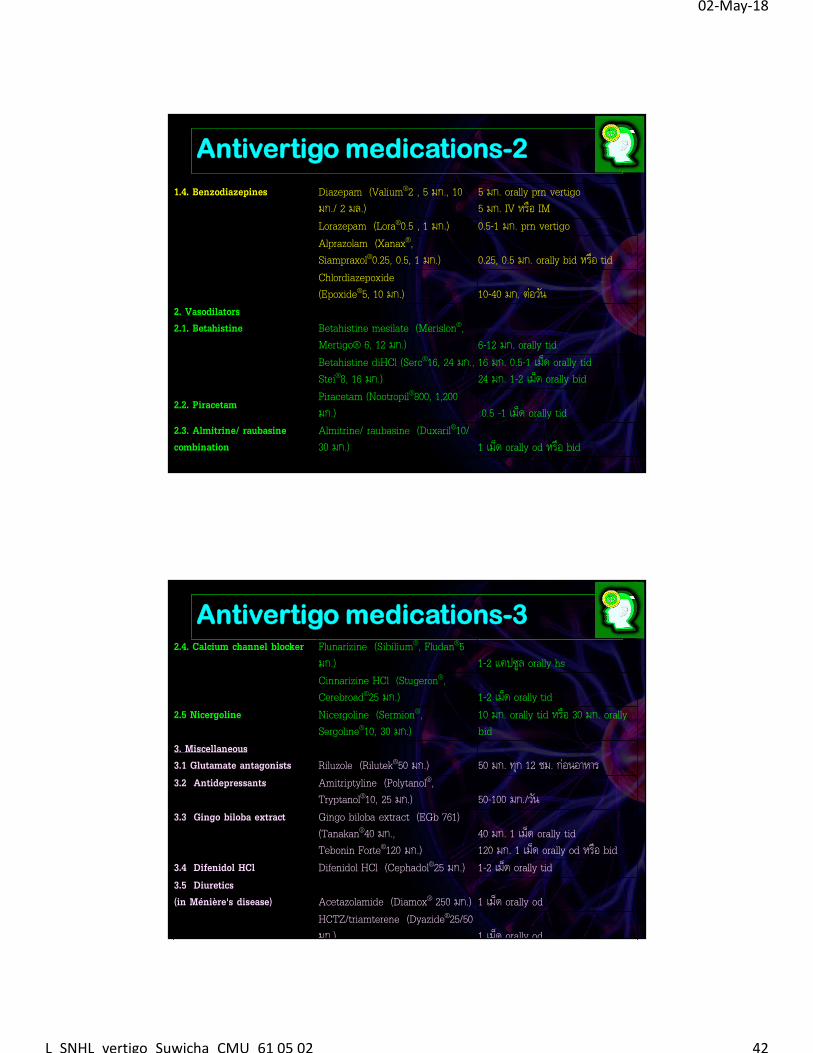
Antivertigo medications-2
1.4. Benzodiazepines Diazepam (Valium®2 , 5 มก., 10 มก./ 2 มล.)
5 มก. orally prn vertigo5 มก. IV หรือ IM
Lorazepam (Lora®0.5 , 1 มก.) 0.5-1 มก. prn vertigoAlprazolam (Xanax®, Siampraxol®0.25, 0.5, 1 มก.) 0.25, 0.5 มก. orally bid หรือ tidChlordiazepoxide(Epoxide®5, 10 มก.) 10-40 มก. ต่อวนั
2. Vasodilators2.1. Betahistine Betahistine mesilate (Merislon®,
Mertigo® 6, 12 มก.) 6-12 มก. orally tidBetahistine diHCl (Serc®16, 24 มก., Stei®8, 16 มก.)
16 มก. 0.5-1 เมด็ orally tid24 มก. 1-2 เมด็ orally bid
2.2. PiracetamPiracetam (Nootropil®800, 1,200 มก.) 0.5 -1 เมด็ orally tid
2.3. Almitrine/ raubasine combination
Almitrine/ raubasine (Duxaril®10/ 30 มก.) 1 เมด็ orally od หรือ bid
Antivertigo medications-32.4. Calcium channel blocker Flunarizine (Sibilium®, Fludan®5
มก.) 1-2 แคปซูล orally hsCinnarizine HCl (Stugeron®, Cerebroad®25 มก.) 1-2 เมด็ orally tid
2.5 Nicergoline Nicergoline (Sermion®, Sergoline®10, 30 มก.)
10 มก. orally tid หรือ 30 มก. orally bid
3. Miscellaneous 3.1 Glutamate antagonists Riluzole (Rilutek®50 มก.) 50 มก. ทกุ 12 ชม. ก่อนอาหาร3.2 Antidepressants Amitriptyline (Polytanol®,
Tryptanol®10, 25 มก.) 50-100 มก./วนั 3.3 Gingo biloba extract Gingo biloba extract (EGb 761)
(Tanakan®40 มก., Tebonin Forte®120 มก.)
40 มก. 1 เมด็ orally tid120 มก. 1 เมด็ orally od หรือ bid
3.4 Difenidol HCl Difenidol HCl (Cephadol®25 มก.) 1-2 เมด็ orally tid3.5 Diuretics (in Ménière's disease) Acetazolamide (Diamox® 250 มก.) 1 เมด็ orally od
HCTZ/triamterene (Dyazide®25/50 มก.) 1 เมด็ orally od
02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 43
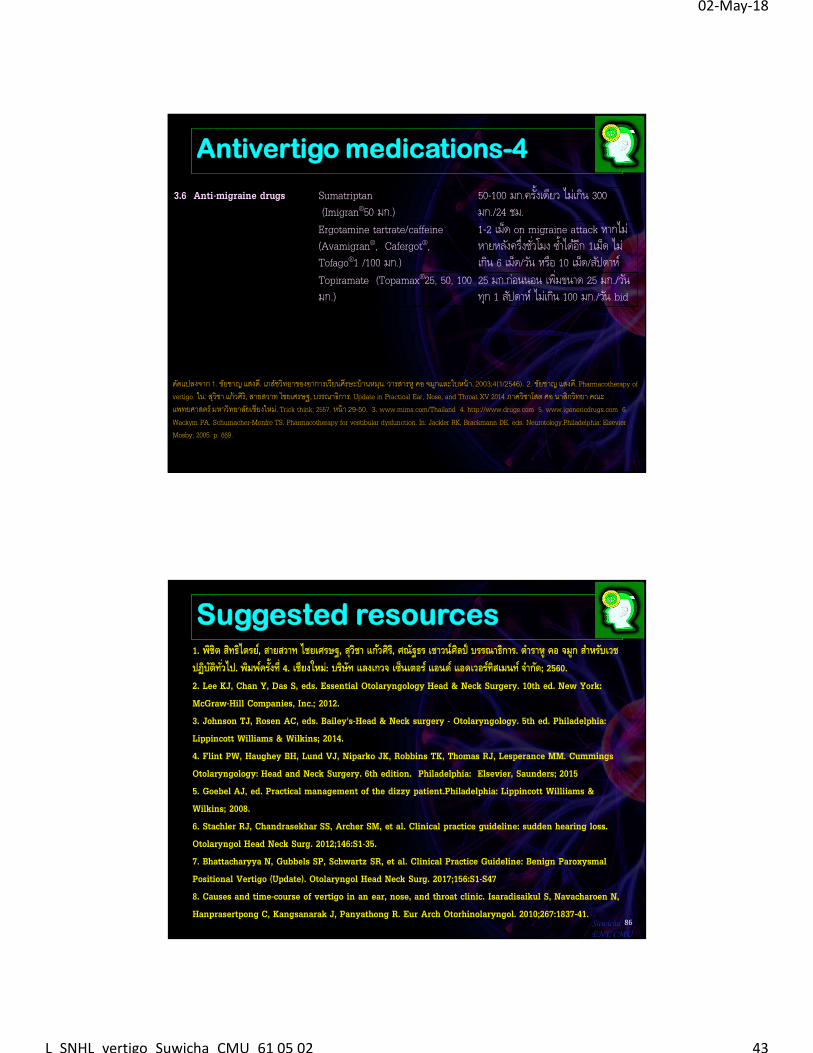
Antivertigo medications-4
3.6 Anti-migraine drugs Sumatriptan(Imigran®50 มก.)
50-100 มก.ครั�งเดยีว ไมเ่กนิ 300 มก./24 ชม.
Ergotamine tartrate/caffeine (Avamigran®, Cafergot®, Tofago®1 /100 มก.)
1-2 เมด็ on migraine attack หากไม่หายหลงัครึ�งช ั �วโมง ซํ�าไดอ้กี 1เมด็ ไม่เกนิ 6 เมด็/วนั หรือ 10 เมด็/สปัดาห ์
Topiramate (Topamax®25, 50, 100 มก.)
25 มก.ก่อนนอน เพิ�มขนาด 25 มก./วนั ทกุ 1 สปัดาห ์ไมเ่กนิ 100 มก./วนั bid
ดดัแปลงจาก 1. ชยัชาญ แสงด.ี เภสชัวิทยาของอาการเวียนศีรษะบ้านหมนุ. วารสารห ูคอ จมกูและใบหน้า. 2003;4(1/2546). 2. ชยัชาญ แสงด.ี Pharmacotherapy of vertigo. ใน: สวุิชา แก้วศิริ, สายสวาท ไชยเศรษฐ, บรรณาธิการ. Update in Practical Ear, Nose, and Throat XV 2014 ภาควิชาโสต ศอ นาสิกวิทยา คณะแพทยศาสตร์ มหาวิทยาลยัเชียงใหม.่ Trick think; 2557. หน้า 29-50. 3. www.mims.com/Thailand 4. http://www.drugs.com 5. www.igenericdrugs.com 6. Wackym PA, Schumacher-Monfre TS. Pharmacotherapy for vestibular dysfunction. In: Jackler RK, Brackmann DE, eds. Neurotology.Philadelphia: Elsevier Mosby; 2005. p. 669.
Suggested resources1. พชิิต สทิธิไตรย,์ สายสวาท ไชยเศรษฐ, สุวิชา แกว้ศิร,ิ ศณัฐธร เชาวนศิ์ลป์ บรรณาธิการ. ตําราหู คอ จมูก สาํหรบัเวชปฏิบตัิท ั �วไป. พมิพค์ร ั�งที� 4. เชียงใหม่: บรษิทั แลงเกวจ เซ็นเตอร ์แอนด ์แอดเวอรท์ิสเมนท ์จาํกดั; 2560. 2. Lee KJ, Chan Y, Das S, eds. Essential Otolaryngology Head & Neck Surgery. 10th ed. New York: McGraw-Hill Companies, Inc.; 2012.3. Johnson TJ, Rosen AC, eds. Bailey's-Head & Neck surgery - Otolaryngology. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2014. 4. Flint PW, Haughey BH, Lund VJ, Niparko JK, Robbins TK, Thomas RJ, Lesperance MM. Cummings Otolaryngology: Head and Neck Surgery. 6th edition. Philadelphia: Elsevier, Saunders; 20155. Goebel AJ, ed. Practical management of the dizzy patient.Philadelphia: Lippincott Williiams & Wilkins; 2008.6. Stachler RJ, Chandrasekhar SS, Archer SM, et al. Clinical practice guideline: sudden hearing loss. Otolaryngol Head Neck Surg. 2012;146:S1-35.7. Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol Head Neck Surg. 2017;156:S1-S478. Causes and time-course of vertigo in an ear, nose, and throat clinic. Isaradisaikul S, Navacharoen N, Hanprasertpong C, Kangsanarak J, Panyathong R. Eur Arch Otorhinolaryngol. 2010;267:1837-41.
86SuwichaENT, CMU

02-May-18
L_SNHL_vertigo_Suwicha_CMU_61 05 02 44
ตาํราหคูอ จมูก สาํหรบัเวชปฏิบติัทั �วไป
87SuwichaENT, CMU