Embed Size (px)
Citation preview
Title Electroencephalographic Study on Abdominal Neurosis
Author(s) NIMURA, YOSHIJI
Citation 日本外科宝函 (1965), 34(4): 849-880
Issue Date 1965-07-01
URL http://hdl.handle.net/2433/206514
Right
Type Departmental Bulletin Paper
Textversion publisher
Kyoto University
s.1<J
Electroencephalographic Study on Abdominal Neurosis
by
YosHur NrMURA
From the 2nd Surgical Division, Kyoto Univer,ity madical Schon! l Director : Prof. Dr. CHU JI K1MUR八)
Rec・ivedfor Publication M,円 10,1965
INTRODUCTION
After laparotomies we sometimes encounter the complaints which we cannot easily
shake off. These complaints--ーinflationof the abdomen, which disappears during general
or spinal anesthesia, obstipation, unsettled abdominal pain etc.---contain the psychoneurotic
factors in the greater part.
According to the denomination of Prof. ARAKI, Kyoto, we call such kind of syndrome
''abdominal neurosis”. Most abdominal operations are ineffective and even harmful to this disease. Sym-
pathectomies (thoracic or lumbar) show a temporal improvement, but the symptoms return
within one year. The posterior rhizotomy in thoracic spinal segments was done by C.
KIMURA and M. MAJIMA and a case could be free fom the symptoms as long as nineteen
months. This is a回記 towhich a surgical treatment was performed with the best effect.
C. KIMURA and his co-workers have been studying since 1945 on the etiology and
the therapy of this disease, nevertheless the pathogenesis is still obscure, and it is very
difficult to find a good surgical treatment.
The etiological obscurity makes us hesitate to regard it a definite disease ; therefore,
besides abdominal neurosis other denominations have been used by other authors, for irト
stance abdominal distention or neurogenic constipation, etc. Recently, Prof. M. MAEKAWA,
Kyoto, maintains spinal arachnitis as a principal etiological factor, and C. KIMURA demon-
strated in laminectomy of his clinical cases the existence of fibrotic change of the spinal
arachnoids with wide adhesions. KIMURA considered that the inflammatory change of the
arachnoid occurred as a result of careless spinal anesthesia technique. However, he considers
other unknown factors in the brain, too, having to do with these diseases. Here, the
present author studied electroencepharograms of these patients, because psychoneurotic ele『
ments seemed to play an important role in it.
Material and method
The present cases are the out-and in-patients of our clinic, experienced from 1961 to
1963 (table 1). Of twenty-seven cases, thirteen were regarded as ・abdominal neurosis,
nine had intestinal adhesion with inveterate abdominal complaints, and five wer己 hardly
differentiated from other abdominal complaints. Almost all of them, except two cases,
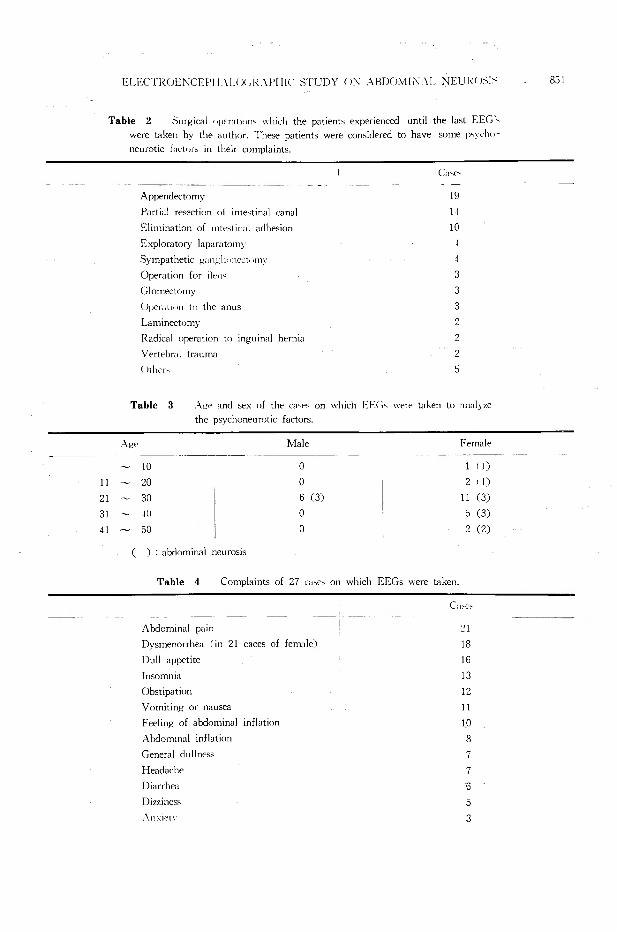
underwent surgery for their abdominal complaints from one to twelve times. Table 2
shows the surgical treatments they experienced and that appendectomy is thεmost com・
mon trigger of this disease. Table 3 shows that female patients in their twenties occupy
the greatest number among them. Table 4 shows their complaints and that six cases had
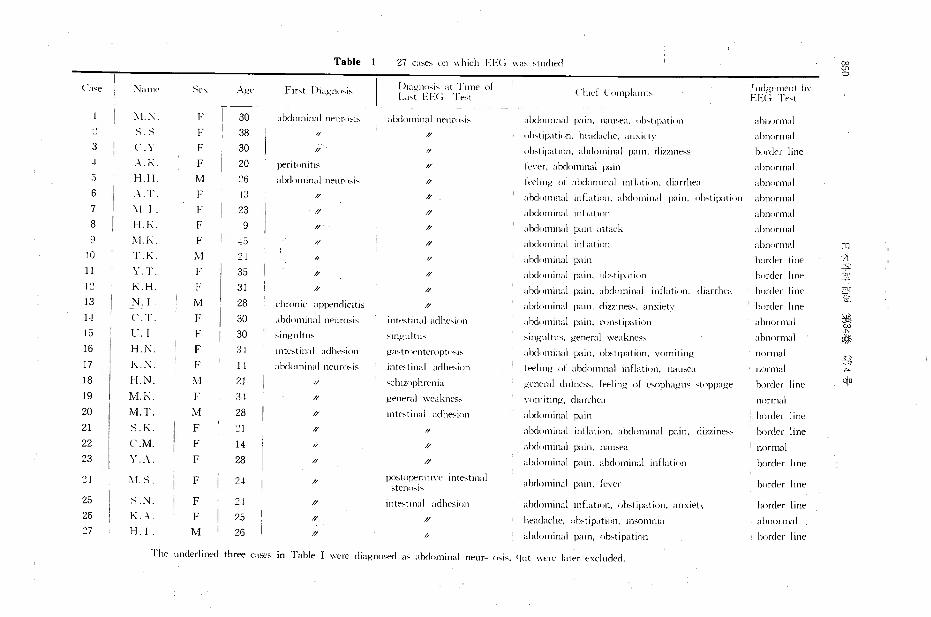
Table 27 ca,e,けnwhich EE<; "'" 'tud1ed Cにt胞コ
一C‘1河 Naml' メぞ、 主ι,. Fir、tDi<1gll<>S伍 Diagn<>、1、‘1tTune of
Clud ぐomplarnt、J udgt'11W11t b¥
l.a,t EE<; Tゎt El二:c;l、作t
1 ~I.:\ 30 ;ibdnminal neu 1・( bi~ abdominal 11cun"1ド abd<11111nal pai11. nau,ea. <】l"tipati<】ll abn<汀malメ:-; 38 ,, ,, けb'1i1川lion.heaζla,he. an,ie¥¥ abnormal
3 ピー\ ド 30 ,, nb,tipat1リn.abdominal pain. dizz1n"'s bordt>r line
:.¥.K. F 20 pentnmtis // fe w•r, abdけminalI旧 i11 abnormal 〈〉 H.H M :.'6 ・"'叫,111inalneuro'i' ,, ftでl川gof al叶川nmalmflat ion. diarrhea abn<irmal 6 礼.T. 13 λγ // abd<川111nal111! lation. abd<汀lllll.il p川1,nb,l1pat1けn abn川mnl7 ¥I.I 23 // ,, abdo1111nal 1nfl.1t1<•11 abnormal 8 H.K. F 9 // // けbd川ninalp川nattack abnormal
~J.K. F ~5 ,, // 江bdo111inalinll1t10n abnor111al 国
10 T. Iく. ル1 2.1 ,, ,, ・1bdorni11alpain bordt'r line す「-$. 11 Y.T ド 35 // // alxlnmiml pain, < 】'"lip.!l ¥Oil l引 rderline 一?で、十
K.H ド 31 h’ // abd《11ninalpain abd《11mnal i11flat1nn, diarrlwa border line 一γl吋』
で~ 日
13 N.1 M 28 chn・>11ic appendicitis // abぞ101111町 iipa111, dizzin民h an"ietv 』 bordl'rl111e
警4持11 C.T. ド 30 屯1bdorni11al11引 1rosis 1ntrsti11,il日dhれ j,川 abd<>rn111al pain,。H1'tipation abnormal 15 ll. I ド 30 singultus 叶 11日ultu、 川ngultus,gent-ral wt>aknf"S.s abnormal
16 H.N. F 31 mtt、tinal川Iht':' inn 日正istn片川teropt<''" al】rln111inalpain,けbst1pat1nn,¥'0111iti11g normal 込、、主一
17 K.:¥ F l』 ‘abdominal neurosis intestiml adhe,ion i付 1111日 4・iabdominal infl孔t1けn. nausea normal ,』
18 H.N. ¥1 21 ,, ドじhwiphrt>nia 日t'nerald11l11酢人 fttlingof e'ophag刷 、いい'"'日ぞ hord肝 line q;ロ
19 恥1.K F 3』 // 日eneral川町l、日目ぷ 、り111it旧日,ぐharrlwa normal
20 M.T. M 28 // mtゎtin刈‘1dh酢 ion ‘1bd日111inalpain border lme
21 S.K F // ,, alxl"rninal inflation, abd<川1111alp川口, d1zzine"'、 lxmler line
22 ぐ.乱1. F 14 。 // 。hdominalpain. nau、e.i 1 nor111al
23 Y.A. F 28 ι, ,, abdom川alp‘1in. ・巾cl,川、inalinllati‘m border Imε
'.2! :¥!. :-; . F 2-1 // p<1'toperat¥¥・c inte,t111al
ah<h>111inal pain, few1 border line stern"'' 25 メN F 2J. ,, intt':'trnal九dhesion alxlorninal inflation, ob、tipalion.an"iety border lme 26 K .. .¥ F 25 // // headache, <>b,11p<1t1011.川川口1111;‘i abn<》rmal~ 7 H.1 孔f 26 ,, ,, λbdominal p川n,ob,tipatin日 ' border I ine
!'he underlin吋 thr田 c<1sesin Table I ''ere diagn"明 1a式日lxlけminalneuト川、is,'l11t ""'"'' later t xcl11ded.
ELECTROENCEPH.¥LO< d~ :\l'Hf( . S’ruDYり>: ABDC>Mli¥.¥L NEUI{りう1:-; 851
Table 2 Surgical t 》per:it1• 川、 which the patients experienced until the last EEG¥
were taken by the author. 1、hesepatients were considered to have some p勺chrド
neurotic t川 tけr当 intheir complaints.
c,.,ト
Appen【lectomy
Vertebral trauma
9
i
0
1
4
3
3
3
2
2
2
5
1
1
1
Partial resection of intestinal canal
Elimination of 1ntestin<1l adh目 ion
Exploratory laparatomy
Sympathetic g;i ng li <• n杭 l<•lll、
Operation for ik11ば
Glomectomy
U1;erat1< >11 t<】 theanus
Laminecto口1Y
Radical operation to inguinal hernia
、、Lt
-
1
1
)
(
Table 3 主日eand詑 xof the e<N.,; on which El・:c;, were taken to ;inalyze
the psychoneurotic factors.
:\日t' Male Female
~ 10 。 I ( 1)
11 ~ 20 。 2 I I)
21 ~ 30 6 (3〕 11 (3)
31 ~ー10 。 5 (3)
41 ~ 50 。 2 (2)
( ) : abdominal neurosis
Table 4 Campi剖ntsof 27山ぜ' on which EEGs were taken.
C‘1吋、
Abdominal pain .I
Dysmenorrh回 (in21 caces of female)
Dull appetite
~I
Insomnia
8
6
3
2
1A
0
8
1
1
1
1
1
1
Obstipat1on
Vomiting or nau田a
Feeling of abdominal inf!山 on
Abdominal inflation
General dullness
Headache
Diarrhea
Dizzi即日
7
.¥11'it't、
勺dnLOFhJqJ

852 日本外科宝函第34巻第4号
a good passage of thεintestines. It is worthy of note that two田 sespresent the syndrome
of abdominal neurosis after vertebral trauma without any experience of laparotomy, which
suggests that arachnitis 回 npossibly be an important factor causing this disease.
None of these patients has the history of convulsive seizure.
Recordings of E. E.G. was made by monopolar leads with eight channels under fol-
lowing conditions :
i. They were kept quietly in spine position, with eyes closed, and recording was
continued for 5 20 minutes.
ii. An enforced hyperventilation was ordered for 3 5 minutes, and then recording
was made again for 5-20 minutes.
iii. Activation was tried with drugs (usually with 60-90 mg. of diphenhydramine
or with 50 100 mg. of Megimide, semetimes with Isomital), and the recording followed
for 20 40 minutes.
Drugs were given with slow intravenous injections.
iv. During these examinations the patients were o.timulated with the sound of a clap.
Mental calculation, opening of the eyes, stoppage of respiration and the like were ordered
exercise.
Recordings were repeated before and after a surgical operation, and whenever a change
of symptoms was observed.
RESULTS
F. A. GIBBS and E. L. GIBBS claim the positive spikes of 14 and 6 cps as the spec-
ific patterns in thalamic and hypothalamiじ epilepsy,while Y. SHIMODA maintains, besides
these, the paroxysmal slow waves as characteristic. The present author studied other
abnormal patterns as a sign of psychoneurotic abnormalities contained in these kinds of
diseases.
Table 5 and 6 show abnormal EEG found in all twentv-seven回 ses.
Table 7 shows abnormal patterns found in the cases of abdominal neurosis.
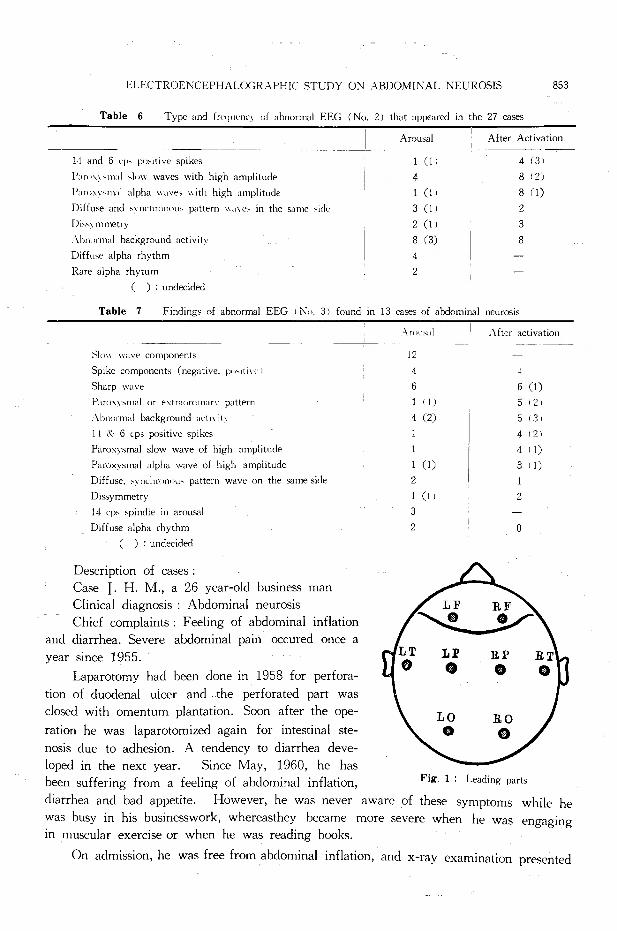
Fig. 1 shows a schema of leading parts.
Table 5 Findings of abnormal EEG (Nりー 1) and the frequenc、of their apparance in the 27 cases
日|リwwave component
Spike component (negative or positt可~)
日harpwave
Spike江nd、.vavecomplex
Pan》xymalor extraordtnar、pattern
¥bnormal background activities
1 ) : unc!Pc・ided
Arou日 l
19 (2)
5 (1)
8 (1) 。6 (!)
8 (3)
After activation
4 (2)
10 (I)
0 (I)
I I (2) 8 (3)
ELECTROENCEPHALOGR主PHIC、STUDYON ABDOMINAL NEUROSIS 853
Table 6 Type and fwc1uen山りfabnormal EEG (No. 2 J that appeared in the 27α世S
14 and 6 cp、p<i>1tivespikes
P"m'いm"I'low waves with high amplitude
I'"n山 い1rnlalpha wav小山ithhigh amplitude
Diffuse and叫 nchronot"pattern """e' in the回 me、idef)j,叫mmetry
λhrn》rndbackground activity
Diffu間 alpharhythm
Rare alpha rhytum
( ) : undecided
Arm四 l I Af肺 Activation
1(11 4(3J
4 8 (2)
1(11 8(1)
3 (1)
2 (1 I
8 (3)
4
2
ヮ’Mq300
Table 7 Finding,.; of abnormal EEG I No. 3) found in 13四 sesof abdominal neurosis
Description of cases :
Case I. H. M., a 26 year-old business man
Clinical diagnosis ・ Abdominal neurosis
Chief complaints: Feeling of abdominal inflation
and diarrhea. Severe abdominal pain occured once a
year since 1955.
Laparotomy had been done in 1958 for perfora-
tion of duodenal ulcer and the perforated part was
closed with omentum plantation. Soon after the ope-
ration he was laparotomized again for intestinal ste-
nosis due to adhesion. A tendency to diarrhea deve-
loped in the next year. Since May, 1960, he has
been sufferinεfrom a feeling of abdominal inflation, Fig. 1 : Leading parts
diarrhea and bad appetite. However, he was never aware of these symptoms while he
was busy in his businesswork, whereasthey became more severe when he was engaging
in muscular exercise or when he was reading books.
On admission, he was free from abdominal inflation, and x-ray examination presented
Slow wave components
Spike components (negative. p< <'ItI¥T I
Sharp wa¥'e
Pam入\'Slllalor extra《》rdmar、pattern
:'l.hnormal background act1、it、ll <'¥: 6ζp> positive spikes
Paroxysmal slow wave of high amplitude
Paroxysmalυlpha wave of high amplitude
Diffuse, wnchmn<川、 patternwave on the臼 meside
Dissymmetry
14ιp、spindlein arousal
Diffuse alpha rhythm
( ) : undecided
Arou出d 1 After activation
12
4
6
1 I I)
4 (2)
~
6 (1)
5 I 21
5 131
4 ( 21
4 I I)
3 I I) )
-
/21
、
1
1
2
1 (I I
3
2
2
。
LP @
RI'
@
LO
@ RO
@
854 日本外科宝函第34巻第4号
no intestinal obstruction.
He recovered from these complaints after the internal treatment with thymoleptica.
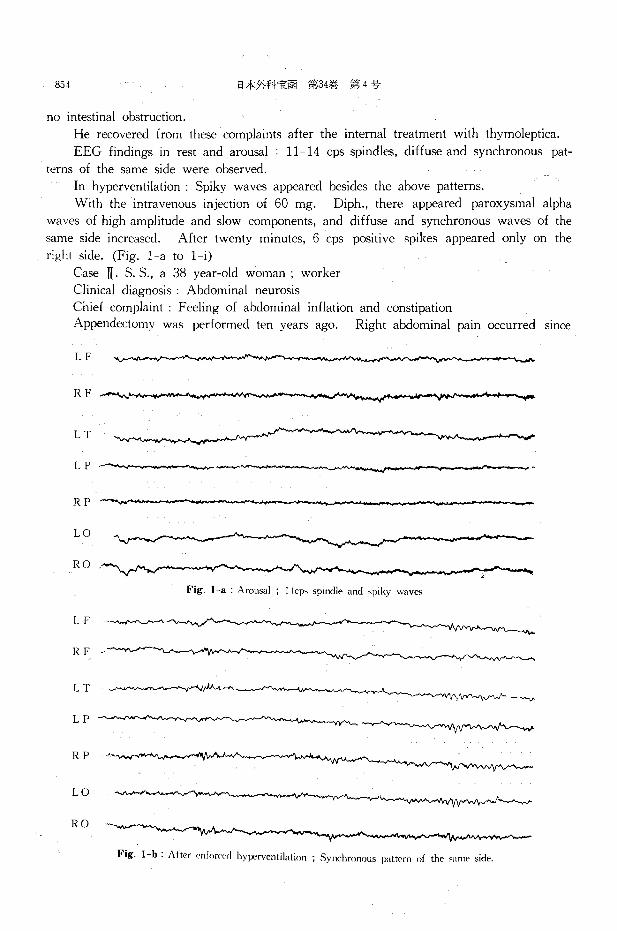
EEG findings in rest and arousal 11 14 cps spindles, diffuse and synchronous pat-
terns of the same side were observed.
In hyperventilation : Spiky waves appeared besides the above patterns.
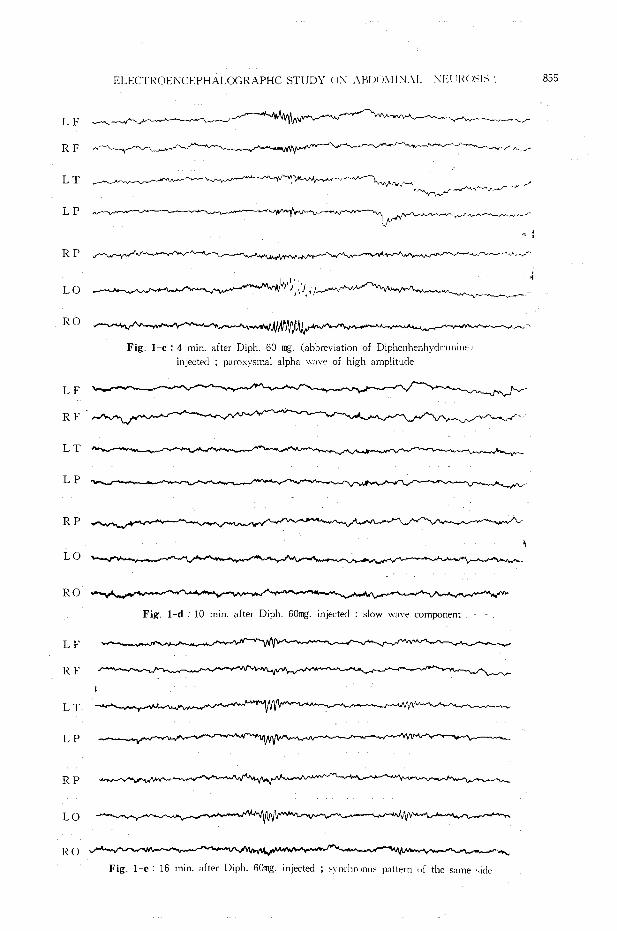
With the intravenous injection of 60 mg. Diph., there appeared paroxysmal alpha
waves of high amplitude and slow components, and diffuse and synchronous waves of the
same side increased. After twenty minutes, 6 cps positive spikes appeared only on the
ri只htside. (Fig. 1 a to 1 i)
Case II. S. S., a 38 year-old woman , worker
Clinical diagnosis : Abdominal neurosis
Chief complaint Feeling of abdominal inflation and constipation
Appendectomy was performed ten years ago. Right abdominal pain occurred since
LF
RF
LT
LP
RP
LO
RO
Fig. 1-a Arousal ; 11cい spindleand >piky waves
F
I
RF ~
LT
LP
R p ~.
LO ~I~~,J
RO
Fig. 1-b: After cnforc("d hyperventilation ; Synchronous pattern of the "'me side.
ELECTROENCEPHALOGRAPHC STUDY < !~記入H!JO:V!l:"J.\L !¥El il.U >メIメ1 855
LF 「ヘ~叫ん-.....~ザん4~ィィスィー_,.- ”’'i¥/l'I' ..- ~ ....,- ---~~__,__..,~r
RF ~-~ ._/~、r./ ,_ ~
LT 刊,W内ぺ~-、平吋f「ヘ叫ん』」べ /
巴一 ”叫刊々〆吋んJ、~『~__.._,-- -
LP
da 万
RP Aψ,、ん戸、引·~-
LO 一唱、~J』~,、
RO
Fig. 1 c : 4 min. after Diph. 60 mg. (abbreviati口nof Diphenhenhyclr:11n111e 1
injected ; parox)’smal alpha、川、・eof high amplitude
LF
RF
LT
LP
RP
LO
RO
Fig. 1-d . IO min. after Diph. 60mg. injected : slow 山口ecomponent
LF
RF
LT
LP
RP
LO
RO ‘市、
Fig. 1 e : 16 min. after Diph. 60mg. injected;川町Im川 ll> pattern of the回 me可【le

856 日本外科宝函 第34巻 ~:n -1 号
LF
RF
LT~刊ザ'/{'f(tf旬、ψ,.,r-
LP . '
計三,
RP
L O ~ヘ伊作.-v,戸川叫t川崎~--
RO
LF
RF
LT
LP
RP
LO
RO
LP
RF
LT
LP
RP
L (J
R (J
Fig. I f 18 min. after Diph. 60mg. inj町 ted; synchronus pattern of回 meside
一一一_,.. ,.. Fig. 1-g 19 min. after Diph. 60mg. injected ; synchronous". pattern of same日ide
'}拘晴、ν-、4・
Fig. 1-h : 20 min. affer Diph. 60 mg. inJ町 t吋; 6cp' ,~ ≫it1ypr,、pike>-川 rights油
ELECTR< !1-::¥CI-:t’HALOGR.¥I’HIC STUDY (J;-.iλBDOMINλL NEU RCがI~ 857
LF
RF .,_,,,......,-」..,...,、,._,.ザ4、~ー
LT
LP
RP
LO
RO
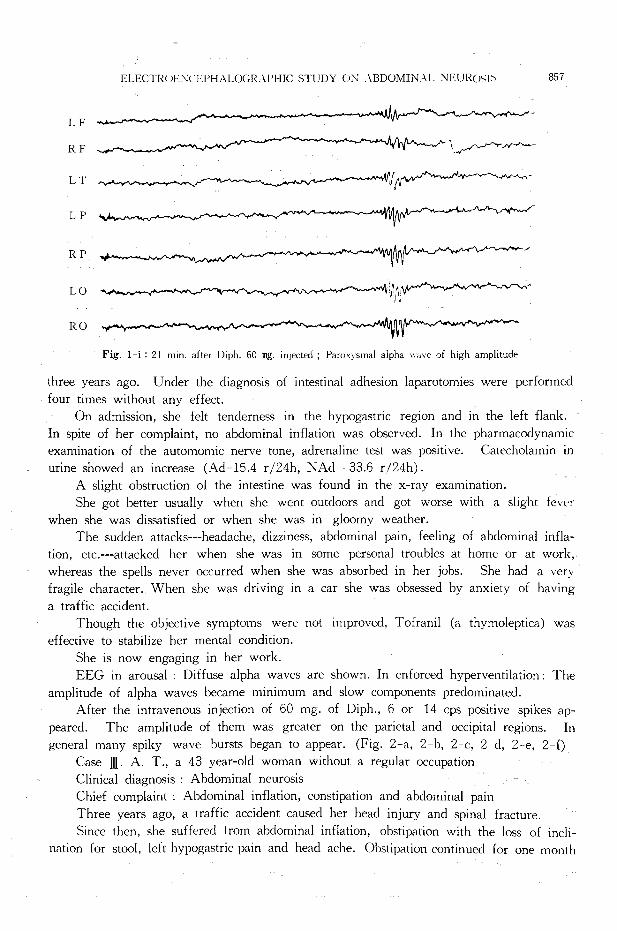
Fig. I i : 21 min. after Diph. 60田1g.injected ; Pan店内malalpha wυve of high amplitude
three years ago. Under the diagnosis of intestinal adhesion laparotomies were performed
four times without any effect.
On admission, she felt tenderness in the hypogastric region and in the left flank.
In spite of her complaint, no abdominal inflation was observed. In the pharmacodynamic
examination of the automomic nerve tone, adrenaline test was positive. Catecholamin in
urine showed an increase (Ad-15.4 r/24h, NAd ← 33.6 r /24h).
A slight obstruction of the intestine was found in the x-ray examination.
She got better usually when she went outdoors and got worse with a slight fever
when she was dissatisfied or when she was in gloomy weather.
The sudden attacks---headache, dizziness, abdominal pain, feeling of abdominal infla-
tion, etc.---attacked her when she was in some personal troubles at home or at work,
where泡Sthe spells never occurred when she was absorbed in her jobs. She had a very
fragile character. When she was driving in a car she was obsessed by anxiety of having
a traffic accident.
Though the objective symptoms were not improved, Tofranil (a thymoleptica) was
effective to stabilize her mental condition.
She is now engaging in her work.
EEG in arousal Diffuse alpha waves are shown. In enforced hyperventilation: The
amplitude of alpha waves became minimum and slow components predominated.
After the intravenous injection of 60 mg. of Diph., 6 or 14 cps positive spikes ap-
peared. The amplitude of them was greater on the parietal and occipital regions. In
general many spiky wave bursts began to appear. (Fig. 2-a, 2 b, 2-c, 2 cl, 2--e, 2-f)
Case J[. A. T., a 43 year-old woman without a regular occupation
Clinical diagnosis . Abdominal neurosis
Chief complaint Abdominal inflation, constipation and abdominal pain
Three years ago, a traffic accident caused her head injury and spinal fracture.
Since then, she suffered from abdominal inflation, obstipation with the loss of incli-
nation for stool, left hypogastric pain and head ache. Obstipation continued for one month

858 日本外科宝函第34巻 句';-11〕
unless a laxative or clyster was used, Medical examinations after the accident proved a slight hypesthesia in the whole body,
urinary incontinence and severe obstipation, which suggested a lesion in the brain and
spinal cord,
LF f川崎町吋仙いM帆んr
Rト
LT
RT ノ
LP
RP
}
{
ー
RO 市川州、・V¥j‘知叫叫似 .'toW-内州/,'
Fig. 2-a:へrリu"d; Diffuse alpha
LF
lミF
LT
RT
LP
RP
LO
RO
Fig. 2 b : Enforced l刊Pぞれでntihtion; ,low wave compon~nts prominent

EしECTROENCE!'l-IALOGRAPHICSTUDY <JN ABDOMINAL :'¥U11く( JS]メ 859
LF _,.,,,.,..齢『』
RF
LT , , ~-,
RT 山司~キ品戸"""""",、..~ヘ向、へでィ ノh dヘ~・ 、
L P ~~一川ん州~市川,J,_,J川川μ布川河ノ吋_,J¥ト'J’へ
RP 内伊内〆れ4いJ九〆へ~ , __、へ
LO 哨州判ャルャ~~i'wV"叫WザムV
RO 申d~~v、d ~吋へ.-4~ザヘJザ仲イポ~仲ザへ/'-'~,,,;--. A~ ~\し
Fig. ,2-c : After Diph. 60 mg. injected ; l~ " it1w·~,p1k, "a刊
LF~へ/叩.......,.,..‘.. 1~-.f"' .... ~仲川ぺ\八,\人ヘ町内んへ市-〆ー刊'\!,;..,...~J
LT 可~,~·~~一一)一一向ー....._.,,... v向山、二λ.人ハりd 、、N'--、.....マーr-
L P ’ぺ--'·~A「I~仙~什吋fメ"'\/Vl_..,,/j¥¥ ¥v¥,A..♂、川町 1f1".γ4円 f ~~♂
R p ... 九.,.._,.可ん~叫
LO ’W叫叫....,,,.,,・ 川川ベ刈竹午、 、;,"'-『..-.rv-ィ
RO ・.,.,...,,...一九へん川叫叫い"'-rfo,v -i'κ刊んィ/'(/V'"'、刊~九九V門Jノ~4、九 f・ぃ
Fig. 2-d ・ 15 min. after Diph. 60 mg. inj町 ted; l';ir・附いmal,1,川 、,\'a¥Tdisch.ir日。
with 6 cが杯出tivespikes

860 日本外科宝函;;~3-1谷第4 号
LF
R F 申
LT
RT 、J』~、-~、ハ~、p、v
LP 〆_,,.._,_,~件f、吋叫'·
1ミP
L O 叫戸_j,
1ミO ~:~時~'~ 、「dれ3小l'y.f¥V、‘ 」ハ、ハ、4旬、、、
Fig. 2 e : 20 min. after Diph. 60 mg目 inj町 ted; paroxysmal positive spiky wave
LF
RF
LT
RT ~
LP
RPγ.t',
LO
RU
Fig. 2-f: 15. min after Diph. 90 mg. injected; 14 cps positive spikes

ELECTIWE:\ぐJ-:PH¥ LUGRAPH!C吋rUDYON :¥BDOMINAL NEUROSIS 861
Fig. 3-a : Photo. ; Intense abdominal inflation.
Abdominal inflation was intense (3 a), and it did not change after defecation, but
it suddenly disappeared under general anesthesia. X-ray examination presented the dilata-
tion of the whole intestines. Slight intellectual debilitv with abnormal character was ob-
served. She was far from smiling and repeated the same complaints whenever we visited
her. Abdominal distention disturbed her from lying in bed, so she was standing all day
long by her bed and would not talk with other patients.
Part of her complaint seemed to be fabricated and delusive, but it was certain that
traumatic arachnitis took a part in her neurotic complaints.
For relieving constipation, the presacral sympathectomy was performed and abdom-
inal inflation and pain disappeared, but constipation is still continuing, though markedly
improved.
EEG showed much more stabilized patterns when she left the hospital than when
she was admitted. This suggests to us that peripheral continuous stimulus can have infl『
uence upon EEG. (Fig. 3 b, 3-c, 3-d, 3-e, 3 f, 3 g, 3 h, 3 i)
LF
RF
LT 、岬申軸"{M;-・.
RT 1~..,,_/、べ"''--明、仏d匂,.,,,.,..,_、_._,,...,,.哨•rN.〆VV.iw""'"'"何、 h f ‘,,. . .,.吋,_.'-,, ・.ρ、、 『 J 〆戸川,.,....,.._~.,..,戸、内
LP J門悼ぜん~{'川~../'小作J州川、同川
RP
LO 1戸川州"' fvv'....,..,『仰向付州 F ‘
RO~仰W叫叩~内川州叩州刑判、川/仰向、拘件以内Fig. 3-b:し叫1伺 l’‘1tr田t; . ¥bnormal l〕ι1ckgroundactivit、(be!けreoperatio日}

862 日本外科宝函第34巻第4号
LF ,.....,帆崎V内N'W~世恥仰向付γ人
RF 作九円、~帆~ λ
LT
RT
L P 叫州、ん吋~-,;-v..t..-.,・ヤザ~·"叩ヘ/\/νハJ ‘-~ '
RP
RO
Fig. 3-c : Arousal ; Sudden appearan目 。fslow wave (before operation)
LF
RF
LT
RT
RP
LO
RO
Fig. 3-d : 10 mg. after Diph. 60 mg. injected (before operation)
向、r 、山パ恥d'
井一♂、「.・'
I~刊、v
、目 d、
.,../'‘、ー
,-四J、’‘

ELEl.Tl<りl・:'¥iCEl'l-IALOGl¥APHlCSTUDY ON A.HD<>/\’11 >!礼L ~ E L' I<り沿い 863
LF 、ドI~岬
IミF 、~
LT
RT ー、”‘ー〆伺,、、. 7ム_,.../・/;¥, 町、へ.,f""'可川、ザ切園、’~”『》
LP μ;\人i"':f\ /\ ,r\~八山内..,...,,i"~~..川持片付時
RP
LO
RO
Fig. 3 e : 21 min. after Diph. 60 mg. injected (before operation)
LF 、ず可f軒哨v-v'"、
RF
LT
I< T /l;-N...,,.,...,.,.,,.,、~fヘJ 明 戸 、fい川'-,,,_/, Jへ九九ん_,.....,___
LP ぺ.;M抑ザ吋~~叫片山川川附刊のJ‘,"'~\大「t"\.fゆ川町九州、
IミP
Lり ザへ.t•'JVん,,...、
RO
Fig. 3-f : 22 min. after Diph. 60 mg. injected ; appearance of 11 cps spindle (before operation)

(
cc一言包CE42)
E戸一戸hZ』』Cω一吉岡号J《 一υZA一ZE二5ニ ・6『
E一塁E2
-U】吉弘S沼己創出一切且EQH4l同国広
JJf玉三ziJミミ三ミ三三ZZJ王室、告とLFI- -21Jゴ-2
・
JizJち主主主ミミ
40J且
4
~
J
,tf
-
11~人宅JJ
’Jrpι一 三F1-Y一三一一一人九三一三三ココ一一三一~~\ぺLektp\一へ一ソ宇一句、ペ,
E
,,,E3313hhミFイ吐く弓
yく
ff~ 可r’yJcjiL三rE1’ ’J5亡、つ3・1-ラ51,ミ/’HM-
、、ごLミ「4
....l
;
{
'}
e
\〉JP、与同」
(口2ち』包2EC}ω』)
ω〉句、FED3カロ吋ω一 七EM舎丘υヱA一zvE一言HUむ[
E-凶EC由よ【】問。むぷ。.2EUN一一回1伺・刷出
jy
/去手よEJ,
Sζ44j三手-57ft
74JreyLF\ゴ732/〉Ez--Z4r手
Jfry-。J
。出
「Av
-
/
i
{ ~
i 5
1之;之
<
;ミ?? 且
4
....l f-< ,..,, -
rIj\{
fE
~ ’山M【
守主jZTr〉Lエ司....l
めニ相め一円Hr国間M担体京特巴
4vu
∞

ELECTROENCEPHALOGRAPHIC STUDY ON ABDOMINAL NEUROSIS 865
LF~山『ザd旬、ーー、『凶作占..,.,,.,._,.』可申~.y
RF
LT
RT ー噌日ーー,、,、,J、~,、へ内,~、,ーへ,~、,、,、,圃戸----J旬、,F『~ぜA,『............__ー】申h,、,、ー,-可F
LP '.!'ハ~明庁、~ゆ~叫叫W叫ザψ、
RP
L O 吋 v"'¥J'VV'叫ペ11/'f¥N'仲 川 町 叫1vMt1仲川/\/,'へい V叩'JVV¥..r.,'I.山川内,\/\./\"A門 ...,.),,,九川内.'v¥}.,fl.\へ叫.('/'>
RO ,,.,.ヤ'V"vVv'.. ',,ヤルヤ....,..,山~、, f、~\¥fVv'.,.《"""''州叫り
Fig. 3 i . Arous3l ; . .¥fter operation (cf. 3 bl
Before operation, EEG in arousal consisted mainly of irregular fast waves, and they
altered suddenly to irregular slow waves.
After the intravenous injections of 60 mg. of Diph., the amplitude of slow waves
decreased, 6 cps positive spikes appeared, and slow waves with high amplitudes and 14
cps spindles became predominant.
The recording under the general anesthesia with isomital showed only a continuance
of 14 cps spindles.
After operation, EEG during arousal became stable and showed 10 cps diffuse alpha
pattern mostly (3 i).
Case 4.恥1.I., a 23 year-old business girl
Clinical diagnosis : Abdominal neurosis
Chief complaint : Abdominal inflation
Appendectomy was performed three years ago, and soon after laminectomy was done
Fig. 4-a : Photo ; intense abdominal inflation m
a case of abdominal neurosis
Fig. 4-b : Photo. ; After lumbar anesth軒目
866 日本外F、ト宝函第34巻第4号
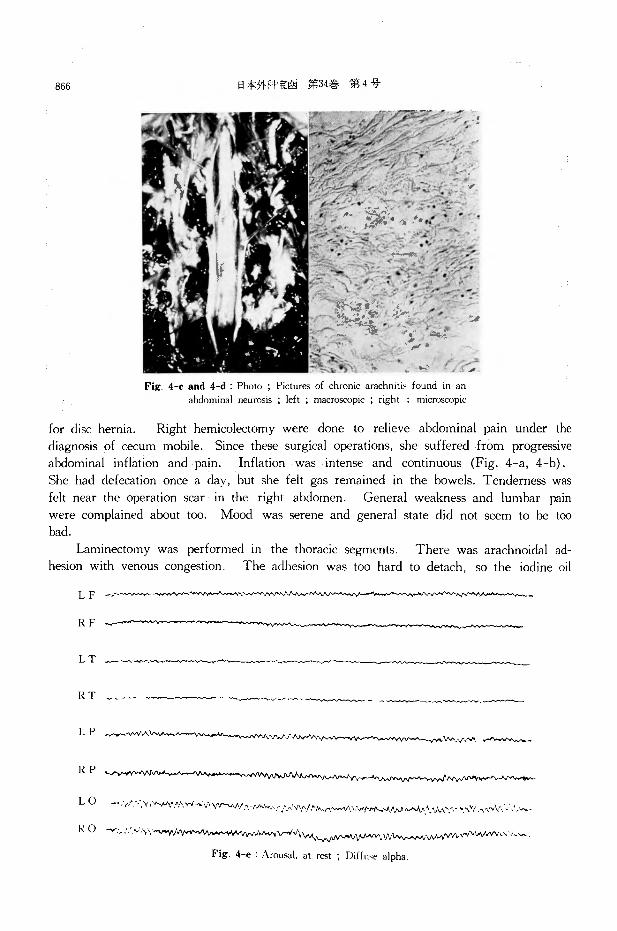
Fig. 4-c and 4-d : Photo ; Pictures of chronic arachniti> found m an abdominal neurosis ; left ; macroscopic ; right : microscopic
for disc hernia. Right hemicolectomy were done to relieve abdominal pain under the
diagnosis of cecum mobile. Since these surgical operations, she suffered from progressive
abdominal inflation and pain. Inflation was intense and continuous (Fig. 4 a, 4-b).
She had defecation once a day, but she felt gas remained in the bowels. Tenderness was
felt near the operation scar in the right abdomen. General weakness and lumbar pain
were complained about too. Mood was serene and general state did not seem to be too
bad.
Laminectomy was performed in the thoracic segments. There was arachnoidal ad-
hesion with venous congestion. The adhesion was too hard to detach, so the iodine oil
L F 一一一一町一九日押町、~./VV"o~ 、九ε申""'·,、伊向、-’,....,_...~.-
RF
LT -~ザ伊
RT vγ 、 一戸一一一一一一一「F♂4~ムん(一一ー一~)〕~-』日戸一一一f一一一~·-一一一一
L p ~,-.,,.、~W人 :¥J'./""'. .'IN-,...;."-" .,.,.』~-・
RP
L 0 ~:1,':-·汁「h州.小川市、v'VV'吋N.小山、ザムゲ〆、ハ·['/.'九八}帆;Vi'/v'札川戸川叫ん山」んやJ「、、,,._...,引いγ,._...,._・
R O ザ, ::.~’,\\『MN• •v吋市川~ψN叫伊川V\\i\んり~v.,んイ叫ん、内、WNV•山、J、h
Fig. 4 e : Arousal. at r田t; Diffu可 alpha.
,ELECTROENCEPHALOGRAPHIC STUDY ON ABDOMINAL NELIROSJS 867
mass remained in the spinal fluid after former myelography was drained, and adhesions
were left untouched. (Fig. 4-c, 4-d) Thereafter she was free from abdominal inflation
for a year and a half, that is, until recurrence.
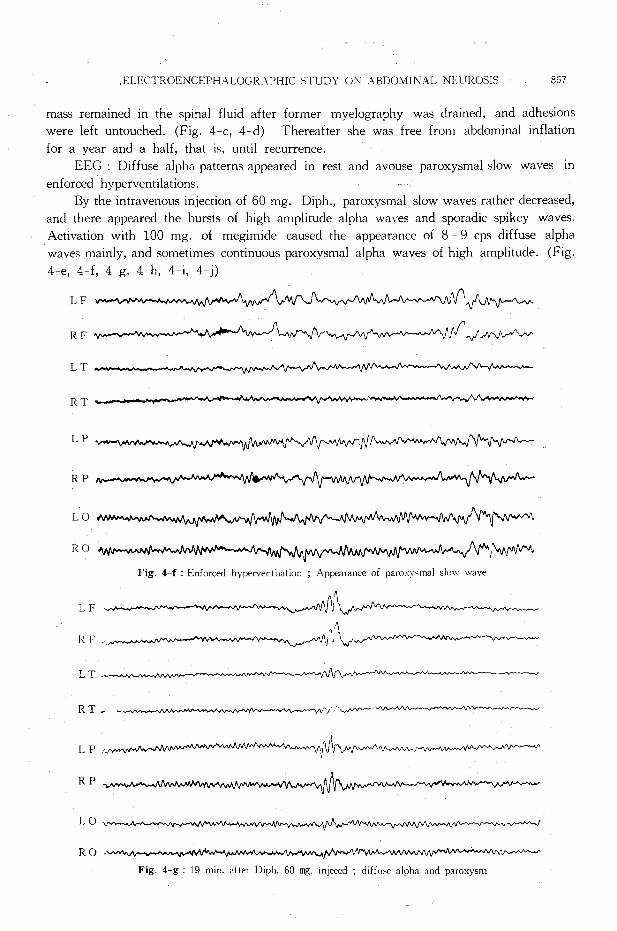
EEG Diffuse alpha patterns appeared in rest and avouse paroxysmal slow waves in
enforced hyperventilations.
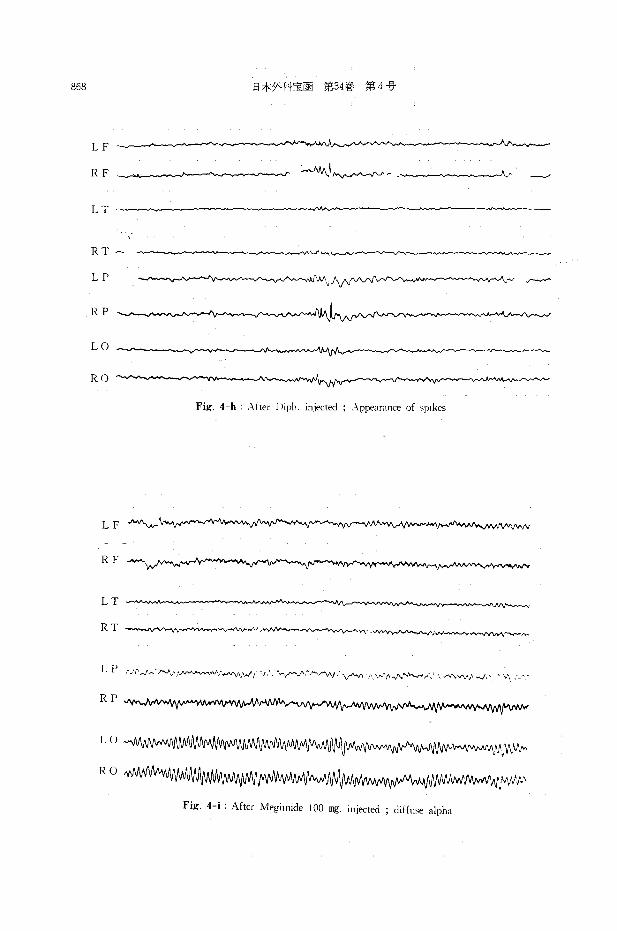
By the intravenous injection of 60 mg. Diph., paroxysmal slow waves rather decreased,
and there appeared the bursts of high amplitude alpha waves and sporadic spikey wav白.
Activation with 100 mg. of megimide caused the appearance of 8 -9 cps diffuse alpha
waves mainly, and sometimes continuous paroxysmal alpha waves of high amplitude. (Fig.
4 e, 4-f, 4-g, 4-h, 4-i, 4-j)
LF
RF
LT
RT
LP
RP
LO
RO
しF
I~ F
LT.
R T,ー
L P~
RP
LO
RO
·Y.吋I~い崎
~~\
'1、八州ハ~,
Fig. 4-f ・ Enforced hyperventilation ; Appearance of paro灯、malslo"' wave
、、p’~、,ー、,,、ー,、内u、、~
へ介九F 『叫
'V~属.,._..,..,.柏、t
Fig. 4-g: 19 min. ;ifter Diph. 60 mg. injeced ; diff1同 alphaand paroxysm
868
LF
RF
LT
RT -
日本外件宝函第34巻第4号
~!~叫ん-./V" r -
~「1
' -ーー〆
LP ('w¥ 《 f 、,--,内同
RP
LO
RO
Fig. 4 h ・λfter Diph. injected ; .¥ppearance of 'Pik田
LF A晴、_\__ 月刊'..N-N’
RF
LT .~ヘF’ー~
RT -』.,..,,....,.』、ヘザ明~}刊『'¥JV--;V,Y~・"""’ V'y-.AJV』品千,域、,_ψ--'v帆戸ψ""'》、.、 p ・,守、.
L f’ ,_1'-.1~·戸J、内/JV叫ん~、刷、’“V\J',',./'/、J人 . ..,...,.,..,、.f"-,',...V"'VV ’九〆hハハ \N'ハィ、内、、』,..,,·,• \ノ内V¥/'品帆J、、 a、,\司、角
RP
LU 川川J~川~仇{IJIJVv'M帆川付人y.,,v,,..
RO小川州刷1W¥fv#ri;州制N"'"'州州Vvv..fiNJ1州 WtlVW'刈吋NvWWINwNN:V/v'/ .. ρ
Fig. 4-i : After Megimide 100 mg. inj町 led; diffu間 alpha
ELECTRO.ENCE!》HALOGRAt》HJ(、 STUDY<JN ABIJり九1JJN孔LNElllくりSIS 869
L F ヘ〆?~ヘ~引\f, 判ザJ叫』『吋ザ叫戸~~
R F ~ルー叫叫_,..;J~ , ふ}吋品川内,・- , )九十J¥fJ.11,一LT
RT """""ん同吋吋』仏ψ快帆戸内/、~,"-.\f\ リー~円九...J\/vv"''小、い‘ゾ川~fa.品川~-Afi1'"ぜ『~叫fりハ~}川、J品川A. v-,._,」内九
L P砂川小竹ル吋./11vVJ '' i伊川川;i1円
RP
L O 伽』J~J\tvrl"V叫'WW,r,;\r叫ん咋刈WMNv~いA州川f\!\JV''--'.-.,vV'山小川前叫ん’んλ
Iミ O 州川凡~小川N内刈川1 ,t,J~ \か竹内
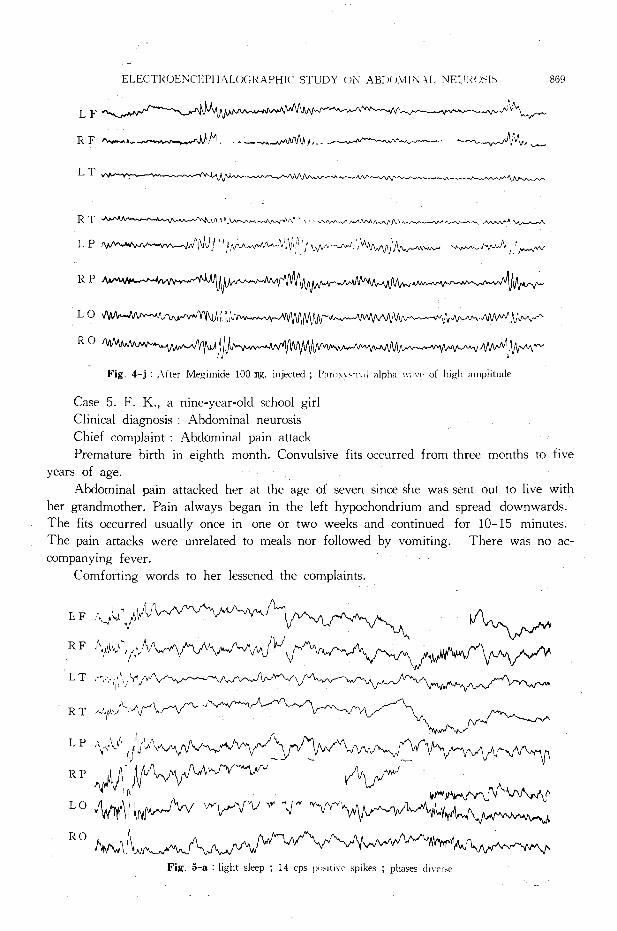
Fig. 4 j : .J..fter Megimide 100 mg目 injected ; P" r什川、m"Ialpha u川 t of high amplitude
Case 5. F. K., a nine-year-old school girl
Clinical diagnosis : Abdominal neurosis
Chief complaint Abdominal pain attack
Premature birth in eighth month. Convulsive fits occurred from three months to five
years of age.
Abdominal pain attacked her at the age of seven since she was sent out to live with
her grandmother. Pain always began in the left hypochondrium and spread downwards.
The fits occurred usually once in one or two weeks and continued for 10 15 minutes.
The pain attacks were unrelated to meals nor followed by vomiting. There was no ac-
companying fever.
Comforting words to her lessened the complaints.
I'. F i¥_)..;. :./Jν
RF川「川いザ\/'-い川久 JHパぃ》ゾ刷
L T ,勺九1',\\ペfへ~戸~~
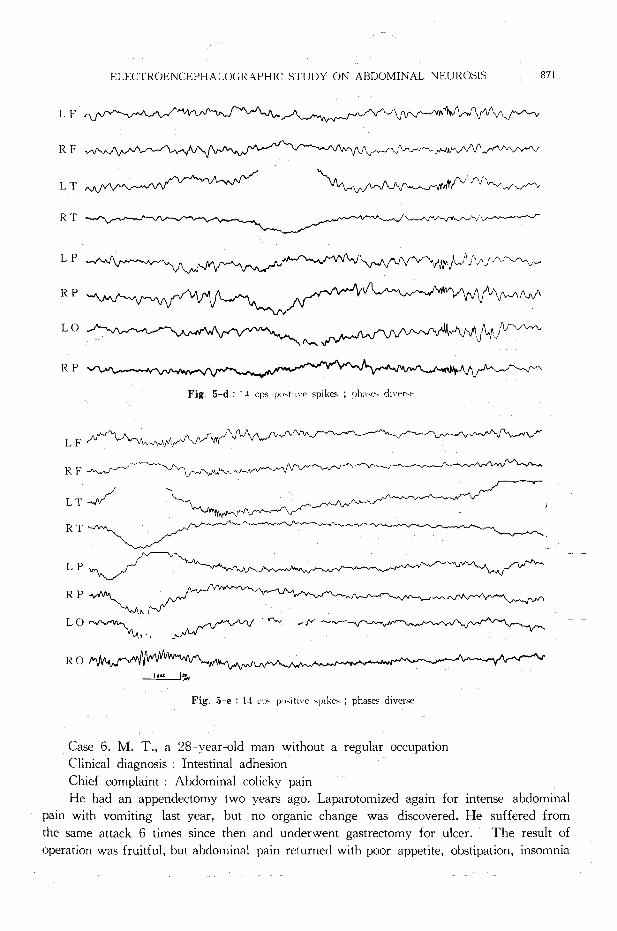
Fig. 5 a : light sleep ; 14 cps l"'''ti、cspikes ; phases【!日er>e

870 日本:外科’i::両 第34巻第4号
With the help of x-ray examination tenderness was detected in the duodenal bulb,
and hypermobility of the cecum was demonstrated. She left the hospital during the course
of internal treatment, which seemed to be fruitless.
EEG : In rest and arousal : About 10 cps alpha waves predominated, and slow wave
components were contained in them.
Natural sleep caused the appearance of 14 and 6 cps positive spikes. Concerning 14
cps positive spikes, as seen in Fig. 5, they were synchronous in all leads in most国 ses,
and the phase on one side inversed sometime to 14 cps negative spikes. Irregularly mixed
positive and negative waves were observed. (Fig. 5 a, 5-b, 5・ c, 5-d, 5-e)
LF
RF
LT、 UへハへFヘ'"v"ルザ~ h 刈 f叫W刊「刊P、'1
R T ~九~4ν巾\斗,rv-・
RO
↑
Fig. 5 b : light sleep ; ~I I cps pn,it川‘spik白 ;phasesdiverse
LE
R守 Y 〆\‘、.叩」ρ‘‘盲:.',\';::;‘ 3、\~ J
ヨ 『 ー て 、J「.....,_,..,叩....,.....,,,.._,,,.,._’\介、l'. .f同~~へ~~ノヘ~~
RT ·-·-~ ~ "'吋f.;.、~ヘ『F~/"'°「~~ ."-._、
LP ,‘ ·"~’ v、炉供/’ ,. 、/~ペヘノ〆、六日勺\:;九仰'/,A'J,’ハ·rY·、.!/,,.~ヘノイヤMψ·./'o'~rfr,/'~ V
R I 、A,,山 、
り一一NJ..,f"X•,j)"' ,..J. ‘ -1.o'1 爪 A~;川V1. f· J 且四 A 入内山舟~~州 、Jヘ爪〆吋 J ./'1 y 川九rf"\/V\'イ~刊..,.,,rr- -..,.
L <J 、,,_.,,,,vvvh./'fv胡刊〓‘一 一-・ •• , Y"Yy'/';ソ''~-!'川町ヘイヘ~J.,/"""'~州い·Jl/V"ψ~ザ~p帆ペ
一」Z竺_J~,
Fig. ::i-c I .1ght sleep ; 6 cps戸)Sitive尽pik白
ELECTROENCEPHAしυGRAPHICSTUDY ON ABDOMINAL NEUROSIS 871
L F ヘYれ~~/ f九vハ~ιんへ'\jト~叫ん、f引ヘベf""-v
RF .~九州/"p./\/\___,ィ'\J\ryv-へ/
LT \ い川刈」川伽N 付 V-.V,,v、_/""v
RT l、vi.介~‘
LP J叫r~〔'\)\p〆γ引戸川F~ム~t州~川庁、t'~"JしへJへんrん~「戸
RP 叩吋吋八九/か~〆γ~心ぃ~州いMLO
(¥.,.,_
RP
Fig. 5 d : 14 cps po,111、ぞ spik田; 1》h;i、。 diver吋
L F 〆ぺへ丸刈λμ〆Mノw~州、ノ~
RF °"""戸山/~.~~「~.
LT~ \川 山川 \/ ヘ
RT
LP
RP 民/レwム_,-ヘ、内Jγ、叫v-F
LO,....,,-.,.州、川町、 ρh門り吋‘~ t〆~..,,.....
RO
一」三三一」%
Fig. 5-e : 14じpspositive spike、; phase<diverse
Case 6. M. T., a 28 year-old man without a regular occupation
Clinical diagnosis : Intestinal adhesion
Chief complaint : Abdominal colicky pain
.~~
·~ゾ~\/
He had an appendectomy two years ago. Laparotomized again for intense abdominal
pain with vomiting last year, but no organic change was discovered. He suffered from
the same attack 6 times since then and underwent gastrectomy for ulcer. The result of
operation was fruitful, but abdominal pain returned with poor appetite, obstipation, insomnia
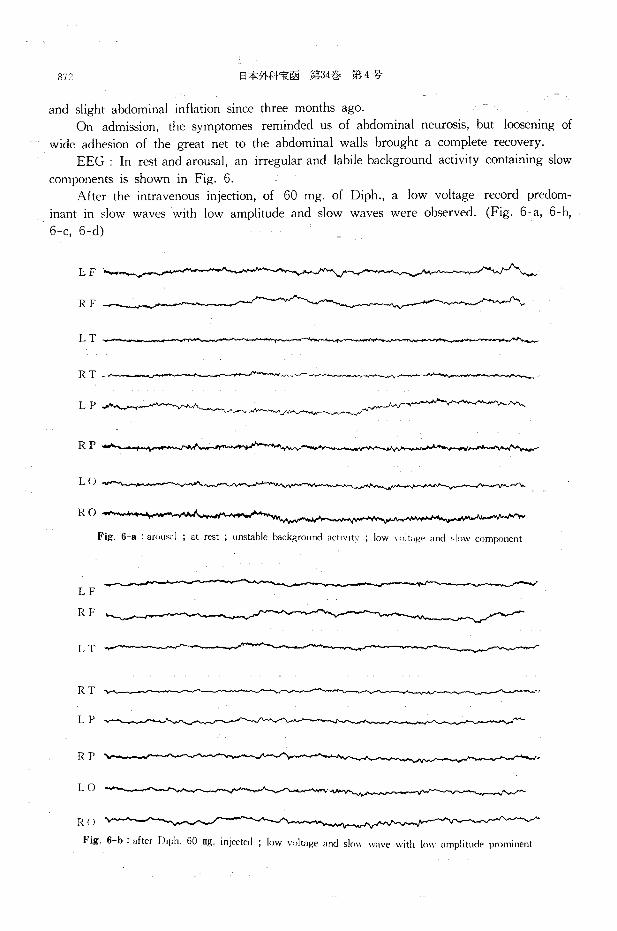
872 日本外科宝函第34巻第4号
and slight abdominal inflation since three months ago.
On admission, the symptomes reminded us of abdominal neurosis, but loosening of
wide adhesion of the great net to the abdominal walls brought a complete recovery.
EEG : In rest and arousal, an irregular and labile background activity containing slow
components is shown in Fig. 6.
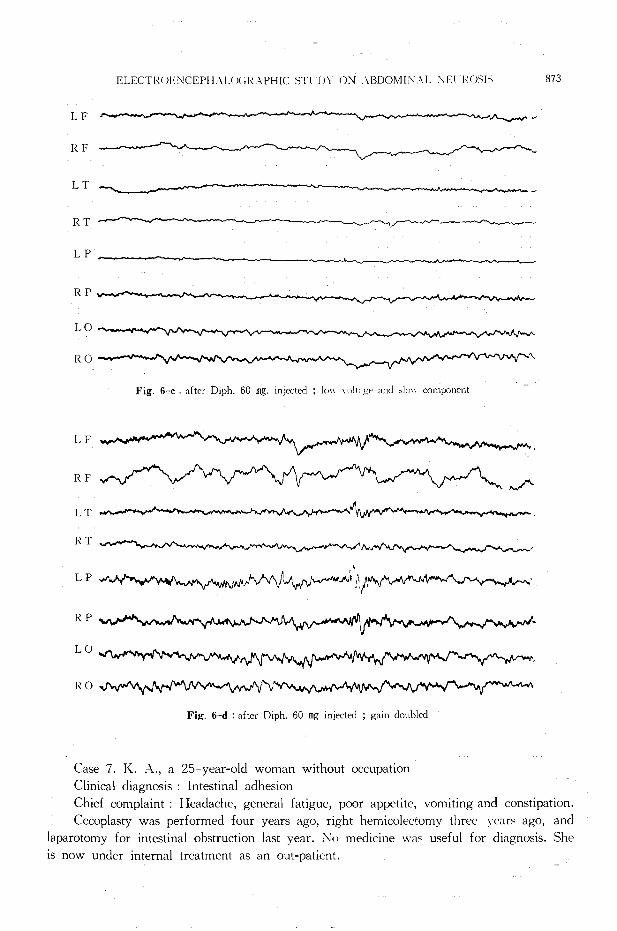
After the intravenous injection, of 60 mg. of Diph., a low voltage record predom-
inant in slow waves with low amplitude and slow waves were observed. (Fig. 6-a, 6-b,
6-c, 6-d)
RF
LT
RT- ~寸dー可,........_______、-・-、...-
LP
RP
L (J
RO
Fig. 6-a : arou日 I; at r田t; unstable background川:t1v1t、; low、,けl t:ig~ and 'low com戸)nent
LF
RF
LT
RT
LP
RP
LO
R()
Fig. 6-b after D1ph. 60 mg. injected ; low vリIt噌eand sic"'’叫 ・avewith l口、、 amplitudeprominent
ELECT!¥( JENCEPH主UJC;RAPHICSTl'llY ON .¥BDOMI:¥.¥L '¥El IIく(肘JS 873
LF
RF
LT
RT .r-、「ノ~司
LP
RP
LO
RO へ
Fig. 6-c : after Oiph. 60 mg. injected ; !"" '""lt:i日rand山川v component
LF
RF M ノヘ
LT
RT
LP 吋れザ判、。へ内臥時れトペへ村ザ吋刻、 :'/""'れゆ州民ヘ~吋、r吋
RP
L O 叫~特~.
Fig. 6-d : after Diph. 60田ginjected ; gain doubled
Case 7. K.λ., a 25 year-old woman without occupation
Clinical diaεnosis : Intestinal adhesion
Chief complaint : Headache, general fatigue, poor appetite, vomiting and constipation.
Cecoplasty was performed four years ago, right hemicolectomy three war~ aεo, and
laparotomy for intestinal obstruction last year. .No medicine w川 usefulfor diagnosis. She
is now under internal treatment as an out-patient.

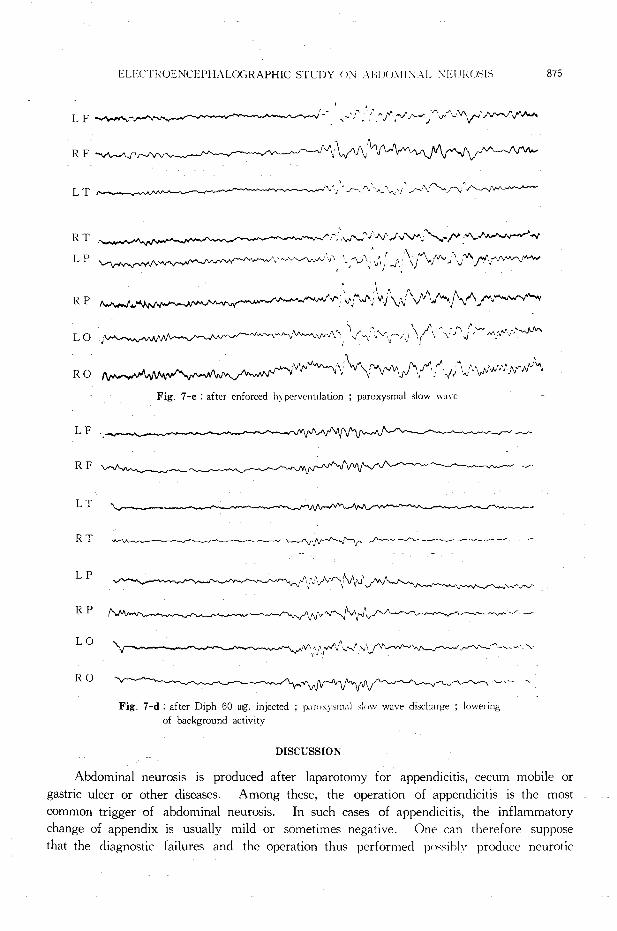
874 日本外科宝函第34巻第1号
EEG : In rest and arousal, EEG show the recordings with slow wave components,
labile background activity and predominance of alpha waves. In enforced hyperventilation,
there appeared multiple paroxysmal slow wave bursts markedly.
After the intravenous injection of 60 mg. of Diph., slow components predominated
in background activity and paroxysmal slow wave bursts with lower amplitudes appeared
frequently. (Fig. 7 a, 7-b, 7-c, 7-d)
LF
RF
LT
RT "'vv+V'·小ι引~吋同,~ 、ー「d 一、〈ー
LP .,、,、、
RP .,
L O へ.,,,...._,.~~h ~Jへ、、ー
RO ぺ、,、、.、、
Fig. 7-a : A.rousal ; Unstable background activity and slow wave component.
L F 、・4’‘同d,,、
RF
LT 'v-,、〆『司、
RT iノV ;-、同ノ』\岬d 叫んヘ《ヘF 吋 J、
LP
RP ~ .v.晶仇>fv*/JV....向'v""'
PO 勺仇へ川'J/川九心;-·--.~·
R 0 -v..)~叫
Fig. 7-b : after enforced hyperventilatiりn; ,J,川 componentsprominent
ヒLEC!、lくOENCEPHALOGRAPHICSTUDY < >>! λBl J( Ji¥11 X主Lr¥E二lTJ<()吋1:-i 875
LF h内同帆、「' - ,~·:' f《〆プハ_,.,.,.\,,,~"YI. /'"'.ムh~へr"'-
ー”.・,' "
RF -v九~.11..J、 V'~ν、へ
LT JトJ~、べ、心~J.~.f'-v.パトー什~一一
RT
LP Lペriv「f内ザ~
へ·~"""'-''\/吋,,/v"-"";~/ゆ旬、./'~·吋
.. ,.小_..rv._,;v'・の,\旬、\";,/ -Jイ\;へ(""'J'Jヘベ〆・,""'JVゲ小切
RP ,...,,.,,._,,
LO
RO
LF
RF
LT
RT
LP
RP
L 0 '-
RO
川t.,,J¥j¥.")'¥f、('-JVベハ/\ハf内い内
へい品川I \;ノJ代、,~'\·入戸町γ
Fig. 7-c : after enforced h) pぞrventdatio日; paroxysmalslow ¥¥ave
'1'~「r-「f
\;Jv人~\1\1\J、J州叫~ー~》、v『れ./"'-"ふ-.;-../"
J~「.f',IV」一一~一月(~_,...,..._,._,,.,.- ~.r, __r
'.,'!'.〆人~、/;._.,\~A.I'-〆""'-'〆~\~、、-.'.,.
Fig. 7-d : after Diph 60田g.injected ;!〕川りxy,;rn.il,;!《>W wave discharge ; lowering of background activity
DISCUSSION
Abdominal neurosis is produced after laparotomy for appendicitis, cecum mobile or
gastric ulcer or other diseases. Among these, the operation of appendicitis is the most
common trigger of abdominal neurosis. In such cases of appendicitis, the inflammatory
change of appendix is usually mild or sometimes negative. One can therefore suppose
that the diagnostic failures and the operation thus performed pけ時ihlv produce neurotic
876 日本外科宝函負}341'-第 4号
comp lam ts.
C. KIMURA called our attention to faulty spinal anesthesia as an etiological factor of
this disease, because he found severe fibrotic arachnitis with adhesions and venous conges-
tions in the laminectomy of these five cases. According to him, the inflammatory change
of the arachnoid was severest in the sacral region, and it extended to the thoracic ar田.
Trauma, bleeding by the needle or the toxic stimulus and infection by injected impure
anesthetics or by instruments in spinal anesthetic process 回 nbe the cause of arachnitis.
Abdominal neurosis回 noccur, on the other hand, following vertebral injuries by accidents
or by a surgical operation as introduced in this report.
This is a fact in favour of KIMURA’s opinion. The organic changes in the abdomen
are too few to explain the specific symptoms of abdominal neurosis, and the greater part
of them seem to consist of psychoneurotic factors.
They are suggestive of intestinal obstruction or dyskinesis, megacolon, intraabdominal
adhesions, dumping syndrome, gastric or duodenal ulcer, epilepsy and other psychiatric
diseases, but none of them explains the symptoms exactly. Adhesive spinal arachnitis has
been pointed out by MAEKA w A, and the pathological picture was demonstrated by KIMURA
in laminectomized patients. The inflammatory focus in the sacral region of the spinal
cord explains well the occurrem、eof obstipation as well as the abdominal inflation. Ho-
wever, arachnitis, too, is not enough to answer the question why such complicated psyc-
hotic symptoms appear. Complications and troubles in patients lives aggravate the symptoms,
while engrossment in a work can set them free from disorders.
ι、hangeof life environment, for instance, marriage, is sometimes beneficial. These
facts suggest to us pathological factors in the brain, in addition to spinal arachnitis.
(、onsideringa psychosomatic disease, the author made an electroencepharographic study
of abdominal neurosis.
Idea of thalamic and hypothalamic epilepsy was established by F. A. GIBBS and E.
L. GIBBS, and there are many works concerning the subject by GIBBS and GIBBS, T. M. GARNSESKI, T. R. GREEN, R. s.孔1oRISONand E. W. DEMPSY, D. B. RrNDSLEY, R. A.
HAYNE and others. GIBBS et al. studied on EEG of sleep and observed that 6 % of his epileptic patients had 14 and 6 cps positive spikes. Most of the patients who had 14 and
6 cps positive spikes complained about some autonomic nervous disorders, so GIBBS pointed
out these spikes as a proof of epileptic deep focus and called this disease “thalamic and hypothalamic epilepsy'’ electroencephalographically. Since then many discussions have been
done on the relationship between the symptoms and the spikes. In Japan Y. SHIMODA,
observed EEG of various autonomic nervous disorders and divided the thalamic and hy-
pothalamic epilepsy into two groups, i. e. one as a 14 and 6 spike type and the other as
a paroxysmal slow wave type. SHIMODA et al. reported the activation with intravenous in-
jection of Diphenhydramine and the present author agrees with this. (Table 6 and 7)
GIBBS et al. illustrate that the form of this spike is brought by elimination of negative
phase from 14 cps spindle wave in normal sleep, and that this app田 rsdiffuse without any relation between left and right side.
R. A. HAYNE, L. BELINSON, and F.ヘ.GIBBS describe that “positive’P originates in the disorders of the deep parh.
ELECTIWENCEPl-L'¥L< Jf ;[\λPHIC STUDY U:'¥! :¥BDOMII¥.¥L :'¥:EURUSI吋 817
Diffuse and not synchronous (left and right) waves of 12 cps are shown with 6 cps
spikes by the author (Fig. 1 b, 1 e, 1-f, 1 g). The author would regard these waves
as ones having the same value as 14 and 6 cps positive spikes, because the ascending
brainstem activating system must be taken into consideration. There is an opinion opposed
to Grnss that 14 and 6 cps positive spike~ are nothing other than spindle waves in a sle-
eping stage. There is another report that the spike has no correlation with autonomic
nervous epilepsy. Fourteen cps spikes synchronous in all leads are not always positive.
The inversion of the phase is recorded independently of the le泡dingparts (Fig. 5-a, 5-b,
5← d, 5 e). The author supposes this may be a varied form of 14 cps positive spike and
is regarded as an abnormal sign in this report, but E. L. Grnss describes that such a
pattern can be detected in the normal youngster.
D. B. LINDSLEY and H. W. MAGOUN made a report on paroxysmal slow wave.
According to their experiment on acute injuries of mid-cerebrum, thalamus or cortex,
the wave is recorded when cortex is free and thalamus or hypothalamus is injured. They
consider this wave relates to ascending brainstem activating system. However, the slow
wave is only a sign of abnormalities, because this is found in epilepsy, psychosis, tumor,
mental weakness, delinquency or other cerebral disorders.
Whether paroxysmal alpha wave of high amplitude (Fig. 1 c, 1 i, 4-g, 4 j) is an
alpha rhythm or the wave built up, it is important to note the prominance in amplitude.
T. WADA interprets this wave suggestive of the activated neuron just under the electrode
synchronous with cortical function and usually comes from epileptic disorders.
As abnormal background activity, there is a recording of low voltage, which is fast
wave without rhythm, and sometimes contains slow wave of low voltage (Fig. 3 b, 6 b,
6 c, 6 d).
Continuous fast waves of a normal person are classified into M type (GOLLA, HuT-
TON and WALTER, 1943). In凶 se3 this pattern transfigurates at light sleep stage into
slow wave and 14 cps spindle wave (Fig. 3 b, 3 c), but normal alpha rhythm is not
seen in transfiguration time. Encephaloglaphically the patient fall from a state of being
wide awake to sudden sleep. In this case such an abnormal background is always seen in
preoperative time, and a stable alpha rhythm is produced after recovery by an operation
(Fig. 3 b, 3-i). Abnormal background is brought by cerebral activation with peripheral
continuous stimulus and a stable alpha rhythm is produced after the stimulus disappears
by an operation.
This is suggestive of peripheral factor which causes abdominal neurosis.
Fourteen, or thereabout, cps spindle wave is originated in thalamus and hypothalamus
or the course from them to the electrodes are disturbed (Fig. 1 a).
Slow wave components in arousal are prominent in the cases of present report (Fig.
1-b, 2 d, 3-c, 6-a, 6-b, 7 a, 7 b). This suggests that there lies slight cortical insuffic-
iency or a disordered relation between cortex and subcortex.
Many spiky waves are seen which appear without focus and unfixed in any leads.
(Fig. 1-a, 2 c, 2 e, 3 d, 4-h)
Many of them are fast alpha waves, which are suggestive of continuous activation of
cortex. These wav引 appearalso in the cerebral angiospasm, which is influenced with
878 日本外科宝函第34巻第4号
thalamic and hypothalamic disorders.
The present author discussed here on abnormal waves and the waves on borderline.
There is no spike and wave complex in his report. Abnormal waves discussed here are
sometimes seen in normal persons, so the above discussed waves have no conclusive in-
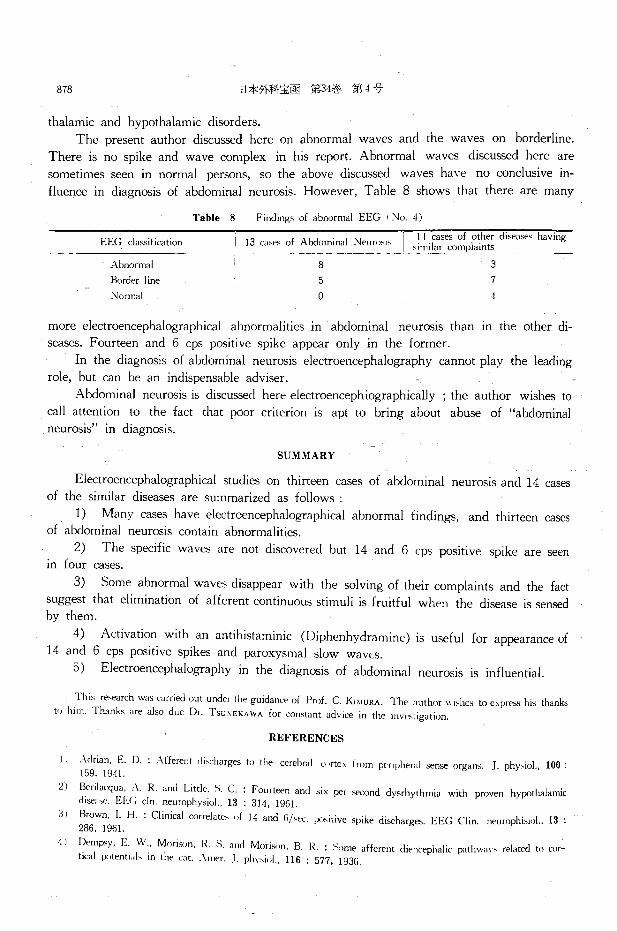
fluence in diagnosis of abdominal neurosis. However, Table 8 shows that there are many
EEG cla田ifi田 t1on
Abnormal
Border line
Normal
Table 8 Findings of abnormal EEG < No. 4)
I II cases of石I辰「dise;i蛇き4五avn" I 13 GI附 d A凶om
8 3
5
0
7
cl
more electroencephalographical abnormalities in abdominal neurosis than in the other di-
seases. Fourteen and 6 cps positive spike appear only in the former.
In the diagnosis of abdominal neurosis electroencephalography回 nnotplay the leading
role, but回 nbe an indispensable adviser.
Abdominal neurosis is discussed here electroencephiographically ; the author wishes to
call attention to the fact that poor criterion is apt to bring about abuse of “abdominal neurosis" in diagnosis.
SUMMARY
Electroencephalographical studies on thirteen cases of abdominal neurosis and 14 cases
of the similar diseases are summarized as follows :
1) Many回 seshave electroencephalographical abnormal findings, and thirteen回 ses
of abdominal neurosis contain abnormalities.
2) The specific waves are not discovered but 14 and 6 cps positive spike are seen in rour cases.
3) Some abnormal waves disappear with the solving of their complaints and the fact
suggest that elimination of afferent continuous stimuli is fruitful when the disease is sensed
by them.
4) Activation with an antihistaminic (Diphenhydramine) is useful for appearance of
14 and 6 cps positive spikes and paroxysmal slow wavt:.s.
5) Electroencephalography in the diagnosis of abdominal neurosis is influential.
This re-earch w出目的吋 outunder the guidance of Prof. C. KIMURA. The author川市白 toexDr,品 histhanks to him. Thanks are also due Dr. Tsu:<EKAWA for constant advice in the川町、tigat川n '
REFERENCES
JIλdrian. E. D.:λfferent di,charg田 tothe cerebra I 山 rtexfrom pt>ripher川|担nseorgans . .I・phy,iol.,100・159. 1941.
2) Berilacqua, :¥. R. and Little, S. C. : Fourt田 nand six per sεcond dysrhythmia with proven hypothalamic ぐlise;i~-. EEG cln. neurophysiol., 13 : 314, 1961.
3J Brown. I. H. : Clinical correlate' nf 14 and 6ハ町 p)'itiveぉpikedischarges. EEG Clin. neurophisiけI.,13 : 286, I 961.
4 J DemP'y, E. W .. Morison, R S. and Morison, B. I~. : Sけmeafferent di刊 cephalicpathwa¥'S related to cor-tirnl potent1;ils in the cJt .. ¥mer. J. phy、iol.,116 : 577, I 936.
ELECTROENCEPH ,¥ Lυ<;RA!’HIC STUDY (JN ABDOMJN,¥L NEUROSIS 879
5) F【irlxヘ,A and M<>ri-.仇 B R. : Cortical r白戸川日 to問 11川 ry,timulation 11nder deep barbiturnte narco山
J. neurophisiol., 2 112, 1939.
6) Garnseski, T. M. & Green, ] . Iミ: Recordingof the fourteen and six per可rnnd,;pike phenomenon. EEG
din. neurophi,iol, 8 : 501, 1956.
7) Gibb,, F. A. &: Gibbs, E. L. : Atlas of electroencephaloglaph、Vol.2, Epilq川ふkli"m-Wc..,.Je¥' pr側
Inc., 1952.
8) Gibbs, E. L.ぶ: Gibbs,F.λ : Electroencephal"graphic evidence of thalamic and hy伊 yhalamicepilep')・Neurology, 1 : 136, 1951.
9) H1¥'lle, R. A., B~lin;on, L. and Gibbs, F.主: Electric:ilactivity of subcortical areas in epileJ>'y. EEG
cl in. neulophisiol, 1 : 437, 1949.
10) Hughes, J. R., Gianturco, D .. Stein. W., Curtin, M. ]. and Bn川 n.V. P. : Electrical correlations in the
positive spike phenomenon. EEG clir、neurophisiol.,13 : 599, 1961
11) Kennard, M. A. EEG ch3ng田 町 curring with dro\\、ine,;, in emotion: lly disturbed children. EEG clin.
neurophisiol., 13 : 305, 1961.
12) Lindsley, D. B., Bowden, J. and M.i.~•Jun , H. W. : Eff町 tupon the electroenceph"l"graph of acute iniury
to the brain stern activating町、tern.EEG clin. neurophy、iol.,1 : 475, 1919. 13) Mary, A. B. Brazier : The electrical activity of the nervous川、tern.Sir 1'.1ac Pitman &白川sLtd. L<Jllciリn,
1959.
14) Niedermeyer. E. and Knott, T. R. : The incidence of 11 and 6んe仁 positivespik田 inpsychiatm・ material.
EEG clin. neurophisiol., 14 : 284, 1962.
15) s,.no, K. and h 伴ishima,C. : Electroenchephalographical and clinical study of autonervous epilepsy. Folia
p、ychi拙tricaet neurologi田 Japonicasupplementum, 3 : 21, 1957.
16) Presthw,, J ., Ref sum,ろ.:うkulated.A. and Osteneji:i, S. : Clinic・al correlates of 14 and 6 per second positive
spike,;. An electroencephaloglaphic and clinical stud) ・ EEG clin・neurophisiol.,14 : 953, 1962.
17) Sellden, U. Electroencephalographic effects of Megimide in normals. EEG clin. neurophisiol., H : 954, 1962. 18) Shimoda, Y., Hanazono, N., Koizumi, A. and Kadowaki, K. : The pri1rnry thalamic and hypothalamic
epilepsy. The Yonago acta medica, 2 : 2. 1957.
19) Shimoda, Y., Koizumi,λand Tanal・伺, K ・ Electroenchephal<】graphicacti¥'atiリnof“Diencephalic epilepsy” with diphenhydrarnine. The Y onago acta medical, 4 . 99, 1960.
20) 荒木千里:外科より見たる内臓の主主痛臨床外科,4: 73, 1949.
21) 荒木千里:外科に於けるヒステリー.日本外科宝函, 22: I, 1953.
22) 東雄司:神経症様愁訴に対する脳波検査の意義.和節、山医学, 12, 1960.
23) 早坂 視:術後腸管癒着の諸問題. 外科治療' 2: 538, 1960.
24) 池見酉治郎.精神身体医学の理論と実際.医学書院, 1962.
25) 池見酉わ;f!I;, 舟橋佑二 :発作性腹部膨満症について.日本医事新特, 1589: 1 ~03. 1954. 26) 今井五郎:慢性便秘とその外科的療法.外科治療, 8: 261, 1963.
27) 石原 隊,吉井直三郎:非行少年と異常脳波型について. 臨床脳波, 3,1961. 28) 亀田治男 :神経症性腹部具満症について, 日本医事新報' 1816 : 23, 1959.
29) 金久卓也p 山本喜三郎:過敏性大腸症候群ーーその精神身体医学的観察 ー .最新~ii "λ17 : 2346, 1962, 30) 木村忠司:以射性通過障害並びに腹部神経症に就て. ~>i·予, 6 : 28, 1950,
31) 木村忠司:消化管の運動失調.日:本医事新報,1960: 103, 1956.
32) 木村忠司 :内臓痛.外科治療' 4・728,1961 33) 木村忠司 :慢性便秘症の外科的療法.外科、冶療, 5: 320, 1961.
34) 木村忠司:疹痛とその対策.外科治療.7 ・ ~3. 196'.:'..
35) 木村忠司,恒川謙吾 :腹部神経症の診断と治療. 治姶, 3:861, 1961.
36) 木村忠司, f亘川謙吾,山本昭孝 腹部神経症の本能に関する最近の知見. n本外科学会総会, 1961,(日外会誌, 62: 1453, 1961)
37) 木村忠司,恒川謙吾p 二村美而,池田正尚:術後性便秘症. 外朴診僚, 5: "17, 1963,
38) 喜多村孝一:臨床脳波に於ける赫波の検討.医療' 13 : 149,
1959.
39) 前川孫三郎:限局性蜘昧膜炎に就て.日本臨床, 5: 565, J ~h7. 40) 前川孫三郎’精神身体医学への一つの警告p 軽症蜘妹膜炎と神経症. 沙問iと;f;i恥 38 81, 1950.
41) 絵本喜幹:慢性便秘症に関する実験的並びに臨床的研究,横浜市大誌, 10: 966, 1960.
42") 松永藤雄:体質性腹部三主徴の解説.日本臨床, 9: 1028, 1951.
880 日本外科宝函第34巻第i号
43)溝田成 :慢性便秘症の検討.治療, 45 : 524, 1963,
H) 中村 武,山本勝美,石嶋福昭,横田俊二:胃腸運動と脳波との関係.日本生理学雑誌, 21 : 872, 1959.
45) 中村一夫:小児科に於ける脳波検査の状況.交通医学' 15 44, I 961,
46) 中山恒明,中村武:機能的消化器疾患の中枢との関係.日本消化器病学会雑誌, 57 1853, 1960.
」71 中村一夫:抗ヒスタ ミン製剤 Benadrylの誘発脳波.交通医学, 15 : 226, 1961.
48) 直井 工事・p 井上令-, 桑村智久,平沼 時p 大熊輝雄:てんかん境界領域の脳波. 臨床脳波, 4: 241,
1962.
49) 小沢凱夫・他:慢性便秘症.日本外科学会雑誌, 13: I 181, 1962.
50) 下回叉季雄:間脳視床下部発作症の臨床, 最新医学, 12・2538,1957.
51) 下回又季雄 自律神経性てんかんの臨床的ならびに脳波学的観察.最新医学, 15・2537,1960.
52) 下回ス季雄.間脳性発作症:脳幹性発作症.日本臨床' 20 : 404, 1962.
53)- 回北周平:腸管癒着症の統計的観察.外科治療, 1・173,1959
5~ ) 内田宗利 :慢性便秘症の臨床的組織学的研究と手術適応について.横浜市大誌、, 10:671, 1960.
55) 和田豊治:臨床脳波.金原出版,東京, 1961.
56) 渡辺武:自律神経症の脳波検査に関する研究.千葉医挙雑誌, 33 : 12日, 1959.
57) 吉井直三郎:条件反射と脳波.精神々経学雑誌,60: 9, 1958.
和文抄録
腹部神経症及び類似疾患の脳波学的考察
京都大学医学部外科学教指第2講座(指導:木村忠司教授)
キサ )'.~ 而
主に,開腹術をうけた後で発症しp いろいろの治療 脳波記録はp いわゆる単極誘導法により,強制過呼
に頑強に抵抗する愁訴たとえば著しい腹部膨満や不定 吸や薬物賦活 (Diphenhydramine,Megimideの静注な
の腹痛とか排便障害などがあり 3 その病状形成の上に ど)を併せ行なった.そして,腹部神経症13例,近似
精神々経性の要素が多分に含まれているものを,腹部 疾患14例の検査の結果p 次の如き結論を得た.
神経症と呼ぶ。このような症例に対して,更に開腹術 1) これら双方の患者では,脳波異常を示すものが
をくり返すことは無効であるばかりでなく,症状を益 多〈,特に腹部神経症では全例に異常が認められP 1l
々悪化させる。またp 各種交感神経手術も一時は奏効 つ類似疾患、と較べてその程度も高かった.
するものの,数週間から l年以内に再発する. 2) 腹部神経症に特有の脳波所見はなかったが, 14
本症の病態や治療法を解明せんとする努力はp 長年 及び 6cps陽性腺波を示した 4例は,何れも腹部神経
続けられて来たにもかかわらず,まだその診断の確か 症の底、者で,自律神経中枢の異常が暗示された.
な根拠さえ乏しい情況にある.そして本症はいろいろ 3) 腹部神経症の異常脳波所見の中には,症状消失
異なる病名のもとに報告されている一方,腹部神経症 と共に消縫する patternがあり,本症治療』こはp その
という病名が乱用されている傾向もある.更に,斯る 病状形成に関与している上行性の持続的刺激状態を取
忠ιは多くの 臨床家の下で難物として苦慮されてい り除く事が有効であると与えられる.
る. 4) 脳波検査に隊長して, 抗ヒスタミ ン剤 〔Diphhn-
著一部む本症が中継神経系と密接な関係を有する点 hydramine)の静注は,異常’波とくに1-1及び 6cps陽性
にi主目しP これにtl~波学的検討を加えてP 診断の一助 州j主や発作性徐波の検出に有効であった.
としp 且つ治療方診の決定に際する示唆創出ょうと試 5) l阿波倹査で多くの異常を発見することは,腹部
みた. 神経症と診断する一つの根拠となる.





























