Embed Size (px)
DESCRIPTION
稳定性冠心病的治疗策略 Therapeutic Strategy of Stable Coronary Artery Disease. 朱建华 Zhu Jianhua M.D. 浙江大学附属第一医院 The First Affiliated Hospital of Zhejiang University 2013.7.26 哈尔滨. 稳定型冠心病的概述. 稳定性冠心病 (SCAD) 也称为 稳定性缺血性心脏病 (SIHD) - PowerPoint PPT Presentation
Citation preview
朱建华Zhu Jianhua M.D.
浙江大学附属第一医院The First Affiliated Hospital of Zhejiang
University
2013.7.26 哈尔滨
稳定性冠心病的治疗策略Therapeutic Strategy of
Stable Coronary Artery Disease
稳定型冠心病的概述稳定型冠心病的概述
稳定性冠心病 (SCAD) 也称为稳定性缺血性心脏病 (SIHD)
Defined as an established pattern of angina pectoris, a history of myocardial infarction, or the presence of plaque documented by catheterization.
Prevalence: 20–40 per 1000 person
Almost 17 million patients in the United States have stable CAD, and nearly 800,000 more will experience an initial event each year.
Circulation 2009;119:e21-e181 Heart disease and stroke statistics—2009 update
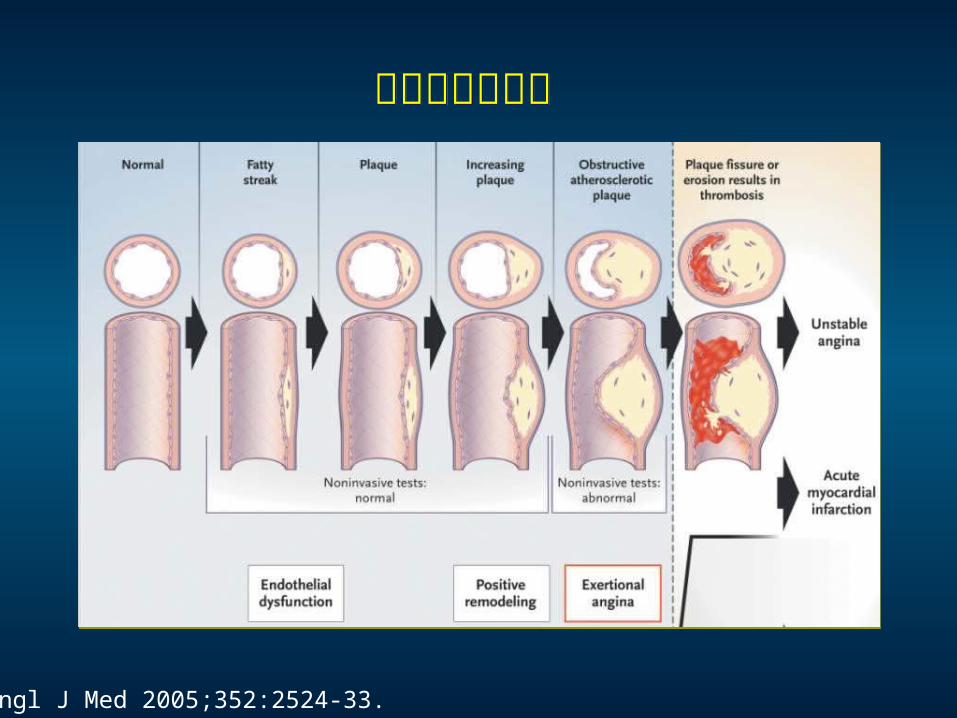
N Engl J Med 2005;352:2524-33.
冠脉病变的进展冠脉病变的进展
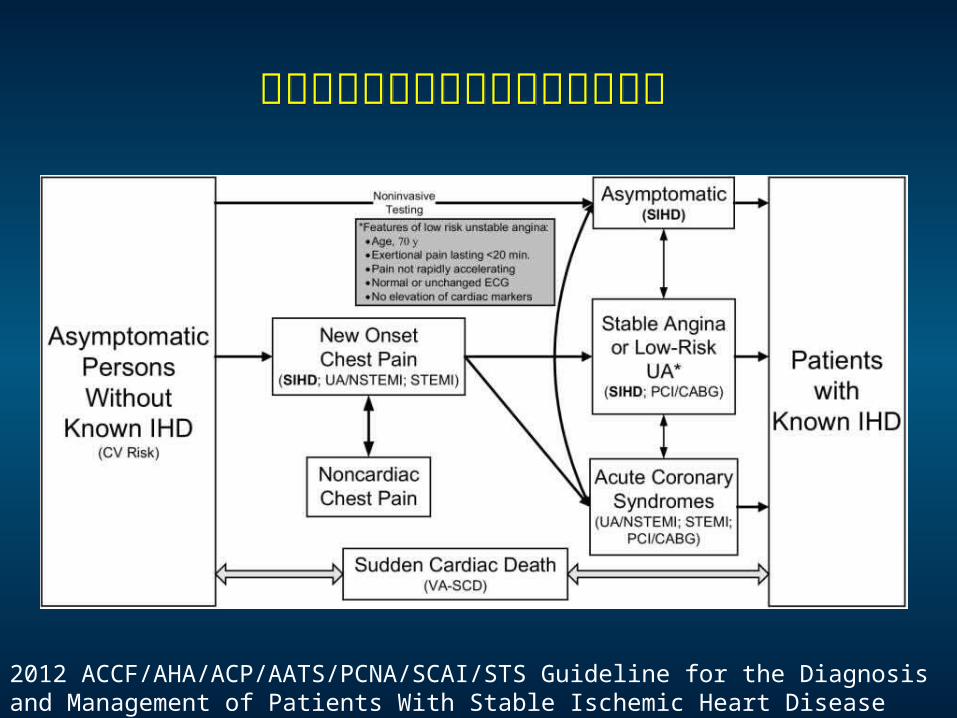
2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease
稳定型冠心病与其他型冠心病的关系稳定型冠心病与其他型冠心病的关系
稳定型冠心病的治疗目标稳定型冠心病的治疗目标
Relief of symptoms and ischemia;
Prevention of premature cardiovascular death;
Prevention of progression of coronary artery disease
leading to myocardial infarction, left ventricular
dysfunction, and congestive heart failure.
Lancet 2010; 375: 763–72
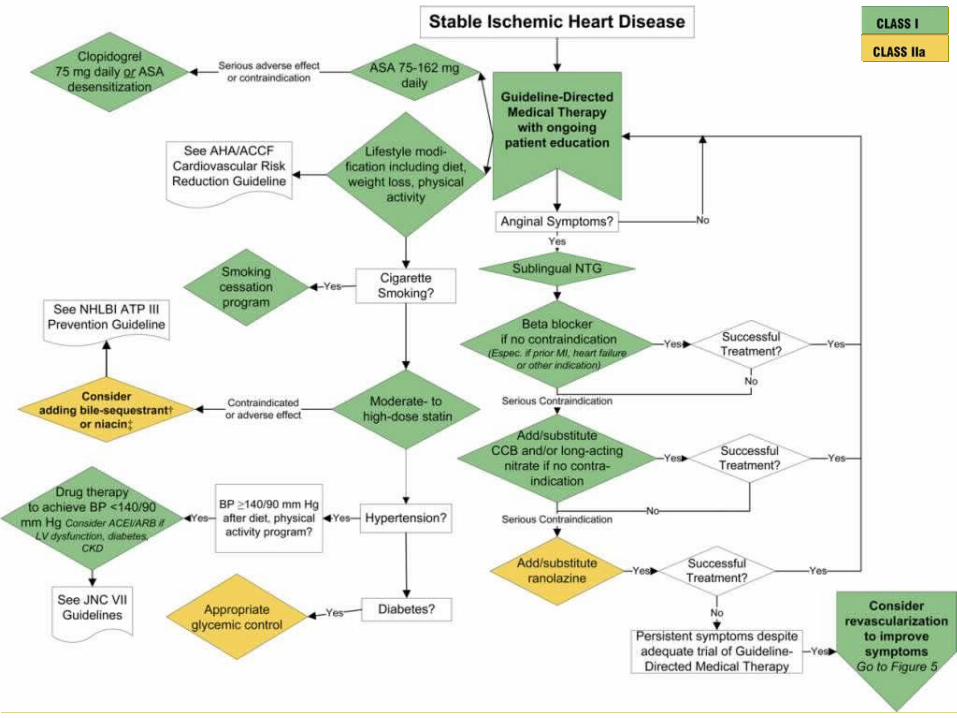
稳定型冠心病的治疗方案稳定型冠心病的治疗方案 生活方式改变 Exercise; weight reduction; smoking cessation; management of psychological factors
危险因素控制 Lipid, blood pressure, diabetes management
药物治疗 抗血小板 : aspirin, clopidogrel B 受体阻滞剂: RAS 抑制剂 : ACEI, ARB 他汀类 : 抗心绞痛治疗 : beta-blocker, CCB, nitrates, ranolazine,
nicorandil, ivabradine, trimetazidine
再血管化治疗2012 Guideline for the Diagnosis and Management of Patients With SIHD
稳定型冠心病再血管化指征稳定型冠心病再血管化指征稳定型冠心病再血管化指征稳定型冠心病再血管化指征 Patients with unacceptable angina
Patients deemed likely to have a survival benefit from revascularization, based upon the location and severity of the lesion, the number of diseased vessels, and the presence of left ventricular dysfunction
From UpToDATE; 中华心血管病杂志 2007 年 3 月第 35 期第 3 卷
中国慢性稳定性心绞痛诊断与治疗指南中国慢性稳定性心绞痛诊断与治疗指南 在药物治疗基础上进行血管重建应考虑以下情况:药物治疗不能成功控制症状使患者满意。无创检查提示较大面积心肌存在风险。手术成功率高,而相关的并发症和死亡率在可接受范围内。与药物治疗相比患者倾向于选择血管重建,并且已向患者充分告知治疗可能出现的相关风险。
对于稳定型冠心病,药物治疗基础上的
再血管化是否能改善预后?
对于稳定型冠心病,药物治疗基础上的
再血管化是否能改善预后?
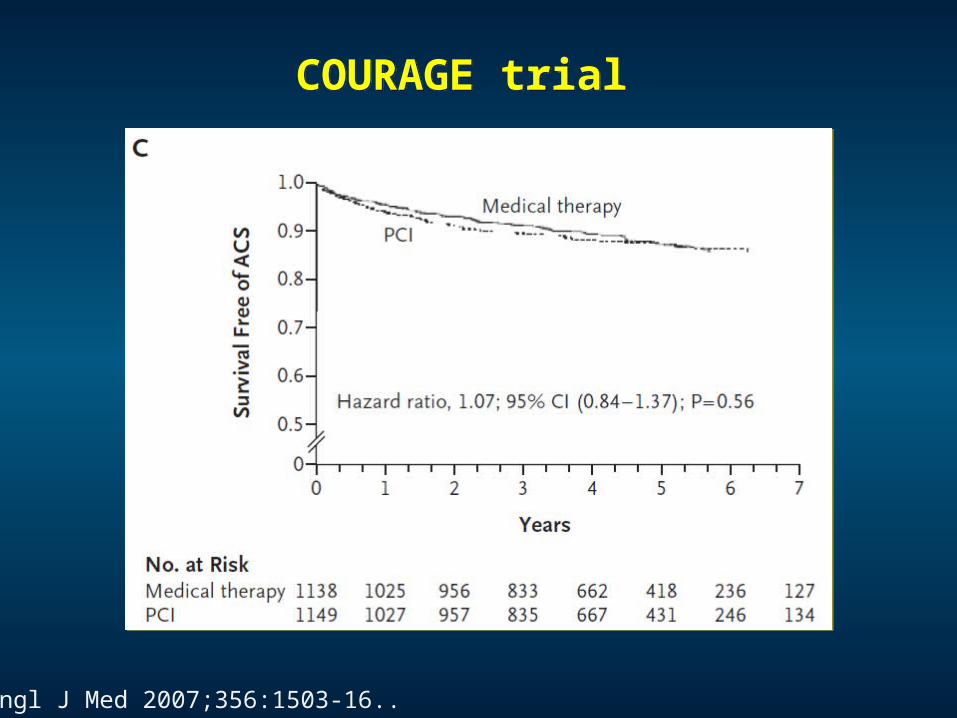
COURAGE trialCOURAGE trial
N Engl J Med 2007;356:1503-16..
在美国和加拿大的 50 个单位进行的多中心随机对照临床试验,从 1999 年 6月至 2004 年 1 月共入选 2 287 例稳定型心绞痛患者,随机分为 2 组。
COURAGE trialCOURAGE trial
药物治疗组患者接受包括运动、戒烟、饮食咨询和体重控制在内的治疗性生活方式改变,并按照现行指南给以单硝酸异山梨酯、长效美托洛尔、氨氯地平等抗心绞痛药物,阿司匹林或氯吡格雷抗血小板聚集,使用他汀类调脂药必要时加用依折麦布,争取使 LDL-C 控制在 1 . 56-2 . 21 mmol/L , LDL-C 达标后加用缓释烟酸制剂等,使 HDL-C>1 . 04 mmol/L 、 TG<1 . 70 mmol/L ,血压控制目标在 130/85 mm Hg) 以下,并给以二级预防药物赖诺普利或洛沙坦。
PCI 组患者除了上述治疗措施外,还进 PTCA/ 支架植入治疗,尽量做到完全性血运重建。该组有 46 例因患者拒绝或冠状动脉解剖原因未能进行介入治疗, 27 例患者介入治疗中未能跨越任何病变。对 1 077 例患者的 1 688 处病变进行了介入干预,其中 590 例植入 1 枚支架, 416 例植入至少 2 枚支架,这些病变有 1 576 处 (93 % ) 处理成功, 958 例患者 (89 % ) 获得临床成功。
N Engl J Med 2007;356:1503-16..
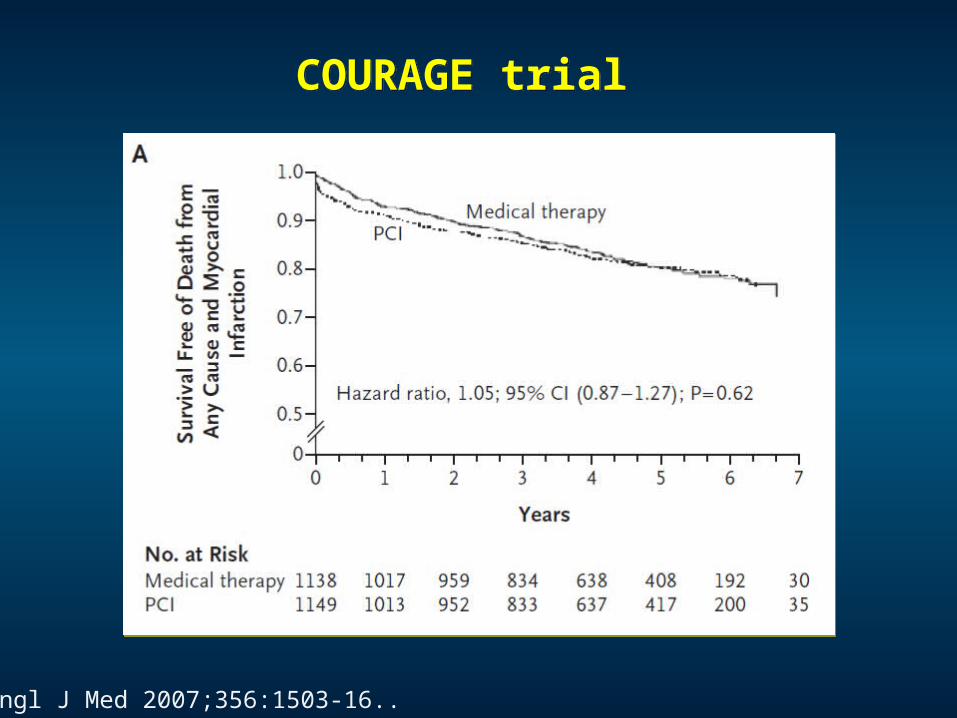
COURAGE trialCOURAGE trial
N Engl J Med 2007;356:1503-16..
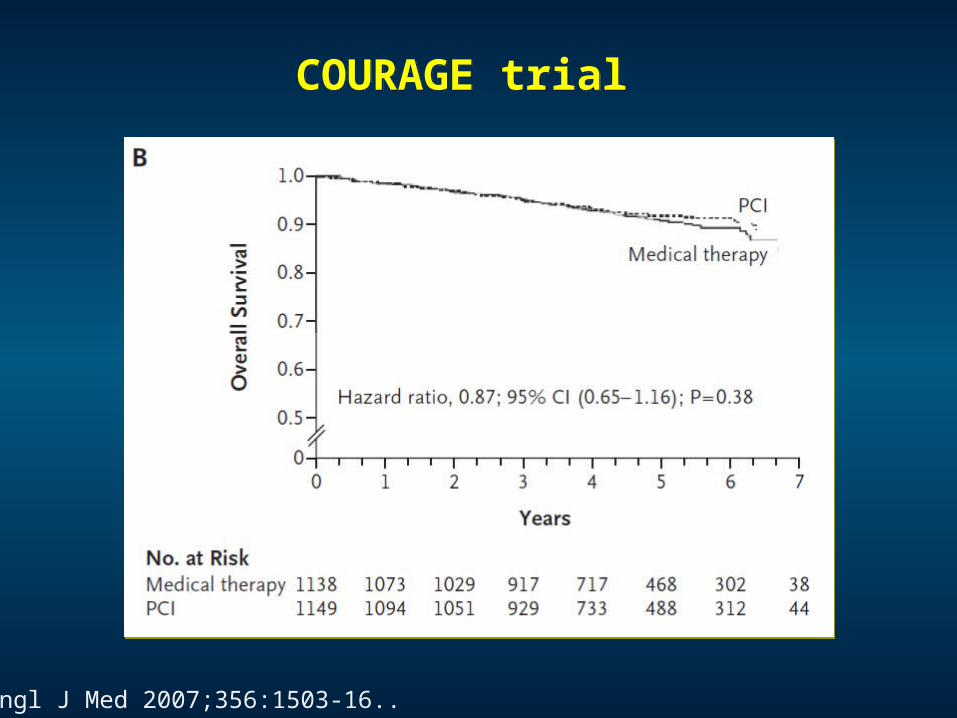
COURAGE trialCOURAGE trial
N Engl J Med 2007;356:1503-16..
COURAGE trialCOURAGE trial
N Engl J Med 2007;356:1503-16..
COURAGE 试验的入选患者中排除了严重心绞痛患者、负荷试验强阳性患者、心功能不全的患者、左室射血分( LVEF ) <30% 的患者,而这些患者恰好是更能从血运重建治疗中获益的人群。
COURAGE 试验中介入治疗组的病变处理成功率只有 93% ,临床成功率只有 89% ,不能反映现有的介入治疗水平。
COURAGE 试验中只有 31 例患者( 1.8% )置入 DES ,绝大数患者置入普通金属裸支架。事实上,药物洗脱支架可以明显降低心绞痛复发率,提高患者的生活质量,而这恰恰是众多患者寻求介入治疗的始动原因。
在 COURAGE 试验中,患者接受的药物治疗达到了很高的强度,动脉粥样硬化的危险因素得到很好的控制。然而,在临床实践中,我国绝大多数患者没能达到这强度,药物治疗效果必然比 COURAGE 试验中的患者差。
COURAGE 试验的局限性COURAGE 试验的局限性
COURAGE 试验后稳定型心绞痛的治疗策略思考 北京大学学报 ; 2007;39 (6)
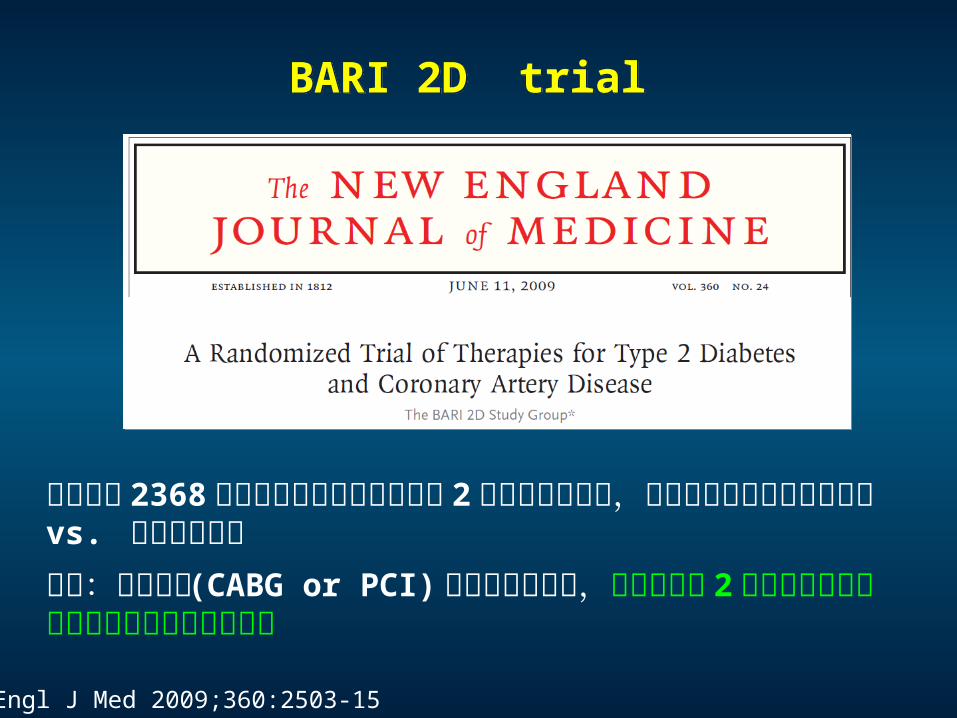
BARI 2D trialBARI 2D trial
N Engl J Med 2009;360:2503-15
研究纳入 2368 例有已证实稳定性冠心病和 2 型糖尿病的患者,随机分配接受快速血运重建 vs. 初始药物治疗结论:再血管化 (CABG or PCI) 与药物治疗相比,并不能降低 2 型糖尿病合并稳定型心脏病患者的死亡风险
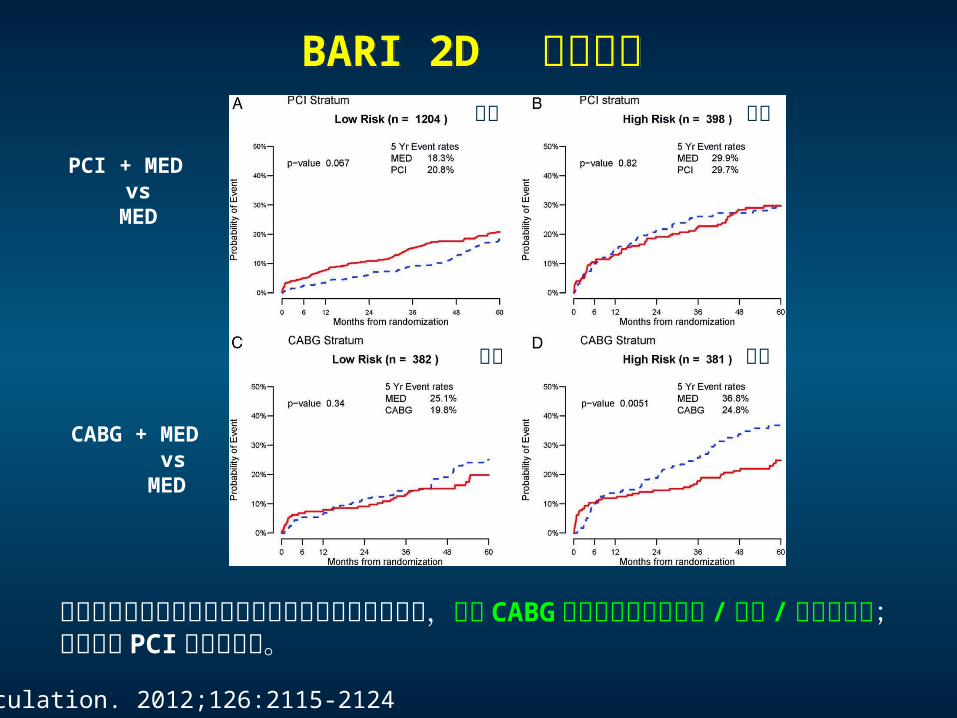
BARI 2D 亚组分析BARI 2D 亚组分析
Circulation. 2012;126:2115-2124
PCI + MED vs
MED
CABG + MED vs MED
在伴有广泛冠脉病变或左室功能受损的糖尿病患者中,即刻 CABG 策略可显著降低死亡 / 心梗 / 卒中发生率;但未发现 PCI 有类似益处。
低危 高危
低危 高危
Evidence from Meta-AnalysisEvidence from Meta-Analysis
PCI-based invasive strategy may improve long-term survival compared with a medicaltreatment-only strategy in patients with stable coronary artery disease.
PCI,as compared with OMT, did not reduce the risk of mortality, cardiovascular death, nonfatal myocardial infarction, or revascularization. PCI, however, provided a greater angina relief compared with OMT alone.
JACC 2008;52:894–904
Percutaneous coronary intervention was associated with greater freedom from angina compared with medical therapy,but this benefit was largely attenuated in contemporary studies.
Circ Cardiovasc Interv 2012;5;476-490
Ann Intern Med. 2010;152:370-379.
在稳定型冠心病中,冠脉支架植入 + 药物治疗是否优于单纯药物治疗?
研究共纳入 8 项研究, 7229 例病人 ,比较死亡、非致死性心梗、未计划的再血管化治疗,持续性心绞痛
Evidence from Meta-AnalysisEvidence from Meta-Analysis
Arch Intern Med. 2012;172(4):312-319
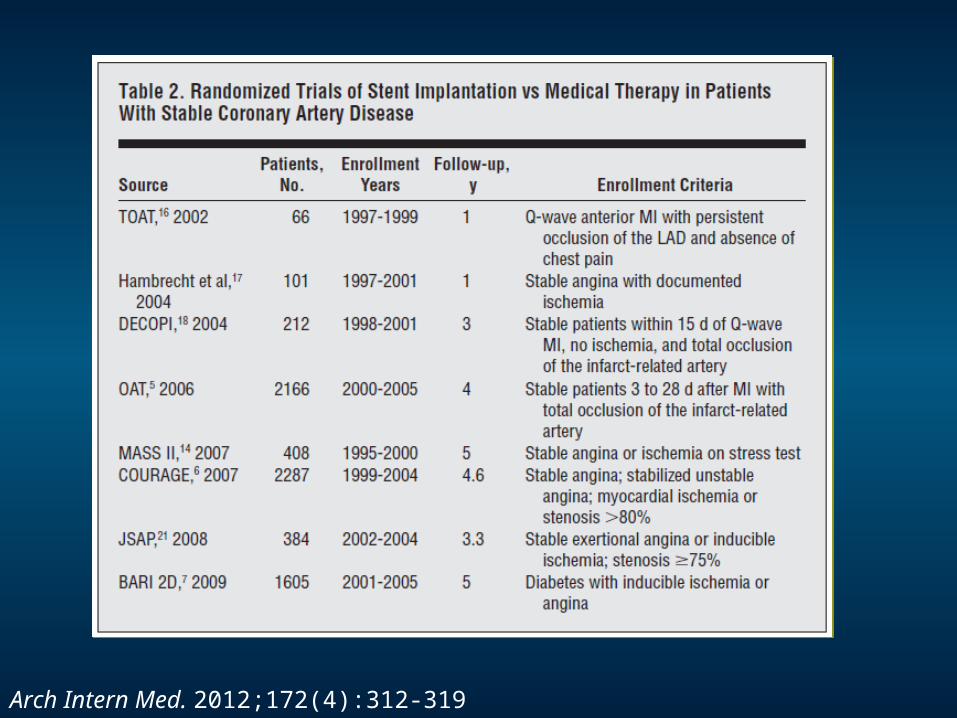
Arch Intern Med. 2012;172(4):312-319
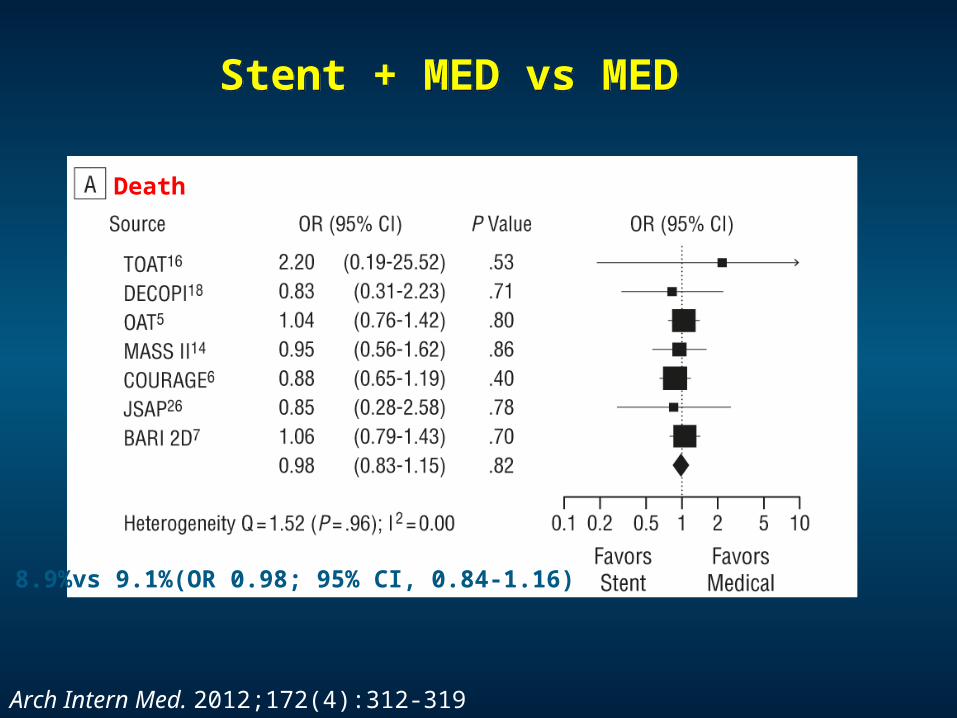
Stent + MED vs MED Stent + MED vs MED
Death
8.9%vs 9.1%(OR 0.98; 95% CI, 0.84-1.16)
Arch Intern Med. 2012;172(4):312-319
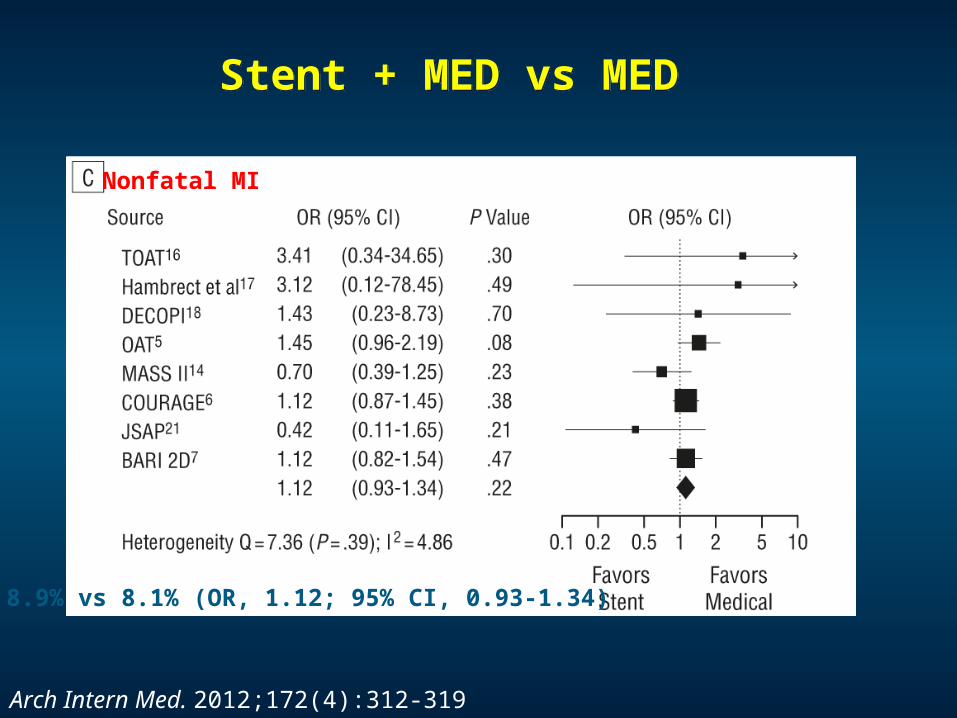
Nonfatal MI
8.9% vs 8.1% (OR, 1.12; 95% CI, 0.93-1.34)
Arch Intern Med. 2012;172(4):312-319
Stent + MED vs MED Stent + MED vs MED
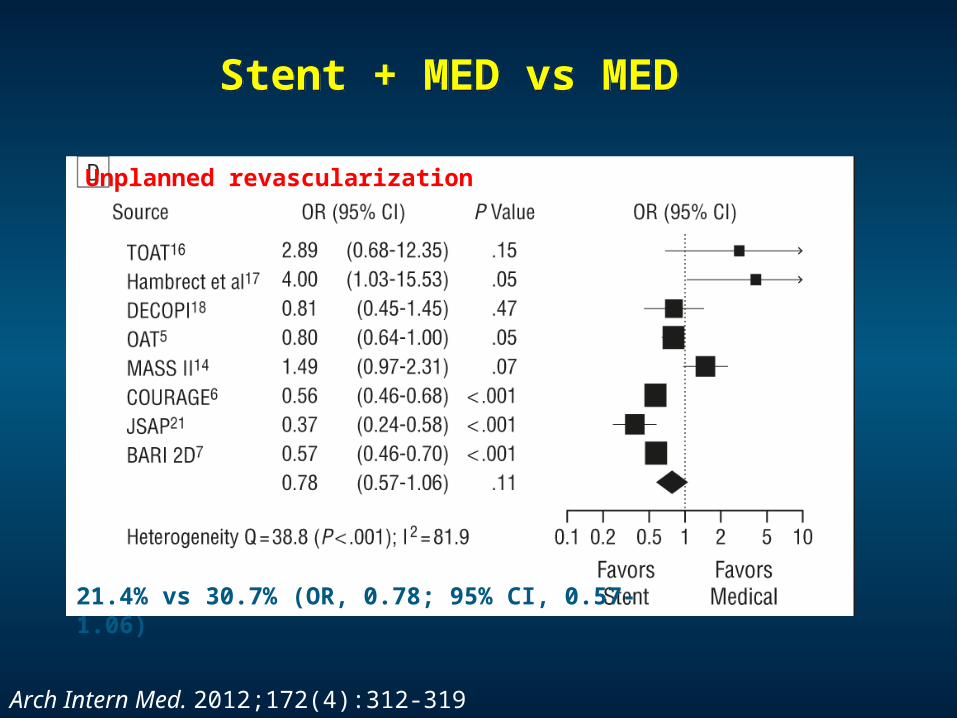
Unplanned revascularization
Arch Intern Med. 2012;172(4):312-319
21.4% vs 30.7% (OR, 0.78; 95% CI, 0.57-1.06)
Stent + MED vs MED Stent + MED vs MED
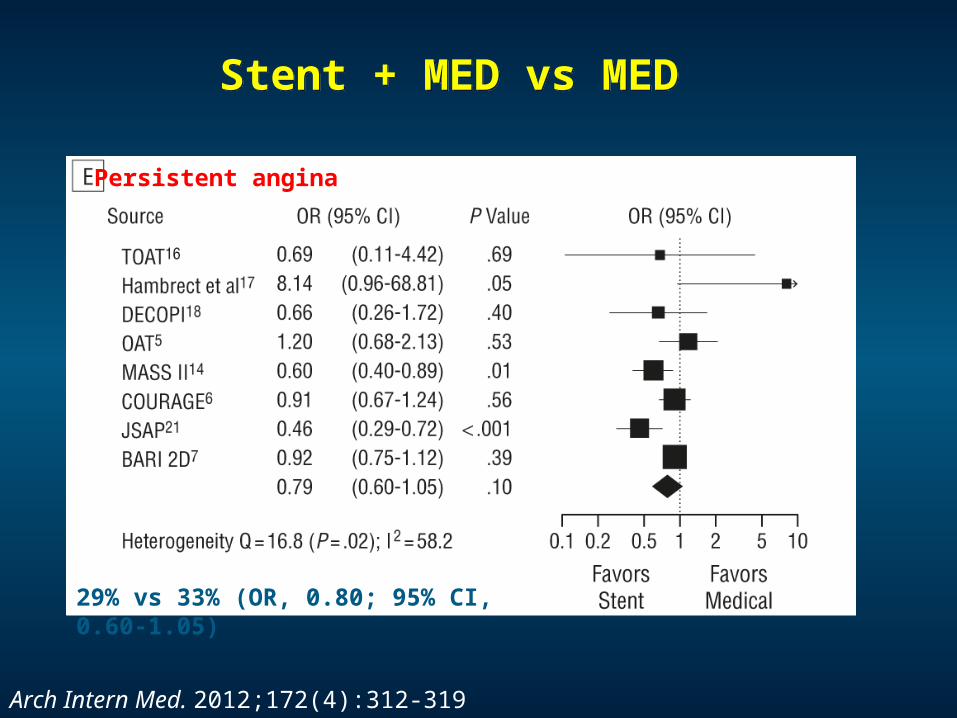
Persistent angina
Arch Intern Med. 2012;172(4):312-319
29% vs 33% (OR, 0.80; 95% CI, 0.60-1.05)
Stent + MED vs MED Stent + MED vs MED
Conclusion:
Initial stent implantation for stable CADshows no evidence of benefit compared with initial medical therapy for prevention of death, nonfatal MI, unplanned revascularization, or angina.
Arch Intern Med. 2012;172(4):312-319
Stent + MED vs MED Stent + MED vs MED
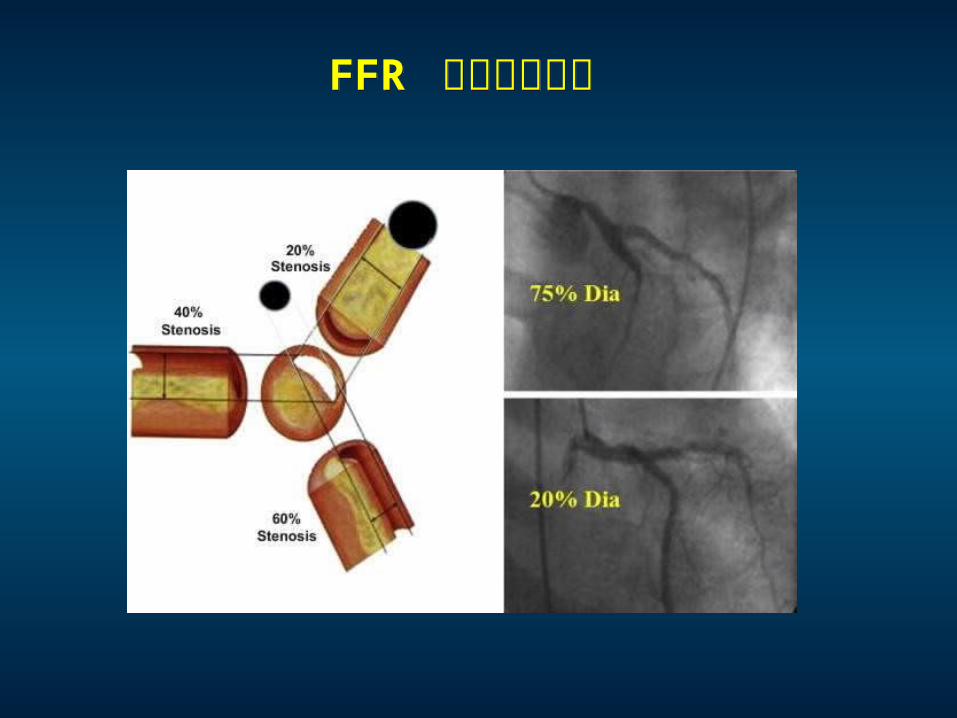
FFR 指导支架植入FFR 指导支架植入
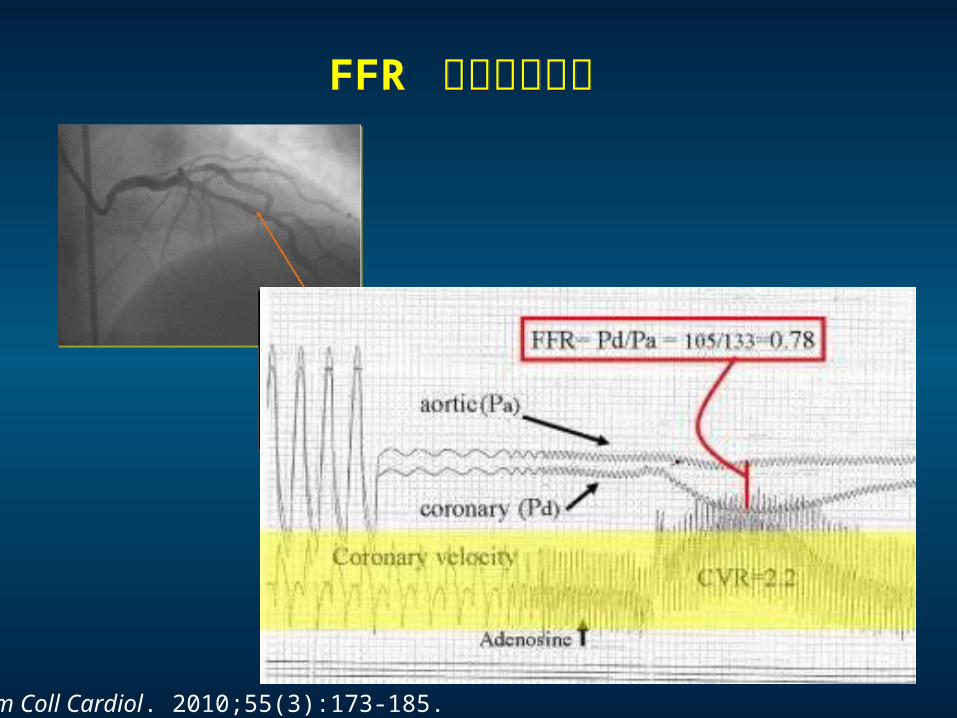
FFR 指导支架植入FFR 指导支架植入
J Am Coll Cardiol. 2010;55(3):173-185.
FAME II Trial FAME II Trial
N Engl J Med 2012;367:991-1001..
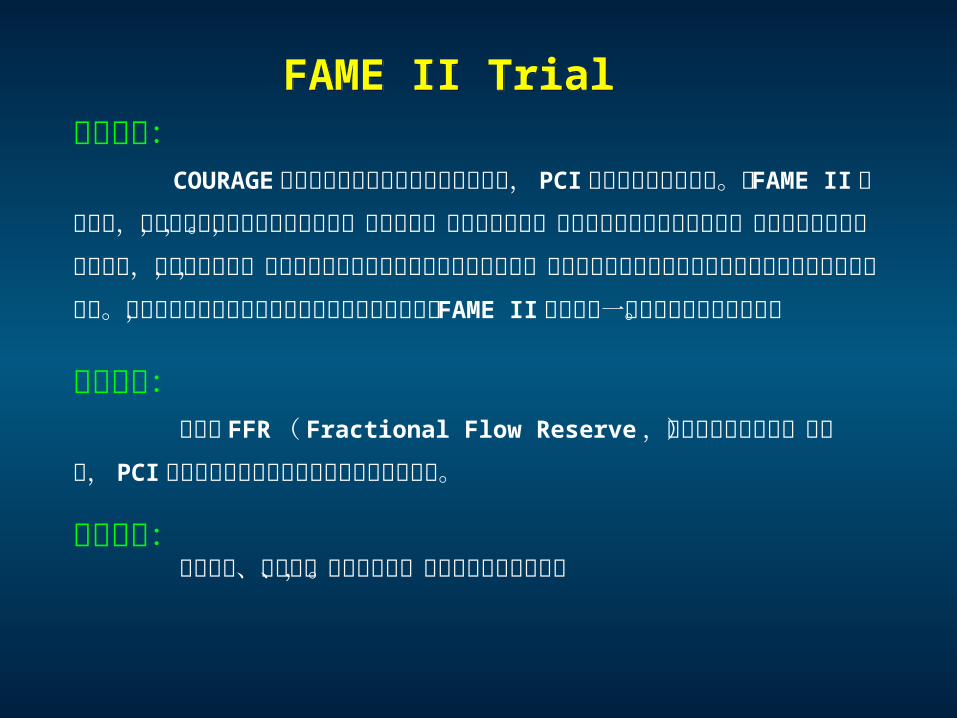
研究背景: COURAGE 研究结果证明对于稳定性冠心病患者, PCI 未能取得更好的疗效。同 FAME II 研究类似,该研究也是对患者进行介入治疗,球囊扩张,最终置入支架。但是由于时代和技术的限制,当时研究中使用的是裸支架,在这种情况下,研究对比结果说明药物治疗优于介入治疗,因此有结论说在稳定性冠心病患者中实施介入治疗不合理。那么稳定性冠心病患者是不是应当进行介入治疗, FAME II 研究为这一话题提供了良好的答案。
研究目的: 讨论在 FFR ( Fractional Flow Reserve ,冠脉血流储备分数)指导下,PCI 对比药物治疗在稳定性冠心病患者中的治疗。
研究性质: 前瞻性的、随机的、有对照组的,国际多中心临床试验。
FAME II Trial FAME II Trial
研究设计:
纳入适合接受 PCI 的稳定型冠状动脉疾病患者及血管造影证实单支、双支或三支冠状动脉病变且适合接受 PCI 的患者,原计划纳入 1,832 例患者,实际共纳入 1,220 例,其中 888 例具有至少 1 处 FFR≤0.80 的狭窄病变:447 例被随机分入 FFR 指导的 PCI+ 最佳药物治疗组, 441 例被分入单纯最佳药物治疗组。 332 例血管造影证实具有明显狭窄病变但狭窄病变 FFR均≥ 0.80 的患者被纳入注册研究,接受单纯最佳药物治疗。平均随访时间为212天。 对所有患者给予阿司匹林 80~325 mg qd 、美托洛尔 50 ~200 mg qd
( 或任何其他 β 受体阻滞剂 ) 、赖诺普利 (至少 5 mg qd ,或其他 ACEI 或
ARB) 和阿托伐他汀 (20~80 mg ,或其他 statins) 。使用第二代 DES 治疗所有 PCI 患者。
FAME II Trial FAME II Trial
N Engl J Med 2012;367:991-1001..
研究终点:
研究的终点是主要心脏不良事件,包括各种原因导致的死亡,记录在案
的心肌梗死,以及紧急血运重建导致的再次入院等。 随访时间包括 1个月、 6个月、 1年、 2年、 3年、 4年和 5年。
FAME II Trial FAME II Trial
FAME II 试验在试验开始后 2012 年 1月提前结束 ! 主要原因是在随机研究组中,实施 PCI联合 MT 的患者,恢复效果明显优于单纯药物治疗组,出于人道主义和医学伦理的考虑,试验提前结束。
N Engl J Med 2012;367:991-1001..
FAME II Trial FAME II Trial
N Engl J Med 2012;367:991-1001..
FAME II Trial FAME II Trial
N Engl J Med 2012;367:991-1001..
FAME II Trial FAME II Trial
N Engl J Med 2012;367:991-1001..
FAME II Trial FAME II Trial
N Engl J Med 2012;367:991-1001..
FAME II Trial FAME II Trial
Limitations of FAME II Trial Limitations of FAME II Trial
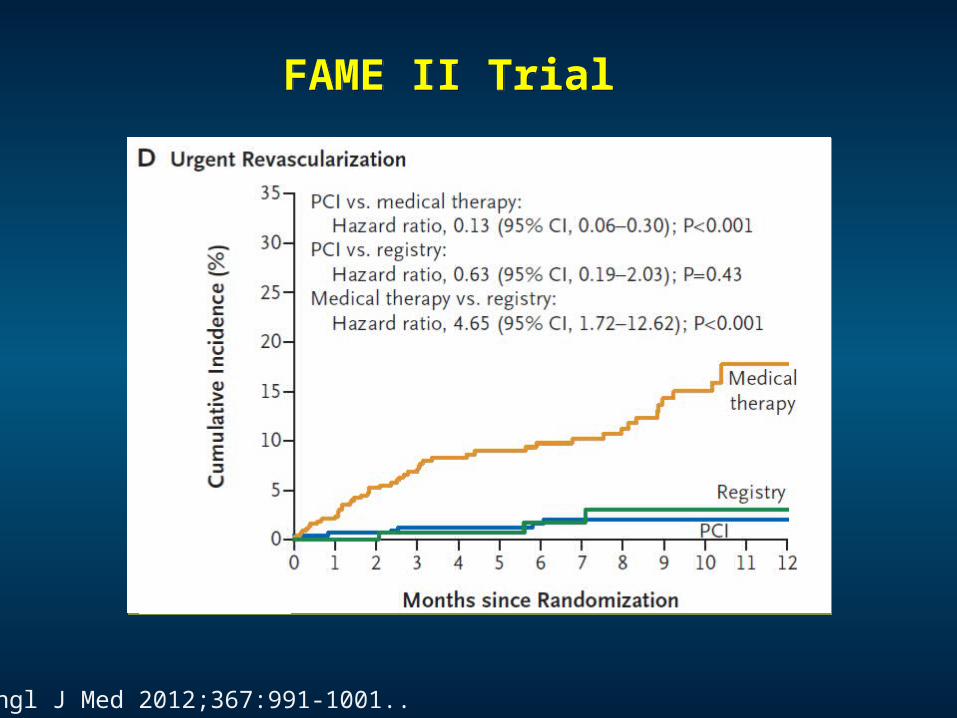
Terminated at a mean follow-up of 7 months because of a highly significant treatment difference - a finding driven solely by a difference in the end point of urgent revascularization (medical-therapy group vs. PCI group; hazard ratio with PCI, 0.13; 95% CI, 0.06 to 0.30; P<0.001).
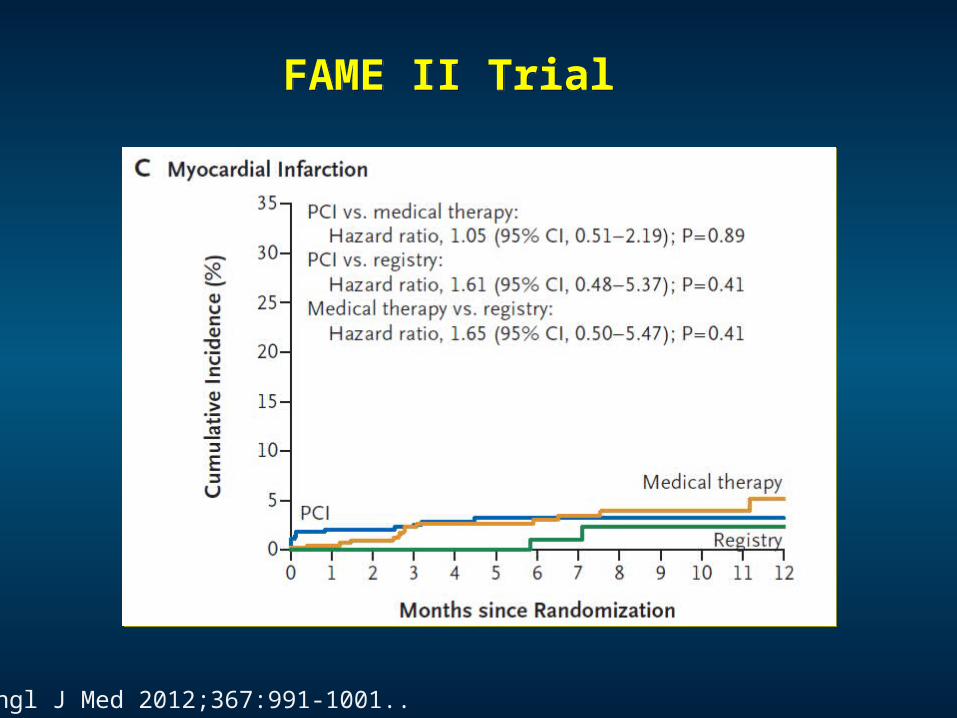
There were very few “hard” events overall, with only four deaths (three in the medical-therapy group and one in the PCI group) and 29 myocardial infarctions (14 in the medical-therapy group and 15 in the PCI group).
Neutral effects on the rate of death or myocardial infarction, and the lack of a significant, sustained treatment effect on the reduction of angina beyond 6 months are not seen.
N Engl J Med 2012;367:1059-1061.
Purpose
To determine the best management strategy for higher-risk patients with stable ischemic heart disease.
This is a multicenter randomized controlled trial with a target enrollment of ~8000 patients with at least moderate ischemia on stress imaging.
Patients will be assigned at random to a routine invasive strategy with cardiac catheterization followed by revascularization plus optimal medical therapy (OMT) or to a conservative strategy of OMT, with cath and revascularization reserved for those with an acute coronary syndrome, ischemic heart failure, resuscitated cardiac arrest or refractory symptoms.
The ongoing ISCHEMIA trialThe ongoing ISCHEMIA trial
ISCHEMIA Trial; ClinicalTrials.gov number, NCT 01471522
稳定型冠心病再血管化治策略的选择:
PCI or CABG ?
稳定型冠心病再血管化治策略的选择:
PCI or CABG ?

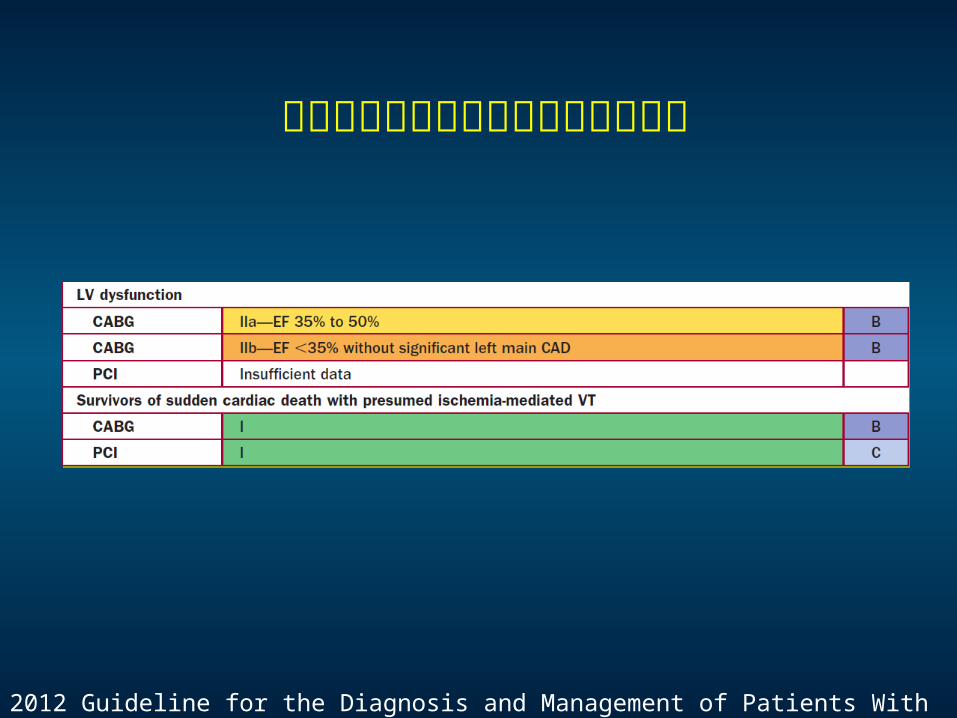
合并左室功能减退或缺血引起的室速
2012 Guideline for the Diagnosis and Management of Patients With SIHD
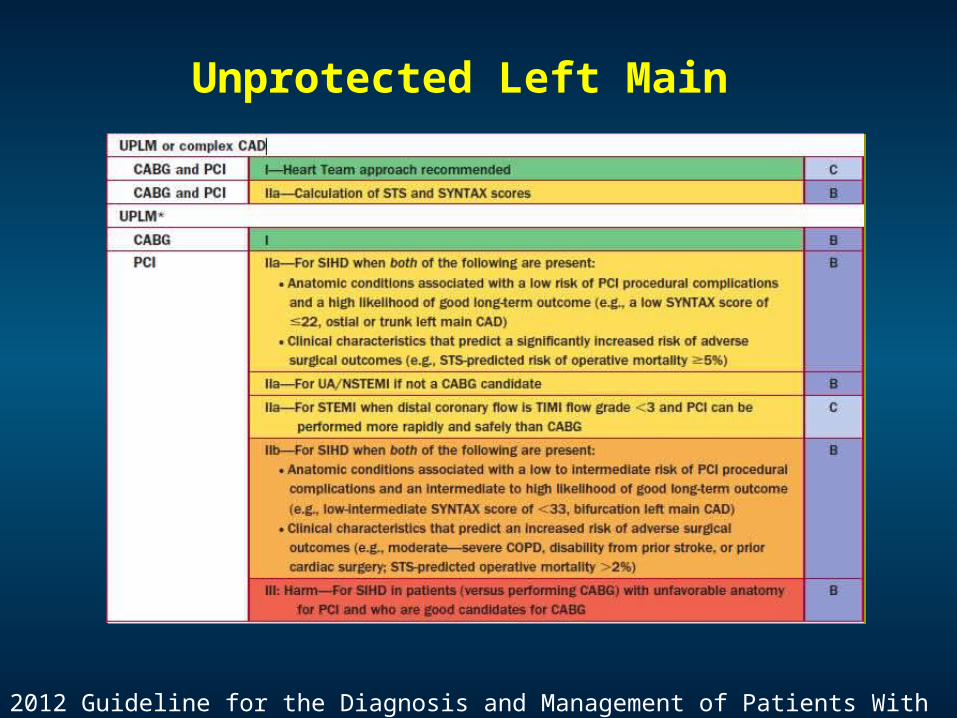
Unprotected Left Main
2012 Guideline for the Diagnosis and Management of Patients With SIHD
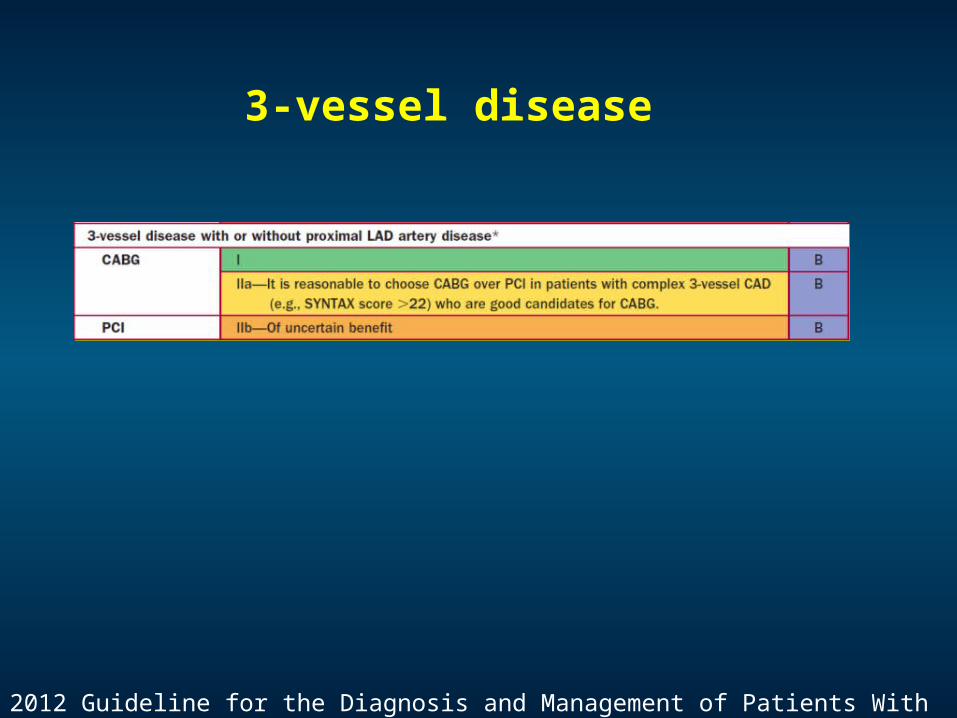
3-vessel disease
2012 Guideline for the Diagnosis and Management of Patients With SIHD
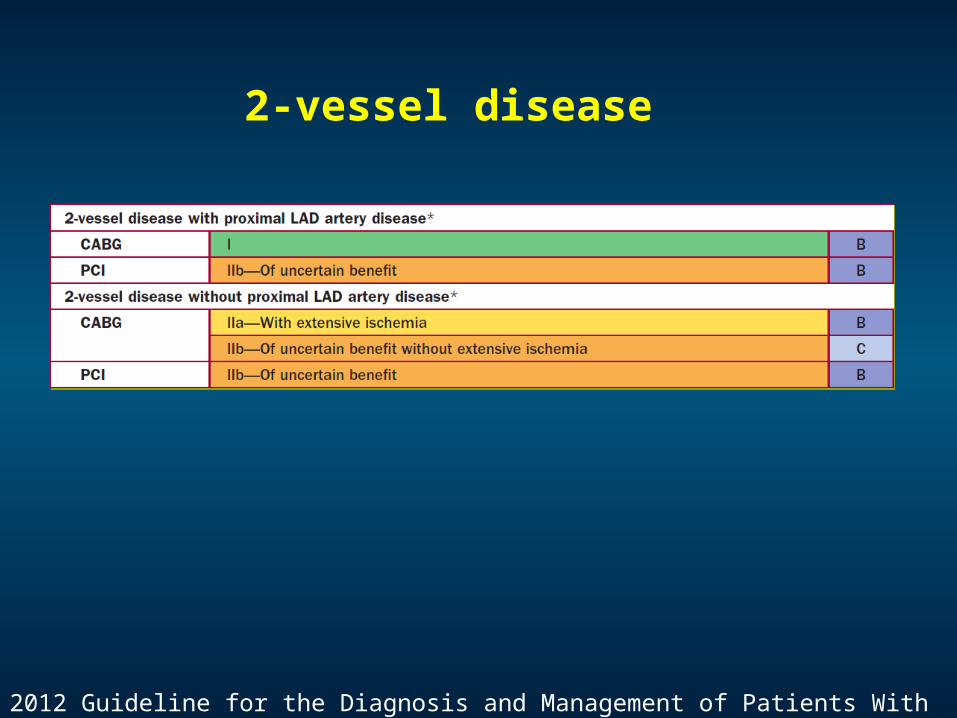
2-vessel disease
2012 Guideline for the Diagnosis and Management of Patients With SIHD
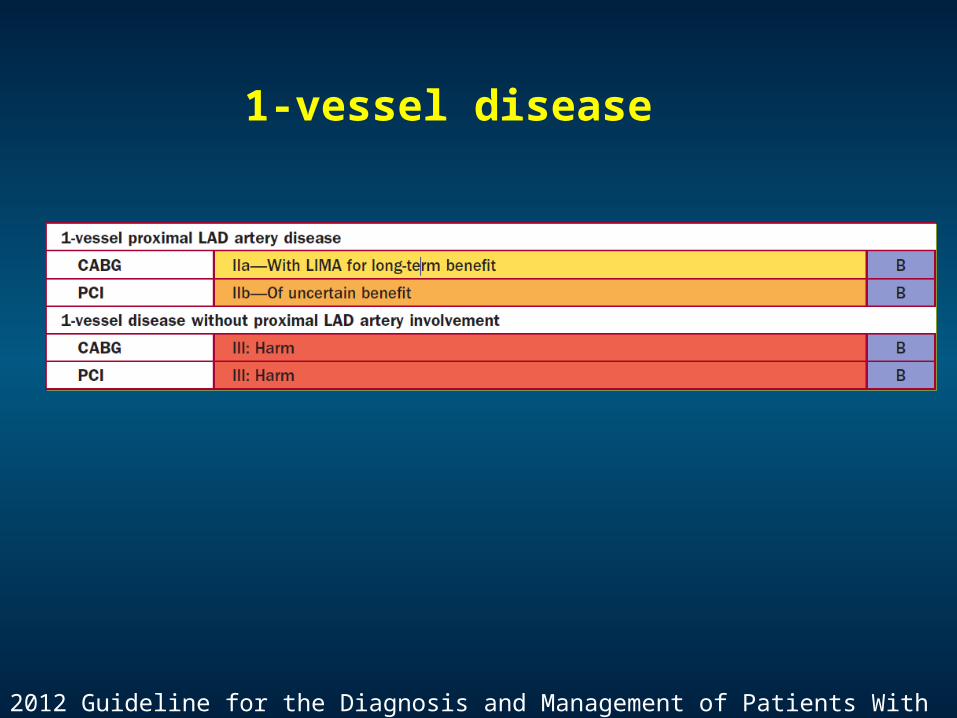
1-vessel disease
2012 Guideline for the Diagnosis and Management of Patients With SIHD
SummarySummary
稳定型冠心病的治疗目标和基本治疗策略稳定型冠心病的治疗目标和基本治疗策略
稳定型冠心病再血管化对预后的改善
稳定型冠心病中 FFR 指导支架植入
稳定型冠心病再血管化治策略的选择