-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
1/15
Infectious
MyelopathiesJoseph R. Berger, MD, FACP, FAAN
ABSTRACT
Every genus of microorganism, as well as prions, has been
associated with disease ofthe spinal cord. The spectrum of
pathogens resulting in myelopathy varies with thepopulation.
Myelopathy is uniquely associated with certain retroviruses,
particularlyHIV type 1 and human T-cell lymphotropic virus type I,
but the myelopathies that occurwith these viruses are chiefly
limited to at risk populations. In the immunocompro-mised
population, a diverse array of pathogens may cause spinal cord
disease,especially viruses from the Herpesviridae family, most
notably cytomegalovirus andvaricella-zoster virus. The prototypical
myelopathy resulting from bacterial infection istabes dorsalis, but
this disorder is vanishingly rare in the modern era. In
developingcountries, Mycobacterium tuberculosis and schistosomiasis
remain significant causesof myelopathy.
Continuum Lifelong Learning Neurol 2011;17(4):761775.
INTRODUCTION
Myelopathies consequent to an infectiousorganism are extremely
diverse in their
presentations. They vary with respectto the populations most
commonly af-fected, the clinical manifestations, theassociated
disorders, and radiographicand laboratory features. An
extensivediscussion of each of the infectiousmyelopathies is beyond
the scope of thisreview, but the salient infectious myelo-pathies
will be addressed by etiology.
Infectious myelopathies present invariegated manners. Those that
are theconsequence of retroviruses, such asHIV, human T-cell
lymphotropic virustype I (HTLV-I), and syphilis, typicallypresent
in a subacutely or chronicallyprogressive manner. Associated
riskfactors for the acquisition of these infec-tions often help the
clinician recognizethem. Other infectious myelopathiestypically
present as acute illnesses, oftenexhibit discrete sensory levels,
and may
be associated with systemic features ofinfection. Fever and
spinal percussion
tenderness are often observed in pa-tients with epidural
abscesses. However,
the most important element to estab-
lishing the correct diagnosis is maintain-ing a high index of
suspicion.
VIRAL MYELOPATHIES
A large number of viruses may causemyelitis (Table 3-1). Acute
viral myelitismay present as an acute flaccid paralysis
(poliomyelitis) or as a disorder in whichlong tract involvement
due to whitematter disease predominates.1 The viralinfections1 that
typically present as anacute flaccid paralysis include
poliovirustypes 1, 2, and 3; Coxsackievirus types Aand B;
Enterovirus 71, and the Flavivi-ruses, which include West Nile
virus.2
Retroviral infection with HIV and HTLVare examples of viruses
that may result ina slowly progressive myelopathy in which
white matter disease predominates.
HIV Type 1
Neurologic disease is common in thesetting of HIV/AIDS. Ten
percent to 20%
Address correspondenceto Dr Joseph R. Berger,740 S
Limestone,Neurology DepartmentKentucky Clinic L-445,Lexington, KY
40536,[email protected].
Relationship Disclosure:Dr Berger has receivedpersonal
compensation forspeaking engagements orconsulting activities
with
Asphelia Pharmaceuticals,Inc., Astellas Pharma US,Inc., Bayer,
EMD Serono,Inc., GlaxoSmithKline,Merck Serono,
MillenniumPharmaceuticals, Inc.,Pfizer Inc., and TevaNeuroscience.
Dr Bergerreceives research support
from Biogen Idec andEMD Serono, Inc.
Unlabeled Use ofProducts/InvestigationalUse Disclosure:Dr Berger
reports nodisclosure.
Copyright* 2011,American Academy ofNeurology. All
rightsreserved.
Review Article
761Continuum Lifelong Learning Neurol 2011;17(4):761775
www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
2/15
of individuals infected with HIV haveneurologic disorders herald
their infec-tion, and ultimately more than halfdevelop some
neurologic complication.
While spinal cord disease occurring in
association with AIDS has been infre-
quently observed in retrospective clinicalseries, autopsy series
predating the an-tiretroviral therapy era indicate that11%3 to 22%4
have pathologic featuresof a unique spinal cord disorder first
de-
scribed by Petito and colleagues.4 The
TABLE 3-1 Viral Etiologies of Myelitis
DNA RNAEnveloped Herpesviruses Togaviruses
Herpes simplex virus,types 1 and 2
Rubella virus
Varicella-zoster virusRetroviruses
Epstein-Barr virusHIV type 1
CytomegalovirusHuman T-cell lymphotropicvirus type I
Herpes simiae (B virus) Orthomyxoviruses
Poxviruses Influenza virus
Vaccinia virus Paramyxoviruses
Variola virus Measles virus
Mumps virus
Bunyaviruses
California virus
Arenaviruses
Lymphocyticchoriomeningitis virus
Rhabdoviruses
Rabies virus
Flaviviruses
West Nile virus
Tickborne encephalitis virus
Nonenveloped H epatitis B virus Picornaviruses
Coxsackievirus
Hepatitis A virus
Encephalomyocarditis virus
Echoviruses
Poliovirus types 1, 2, and 3
Other Enteroviruses
Adapted from Tyler KL, Gross RA, Cascino GD. Unusual viral
causes of transverse myelitis: hepatitis A virus and
cytomegalovirus. Neurology 1986;36(6):855Y888. Copyright B1986,
AAN Enterprises, Inc. All rights reserved.
Infectious Myelopathies
762 www.aan.com/continuum August 2011
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
3/15
discord between clinical and patho-logic series suggests that
this mye-lopathy is common but clinically un-
derrecognized. Although the clinicalpresentation of
HIV-associated vacuo-lar myelopathy (Case 3-1) may overlap
with that of other myelopathies asso-ciated with HIV-1 infection
(Table 3-2),the pathologic appearance is quitedistinct. Clinically,
these patients fre-quently report initial paresthesia and
vague discomfort in their legs followedby leg weakness,
imbalance, and gaitimpairment. In more than one-half of
patients, incontinence of bladder andbowel supervenes. Typically
this myel-
opathy is seen late in the course ofHIV-1 infection. It has been
described,however, as the presenting manifesta-
tion of this viral infection.6,7 Physicalexamination reveals a
spastic parapare-sis in which spasticity is more prom-inent than
the degree of weakness.The involvement is typically, but notalways,
symmetric. Gait ataxia andlower extremity dysmetria and dyssy-nergy
are seen. Although upper ex-tremity strength may be
unaffectedinitially, pathologically brisk reflexes inboth upper and
lower limbs are antici-
pated, unless, as is commonly the case,a superimposed peripheral
neuropathy
KEY POINTS
h HIV-associated
myelopathy is
underrecognized.
h The diagnosis of
HIV-associated
myelopathy is one
of exclusion.
Case 3-1A 47-year-old man with known HIV infection of 12 years
duration noteddifficulty ascending stairs in his home. He described
a sense of increasingleg stiffness and in the following months
developed a feeling that hislegs wanted to scissor when he walked.
He was plagued by urinaryfrequency and described a sense of
numbness in both feet. Ten monthsafter the onset of his initial
symptoms, he began using a cane toambulate. He denied any problems
with his upper extremities.Examination and self-assessment
demonstrated slowing of cognition, but
this did not markedly impede his activities of daily living. He
had noLhermitte sign on neck flexion and no spinal percussion
tenderness.Strength and tone were normal in the upper extremities.
He hadspasticity in both lower extremities with easily elicitable
clonus at theankles, but lower extremity strength was normal. His
gait was slow,stiff legged, and wide based. He was unable to
tandem. Reflexes werebrisk in the upper extremities with
bilaterally positive Hoffmann signs 3+at the knees and trace at the
ankles with bilaterally positive Babinskisigns. He could not
perceive a briskly struck tuning fork at the toes andexhibited a
positive Romberg sign. Pinprick and temperature sensewere impaired
to the midcalves. He had no sensory level to pinprickover his
trunk.
A cranial MRI showed brain atrophy and multiple hyperintense
signalabnormalities on T2-weighted imaging and FLAIR in deep white
matter.Cervical and thoracic MRIs were normal. CSF analysis was
normal. EMGand nerve conduction studies were compatible with a
sensorimotorneuropathy. Laboratory studies were unrevealing,
including vitamin B12level and homocysteine and methylmalonic acid
levels. His CD4 count was230 cells/mm3, and his viral load was
undetectable.
Comment. This man exhibits the cardinal features of
HIV-associatedvacuolar myelopathy, namely a slowly progressive
myelopathypredominantly involving the corticospinal tracts. As is
commonly observed,he has other HIV-related neurologic problems,
including cognitive deficitsand peripheral neuropathy.
763Continuum Lifelong Learning Neurol 2011;17(4):761775
www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
4/15
is present. Extensor plantar responsesand other features of
upper motorneuron disease are observed. Sensory
examination reveals that vibratory andposition sense are
disproportionatelyaffected in comparison to other sen-sory
modalities. A sensory level over thetrunk should suggest an
alternativediagnosis. Electrophysiologic studiesmay reveal a
prolonged latency of cor-tical evoked responses following
tibialnerve stimulation.
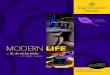
The striking pathologic findings ofHIV-associated myelopathy are
loss of
myelin and microvacuolization due tointramyelin swelling that is
accompaniedby lipid-laden macrophages. Axons arepreserved except in
areas of marked
vacuolization (Figure 3-1), and althoughmicroglial nodules may
be detected inthe spinal cord gray matter, inflamma-
tion and intranuclear viral inclusions arenot generally
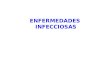
observed. The abnormal-ities predominate in the middle andlower
thoracic cord, but the cervicalcord may be similarly affected. The
lat-
eral and posterior columns are typicallyinvolved to a greater
extent than theanterior columns (Figure 3-2). The pa-thology bears
a strong resemblance tothat of subacute combined degenera-tion of
the spinal cord.4 The patho-genesis of HIV-associated
myelopathy
remains uncertain. A similar clinicopa-thologic condition has
been observedin patients with cancer or other immuno-suppressive
conditions in the absenceof HIV infection.8
The diagnosis of HIV-associated mye-
lopathy remains one of exclusion becausemyelopathy in HIV
infection has beenassociated with many other etiologies(Table 3-1).
Among the myelopathiesthat have been observed is an acutemyelitis
occurring at the time of HIVseroconversion.9 Whether this is
theconsequence of HIV infection of thecord or an autoimmune
disorder trig-gered by the infection remains uncertain.
KEY POINT
h HIV-associated
myelopathy is often
accompanied by HIV
dementia and
HIV-associated
peripheral
neuropathy.
TABLE 3-2 Myelopathies
Associated WithHIV Infection
b Infectious Etiologies
Viral
Primary HIV infection
Acute transient myelopathyoccurring at the time
ofseroconversion
Chronic progressivemyelopathy (HIV-associated
vacuolar myelopathy)Human T-cell lymphotropicvirus type I
Cytomegalovirus
Herpes simplex virus
Herpes zoster virus
Bacterial
Epidural abscess
Mycobacterium tuberculosis
Treponema pallidum
Cryptococcus neoformans
Others
Parasitic
Toxoplasma gondii
b Noninfectious Etiologies
Multiple sclerosisYlike illness
Tumors5
Plasmacytoma
Spinal cord astrocytomas
Others
Epidural hemorrhage secondaryto thrombocytopenia
Vascular injury secondary tovasculitis
Adapted from Berger JR. Medical myelopathies. In:
Herkowitz HN, Garfin SR, Eismont FJ, et al, editors.
Rothman Simeone: the spine. 5th ed. Philadelphia:
Saunders, 2006:795Y813. Copyright B2006, with
permission from Elsevier.
Infectious Myelopathies
764 www.aan.com/continuum August 2011
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
5/15
Typically, MRI of the spinal cord isunremarkable, but on rare
occasionshyperintense signal abnormalities onT2-weighted imaging
may be observedin the affected posterior and lateral
columns.10,11 This finding is helpful inexcluding other
potential etiologiessuch as lymphoma, abscess, or
epidurallipomatosis. Myelography seldom addsto the diagnostic
evaluation. CSF analy-
sis is important to rule out other po-tential pathogens and
should includeroutine bacterial and fungal cultures andcryptococcal
antigen as well as studiesfor cytomegalovirus (CMV), herpes
sim-plex virus (HSV) type 1 and 2, and
varicella-zoster virus (VZV), among otherpathogens. No
established therapy forHIV-associated myelopathy exists;
anti-retroviral therapy does not affect thenatural history of the
disorder.12 Thedisorder typically plateaus eventually.
Human T-cell LymphotropicVirus Type I
HTLV-I remains relatively rare in theUnited States; a study of
volunteer blooddonors by the American Red Cross re-
vealed a seropositivity rate of 0.025%.13
However, its seroprevalence rate amongparenteral drug abusers
and commercialsex workers is 25% in some communi-ties.14
Transmission of HTLV-I by blood
transfusion associated with myelopathyis well confirmed. The
myelopathy thatoccurs with HTLV-I has been referred toas tropical
spastic paraparesis (TSP) orHTLV-IYassociated myelopathy
(HAM).Clinically, the disorder is typically aslowly progressive
myelopathy develop-ing over years with symptoms of spasticlower
extremity weakness and a spasticbladder predominating. Sensory
abnor-
malities including paresthesia, pain, andnumbness may also be
observed. Amore rapid course, with progression tothe patient
becoming wheelchair de-pendent occurring over weeks tomonths, has
been reported in as many
FIGURE 3-1 Microvacuolization of the posterior columnsof the
spinal cord in HIV-associatedvacuolar myelopathy.
FIGURE 3-2 Demyelination in posterior, lateral, andanterior
columns of the spinal cord inHIV-associated vacuolar
myelopathy.
765Continuum Lifelong Learning Neurol 2011;17(4):761775
www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
6/15
as 8% of cases15 and appears to be morecommon in those infected
by bloodtransfusion.16 It is estimated that one in
250 individuals infected with HTLV-I willdevelop HAM/TSP.17 The
major patho-logic feature is chronic inflammation ofthe spinal cord
characterized by peri-
vascular inflammation, macrophage in-filtration, and
astrogliosis coupled withlong tract degeneration and demyeli-nation
chiefly affecting the pyramidal,spinocerebellar, and
spinothalamictracts extending from the upper cervicalcord to the
lumbar regions.18 Various
therapeutic modalities have been used,including immunomodulatory
and anti-viral strategies, but no ideal therapy hasbeen identified
yet.19 As with HIV-1 in-fection, a peripheral neuropathy may
beassociated with this infection.
HTLV-II, a related type C retrovirus,may rarely result in a
myelopathy similarto HAM/TSP.20 The epidemiology of this
virus is somewhat different than that ofHTLV-I because the
populations princi-pally affected are American Indians and
parenteral drug abusers; nonetheless, itsmode of transmission
parallels that ofHTLV-I and HIV.
Herpesviruses
Immunosuppression frequently predis-poses patients to the
development ofmyelopathy resulting from herpesvi-ruses. After
initial infection, the VZVremains latent within the dorsal
rootganglia. Following reactivation, it spreadscentrifugally along
the correspondingnerves resulting in a severely painful,blistering
dermatomal eruption referredto as shingles. On rare occasions
whenthe thoracic dermatomes are involved,the virus may spread
centripetally andresult in a necrotizing myelopathy.21 Inthe
immunocompetent host, VZV mye-litis occurs within 1 to 2 weeks of
theappearance of the dermatomal rash.
Very rarely, it may occur in the absence
of an observed rash. The myelitis occursat the level of the
affected dermatomeand results in paraparesis. In contrast,
VZV myelopathy often occurs insidi-ously and progresses slowly
in theimmunosuppressed host. The closetemporal relationship to the
rash sug-gests the diagnosis, which is confirmedby the presence of
VZV DNA by PCR inthe CSF or VZV antibody in the CSF. Inthese cases,
treatment with IV acyclovir(10 mg/kg every 8 hours) should
beinitiated.
In rare instances, usually with primary
infection, HSV-2, the etiology of genitalherpes, may cause a
sacral radiculitis22 oran ascending myelitis.23 These neuro-logic
complications are rarely observed
with recurrent HSV-2.24 Epstein-Barrvirus,25,26 the etiologic
agent of infec-tious mononucleosis, and CMV27 mayalso result in a
transverse myelitis at thetime of primary infection.
Intheimmunocompromisedhost,par-ticularly in the setting of HIV
infection,CMV may result in a transverse myelitis
or a polyradiculomyelitis. In exceptionalcases, it may be
observed in immuno-logically healthy individuals.28 CMVtransverse
myelitis may present withparaplegia, tetraplegia, urinary
retention,and sensory deficits, whereas CMV poly-radiculomyelitis
typically presents as aprogressive ascending hypotonic weak-ness
with hyporeflexia, paresthesia, hyp-esthesia, and early urinary
retention.29
MRI findings may include a thickenedcauda equina and enhancement
of theleptomeninges, dorsal roots, and caudaequina. A mixed
pleocytosis or polymor-phonuclear cell predominance on CSFanalysis
may suggest the diagnosis,
which can be confirmed by PCR. Whilefew controlled trials have
been reported,ganciclovir is recommended in combi-
nation with foscarnet if the patient hasbeen previously treated
or exhibits dis-ease progression.29 Cidofovir also hasactivity
against CMV.
KEY POINTS
h Many herpesviruses
may result in a
transverse myelitis.
h The presence of a
polymorphonuclear
pleocytosis in the
appropriate clinical
context suggests
cytomegalovirus
polyradiculoneuritis.
Infectious Myelopathies
766 www.aan.com/continuum August 2011
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
7/15
Enteroviruses
Enteroviruses, particularly poliovirus,can affect the spinal
cord. Fortunately,
effective vaccination has made this ill-ness very rare in the
Western world. Inthe United States in the recent past,approximately
10 to 15 cases of poliohave been reported yearly; most of these
were vaccine associated, although sev-eral occurred in
immigrants. Paralyticpoliomyelitis is a rare complication
ofpoliovirus infection (1% to 2%); mostinfections result in
inapparent infection(90% to 95%) or a minor illness with
mild systemic symptoms (5% to 10%).The poliovirus has a unique
predilectionto affect the anterior horn cells of thespinal cord and
therefore results in alower motor neuron type of weakness,
which is characterized by a flaccid weak-
ness with wasting, fasciculations, andareflexia. Weakness may
arise rapidlyover a 48-hour period or occur in adelayed fashion
over weeks from thetime of infection. Sensory and
sphincterfunctions are spared. Age of acquisition
of the infection determines the risk ofparalysis. Infants are
rarely paralyzed,childrens risks are intermediate, andadults are
much more frequently para-lyzed. Other Enteroviruses,
includingCoxsackieviruses and echoviruses, mayalso result in
myelitis.
West Nile Virus
West Nile virus is a mosquitoborneFlavivirus first recognized in
the Westernhemisphere in 1999 when 59 infectedpersons in New York
City were identi-fied.30 Following its introduction, the
virus rapidly spread widely throughoutthe United States.31
Approximately 5%of patients with symptomatic WestNile virus
infection (fewer than 1 in 5infected patients display
symptoms)develop severe neurologic disease, in-cluding meninigitis,
encephalitis, a polio-myelitis-like acute flaccid paralysis,
andother neurologic manifestations.32 The
flaccid weakness has been attributed toloss of anterior horn
cells.33 It typicallymanifests during the subacute phase of
the illness and peaks in 2 to 8 days. Theweakness affects one or
more limbs andis associated with flaccid tone andhyporeflexia or
areflexia. Mechanical
ventilation may be required because ofrespiratory muscle
weakness. MRI oftenshows cauda equina enhancement andparenchymal
spinal cord and leptome-ningeal signal changes, and the CSFshows a
neutrophilic leukocytosis.33
Pathologic features include perivascular
chronic inflammation and anterior horncell dropout.33
Other Viruses
While viruses may result in an acutemyelitis, they may also
trigger an auto-immune transverse myelitis. Distinguish-ing an
infectious from a parainfectiousdisorder can be difficult. It has
beenestimated that as many as 20% to 40% ofall patients with
transverse myelitis havea preceding or concurrent viral
infection.
Even in instances of neuromyelitisoptica, the consequence of an
antibodyto aquaporin 4, viral as well bacterialpathogens have been
considered poten-tial precipitants.34
BACTERIAL MYELOPATHIESSyphilis
CNS invasion by Treponema pallidumgenerally occurs within the
first year ofsyphilitic infection, and the frequency ofabnormal CSF
results in untreated pa-tients with primary or secondary syph-ilis
varies between 13.9% and 70%.Despite the high frequency of
CNSinvasion, only about 5% of patients withsyphilis will develop
clinical neurosyphi-lis if left untreated. At one time, syph-ilitic
spinal cord disease, particularlytabes dorsalis, was among the
mostcommon expressions of neurosyphilisand was 10 times more common
thanother forms of spinal syphilis. Syphilitic
767Continuum Lifelong Learning Neurol 2011;17(4):761775
www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
8/15
meningomyelitis and spinal vascularsyphilis were the second and
third mostcommon forms of spinal syphilis, re-
spectively. Spinal syphilis rarely occursin the absence of
syphilitic involvementat other sites of the neuraxis. It hasbeen
estimated that the incidence ofpure spinal syphilis is
approximatelyone-fifth the incidence of cerebrospinalsyphilis.
Syphilis may affect the spinal cord in avariety of fashions.35
The pathology maybe predominantly meningovascular orparenchymatous
in nature. Gummas
may grow within the substance of thecord or compress the cord by
growthfrom the surrounding meninges. Theclinical picture of spinal
cord compres-sion in syphilis may also arise as a resultof
hypertrophic pachymeningitis or ver-tebral lesions resulting from
syphiliticosteitis.
Tabes dorsalis. Tabes dorsalis(Case 3-2) is the prototypical
spinalcord disorder associated with syphilis.Currently, tabes
dorsalis accounts for no
more than 5% of neurosyphilis. Thelatency from infection to the
develop-ment of tabes averages 10 to 15 years but
varies between 2 and 38 years. As manyas 65% of patients recall
a history of
venereal infection. The disorder pre-dominantly appears in the
fourth andfifth decade, with an average age of on-set of 40 years.
Men are affected 10 timesmore often than women. Tabes dorsalis
has been observed, albeit rarely, as aconsequence of congenital
infection.
The clinical course of tabes has his-torically been divided into
three separate
phases: preataxic, ataxic, and terminal.The preataxic phase
begins insidiouslyand lasts on average 3 years. Subjective
symptoms predominate, including theclassic crisis, a severe
lancinating pain.The painful crisis heralds the disorder in70% of
patients and is ultimately presentin 90%. Impotence and sphincter
dys-function may be early features. Physicalexamination typically
shows absent
reflexes, sensory impairment, positiveRomberg sign, and Argyll
Robertson
Case 3-2A 54-year-old woman had noted severe painful spasms
affecting her abdomen and groin 3 monthsprior to examination. The
paroxysms of pain had no known precipitants and persisted despite
the useof a variety of analgesic medications. She also reported
that her legs were weak and heavy and thatshe had recently begun
using a laxative to induce bowel movements. She had recently moved
toKentucky from New York City to assist her 30-year-old daughter in
caring for her child. She reportedthat at the time of her daughters
birth she had been addicted to crack cocaine and in prenatal
testinghad been Venereal Disease Research Laboratory (VDRL)
positive. She recalls receiving one injection ofpenicillin at that
time. No lumbar punctures were performed.
On examination, she had irregular, small pupils that reacted to
light and accommodation. Lower
extremity strength was graded as 4+/5 and the legs were spastic,
but knee and ankle jerks could notbe elicited. Plantar responses
were extensor bilaterally. Her gait was spastic and ataxic and she
couldnot tandem. Her gait had a slapping quality, but no footdrop
was evident. Vibratory sense wasseverely impaired to the knees and
she could not sense toe movement well in either foot. Rombergtest
was positive.
Serum VDRL was positive at 1:64 and microhemagglutination assay
was positive, providing serologicevidence of syphilis. An MRI of
the cervical and thoracic cord was unremarkable. CSF analysis
showed9 lymphocytes/mm3, protein of 72 mg/dL, and positive VDRL.
Treatment with IV penicillin wasadministered for tabes
dorsalis.
Comment. This patient had tabes dorsalis with a 30-year hiatus
from the time of inadequatetreatment for syphilis.
Infectious Myelopathies
768 www.aan.com/continuum August 2011
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
9/15
pupils. Hypalgesia, hyperalgesia, allo-cheiria (sensation of a
stimulus in onelimb is perceived in another), pallesthe-
sia (sensation of mechanical vibration), adelay in pain
perception of up to 15seconds following the application of
thestimulus, and an aftersensation lasting upto 30 seconds may all
be reported. Lossof deep pain sensation is evidenced bydiminished
sensation to the applicationof pressure to various anatomic sites:
theulnar nerve (Biernacki sign), the Achillestendon (Abadie sign),
and the testicle(Pitres sign). Despite the loss of pain,
superficial tactile sensation is generallywell preserved early
in the course of thedisorder.
The ataxic phase lasts between 2 and10 years and is
characterized by severe,predominantly lower limb, ataxia.
Gen-erally the tabetic pains worsen duringthis period. Arthropathy
develops in 5%to 10% of patients because of recurrenttraumatic
injury resulting from loss ofdeep pain sensation. Proprioceptive
lossthat causes a slapping gait predisposes
the knee joint to this injury. The tarsaljoints, hip, ankle, and
spine, as well asother joints, can be similarly involved.
The terminal phase also has an aver-age duration of between 2
and 10 years.Cachexia, leg stiffness and paralysis, andautonomic
dysfunction with obstinateconstipation and bladder incontinenceare
prominent. Sepsis from decubitusinfections and pyelonephritis is
fre-quently the terminal event.
The classic signs of tabes dorsalis areabsentin approximately
50% of patients inthe early stages of the disease because asmany as
10% of tabes dorsalis casesremain atypical throughout their
course.Other neurosyphilitic manifestations arefrequently observed
with tabes dorsalis,including generalparesis,
syphiliticmenin-gomyelitis, and spinal cord gummas.
The posterior spinal roots and poste-rior spinal columns of the
lower spinalcord are predominantly involved in
tabes dorsalis, and pathologic examina-tion reveals
leptomeningitis with de-myelination of the dorsal columns, root
entry zone, and Lissauer tract. Posteriorroots are destroyed and
replaced byfibrosis.
Syphilitic meningomyelitis. In the
present era, syphilitic meningomyelitisoccurs more frequently
than tabes dor-
salis. Syphilitic meningomyelitis affectspredominantly men
between the ages of
25 and 40 years. The latency from theonset of the infection to
the onset of
symptoms averages 6 years (range 1 to
30 years).
36
The first symptoms are asense of heaviness in the legs,
generallybilaterally. Paresthesia and fleeting pains
may be reported, with little apparent sen-sory disturbance on
examination. Thesymptom complex mirrors that of cer-
vical spondylotic myelopathy. Precipitate
frequency, hesitancy, and impotence arecommon. The predominant
finding onneurologic examination is a spastic weak-ness in the
extremities, especially thelower extremities. Muscle bulk is
pre-
served, and muscle stretch reflexes areexaggerated with positive
Babinskisigns. Sensory loss is slight. Occasionallya Brown-Sequard
syndrome, significantamyotrophy, or a clinical picture of
atransverse myelitis may complicatesyphilitic meningomyelitis.
Pathologicexamination reveals thickened, inflamedmeninges
predominating in the cervicalregion, with involvement of the
periph-ery of the spinal cord, especially the lat-eral columns.
Vascular involvement ofthe cord by both Heubner endarteritis,a
syphilitic medium-sized vessel vasculi-tis, and Nissl-Alzheimer
endarteritis, asyphilitic small vessel vasculitis, is seen.
Other forms of spinal syphilis. Awide variety of other
syphilitic spinalcord abnormalities can be found in
the literature, including hypertrophicpachymeningitis, gummas of
the spinalcord, spinal cord compression fromspinal gummas,
syphilitic osteitis (or
KEY POINT
h Syphilitic meningomyelitis
is more common than
tabes dorsalis.
769Continuum Lifelong Learning Neurol 2011;17(4):761775
www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
10/15
syphilitic aortitis), and spinal cord in-farction from
syphilitic vasculitis.
The recommended treatment of spi-
nal cord syphilis is the same as that ofother forms of
neurosyphilis, namely 12to 24 million units of aqueous
penicillindaily in divided doses administered every4 hours for 10
to 14 days.37 Othertreatment regimens38 using
doxycycline,ceftriaxone, or erythromycin may beconsidered if the
patient is intolerantof penicillin. However, these
treatmentregimens are not well established intreating symptomatic
neurosyphilis.
Tuberculosis
Neurologic complications of Mycobacte-rium tuberculosis remain
common insome parts of the world and should al-
ways be considered in individuals whohave emigrated from these
regions. It isestimated that 10 to 15 million peopleare infected
with M. tuberculosis in theUnited States. The most common causeof
myelopathy with tuberculosis arisesfrom skeletal involvement,
namely Pott
disease or tuberculous spondylitis,which accounts for one-half
of all skele-tal tuberculosis and develops in less than1% of all
infected persons.39 The myco-bacteria spread to the vertebrae
viablood, lymph, or direct contiguity fromthe lung. Symptoms and
signs of spinalcord involvement develop slowly and in-sidiously,
often without any systemic fea-tures to suggest tuberculosis. Back
painpredominates in most patients. The char-acteristic
roentgenographic defect is an-
terior wedging of two adjacent vertebraewith loss of the
intervening disk space.The spine is enveloped by pus
extrudinganteriorly from the affected vertebrae.Myelopathy
typically results from pres-sure on the anterior spinal cord
bycaseous or granulating tissue, inflamma-tory thrombosis of the
anterior spinalartery, or injury to the cord from
spinalinstability. Complete spinal cord tran-section may result
from the latter insult.
Myelopathy occurring in associationwith tuberculous infection
may alsooccur as a consequence of intramedul-
lary tuberculomas, intradural tuberculo-mas, and arachnoiditis
that may beunassociated with bony lesions.40 Inone study of spinal
tuberculosis,41 neu-rologic deficits were seen in 54% ofpatients
with bony tuberculous lesions,39% of patients with intraspinal
granulo-matous tissue occurring in the absenceof bony lesions, and
7% of patients withintraspinal tuberculomas.
A high index of suspicion for tuber-
culous myelopathy is required. In onestudy, only 41% of patients
exhibited apositive purified protein derivative test.39
Therapy of patients with spinal tuber-culosis requires at least
12 months ofantibiotic treatment as well as surgicaldecompression
in the presence of neu-rologic abnormalities.41 In the settingof
intraspinal granulomatous disease
without significant bony destruction,laminectomy and debridement
is ade-quate41; however, more aggressive ther-
apy is warranted when vertebral bodiesare involved. A two-stage
procedure com-prised of posterior instrumental stabi-lization
followed by anterior radicaldecompression permits earlier
mobiliza-tion after neurologic recovery,42 althoughcomplications
are common.43 Reports ofthe frequency of neurologic recovery
withspinal tuberculosis vary, but functionalrecovery rates as high
as 90% have beenreported.44 Patients with thoracic lesions
with severe neurologic deficits show theleast improvement, while
patients withlumbar disease have the best outcomes.44
Other Forms of BacterialMyelopathy
A number of other bacterial infectionshave been associated with
myelitis.On rare occasions, the spinal cordmay be seeded by
bacteria leading toa suppurative myelitis with abscess for-mation.
In a review by Dutton and
Infectious Myelopathies
770 www.aan.com/continuum August 2011
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
11/15
Alexander,45 direct spread from adjacentinfections was most
commonly ob-served; however, hematogenous dissem-
ination from endocarditis, pulmonaryinfections, and other sites
was also fre-quently observed. Staphylococci, Strep-tococci,
Escherichia coli, and Nocardiaare among the organisms that have
beenisolated in these cases. Catscratch dis-ease resulting from
Bartonella henselaehas been reported to cause a myelitis
with Brown-Sequard syndrome.46 In ad-dition to the typical
meningoradicu-litis and cranial neuropathies observed
with Lyme disease, the treponemal in-fection with Borrelia
burgdorferi, amyelopathy,47 and meningomyelitis48
may also occur. Rarely, Whipple diseasedue to Tropheryma
whippelii can alsocause a myelopathy.49,50
Myelopathies seen in association withbacterial infection may be
parainfectious.The transverse myelitis that accompaniesa bacterial
infection is similar clinically andpathologically to that following
viral infec-tion or vaccination. Among the reported
potential causes51,52
are scarlet fever,pertussis, whooping cough,
Mycoplasmapneumonia, and pneumococcal pneumo-nia, but it is likely
that transverse myelitismay follow any bacterial infection.
FUNGAL MYELOPATHIES
Isolated fungal disease of the spinalcord is rare. Certain fungi
(Blastomyces,Coccidiodes, and Aspergillus) may in-
vade the spinal epidural space. Gener-ally, the spinal cord is
compromised bylesions arising from a vertebral osteomye-litic focus
or by those extending throughthe intervertebral foramina. Certain
fungi,such as Cryptococcus neoformans, re-sult in granulomatous
meningitis, whichmay lead to intraspinal or extraduralgranulomas
that can compromise thespinal cord. Alternatively, these organ-isms
can lead to spinal cord infarctionas a result of the associated
meningo-
vascular inflammation. Aspergillosis is
generally observed only in patients whoare immunosuppressed,
with leukemiaand lymphoma being common predis-
posing illnesses. Aspergillosis has beenreported to affect the
spinal cord inseveral different fashions, including bycompromise of
the blood supply occur-ring in association with fungal
endar-teritis, by direct parenchymal infiltrationof the spinal
cord, or by cord compres-
sion from osteomyelitis, paravertebralmass,53 and epidural
abscess.54 Excep-tional case reports of myelopathy fromother fungi
can be found, including
Candida, Histoplasma capsulatum,Pseudallescheria boydii ,
Cladospo-rium trichoides, and paracoccidomy-cosis, among
others.
PARASITIC MYELOPATHIES
On a global scale, Schistosoma,55 partic-ularly S. haematobium
and S. mansoni,represents one of the most commoncauses of
infectious myelopathy. Theseorganisms are only seen in certain
geo-graphic regions, namely the Far East,
South America, and Africa. A history oftravel to these regions
and swimming orbathing in fresh water contaminated
with the cercariae that are released fromcertain aquatic snails
may suggest the
diagnosis. The disease results from granu-lomatous involvement,
typically of thelower spinal cord. The presentation maybe acute or
subacute. Lower limb pain and
weakness, sensory impairment, and blad-der and bowel dysfunction
are coupled
with MRI features that suggest an inflam-matory myelopathy. The
CSF exhibits aninflammatory pattern with or withouteosinophils.
Early diagnosis and treatmentare important for a good
outcome.56
Hydatid disease, which results fromthe larval form of the canine
tapeworm,Echinococcus granulosus, may causespinal intramedullary
cysts or compressthe spinal cord and roots because ofbone invasion.
The latter chiefly occursin the lower thoracic region.
KEY POINTS
h Bacterial and viral
infections may each
serve as a trigger
for autoimmune
transverse myelitis.
h Schistosomiasis should
always be considered in
those individuals with a
lower cord myelitis who
have traveled to regions
where the parasite
is endemic.
771Continuum Lifelong Learning Neurol 2011;17(4):761775
www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
12/15
Cysticercosis is the result of infectionwith the larval form of
pork tapeworm,Taenia solium. It is endemic in China,
southeast Asia, India, sub-SaharanAfrica, and Latin America.
Spinal cordinvolvement may complicate as manyas 5% of cases,
although the brain is thepreferred site in the CNS.
Cysticercosismost frequently infiltrates the subar-achnoid space,
but intramedullary fluid-
filled cysts are also observed. A slowlyprogressive myelopathy
implicating alesion in the cervical or thoracic spinal
cord is the typical mode of presen-tation for these lesions.
Therapy withalbendazole may be effective in eradi-cating the live
parasite.
Paragonimiases, a lung fluke acquiredby eating undercooked
freshwater crabs,occurs chiefly in China but may be seenin other
parts of the world. Spinal corddisease results from extradural, or
morerarely, intradural granuloma formation.Angiostrongylus
cantonensis, the mostcommon cause of eosinophilic menin-
gitis and meningoencephalitis in theworld, has also been
reported to causespinal cord disease.57 In patients with
AIDS, toxoplasmosis has been reportedin rare instances to cause
an abscess ofthe spinal cord.
EPIDURAL ABSCESSES
Spinal epidural abscess may present as asurgical emergency
evolving rapidlyover several days or may arise more
Case 3-3A 72-year-old man with diabetes presented with fever,
low back pain, a
sense of lower extremity weakness, and difficulty urinating and
defecating3 weeks after undergoing prostate surgery. He stated that
the back painstarted approximately 10 days ago and was accompanied
by fever, chills,and sweats. He attributed the problem to the flu
and treated himself withantipyretics and analgesics. A sense of
weak knees and difficulty withsphincter function that developed
over the preceding 24 hours promptedhim to seek medical attention.
Examination was remarkable for atemperature of 38.3-C (101-F),
percussion tenderness over the middleportion of his lower spine,
4/5 strength in the quadriceps and footdorsiflexors, and depressed
knee and ankle jerks. Sensory perception wasimpaired to vibratory
sense in distal lower extremities. An MRI showed anepidural abscess
extending from L2 to L5. He recovered completelyfollowing surgical
evacuation and antibiotic administration. Enterococcus
was cultured from the surgically evacuated pus.Comment.
Infectious myelopathies are often diagnostically challenging.
They can present in myriad fashions, and their onset may be
acute,subacute, or chronic. Pain, weakness, spasticity, sensory
symptoms, orsphincter disturbances may be the dominant feature. A
high index ofsuspicion is required by the clinician. Clues to the
correct diagnosis areoften, but not invariably, present in the
history and physical examination.
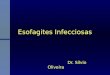
FIGURE 3-3 Epidural abscess. This midthoracic epiduralabscess
shows extension over several vertebrallevels on gadolinium-enhanced
MRI.
Infectious Myelopathies
772 www.aan.com/continuum August 2011
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
13/15
indolently. Staphylococcus aureus isthe etiologic agent in over
50% of acutespinal epidural abscesses, although a
broad spectrum of other organismsmay be implicated.58 Infection
mayspread directly from a focus of osteo-myelitis or hematogenously
from adistant site, such as skin furuncles orpulmonary infections.
Trauma to theback, typically very minor in nature, hasbeen reported
by as many as one-thirdof individuals developing spinal epi-dural
abscess (Case 3-3).59 A high de-gree of suspicion for spinal
epidural
abscess should be maintained when IVdrug abusers present with
fever andback pain. Patients with an acute epi-dural abscess
typically have more sys-temic illness than those with
vertebralosteomyelitis.60 The definitive diagnosisis based on
identification of the offend-ing organism from pus from the
ab-scess, although blood cultures arepositive in 60% of cases.60
MRI is thediagnostic modality of choice and gado-linium
administration increases diag-
nostic sensitivity (Figure 3-3).
REFERENCES1. Kincaid O, Lipton HL. Viral myelitis: an
update.
Curr Neurol Neurosci Rep 2006;6(6):469Y474.
2. Sejvar JJ, Marfin AA. Manifestations of West
Nile neuroinvasive disease. Rev Med Virol
2006;16(4):209Y224.
3. de la Monte SM, Ho DD, Schooley RT, et al.
Subacute encephalomyelitis of AIDS and its
relation to HTLV-III infection. Neurology
1987;37(4):562Y569.
4. Petito CK, Navia BA, Cho ES, et al. Vacuolar
myelopathy pathologically resembling
subacute combined degeneration in patients
with the acquired immunodeficiency
syndrome. N Engl J Med 1985;312(14):
874Y879.
5. Weill O, Finaud M, Bille F, et al. [Malignant
spinal cord glioma. A new complication of
HIV virus infection?]. Presse Med 1987;
16(39):1977.
6. Honig LS, Vogel H, Horoupian DS. Chronic
myelopathy as a presenting syndrome in HIV
infection. Neurology 1989;(suppl 1):419.
7. Eyer-Silva WA, Auto I, Pinto JF,
Morais-de-Sa CA. Myelopathy in a previously
asymptomatic HIV-1-infected patient.
Infection 2001;29(2):99Y102.
8. Kamin SS, Petito CK. Idiopathic myelopathies
with white matter vacuolation in
non-acquired immunodeficiency syndrome
patients. Hum Pathol 1991;22(8):816Y824.
9. Denning DW, Anderson J, Rudge P, Smith H.
Acute myelopathy associated with primary
infection with human immunodeficiency
virus. Br Med J (Clin Res Ed) 1987;294(6565):
143Y144.
10. Sartoretti-Schefer S, Blattler T, Wichmann
W. Spinal MRI in vacuolar myelopathy, and
correlation with histopathological findings.
Neuroradiology 1997;39(12):865Y869.
11. Shimojima Y, Yazaki M, Kaneko K, et al.Characteristic spinal
MRI findings of
HIV-associated myelopathy in an AIDS
patient. Intern Med 2005;44(7):763Y764.
12. Di Rocco A, Simpson DM. AIDS-associated
vacuolar myelopathy. AIDS Patient Care
STDS 1998;12(6):457Y461.
13. Williams AE, Fang CT, Slamon DJ, et al.
Seroprevalence and epidemiological
correlates of HTLV-I infection in U.S. blood
donors. Science 1988;240(4852):643Y646.
14. Khabbaz RF, Darrow WW, Hartley TM, et al.
Seroprevalence and risk factors for HTLV-I/II
infection among female prostitutes in the
United States. JAMA 1990;263(1):60Y64.
15. Lima MA, Harab RC, Schor D, et al. Subacute
progression of human T-lymphotropic virus
type I-associated myelopathy/tropical spastic
paraparesis. J Neurovirol 2007;13(5):468Y473.
16. Sheremata WA, Berger JR, Harrington WJ Jr,
et al. Human T lymphotropic virus type
I-associated myelopathy. A report of 10
patients born in the United States. Arch
Neurol 1992;49(11):1113Y1118.
17. Vernant JC, Maurs L, Gessain A, et al. Endemic
tropical spastic paraparesis associated with
human T-lymphotropic virus type I: a clinical
and seroepidemiological study of 25 cases.Ann Neurol
1987;21(2):123Y130.
18. Akizuki S, Nakazato O, Higuchi Y, et al.
Necropsy findings in HTLV-I associated
myelopathy. Lancet 1987;1(8525):156Y157.
19. Nakamura T, Nishiura Y, Eguchi K. Therapeutic
strategies in HTLV-I-associated myelopathy/
tropical spastic paraparesis (HAM/TSP). Cent
NervSyst Agents MedChem 2009;9(2):137Y149.
20. Lehky TJ, Flerlage N, Katz D, et al. Human
T-cell lymphotropic virus type II-associated
myelopathy: clinical and immunologic
profiles. Ann Neurol 1996;40(5):714Y723.
773Continuum Lifelong Learning Neurol 2011;17(4):761775
www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
14/15
21. Rose FC, Brett EM, Burston J. Zoster
encephalomyelitis. Arch Neurol 1964;
11:155Y172.
22. Caplan LR, Kleeman FJ, Berg S. Urinaryretention probably
secondary to herpes
genitalis. N Engl J Med 1977;297(17):920Y921.
23. Klatersky J, Cappel R, Snoeck JM, et al.
Ascending myelitis in association with
herpes-simplex virus. N Engl J Med 1972;
287(4):182Y184.
24. Berger JR, Houff S. Neurological complications
of herpes simplex virus type 2 infection. Arch
Neurol 2008;65(5):596Y600.
25. Grose C, Feorino PM. Epstein-Barr virus and
transverse myelitis. Lancet 1973;1(7808):892.
26. Silverstein A. Epstein Barr virus infections of
the nervous system. In: Vinken PJ, Bruyn GW,ed. Handbook of
clinical neurology: infections
of the nervous system. Vol 34. Amsterdam:
North Holland Publishing, 1978.
27. Tyler KL, Gross RA, Cascino GD. Unusual viral
causes of transverse myelitis: hepatitis A
virus and cytomegalovirus. Neurology 1986;
36(6):855Y858.
28. Fux CA, Pfister S, Nohl F, Zimmerli S.
Cytomegalovirus-associated acute transverse
myelitis in immunocompetent adults. Clin
Microbiol Infect 2003;9(12):1187Y1190.
29. Maschke M, Kastrup O, Diener HC. CNS
manifestations of cytomegalovirus
infections: diagnosis and treatment. CNSDrugs
2002;16(5):303Y315.
30. Nash D, Mostashari F, Fine A, et al. The
outbreak of West Nile virus infection in the
New York City area in 1999. New Engl J Med
2001;344(24):1807Y1814.
31. Huhn GD, Sejvar JJ, Montgomery SP,
Dworkin MS. West Nile virus in the United
States: an update on an emerging infectious
disease. Am Fam Physician 2003;68(4):
653Y660.
32. Campbell GL, Marfin AA, Lanciotti RS,
Gubler DJ. West Nile virus. Lancet Infect Dis
2002;2(9):519Y
529.33. Jeha LE, Sila CA, Lederman RJ, Prayson RA,
Isada CM, Gordon SM. West Nile virus
infection: a new acute paralytic illness.
Neurology 2003;61(1):55Y59.
34. Sellner J, Hemmer B, Muhlau M. The clinical
spectrum and immunobiology of
parainfectious neuromyelitis optica (Devic)
syndromes. J Autoimmun 2010;34(4):371Y379.
35. Berger JR, Moskowitz L, Fischl M, Kelley RE.
Neurologic disease as the presenting
manifestation of acquired immunodeficiency
syndrome. South Med J 1987;80(6):683Y686.
36. Fisher M, Poser CM. Syphilitic meningomyelitis:
a case report. Arch Neurol 1977;34(12):785.
37. Centers for Disease Control and Prevention.
Syphilis: recommended treatment schedules,1976. Recommendations
established by
the Venereal Disease Control Advisory
Committee.Ann Intern Med 1976;85(1):94Y96.
38. Berger JR. Neurosyphilis. In: Johnson R, ed.
Current therapies in neurology.
Philadelphia: B. C. Decker, 1990:143Y148.
39. Schlesinger N, Lardizabal A, Rao J,
McDonald R. Tuberculosis of the spine:
experience in an inner city hospital.
J Clin Rheumatol 2005;11(7):17Y20.
40. Hristea A, Constantinescu RV, Exergian F,
et al. Paraplegia due to non-osseous spinal
tuberculosis: report of three cases and
review of the literature. Int J Infect
Dis2008;12(4):425Y429.
41. Nussbaum ES, Rockswold GL, Bergman TA, et al.
Spinal tuberculosis: a diagnostic and
management challenge. J Neurosurg 1995;
83(2):243Y247.
42. Moon MS, Ha KY, Sun DH, et al. Potts
paraplegiaV67 cases. Clin Orthop Relat Res
1996;(323):122Y128.
43. Jain AK, Dhammi IK. Tuberculosis of the
spine: a review. Clin Orthop Relat Res 2007;
460:39Y49.
44. Vidyasagar C, Murthy HK. Spinal tuberculosis
with neurological deficits. Natl Med J India1996;9(1):25Y27.
45. Dutton JE, Alexander GL. Intramedullary
spinal abscess. J Neurol Neurosurg Psychiatry
1954;17(4):303Y307.
46. Pickerill RG, Milder JE. Transverse myelitisassociated with
cat-scratch disease in an
adult. JAMA 1981;246(24):2840Y2841.
47. Reik L, Steere AC, Bartenhagen NH, et al.
Neurologic abnormalities of Lyme disease.Medicine (Baltimore)
1979;58(4):281Y294.
48. Viader F, Poncelet AM, Chapon F, et al.
[Neurologic forms of Lyme disease. 12 cases].
Rev Neurol (Paris) 1989;145(5):362Y368.49. Clarke CE, Falope ZF,
Abdelhadi HA, Franks AJ.
Cervical myelopathy caused by Whipples
disease. Neurology 1998;50(5):1505Y1506.
50. Schroter A, Brinkhoff J, Gunthner-Lengsfeld T,
et al. Whipples disease presenting as an
isolated lesion of the cervical spinal cord. Eur
J Neurol 2005;12(4):276Y279.
51. Gibbons JL, Miller HG, Stanton JB.
Para-infectious encephalomyelitis and
related syndromes; a critical review of the
neurological complications of certain specific
fevers. Q J Med 1956;25(100):427Y505.
Infectious Myelopathies
774 www.aan.com/continuum August 2011
Copyright @ American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/22/2019 00132979-201108000-00006 - Mielopatas Infecciosas
15/15
52. Kincaid JC, Dyken M. Myelitis and myelopathy.
In: Baker A, Baker L, eds. Clinical neurology.
New York: Harper & Row, 1982:1Y31.
53. Koh S, Ross LA, Gilles FH, et al. Myelopathyresulting from
invasive aspergillosis. Pediatr
Neurol 1998;19(2):135Y138.
54. Hendrix WC, Arruda LK, Platts-Mills TA, et al.
Aspergillus epidural abscess and cord
compression in a patient with aspergilloma
and empyema. Survival and response to high
dose systemic amphotericin therapy. Am Rev
Respir Dis 1992;145(6):1483Y1486.
55. Suchet I, Klein C, Horwitz T, et al. Spinal
cordschistosomiasis: a case report and review ofthe literature.
Paraplegia 1987;25(6):491Y496.
56. Ferrari TC, Moreira PR, Cunha AS. Clinical
characterizationof neuroschistosomiasis due to
Schistosoma mansoni and its treatment. Acta
Trop 2008;108(2Y3):89Y97.
57. Petjom S, Chaiwun B, Settakorn J, et al.
Angiostrongylus cantonensis infectionmimicking a spinal cord
tumor. Ann Neurol
2002;52(1):99Y101.
58. Kaufman DM, Kaplan JG, Litman N. Infectious
agents in spinal epidural abscesses. Neurology
1980;30(8):844Y850.
59. Baker AS, Ojemann RG, Swartz MN,
Richardson EP Jr. Spinal epidural abscess. N
Engl J Med 1975;293(10):463Y468.
60. Currier BL, Kim CW, Eismont FJ. Infections of
the spine. In: Herkowitz HN, Garfin SR,
Eismont FJ, et al, editors. Rothman Simeone:
the spine. 5th ed. Philadelphia: Saunders,
2006:1265Y1316.
775Continuum Lifelong Learning Neurol 2011;17(4):761775
www.aan.com/continuum