-
7/28/2019 04 Hemoglobin Thalassemias
1/37
Thalassemia
-
7/28/2019 04 Hemoglobin Thalassemias
2/37
Objectives
Explain the pathophysiology that causes
thalassemia & hemoglobinopathies.
Explain how thalassemias are categorized. Correlate the results
of laboratory testing w/
specific thalassemias & hemoglobinopathies.
Dithionite tube test
Hemoglobin electrophoresis
Alkali denaturation test for fetal hemoglobin
-
7/28/2019 04 Hemoglobin Thalassemias
3/37
Objectives
Discuss specifics of specimen collection,handling, storage, and
preparation.
Explain the physiologic theory relevant to
thetest/procedure.
Explain the principle of the test/procedure
Identify the disease manifestation/clinical
correlation. Differentiate or resolve technical, instrument,
or
physiologic causes of problems or unexpectedtest results.
-
7/28/2019 04 Hemoglobin Thalassemias
4/37
-
7/28/2019 04 Hemoglobin Thalassemias
5/37
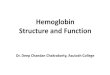
Characteristics: Thalassemia
Hereditary disorders
Results into moderate
to severe anemia Basic defect: reduced
production of selected
globin chains
Epidemiology:
Mediterranean, Africa,
Western SEA, India,Burma
Distribution parallels
that of P. falciparum
-
7/28/2019 04 Hemoglobin Thalassemias
6/37
-
7/28/2019 04 Hemoglobin Thalassemias
7/37
Special Cases
Thalassemia Hb Lepore: fusion seen in some types
of thalassemia
Hb Constant Spring
chain with 31 additional amino acids
--/cs
Hereditary persistence of fetal hemoglobin(HPFH)
-
7/28/2019 04 Hemoglobin Thalassemias
8/37
Clinical Picture
Thalassemia minor:Asymptomatic or minimal pallor and mild
splenomegaly
Thalassemia major: Severe pallor / Jaundice (muddy face)
HSM
LAD
Growth retardation
Mongoloid face
-
7/28/2019 04 Hemoglobin Thalassemias
9/37
Laboratory Investigations
Peripheral blood exam: Microcytic hypochromic anemia -
Reticulocytic ct S. iron and S. Ferritin - B1
Hb electrophoresis: Hgb Barts; Hgb H HbF; HbA2
B.M exam: Erythroid hyperplasia
Alkaline denaturation test: Resistant
Radiological Investigations: (Beta Thal) X-Ray skull: wide
diploic space and Hair on end appearance
Long bones: widen medullary cavities; Trabeculations
-
7/28/2019 04 Hemoglobin Thalassemias
10/37
Differential Diagnosis
Other microcytic hypochromic anemias
(ATIS)
Other hemolytic anemias: Facialappearance; Hb
electrophoresis
-
7/28/2019 04 Hemoglobin Thalassemias
11/37
Course and Treatment
Thalassemia Time of presentation
Related to degree of severity
Usually in first few years of life
-
7/28/2019 04 Hemoglobin Thalassemias
12/37
Course and Treatment
Thalassemia Untreated severe T:
--/--: Prenatal orperinatal death
--/- & --/cs:
Normal life span w/chronic hemolytic
anemia
Untreated T:
Major: Death in first orsecond decade of life
Intermedia: Usually
normal life span Minor/Minima: Normal
life span
-
7/28/2019 04 Hemoglobin Thalassemias
13/37
Treatment
Blood transfusion: when Hb 6 gm% Keep Hb 10 (hypertransfusion)
Keep Hb 12 (supertransfusion)
Iron chelating agent (Desferroxamine)
Folic acid
Antibiotics for Intercurrent infections
Spleenectomy Hypersplenism Pressure manifestations
BMT
-
7/28/2019 04 Hemoglobin Thalassemias
14/37
Complications:
Heart Failure
Liver Failure
Intercurrent Infections
-
7/28/2019 04 Hemoglobin Thalassemias
15/37
Thalassemia
N to inc RPI
Normal RDW
PBS: Target cells Mentzer index
-
7/28/2019 04 Hemoglobin Thalassemias
16/37
Alpha Thalassemia
-
7/28/2019 04 Hemoglobin Thalassemias
17/37
Alpha Thalassemia
Each RBC precursorhas 2 alpha globingenes on each chr16, a total
of 4 alphaglobin genes
Types of alphathalassemia resultfrom deletion of 1 ormore of
these genes
-
7/28/2019 04 Hemoglobin Thalassemias
18/37
AT 1 (Hetero -)
SEA
AT Trai t
AT 2 (Hetero -)
Afr ican/ Medit
Silent Carrier
AT 2 (Homo-)
A fr ican/ Medit
AT Trai t
Genedeletions
Clinical
(s/s)
Minimal / no
anemia
Microcytosis w/
dec MCV
Silent / no
anemiaNo RBC
abnormality in
adults
Minimal / no
anemia
Microtytosis w/
dec MCV
HgbBarts
4 to 10% in NB 1 to 3% in NB 4 to 10% in NB
Hgb H (+) in NB & adult Normal Hgb
electrophoresis
in adults
(+) in NB & adult
-
7/28/2019 04 Hemoglobin Thalassemias
19/37
-
7/28/2019 04 Hemoglobin Thalassemias
20/37
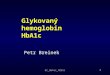
Hemoglobin H Disease
.
Survive to adulthood
10 to 25% Hgb H in NB & adults
Tetramer unstable & precipitate as Heinz
bodies or lead to increased poikilocytosis
-
7/28/2019 04 Hemoglobin Thalassemias
21/37
Hemoglobin H Disease
Marriage: AT 1 minor XAT 2 minor
Unusual, because ofmarked disparity ingeographic &
racial
distribution, Except for asmall number of personsin SEA who have
AT 2
W/ Hgb Constant Spring,in SEA population alongw/ AT 1
Hgb-CS: Presence of anon-functional alphaglobin gene on 1 chr 16
Heterozygous- no
detectable abnormality
Homozygous- w/ an
abnormal gene on each chr16- mild hemolytic
anemia(normocytic)
-
7/28/2019 04 Hemoglobin Thalassemias
22/37
Hemoglobin H Disease
Marriage: Heterozygous AT 1 + homo- or
hetero- zygous for Hgb CS Hgb H dse
-
7/28/2019 04 Hemoglobin Thalassemias
23/37
Alpha Thalassemia Major
AT 1 (Hetero-) + AT 1 (Hetero-) = AT major(Homozygous)
Most common cause for hydrops fetalis inpersons of SEA
ancestry
Anemic in utero; severe hydrops fetalisstillbirth, or death soon
after birth from
pulmonary hypoplasia or cardiac failure 80% Hgb Bart's & 20%
Hgb Portland
(sometimes Gower 1)
-
7/28/2019 04 Hemoglobin Thalassemias
24/37
Alpha Thalassemia Major
Marked
anisopoikilocytosis, w/
presence of immatureRBC's
(Polychromasia,
NRBC's &
erythroblasts)
-
7/28/2019 04 Hemoglobin Thalassemias
25/37
-
7/28/2019 04 Hemoglobin Thalassemias
26/37
Beta thalassemia
-
7/28/2019 04 Hemoglobin Thalassemias
27/37
Beta T GENERAL FEATURES:
PBS:
HYPOCHROMIC
RBCs
TARGET CELLS
Basophilic STIPPLING
NRBC
N- INC. SERUM Fe INC. Hb F & A2
BM
Erythroid Hyperplasia
Skeletal Deformities Extramedullary
Hematopoiesis
HSM
-
7/28/2019 04 Hemoglobin Thalassemias
28/37
BETA (MEDITERRANEAN/
COOLEYS) MINOR
(HETEROZYGOUS) ASYMPTOMATIC (DDx vs
IDA)
DEC. Hb RBC> 5 (MILD ANEMIA)
INC. A2 & F
INC. S. Fe/ N TIBC
INTERMEDIA MOD SEVERE ANEMIA NO NEED FOR
TRANSFUSION
MAJOR(HOMOZYGOUS) FATAL BEFORE 10 Y/O
MASSIVE SPLEENOMEG/HEMOLYSIS
INC. HbF & A2
VARIANTS: BETAo;BETA+; DELTA BETA
-
7/28/2019 04 Hemoglobin Thalassemias
29/37
-
7/28/2019 04 Hemoglobin Thalassemias
30/37
-
7/28/2019 04 Hemoglobin Thalassemias
31/37
-
7/28/2019 04 Hemoglobin Thalassemias
32/37
-
7/28/2019 04 Hemoglobin Thalassemias
33/37
Thalassemia
-
7/28/2019 04 Hemoglobin Thalassemias
34/37
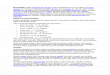
Thalassemia
Hair on end appearance of the skull on X-ray-
due to extramedullary hematopoiesis
Microcytic
hypochromicRBCs
Puffy cheeks & frontal bossing
Pencil
shapedRBCs
Target
cells
-
7/28/2019 04 Hemoglobin Thalassemias
35/37
Beta T Major: Complications:
Hemolytic A, Ineffective Erythropoiesis
Growth Retardation
Systemic Iron Overload (Chronic BT)
Death (2nd-3rd Decade)
-
7/28/2019 04 Hemoglobin Thalassemias
36/37
WWW Sites of Interest
Joint Center for Sickle Cell and Thalassemic
Disorders: http://www-
rics.bwh.harvard.edu/sickle/ (Overview of sicklecell disease,
thalassemia and iron kinetics)
The Sickle Cell Information Center, Emory
University:
http://www.emory.edu:80/PEDS/SICKLE/(Includes PowerPoint
presentations on sickle
cell disease)
-
7/28/2019 04 Hemoglobin Thalassemias
37/37