Embed Size (px)
Citation preview

STORY진단검사
Microsatellite Instability(MSI) test
2015.March
Vol.23
발행일자_ 2015년 3월 2일
발행기관_ 의료법인 삼광의료재단
발행부서_ CRM팀
문 의 처_ 02) 3497-5100
www.smlab.co.kr
현미부수체 불안정성 검사
유전성 비용종증 대장암(HNPCC, Hereditary NonPolyposis Colorectal Cancer)
유전성대장암은 전체 대장암의 약 5%정도를 차지하는데, 이 중 유전성 비용종증 대장암(HNPCC,
Hereditary NonPolyposis Colorectal Cancer)이 가장 흔하며 전체 대장암의 2~3%를 차지합니다.
HNPCC는 복제실수교정유전자(mismatch repair gene, MMR)의 결함으로 발생하며, 임상적으로 한
가계 내에 여러 명의 대장암 환자가 발생하고, 대체로 조기에 발병합니다.
HNPCC는 상염색체 우성 유전질환으로 대장암을 비롯하여 다양한 장기의 암을 발생시키는 질환
입니다. HNPCC과 관련된 유전자 돌연변이를 가지고 태어난 경우 일생동안 대장암에 걸릴 확률은
70~90%이며, 여성의 경우 대장암 외에 자궁내막암에 걸릴 확률은 40~70%, 난소암은 5~25%입니다.
그 외 비뇨기계암, 위암을 포함한 소화기암이 발생할 가능성도 높습니다.
MMR의 배선돌연변이는 전체 HNPCC 중 약 50%에서 발견됩니다. hMHL1, hMSH2 유전자의 돌연
변이가 가장 흔하며 전체 환자 중 약 26~30%가 hMSH2 유전자, 15~20%가 hMHL1유전자, 그 다음
으로 hMSH6 유전자에서 발견됩니다.
Contents
•유전성 비용종증 대장암
•유전성 비용종증 대장암의 진단
•MSI (현미부수체 불안정성) 검사
• 검사정보
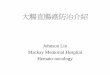
Sporadic CRCs
(65-85%) Familial CRCs (10-25%)
Peutz-Jeghers syndrome Juvenile polyposis (‹ 1%)
MYH-associated polyposis (‹ 1%)
Hereditary nonpolyposis colorectal cancer (2-3%)
Familial adenomatous polyposis (1%)
Fig 1. Hereditary colorectal cancer

▒ HNPCC의 암 발생기전
HNPCC의 암 발생기전은 현미부수체 불안전성(MSI)와 복제실수기전(MMR)으로 설명할 수 있으며, 산발성 대장암의 약
15~25%에서도 이와 같은 암 발생기전에 의하여 암이 발생합니다. 그러나 HNPCC의 경우 이미 한 쪽 대립유전자에 MMR
돌연변이를 가지고 있어 나머지 한 쪽에만 돌연변이가 생기면 암이 발생하므로 두 대립유전자에 모두 돌연변이가 발생해야
암이 발현되는 산발성 대장암보다 암이 쉽게 발생합니다. MMR 돌연변이에 의하여 세포 내 유전자 상 MSI가 축적되고, 특히
암 억제, 발생과 관련된 세포성장조절, 세포자멸사, 세포 내 신호전달 등의 기능을 하는 유전자들이 영향을 받게 되면 유전체
의 안정성이 붕괴되어 결국 암이 발생합니다.
HNPCC 환자의 암 조직 DNA를 정상조직 DNA와 비교하면 현미부수체(microsatellite)의 길이가 짧아지거나 길어지는
것을 발견할 수 있는데, 이를 현미부수체 불안정성(MSI, microsatellite instability)이라고 합니다. MSI는 HNPCC에서 아
주 특징적인 현상이므로 HNPCC를 진단하는데 매우 중요합니다.
유전성 비용종증 대장암의 진단
HNPCC의 진단에는 정확한 가족력을 바탕으로 하는 가계도 분석이 가장 중요합니다. 특히 대장암이 일찍 발생하거나, 동
시성 및 이시성 암이 있는 경우, 자궁내막암을 비롯한 관련 암의 가족력이 있는 경우에는 의심해보아야 합니다. HNPCC
의 진단기준은 현재 1999년에 발표된 암스테르담 진단기준 II와 수정된 암스테르담 진단기준이 많이 사용되고 있습니다.
암스테르담 진단기준을 만족하는 경우 반드시 유전자 검사를 받아야 합니다. 유전자 검사는 질병의 원인이 되는 MMR 돌
연변이 유무를 확인하는 것으로 환자의 진단·치료 및 가족구성원의 건강관리에 매우 유용합니다.
HNPCC의 MMR 배선돌연변이의 90% 이상은 hMSH2와 hMLH1 유전자에서 발견되므로 우선 이 두 유전자에 대한 돌연
변이가 발견되지 않는 경우, 추가적으로 hMSH6 유전자 돌연변이에 대한 검사를 시행할 수 있습니다.
Table 1. Diagnosis of Hereditary Nonpolyposis Colorectal Cancer
Amsterdam criteria II
1. At least three family members with HNPCC-related cancer*, one of whom is first-degree relative of the other two.
2. At least two generations with HNPCC-related cancer
3. At least one individual <50 y at diagnosis of HNPCC-related cancer.
Modified Amsterdam criteria
1. Two first-degree relatives with colorectal cancer involving two generations.
2. At least one case diagnosed before 55 y or
3. Two first-degree relatives with colorectal cancer and a third relative with endometrial cancer or another HNPCC-related cancer.
Abbreviations: HNPCC, Hereditary nonpolyposis colorectal cancer.
*HNPCC-related cancer: colorectal, endometrial, small bowel, ureter, renal pelvis
유전성 비용종증 대장암 진단의 중요성
첫째, 대장암 가족력이 있는 가족 중 고위험군 구성원 조기 발견
둘째, 정기검진을 통한 질병의 예방 및 조기 검진

그러나 위의 유전자검사는 시간과 비용이 많이 소요되므로 유전자 검사 대상을 선정하기 위해 현미부수체 불안정성 검사
를 시행할 수 있습니다.
미국 베데스다 가이드라인에서는 HNPCC의 임상 양상을 보이는 환자의 경우 MSI 검사를 선별검사로 시행 할 것을 권고
하고 있습니다.
MSI는 유전성이 없는 산발성 대장암 조직의 10~15% 정도에서만 발견되지만 HNPCC에서는 거의 대부분에서 발견되므로
HNPCC가 의심되는 환자 중 유전자 진단이 필요한 환자를 선별하는데 중요하게 사용할 수 있습니다.
MSI (현미부수체 불안정성) 검사
본 검사는 기존 USA NCI(national cancer institute)를 시작으로 범용적으로 사용되었던 Bethesda loci가 아닌 통계
Database를 통해 선정된 Quasi loci를 사용함으로써 MSI 분석에 있어 기존의 Bethesda loci보다 높은 정확도를 가집니다.
Bethesda loci와 Quasi loci의 민감도와 특이도를 비교한 자료는 아래와 같습니다.
Bethesda markers : D2S123, D17S250, D5S346, BAT-25, BAT-26
Quasi markers : NR-27, NR-21, NR-24, BAT-25, BAT-26
종양세포와 정상세포에서 DNA를 추출하여 Quasi loci에 있는 현미부수체인 NR-27, NR-21, NR-24, BAT-25, BAT-26
마커를 PCR반응으로 증폭하여 분석합니다.
Markers LocusChromosomal
locationsRepeat Sensitivity(%) Specificity(%)
Bethesda
D2S123 Di 91 86
D17S250 Di 88 93
D5S346 Di 81 98
Bethesda
Quasi 공통
BAT-25 4q11-12 Mono 96 99.5
BAT-26 2p22-21 Mono 93 100
Quasi
NR-27 2p22.1 Mono 98 100
NR-21 14q11.2 Mono 99 100
NR-24 2q11.2 Mono 92 100
Table 2. The Revised Bethesda Guidelines for testing colorectal tumors for microsatellite instability (MSI)
Tumors from individuals should be tested for MSI in the following situations:
1. Colorectal cancer diagnosed in a patient who is less than 50 years of age.
2. Presence of synchronous, metachronous colorectal, or other HNPCCassociated tumors,* regardless of age.
3. Colorectal cancer with the MSI-H† histology‡ diagnosed in a patient who is less than 60 years of age.§
4. Colorectal cancer diagnosed in one or more first-degree relatives with an HNPCC-related tumor, with one of the cancers being
diagnosed under age 50 years.
5. Colorectal cancer diagnosed in two or more first- or second-degree relatives with HNPCC-related tumors, regardless of age.
* Hereditary nonpolyposis colorectal cancer (HNPCC)-related tumors include colorectal, endometrial, stomach, ovarian, pancreas, ureter and renal pelvis, biliary tract, and brain (usually glioblastoma as seen in Turcot syndrome) tumors, sebaceous gland adenomas and keratoacanthomas in Muir–Torre syndrome, and carcinoma of the small bowel (48).
† MSI-H = microsatellite instability–high in tumors refers to changes in two or more of the five National Cancer Institute-recommended panels of microsatellite markers.
‡ Presence of tumor infiltrating lymphocytes, Crohn’s-like lymphocytic reaction, mucinous/signet-ring differentiation, or medullary growth pattern.
§ There was no consensus among the Workshop participants on whether to include the age criteria in guideline 3 above; participants voted to keep less than 60 years of age in the guidelines.

Reference
1. Quasimonomorphic mononucleotide repeats for high-level microsatellite instability analysis. Disease Markers 2004; 20: 251-257
2. Detection of Microsatellite Instability in colorectal cancer using an alternative multiple assay of Quasi-Monomorphic Mononucleotides
markers. Journal of Molecular Diagnostics 2008; 10: 154-159
3. Simplified MSI marker panel for diagnosis of colorectal cancer. Asian Pacific Journal of Cancer Prevention. 2011; 12: 2101-2104
4. 김덕우. 유전성 대장암. Journal of Genetic Medicine 2010; 7: 24-36
5. Revised Bethesda guidelines for Hereditary nonpolyposis colorectal cacer (Lynch syndrome) and Microsatellite instability. Journal of the
National Cancer Institute, 2004; 96(4) 261-268
검사정보
검사코드 검사항목 검체 검사법 검사일정 보험코드
27694MSI(Microsatellite Instability)
Paraffin block(정상조직과 종양조직)
or
Unstained slide(정상조직과 종양조직 각 2장 이상)
PCR fragment analysis
화
7일
너274
CX574006
* 검체 주의사항 : 반드시 환자의 정상조직과 종양조직을 같이 주셔야 합니다.
* 유전자검사의뢰서와 유전자동의서를 함께 보내주십시오.
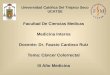
5개의 현미부수체 중 2개 이상의 마커에서 이상이 있는 군을 MSI-H(high)로 보고하고, 하나의 마커에서만 이상
이 있는 군은 MSI-L(low), 모든 마커에서 이상이 없는 군은 MSS(stable)로 보고합니다. 거의 모든 HNPCC에서
MSI-H 결과를 보이며, 간혹 MSI-L의 결과를 보이는 대장암 환자의 경우 일부에서 hMSH6 유전자의 돌연변이와
관련된 것으로 알려져 있습니다.
● MSS
NR-27 NR-21 NR-24 BAT-25 BAT-26
NR-27 NR-21 NR-24 BAT-25 BAT-26
● MSI-H