Embed Size (px)
Citation preview

1/23
Ch. 14.
INTRAPARTUM ASSESSMENT
부산백병원 산부인과부산백병원 산부인과
R1 R1 손영실손영실

2/23
INDEX
1. Periodic Fetal Heart Rate1. Periodic Fetal Heart Rate
2. Amnioinfusion2. Amnioinfusion
3. Second-stage Labor FHR Patterns3. Second-stage Labor FHR Patterns
4. Fetal Scalp Blood Sampling4. Fetal Scalp Blood Sampling
5. Complications From Electronic Fetal5. Complications From Electronic Fetal
MonitoringMonitoring

3/23
- Deviations from baseline that are related to - Deviations from baseline that are related to uterineuterine
contractionscontractions
① ① AccelerationAcceleration
- increase in FHR above baseline- increase in FHR above baseline
② ② DecelerationDeceleration
- decrease below baseline rate- decrease below baseline rate
- early, late or variable type- early, late or variable type
- the waveform of these deceleration is also - the waveform of these deceleration is also significantsignificant
for pattern recognitionfor pattern recognition
PERIODIC FETAL HEART RATE

4/23
- slope of FHR change- slope of FHR change
early and late decelerationearly and late deceleration
⇒ ⇒ gradual, resulting in a curvilinear and uniformgradual, resulting in a curvilinear and uniform
or symmetrical waveformor symmetrical waveform
variable decelerationvariable deceleration
⇒ ⇒ abrupt and erratic, giving the waveform a jaggedabrupt and erratic, giving the waveform a jagged
appearanceappearance
◎ ◎ Another system (based on the pathophysiological cause)Another system (based on the pathophysiological cause)
• • type Ⅰ : early type ⇒ head compressiontype Ⅰ : early type ⇒ head compression
• • type Ⅱ : late type ⇒ uteroplacental insufficiencytype Ⅱ : late type ⇒ uteroplacental insufficiency
• • type Ⅲ : variable type ⇒ cord compression patterntype Ⅲ : variable type ⇒ cord compression pattern
PERIODIC FETAL HEART RATE

5/23
1) Acceleration1) Acceleration - abrupt increase (defined as onset of acceleration to a - abrupt increase (defined as onset of acceleration to a peak in <30 seconds) in FHR baselinepeak in <30 seconds) in FHR baseline - occur most commonly antepartum, in early labor,- occur most commonly antepartum, in early labor, and in association with variable decelerationsand in association with variable decelerations - proposed mechanisms- proposed mechanisms • • fetal movementfetal movement • • stimulation by uterine contractionstimulation by uterine contraction • • umbilical cord occlusionumbilical cord occlusion • • fetal stimulation during pelvic examfetal stimulation during pelvic exam • • fetal scalp blood sampling & acoustic stimulationfetal scalp blood sampling & acoustic stimulation - can occur during labor without any apparent stimulus- can occur during labor without any apparent stimulus
PERIODIC FETAL HEART RATE

6/23
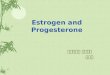
2) Early deceleration2) Early deceleration - gradual decrease and return to baseline associated with - gradual decrease and return to baseline associated with a contractiona contraction
• • drop in a heart rate withdrop in a heart rate with uterine contractionsuterine contractions • • related to cervicalrelated to cervical dilatationdilatation • • physiologicalphysiological
- generally seen in active labor between 4~7 cm dilatation- generally seen in active labor between 4~7 cm dilatation
PERIODIC FETAL HEART RATE
Features of early fetal heart rate deceleration. Characteristics include gradual decrease in the heart rate with both onset and recovery coincident with the onset and recovery of the contraction. The nadir of the deceleration is 30 seconds or more after the onset of the deceleration.

7/23
- not associated with fetal hypoxia, acidemia,- not associated with fetal hypoxia, acidemia, or low Apgar scoresor low Apgar scores - head compression probably cause vagal nerve activation- head compression probably cause vagal nerve activation due to dural stimulationdue to dural stimulation ⇒ ⇒ mediate HR decelerationmediate HR deceleration
PERIODIC FETAL HEART RATE

8/23
3) Late deceleration3) Late deceleration - FHR response to uterine contractions- FHR response to uterine contractions : an index of either uterine perfusion or placental: an index of either uterine perfusion or placental perfusionperfusion - a smooth, gradual symmetrical decrease in FHR- a smooth, gradual symmetrical decrease in FHR beginning at or after the peak of the contraction andbeginning at or after the peak of the contraction and returning to baseline only after the contraction has endedreturning to baseline only after the contraction has ended - the magnitude is rarely more than 30~40 bpm below- the magnitude is rarely more than 30~40 bpm below baseline and typically not more than 10~20 bpm inbaseline and typically not more than 10~20 bpm in intensityintensity - usually not accompanied by acceleration- usually not accompanied by acceleration - maternal hypotension (m/c), excessive uterine activity,- maternal hypotension (m/c), excessive uterine activity, or placental dysfunctionor placental dysfunction ⇒ ⇒ induce late decelerationinduce late deceleration
PERIODIC FETAL HEART RATE

9/23
PERIODIC FETAL HEART RATE

10/23
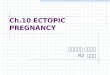
4) Variable deceleration4) Variable deceleration - most common deceleration pattern encountered during- most common deceleration pattern encountered during labor (d/t umbilical cord occlusion)labor (d/t umbilical cord occlusion) • • labor progressed to 5cm dilatation ⇒ 40%labor progressed to 5cm dilatation ⇒ 40% • • the end of 1st stage ⇒ 83%the end of 1st stage ⇒ 83%
PERIODIC FETAL HEART RATE
Features of variable fetal heart rate decelerations. Characteristics include abrupt decrease in the heart rate with onset commonly varying with successive contractions. The decelerations measure ≥ 15 bpm for 15 seconds or longer with an onset to nadir phase of less than 30 seconds. Total duration is less than 2 minutes.

11/23
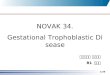
◎ ◎ two type of variable decelerationtwo type of variable deceleration
• • A : seen with complete umbilical cord A : seen with complete umbilical cord occlusionocclusion
• • B : different configuration because of the B : different configuration because of the “shoulders”“shoulders”
of acceleration before and after the of acceleration before and after the decelerationdeceleration
componentcomponent - the variation of variable decelerations was - the variation of variable decelerations was
caused bycaused by differing degrees of partial cord occlusiondiffering degrees of partial cord occlusion
PERIODIC FETAL HEART RATE
Varying (variable) fetal heart rate decelerations. Deceleration B exhibits “shoulders” of acceleration compared with deceleration A.

12/23
◎ ◎ physiological schemephysiological scheme ① ① only vein occlusiononly vein occlusion ⇒ ⇒ reduce fetal blood returnreduce fetal blood return ⇒ ⇒ triggering a baroreceptortriggering a baroreceptor -mediated acceleration-mediated acceleration ② ② subsequent completesubsequent complete occlusionocclusion ⇒ ⇒ umbilical artery flowumbilical artery flow obstructionobstruction ⇒ ⇒ result in fetal systemicresult in fetal systemic hypertensionhypertension ⇒ ⇒ baroreceptor-mediatedbaroreceptor-mediated decelerationdeceleration
PERIODIC FETAL HEART RATE

13/23
◎ ◎ significant variable decelerationsignificant variable deceleration decreasing to less than 70 bpmdecreasing to less than 70 bpm lasting more than 60 secondslasting more than 60 seconds ⇒ ⇒ pathologicalpathological ◎ ◎ saltatory baseline HRsaltatory baseline HR - rapidly recurring couplets of- rapidly recurring couplets of acceleration and decelerationacceleration and deceleration causing relatively largecausing relatively large oscillations of baseline FHRoscillations of baseline FHR - related to cord occlusion- related to cord occlusion - in the absence of other FHR- in the absence of other FHR finding, these do not signalfinding, these do not signal fetal compromisefetal compromise
PERIODIC FETAL HEART RATE

14/23
5) Prolonged deceleration5) Prolonged deceleration - isolated decelerations lasting 2 minutes or longer- isolated decelerations lasting 2 minutes or longer - but less than 10 minutes from onset to return- but less than 10 minutes from onset to return - difficult to interpret (d/t many different clinical situations)- difficult to interpret (d/t many different clinical situations) - more common cause- more common cause ① ① cervical examcervical exam ② ② uterine hyperactivityuterine hyperactivity ③ ③ cord entrapmentcord entrapment ④ ④ maternal supine hypotensionmaternal supine hypotension - others- others : epidural, spinal analgesia, maternal hypoperfusion or: epidural, spinal analgesia, maternal hypoperfusion or hypoxia, placental abruption, umbilical knots orhypoxia, placental abruption, umbilical knots or prolapse, maternal seizure, impending birth, maternalprolapse, maternal seizure, impending birth, maternal valsalva maneuvervalsalva maneuver
PERIODIC FETAL HEART RATE

15/23
- fetus may die during prolonged deceleration- fetus may die during prolonged deceleration
- thus, management can be extremely tenuous- thus, management can be extremely tenuous
PERIODIC FETAL HEART RATE

16/23
◎ ◎ infused saline through the intrauterine pressure catheter ininfused saline through the intrauterine pressure catheter in laboring women who had either variable decelerations orlaboring women who had either variable decelerations or prolonged deceleration attributed to cord entrapmentprolonged deceleration attributed to cord entrapment ⇒ ⇒ such therapy improved the heart rate pattern in halfsuch therapy improved the heart rate pattern in half ◎ ◎ clinical areas of transvaginal amnioinfusionclinical areas of transvaginal amnioinfusion ① ① treatment of variable or prolonged decelerationstreatment of variable or prolonged decelerations ② ② prophylactically in cases of known oligohydramnios, asprophylactically in cases of known oligohydramnios, as with prolonged rupture of membraneswith prolonged rupture of membranes ③ ③ in an attempt to dilute or wash out thick meconiumin an attempt to dilute or wash out thick meconium ◎ ◎ protocolprotocol - 500~800 ml bolus warmed normal saline followed by a- 500~800 ml bolus warmed normal saline followed by a continuous infusion of approximately 3 ml/hrcontinuous infusion of approximately 3 ml/hr
AMNIOINFUSION

17/23
AMNIOINFUSION
ComplicationComplication
Centers Centers ReportingReporting
No. (%)No. (%) Uterine hypertonusUterine hypertonus 27 (14)27 (14) Abnormal fetal heart rate tracingAbnormal fetal heart rate tracing 17 (9)17 (9) AmnionitisAmnionitis 7 (4)7 (4) Cord prolapseCord prolapse 5 (2)5 (2) Uterine ruptureUterine rupture 4 (2)4 (2) Maternal cardiac or respiratory Maternal cardiac or respiratory compromisecompromise 3 (2)3 (2)
Placental abruptionPlacental abruption 2 (1)2 (1) Maternal deathMaternal death 2 (1)2 (1)
[ Complications Associated with Amnioinfusion from a Survey of 186 Obstetrical Centers ][ Complications Associated with Amnioinfusion from a Survey of 186 Obstetrical Centers ]

18/23
◎ ◎ only 1.4% of over 7,000 deliveries did not have FHRonly 1.4% of over 7,000 deliveries did not have FHR
deceleration during 2nd stage labordeceleration during 2nd stage labor
(by Melchior & Bernard, 1985)(by Melchior & Bernard, 1985)
◎ ◎ both cord compression and fetal head compression haveboth cord compression and fetal head compression have
been implicated to cause decelerations and bradycardiabeen implicated to cause decelerations and bradycardia
during 2nd stage laborduring 2nd stage labor
◎ ◎ loss of beat-to-beat variability and baseline FHR less thanloss of beat-to-beat variability and baseline FHR less than
90 bpm were predictive of fetal acidemia90 bpm were predictive of fetal acidemia
SECOND-STAGE LABOR FHR PATTERNS

19/23
◎ ◎ measurement of the pH in capillary scalp bloodmeasurement of the pH in capillary scalp blood ⇒ ⇒ help to identify the fetus in serious distresshelp to identify the fetus in serious distress ◎ ◎ procedureprocedure ① ① an illuminated endoscope is inserted through the dilatedan illuminated endoscope is inserted through the dilated cervix after ruptured membranes so as to press firmlycervix after ruptured membranes so as to press firmly against the fetal scalpagainst the fetal scalp ② ② skin is wiped clean with a cotton swab and coated withskin is wiped clean with a cotton swab and coated with a silicon gela silicon gel ③ ③ an incision is made through the skin to a 2mm depth withan incision is made through the skin to a 2mm depth with a special blade on a long handlea special blade on a long handle ④ ④ as a drop of blood forms on the surface, it isas a drop of blood forms on the surface, it is immediately collected into a heparinized glass capillaryimmediately collected into a heparinized glass capillary tube, and the pH of the blood is promptly measuredtube, and the pH of the blood is promptly measured
FETAL SCALP BLOOD SAMPLING

20/23
◎ ◎ protocol to try to confirm fetal distressprotocol to try to confirm fetal distress
① ① pH > 7.25pH > 7.25
⇒ ⇒ labor is observedlabor is observed
② ② 7.20 < pH < 7.257.20 < pH < 7.25
⇒ ⇒ the pH measurement is repeated within 30 the pH measurement is repeated within 30 minutesminutes
③ ③ pH < 7.20pH < 7.20
⇒ ⇒ another scalp blood sample is collectedanother scalp blood sample is collected
immediatelyimmediately
mother is taken to an operating room mother is taken to an operating room and preparedand prepared
for surgeryfor surgery
delivery is performed promptly if the low delivery is performed promptly if the low pH ispH is
confirmedconfirmed
FETAL SCALP BLOOD SAMPLING

21/23
FETAL SCALP BLOOD SAMPLING

22/23
① ① injury to the fetal scalp or breech by the injury to the fetal scalp or breech by the electrodeelectrode
- rarely a major problem- rarely a major problem
- the eye in case of face presentation ⇒ serious- the eye in case of face presentation ⇒ serious
② ② fetal vessel in placenta may be ruptured by fetal vessel in placenta may be ruptured by cathetercatheter
③ ③ penetration of the placentapenetration of the placenta
④ ④ uterine perforationuterine perforation
⑤ ⑤ infectioninfection
COMPLICATIONS FROM ELECTRONIC FETAL MONITORING

23/23
감사합니다감사합니다 ..