-
8/11/2019 1.5 Neoplasia
1/9
`
Page 1 of 9
1 5 NEOPLASIA
P THOLOGY
NEOPLASIA New growth
It is defined as abnormal mass of tissue, the grow th of
which
exceeds and is uncoordinated with that of the normal tissue
and persists in the same manner after cessation of stimuli
w hich evoked the change Cancer- common term to all
malignancies
All neoplasms ultimately depends on the host for their
nutrition
and vascular supply.
Two basic components of Neoplasia:
1. Proliferating neoplastic cell-parenchyma
2. Supportive stroma- connective tissue and blood vessels.
INCIDENCE & MORTALITY DATA 10.1 Million new cases
6.2 Million deaths
22.4 Million living w ith Cancer year 2005
Increase of 19% in incidence
Increase of 18% in mortality since 1990
MOST COMMON CANCER CAUSING DEATHLung 17.8 %
Stomach 10.4 %Liver 8.8 %
MOST COMMON CANCER WORLDWIDELung Cancer 12.3 %
Breast CancerProstate Cancer
10.4 %
Colorectum 9.4 %
NOMENCLATUREParenchymaProliferating neoplastic cells
Stroma Connective tissue and blood vessels
Benign Tumors
suffix oma
Malignant Tumors
2 broad categories:
Carcinomas - epithelial cells
sarcomas - mesenchymal tissues
Some tumors w ith more than one parenchymal cell type: mixed
tumors & teratomas
Two non-neoplastic lesions bear the names that are
deceptively similar to tumors: choristomas& hamartomas
CLASSIFICATION OF NEOPLASMSA. Site
B. Biologic Behaviorbenign, borderline, malignant
C. Cell ( tissue of origin )
D. Embryologic derivation
E. Diff erentiation potential of cell of origintotipotent cellF.
Etiology
Tumors are classified to 2 broad categories: benign and
malignant.
BENIGN MALIGNANTSlow grow ing Rapidly grow ingEncapsulated Not
encapsulated
No infiltration/Expansile grow th Infiltrative grow thNo
metastas is Metastas is
Well diff erentiated Well-poorly diff erentiatedHigh patient
survival after
successful surgical removalPoor patient survival rate;
tendency for local and distantrecurrence
BENIGN MALIGNANT
GROSS FEATURESSmooth surface with a fibroticcapsule; compress
surroundingtissue
Irregular surface withoutencapsulation; destruction
tosurrounding tissue
Slow rate of growth Rapid rate of grow thRarely fatal Usually
fatalSmall to large Small to large
MICROSCOPICGrowth by compression Growth by invasionHighly diff
erentiated Well or poorly diff erentiatedCell similar to normal
andresembling to one another
-Cytologic abnormalities(Pleiomorphism)- Anaplasia
(MorphologicHALLMARK of malignancy)
No mitosis With mitosisWell formed blood vessel Poorly formed
and numerous
blood vessel(-) Necrosis/Hemorrhage(-) Metastasis
(+) Necrosis & Hemorrhage(+) Metastasis
INVESTIGATIVE TECHNIQUEDNA content usually normal DNA content of
cells usually
increasedKaryotype normal Aneuploidy
PolyploidyClonal GeneticAbnormality
Fig1. Comparison of Leiomyoma & Leiomyosarcoma
Fig 2. Choristoma: Ectopic rest of normal tissue
Fig 3 & 4. Hamartoma: mass of disorganized but mature
specialized cells or tissue native to the particular s ite
BENIGN TUMORS
Cell of origin + OMA
AdenomaBenign tumor arising from glandular cells
LeiomyomaBenign tumor arising from smooth muscle cells
ChrondromaBenign tumor arising from chondrocytes
Papilloma Has finger-like projections
PolypProjects upw ard, forming a lump
CystadenomaHas hollow spaces (cysts) inside
Fig 5 & 6. Tubular adenoma, colon
-
8/11/2019 1.5 Neoplasia
2/9
Page 2 of 9
1 5 NEOPLASIA
Pathology
Fig 7. Papillomas: architecture finger like projections
Fig 8 & 9. Polyp: macroscopic projection of mucosal
surfaceMALIGNANT NEOPLASMS
Malignant tumors: Differentiation and anaplasia Dysplasia Rapid
rate of grow th Widespread invasion Metastases
Carcinomasarise in epithelial tissue Adenocarcinomamalignant
tumor of glandular cells Squamous cell carcinomamalignant tumor
of
squamous cells Sarcomasarise in mesenchymal tissue
ChrondrosarcomaMalignant tumor ofchondrocytes
AngiosarcomaMalignant tumor of blood vessels
RhabdomyosarcomaMalignant tumor of skeletal
muscle cellsANAPLASIA
Lack of differentiation Hallmark of malignant transformation
Numerous morphologic changes
Fig 10. Pleomorphism: variation in size and shape
Fig 11. Abnormal nuclear morphology: hyperchormatic
(abundant DNA), increased N:C ratio (normal 1:4- 1:6)
Fig 12. Mitoses: Increased, bizarre
Fig 13. Loss of polarity
Fig 14. Tumor giant cells
Fig 15 & 16. Dysplasia : Disordered grow thCELL (TISSUE OF
ORIGIN)
I. Composed of One Parenchymal Cell type:
A. EpithelialB. Mesenchymal
II. More than one Neoplastic Cell Type derived from one germ
layer:A. Salivary GlandB. BreastC. Renal Anlage
III. More than one Neoplastic Cell Type derived from more than
one germlayer: Teratoma
TISSUE OF ORIGIN BENIGN MALIGNANTMesenchymal/
connective tissueFibromaLipoma
ChondromaOsteoma
FibrosarcomaLiposarcoma
ChondrosarcomaOsteogenic sarcoma
Endothelial & relaxedtissue
HemangiomaLymphangioma
Meningioma
AngiosarcomaLymphangiosarcoma
Synovial sarcomaMesotheliomaInvasive meningioma
Hematopoietic LeukemiasLymphoma
Muscle LeiomyomaRhabdomyoma
LeiomyosarcomaRhabdomyosarcoma
Epithelial Squamous papillomaAdenomaPapilloma
CystadenomaBronchial adenoma
Renal tubularadenoma
Liver cell adenomaTransititonal cell
papillomaHydatiform mole
SCC or epidermoidCABCC
AdenocarcinomaPapillary carcinoma
CystadenocarcinomaBronchogenic
carcinomaRenal cell carc inoma
Transitional cellcarcinoma
ChoriocarcinomaSeminoma
Embryonal CAMelanocytes Nevus Malignant Melanoma
MIXED TUMOR Mixed tumors show divergent differentiation
Examples
o Pleiomorphic adenomaglands + f ibromyoid stroma Teratomas
-
8/11/2019 1.5 Neoplasia
3/9
Page 3 of 9
1 5 NEOPLASIA
Pathology
MORE THAN ONE NEOPLASTIC CELL MIXEDSalivary gland
Pleomorphic
AdenomaMalignant mixedtumor of salivarygland origin
Renal Wilms tumorTERATOGENOUS (FROM MORE THAN ONE GERM CELL
LAYER)Totipotential cells Mature
teratoma/dermoid cystImmature tertoma,teratocarcinoma
CONFUSING TERMS Malignant tumors that sound benign
o Lymphomao Mesotheliomao Melanomao Seminoma
Non tumors that sound like tumorso Hamartoma mass of
disorganized indigenous
tissueo ChoristomaHeterotopic rest of cells
Names that seem to come out of now hereo Nevuso Leukemiao
Hyatidiform mole
BORDERLINE TUMORS Variable grow th rate Locally infiltrative Low
or no metastatic potential Intermediate patient survival rate;
tendency for local recurrence
after successful surgical removal INTACT BASEMENT MEMBRANE
PRE-MALIGNANT (PRE CANCEROUS) LESIONSA. Hyperplasia
-Endometrial Hyperplasia-Lobular and Ductal
Hyperplasia-Cirrhosis of the liver
B. DysplasiaC. Metaplasia
-Barrets EsophagusD. Inflammatory Lesions
-Ulcerative Colitis, Atrophic Gastritis-Autoimmune (Hashimotos)
Thyroiditis
E. Benign neoplasms- Colonic Adenoma
MECHANISMS & CAUSES OF NEOPLASIA At MOLECULAR LEVEL ,
neoplasia is defined as disorder of grow th
regulatory genes ( proto-oncogenes and tumor suppressor genes ).
Origin of Neoplasia: Monoclonal Origin Field Origin MONOCLONAL
THEORY- The initial neoplastic change aff ects a single cell, w
hich then
multiplies and give r ise to neoplasm. FIELD THEORY- A
carcinogenic agent acting on a large number of s imilar cells
mayproduce a filed potentially neoplas tic cells. Then neoplasms
may then
arise from one or more cells within this field.MOLECULAR BASIS
OF CANCER Inherited cancer syndrome, usually involving germ-line
mutation in
tumor suppressor or DNA repair genes, accounts f or 4 % of
allCancer
Genetic susceptibility significantly alter the risk from
environmentalexposures
Fundamental Principles: Non-lethal genetic damage lies at the
heart of carc inogenesis. A tumor is formed by the clonal expansion
of a single precursor
cell that has incurred genetic damage. Carcinogenesis is a
multistep process hence multiple
mutations. The 7 key changes are the ff : (Essentials for
malignant
transformation) Self-suf ficiency in growth signals
Insensitivity to grow th inhibitory signals
Evasion of apoptosis Limitless replicative potential Sustained
angiogenesis Ability to invade and metastas ize
Defects in DNA repair
Fig 17. Events in neoplastic transformation Oncogenes and
Cancer
Oncogenes Proto-oncogenes
Protein products of Oncogenes Activation of Oncogenes
Point mutations Chromosomal rearrangements Gene
amplifications
Oncogenes are genes capable of causing cancer. The genes are
activated by mutation, amplification, or
translocation. Activation can lead to the loss of
normalregulation and differentiation, increased proliferation.
Activationis the functional concept whereby the normal
action of grow th regulation is diverted into oncogenesis.
Mechanisms of Occurrence:
1. Mutation
2. Translocation
3. Insertion
MOLECULAR BASIS OF NEOPLASIA Basic unde rlying cause of
cancer:
DISORDER IN THE GROWTH REGULATORY GENE Four kinds of normal
genes are damaged:
1. Genes that promote grow th (protooncogenes)2. Genes that
inhibit grow th (tumor-suppressor genes)
3. Genes that regulate apoptosis4. Genes involved in DNA
repair
Cancers develop in multiple steps
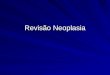
Fig.18 Transformation of NeoplasiaHALLMARKS OF CANCER
Fig. 19. Hallmarks of Cancer
-
8/11/2019 1.5 Neoplasia
4/9
Page 4 of 9
1 5 NEOPLASIA
Pathology
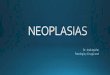
GROWTH FACTOR SIGNALING PATHWAYS IN CANCER
Fig 20. Growth Factor Signaling pathways in Cancer
Fig 21. Escape from senescence and mitotic catastropheSELF
RENEWING CAPACITY IN CANCER CELLS
PATHOGENESIS IN RETINOBLASTOMA
Fig 22.Retinoblastoma PathogenesisEVASION OF IMMUNE
SURVEILLANCE
Different classes of tumor antigens are products of:1. Mutated
proto-oncogenes2. Tumor suppressor genes3. Overexpressed or
aberrantly expressed proteins4. Tumor antigens produced by
oncogenic viruses5. Oncofetal antigens6. Altered glycolipids and
glycoproteins7. Cell types specific diff erentiation antigens
Tumors may avoid the immune system by:1. Selective outgrow th of
antigennegative variants2. Loss or reduced expression of
histocompatibility antigens3. Immunosuppression mediated by
expression of certain factors
(ex. TGF-B, PD-1 ligand, galectins) by the tumor cells.
HOST DEFENSE AGAINST TUMOR IMMUNITY
Fig 23. Tumor antigens recognized by CD8+ T cells
Fig.24. Mechanisms by w hich tumors evade the immune
system.GENETIC LESIONS IN CANCER
Oncogenic mutations, including point mutations and
othernonrandom chromosomal abnormalities, such astranslocations,
deletions, and gene amplifications.
Balanced translocations. Deletions Gene amplification Numerous
cryptic(subcytogenetic) rearrangements.
TUMOR EVOLUTION
Fig 25.
-
8/11/2019 1.5 Neoplasia
5/9
Page 5 of 9
1 5 NEOPLASIA
Pathology
MOLECULAR MODEL FOR CANCER EVOLUTION
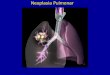
Fig 26. Molecular model for the evolution of colorectal
cancersthrough the adenoma-carcinoma sequence.
Each cancer must result from the accumulation of
multiplemutations.
CARCINOGENIC AGENTS AND THEIR CELLULAR INTERACTIONS Steps
involved in Chemical Carcinogenesis
1. Initiation results from exposure of cells to a suff icient
dose of acarcinogenic agent. (initiator)
2. Initiation causes permanent DNA damage. (mutations)3.
Promoters can induce tumors in initiated cells, but they are
non
tumorigenic by themselves.CHEMICAL CARCINOGENESIS
Chemical carc inogens have highly reactive electrophile
groupsthat directly damage DNA, leading to mutations and
eventuallycancer.
Direct acting agents do not require metabolic conversion
tobecome carcinogenic.
Indirect-acting agents arent active until converted to
anultimate carcinogen by endogenous metabolic pathways.
DEVELOPMENT OF A CANCER
Fig 27. Tumor progression and generation of
heterogeneity.CARCINOGENIC AGENTS AND THEIR CELLULAR INTERACTIONS
Radiation Carcinogenesis
o UV rayso Ionizing radiation
Microbial Carcinogenesiso Onconegenic RNA viruses
Human T cell Leukemia Virus Type Io Onconegenic DNA viruses
Human papilloma virus Epstein Barr virus Hepatitis B & C
virus
Bacterial Carcinogenesiso Helicobacter pylori
RADIATION CARCINOGENESIS Ionizing radiation causes chromosome
breakage,
translocations, band, less frequently, point mutations,
leadingtobgenetic damage and carcinogenesis. (X-rays, gamma
rays,alpha, beta, positrons, protons, neutrons and primary
cosmicradiation)
UV rays induce formation of pyrimidine dimers w ithin DNA,
leading to mutations.GENES CANCER GENES
Autonomous grow th Insensitivity to grow th-inhibitory signals
Evasion of apoptosis Limitless replication Sustained angiogenesis
Invasion and metastasis
PROTO-ONCOGENES (CELLULAR ONCOGENES) Code for a variety of
growth factors, receptors, and signal-relay
or transcr iption factors which act in concert to control entry
intothe cell cycle.
PROTO-ONCOGENES code for a number of protein products(grow th
factors, kinases, etc). The expression is w ell controlled,playing
a role in normal grow th and development.
o Normal cellular genes w hose products promote
cellproliferation.
Ras- proto-oncogene: a G protein defect. SRC proto-oncogene:
tyrosine kinase deficiency.
Sis proto-oncogene: platelet derived grow th factor
receptordefect.
Erb B proto-oncogene- epidermal grow th factor receptor defect.
Myc (c-myc, n-myc, l-myc) proto-oncogenes- nuclear factors.
HER-2/neu over expression in 15-30% of pts w ith breast
cancer. LiFraumeni syndrome: defect in p53 gene. Patients
get
childhood sarcomas, breast cancer, brain tumors,
leukemia,adrenal cancer.
Medullary thyroid cancer: associated with Ret proto-oncogeneon
chr 10. Patients w ith Ret oncogene defect plus familyhistory- 90%
get medullary cancer of thyroid, need totalthyroidectomy.
MENIN a product of MEN1 gene also associated withmedullary
cancer of thyroid.
ONCOPROTEIN: A protein encoded by an oncogene that
drives increased cell proliferation through one of
severalmechanisms. ONCOGENES: Mutated or overexpressed versions of
proto-
oncogenes that function autonomously.ONCOGENES, THEIR MOA &
ASSOCIATED HUMAN TUMORS
CATEGORY PROTOCONCOGENES MECHANISM A.TUMORGrowth factors
PDGF- chain sis Ov erexpression Astrocy toma
Growth Factor Receptors
EGF-receptorfamily
erb-B1 Ov erexpression Squamouscell CA ofthe lungs
Proteins involved in Signal Transduction pathway
GTP-binding ras Pt mutations CA
ofLung,colon,pancreas;manyleukemias
Nuclear Regulatory proteins
Transcriptionalactivators
myc Translocation Burkittlymphoma
Cell Cycle Regulators
Cyclins cyclin D Translocation Mantle celllymphoma
TUMOR SUPPRESOR GENES (ANTI ONCOGENES)Which serve to dow
n-regulate the cell cycle.
Note: a net increase in the production of s timulatory
(promoter) factors , adecrease in inhibitory (suppressor) growth
factors may lead touncontrolled cell grow th.
Cancer-Suppressor Genes Protein Products of Tumor Suppressor
Genes
Gene amplifications p53 BRCA-1 and BRCA-2 APC gene NF-1 gene
cell surface receptors WT-1
Genes That Regulate Apoptos is bcl-2
Genes That Regulate DNA Repair hMSH2 and hMLH1
Molecular Basis of Multistep Carcinogenesis gatekeeper genes-
APC, NF-1, and Rb caretaker genes- DNA repair genes
Retinoblastoma (RB1)- chr 13: involved in cell cycle. P53- chr
17: involved in cell cycle (normal gene induces cell
cyc le arrest and apoptosis, abnormal gene allows
unrestrainedcell grow th.
APC- chr 5; involved w ith cell adhesion and
cytoskeletonfunction.
-
8/11/2019 1.5 Neoplasia
6/9
Page 6 of 9
1 5 NEOPLASIA
Pathology
BRCA I and IIRB
Governor the cell cyc le When hypophosphorylated, RB exerts
antiproliferative Normal grow th factor signaling leads to RB
hyperphosphorylation and inactivation.1. Loss of function
mutations aff ecting RB2. Gene amplifications of CDK4 and cyclin 0
genes3. Loss of cyclin-dependent kinase inhibitors (p16/INK4a)4.
Viral oncoproteins that bind and inhibit RB (E7 protein of
HPV)P53
Guardian of the genome The p53 protein is the central monitor of
stress in the cell. Involved in cell cycle arres t, DNA repair,
cellular senescence
and apoptosis. Kinases phosphorylate p53, liberating it from
inhibitors causing
cell-cycle arrest at the G1-S checkpoint. This pause allows
cells to repair DNA damage. The majority of human cancers
demonstrates biallelic loss of
function mutations in TP53.
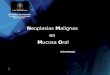
Fig 28. Role of p53 in maintaining the integrity of the
genome.KARYOTYPIC CHANGES IN TUMOR CELLS
Three types of nonrandom chromosomal abnormalities have
beendescribed:
(1) translocation (2) deletions (3) amplification
CYTOGENETIC ABNORMALITIES IN HUMAN NEOPLASMSTUMOR
CYTOGENETIC
ABNORMALITYEFFECTS
Chronic myeloidleukemia
Translocationbetw een chromosome9 & 22 (Philadelphia
chromosome)
Forms a protein w ithtyrosine kinaseactivity (bcr-abi
protein)Follicular lymphoma Translocation
betweenchoromosome 14 &
18
Production of protein
that prevents celldeath (bcl 2 product)
Neuroblastoma Homogenous regionsand double minute
chromosomes
Amplification of n-mycin poor prognosis type
Ew ings tumor Translocationbetw een chromosome
11 & 22
Uncertain
CHARACTERIZED HERITABLE NEOPLASIA SYNDROMESYNDROME TUMOR CAUSED
DEFECT
MEN syndrome Multiple tumor inendocrine organs
Mutations onchromosomes 10 &11
Polyposis coli Adenomata and
carcinomas of thecolon
Absnt tumor
suppressor gene
Li-Fraumeni Breast cancer andsarcomas
Mutated tumorsuppressor gene
XerodermaPigmentosum
Skin cancer Abnormal DNA repair
Familialretinoblastoma
Malignant tumor of theretina
Absent tumorsuppressor gene
NeurofibromatosisType I
Benign and malignanttumors of peripheralnerves
Abnormal tumorsuppressor gene
Neoplasia Associated with Constant Genetic Abnormality:a.
Philadelphia Chromosome- CMLb. Retinoblastoma-Rb genec. Wilms
Tumor-WT-1d. Familial Polyposis Coli-APC
There is increasing recognition of the causative role of li
festyle
factors, including diet, physical activity and
alcoholconsumption.
The most important human carcinogens include tobacco,asbestos,
aflatoxins and ultraviolet light.
TOBACCO SMOKING Accounts for 30 % of all malignant tumors 25 %
of all Cancers in Men 4 % of all Cancers in Women 16 % both, in w
ell developed countries 10 % in less developed countries
ALCOHOL Accounts for 3 % of all cancers 4% of Cancer in Men 2%
of Cancer in Women Analytical epidemiological studies of cohort and
case-control
type conducted, the causal association of drinking alcohol
has
been established in oral, esophageal and liver cancer Risk for
cancer is a linear function of the level of consumption,
up to an intake of about 80 g/day.OCCUPATIONAL EXPOSURE
20 % - proportion of cancer attributable to
occupationalcarcinogen exposure
4.5% - estimated proportion of Cancer in developed countries
Lung Cancer is the most frequent
ENVIRONMENTAL EXPOSURE 1-4% of all Cancer are attributed to
pollution of air, soil and
w ater Asbestos is one of the best characterized cause Less than
5 %, a small proportion of Lung Cancer is attributed
to air pollutionCHRONIC INFECTION
Infections agents are one of the main causes of cancer
accounting for 18 %(1.6 million) of cases worldwide
Approximately 9 million new cases of Cancer attributed to
infectious agents 23 % in developing countries 9 % in developed
countries EBV
- 65% for Burkitts Lymphoma and Nasopharyngeal CA Hepatitis B
virus
-60% of cases of Primary Liver CA w orldwide-67 % in developing
countries
Hepatitis C virus-25 % of cases of Liver CA
HPV- 80 % of Cervical CA- 35 % of Cancers of the Vulva, Vagina,
Penis & Anus
BIOLOGY OF TUMOR GROWTH
Kinetics of Tumor Cell Growth variables influence tumor cell
grow th:
doubling time of tumor cells grow th fraction cell production
and loss
Tumor Angiogenesis 2 most important tumor angiogenic factors
are:
vascula r endo thelial growth factor(VEGF)
basic fi broblast gr owth factor (bFGF). Tumor Progression and
Heterogeneity Me chanisms of Invasion and Metastasis
Invasion of Extracellular Matrix Detachment of tumor cells
attachment to matrix components degradation of extracellular matrix
Migration of tumor cells
Vascular Dissemination and Homing of Tumor Cells
METASTASIS Establishment of a second neoplastic mass thru
transfer of
neoplastic cells from the first neoplasm to a secondary
locationseparate from the original tumor
Tumor not contiguous to its primary site. Definitive proof of
malignancy1. Lymphatic Spread: Occurs early in carc inomas and
melanomas but is an unusual
occurrence in most sarcomas. Malignant cells are carried by the
lymphatics to the regional
lymph nodesw here their advance may be temporarilyarres ted by
immune response.
-
8/11/2019 1.5 Neoplasia
7/9
Page 7 of 9
1 5 NEOPLASIA
Pathology
2. Hematogenous Spread:
Believed to occur during the early clinical course. Malignant
cells are destroyed by the immune system, but some
become ocated w ith fibrin and entrapped in the capillaries.
Metastasis occur only if enough cancer cells survive in the
tissue and proliferate. TAF ( tumor angiogenesis fac tor )3.
Direct Seeding or Metastasis via body cavities (pleura,
peritoneum, preicardium): Entry of malignant cells into the body
cavities may be followed
by dissemination of the cells elsew here.METASTATIC PROCESS
Ineff icient, multistep process called the metastatic cascade.
Detachment and invasion: pass in to lymphatic or venous
system. Transport: to a distant site of grow th. Has to survive
a bunch of
host defenses on the w ay. Arrest and extravasation: Stuck up in
target organ. Digestion of
BM to invade. Establishment of new growth.
METASTATIC CASCADE1. Primary tumor w ill undergo donal expansion
, grow th,
diversification
2. Metastatic subclone3. Adhes ion to and invasion of basement
membrane4. Intravasation5. Interaction w ith host lymphoid cells6.
Tumor cell rmbolus7. Adhes ion to basement membrane8.
Extravasation9. Metastatic deposit
Fig 29. Cellular events needed for metastasis
HOST DEFENSE AGAINST TUMORS
Fig 30. Main routes for tumor spread
Fig 31. Main sites of blood borne metastasis
CANCER SPREAD Supraclavicular: breast, lung, stomach (Virchows),
pancreas. Ax illary: lymphoma (#1), breast, melanoma.
Periumbilical: pancreas (SMJ node). Ovarian: stomach (Krukenberg
tumor), colon. Bone mets: Breast (#1), prostate. Skin mets: breast,
melanoma.
CARCINOGENIC SITES Chemical Carcinogenesis
Initiation Promotion
Molecular Targets of Chemical Carcinogens DNA
Carcinogenic Chemicals alkylating agents, aromatic hydrocarbons,
azo dyes
etc
Radiation Carcinogenesis UV rays and ionizing radiations
Viral and Microbiological Carcinogenesis DNA Viruses
(1) HPV, Epstein-Barr virus (EBV) andHepatitis B virus (HBV)
RNA Oncogenic Viruses (HTLV-1)
VIRUSES IMPLICATED IN HUMAN NEOPLASIAVIRUS NEOPLASMEpsetin-barr
virus Burketts lymphoma
Nasopharyngeal carcinomaOther B cell lymphomas and somecases of
Hodgkins disease
Hepatitis B virus Hepatocellular carc inoma
Human papilloma virus Cervical carcinomaSome forms f carcinoma
of theskin
HTLV-I T-cell leukemia / lymphoma Immunosurveillance
Increased frequency of cancers in patientsw ith congenital or
acquiredimmunodeficiency
increased susceptibility to EBV infectionsand EBV-associated
lymphoma in boysw ith X-linked immunodeficiency
Tumors may escape immunosurveillance selective outgrowths of
antigen-negative
variants loss or reduced expression of
histocompatibility antigens tumor-induced immunosuppress ion
failure of sensitization apoptosis of cytotoxic T cells
CLINICAL FEATURES OF TUMORS Local and Hormonal Effects
related to location hormone production
Cancer Cachexia Paraneoplastic Syndromes
endocrinopathies Hypercalcemia Acanthosis nigricans clubbing of
fingers and hypertrophic osteoarthopy thr om boembolic
diatheses
-
8/11/2019 1.5 Neoplasia
8/9
Page 8 of 9
1 5 NEOPLASIA
Pathology
APPROACH TO CANCER DIAGNOSISI. Clinical SuspicionII. Screening
TestsIII. Tumor MarkersIV .Definitive Diagnosis
- tissue biopsy ( most accurate )1.Ordinary H and E stain2.
Immunohistochemistry3. Electron Microscopy
LABORATORY DIAGNOSIS OF CANCER Histologic and Cytologic Methods
Immunohistochemistry and flow cytometry Molecular diagnosis
Molecular prof ile of tumors Proteomics Fine-Needle Aspiration
Cytologic (Papinacolaou Smears) DNA Probe Analysis Tumor Markers
Assays of circulating tumor cells and of DNA
GRADING & STAGING OF TUMORS GradingDetermined by cytologic
appearance; based on the
idea that behavior and differentiation are related, w ith
poorly
differentiated tumors having more aggressive behavior. Grades I
to IV w ith increasing anaplasia Imperfect because
(1) the differentiated parts of the sametumor may display diff
erent degrees ofdifferentiation
(2) the grade of tumor may change as thetumor grows
StagingDetermined by surgical exploration or imaging, isbased on
size, local and regional lymph node spread, anddistant metastases;
of greater clinical value than grading.
anatomic extent of the tumor TNM
Information Provided by Pathologic Diagnosis:1. Type of Neoplasm
- name of the neoplasm2. Biologic Behavior- benign or malignant3.
Histologic Gradedegree of diff erentiation4. Degree of Invasion-
depth5. Staging - size of the mass/depth of involvement
- involvement of nodes- +/- metastasis
OTHER CLINICAL ASPECTS OF TUMORS CachexiaProgressive loss of
body fat and lean body mass,
accompanied by profound weakness, anorexia and anemia.
Paraneoplastic syndromesSymptom complexes in
individuals w ith cancer that cannot be explained by tumorspread
or release of hormones that are indigenous to the tumorcell of
origin.
PARANEOPLASTIC SYNDROMES Endocrinopathies (Cushing syndrome,
hypercalcemia) Neuropathic syndromes (polymyopathy, peripheral
neuropathies, neural degeneration, myasthenic syndrome) Skin
disorders (acanthosis nigricans)
Skeletal and joint abnormalities
(hypertrophicosteoarthritis)Hypercoagulability (migratory
thrombophlebitis,disseminated intravascular coagulation,
nonbacterialthrombotic endocarditis)
TREATMENT OF NEOPLASMSA. Benign
Surgical removalB. Malignant
- Surgery ( radical, w ide excision, palliative surgery )- Lymph
node removal- Palliative:
a. Chemotherapyb. Radiotherapyc. Immunotherapy
The goal of primary prevention is to avoid the development
ofCancer by reducing or el iminating exposure to
cancer-causingfactors and by frequent medical check-ups and
populationbased-screening programs
World Cancer Report
World Health Organization2003
IMPORTANT DEFINITION RELATED TO CANCER SCREENINGSCREENING
Testing people who have no symptoms and have not noticed
anyproblems suggestive of disease.
A particular screening test may be suggested for everyone or
onlyfor people with certain risk factors.
Ideally, a screening test would stage or be able to detect
cancerat an early before cancer has developed.
PREVENTION Removing the cause or risk for a certain type of
cancer. Prevention often consists of life-style changes like
quitting
smoking or using sunscreen properly Screening is not considered
prevention. Screening involves checking for cancer or cancerous
conditions in persons w ithout symptoms Screening for some
cancers is eff ective in detecting
precancerous cells or f inding cancer at an early stage w
hentreatment is more eff ective.
Screening procedures include visual exams, laboratory tests,or
procedures such as mammography or colonoscopy that testfor internal
cancers.
TUMOR MARKERS Secreted into the blood in measurable
concentration only after
the cells produce it had undergone malignant transformation.
Adjunct tow ards correct diagnosis. Marker for prognostic and risk
factors
QUALITY INDEX SENSITIVITY percentage of test results w hich are
correctly
positive in the presence of a tumor
SPECIFICITY percentage of healthy persons or persons withbenign
conditions in w hom the test correctly gives a negativeresult
* The signifi cance of the data on the diagnostic specificity
and sensitivityof a tumor marker is critically dependent upon tumor
stage and selectionof control groups
POINTERS IN USING TUMOR MARKERS1. Never rely on the result of a
s ingle test.2. When ordering serial testing, be certain to order
every test f romlaboratory using same assay kit.3. Be certain that
the tumor marker selected for monitoring recurrencew as elevated in
patient prior to surgery4. Consider the half-life of the tumor
marker w hen interpreting the result.5. Consider how the tumor
marker w as removed or metabolized f rom theblood circulation.6.
Consider order ing multiple tumor markers to improve both
thesensitivity and specificity of the diagnosis.7. Be aw are of the
presence of ectopic tumor marker. (AFP, Calcitonin,Chromogranin A
HCG, Thyroglobulin).8. Be aw are of the possibility of hook eff
ect.- Takes place w hen the assay tends to give a falsely low value
when
the tumor marker concentration in the specimen rises above a
certainhighly elevated concentration.
CARCINOEMBRYONIEC ANTIGEN (CEA) Glycoprotein Oncofetal antigen
produced during embryonic and fetal life Scarcely detectable in
normal adults (2.5-5 ng/ml) Found mostly in the gastrointestinal
tract and serum of fetus Small quantities in the intestinal,
pancreatic, and liver tissues of
healthy adultsALPHA-FETOPROTEIN (AFP)
Glycoprotein
Formed phys iologically in the yolk sac, fetal liver and fetal
GItract.
Hepatocellular carc inoma, germ cell tumors Maybe elevated in
breast, bronchial and colorectal carc inomas
CANCER ANTIGEN 19-9 (CA 19-9) Glycolipid Fetal stomach,
intestine and pancreas Reference range 37 U/ml Marker of choice for
pancreatic carcinoma
CANCER ANTIGEN 125 (CA 125) Differentiation antigen that arises
in fetal tissue from coelomic
epithelial derivatives. Applicable for ovarian neoplasms. Maybe
elevated in benign gynecologic tumors and
inflammation of adnexa.
NEURON SPECIFIC ENOLASE (NSE)
Glucose splitting enzyme identified in neurons of the brain
andperipheral nervous system.
Also found in neuroendocrine tissue and APUD cells. False
positive: hemolysis and delayed centrifugation of blood.
Neuroblastoma, Carcinoid
HUMAN CHORIONIC GONADOTROPIN (HCG) Glycoprotein Formed
physiologically in syncytiotrophoblast Diagnosing and monitoring
GTD. Monitoring germ cell tumor of the testis and ovaries
ESTROGEN RECEPTOR & PROGESTERONE ASSAY Used to identify
patients who are to benefit from endocrine
therapy. Indicate good prognosis, longer disease-f ree
survival
-
8/11/2019 1.5 Neoplasia
9/9
Page 9 of 9
1 5 NEOPLASIA
Pathology
55-60% patients are positive to eER or PR only 85% positive to
both.
WHAT ARE THE FINAL COMPLICATIONS OF MALIGNANCY(CAUSES OF
DEATH)
Pneumonia Cachexia Renal Failure Bleeding Severe anemia,
Thrombocytopenia Infections Hypercoagulability DIC Pain more of
devastating symptom than a complication. It has
to be controlled Multiple Organ Failure
END OF TRANS