-
7/31/2019 20456347 Git Physiology
1/95
PHYSIOLOGY OF THE GI TRACT
Peter C A Kam
-
7/31/2019 20456347 Git Physiology
2/95
FUNCTION OF THE GI TRACT
1. Ingestion Motility mechanical breakdown offood, propulsion of
food through gut
2. Digestion Secretion secretion of enzymes,water & ions
3. Absorption
Control of motility and secretion bynervous system and
hormones
4. Egestion
-
7/31/2019 20456347 Git Physiology
3/95
-
7/31/2019 20456347 Git Physiology
4/95
Properties of GI smooth muscle
5-10m
200mForm hollow tubes not contracting against skeletonForm a
syncitium electrically couple, joined by gap junction
contractions
synchronousActin:myosin ratio 15:1 (skeletal muscle
2:1)Contractile elements not arranged in sarcomeres not
striatedStimulated by neurotransmitter released from
varicositiesHave slow wave activity.
-
7/31/2019 20456347 Git Physiology
5/95
0
Me
Acetylcholine
M e m
b r a n e
P o
t e n t i a
l ( m V )
Tension
Tension
0
-60
0
-60
-
7/31/2019 20456347 Git Physiology
6/95
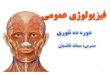
Slow waves in GI smooth muscle
Slow waves are changes in resting membrane potential IE 3-12
cycles per minute depending on area of GI tract 3/min in
stomach, 12/min small intestine. Always present but do not
always cause contractions. Frequency of contractions dictated by
frequency of slow waves. Slow wave frequency and height modulated
by body temp &
metabolic activityIntrinsic & extrinsic nerves (increased by
Ach, SP; decreased bynoradrenaline, No. VIP). Circulating hormones
(esp. CCK,motilin)
-
7/31/2019 20456347 Git Physiology
7/95
Myosin (PO 4)2
Calcium activates contraction
OUT Depends on influx of calciumfrom extracellular space
IN Ca 2 through calcium channels
Calcium-calmodulin complexactivates myosin light chainkinase
(Ca 2)4-CalmodulinContraction explained bysliding filament
theory
Inactive myosin Active myosin lightlight chain kinase chain
kinase
MUSCLECONTRACTION
Contraction of GI smooth muscle
-
7/31/2019 20456347 Git Physiology
8/95
Innervation of the GI tract
2. Extrinsic nervesParasympathetic innervation
- Via preganglionic fibres in vagus and pelvic nerves- Synapse
on ganglionic neurons in enteric nervous system- Excitatory through
release of acetylcholine
Parasympathetic nervous system- Postganglionic fibres from
coeliac, superior and inferior
mesenteric system.- Inhibitory through release of
noradrenaline
-
7/31/2019 20456347 Git Physiology
9/95
Parasympathetic n.s. Sympathetic n.s.
Vagal nuclei CNSPreganglionic Fibres
Preganglionic fibres
Sacral spinal Sympathetic
cord gangliaPostganglionic fibres
Enteric nervous SystemMyenteric Submucosal
plexus plexus
Smooth Secretory Endocrine BloodMuscle cells cells vessels
-
7/31/2019 20456347 Git Physiology
10/95
Effect of different stimuli on
muscle contractionStimulus Effect on muscle
more depolarised smooth
1. Stretch of GI tract wall muscle, more excitable 2.
Acetylcholine release Leads toaction potential 3. Parasympathetic
stimulation generation and smooth
muscle contraction.
4. Noradrenaline release more hyperpolarised smooth5.
Sympathetic stimulation muscle, Less excitable and
fewer contractions .
-
7/31/2019 20456347 Git Physiology
11/95
Musculature of the GI tract
All smooth muscle except :
Upper third of oesophagus striatedMiddle third of oesophagus
mixedExternal anal sphincter striated
Areas of striated muscle are areas thatare under conscious
control .
-
7/31/2019 20456347 Git Physiology
12/95
GASTRIN
3 Main forms polypeptides
II G34 - T = 15 minsIII G17 T = 2-3minsIV G14I G45V G 4
Produced by G cells in Antral part and duodenal bulb.
Physiological Actions
Gastric AcidGastrin Pepsin
Also insulin + glucagon after a mealGastric motility
++Gastro-oesophageal sphincter.
Release
Amino Acids LuminalPeptides Acids
Distention of SecretinStomach G Cell GlucagonVagus Gastric
Inh
PeptidesCatecholamine Intestinal inh.
Peptides
-
7/31/2019 20456347 Git Physiology
13/95
CHOLECYSTOKININ - PANCREOZYMIN
SECRETED BY UPPER SMALL INTESTINE
STRUCTUREAmino Acids CCK 39, 33, 12, 8, 4C5 terminal amino acids
similar to Gastrin
ACTIONS1. Gall Bladder contraction2. Pancreatic juice - rich in
enzymes3. INHIBIT gastric emptying4. Augments pyloric sphincter
tone to delay gastric emptying5. Enterokinase Secretion6. Augments
action of secretion
7. Glucagon
SECRETION Peptides / amino acid in intestineFA > 10 carbon in
duodenum
+ve feed back with protein or fat digestion
-
7/31/2019 20456347 Git Physiology
14/95
SECRETIN
Produced by small intestineAmino acid structure glucagonT = 5
mins.
Action HCO 3- Pancreatic Juice
Water Content
Augments CCK actionGastric HClInsulin secretion
-
7/31/2019 20456347 Git Physiology
15/95
GIP
43 amino - residuesSecretion duodenum + jejunumStimulated by
glucose + fat in duodenum
ACTION - insulin SecretionInhibit gastric motility +
secretion
-
7/31/2019 20456347 Git Physiology
16/95
VIP
28 amino acidT 2 mins.In blood + gutStimulates Electrolytes
& H2O of intestinal secretions.Dilate blood vessels
Gastric acid secretion
-
7/31/2019 20456347 Git Physiology
17/95
GI motility
There are many types of contractions in differentAreas of the GI
tract. Some muscles contract and
relax in seconds
- phasic contractions peristalsissegmentation
Some maintain contractions over minutes or hours
- tonic contractions sphincters.
-
7/31/2019 20456347 Git Physiology
18/95
GI motility controlled by both humoral and neuralMechanisms1.
Extrinsic nervous systemParaymp = acetylcholine release = increased
contraction
2. Intrinsic nervous systemReceptors in GI tract/stretch = Ach,
SP release = increased contraction
3. Hormones
Only hormones known to have physiological effects on motility
are
motilin = increased gastric and intestinal
motilitycholecystokinin = decreased gastric emptying
-
7/31/2019 20456347 Git Physiology
19/95
Gastric motility
Fundus acts as food storeBody and antrum mix food 1. Relaxtion
of fundusPylorus contracts to limit exit of chyme (vagovagal
reflex
3. Pylorus contracts
4. Mixing byretropulsion
2.Contractionof bodyand antrum
-
7/31/2019 20456347 Git Physiology
20/95
-
7/31/2019 20456347 Git Physiology
21/95
Slow waves in the stomach cause
contraction without action potential
Em
Tension
4s
-
7/31/2019 20456347 Git Physiology
22/95
Control of gastric motility
Vagovagal reflex - Fundal relaxationMyenteric plexus - Slow
waves
contractions
Parasympathetic - inc contraction forceand freq
Sympathetic - dec contraction forceand freq
-
7/31/2019 20456347 Git Physiology
23/95
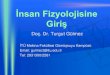
Control of gastric emptying
Chyme only empties from stomach when particle size is
smallEnough to pass through polyrus
Most important mechanism is strong stomach contractions
Contractions stimulated by :
1. Presence of food
2. Gastrin
But control of stomach emptying by these factor is fairly
weak
-
7/31/2019 20456347 Git Physiology
24/95
solids
liquids
Time
-
7/31/2019 20456347 Git Physiology
25/95
Control of gastric emptying
Most control of stomach emptying is done throughInhibitory
mechanisms in the duodenum and jejunumThrough nervous reflexes and
hormones
Inhibitory reflexes - direct - myenteric plexusindirect via
extrinsic nervesNeural reflexes stimulated by :Distension,
irritation, acidity, high osmolality,Protein/fat.Fats and acids
also stimulate release of humoral factors whichReduce gastric
emptyingCholecystokinin stim. By fatsSecretin stim. By acids.
-
7/31/2019 20456347 Git Physiology
26/95
Gastric motility on fasting
Migrating Motor Complex Occurs on fasting I.e. after digestion
and absorption of last meal, toclear undigested food particles.
Peristatic contractions sweep down stomach and duodenum pylorus
relaxes.
Pattern of contraction approx every 90 min. on fasting
Slow peristatic waves sweeping whole of GI tract
Thought to be controlled by motilin
-
7/31/2019 20456347 Git Physiology
27/95
Control of intestinal motility- neuronal
Mixing segmentationfrequency set by slow waves (12/minute
dudenum)additional control myeneteric plexus
Propulsion peristalsisLocal reflex stretch causes relaxation
distal andcontraction proximal ( Bayliss-Starling law of the
intestines)moves bolus through intestines.
Intestino-intestinal reflex extrinsic nervesLocal stretch in one
area inhibits contractions in rest of bowel
-
7/31/2019 20456347 Git Physiology
28/95
Reflex control of gut activity
CNS
Parasympathetic andSympathetic efferents Parasympathetic
and sympatheticSplanchnic efferent
And vagalAfferents Myenteric Submucosal
plexus plexus
Local efferentsLocal afferents
Gut wall muscleChemoreceptors Endocrine cellsmechanoreceptors in
Secretory cellsgut wall Blood vessel
-
7/31/2019 20456347 Git Physiology
29/95
Na + low Na + high
K+
diffusion Na + ATP
Na + Cl-
Na + also absorbedIn active transportProcesses eg
Glucose, aminoAcids, H + ions Osmosis H2O
Aldosterone stimulates Na + absorption
Absorption of electrolytes and water
-
7/31/2019 20456347 Git Physiology
30/95
Disorder of fluid absorption
consequence - diarrhoea
Hyperosmotic chyme e.g. high intake of
artificial sugars or high acid content. Infection e.g.
cholera
Colon can absorb 7L water per day but if smallIntestine secretes
more than this, result isDiarrhoea.
-
7/31/2019 20456347 Git Physiology
31/95
Reflex Stimulus Effect
gastroenteric Stomach distension Sl activitygastrocolic
Distension,emptying Colonicduodenocolic distension motility
enterogastric Chyme stomachacid/protein/fat emptyingirritant
vagovagal Food in stomach Fundal relax.intestointestinal
distention relaxation
-
7/31/2019 20456347 Git Physiology
32/95
Clinical problems with motilityGastric emptying
too slow = gastric carcinoma orulceration (vagotomy)
Results in nausea and vomiting, diarrhoea, cramps.Patients seek
help for difficulty swallowing (oesophageal scarring)or dental
erosion.
too fast = usually found in patients with
duodenal ulcer
Dont know if cause or effect overwhelms protective defences
ofduodenum
-
7/31/2019 20456347 Git Physiology
33/95
VOLUME OF G.I.T. SECRETIONS
Saliva 1000mlGastric Juice 3000mlPancreatic Juice 1000mlBile
1000mlIntestinal Juice 3000ml
TOTAL 9000ml
DAILY EXCRETION OF ELECTROLYTESIN GIT SECRETIONS
Na K Cl
Saliva 200 10 100Gastric J 150 20 250Pancreatic J 70 3 50Bile
100 4 50Intestinal J 300 15 300
Mmol/day 820 52 750
-
7/31/2019 20456347 Git Physiology
34/95
GASTRIC SECRETION
William Beaumont first identified actions of gastricJuice,
hydrochloric acid content, mucus secretion,and observed gastric
motility directly in 1825.
Protection of mucosamucusbicarbonate
Digestion and absorption of food, control of motilityacid
gastrinpepsinogen cholecystokeninintrinsic factor histamine
-
7/31/2019 20456347 Git Physiology
35/95
Oxyntic gland mucosasecretesmucusacid from parietal
cellsPepsinogen from pepticcellsIntrinsic factor from
parietal cells in humans(peptic cells in otherspecies.
Endocrine cells
Pyloric gland mucosa secretes throughout
mucosasecretesmucushistaminegastrin from G cells
-
7/31/2019 20456347 Git Physiology
36/95
Gastric secretions Mucus
Physical/ChemicalpH
-
7/31/2019 20456347 Git Physiology
37/95
Parietal cell - secretingTubulovesicles fuse withcanaliculus,
increased surface area
and numbers of H +K+ATP aseincreases acid secretion into lumenof
gut.
H+Acid secretion is against a 3million fold
concentrationgradientH+ inside = 4x 10 -8MH+ outside = 0.1 M
NEEDS ENERGY
-
7/31/2019 20456347 Git Physiology
38/95
Blood Parietal cell LumenAt rest 70mV
Secretion 40mVK+ K+ HCO 3-
HCO 3- ATPH+ H+
H2CO 3Na + Na +
ATP H2O + CO 2 Na + Na +
K+ K+ ATP
Cl- Cl - Cl -
ATP
H2O H2O
-
7/31/2019 20456347 Git Physiology
39/95
Na +K+
Cl -
H+
-
7/31/2019 20456347 Git Physiology
40/95
Gastric secretions
Pepsinogen Inactive precursor of pepsin whichinitiates protein
digestion
Is not necessary for completedigestion of dietary protein
pancreatic enzymes are sufficient
active only when the pH < 3.5Released by Ach
Pesinogen pepsin
Acid
-
7/31/2019 20456347 Git Physiology
41/95
Gastric secretions
Intrinsic factor
- Secreted from parietal cells in humans, chief cell in
other
Species.- Forms a complex with vitamin B 12 in the gut
- The complex is resistant to digestion & therefore
enablesAbsorption of vitamin B 12
Lack of intrinsic factor causes Vit B 12 deficiency(Pernicious
anaemia) as all the Vit B 12 is digested andTherefore none can be
absorbed
Only gastric secretion that isEssential for health
-
7/31/2019 20456347 Git Physiology
42/95
HCl SECRETION
CELLINTERSTITIAL JUICE
Cl Cl
CO 2 + H2Oc.A.
H2O CO 3
HCO 3- + H+
K
OH - H+
H2O
-
7/31/2019 20456347 Git Physiology
43/95
Gastric hormones
GastrinRelease from G-cells in the pyloric glands is stimulated
by Distension of stomach causes gastrin releasing
peptide (GRP) release from submucosal plexus-GRP causes gastrin
release
Presence of amino acids in stomach stimulateschemoreceptors
local reflexes cause gastrin release.
Release inhibited by pH
-
7/31/2019 20456347 Git Physiology
44/95
Gastric secretionControl is in 3 phases
1. Cephalic phase entirely dependent on the vagal nerve
accountsfor 10% - 15% total volume of secretion
acid secretion stimulated by sight, smell, chewing
and swallowingOral/nasal chemoreceptors vagal nucleus Ach +
GRPRelease acetylcholine + gastrin + histamine = acid secretion
Vagalafferents
-
7/31/2019 20456347 Git Physiology
45/95
2. Gastric phase accounts for at least 50% of
gastricsecretion
Controlled by local reflexes, vagovagal reflexes and
hormones
Distension of stomach local mechanoreceptors acetylcholineand
gastrin release acid and pepsinogen secretionAmino acids/peptides
local chemoreceptors gastrin release
acid and pepsinogen secretion
3. Intestinal phase - about 5% of secretion
Primarily hormonal denervated stomach will be stimulated
to secrete acid by protein in duodenumHormone still unknown
Very small number of G-cells in duodenum also release gastrin in
responseto amino acids.
-
7/31/2019 20456347 Git Physiology
46/95
Inhibition of gastric secretionAll mechanisms for the inhibition
of acid secretion act to ensure effectivedigestion of food.
1. Control by the stomachFall in pH
-
7/31/2019 20456347 Git Physiology
47/95
Secretion of the small intestine,pancreas and liver
Small Intestine
many villi on surface of intestine
crypts/glands of Lieberkuhn between villi epithelial cells
havebrush border.
Secretions are from cells within the crypts of Lieberkuhn and
fallInto two groups
secretions into the lumen (from enterocytes)secretions into the
blood (from endocrine cells)
-
7/31/2019 20456347 Git Physiology
48/95
Secretion into the lumen - mucus
Pancreas
First protectionFor duodenumFrom acid
Brunner s glands Compound mucus glands,Secreting
- alkali- mucus
SecretionStimulated byPara-sympathetics
Inhibited by
Sympathetics
?stress relatedulceration
-
7/31/2019 20456347 Git Physiology
49/95
Secretions into the lumen-aqueous
Absorption of nutrients andSecretion occurs at brushBorder in
matureenterocytes
Secretion moves up and outOf the crypts, mixes withChyme and
washes over theVilli into the lumen
Water and electrolyteSecretion fromUndifferentiated
enterocytesIn the bottom of crypts
-
7/31/2019 20456347 Git Physiology
50/95
Intestinal secretions
Small intestineMucus/alkali secretions mucosal protection
Aqueous secretionsunder local nervous controlsome minor hormonal
control (secretin, CCK)
Large intestineSecretion primarily consists of mucus. Can also
secrete waterIn response to irritation
-
7/31/2019 20456347 Git Physiology
51/95
-
7/31/2019 20456347 Git Physiology
52/95
Pancreatic secretions
Endocrine insulin & glucagonExocrine enzymes and
bicarbonate
essential for digestion
almost under separate hormonal control
Key hormones in stimulation of secretion are :
Cholecystokinin (CCK)
Secretin
Both released from the small intestine
-
7/31/2019 20456347 Git Physiology
53/95
Pancreas
Stomach
duodenum
PeptidesAmino acids, H +
FAT
I Cells
CCK
Cholecystokinin
-
7/31/2019 20456347 Git Physiology
54/95
Pancreatic enzymes
Essential for digestion - essential for life
Acinar cells
Proteases Lipases Amylases
Inactive form
Active enzymesActivated in gut
-
7/31/2019 20456347 Git Physiology
55/95
SECRETIN
FAT H +
HCO 3-
S cells
SECRETIN
-
7/31/2019 20456347 Git Physiology
56/95
ATP
Bicarbonate secretionLumen Blood
H2O CO 2 CO 2
H2CO 3
HCO 3- HCO 3- H+ H+
Cl - Cl - Na + Na + Na +
H2O H 2O
-
7/31/2019 20456347 Git Physiology
57/95
Pancreatic secretion
- secretion in 3 phasesCephalic phase - only 10-15% of total
secretion
activation of vagal efferents stimulates enzymerelease
Gastric phase - only present in some speciesNOT SIGNIFICANT IN
HUMANS
Intestinal phase - majority of secretioncombination of hormones
CCK and secretinresults in maximal enzyme and
bicarbonaterelease
-
7/31/2019 20456347 Git Physiology
58/95
Intestinal phase of secretion
VAGUS
CCK
PeptidesAmino acids
Fat, H +
Secretin HCO 3-
Enzymes
ACH
-
7/31/2019 20456347 Git Physiology
59/95
Functions of bile
- emulsification of facts- increased absorption of lipids
into
enterocytes.
- cholesterol excretion (only route)
- excretion of breakdown products ofhaemoglobin (bilirubin)
-
7/31/2019 20456347 Git Physiology
60/95
Secretion and storage of bile
Constituents of bileLiver Gallbladder
Water 98% 92%Bile Salts 1% 6%Bilirubin 0.04% 0.3%Cholesterol
0.1% 0.3-0.9%Fatty acids 0.12% 0.3-1.2%
Lecithin 0.04% 0.3%
-
7/31/2019 20456347 Git Physiology
61/95
Liver Secretion
Function and fateOf bile acids - theEnterohepaticcirculation
Bile acids almost totally
Reabsorbed in terminal illeum.20% excreted daily. Inhibition
ofReabsorption results inSynthesis of new bile acids andLowering of
cholesterol levels.
Portal vein
Gallbladder-Storage &concentration
CommonBile duct
DuodenumDigestion &emulsification
Ileum Absorbption ofBile acids
-
7/31/2019 20456347 Git Physiology
62/95
Secretions of the intestine, pancreasand liver-summary
Small intestine- mucus and fluid involved in protection and
absorption- hormones control of pancreatic and bile secretions.
Pancreatic secretions- Bicarbonate for neutralisation of acids,
optimises
conditions for enzyme action- Enzymes for digestion
Liver- bile for emulsification of fat
-
7/31/2019 20456347 Git Physiology
63/95
Digestion of carbohydrate, protein and fats by catalytic
hydrolysis
enzymes are either luminal (e.g. from salivary glandsor
pancreas) or membrane bound
Digested nutrients / fluids absorbed through the brushBorder
by
active transportdiffusion passive
facilitatedsolvent drag
-
7/31/2019 20456347 Git Physiology
64/95
Carbohydrate digestion- Initiated by salivary amylase from
salivary glands- majority by pancreatic amylase in small intestine-
pH optimum 7, activated by Cl - ions
1,4 bonds give straight chains
1,6 bonds give branched chains
Amylase can only hydrolyse 1,4bonds branched chains cannot
be
broken down by amylase
-
7/31/2019 20456347 Git Physiology
65/95
Carbohydrate digestion
StarchGlycogen
-dextrins, di-&trisaccharides
Glucose, galactosefructose
Luminal digestionamylase
Membrane digestione.g. sucrase, lactase
Humans do not haveCellulase-cellulose makesUp most of undigested
fibreIn diet
-
7/31/2019 20456347 Git Physiology
66/95
Absorption of simple sugars
Limiting step on simple sugar availability is rate ofAbsorption
large excess in small intestine.
Majority absorbed in duodenum and jejunum
Digested at membrane so available for transport
Fructose absorbed by facilitated diffusion
Glucose/galactose absorbed passively (small quantities)Under
anaerobic conditions and actively absorbed by sameCarrier when O 2
available.
Deficiencies of brush border enzymes cause osmotic diarrhoea
Human Sl can absorb up to 10kg sucrose per day
-
7/31/2019 20456347 Git Physiology
67/95
Absorption of glucose
Na+
Na +
Glu
Glu
Glu
Na +
ATP
K+ Low Na +
Na +
diffusion
Facilitated transport
Glu
-
7/31/2019 20456347 Git Physiology
68/95
-
7/31/2019 20456347 Git Physiology
69/95
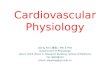
Activation of pancreatic proteases
Enterokinases
Trypsinogen Trypsin
TrypsinogenChymotrypsinogen
ProelastaseProcarboxypeptidase
TrypsinChymotrypsin
ElastaseCarboxypeptidase
Active proteases inactivated by trypsin
-
7/31/2019 20456347 Git Physiology
70/95
TransportersPeptidases
aminopolypeptidase Transporters
Cytoplasmic peptidase
Amino acids
Protein
PeptidesDi/tripeptides
Amino acids
-
7/31/2019 20456347 Git Physiology
71/95
Absorption of peptides and amino acids
Transport at the brush border1. Active transport by carrier.2.
Mostly dependent on Na + gradient co-transport similar to that
for glucose.3. Some amino acids (basic, and neutral with
hydrophobic side
chains) are absorbed by facilitated diffusion.
Protein assimilation affected by :
Pancreatitis, congenital protease deficiencies, deficiencies of
specificTransporters.
-
7/31/2019 20456347 Git Physiology
72/95
-
7/31/2019 20456347 Git Physiology
73/95
Absorption of vitamins
Vitamin Soluble in fat Soluble in waterA B1 B2
Niacin C D E K
Folic Acid B6 B12
-
7/31/2019 20456347 Git Physiology
74/95
Calcium absorption
Skin Vit D 3
Liver 25, OH-D 3
Kidney 1,25 (OH) 2D3
Parathyroid hormone
Ca 2
CBPCa 2+
Ca 2+
-
7/31/2019 20456347 Git Physiology
75/95
Absorptive capacity of theintestine
Actual Capacity
500g Carbohydrate 10g100g Fat 500g
50-100g Protein 700gaminoacids
7 8L Water 20+ L
-
7/31/2019 20456347 Git Physiology
76/95
Iron absorption transferrinmediated uptake
Fe 2+ + plasma transferrin
Ferritin
Fe Fe
Fe
Fe
Fe
Fe
TF
-
7/31/2019 20456347 Git Physiology
77/95
Digestion and absorption
Digestion by hydrolysis Importance of pancreatic enzymes
Types of membrane bound enzymes Mechanism of absorption :
Carbohydrates, fats, proteins, electrolytes, water, special
cases
Effect of disturbances in digestion / absorption.
-
7/31/2019 20456347 Git Physiology
78/95
Nutrition and control of foodintake
Control of appetite, hunger and satietyNutritional
requirements
Essential fatty acidsEssential amino acidsCarbohydratesVitamins,
minerals
Special cases, pregnancy & lactationMalnutrition &
dental relevance
-
7/31/2019 20456347 Git Physiology
79/95
Experimental evidence that hungerand satiety are controlled
centrally
lateral nucleus feeding centreElectrical stimulation
hyperphagia
Destruction aphagia
Endogenous control of feeding
Low plasma glucose and amino acidsInput from olfactory ( smell
), gustatory ( taste ) andVisual primary afferents
-
7/31/2019 20456347 Git Physiology
80/95
Ventromedial nucleus satiety centre
Stimulation refusal to eatDestruction uncontrolled eating,
obesity
Endogenous control of feedingAlso responds to low plasma
[glucose] and[amino acids] BUT IN OPPOSITE WAYOther inputs :
stomach distension, plasma CCK
& insulin all stimulateAmphetamines potentiate
neurotransmitter effects in the VMN andSuppress feeding
-
7/31/2019 20456347 Git Physiology
81/95
Regulation of food intake
Glucose (GI & plasma)Amino acidsLipids (CCK)
Ventromedial nucleussatiety centre
Lateral nucleusfeeding centre
++ -
- -Feeding
-
7/31/2019 20456347 Git Physiology
82/95
Regulation of appetite food choice
Controlled by dietary need (exp.animals) Controlled by limbic
system (amygdala)
acting on hypothalamusArea of brain involved in emotional
control
Lesions abolish food choice
Major control in humans (developed world)probably taste rather
than dietary need,
-
7/31/2019 20456347 Git Physiology
83/95
Long termBodyTemperature-Energyavailable
GlucostaticAminostaticlipostatic
Control of food intake
Short termWhat stops you eating
Hormones CCK,Insulin,glucagon
Gl distensionOral meter
-
7/31/2019 20456347 Git Physiology
84/95
-
7/31/2019 20456347 Git Physiology
85/95
Nutrition what we need and why ?Amino acids protein
synthesis
Essential, conditionally essential, non -essential plus
Extra
Protein requirements 0.6g/kg adult per dayMore in growth &
repair e.g. infants, infection, pregnancy
Protein required due to turnover in tissuesIn growth or wasting,
tissues which turnover protein fastest will alter most in mass
I.e. Liver, gut, white cells
Loss of protein = loss of function
-
7/31/2019 20456347 Git Physiology
86/95
-
7/31/2019 20456347 Git Physiology
87/95
Nutrition what we need and why
Fatty acid deficiency in animals -failure to grow linolenic
acid
skin & kidney lesions
Linoleic and arachidonic acids reverseother deficiencies.
BODY CANNOT MAKE THESE FATTY ACIDSESSENTIAL
-
7/31/2019 20456347 Git Physiology
88/95
Nutrition what we need and why
Carbohydrates- non-essential
except for non-starch polysaccarhides (fibre).
Insufficient fibre results in poor blood glucose and lipid
control, increasedGut infection and incidence of cancer.
- preferred source of energy- Sucrose most cariogenic
substance
-
7/31/2019 20456347 Git Physiology
89/95
Vitamins
Deficiency becoming more common inSome urban populations in
UK
Vit D - ricketsVit C - scurvy
Long history of recognised importance -Deficiency disease
e.g. beri-beri (B 1; 2000BC), scurvy(C; in sailors 1400 AD)
-
7/31/2019 20456347 Git Physiology
90/95
Vitamins requirements and deficiencies
1. Water solubleVitamin Recommended daily intake (mg)
Deficiency
B1 (Thiamine) 1.5 Beri-beriRiboflavin 1.8Niacin 20 PellagraC 45
ScurvyFolic acid 0.4 Anaemia, spina bifida
B12 0.003 Pernicious anaemiaB6 2Panthothenic acid unknown
Not stored in body deficiency leads to rapid clinical
symptoms.Most important ones in terms of dentistry are :B12
(fiboflavin) important for cellular metabolism in mouth, cornea
& skin
deficiency glossitis, angular stomatitis, corneal
vascularisationphotophobia
Vitamin C necessary for collagen formationdeficiency (scurvy) =
gingival oedema & bleeding, delayed healing,brusing.
-
7/31/2019 20456347 Git Physiology
91/95
Vitamins requirements and deficiencies
2. Fat solubleVitamin Recommended daily intake Deficiency
A 5000 IU Blindness, dry mucous membrane, abortiongrowth
failure.
D 400 IU Rickets, poorly calcified dentition,
delayederuption
E 15 IU Foetal resorptionK 70 g Poor clotting
Particularly important in dentistry :Vitamin A - 500,000 new
cases per year in developed countriesVitamin D - may be prevalent
in racial groups moving from sunny to
temperature climates
-
7/31/2019 20456347 Git Physiology
92/95
Minerals and trace elementsMineral/ trace element Recommended
daily intake Required for
Iron 10-20mg Oxygen carriage haemoglobinCalcium 800-1200mg
Calcification, cell excitabilityCobalt part of Vitamin B 12 Iodine
150 g thyroid function Copper ossification Zinc 15mg immune
response
Fluorine 1ppm drinking water prevention of caries
Ion deficiency anaemia. May present with pale mucous
membranes.Fairly common particularly in women (pregnancy).Calcium
deficiency - rare except in vegetarians
Iodine = extremely rare as salt is iodinated
Deficiency of trace elements extremely rare as requirements are
so low
-
7/31/2019 20456347 Git Physiology
93/95
FASTINGA. 6 24 hours
Liver Glycogen glucose insulin (100g)Major source - free fatty
acids from ADIPOSE TISSUE
Gluconeogenesis glucoseSmall amount of acetoacetate, B OH
butyrateMajor response due to insulin
B. 2 4 days
Liver Glycogen depletedGlyconeogenesis ++ from amino acids
mainly from muscle, glycerolfrom adipose tissue + lactate from
Rbc
FA Ketones in liver
Hormones InsulinCortisol & adrenalineGlucagon & this
peaks at 4 days.
-
7/31/2019 20456347 Git Physiology
94/95
FASTED STATE > 2 WEEKS
1. Ketone Bodies formed as main source of energy =mainly in
LIVER
2. Gluconeogenesis
3. Insulin conc. Tends to be lowCortisol be responsible foHigh
levels
Adrenaline
Glucagon levels and may r reduced levels ofGluconeogenesis.
T k h
-
7/31/2019 20456347 Git Physiology
95/95
Take home message
Energy in = energy out Avoid faulty diet balanced diet few
deficienciesSpecial care in special circumstances
Less fat, more CHO
(watch the sucrose!)
Extra care in :
Less meat, more fish(EFF)
Pregnancy moreEnergy & protein plusFe, Ca, Vit D, etc
etc
More exercise
Enough Fe & Ca
Fluorides (?)
Weaned infants -Protein, fatty acids, vitC etc.etc.