-
8/14/2019 3.neuro
1/16
NEURO-OPHTHALMOLOGY
Chuanbao-Li
-
8/14/2019 3.neuro
2/16
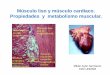
Introduction
As demonstrated by their common embryological origin, theretinas
and anterior visual pathways (optic nerves, opticchiasm, and optic
tracts) are an integral part of the brain,
providing a substantial proportion of total sensory input.
They frequently give important diagnostic clues to
centralnervous system disorders.
Intracranial disease frequently causes visual
disturbancesbecause of destruction of or pressure upon some portion
of theoptic pathways.
Cranial nerves III, IV, and VI, which control ocularmovements,
may be involved, and nerves V and VII are alsointimately associated
with ocular function.
-
8/14/2019 3.neuro
3/16
Clinical Examination
Visual Acuity
Colour Vision
Visual Fields
Pupils
-
8/14/2019 3.neuro
4/16
Normal Optic Disc
Cupped disc
-
8/14/2019 3.neuro
5/16
The swollen optic disc
Papilloedema
Papillitis
Malignant hypertension
Ischaemic optic neuropathy
Diabetic optic neuropathy
CRVO
Intraocular inflammation
-
8/14/2019 3.neuro
6/16
The pale optic disc
Congenital
Secondary to
raised IOPvascular
retinal disease
optic
neuritis
optic nerve
compression
trauma
Glaucoma
-
8/14/2019 3.neuro
7/16
Ocular motility
abnormalities Third nervepalsy
Double vision
Eye turned down & out Ptosis
Dilated pupil &
headache
Sixth nerve palsy
Double vision
Eye turned in
-
8/14/2019 3.neuro
8/16
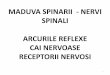
shows the types of field defects causedby lesions in various
locations ofthe pathway.
Lesions anterior to the chiasm (ofthe retina or optic nerve)
causeunilateral field defects;
lesions anywhere in the visualpathway posterior to the
chiasmcause contralateral homonymous
defects. Chiasmal lesions usually cause
bitemporal defects.
Localising the lesion
visual pathway
-
8/14/2019 3.neuro
9/16
Optic Neuritis
swollen optic disc
-
8/14/2019 3.neuro
10/16
Optic Neuritis
Symptoms
Loss of vision deteriorating over hours (rarely) to days(most
commonly), with the nadir approximately 1 week
after onset. Visual loss may be subtle or profound. Usually
unilateral,
but may be bilateral.
Age typically 18 to 45 years. Orbital pain, especially with
eye movement. Acquired loss of color vision. Reduced perception
of light
intensity.
RAPD(Relative afferent pupillary defect )
-
8/14/2019 3.neuro
11/16
Optic Neuritis
RAPD(Relative afferent pupillary defect )
-
8/14/2019 3.neuro
12/16
Optic Neuritis
Etiology
Idiopathic.
MS(multiple sclerosis) : Frequently optic
neuritis is the initial manifestation of MS.
Childhood infections or vaccinations.
Other viral infections: e.g., herpes zoster.
Contiguous inflammation of the orbit
-
8/14/2019 3.neuro
13/16
Optic NeuritisTreatment
If patient seen acutely with no prior history of MS or
opticneuritis:
If MRI reveals at least one typical area of demyelination,
offer
pulsed intravenous injection steroid in the following
regimenwithin 14 days of decreased vision
Methylprednisolone 1 g/day i.v. for 3 days, then
Prednisone 1 mg/kg/day p.o. for 11 days, then
Taper prednisone over 4 days (20 mg on day 1, 10 mg on days
2 and 4).Antiulcer medication (e.g., ranitidine 150 mg p.o.,
b.i.d.) forgastric prophylaxis.
-
8/14/2019 3.neuro
14/16
Optic NeuritisTreatment
If MRI shows two or more characteristic
demyelinating lesions, treat with the
aforementioned steroid regimen. Refer to
neurologist for possible treatment
With a negative MRI, the risk of MS is low
In a patient with diagnosis of prior MS or optic
neuritis:
Observation.
-
8/14/2019 3.neuro
15/16
Optic NeuritisNote
NEVER use oral prednisone as a primarytreatment because of
increased risk ofrecurrence.
-
8/14/2019 3.neuro
16/16