Embed Size (px)
Citation preview

8/14/2019 9018
http://slidepdf.com/reader/full/9018 1/82
inding the Rx for Managing Medical Wastes
October 1990
OTA-O-459
NTIS order #PB91-106203

8/14/2019 9018
http://slidepdf.com/reader/full/9018 2/82
Recommended Citation:
U.S. Congress, Office of Technology Assessment, Finding the Rx for Managing Medical
Wastes, OTA-O-459 (Washington, DC: U.S. Government Printing Office, September 1990).
For sale by the Superintendent of DocumentsU.S. Government Printing Office, Washington, DC 20402-9325
(Order form can be found in the back of this report.)

8/14/2019 9018
http://slidepdf.com/reader/full/9018 3/82
Foreword
The adequate management of medical wastes first became a major focus of publicattention when medical wastes with other debris washed ashore on the East Coast in thesummer of 1988. In October of that year, as part of OTA’s assessment of municipal solid waste
management, OTA issued a background paper entitled Issues in Medical Waste Management.That study provided an overview of medical waste disposal practices and potential risksassociated with them, and discussed the need for further Federal involvement in managingmedical wastes.
Also in October of 1988, Congress passed the Medical Waste Tracking Act, establishinga 2-year demonstration tracking program for medical waste management and directing theEnvironmental Protection Agency and the Agency for Toxic Substances and Disease Registryto complete several studies to evaluate management issues and potential risks related tomedical waste disposal.
Some studies by these and other government agencies, and by private-sector interests,
have been completed since that time on various aspects of medical waste management issues.The focus of concern has shifted primarily to the adequacy of handling, treatment, and disposalpractices for medical wastes. Public concern remains high and much of the confusion andinconsistency associated with medical waste policy persists.
This OTA report was requested by the House Committee on Science, Space, andTechnology, the House Subcommittee on Transportation and Hazardous Materials, Commit-tee on Energy and Commerce, and the House Subcommittee on Regulation, BusinessOpportunities and Energy, Committee on Small Business. The report evaluates medical wasteissues in the broader context of a waste management policy for the Nation. Waste reductionand recycling options for medical waste management, as well as incineration andnon-incineration treatment alternatives are examined.
Applying a more comprehensive waste management approach to medical wastes, suchas has evolved for municipal solid waste and hazardous waste, could help ensureenvironmentally sound and economically feasible waste practices. At a minimum, we realizethat (as with most waste problems) there is no one management scenario to “solve” ourmedical waste problems; rather the most important task is to devise policies that will facilitateadoption of individually optimal solutions to specific problems.
OTA benefited from the assistance received from many organizations and individualsduring the course of this study. We express our gratitude and thanks to the review panel andthe many other reviewers for their input which greatly facilitated the preparation of the report.
OTA, however, is solely responsible for the contents of this report.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 4/82
Review Panel and Medical Waste Workshop Participants forFinding the Rx for Managing Medical Waste
Barry Rabe, ChairmanSchool of Public Health
University of Michigan
Richard BernsteinGeneral Medical Corp.
Leland CooleyRadiation Safety/Biosafety OfficeUniversity of Maryland at Baltimore
Frank CrossCross/Tessitore & Associates, P.A.
John Cusack Asea, Brown & Boveri
Janet EmmermanWaste Management, Inc., Medical Services
Roger EtterJohn Zink Co.
Martin S. FaveroCenters for Disease Control
Randell Forshey
San-i-pak Pacific, Inc.
Barbara FryState of CaliforniaAir Resources Board
Allen HershkowitzNatural Resources Defense Council
Ode KeilJoint Commission on Accreditation
of Healthcare Organizations
Janis KurthMetropolitan Hospital
Jenny Lezak Health Organization to Protect Our Environment
Daniel LibermanMassachusetts Institute of Technology
Thomas J. Murphy
Thomas J. Murphy AssociatesEdward NormanState of North Carolina Health Department
Claude D. RoundsAlbany Medical Center
James SharpStericycle
Robert Spurgin, OTA ContractorSpurgin & Associates
Martha TruslerMethodist Health Systems
Wayne TurnbergDepartment of EcologyState of Washington
Michelle WilsonU.S. Environmental Protection Agency
NOTE: OTA appreciates and is grateful for the valuable assistance and thoughtful critiques provided by the workshop participants,advisory panel members, and reviewers. These participants do not, however, necessarily approve, disapprove, or endorse thisspecial report. OTA assumes full responsibility for the special report and the accuracy of its contents.
iv

8/14/2019 9018
http://slidepdf.com/reader/full/9018 5/82
OTA Medical Waste Management
John Andelin, Assistant Director,
Project Staff
OTA
Science, Information, and Natural Resources Division
Robert Niblock, Oceans and Environment Program Manager
Kathryn Wagner, Project Director
Contractors
Robert Guttman, Esq.
Robert Spurgin, Spurgin & Associates
Administrative Staff
Kathleen Beil Sally Van Aller

8/14/2019 9018
http://slidepdf.com/reader/full/9018 6/82
Reviewers and Contributors
Robert AshworthBrowning-Ferris Industries
Charlotte BakerUniversity of California
Robert G. BartonEnergy & Environmental Research Corp.
John N. Basic, Sr.Basic Environmental Engineering
William F. BinaNaval Medical Command
Jack D. BradyAnderson 2000, Inc.
Theodore G. BrnaU.S. Environmental Protection Agency
Joy Buck City Hospital, Inc.
Robert E. CampbellJohnson & Johnson
Sherry ClayTexas Department of Health
Peter S. DaleyChemical Waste Management, Inc.
Milton DezubeAmerican Hospital Association
Henry L. Diamond, Esq.Beveridge & Diamond, P.C.
Lawrence DoucetDoucet & Mainka
Dennis DowningCornell University
Al Dozier
Advanced Concepts, Inc.Kenneth L. DuFourMedical Disposal Systems
George EstelNew York State Department of Health
Jacquelyn FloraBrowning-Ferris Industries
Robin GillespieService Employees International Union
Martin E. Gilligan, Jr.Donlee Technologies, Inc.
Mary GreeneU.S. Environmental Protection Agency
Roger GreeneState of Rhode Island
Dieter GroschelUniversity of Virginia Medical Center
Robert Guttman, Esq.
Shari HaleyAmerican Hospital Association
John HallSan-i-pak Pacific, Inc.
Susan HarwoodU.S. Department of Labor
Steven A. HickersonEMCOTEK
Travis HoneycuttIsolyser
Wally JordanWaste Tech
Edwina JuilletMartha Jefferson Hospital
Larry King
Poly-Flex
Jonathan KiserNational Solid Waste Management Association
Carolyn KonheimKonheim & Ketcham
Judy KowalskiNew Mexico Energy, Minerals
and Natural Resources Department
Jack Lauber
New York State Department of Environmental Conservation
Cc. LeeU.S. Environmental Protection Agency
Howard LevensonOffice of Technology Assessment
Maureen LitchveldAgency for Toxic Substances and Disease Registry
Edward LondresNew Jersey Department of Environmental
Protection
Hugo LopezBeth Israel HospitalRebecca Goldberg
Environmental Defense Fund
vi

8/14/2019 9018
http://slidepdf.com/reader/full/9018 7/82
Robert LordNassau-Suffolk Hospital Council, Inc.
Rodney W. LowmanThe Council for Solid Waste Solutions
Donald C. MalinsPacific Northwest Research Foundation
Ted MalloyStanford University
John ManuelOntario Ministry of the Environment
Gretchen McCabeHuman Affairs Research CenterBattelle
Jean-Ann McGraneNew York City Health & Hospitals Corp.
Jim McLaineyAmerican Hospital Association
Allan McLeanThe University of Chicago Medical Center
John McVicarCenters for Disease Control
Tom MerskiUniversity of Pittsburgh
Thomas W. MoodyState of Florida Department
Environmental Regulation
Pat MooreU.S. General Accounting Office
Sue MorelandUniversity of Tennessee
Phil MorrisSouth Carolina Department of
Health and Environmental Control
Regina MornsNew York Department of Sanitation
Liisa NenonenThe RACOURSE Network
Jerry NessNorthwestern Memorial Hospital
Ross PattenBFI Waste Systems
Jacqueline PolderCenters for Disease Control
Sven E. RodenbeckAgency for Toxic Substances and Disease Registry
Claude RoundsAlbany Medical Center
William RutalaUniversity of North Carolina
School of Medicine
Jacqueline W. SalesHazmed
W. Thomas SchipperKaiser Permanence
Steve SchulerJoy Energy
Harvy SchultzNY City Department of Environmental Protection
Robert SheehanMedi-Gen
Robert SpurginSpurgin & Associates
Jeffrey SteinerMayo Clinic
Tom Stewart
State University of New York Christopher B. StrasserThe Allentown Hospital—
Lehigh Valley Hospital Center
Pam SulmerState of Minnesota
Attorney General’s Office
Kevin TonatNational Institutes of Health
Jim Tripodes
University of California
Jacqueline WarrenNatural Resources Defense Council
Joe WilsonMedical Safetec
Robert PetersNational Solid Waste Management Association
vii

8/14/2019 9018
http://slidepdf.com/reader/full/9018 8/82
Contents
Page
Introduction, Major Findings, and Policy Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
SUMMARY OF FINDINGS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 4POLICY ISSUES FOR FEDERAL ACTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Chapter 1. Characterizing Medical Wasteland Applying a Comprehensive Management Strategy. 9MEDICAL WASTE IN A COMPREHENSIVE WASTE MANAGEMENT STRATEGY . . . . . . . . . . 9WASTE CHARACTERISTICS AND TYPES-TREATMENT IMPLICATIONS . . . . . . . . . . . . . . . . 11
Chemical Characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Biological Characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Physical Characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Chapter 2. Before Treatment: Waste Reduction and Recycling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
BEFORE-TREATMENT APPROACHES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19WASTE REDUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19RECYCLING AND SOURCE SEPARATION PRACTICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Chapter 3. Non-incineration Treatment Technologies and Trends . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
AUTOCLAVING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Capacity and Siting Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Suitability for Different Medical Wastes and Associated Risks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Costs and Volume Reduction Issues. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
AUTOCLAVING AND COMPACTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32MECHANICAL/CHEMICAL DISINFECTION. , . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33MICROWAVE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36IRRADIATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36OTHER POTENTIAL TREATMENT TECHNOLOGIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Chapter 4. Incineration Treatment Issues and Trends . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
REGULATORY TRENDS AND MEDICAL WASTE INCINERATION . . . . . . . . . . . . . . . . . . . . . . . . . 42
CAPACITY, COSTS, AND RISKS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46Capacity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46costs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Risks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
TRENDS IN AIR POLLUTION CONTROL SYSTEMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51OPERATOR TRAINING.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53OFF-SITE INCINERATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Off-Site v. On-Site Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54Co-Incineration or Co-Firing of Wastes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54Regional Incineration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .57
Chapter 5. Special Treatment Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .59
SHARPS MANAGEMENT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59Manufacturing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59Mechanical/Chemical . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60Encapsulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60Mail Shipment for Disposal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
SMALL GENERATOR MANAGEMENT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61OTHER TREATMENT TECHNIQUES: SEWER USE AND SHREDDING . . . . . . . . . . . . . . . . . . . . . 62
Sewer Use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62Shredding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
Chapter 6. Comparisons of Treatment Alternatives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65CAPABILITIES AND RISKS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
COSTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
Appendix A. The Medical Waste Tracking Act . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69

8/14/2019 9018
http://slidepdf.com/reader/full/9018 9/82
Contents—Continued
Boxes
Box Page
A. Management of Medical Low-Level Radioactive Waste (LLW) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16B. Disposables: Infection Control and Waste Management Implications . . . . . . . .......... . . . . . 20
C. California and Its Dioxin Control Measure: A Case Study of One State’s Approach to
FiguresFigure Page
l. Schematic of One Hospital’s Proposed Segregation Categories and ComprehensiveMedical Waste Management Approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .... 23
3. Typical Sterilization Destruction Curve . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ... 30
5. Mechanical/Chemical Disinfection Unit. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 356. Mobile Microwave Medical Waste Disinfection Unit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 37
8. Controlled Air Incinerator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ............ . 459. Comparison of PCDD/PCDF Concentration in Medical and Municipal Wastes. . . . . . . . . . . . . . . . . . . 49
IO. Comparison of PCDD/PCDF Emissions From a Variety of Icinerators . . . . . . . . . . . . . . . . . . . . . . . . . 4911. Comparisons of Cadmium Emissions From a Variety of Incinerator s..... . . . . . . . . . . . . . . . . . . . . . . 50
TablesTable Page
l. Major Federal Agencies Addressing Medical Waste Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32. Types of Wastes Designated as Infectious by Various Entities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123. Percentages of Waste Types Produced at Different Medical/Health-Care Facilities in the
State of Washington . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .... 144. Characteristics of Medical Waste . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175. Comparison of the Composition of Medical and Municipal Waste . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 176. Emissions of Dioxins and Cadmium From Medical Waste Incinerators in California . . . . . . . . . . . . . . . 487. Performance Data of Medical Waste Incinerators With Pollution Control Equipment . . . . . . . . . . . . . . 528. Comparison of Treatment Technologies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66

8/14/2019 9018
http://slidepdf.com/reader/full/9018 10/82
Introduction, Major Findings, and Policy Issues
Two years after the beach washups of medicalwastes in a hot summer,
lpreliminary results from
investigations by Federal agencies into medicalwaste management issues are being reported.
2At the
same time, many State and local governments (107,139,110) and several private groups (77) haveundertaken efforts to better address the managementof medical wastes. Certainly, more is known aboutcurrent medical waste management practices thanprior to the passage of the Medical Waste TrackingAct (MWTA) in October 1988
3(see app. A). Yet,
much of the confusion and inconsistency associ-
ated with medical waste policy persist. Basicinformation as well as consensus on some funda-mental management issues remain absent from theefforts to formulate a adequate national medicalwaste policy.
As current governmental studies and efforts arecompleted, it is clear that critical aspects of medicalwaste issues need to be addressed further:
Consensus on the definition of regulated medi-cal wastes must develop, based on the potential
health risks posed by these wastes (e.g., theability of a particular type of medical waste topose a risk of infectious disease transmissionbeyond that associated with municipal solidwaste).Basic, more precise information on the genera-tion (amounts and disposal methods) of medi-cal wastes, particularly by non hospital sources,is needed.Potential waste reduction and recycling opportu-nities to improve medical waste management
need to be investigated, including considera-tion of product redesign to produce reusableand recyclable medical products where appro-priate, or to avoid use of problematic (e.g.,cadmium and lead) components in products.Appropriate workplace practices for occupa-tional groups in frequent contact with medicalwastes (e.g., health-care workers, refuse work-ers) need to be developed by relevant govern-
q
q
q
mental agencies and adopted by employers tominimize the occupational hazards posed bythese wastes.
Information on treatment technologies, inparticu-lar nonincineration alternatives, needs to bemore readily available to State and localregulators, to generators, and to the generalpublic.
Air emission standards for medical wasteincinerators, expected to be completed in acouple of years by the Environmental Protec-tion Agency (EPA), are needed to create a more
certain regulatory climate. Procedures to estab-lish the safety and efficacy of new treatmenttechnologies are needed.
Management options for small generators of medical waste (including households) must bedeveloped and information on their availabilityshould be more readily available.
Before a comprehensive approach to medicalwaste management can be pursued, gaps in informa-ion and research that limit resolution of these issues
must be better addressed. Some of the necessarystudies, particularly those that better characterize thenature of health risks posed by medical wastes, willrequire significant commitments of time and fund-ing, e.g., for epidemiologic and longitudinal studies.
The Office of Technology Assessment (OTA), ina background paper released in October 1988, Issuesin Medical Waste Management, briefly examinedthe adequacy of current medical waste disposalpractices, the potential risks from such practices, and
the need for further Federal requirements for thehandling, treatment, storage, and disposal of medicalwastes. The focus of this OTA report is: 1) to placemedical waste problems in a broader waste reductionand materials management perspective, as is evolv-ing for municipal solid waste (MSW) and hazardouswaste; and 2) to address a number of outstandingissues on incineration and other medical wastetreatment technologies.
l~ e cau s e s and impa cts of the beach wa s h u p s of medical waste a re discussed in a sep~ate effofi (11s).
~amely, the studies of medical wast e issues manda ted by the Medical Waste Tr acking Act t o be completed by th e Environm enta l Protection Agencyand the Agency for Toxic Substances and Disease Registry, as discussed below.3 ~ e Me~~ Wwt e T ~ a & @ Ac t is m e n d e d ~ n ew s u b t i ~ e J t o t i e s o ~ d w a s t e D i s p o s ~ Ac t a n d t i e Re s o u r c e Conserva tion a nd Recovery Act
(Public Law 89-272; 42 U.S.C. 6901 et seq.).
– l -

8/14/2019 9018
http://slidepdf.com/reader/full/9018 11/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 12/82
Introduction, Major Findings, and Policy Issues q 3
incinerators is regulated medical waste, the remain-ing 40 percent being municipal waste (107).
EPA, the Centers for Disease Control (CDC), the
Occupational Safety and Health Administration(OSHA), and other Federal agencies have issueddifferent, general guidelines for infectious andmedical waste management (see table 1). Differ-ences of opinion exist over the importance andimpact of variations between the definitions andrecommendations of these government agencies.Any remaining confusion over government posi-tions on these matters could be eliminated if Congress designated a lead agency to coordinate andclarify the Federal Government positions on medical
waste issues. As noted in OTA’s previous back-ground paper on medical waste, EPA is the agencywith the most comprehensive authority to provideFederal leadership on the management of medicalwastes (114).
OTA’s statement in that background paper stillapplies: “Currently, no Federal regulations existthat comprehensively address the handling, transpor-tation, treatment, and disposal of medical waste”(emphasis added; 114). This means that variationexists among the requirements that States and
localities have devised for medical waste manage-
ment. In recent years, such variations have ledobservers to suggest that the Federal Governmentneeds to establish some baseline, uniform standardsand guidelines for medical waste management. To
date, the Federal Government has been reluctant toact without greater information on a number of issues related to medical waste management (114).
Some of this information may come from studiesthat both the EPA and the Agency for ToxicSubstances and Disease Registry (ATSDR) arerequired to conduct under MWTA (sees. 11008 and11009). MWTA (sec. l1008(a)) requires EPA toevaluate and include in reports to Congress: genera-tor information (types, number, and size); on-site
and off-site management practices, including seweruse; types and amounts of medical wastes; costsassociated with the improper management of medi-cal waste and those from compliance with theregulatory requirements of MWTA demonstrationprogram; available and potential reduction, reuse,and management methods; implications of regula-tory exemptions of household and small quantitygenerators; guidelines for the management of medi-cal waste from households and small-quantity gener-ators; existing State and local controls; and the
appropriateness of applying Subtitle C requirements
Table l—Major Federal Agencies Addressing Medical Waste Issues
Agency Authority Activity
U.S. Environmental ProtectionAgency (EPA)
Occupational Safety and HealthAdministration, U.S. Departmentof Labor (OSHA)
Centers for Disease Control, U.S.Department of Health and HumanServices (CDC)
Agency for Toxic Substances andDisease Registry, Public HealthService, U.S. Department ofHealth and Human Services(ATSDR)
Guidance and Regulatory a Issued Guide for Infectious Waste Management; issuedregulations to establish the Medical Waste TrackingProgram; establishing new source performance stan-dards for medical waste incinerators; completing stud-ies requested by the Medical Waste Tracking Act;authority under the Resource Conservation and Recov-ery Act to regulate the handling, storage, and transpor-tation of medical wastes.
Guidance and Regulatory b Issues advisory notices and workplace standards focusingon occupational exposure to infectious materials andwastes.
Guidance and Recommendations c Issues notices and advisories, sometimes jointly withOSHA, focusing on infection and control issues.
Study and Revievc Completing study required by the Medical Waste Tracking
Act, focusing on evaluating health effects associatedwith medical wastes.
aEpA’$ c om p r e h e n s i ve au t lmf i t y to regulate medical waste management is granted under the Resource Conservation and Recovery Act. The Agency alsohas special regulatory authority to administer a demonstration medical waste tracking program and is required to complete a number of studies related tomedical waste management under the Medical Waste Tracking Act (42 U.S.C. 6901 et seq.).
b@J+A~$ Pnmwy a~honty is granted under t h e ~upat iona[ safety and Health Act (29 IJ.S.C. 651 et seq . ) . Gu ide l i n e s o r r e g u l a t i o n s only appiy tO priVd43
facilities, unless a State extends cmverage to employees of public facilities as well.CDCMM not have the authority to issue regulations.
SOURCE: Office of Technology Assessment, 1990.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 13/82
4 q Finding the Rx for Managing Medical Wastes
(i.e., the hazardous waste provisions) of the Re-source Conservation and Recovery Act (RCRA) tomedical wastes.
EPA has concentrated its implementation effortsthus far on promulgating and implementing therequirements for the MWTA demonstration pro-gram. The regulations were promulgated ahead of schedule in March 1989 and became effective inJune 1989 (Federal Register, Mar. 22, 1989). TheAgency and its contractor convened a meeting inNovember 1988 with health-care and waste indus-try, environmental, and various State and FederalGovernment representatives to discuss ways to
collect information on medical waste generation andmanagement practices as part of this effort (123).EPA’s first of three required reports to Congressunder the law, highlighting the efforts to address theissues under study, was delayed by more than a year.This delay was due, at least in part, to inaction by theOffice of Management and Budget (OMB) in itsreview of the report. The first report is expected toreview what EPA plans to study and focus on theproposed approach for a health hazard assessment(89).
ATSDR is required to report on such healtheffects of medical waste as: estimates of the numberof people annually infected or injured by medicalwastes (including sharps), including descriptions of the nature and seriousness of those incidents; andestimates of the number of cases traceable to medicalwaste of diseases that could be spread by impropermanagement of such wastes (in particular, hepatitisB virus (HBV), and immunodeficiency virus (HIV),or AIDS). Its report to Congress on the public health
implications of medical waste is expected to bereleased on schedule on November 1, 1990.8
The EPA and ATSDR studies are limitedbecause existing information and data are inade-quate (134). Still needed are research, surveysand studies that generate new information andaddress existing data gaps.
To address these research needs is beyond thescope of this report, which is intended to provide aframework for considering medical waste manage-
ment issues and to assess in a preliminary way thepotential of various reduction and treatment meth-ods for medical waste.
9The report is divided into six
chapters: 1) applying a comprehensive waste man-agement strategy to medical waste and a brief reviewof Federal efforts undertaken to date; 2) exploringpretreatment approaches (e.g., waste reductions andrecycling options); 3) exploring nonincinerationmedical waste treatment technologies and emergingtreatment technologies; 4) examining current issuesregarding incineration of medical wastes; 5) discuss-ing special treatment issues, such as sharps (e.g.,needles, glass, etc.) management and small genera-tor issues; and 6) comparing various management
treatment alternatives.
SUMMARY OF FINDINGS
Two of the critical findings of this study areconsistent with a comprehensive waste reductionand materials management approach to wastemanagement. First, treatment technologies willcontinue to be needed for waste management, butthey can be preceded and complemented byprevention and pretreatment efforts (i.e., reduc-
tion and recycling). Second, while there is no onepreferred treatment method, source separationpractices (i.e., separating wastes based on thephysical, chemical, and infectious characteris-tics) are key to targeting particular materials/ wastes for the most appropriate treatment method.
Other findings of this report include:
. The commercial viability of nonincinerationtreatment alternatives has increased in re-cent years due to the increased cost of
incineration, the difficulty associated withpermitting incinerators, and the perceiveddesirability of reducing dependence on incin-erators given concern over their emissions.Alternative treatment technologies such asautoclaving (steam sterilization) with com-paction, microwaving, and mechanical/chemi-cal disinfection are likely to be less capitalintensive and have fewer emission concernsthan incineration processes. Yet, further inves-tigation of treatment alternatives (e.g., health
8~e~e fi&g~, h~wever, ~ be ~ t ed by t h e Mme of t h e e,xisfig &M base ~d litera~e fiom Wtich & findings a r e drawn . Th e number Of
unreported occupational injury cases, the baseline health status of workers, and the significance of potential exposure routes not yet studied (e.g.,aerosolization of substances during r e a tme n~ etc.) ar e crucial un knowns wh ich could strongly impa ct risk det ermina tions of VfiOUS @aWenttechnologies.
%eatrnent methods throughout this report refer broadly to any management technique and processes intended to render the wastes suitable fordisposal. Treatmen t of medical wastes is intended both t o render wa stes noninfectious and to lead to environmentally sound disposal.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 14/82
Introduction, Major Findings, and Policy Issues q5
Photo credit: Extrufix, OrIando, Florida
The diversity of the medical waste stream indicates thatsource separation practices can help target particular
materials/wastes to the most appropriate managementmethod, based on the physical, chemical, and infectious
q
characteristics of that waste.
risks) and determination of appropriate per-formance standards is warranted, as well asconsideration of research and developmentfunding to encourage innovative technologies.
Current regulatory activity at all levels of government tends to encourage incineration
either by focusing most of its activity onincineration and/or by identifying it as apreferred treatment method in regulations orguidelines with minimal attention to alterna-tives. Congress may alleviate concerns overthe difficulties associated with introducingalternative treatment technologies by direct-ing EPA to specify approval or certificationprocesses for treatment alternatives capableof rendering infectious medical wastes non-infectious. A program taking these factors intoaccount might help stimulate the development
of innovative and improved treatment proc-esses.
Incineration remains and is likely to con-tinue to remain a primary treatment methodfor medical wastes for the foreseeable future.Advanced pollution control equipment is be-coming a standard part of many new inciner-ators. An important concern is the impactFederal regulation of air emissions from medi-cal waste incinerators will have when they arefinalized in 1991, since stringent regulationshave been already enacted by some States.
New incinerators for a variety of reasons (asnoted above) are tending to be larger facili-
ties that operate on a more continual basisthan facilities in the past. A number of regional incinerators, either nonprofit/gen-erator or commercial ones, are being planned.Yet some medical waste generators prefer tocontinue managing their own waste in an effortto maintain greater control over their costs andliability. A number of factors weigh in favor of or in opposition to on-site and off-site manage-ment, leaving the particular circumstances of the medical waste generator and the host
community to be the main determinants for thetype of treatment selected.
A fundamental policy issue of importancethat the Federal Government could addressis the extent to which medical wastes are tobe regulated on the basis of their potentialthreat to public health (i.e., infectious na-ture) and their aesthetic characteristics (i.e.,recognizability as a medically related item).That is, Congress could clarify whether thenonrecognizability criteria of MWTA should
remain a part of future regulations by address-ing this issue either as part of the currentResource Conservation and Recovery Act (RCRA)reauthorization or as part of the evaluation of MWTA upon its expiration in 1991.
A need exists for further education about thenature of the risks posed by medical wastesand methods for their proper handling andmanagement for health-care workers, otherworkers at risk, and the general public.These efforts could be undertaken by either orboth the health-care community and the gov-ernment. Such efforts could include instructionfor health-care workers and housekeeping staff exposed to medical wastes and incinerator

8/14/2019 9018
http://slidepdf.com/reader/full/9018 15/82
6 q Finding the Rx for Managing Medical Wastes
operating training for workers responsible formedical waste management.
This brief study discusses what is known regarding
various medical waste treatment technologies andrelated management issues. Possible directions forFederal policy and areas where further informationto facilitate policy development and improvedmanagement are suggested by the study’s findings.
POLICY ISSUES FORFEDERAL ACTION
The reauthorization process for RCRA pro-vides an opportunity to revisit the medical wasteissues first addressed by Congress in 1988. In1991, the completion of the MWTA demonstrationprogram will provide further opportunity to incorpo-rate what is learned from the program and from themandated studies by EPA and ATSDR into thedecision making process for any further Federalaction on medical wastes management.
One possible option regarding medical wasteissues for Congress to choose is to do nothing in thisarea once the MWTA demonstration program and
agency studies are completed. EPA will set airemission standards for medical waste incineratorsand Congress could defer to the Agency, as it has inthe past, for any further policy action as considerednecessary. Given the general concern over EPA’spast reluctance to act on medical waste issues andcurrent efforts at improving waste managementpractices in the country coupled with concern overState variations in the regulation of medical wastes,this appears to bean unlikely course for Congress.
More likely, Congress will address at least someissues regarding medical waste management as partof the RCRA reauthorization, whatever action mayor may not be taken once MWTA expires. 10 Con-gress could move beyond the current approach tomedical waste management and define a morecomprehensive approach. A comprehensive ap-proach might incorporate medical waste into thetype of waste reduction and materials managementapproach suggested by OTA (1 16) for MSW. Suchan approach could, for example, include determi-
nations on the definition of regulated medicalwastes; address waste reduction and recyclinggoals/objectives; encourage the development and
adoption of baseline, uniform standards for eachtype of treatment method; establish a protocol forapproving or certifying new treatment alterna-
tives; and include medical wastes in State wastemanagement plans. In these plans, States could berequired to consider waste reduction options, recy-cling opportunities, capacity needs for treatment,and similar planning issues for medical waste, asthey would be required to do for MSW.
Within this more comprehensive approach tomedical waste management, or independent of it, anumber of other policy issues can be addressed.These include the following:
q
q
q
q
A
Reduction and recycling issues-Greater atten-tion to opportunities for toxicity and volumereduction and recycling of medical wasteswould complement the efforts suggested andbeing adopted throughout the country for MSW.Dissemination of information through the EPAclearinghouse and possibly research and devel-opment (R&D) funding, could bring attentionto these opportunities.Non-incineration treatment technologies—Further investigation of treatment alternatives
is warranted, e.g., health risks; need for per-formance standards (e.g., waste loadings, tem-peratures); operator and maintenance proce-dures, etc.Incineration treatment issues—Monitoring andoperating requirements for medical waste incin-erators and operator training and certificationrequirements could be specified; standards forair emissions and ash management could beestablished.Small generator management-Information and
assistance for households and other nonhospi-tal sources of medical wastes could be madeavailable through the clearinghouse for solidwaste, which RCRA already directs EPA toestablish and the Agency is currently develop-ing.
number of these issues will need to beaddressed by nongovernmental entities, such ashospitals and other generators of medical wastes,the manufacturers of medical supplies, and the
waste management industry. In particular, a hospi-tal or medical facility itself can best identifystandard operating procedures that affect waste
IONote t i t ~ ~ m b e r of b~S on “fi~uS ~Sp=~ of medic~ ~aS t e m~agement ~ve been fi~oduced ~ con~ess, @he focus Of act ivi ty iS ~ely
to center on how medical waste issues are addressed in the reauthorization of RCRA.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 16/82
Introduction, Major Findings, and Policy Issues q 7
Photo credit: R. Guttman
Careful planning and a comprehensive approach to wastemanagement, which may include recycling efforts, are
likely to reap cost savings to a medical facility, as well asenvironmental benefits for its community.
segregation practices, safe handling of waste materi-als, and adoption of waste reduction, reuse, orrecycling practices.
Medical waste management is a small part of ahealth-care facility’s function, but careful plan-ning and a comprehensive approach to waste
management are likely to reap cost savings to thefacility, as well as environmental benefits for itscommunity. This type of planning would involveconsideration of purchasing practices, use of differ-
ent types of products, methods of waste segregation,and selection of treatment option(s) based on consid-eration of the full range of available alternatives. Thebenefits of such efforts may include cost savings tothe facility as well as a reduction in the amount of waste requiring management.
Education efforts regarding the nature of therisks posed by medical wastes and methods fortheir proper handling and management can alsobe effectively undertaken by health-care providers-
for health-care workers, other workers at risk,and the general public. These efforts can includeincinerator operating training and personal protec-tive equipment and instruction for housekeepingstaff exposed to medical wastes. The government,waste generators and others involved in medicalwaste management also can undertake such efforts(see ch. 4).
For example, the American Diabetes Associationhelps educate diabetic patients on the safe disposal
of their syringes (4). The government also couldmake information and assistance for households andother nonhospital generators of medical wastes morereadily available. One possibility is to include sucha focus in the clearinghouse for solid waste beingestablished by EPA, as currently required by RCRA.The resources spent on various education effortswould improve understanding of how medicalwastes can properly be managed, their associatedrisks, and would facilitate adoption of improvedmanagement practices.
Other more specific issues for which policyclarification by Congress will be useful are whetherthe nonrecognizability criteria of MWTA will re-main a part of future regulations; whether shreddingrequirements should or will be adopted; and alsosome specific packaging, transportation, and mail-ing issues.
1lOf these issues, a fundamental one of
critical importance that the Federal Governmentcould address is the extent to which medicalwastes are to be regulated on the basis of their
1 IFOreX~ple, t wo b i l k (s . 2393 and H .R . 3386) curren tly before Congress a ddress t he tr an sportat ion of medicalwaSteS a s it is Pa r t of th e ba c@*g
of waste. The legislation seeks to requ ire th e use of dedicated vehicles for some su bstan ces, such a s medical wastes, to avoid the tra nsporta tion of foodin vehicles used to haul such wastes. The Department of Transportation, however, does not want the authority to regulate b a c k h a u l i n g (as the proposedlaw would grant them) and instead believes the EPA, Department of Agriculture, and the Food and Drug Administration could better take the lead in
determining the necessary stan dards.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 17/82
8 q Finding the Rx for Managing Medical Wastes
potential threat to public health and their aes-thetic characteristics.
Considerable expense can be associated with
managing wastes (e.g., certain IV tubing) that poselittle public health threat but are recognizable asmedical items. A health-care organization officialrecently mused something to the effect that medicalwaste is probably as much in need of an imageconsultant as it is in need of regulation. The adoptionof regulations that treat wastes purely for aestheticreasons reinforces a “bad image” for medicalwastes, or at least the notion that more of this wasteposes hazards than may be true. It may be that themost appropriate treatment criterion with respect to
medical waste is the ability of a treatment system torender wastes noninfectious.
Clarifying the definition of regulated medicalwastes to include only the waste types consideredinfectious based on objective criteria may facilitatespecial management of those wastes that pose thegreatest risk to human health without risking" over-regulation” (e.g., special management of wastes forprimarily aesthetic reasons). Concerns over such‘‘needless and expensive’ requirements are particu-
larly heard from public officials and generators of medical wastes in rural areas or areas where medicalwastes have not been as much of a public concern asthey have in the Northeast and other coastal andmore densely populated areas. The potential impli-cations of national legislation on areas of the countryprimarily concerned with the infectious potential(and not appearance per se) of medical wastes needto be carefully considered and balanced against theneeds of coastal areas and more densely populatedareas. In these areas, the medical waste beach
washups and other waste related problems in recentyears create entirely different waste managementcircumstances.
Another important issue centers on addressing
whether a “level playing field” exists for all theavailable treatment alternatives. Congress mightfacilitate the introduction of new treatment technol-ogies through specification of certification or ap-proval processes for treatment alternatives capable
of rendering infectious medical wastes noninfec-tious. The same testing will not be appropriate for alltreatment technologies and determining potentialrisks and identifying any necessary control measureswill also vary depending on the nature of thetreatment technology.
A protocol to evaluate new technologies by
identifying appropriate tests, establishing standardsto demonstrate effective microbial kill, establishingoperating parameters and evaluating potential riskscould be adopted. Veterans hospitals or otherFederal medical laboratories and facilities mightalso be possible pilot/test sites for new treatment
technologies. Funding for the research, develop-ment, and testing of alternatives would also encour-age innovation and improvement in medical wastemanagement.
It will be an important part of any programregarding the management of medical wastes toinclude a provision addressing how the adequacy of various treatment alternatives (which in fact mightevolve in response to the regulatory program) will beconsidered. As noted, such a program could provideinterim approval or certification status and/or fund-ing for a pilot/test facility to facilitate gathering theinformation necessary to determine whether routine
adoption of the technology would be acceptable.Such a program might help stimulate the develop-ment of improved treatment processes.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 18/82
Chapter 1
Characterizing Medical Wastes and Applying aComprehensive Management Strategy
The Medical Waste Tracking Act (MWTA) of 1988 represents an attempt by Congress to addressthe problems of beach washups and illegal disposalof medical wastes .
1A more comprehensive ap-
proach to medical waste management, one consis-tent with the broader waste management strategyevolving nationally, could be formally established if the issue of medical wastes remains part of thecurrent RCRA reauthorization effort. Medicalwastes need to be put into a broader frame of reference along with other wastes (e.g., municipaland industrial hazardous and nonhazardous wastes)if we are to establish appropriate levels of protectionfor humans and the environment. The relative risksposed by all these types of wastes must be consid-ered when determining appropriate managementmethods for them.
This chapter consists of a brief discussion of thecontext within which the current Federal approach towaste management for other hazardous and nonhaz-
ardous wastes evolved and consideration of theimplications of a broader, more comprehensivewaste management strategy for medical waste.Appendix A to this report provides a short review of MSVTA, the first major Federal effort to addressmedical wastes.
MEDICAL WASTE IN A
COMPREHENSIVE WASTE
MANAGEMENT STRATEGYThe Resource Conservation and Recovery Act
(RCRA),2passed by Congress in 1976, is the major
Federal statute addressing management of the Na-tion’s wastes—hazardous, municipal, industrial, andother types of solid waste, including medical waste.
3
EPA has authority under RCRA to regulate thehandling, storage, treatment, transportation, anddisposal of all of these wastes. Before passage of MWTA, EPA’s activity regarding medical wasteissues was mostly limited to distribution of itsguidance document for the management of infec-tious wastes. Other medical wastes were consideredto be like any other solid waste and subject torelevant RCRA Subtitle D regulations (114).
OTA finds four key challenges which need to beresolved for medical waste management:
1.
2.
3.
4.
The
better defining/identifying infectious and othermedical wastes, to facilitate more consistentand adequate handling and treatment of wastes;
better addressing the diversity of generators(e.g., home health care, small doctors’ offices,clinics, etc.) to minimize contradictory re-
quirements and inequities they pose;improving the segregation of wastes for theirproper treatment; and
identifying appropriate treatment alternatives.
very nature of these issues indicates that acomprehensive, flexible, yet cost-conscious ap-proach is needed for medical waste management.These challenges can be met by a broader approachto medical waste management that emphasizeswaste prevention efforts and management of differ-ent portions of the medical waste stream based ontheir physical, chemical, and biological (i.e., infec-tious) properties. Such a comprehensive approach towaste management is beginning to be applied tohazardous waste and more recently to municipalsolid waste (MSW).
ICongress alSO amended the Marine Protection Research and Sanctuaries Act (also known as the Ocean Dumping Act) h 1988 to fif=ase thepenalties for illegal disposal of medical wastes by public vessels (33 U.S.C. 1401 et seq.). See app. A and (115) for dis cussion of MWTA.
Zwbhc bW 94-580 (1976); 42 U.S.C. 6901 et seq . The Solid Waste Disposal Act of 1965 (Public Law 89-272; as amended by the Resource RecoveryAct of 1970, Pu blic Law 91-512) was t he law by which Congress first est ablished a F~e r a l role in solid waste ma na gement. The most recent majorrevision of RCRA was by t he H azard ous an d Solid Waste Amendmen ts of 1984 (Pu blic Law 98-616), which id not addr ess medical waste issues in
any detail. RCRA is currently in the process of further revision and reauthorization.30m (1 15 ) recenf ly c o m p l e t e d its assessment of municipal solid waste, of which the 1988 background paper on medical wastes wa s a Par t . Cur renf lY ,
OTA is completing a background paper on industrial solid (Subtitle D, RCRA) waste issues (expected to be rdeased in early 1991). Hazardous wasteissues h ave been addr essed by several OTA reports (e.g., 112, 113).
It sh ould be noted tha t t he following discussion is based in pa rt on r ef. 137.
-9 -

8/14/2019 9018
http://slidepdf.com/reader/full/9018 19/82
10 q Finding the Rx for Managing Medical Wastes
Photo credit: L. Swanson
Beach washups containing medical debris, such assyringes, helped prompt passage of the MWTA.
Subsequent studies indicate the sources of most washupsto be related more directly to sewage treatment systems
operation than illicit waste management practices.
There is some consensus that at least portions of the medical waste stream can be treated like otherMSW. Indeed, in practice this appears to occur. TheCalifornia Air Resources Board reports, as notedabove, that typically 40 percent or more of the wasteburned by medical waste incinerators in their Stateis waste, comparable to MSW in nature (106, 108,29).
4Available evidence also seems to indicate that
most medical waste poses no more public health orenvironmental hazard when properly handled than
does MSW (109, 56, 107, 139). Yet, when medicalwaste is incinerated (or treated by some other means)its emissions may be hazardous if not properlycontrolled (as is the case with any other waste).Thus, basic policy determinations regarding man-agement approaches, and weighing risks and costs,etc., are common to any waste problem.
It is instructive to consider the current trends inhazardous waste and MSW treatment in which thereis a movement away from treatment methods that
manage indiscriminately mixed wastes and towardsource separation programs that encourage manage-ment based on the properties of the materials in the
wastes (e.g., recyclability, ability to destroy orneutralize, etc.). OTA’s assessment of the MSWissue found that environmentally sound waste man-agement requires focusing on how the Nation usesmaterials from manufacturing through subsequentdistribution and disposal (116). On this basis, OTAconcluded that,
A clear national policy on MSW that addressesthe use of materials is essential for providing abroader context in which specific MSW programscan be developed and implemented. Waste preven-tion and materials management should be thefoundation of this policy.
The basic steps are: 1) characterizing the wastestream in light of categories used for differentalternative treatment options; 2) segregating wastesat the point of origin to facilitate management basedon their characteristics; and 3) examining theproduction of the waste, i.e., looking upstream toconsider possible opportunities for waste reduction(in either volume or toxicity) that may include use of different products which are reusable or recyclableor contain less problematic substances for wastetreatment.
For example, government agencies and/or thehealth-care industry could examine prospects forwaste reduction in health-care settings (see ch. 2).Although the growth in the volume of medicalwastes is not well documented, there is generalacknowledgment that the use of disposable inhealth care has increased significantly in the last twodecades. Clearly, in some cases the use of disposa-ble is important for infection control. Yet, thoseuses driven primarily by economies may need to be
reassessed (see ch. 2).From a management perspective, the presumption
held by some regulators and members of interestgroups that incineration is the “preferred’ treatmentoption for medical wastes warrants closer examina-tion. Most of the recent regulatory activity formedical waste management at all levels of govern-ment tends to focus on incineration and does notusually include specific procedures for the regula-tory approval of nonincineration alternatives.
For example, the “treat and destroy or track”requirement of MWTA does not include a proc-ess with specific criteria for how the standard can
4B~~~d on ~~ m e of ~omation, ~~~~ion d a t a from medic~ an d MSW facilities ca n be c o m p a r ~ , a s l o n g as t h e &p e a n d s i z e of incinerator Or
other technology and the mix of wastes is taken into account (see ch . 5).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 20/82
Chapter 1-Characterizing Medical Wastes and Applying a Comprehensive Management Strategy q11
be met by various treatment alternatives, anddoes not specify how new non-incineration treat-ment alternatives can be introduced. A number of such alternatives (e.g., several types of disinfection
units) are commercially viable and warrant consider-ation (see ch. 3).
Further, a number of unanswered questions re-main regarding incineration, e.g., the nature of emissions and proper controls, the nature andadequate treatment of ash residues, and the costcompared with alternative management methods(see ch. 4). Information on operating parameters,risks, and costs for various alternative treatmentmethods is also needed. As with the hazardous and
solid waste streams, a combination of managementoptions may prove optimal for managing medicalwaste once the material composition of its compo-nents is considered.
That is, landfilling, incineration, and othertreatment alternatives, as well as recycling andwaste reduction all may be viable managementoptions for medical waste—when it is consideredon a waste component basis. Ultimately, this mayhelp to control costs and minimize any hazardsassociated with medical waste management. This isone way, given the experience gained in regulatingother waste streams, that programs to managemedical wastes can be devised wisely and efficientlyin order to alleviate public concern, protect workers,and provide environmental protection.
WASTE CHARACTERISTICS AND
TYPES—TREATMENT
IMPLICATIONS
Examining various treatment options underscoresthe importance of considering the properties of different types of medical waste and matching themto the capabilities of the treatment technologies.Although the medical waste stream is hetero-geneous, the focus of concern is on the portion of thewaste stream termed ‘‘infectious, ’ and how thesewastes are classified (e.g., solid, hazardous, orspecial) and regulated. The regulated waste stream,
i.e., the medical wastes covered by MWTA, includesinfectious, potentially infectious, and some wastesidentified as requiring special handling. Most esti-mates are that 10 to 15 percent of medical wastes
generated by hospitals are infectious, although thisfigure can range as high as 80 percent depending onthe generator’s definition. Determining which por-tion of medical waste is infectious remains at theheart of definitional issues. How infectious waste isdefined can greatly affect the cost of waste manage-ment, and ultimately the choice of disposal options(114).5
Currently, both aesthetic considerations andhealth risks posed by medical wastes can lead to the
classification of a medical waste as infectious and/orregulated and requiring special management. TheState of Washington has defined infectious wastebased on risk criteria, particularly the determinationof “infectious disease causation potential’ (139). Aconsensus on which medical waste warrantsspecial regulation and management might beforged if the definition of regulated medical wasteis based on the potential health risks associatedwith the waste (i.e., the ability of a particularmedical waste-given organism concentration,ability of the waste to penetrate skin, etc.—topose a risk beyond that associated with MSW totransmit infectious disease).
As noted, no consensus exists on the types of medical wastes that should be designated as infec-tious or that require special handling, althoughseveral categories of wastes are included in mostlists (114; also see table 2). Under MWTA (seebelow), EPA has listed seven types of medical waste(commonly and hereafter refer-red to as “regulatedwaste types’ to be tracked in the demonstrationprogram. These are:
1. microbiological wastes (cultures and stocks of infectious wastes and associated biologicalthat can cause disease in humans);
2. human blood and blood products (includingserum, plasma, and other blood components);
Ssome confusion was created over the Cent ers for Disease Control (cDC) universa l precaut ions guidan ce issued in August 1987 , t it suggestti t itall patients be considered potentially infected with human immunodeficiency virus (HIV) (i.e., the virus wh ich cau ses acquiredmmunodeficiency
syndrome, AIDS) and/or other blood-borne pathogens and that workers should adhere to rigorous infection-control procedures. In October 1987, CDCissued a joint advisory notice with th e Departm ent of Labor furth er addr essing protection aga inst occupa tional exposure to Hepatit is B (HBV) and H IV.After these advisories led to a great inflation of the amount of waste designated as infectious, the CDC issued a cltilcation in August 1988, indicatingto which types of secretions and circumstances its recommendations applied and that CDC did not intend for generators to alter waste mamgementprocedur es, but only mean t to protect health -care workers. In May 1989, the Occupational Safety and H ealth Administ rat ion (OSHA) of th e U.S.Department of Labor issued a proposed job hea l t h standard for protecting health-care workers from blood-borne diseases.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 21/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 22/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 23/82
Table 3—Percentages of Waste Types Produced at Different Medical/Health-Care Facilities in the State of Washington
Type of facility
SurgeryAll cases Total Funeral Nursing Vet Lab centers Hospital Clinic Dental Research Medical
Wastes produced (*) ... , . . . . . . . . . . . 100% 1 00% 100 ”/0 1 00% 1 00% 100”/0 100”/0 100% 100% 10070 10070(350) (32) (43) (49) (25) (8) (51) (60) (32) (17) (33)
Wastes with excretions/secretions , ., 75 91 84 64 63 96 70Microbiological , ., . . . . . . . , . . . . . . . . . 42 0 16 41 44 25 92 57 3 65 42Human blood and blood products . . . . 56 88 23 2 88 38 96 63 44 53 64Animal blood and blood products . . . . 15 0 0 69 12 0 10 0 0 59 3Pathological . . . . . . . . . . . , ., ., . . . . . . 44 28 5 86 32 50 88 32 31 24 30Sharps . . . . . . . . . . . . . . . . . . . . . . . . . . 94 94 98 96 92 100 98 87 91 88 100Wastes from surgery . . . . . . . . . . . . . . 64 69 16 92 8 88 98 67 78 12 76Dialysis unit wastes ., . . . . . . . . . . . . . 7 19 0 0 0 0 25 5 0 6 3Contaminated animal carcasses/
bedding . . . . . . . . . . . . ., . . . . . . . . . 14 3 0 76 0 0 4 0 0 47 0Isolation patients’ wastes ., . . . . . . . . . 32 47 77 37 8 0 78 5 0 0 6Radioactive wastes ... , ., ., . . . . . . . . 15 0 0 0 40 0 49 10 0 53 9Chemotherapy wastes . . . . . . . . . . . . . 18 9 2 10 12 13 69 15 0 0 18None of the above ., . . . . . . . . . . . . . . 3 3 0 0 8 0 2 10 3 6 0
(*) percentages may not add to 100 percent because of multiple responses.
SOURCE: Washington State Department of Ecology, Solid and Hazardous Waste Program, “Report to the Legislature: Washington State Infectious Waste Project and Attachments” (Olympia, WA:Dec. 30, 1989).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 24/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 25/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 26/82
Chapter l--Characterizing Medical Wastes and Applying a Comprehensive Management Strategy q 17
Table 4-Characteristics of Medical Waste
Bulk density as fired Moisture content as fired Heating value as fired
Waste component (Ib/cu.ft.) (weight percent) (Btu/lb)
Human anatomical ... , . . . . . . . . . . . . . . . . . . . . . . . . . 50-75 70-90 800-3,600Plastics , . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5-144 0-1 13,860-20,000Swabs, absorbents ., ., . . . . . . . . . . . . . . . . . . . . . . . . . 5-62 0-30 5,600-12,000Alcohol, disinfectants . . . . . . . . . . . . . . . . . . . . . . . . . . . 48-62 0-0.2 10,980-14,000Infected animals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30-80 60-90 900-6,400Glass ... , .., , . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175-225 0 0Bedding, shavings, paper, fecal matter . . . . . . . . . . . . . 20-46 10-50 4,000-8,100Gauze, pads, swabs, garments, paper, cellulose . . . . 5-62 0-30 5,600-12,000Sharps, needles ., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 450-500 0-1 0-60Fluids, residuals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62-63 80-100 0-2,000
KEY: 1 Ib/cu.ft. = 16.03 kg/m3
1 Btu/lb = 2.324 J/g
SOURCE: T. Milburn, “Biomedical Waste Incineration BACT Application Considerations, ” Proceedings of the Third National Symposium on Infectious Waste
Management, Chicago, IL, April 1989, as cited in R. Barton, G. Hassel, W. Lanier, and W. Seeker, State of the Art Assessment of Medical WasteThermal Treatment EPA Contract 68-03-3365 and ARB Contract A832-155 (Irvine, CA: Energy & Environmental Research Corp., 1989).
this effort will be reported in the Agency’s finalreport to Congress, although EPA anticipates thatfurther studies on the issue beyond this effort maybewarranted (14 1).
Disinfection rates for nonincineration treatmentalternatives can also be high, if the treatment systemis properly designed and operated. A source of general concern and confusion is the extent to whichvarious treatment alternatives ‘‘disinfect’ medical
wastes. The efficacy of a treatment method shouldbe demonstrated by development of an appropriatebiological testing program. It appears reasonablethat the degree of disinfection not be required toexceed microbial and virulence levels that maygenerally be found in MSW (111).
Physical Characteristics
The basic physical forms of medical wastes (solid,liquid, and gas) should be taken into account for their
handling and management. Segregation of wastes byhealth-care facilities into types based on thesephysical states is likely to occur, e.g., liquid wastes,non-sharp/solid wastes, sharp wastes (see tables 4and 5).
Both physical characteristics (e.g., heat value andmoisture content) of waste components and thebiological make-up and chemical (elemental) composi-tion of the waste are important determinants of themost appropriate treatment technology and haveimportant impacts for that treatment. Despite the factthat medical waste is heterogeneous in its physicaland chemical nature, the waste is rarely managedinitially as a mixture of all the wastes from thefacility. That is, it is likely that a medical facility will
Table 5-Comparison of the Composition of
Medical and Municipal Waste
Amount in waste,percent by weight
Medical Municipal HazardousWaste component waste waste wastea
Dry cellulosic solids . . . . . . . . . 45.1 54.2 0Wet cellulosic solids . . . . . . . . 18.0 12.2 0Plastics . . . . . . . . . . . . . . . . . . 14.2 7.4 12Rubber . . . . . . . . . . . . . . . . . . 0.7Solvents . . . . . . . . . . . . . . . . . . 58
Noncombustibles . . . . . . . . . . 20.4 26.2Pathological . . . . . . . . . . . . . . . 1.6Heating value (Btu/lb) . . . . . . . 6,000 4,335 6,030
aFOr a typICaI comrneraal incinerator accepting a broad range Of wastes.1 Btu/lb = 2.324 J/g
SOURCE: D. Campbell, “Hospital Waste Management in Canada,” Pro-
~wadings of the Nat]onal Workshops on Hospital Waste inciner-
ation and Hospital Sterilization, U.S. Environmental Protection
Agency, San Franciscx, CA, May 19843, as cited in R. Barton, G.Hassel, W, Lanler, and W. Seeker, State of the Arf Assessmentof Medical Waste Thermal Treatment, EPA Contract 68-03-
3365 and ARB Contract A832-155 (Irvine, CA: Energy &
Environmental Research Corp., 1989).
collect wastes from various departments separately
(i.e., computer printouts are collected from theaccounting department; kitchen waste, patient waste,etc. are collected separately), although they may bemixed for treatment (e.g., incineration) (12, 139).
Given the important impact chemical characteris-tics of wastes can have on the effectiveness of various treatment technologies to safely managemedical waste, it appears sensible to keep wastesseparate based on their physical and chemicalproperties, at least as carefully as possible intohazardous, solid, and regulated medical/infectiouswaste categories, to ensure the wastes receiveappropriate treatment/management. This will be truewhether incineration or nonincineration treatment

8/14/2019 9018
http://slidepdf.com/reader/full/9018 27/82
18 q Finding the Rx for Managing Medical Wastes
technologies are used. It will also facilitate efforts torecycle wastes when feasible and identify opportuni-ties for waste reduction.
EPA adopted as part of its regulations underMWTA (40 CFR Part 259) segregation requirementsto control and reduce costs for waste disposal andminimize worker exposure to certain medicalwastes. The Agency reports, however, that facilitiesin MWTA demonstration program base their segre-gation policies primarily on the basis of convenienceand barriers associated with reeducating their staff to
change management practices (141). A recent studycommissioned by the New York City Health &Hospitals Corp. and conducted by Waste Tech, finds
that facilities required to comply with MWTA couldreduce the cost and volume of their waste manage-ment through more careful segregation and reduc-tion practices (62, 63). Waste management compa-nies also report that segregation at the point of generation is key to containing handling and treat-ment costs, as well as assisting in appropriaterecycling opportunities (43) (see ch. 4).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 28/82
Chapter 2
Before Treatment: Waste Reduction and Recycling
Waste management concerns now confronting themedical waste generator are largely reflective of thegeneral movement toward minimizing the quantityof waste warranting disposal. Effective managementof medical waste incorporates a waste reduction andrecycling component where appropriate. These ac-tivities should be fostered via policy incentives.
This chapter explores the implications of applyinga waste prevention and materials management ap-proach (ch. 1) to medical wastes by considering
“before treatment” approaches to controlling medi-cal wastes. This exploration includes a discussion of careful on-site planning, and waste reduction andrecycling opportunities in health-care facilities.
BEFORE-TREATMENTAPPROACHES
Lessons from the management of other wastestreams, notably hazardous waste and MSW, indi-cate that (as noted in ch. 1) a sound control strategyfor waste management follows the basic steps of characterizing the waste stream in light of differenttreatment alternatives, segregating some wastes tofacilitate management based on these characteris-tics, and looking “upstream” to discover anyopportunities to reduce the volume and/or toxicity of waste. Achieving this strategy requires some form of planning to garner the necessary information forreduction and management decisions.
The value of on-site management plans or strate-gies appears to be gaining r e c o g n i t i o n a s m o r e
medical and health-care facilities grapple with howto respond to increasingly complicated regulationsfor waste management (94). Waste audits of someform are becoming more common in hospitalsand other medical institutions. The advantages of these waste audits or more comprehensive plans fora facility include using the information they providenot only to devise a strategy for compliance withenvironmental requirements, but also to determinethe most cost-effective means to meet requirementswithout compromising the quality of patient care
and to identify waste reduction, reuse, and recyclingactivities as well as other management options thatcould be adopted.
Every facility must tailor its own strategy basedon its characteristics, but several areas should beaddressed in any attempt to analyze waste options.First, the definition and segregation of wastesshould be examined because facility standard oper-ating procedures (SOPS) for waste segregation havea direct impact on type and cost of medical wastetreatment. For example, sometimes when a facilitydesignates “surgery waste” as infectious waste allwaste from that department is managed as infectiouswaste, some of which could be managed as nonin-
fectious (e.g., paper from the administrative area).
Second, the types of products and packaging(e.g., for wastes) used in the facility and their impacton the waste stream can be considered, withoutcompromising infection control goals. For example,woven linens may be substituted for some applica-tions of disposal linens with little risk of increasedinfection potential; and, based on preliminary datafrom the New York City Medical Waste Study,considerable reduction in the volume of waste and
significant cost savings (see box B) (62, 63, 94).Careful purchasing might help reduce the level of toxic emissions from an incinerator. Finally, thetypes of on-site versus off-site disposal optionsavailable to a facility need to be considered fromhandling and management perspectives and theircosts and risks compared.
WASTE REDUCTION
Source reduction, or prevention, of waste is
defined by OTA as “activities that reduce thetoxicity or quantity of discarded products before theproducts are purchased, used, and discarded” (1 16).
1
Source reduction can be achieved by: 1) manufactur-ers considering waste issues in designs of currentand planned medical and health-care products andtheir packaging; and 2) consumers of medical andhealth-care products (e.g., hospitals) directing theirpurchasing decisions, product use, and the discard-ing of products toward waste reduction goals. Thetwo fundamental characteristics of wastes that are
the focus of reduction efforts are: toxicity, i.e.,eliminating or finding benign substitutes for sub-stances that pose risks when they are discarded; and
IA basic distinction is made between prevention and management, the latter occurring after Waste is generated.
–19–

8/14/2019 9018
http://slidepdf.com/reader/full/9018 29/82
20 q Finding the R X for Managing Medical Wastes
Box B—Disposables: Infection Control and Waste Management Implications
It appears that the use of disposable can be carefully tailored, from an infection control perspective, to those
procedures where disposable have the greatest benefit (e.g., isolation situations). Based on a literature search of research to date, OTA found that handwashing is widely considered to be the most important barrier to transmissionof infections (119, 53, 59, 61). A clear understanding of modes of infection transmission and the factors that affectit can ensure that the most effective infection control practices are undertaken (53, 59,98, 105). Measures to controlinfections include handwashing, the use of sterile disposable items, and other measures (e.g., closed urinarydrainage, intravenous catheter care, nontouch dressing techniques, and proper care of respiratory equipment andperioperative chemoprophylaxis) (119, 120, 53).
In some cases, the benefits of isolation (in which typically disposable, nonwoven polypropylene gowns andnonsterile latex gloves are used) have been demonstrated for reducing the incidence of nosocomial bacterial andfungal infection, particularly in cases of prolonged (more than one week) intensive care for a patient (64). Yet, oftenthe sources of infections in hospitals are discovered to be related to misuse of medical equipment andperson-to-person transmissions. In one London hospital, the investigation of a number of incidents of
cross-infection with an antibiotic resistant infection (Klebsiella aerogenes) led to the conclusion that, ‘While manyunits practise [sic] almost ritual cleansing of selected equipment, and rely heavily on disposable, there are oftencircumstances when the misuse of simple ward equipment [in this case, contamination of portable suction apparatus]becomes an accepted routine with inevitable consequences” (37a).
Some infection control measures are proven and standard practices for every hospital, while others aresupported by less extensive studies, and some proposed measures are not supported by study data (e.g., floordisinfection). A disposable item maybe in any one of these categories regarding its value as an effective infectioncontrol measure depending on the particular item and its use. Studies have found, for example, that nonwovendisposable gown and drape fabrics were no better barriers to infection than reusable, woven, cotton gowns anddrapes; and, in point of fact, the protective value as well as the transmission potential of gowns, shoe covers, andeven masks has been questioned (50, 16, 59).
1Potential volume reduction of disposable linens and medical
apparatus could be considerable, perhaps between 30 to 60 percent depending on the specific health-care facility(63).
With other disposable items, e.g., some catheters and syringes (by diabetics), reuse is not a simple yes-or-noissue. Studies to date indicate that morbidity associated with reuse of cardiac catheters, for example, is low (46, 37,60). With regard to the reuse of disposable syringes, it appears both safe and practical for diabetics to use disposablesyringes and needles for more than one injection (4, 52, 23, 90, 46).
2
Nonetheless, the practicality of reuse, given liability concerns and standard operating procedures for aparticular health-care facility, may preclude reuse of particular medical items at an institutional level.
3Certain
disposable items though are advantageous over reusable items for various reasons including controlling infection,saving labor costs for processing, and minimizing exposure to hazardous chemicals used in chemical sterilizationprocesses. The use (and reuse) of disposable can be considered on an item by item basis, in light of how they willbe used, including consideration of infection risks and other factors associated with those risks. Some institutionsare beginning to examine the opportunities for use of fewer disposable and other waste reduction options (seebelow).
lb my ~~e, one s~dy r e p o r t s t h a t l i n e n pos e s a higher infection risk to laundry workers tin to patients (Zla).
21 t should be noted that these studies focused on th e reu se by the sa me pa tient, i.e., a diabetic, u s i n g t h e Same S@nge. Dhbetic pat i~ ts
who used the same plastic disposable syringe (up to 7 days) were not found to develop infection at the site and little or no c o n t amma“ tion of thesyringes was found (23, 90).
The Amer ican Dia betes Associat ion (ADA) in it s Position St atement on Insulin Administra tion sta tes th at although manufacturers of disposable syringes recommend tha t t hey be used only once, most insu lin prepara tions have ba c t e nos t a t i c additives to inhibit growth of bacteriacomm only found on th e sic@ an d genera lly “it appea rs both sa fe an d pra ctical for th e syringe to be reused if the pat ient so desires” (4). Thesyringes must be discarded wh en th e needle is dull or if it becomes c o n t am i n a ted in some way. The ADA stat ement a lso discusses the importan ceof such practices as good personal hygiene and proper handling of syringes (i.e., procedures to recap a syringe safely) by patients.
3Th e potential for ~c r~sed Habfi ty of a he~th-cme facility using nondisposables v. disposable for different medical a p p t i C a t iOm ~been ra ised. OTA asked only one insura nce company about t his concern a nd was told that insura nce companies insure for n egligence anddistinguish between real an d perceived risk in such a wa y that the u se of disposable v. nondisposables would not usually matter ho rn a liabilityperspective. It was also noted that insura nce companies do attempt to ensure t hat proper procedures ar e followed to help keep risks as low aspossible (15).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 30/82
Chapter 2-Before Treatment: Waste Reduction and Recycling q 21
quantity, i.e., changing the design or use of productsto minimize the amount of waste generated whenthey are discarded.
For waste reduction, reuse, or recycling to occurwithin a medical facility, a waste audit that empha-sizes characterization of the waste stream anddevelopment of a plan delineating necessary segre-gation techniques and education/training of theapproach to be taken to the employees of thehealth-care facility is necessary. Currently, mosthealth-care facilities resist waste segregation be-cause of its perceived inconvenience and the diffi-culty of ensuring staff compliance. The increasedcosts associated with new regulatory requirements,
however, are creating an economic incentive forgreater waste segregation by health-care facilities.
From both volume and toxicity perspectives, theuse of plastics in society is a focus of wastemanagement concern. EPA’s recent report on plas-tics in MSW found that plastics production has hadan average annual growth of 10 percent for the last30 years (132). The report also noted that “sourcereduction and recycling are the best way to reducepotential environmental impacts from plasticwastes” and discusses a number of activities EPA
will undertake toward these ends. A higher percent-age of plastics is contained in medical wastes than inMSW, approximately 20 percent (by weight) inmedical wastes (and perhaps higher)
2and slightly
under 10 percent (by weight) in MSW (1 14, 116).3The medical community is projected to consume 2.4billion pounds annually by 1994 (13).
As in general public use, plastics are utilized forboth products and packaging. While single-usedisposal plastic items are often preferable from an
infection control perspective, other forces havestimulated the use of these products. For instance, tofacilitate pricing patient procedures individually,disposable products are individually wrapped tomake bookkeeping easier both internally and forthird-party reimbursement. Certain internal prac-tices within health-care institutions reduce wasteeven if they were not initially developed for thispurpose. For instance, inventory programs that keeppackaging and corrugated cardboard boxes out of thehealth-care facility, and often times discourage
single-item packaging, can have a positive effect.
Photo credit: R. Guttman
Corrugated cardboard-including that used to speciallypackage regulated medical waste s-can comprise asignificant portion of a hospital’s waste stream. Somehospitals have purchased balers to facilitate handling
and marketing of reclaimed cardboard.
Procedural trays that are prepackaged by distributorsreduce individual packaging and put all necessaryproducts for a procedure within a single container.
The type of plastic used and its impact on wastetreatment is one example of how waste reductionefforts focused on reducing certain emissions canlink pretreatment and treatment management efforts.The higher concentrations of hydrogen chloride(HCl) in emissions, on average, from medical wasteincinerators compared with MSW incinerators maybe due to the higher levels of polyvinyl chloride(PVC) plastics in medical wastes. Almost all of thechlorine in these wastes is converted to HCl duringthe combustion process (assuming a high combus-tion efficiency). In this way, chlorinated plastics
may contribute to the high emission rates of HCl and%%e recent survey of New York City hosp i t a I s foun d 26 percent of medical wast e to be plast ics (63).
3Ye. @ven t it ~edic~ wa s t e is a ~m ~ p e r c e n ~ g e of MSW, it is l ikely ~t m e fofu/ r e l e ~e of H C1 from m~ic~ wrote incinera tion is compara bly
lower (despite the higher concentration). In a local a r e% however, it could be a s i gn i l l c a n t source of such em issions.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 31/82
22 q Finding the Rx for Managing Medical Wastes
possibly the formation of dioxins (particularly if combustion efficiency is low) (114).
PVC plastics were reported to account for 9.4percent of the weight of infectious wastes in onestudy of two Houston hospitals (cited in 139).
4
Concerns over hydrogen chloride generationthrough on-site incineration, as well as off-site, havebegun to put pressure on the producers of plasticmedical products to switch from polyvinyl chlorideplastic to one that does not carry the same type of environmental concerns, such as polyethylene (51,43). Unfortunately, because of certain physicalcharacteristics, the PVC plastic is more desirable in
certain products. Increased efforts to find alternatematerials for products such as intravenous tubingshould be encouraged. For other products, such asslide holders, trays, and garbage bags, manufacturersmay be able to easily substitute materials (139, 43).
Sometimes there can be a direct tradeoff betweenthe potential environmental harm caused by onemanagement practice versus another. For example,the issue of whether using disposable or reusableitems is “better” can be difficult to determine. It
will depend on which particular goal (e.g., infec-tion control, convenience/labor savings, cost sav-ings, safe waste management) is deemed mostimportant regarding the product’s use. Oneexample of where such a determination has to bemade regards the use of products and equipmentgenerating chlorofluorocarbon (CFC) emissions,which are used by the medical and health-careindustry to sterilize reusable items for patientprocedures.
The medical and health-care industry is responsi-ble for less than 4 percent of the total amount of CFCs released to the atmosphere. Given the con-cerns over the association of CFCs with ozonedepletion and possible global warming effects, theAmerican Hospital Association has recommendedthat hospitals reduce consumption of all CFC-basedproducts and chemicals used for sterilization pur-poses.
5This reduction can be achieved through the
use of disposable, but any significant growth in theuse of plastics containing CFCs might negate overall
CFC reduction. It maybe that other solutions wouldavoid greater contributions to the medical and solid
waste streams, e.g., the greater use of steam steriliza-tion or other substitutions for CFC-dependent steri-lization systems, or use of non-CFC, recyclableplastics (76, 129).
The increased use of disposable in health-caresettings is widely acknowledged, if not well docu-mented. Battelle recently has undertaken a project,Medpak, to study the consumption, use, and disposalof medical products and packaging by health-carefacilities in order to assist health-care productcompanies to develop products, packages, andprocess concepts that would reduce the volume andcost of managing medical wastes by hospitals andother medical facilities (13).
The growth in the use of disposable in health-care settings is attributable to a number of converg-ing factors in recent decades. These include:
1.
2.
3.
4.
One
increased concern over infection control;
decreased available nursing staff (and a need toprovide more expedient treatment and moreconvenient clinical practices);
increased cost of health-care labor (and con-cern over the time needed to handle and
sterilize reusable items); and
consideration of disposable as part of thegeneral solid waste stream of the health-carefacility (with, in the past, resultant low cost forhandling and disposal) (94, 17).
widely held presumption is that the use of disposable is important from the perspective of infection control. Nosocomial (hospital-acquired)infections are a serious concern in U.S. hospitals,with 2 to 15 percent of all in-patients acquiring themand millions of dollars spent to control them (37).
Yet, infection control studies do not indicate aconstant and consistent reduction in nosocomialinfections where disposable replace reusableproducts. Other factors also come into play (seebox B). Competing concerns over the cost, andmore recently the waste implications, of usinglarge quantities of disposable in health-carefacilities are now being raised, particularly forproducts that do not have a direct effect on
infection control and patient care (e.g., disposa-ble telephones).
4~es of plastics in products ordered by hospitals include: polyvinyl chloride, polyethylene, polypropylene, polystyrene, and polyurethane (139).
SH~ t h fisks t . employ=s proc.~sfig ~~pment vi a ethylene Ofide ~te~~tion also p r om p t ~ c o n ~ m s . Often e q u ip m e n t s t e r i l i z e d b y t h i S IIMMIM,
however, cannot be steam sterilized because damage to the equipment wou ld result .

8/14/2019 9018
http://slidepdf.com/reader/full/9018 32/82
Chapter 2-Before Treatment: Waste Reduction and Recycling . 23
RECYCLING AND SOURCESEPARATION PRACTICES
In addition to reduction efforts, source separationpractices (i.e., segregation of materials as they arediscarded based on their characteristics) that targetparticular materials/wastes for recycling and themost appropriate treatment method can lead to moreenvironmentally sound medical waste management.Source separation before incineration or any othertype of treatment has been shown to improve theoperation of MSW incinerators, and the same maybe true for medical waste treatment as well (1 16).
Most health-care facilities segregate infectious andnoninfectious waste streams, but separation of otheritems for recycling may also facilitate managementefforts. Yet, any recycling efforts must also considerand address the potential of increased exposure towastes to health-care workers and waste handlersfrom such management efforts.
A number of hospitals are adopting recyclingprograms as part of their waste management pro-
grams, although in the past little recycling hasoccurred by hospitals. A recent reported surveysponsored by the Greater Boston Chamber of Commerce found that hospitals were discarding tonsof waste that could be reused or sold and were payingmore than other businesses to dispose of noninfec-tious, commercial solid waste. Hospitals in thismetropolitan area, including Massachusetts GeneralHospital and Beverly Hospital, however, have begunpaper recycling programs (9).
Some health-care facilities are planning anddeveloping comprehensive waste management pro-grams, of which recycling is an integral part. Forexample, Bayfront Medical Center(a518-bed acute-care community hospital) in St. Petersburg, Florida,has proposed a recycle-and-reclaim project in con-
junction with its proposed waste-to-energy system(see figure 1). This system represents a comprehen-sive waste strategy designed to recycle materials aspossible, effectively render infectious medical wastenoninfectious, reduce the amount of waste going toa landfill, generate energy to power the hospital’slaundry, and reduce some of the risks and costsassociated with waste management (14).
Figure l—Schematic of One Hospital’s Proposed
Segregation Categories and Comprehensive MedicalWaste Management Approach
Pharmacy &
Patient care
Food Off Icelaboratory Housekeeping &
services supplies medicalsupplies supplies
I
H o s p i t a l
1
[
Off Ice paperAluminum cans
Green barRegulated Cardboard
Selected plastics Batteries medical &
Selected glasscomputer
waste food wastepaper
I I
SOURCE: Bayfront Medical Center, St. Petersburg, FL.
Cardboard, food, and other general wastes cancomprise as much as 85 to 90 percent of a hospital’swaste stream, with pathological and infectiouswastes comprising the rest (29, 12).
6Some hospitals
are beginning to focus on the nonpatient sources of wastes in their facility and target materials forrecycling. For example, corrugated cardboard, com-puter paper, cans and bottles, and other items (whichcan contribute metals, particulate, and volatiles toflue gas emissions from incinerators) can be segre-gated for recycling. Batteries and other non-combustible items that can contribute air emissionsof cadmium and lead from incinerators, or if state-of-the-art air pollution control equipment is inplace can affect the ash, can also be segregated formore appropriate management efforts.
A Department of Energy study of three MSWincinerators found that presorting not only reduceduncontrolled emissions significantly, but also led to
~s estimate is based on hospital survey information reported by Cross (30), see also Cross data cited in (12).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 33/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 34/82
Chapter 2-Before Treatment: Waste Reduction and Recycling . 25
Photo credit: R. Guttman
Increasingly hospitals are adopting recycling programs to help reduce the volume of waste requiring disposal.
publicity efforts associated with the Beth IsraelRecycling Program (67).
The Iroquois Healthcare Consortium, located innortheastern New York, has implemented an ag-gressive effort to educate its 56 member facilitiesand assist them in developing and implementingcomprehensive recycling programs. The region’ssuccess stories include the Albany Medical Center,which currently recycles over 350,000 pounds of cardboard, paper, glass, aluminum cans, and plasticannually. The region has also developed successfulprograms working closely with local government. InOtsego County, New York, the A.O. Fox Hospitaland Mary Imogene Bassett Hospital are two commu-nity hospitals that have worked closely with countyofficials to develop and implement an effectiveprogram now being used as a model in the develop-ment of the region’s recycling program (94).
In several areas of the country, commercial wastesfrom institutions such as health-care facilities areincluded in community recycling programs. In thesesituations, the special nature of the medical wastestream should be taken into account by localplanners (e.g., the lower percentage of paper content
in hospital wastes than in wastes from some othercommercial facilities). Again, health-care facilitieswill need to ensure proper worker education andtraining, necessary so that separation practices forrecycling will not pose increased hazards to workers.
Recycling efforts by hospitals have been inhib-ited in some cases by the lack of available marketsand in some cases by discrimination against dis-carded medical materials. For example, in New York State glass intravenous (IV) bottles are not acategory of regulated medical wastes, but hospitalsreport they are unable to successfully market theglass for recycling because it is perceived to beinfectious/medical waste (94).
This underscores the need for greater educationefforts and better understanding of the nature andactual public health risks posed by the variouscomponents of the medical waste stream. In part to
address this need, the Iroquois Healthcare Consor-tium held a meeting sponsored by hospitals at theAlbany Medical Center in June 1990 to discussopportunities and existing programs for recyclingcertain materials from the medical waste stream(94).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 35/82
26 q Finding the Rx for Managing Medical Wastes
Obviously, some items (e.g., most sharps) inhealth-care settings are not likely candidates forrecycling or reuse, but a surprising volume of
materials in health-care settings have reduction,recycling, and reuse potential. For example, a newcompany (a joint venture of Standard Textile Co.and Marriott Food & Service Management) wasrecently announced that will offer hospitals recycla-ble, protective, sterile surgical linen packs. Thecompany claims the specially designed barrier fabricproducts (e.g., surgical drapes and gowns) will behighly protective and safely recycled at a cost lowerthan disposable (69).
The importance of product packaging on the totalwaste stream can also be significant and a focus of waste reduction efforts. Health-care facilities canhold medical product manufacturers accountable forreductions in packaging and for constructing prod-ucts that use recycled materials and/or that arereusable or recyclable (65).
Some organizations encourage the recovery of medical items that would otherwise be discarded.For example, sometimes more than one disposable
kit is opened in order to use just a part of it for a
procedure, or items are opened and then not used.
Rather than being discarded, sometimes these items
are stored, desterilized (if necessary), and then sent
overseas for use there. Outmoded medical equip-ment that can still be used in other countries is also
sometimes sent (139, 84). (It should be noted that no
governmental guidelines exist currently to ensurethe safety of these practices.)
An organization in Texas, the Medical Benevo-
lence Foundation Presbyterian Medical Mission
Fund, is one such organization that collects equip-ment from medical facilities in the United States to
send to developing countries where it will be used(139). A network of surgical nurses supporting this
type of ‘recycling” is being organized in Oakland,
California (84). The group, called RACORSE Net-work (Recycling, Allocation, and Conservation of
Operating Room Supplies & Equipment), hopes to
facilitate efforts to direct needed medical supplies
overseas that would otherwise be discarded here.12
1 2 ~ g ~ ~ p l i a t i o m o f ~S ~ c t i v i ~ ~d it s s ~ e ~ m e b e i n g r e v i ew e d by th e group. The goal of RACORSE is to help tie tie practice Safer by
establishing recommended protocols (84).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 36/82
Chapter 3
Non-incineration Treatment Technologies and Trends
Of the still unresolved issues regarding medicalwaste management, one of the most critical is whichtechnologies and controls are most appropriate fortreatment.
1Clearly, the answer depends on the
particular circumstances of the medical waste gener-ator and the host community for the treatmentfacility. Factors such as the nature (quantity andtypes) of the medical waste, the availability of permitted landfill space, local air quality conditions,and other demographic and geographic factors (e.g.,urban v. rural locations) need to be considered when
selecting the most appropriate management strategy.Safety, reliability, and costs of alternative treatmentmethods and the regulatory certainty associated withtheir use also affect selection of treatment alterna-tives. Knowledge of various incineration and non-incineration alternatives can also facilitate adoptionof medical waste policies at all levels of government.
While some States and localities actively encour-age incineration as a preferred method of treatment,others have enacted moratoriums on incinerators to
suspend permitting until further information on thesafety of the option is available or new regulationsgoverning it are completed. Thus, incompletenessand uncertainty characterize regulatory activity formedical waste management.
The dilemma now facing New York State facili-ties, for example, can occur elsewhere dependingupon how a State adopts regulations. Facilities theremust make management decisions regarding whetherto upgrade existing on-site incinerators no later than
the fall of 1990 in order to be able to meet New York State’s new air quality standards by January 1, 1992.At present many facilities are seeking treatmenttechnologies alternative to incineration; however, todate the State Health Department has not developedand implemented standards for the approval of treatment alternatives. As a result, the State govern-ment is limiting the available treatment technologiesto the previously approved methods of incineration
and autoclaving. This delay in the evaluation andapproval of alternative technologies may preventmany New York State facilities from using them,including technology already approved in otherStates and/or technology which could be moreattractive from both financial and environmentalperspectives (94).
This chapter, based on available information,addresses the variety of available and emergingnon-incineration treatment alternatives, their techni-cal capabilities, and their risks and costs. First,treatment of medical wastes by autoclaving (i.e., aprocess of steam sterilization), the most frequentlyemployed alternative to incineration, is discussed.Then, a number of other alternative treatments areexamined: steam disinfection and compaction; mechani-cal/chemical disinfection; microwaving; irradiation;and other emerging treatment technologies.
2Chap-
ter 4 discusses various incineration options, includ-ing co-incineration and regional incineration, and
pollution control issues, as well as risk and costimplications. A comparison of non-incineration andincineration treatment alternatives is included inchapter 6.
Increasingly, questions are raised about the avail-ability and performance of non-incineration treat-ment alternatives for medical wastes. While themajority of medical waste is autoclave or inciner-ated, some medical waste (treated or untreated) islandfilled, including some categories of infectious
wastes. The State of Washington found in its surveyof medical facilities that some infectious wastes areabout as frequently treated by autoclaving as byincineration (139). In addition, other treatmentmethods, including disposal into the sewer system,are not rare. It should be noted again that mosttreatment alternatives some form of solid wastedisposal, usually either incineration or landfilling,will be necessary.
II t sho~d be no t~ t it ~~tment in t h i s r e p o f l refers to a process to render wastes noninfectious, unless otherwise indicated, sucb a s ~a tmen t t o
reduce toxicity of wastes, or treatment to render wastes nonrecogn izab le .
z~ s ~~pter re l i es on t ie Om con~act repo~ ‘‘Medical Waste Treatment Tw~ologies,’ completed by Robert Spurg@ Spu rg i n & Associates,March 1990. See alSO (30) and (73). It should be noted th t mention of a specific company or treatment technology does not constitute endorsementof it by OTA. OTA tloes not endorse any specific application of the various incineration and nonincineration treatment alternatives.
–27-

8/14/2019 9018
http://slidepdf.com/reader/full/9018 37/82
28 q Finding the Rx for Managing Medical Wastes
The viability of alternative technologies hasincreased in recent years due to the increased costof incineration, the difficulty associated with
permitting incinerators, and the perceived desir-ability of reducing dependence on incineratorsgiven concerns over their emissions. A number of States (e.g., New Jersey, California, Washington)are attempting to encourage adoption of alternativetechnologies for such reasons. EPA is conductingseveral research projects to evaluate various wastetreatment technologies as required by MWTA (92).
The extent of detail contained in these EPAstudies is not known, but the Agency does report that‘‘most of the treatment technologies are as effective[as incineration] in rendering medical waste nonin-fectious” (141). In addition to the usually highercapital, maintenance, and operating costs of inciner-ation, EPA cites the public perception problems anduncertain regulatory climate associated with inciner-ation as disadvantages of incineration compared toalternative treatment technologies (141). Landfillavailability and other factors, however, will alsoinfluence a medical or health-care facility’s choiceof treatment technology.
Alternative treatment technologies are less capitalintensive and have fewer emission concerns thanincineration processes. Although it is important torecognize that oftentimes more than one treatmenttechnology may be needed to manage all compo-nents of the waste stream (e.g., incineration of pathological wastes that cannot be autoclave).Further, the nature of emissions and efficacy of newtreatment technologies must be demonstrated.
AUTOCLAVING
Historically, autoclaving or steam sterilizationhas been used as a treatment method in laboratorysettings to sterilize microbiological laboratory cul-tures (104).
3The first commercial steam sterilization
process for medical infectious waste was introducedin California in 1978. As incineration requirementswere tightening in California, it became clear thatinsufficient off-site capacity existed to replace
closed on-site incinerators, which would not meetthe State air emission standards (see ch. 5).
Autoclaving is a process by which wastes are
either sterilized or disinfected prior to disposal in alandfill (114) (see figure 2).
4Autoclaving can be a
sterilization process if all microorganisms are ex-posed to the steam for a sufficient temperature/pressure/ time period to assure their destruction. The routineachievement of sterilization can be monitored byplacing Bacillus stear other mophilus spores into thecenter of a load to be autoclave. If the sporessurvive, then the conditions for sterilization have notbeen achieved; if the spores are destroyed (i.e., fail
to grow in microbiological media after steamsterilization), then the conditions for sterilizationhave been achieved (given the practical limitationsof this routine test).
If the spores have not been destroyed during steamsterilization, then sterilization has not occurred.However, some level of disinfection of the wastewould likely have resulted. Unfortunately, the levelof disinfection cannot be routinely or practicallymeasured. Sterilization of infectious waste is gener-ally regarded as “overkill” for most waste disposalsituations. Disinfection of infectious waste is proba-bly a more reasonable goal for most infectiouswastes, though some appropriate and measurabledisinfection goal should be established (1 11).
Most steam sterilizers in use for treating infec-tious wastes are of the high-vacuum type (92). In theautoclaving process, bags of infectious waste areplaced in a chamber and steam is introduced for adetermin ed period of time (usually about 15 to 30minutes) and pressure. The use of pressure helpsreduce the required time for disinfection of medicalwastes, yet the amount of time required will still varydepending on the type and volume of waste (141).Steam temperatures are usually maintained at 250‘For slightly higher (to disinfect the waste morequickly and allow for shorter cycle times).
Autoclaving parameters, e.g., temperature andresidence/cycle time, are determinedby the factorsinfluencing the penetration of steam to the entire
s E t h y l e n e oxide and o the r ga s sterikation processes are typically used to sterilize processes for medical e q u i pme n~ but are dSO SOmebes used totreat wast es. EPA, however, does not recommend ethylene oxide for treating infectious wastes because of its toxicity and given that other treatmentoptions are available (122).4st~~ation i5 a Pmwss tit des~oys ~ ~cmorg~5m5 (e.g., Pathogem). Disinfection is a p r o c e s s i n t e n d e d t o r e d u c e t h e n u m b e r o f
microorganisms or pathogens as low a level as possible, at least below the level at which exposure to a susceptible host could not result in an infectiousdisease. Actual ster ilization is not likely to be maint ained once wastes leave th e au toclave,m is tr ue of incineration as h r esidue (see studies cited in 134);thu s, disinfection is a more accura te term .
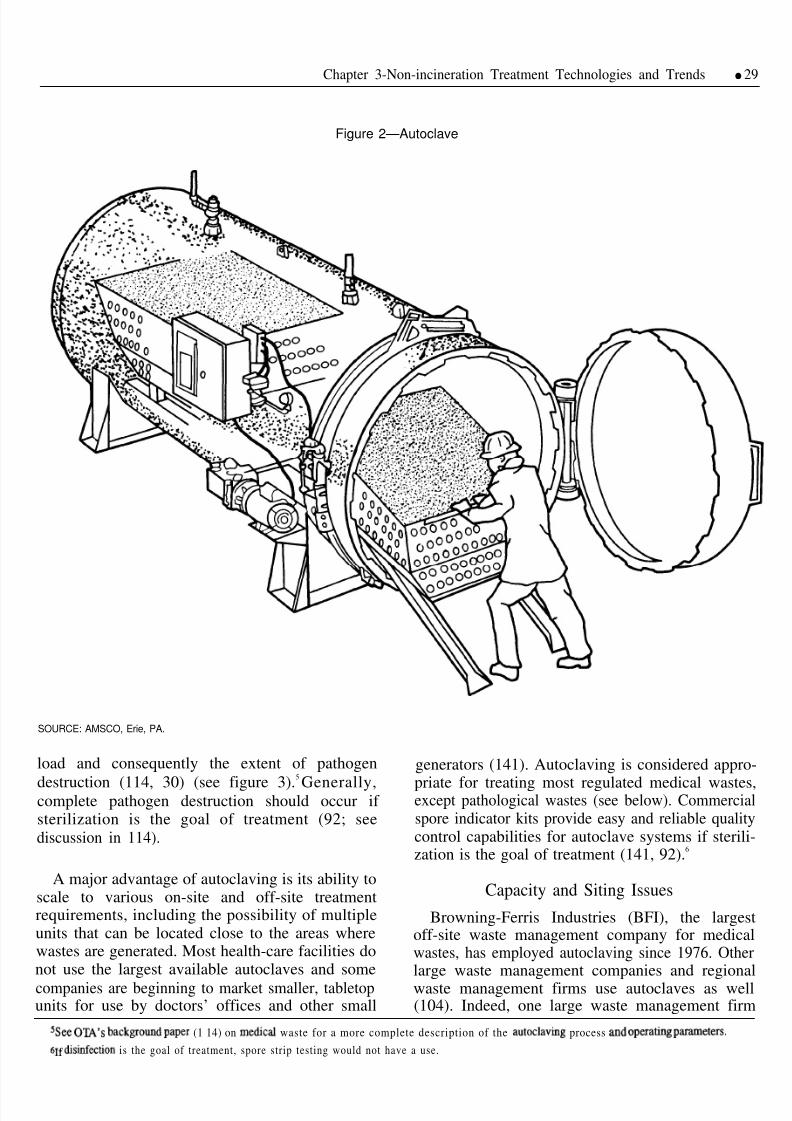
8/14/2019 9018
http://slidepdf.com/reader/full/9018 38/82
Chapter 3-Non-incineration Treatment Technologies and Trends q 29
Figure 2—Autoclave
SOURCE: AMSCO, Erie, PA.
load and consequently the extent of pathogen
destruction (114, 30) (see figure 3).5
Generally,complete pathogen destruction should occur if sterilization is the goal of treatment (92; seediscussion in 114).
A major advantage of autoclaving is its ability toscale to various on-site and off-site treatmentrequirements, including the possibility of multipleunits that can be located close to the areas wherewastes are generated. Most health-care facilities donot use the largest available autoclaves and some
companies are beginning to market smaller, tabletopunits for use by doctors’ offices and other small
generators (141). Autoclaving is considered appro-
priate for treating most regulated medical wastes,except pathological wastes (see below). Commercialspore indicator kits provide easy and reliable qualitycontrol capabilities for autoclave systems if sterili-zation is the goal of treatment (141, 92).
6
Capacity and Siting Issues
Browning-Ferris Industries (BFI), the largestoff-site waste management company for medicalwastes, has employed autoclaving since 1976. Otherlarge waste management companies and regionalwaste management firms use autoclaves as well(104). Indeed, one large waste management firm
ssee C)W’S back~o~d paper (1 14) on medic~ waste for a more complete description of the autoclaving process md Op e r a d n g P~eters.
b lf dis~ection is the goal of treatment, spore strip testing would not have a use.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 39/82
30 qFinding the Rx for Managing Medical Wastes
Figure 3—Typical Sterilization Destruction Curve
‘F ‘C
250(1 27)
240(1 16)
220(104)
200(93]
180(82
160(71)-
140(60)-
120(49)
100(38)
Temperature
O 5 lb microbiological wastes
q 15 lb microbiological wastes
10 20 30 40 50 60 70 80 90
Time (rein)
SOURCE: WilliamRutala et al., “Decontamination of Microbiological Wasteby Steam Sterilization,” Applied Environment/ Microbiology,vol. 33, 1982.
reports that it is currently siting more autoclavesthan incinerators. Meanwhile, some hospitals con-
tinue to use on-site autoclaves for treating their ownmedical waste. The demand for autoclaving appears
to be increasing across the Nation, as the rest of the
country begins to experience the shift from heavyreliance on incineration and the increased need foroff-site medical waste treatment that emerged in
California in the late 1970s.
A major advantage of autoclaving is the capacitya single unit can provide without the spatial require-ments associated with incineration systems. Thecapacity of an autoclave is a function of its size and
throughput. 7 For example, an autoclave capable of disinfecting 4,000 pounds per hour of medical wastemeasures 8 feet in diameter by 24 feet in length,which means it occupies about as much space as a500-pound-per-hour incinerator (104).
Autoclaving maybe limited in some applicationsbecause wastes that are only autoclave are stillrecognizable-unless they are then shredded orcompacted (see below).
8EPA points out that the
‘‘recognizability’ of medical wastes is only an issue
in States covered by MWTA and that most Stateshave not found it necessary or practical to adopt sucha requirement (141). The potentially high costs of requiring the nonrecognizability of treated wasteshave led some to question the wisdom of a require-ment to address solely an aesthetic concern.
In the past, landfill refusals of autoclave medicalwastes frequently occurred. A variety of reasonsaccount for these refusals, but usually they happenedbecause landfill operators could not easily identify
whether waste had been treated and disinfected.Efforts to use bags that change in some visible wayin response to autoclaving (e.g., that melt in theautoclaving process or have a strip that changescolor) apparently have met with mixed results (104).A nonrecognizability requirement is one solution tothis problem, albeit a potentially costly one.
Another solution is for commercial users to havetheir own private, permitted landfills for disposal.Informal discussions by OTA with a number of
hospital officials across the country indicate, how-ever, that few refusals occur if a hospital worksclosely with landfill operators to explain their wasteprocedures. The State of Washington reports fromits 1989 survey that 86 percent of the hospitalsresponding to the survey have not had a wastecollector or landfill refuse to accept its wastebecause of its potentially infectious nature (139).
For States under the MWTA program, wastesmust be treated and destroyed or rendered nonrecog-nizable to be exempt from the tracking program.This would necessitate that some form of shredding
7~e ~~e of tie autoclave loading hopper and the cycle time needed for disinfection% however, affect a n d limit autoclave ~ou@Pu t (63).
8Histofic~ly, p r o b l e ~ t i c o p e r a t i o n has also been a factor leading some h ospitals to aban don autoclavfig (1 14). Appmently, re~n t ~Provements
in th e technology have mi n im i z ed some of these concerns. Proper operat io% however, is key to the effective functioning of any treatment technology.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 40/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 41/82
32 q Finding the Rx for Managing Medical Wastes
ment lifetime of 10 to 15 years. Landfill costs mustalso be taken into account, but overall this treatmentoption appears less expensive than incineration and
management of its ash residue (if it has to be sent toa hazardous waste landfill). The State of Californiaconcluded from its preliminary cost data that auto-claving and other non-incineration alternatives maybe more economical for some small medical facili-ties than retrofitting existing incinerators to meettheir newly proposed air emission control measure(108).
If autoclave waste is not subsequently com-pacted or shredded, there is no significant volumereduction. Yet, given that medical waste represents
such a small percentage of the solid waste stream, itdoes not pose a significant contribution to landfillcapacity problems experienced in some areas of thecountry (and landfill waste cost is usually chargedon a weight rather than a volume basis). Forexample, California reports that if all on-site incin-erators are abandoned for alternative treatmentmethods, the medical waste requiring landfillingwould only represent 0.03 percent of the wastecurrently handled at MSW landfills in the State
(108).
AUTOCLAVING AND
COMPACTION
High-vacuum steam sterilization combined withthe compaction of treated waste began in Californiain 1978 and is increasingly being used in theNortheast and Mid-Atlantic areas of the country. Asof May 1990, over 100 units are in operation. Thistreatment process combines an autoclave with a
stationary compaction unit intended to handle theregulated medical waste as well as the solid wastefrom a health-care facility (see figure 4). The systemis designed to be used as an on-site treatmentalternative (104, 48, 30).
14
The high-vacuum autoclave removes air, whichacts as a steam displacement barrier, and therebyshortens the time for the steam to achieve thenecessary operating temperature (approximately 284°F) and permeate the entire waste load. This means
that exposure to the waste is faster and the cycle timeis reduced, which is estimated to be between 40 and50 minutes from loading to loading (104).
The disinfected waste is then hydraulically fedinto the solid waste hopper, where it is compactedwith general refuse from the facility and automati-
cally fed into the refuse bin or trailer for hauling toa solid waste facility. Operators are not exposed tothe treated medical wastes, reducing the risk of exposure to sharps, fluids, or other waste items. Aswith most autoclaves, no separate fuel source isusually needed since live steam from existing boilersin the facility’s physical plant can usually power thesystem (104). The compaction process achieves a 60percent reduction of volume of the waste, and higherlevels of up to 80 can be achieved if corrugatedcardboard and other recyclable materials are sepa-
rated from the waste to be compacted and landfilled.The system is increasingly being adopted on the
east coast, even in States covered by MWTA (wherethe autoclaved/compacted waste must be tracked).In New York State, however, the two restrictionsassociated with compacted, autoclave waste havelimited the application and acceptance of thisalternative. First, the New York State Department of Health is requiring that the sharps treated in autoclave/ compaction units, such as the San-i-pak units, must
be in compaction-resistant containers to preventspillage and/or exposure to sharps when the com-pacted waste is placed in the landfill. Second, the‘‘recognizability’ of the compacted waste hasresulted in refusal by many local landfills to acceptthe waste (94). As noted above, however, in otherareas of the country such refusals appear lessdifficult to overcome with explanation and demon-stration of the process to landfill operators.
The capital costs are approximately $115,000 to$130,000 for equipment suitable for a 400 bedhospital, with estimates of $35,000 to $60,000 forsite preparation (including utilities, slab, drainage,etc.) (48, 94). Operating costs, according to the solemanufacturer, San-i-pak, range from $0.03 perpound when the solid waste disposal costs are $300per pull (haul) to $0.10 per pound when pull costsrun as high as $1,600. Fuel costs are stated to be$0.003 per pound of steam used (47). The operatingcost estimate includes this steam and electricity cost,as well as repairs and maintenance, the capitalizedcost of the equipment, labor, and bags (48). Thesystems have an expected lifetime of 15 years(similar to that of most incinerators). The operating
laFour sizes of th e au t oc l a ve and compaction un it a re a vailable which will accommodate 1,3,7, or 16 au toclave bags,m = s ~ appm~a t e l y 38x44inches each in a given cycle. Some l imitt i a t t e m p ~ h a v e been made for a commercial off-site use of the technology; such use, however, does not appearas practical as th e on-site a pplication for wh ich the u nit wa s designed (104).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 42/82
Chapter 3-Non-incineration Treatment Technologies and Trends q 33
Figure 4—Autoclave and Compaction Unit
Sterilizerload door(for medicalwastes)
Compactorload door(for othersolidwastes)
(roll-off)interface
Time and
Compactortemperature
controlchart recorder
panel /
Sterilizer
/
controlpanel
Ratchet I
jack “eye” Gaugesconnector
SOURCE: San-i-pak Pacific, Inc., Tracy, CA.
cost includes hauling costs for infectious and generalwastes, and specially hauled wastes, i.e., chemother-apeutic, radioactive, and pathological wastes (esti-mated to be less than 1 percent of a facility’s totalwaste).
MECHANICAL/CHEMICALDISINFECTION
Chemical agents such as chlorine have been usedas disinfectants for medical products for some time,although the application to large volumes of infec-tious wastes generated by hospitals and laboratoriesis more recent (104). This type of technology, whichhas been available since the mid- 1980s, is referred toas “mechanical/chemical’ because of mechanical
maceration and chemical disinfection (a result of forcing a reaction that occurs to volatilize wastematerial and expose all of the pathogens to a
chemical disinfectant in a controlled environment);the residue is discharged to the sewer system.
15
Chemical disinfection processes, according toEPA, are most appropriate for liquid wastes, al-though they can be used to treat solid wastes (122).
The appropriateness of the process for pathologicalwastes is not clear (92). A number of factors shouldbe considered regarding the effective use of chemi-cal disinfection, including: the types and biology of microorganisms in the wastes; degree of contamina-tion; type of disinfectant used (usually sodiumhypochlorite, commonly known as chlorine bleach)and its concentration and quantity; the contact time;mixing requirements; etc. (122). As with othertreatment alternatives, efficacy of the method needsto be demonstrated through the development of a
biological testing program and monitoring on aperiodic basis using appropriate indicators in orderfor the system to be adopted and used on a routine
ls~s me of system is a lso sometimes referred to as “hydropulptig” (see 30).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 43/82
34 Ž Finding the Rx for Managing Medical Wastes
basis. Test results reported to date find the process,using chlorine bleach, to be an effective disinfectantfor medical wastes contaminated with vege tab lebacteria and viruses, but less effective against
spore-formin g bacteria (92).16 No standard protocolhas been developed to evaluate the efficacy of thesystem and to assist in developing standard operat-ing procedures for it (92).
Maceration of the medical waste, involving high-speed hammermill blades and/or shredders, requiresuse of copious amounts of water. To keep the unitfrom overheating as well as to disinfect the waste,water is introduced along with the disinfectant(usually chlorine-based) during the maceration phase.
The simultaneous volatilization and introduction of the disinfectant is designed to render the wastesnoninfectious. The introduction of water creates aliquid waste, which is discharged to the sewer.
17
This means an industrial waste water dischargepermit from the local sewage district may berequired.
According to Research Triangle Institute’s (RTI)contractor report to EPA, “Once the proper operat-ing parameters such as the flow rates for water and
chlorine solutions are established the device issimple to operate and requires little training” (92).The nonrecognizable nature of the byproduct of themechanical/chemical treatment process and its abil-ity to treat liquid medical waste before dischargingit to the sewer system are important factors account-ing for the favorable market response to thistreatment alternative. The waste treated by theprocess is rendered nonrecognizable by the shred-ding and pulverizing phases, which are primarily fortreatment efficiency but act to destroy the waste aswell (104).18 This means that the waste meets thenonrecognizability criteria of MWTA and would nothave to be tracked under its manifest system.
Increased concern over the practice of discharginguntreated liquids (e.g., blood and other body fluids)into the sewer system also makes the mechanical/ chemical process with its discharge of treated
liquids an attractive alternative. Yet, it is not clearthat this system would reduce any risks that mightexist as a result of direct discharges in a facility of blood and body fluids into the sewer system (see ch.
5). Further, the sewage system contains countlesshuman pathogens from the vast quantity of humanbody waste. Liquid medical waste comprises only aminor fraction of this overall waste flow. Microbio-logically, there is little difference between bloodwaste and fecal/urine waste (except that fecal wasteswould be expected to have a far greater number of human pathogens) (11 1).
The process is designed for on-site use with
possible applications to a variety of medical andhealth-care settings (see figure 5). The frost companyto manufacture such a system (Medical SafeTec.,Inc.) currently offers three machines, one for largerapplications and the other two for laboratory set-tings. A similar system was designed by a companyfor application in the funeral industry. This companyalso has a clinical machine for sharps and plans tooffer over 200 separate machines for a wide varietyof health-care applications. While the one companyis offering a system that would require a large
facility to purchase one unit, the other company ismarketing smaller machines for use throughout thehospital (104).
States such as California and New Jersey, whichare open to innovative technology for medical wastegenerally, are a responsive market for this alterna-tive. Some large generators converted to this system,rather than replacing or retrofitting existing incin-erators (104). Currently, about 40 of the smallerunits are in use, primarily for sharps management.These systems can treat pathological waste (e.g.,formalin-fixed tissue samples) and most other medi-cal wastes.
19The system is powered electrically with
standard electrical requirements. Sewer connectionis mandatory, and, as noted, a local discharge permitmay be necessary. Concern has been raised over thelevel of metals, organics, and other contaminantsthat may be in the sewage discharge (5).
IGHwa rd a n d ocwpation~ r isk from t ie ha ndling, stora ge, and use of chlorine ha ve been suggested as a potent ial disadvanta ge of ~s tec~olog’y
(94).
1 7Rep o f i e d l y , s y s t e m s t h a t s h r e d an d d i s i n f e c t m e d i c a l w a s t e s t ha t w i ll not requ ire use of copious am ounts of wat er or a sewer dkchge a r e being
developed (63). One such process will combine conventional shredding technology with the use of special red bags. These red bags have a small seamthat envelops a few grams of formulated powder (a water-activated disinfectant). Treated material is “only slightly moist, no longerrecognizable. . disinfected and volume-rcxiuced” (78).
18A pres~~~g system which is pa r t of the large hammermill, breaks up t he waste m aterials before th e h a .mme rm i l l pulverims hem.
lg~e EPA s~tes, however, that these units are not normally recommended for patiOIOgicd wa s t e ~es (141).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 44/82
Chapter 3-Non-incineration Treatment Technologies and Trends .35
Figure 5-Mechanical/Chemical Disinfection Unit
Negative pressure
Mepa filter system blower
1
SOURCE: Medical SafeTec, Inc., Indianapolis, IN.
The percentage of dissolved solids in the dis-charge into the sewer is high (up to 10,000 ppm v.300 ppm for residential users), but the manufacturerstates that changes necessary to reduce the level tothat of other points of discharges are now feasible(104). Even so, the liquid effluent contains highconcentrations of substances, e.g., chlorine, that mayrequire pretreatment before being discharged to the
municipal sewer system. It would appear that localpermit levels for sewage discharges would have tobe met.
20
Solidwaste
collectioncart
\
designed to control emissions and force air througha series of prefilters and a chlorine-resistant falterbefore discharging it to the atmosphere (141, 5). Theuse of chlorine and the potential impact on sewagedischarges is also raised as a concern with thechemical disinfection process. Further study of theseissues is needed, possibly as part of EPA’s currentresearch on alternative treatment methods.
There are no air quality regulations that arerelevant. Although it is not clear there is a need forany air regulations, given that no known air emis-sions problems have been encountered, little hasbeen reported about the nature of the emissions.There is some concern over the potential forproducing volatile chemicals and/or microbes dur-ing the shredding process, although the system is
The mechanical nature of the equipment, with somany moving parts, means it could require a highlevel of maintenance. This also means there is morepotential occupational exposure. The manufacturersnote that no injuries involving equipment repair ormaintenance have been reported.
21As with an
autoclave unit, the space needed for a mechanical/ chemical unit is not large and the capacity is thenmainly a factor of the throughput rate for the unit.The smaller units require an area approximately 10
20R~ (92) ~Wo~ tit ~a~te ~eatment effluent from the Medical S~eT& tit has been tested according to the specitlcations published under the
Clean Water Act for pollutan t a nalysis (40 CFR, Part 136).
2 1Ye~ ~S ~ t h o ~ e r ~ ea t m e n t ~ t e r n a t i v e s , it is n o t c l e a r h o w f r ~ u e n t l y a ~ i d e n t s a r e r e p o r t e d (g iven m n c e r n s OVer p O t e I l ~ h p i i C t S 011 kMIKZIIICe
pre miums, etc.).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 45/82
36 qFinding the &for Managing Medical Wastes
feet by 9 feet and the units with additional capacitywould require areas of 11 feet by 10 feet.
Capital costs are approximately between $40,000
and $50,000 (equipment and installation) for thesmaller units and approximately $350,000 for thelarger sized unit. Operating costs are reported to be$0.06 per pound of waste per hour of treatment(104).
MICROWAVE
The application of microwave technology todisinfect medical waste was introduced in Europeseveral years ago. The technology is from West
Germany and just recently is being marketed in theUnited States (34). The units can be on-site ormobile facilities. The first on-site installation was inNorth Carolina in March 1990. A second commer-cial system began operation shortly after this inCalifornia as a supplemental technology to anexisting regional incinerator (104, 34).
Powered by electricity, the unit shreds the wastein a controlled environment; the waste then entersthe chamber for exposure to the microwaves (see
figure 6). The disinfection process takes placethrough microwave heating, which occurs inside thewaste material (unlike other thermal treatmentmethods which heat wastes externally) and wettingand shredding the waste to facilitate heating andsteam penetration of the waste. The material isdischarged to a storage bin for ultimate disposal.
Computerized controls, as with most other treat-ment technologies, are used to ensure the minimumparameters for disinfection and proper function of the equipment. Fire and temperature conditionsnecessary for waste sterilization are the same asthose for autoclaving (92). Studies conducted inGermany by the Institute of Hygiene, University of Gottingen concluded that the process treated ma-terial to a lower level of bacteria content thanordinary household wastes (as reported by ref. 35).Performance tests at a unit operating in the UnitedStates, using a Bacillus subtilis microbiologicalspore test indicator, found the wastes to be treatedunder conditions to render it sterilized (35). Re-
search Triangle Institute reports that although themethod is essentially a steam sterilization method, itis necessary to confirm that conditions required forsteam sterilization exist in the microwave process(92).
Photo credit: Vetco Sanitec Corp.,Combustion Engineering, Stamford, CT
Microwave units can be installed on-site or be used asmobile units. Mobile units could facilitate collection of
regulated medical wastes from home health-care settings,
doctor offices, and other small generators of medicalwastes. This type of mobile microwave unit has been used
in Berlin, West Germany for several years.
As with autoclaving, approximately 90 percent of medical wastes can be treated by this method (it isnot recommended for pathological wastes). The useof electricity averages about $0.02 per pound.Energy use is reportedly lower than that of anincinerator (35). The shredding process results in avolume reduction of 80 percent prior to disposal.Treated wastes are suitable for disposal in a solidwaste landfill. Given that the process is used inEurope with no reported emission problems, itsacceptance is anticipated in the United States (35,104).
The microwave system is designed to be operatedby unskilled labor. All adjustments in wastes levelsand time are preprogrammed into the system (92).Operating and maintenance costs are reported to beapproximately $0.10 or $0.07 per hour, dependingon whether the system is operated 8 hours or 10
hours a day, respectively. Capital costs are about$500,000 for a unit (35). It appears that health risksassociated with the unit would primarily be associ-ated with the maintenance of the shredder compo-nent of the system. Potential operator exposure tovolatized chemicals during loading or cleaning/ maintenance should be examined, h o w e v e r .
IRRADIATION
A common practice is to treat medical products
with radiation for sterilization purposes (104). Thehigh cost of cobalt used in the process and highoperating costs have discouraged commercial ven-tures from using the technology for medical wastemanagement. In February 1990, however, the first

8/14/2019 9018
http://slidepdf.com/reader/full/9018 46/82
Chapter 3-Non-incineration Treatment Technologies and Trends q 37
Figure 6—Mobile Microwave Medical Waste Disinfection Unit
\
u
12
o11
I
I1
‘%31 0)
o- 13
1.
2.
3.
4.
5.
6.
7.
8.
9.
Process scheme of a mobile microwave-disinfection unit
Feeding hopper
Feeding crank
Shredder
Connecting hopperwith inspection window
Level sensors
Main conveyor auger
Microwave generators
Temperature holding section
Discharge conveyor auger
SOURCE: Vetco Sanitec Corp., Combustion Engineering, Stamford, CT.
commercial medical waste irradiation facility wasopened in Arkansas, and additional facilities areplanned in California and New Jersey. Questionshave been raised about the actual process of radiat-ing the material and achieving adequate disinfection(104) (see figure 7). Garoma radiation sterilizesinfectious waste by penetrating the waste andinactivating microbial contaminants. T h e i o n i z i n gradiation hydrolyzes the water molecules within the
10.
11.
12.
13.
14.
15.
16.
17.
Temperature sensors
Filter system, 2-stage
Water tank with pumpand spraying connection
Steam generator
Steam connection
Hydraulic aggregate
Room heater
Container
micro organisms and these intermediate hydrolysisproducts interact with the gamma radiation andbiological compounds, are broken down and arerendered noninfectious. The company pursuing thistreatment technology emphasizes that the waste willnot be disposed of as solid waste. Rather, it isshredded, rendering it nonrecognizable, and isshipped to a cement kiln where it is burned as fuel(104).22 Eventually, one such operator of a system
~t should be noted that concerns have also been raised about the practice of burning wastes in cement kilns, which typically are not subject to airemission standar ds (other than the n ew source performance standard NSPS ) for pa rticulate matt er emissions). The a ssumption is tha t these kilns operateat such high temperatures that wastes used as fuels are destroyed without producing harmful emissions. This is an unsettled regulatory issue. It is true,however, that any cement kiln b urning MSW would be subject to air emissions standards for MSW incinerators as proposed by EPA in December 1989.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 47/82
38 q Finding the Rx for Managing Medical Wastes
Figure 7—irradiation Unit
Cobalt 60 radiation chamber
Infectious waste
SOURCE: Technology Process, Inc.
plans to separate the plastic waste and sell the treatedplastic residues for recycling (92, 101).
The process is highly predictable, according toRTI’s analysis (92). Verification of the conditions
for disinfection involves using Bacillus pumilis as atest indicator organism. According to RTI, nostudies specifically addressing the efficacy of gammairradiation of medical waste for disinfection (92). Inaddition, film is placed between every few boxes toquantify the amount of radiation each box receives(104).
Again, this treatment method is not recommendedby EPA for pathological wastes. The capacity of these units is a factor of the throughput rate. Theunits are an off-site alternative and can manage alltypes of waste, except pathological wastes. Theapproximate operating cost could be $0.15 per
Treated waste
pound. Potential risks of this alternative treatmenttechnology are primarily associated with the possi-bility of radiation exposure to workers.
23
OTHER POTENTIAL
TREATMENT TECHNOLOGIES
Other technologies with potential application tomedical waste management are in a conceptual orexperimental stage in their development. Several arementioned here to illustrate the variety of attemptsto develop treatment alternatives for medical wastes.
One technology that has recently been announcedas available and capable of thermally destroyingbiomedical wastes uses an electric molten glassfurnace. At least with other waste types, the wastesare fed into the furnace and are subjected to intenseheat (2,300 ‘F) and air and water vapor. The result
~Worker~ ~pma@ ~ese systems ~~~d ~ve to be @ain ed according t o t ie IfJ ~ ‘‘S~nd~ds for Protection Ag&t Radiation” re@tiOIIS.
Operators would need to be highly trained to ensure the efficient and safe operation of the process.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 48/82
Chapter 3--IVon-incineration Treatment Technologies and Trends q 39
is the vaporization or oxidation of some wastes anda inert stable glass residue (87).
Electrohydraulic disinfection and pulse-power
technology were created as disinfection systems forcontaminated liquids. Their uses are not widespread,although the concept of applying the technology tomedical waste disinfection has been suggested. Itappears that the perceived high cost of this technol-ogy is a major reason it has not yet been developed.The process involves the use of pulsed plasma of electrical discharges in water, using ultravioletradiation, hydrogen, hydroxil, ozone and shock waves to act as disinfectants. One application of pulse power technology does not require the use of radioisotopes (104).
Future application of plasma torch technology tomedical wastes (and other hazardous wastes) hasbeen suggested (42, 39, 31). A “pyroxidize,” asmall pyrolysis on-site laboratory waste disposalunit, is being developed (92). Another recentlyannounced potential treatment technology is anelectrocatalytic oxidation system (38).
Adaptations of existing technologies have beensuggested, for example, a sterilization/dry grindingmethod (30). This system would combine an auto-clave system with dry grinding/shredding in ahammermill to achieve both volume reduction andnonrecognizability of the wastes. Projected costs forthis hypothetical alternative treatment are $0.08 perpound (30). It is not clear whether the increasedmaintenance cost usually associated with shreddersis taken into consideration in these calculations. Onereason frequently given for the limited application todate of shredders is that they require a high level of maintenance. Thermal inactivation or dry heatsterilization, reportedly sometimes used for bothsolid and liquid medical wastes, also could possiblybe used in conjunction with a shredder or compactor(although it is not considered as efficient as steamdisinfection) (73).
SUMMARY
Several non-incineration alternative treatmenttechnologies for medical wastes are commerciallyavailable, others are at a conceptual or developmen-tal stage. Autoclaves, autoclave/compaction units,
mechanical/chemical units, and most recently mi-crowaving and irradiation treatment alternatives arein use in medical facilities across the Nation. Mostof these units are on-site treatment alternatives and
most appear less costly than incineration. Many of the alternatives will achieve significant volumereduction (of 60 percent or more) of the medicalwaste and all can render wastes nonrecognizable (if
a compactor or shredder is added). Weight reductionmay or may not occur, particularly if water is addedduring the treatment process. In fact, some of thesetreatment alternatives can add to the weight of waste, given their use of water. These alternativesappear to have fewer emissions concerns (althoughthese warrant further study) than incinerators. Mostof these alternatives do not appear appropriate forpathological wastes.
Health risks associated with these technologieshave not been thoroughly investigated. Furtherexamination of potential health risks is warranted(particularly for the newest applications, e.g., micro-wave and irradiation). When any waste treatmentalternative is considered, any new or additionalemployee exposures that could result from utiliz-ing the new method should be identified andevaluated.
Before adopting a medical waste managementstrategy, medical waste generators must first knowthe applicable regulatory requirements and then
assess the capabilities, costs, and associated healthand environmental risks of various treatment tech-nologies as applied to their facility in order to adoptthe most appropriate technology for their needs. It islikely that the emergence of these non-incinerationalternative treatment methods will reduce but noteliminate the current level of dependence on inciner-ation for medical wastes. Many of these alternativescan be viewed as supplementing the use of incinera-tion for treating medical wastes. Pathological wastesare the one type of regulated medical wastes for
which incineration remains the preferred treatmentalternative (122, 92).
It appears most prudent for any regulatory pro-gram for medical waste to avoid directly or indi-rectly encouraging a particular type or application of treatment technologies. Rather, flexibility for thegenerators to meet their management needs andcomply with regulatory requirements will allow foradoption of the most appropriate treatment optionsand help ensure safe management of medical wastes.
Government agencies, particularly EPA, couldfacilitate the evaluation and adoption of newtreatment alternatives by developing a programfor demonstrating the efficacy of a treatment

8/14/2019 9018
http://slidepdf.com/reader/full/9018 49/82
40 q Finding the Rx for Managing Medical Wastes
method. A general protocol for the certification of approval of any type of waste treatment technology(e.g., hazardous, solid, medical) could be establishedwith adjustments made for developing appropriatetesting programs (e.g., biological testing of medicaltreatment methods).
Interim approval status might be given while testprotocols and results are developed and/or pilotprojects, perhaps at veterans’ hospitals or othergovernment facilities could be used. Monitoringnew facilities on aperiodic basis, perhaps with somesupporting funding, could facilitate developing ap-
propriate operating parameters and specifications. Aprogram similar to the Superfund Innovative Tech-nology Evaluation Program has been suggested as amodel for a program evaluating new medical wastetechnologies (31, 124).
Such efforts could help ensure that governmentregulatory activity does not create barriers forevaluation and adoption of new technologies. Animportant task for State and Federal regulators thenis to rid the current regulatory system of inconsisten-cies and ambiguities and enable the “market” tomove ahead with optimum management solutions.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 50/82
Chapter 4
Incineration Treatment Issues and Trends
Incineration of medical wastes remains a preva-lent treatment method in the United States.lIt is also
the treatment technology most often used for medi-cal wastes in other Western countries (57, 58). Theadvantages of incinerating medical wastes, are thoseassociated with the incineration of any type of waste:significant volume reduction (by about 90 percent),assured destruction, sterilization, weight reduction,and the ability to manage most types of wastes withlittle processing before treatment.
2The disadvan-
tages include potential pollution risks associated
with incineration processes and increased costsassociated with controlling pollution emissions (114,116).
3
In some European countries it appears thatregional off-site incineration facilities have beenencouraged to optimize the economical applicationof advanced pollution control technologies (57).Inthe United States, incineration continues to occur
on-site in smaller units, most of which have few orno pollution controls. As some States adopt morestringent air standards for medical waste incine-
rators, 90 percent or more of these existing units canbe expected to retire when these new standards gointo effect within the next several years (e.g., NewYork State, California) (12). New on-site as well asoff-site units can be designed to meet stringentemission control standards, and some older, on-sitefacilities can be retrofitted with air emission controls(if sufficient space and the economics make thispractical). Retrofitting can include modifying theincinerator, adding or changing pollution controldevices, or both.
While new regional facilities are being estab-lished and other new on-site facilities are operatingin the United States, it is also likely that incinerationwill be supplemented by other treatment technolo-gies. Nearly 80 percent of the hospitals in Californiause alternatives to on-site incineration (49). Severalinterrelated factors account for the likely decreaseddependence on incineration:
1.
2.
3.
4.
the increased cost of incineration due toincreased equipment needs to meet new emis-sion standards and permit requirements;
siting and permitting difficulties associatedwith locating new incineration facilities;
regulatory uncertainty associated with incinera-tion requirements at the local, State, andnational levels of government; and
the increasing availability of nonincinerationalternatives for treatment of medical wastes.
In fact, increasing concern over incineration ingeneral and particularly for medical waste hasresulted, in some States, in indirect regulatoryencouragement for developing alternative treatmenttechnologies.
More specifically, the regulatory emphasis byStates has been on operation requirements forincreasing temperature, residence times, and com-bustion efficiency to foster destruction of toxiccompounds in the combustion process in order topreclude their release to the atmosphere. The re-
quired temperatures are tending to be set increas-ingly higher than necessary to destroy pathogens.According to EPA, the incinerator conditions neededto destroy gas stream pathogens emitted from themedical wastes are a function of temperature,residence time, and good mixing to preclude ‘pock-ets’ of gases (which do not reach the requiredtemperature). Based on limited available data, attypical residence times, temperatures (for the secon-dary chamber) necessary for pathogen destructionare 1,600 ‘F or more. Most existing regulations
usually require temperatures of 1,800 or 2,000 ‘F,higher than the temperature probably needed forpathogen destruction, but considered necessary tocontrol other emissions such as volatile organics(e.g., chemotherapy agents) (41).
Incineration technology continues to evolve, andmore sophisticated pollution control equipment isbecoming available. Another source of concern,
IMos t of ~ese~c~erators a r e of t ie controlled-air type (see below an d 114). This type of inciner at or is popub.rfor medicd wastes because it mica.llY
is more fuel-efficient an d ha s lower par ticulate emissions tha n other sm aller, modular combust ion systems a nd it s solid heart h can vapo r - c ombus t liquid
wastes and ensu re tha t needles are rendered noninfectious.
2A]t iough sepa ra t i on of noncombust ibles an d items with problematic constituen ts impr oves maint enan ce and p ossibly a ir emissio~.
30nce other ~mtment me~ods (e.g., ~utoclaving) me more ~ o r o u g h l y s ~ d i e d , h ow e v e r , ~ c r e a s e d cosc s t o e n s u r e t i e i r env i romnent i safety ma y
also occur. Nonet heless, most non inc ine r a t i on a l t e rm t i v e s are less capita l-intensive tha n incineration.
- 4 1 –

8/14/2019 9018
http://slidepdf.com/reader/full/9018 51/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 52/82
Chapter Incineration Treatment Issues and Trends q 43
including medical waste incinerators in their pro-posed air emission standards for all incineratorsburning more than 50 percent MSW on November30, 1989. Those proposed standards would haveapplied to most medical waste incinerators andrequired a 90 percent reduction in air emissionsthrough emissions limits, operating standards, andsome source separation and recycling requirements.Apparently, at this time EPA is considering a lowersize cutoff for the MSW NSPS standard, whichwould essentially exclude medical waste incinerat-ing. Instead, a specific NSPS for medical wasteincinerators would be adopted (41).
At the State level, over half the States havechanged their requirements for medical waste man-agement within the last 2 years (107). Most of thisregulatory activity focuses on setting stricter air
emission standards for medical waste incinerators.Currently, the standard-setting process for air emis-sions from medical waste incinerators in Californiais attracting considerable attention (see box C). The
California Air Resources Board (CARB) is propos-ing regulations for medical waste incinerators thatwould require reducing emissions of dioxins by 99percent or to 10 nanograms per kilogram. There is nocadmium requirement, but local air districts arerecommended to evaluate the need for such stan-dards on a case-by-case basis.
Originally, the proposal required the use of a dryscrubber/baghouse combination for air pollutioncontrol equipment, as the best available controltechnology (BACT), to achieve the desired removalrates. Any other technology that could document thenecessary reductions in dioxins could also be
Box California and Its Dioxin Control Measure: A Case Study of One State’s Approachto Regulation of Air Toxics and Medical Waste Incinerators
On July 12, 1990, a proposed “air toxic control measure” (ATCM) requiring a 99 percent reduction in dioxinsor control to a level no greater than 10 rig/kg of medical waste burned was adopted by the State of California.
1It
is the culmination of an effort begun when the California Air Resources Board (CARB) identified dioxins as toxic
air contaminants in July 1986.
2
CARB is required to evaluate the need for and the appropriate degree of control fora compound that is identified as a toxic air contaminant (106, 108).
Through a formal risk management process, medical waste incinerators were found to have the greatestindividual risk potential of all dioxins sources the State identified. This, combined with the facts that most of theincinerators are uncontrolled and located in residential areas and that emission test results from eight test facilitiesfound that they were also sources of other pollutants (e.g., cadmium, benzene, polycyclic aromatic hydrocarbons,lead, mercury, nitrogen oxides, sulfur dioxide, particulate matter, and hydrochloric acid), led CARB to give medicalwaste incinerators the highest priority for the dioxin ATCM (106, 108).
CARB identified 146 facilities that incinerate medical wastes in the State of California. Of these, 137 areon-site facilities incinerating 28 percent of the total amount of medical waste incinerated, and 9 are off-site, regionalfacilities incinerating the remaining 72 percent of the medical waste incinerated. The on-site incinerators are
typically located at a medical facility and mainly incinerate general solid waste (70 to 95 percent by weight of thetotal amount of waste incinerated), similar to MSW, with infectious and pathological waste (5 to 30 percent byweight of the waste incinerated). The incinerator may generate steam and hot water, but the only current air emissionregulation is a particulate matter emission standard set by the local air pollution control district (49, 106, 108).
Regional incinerators in California are located to serve many medical facilities and incinerate only pathologicaland infectious wastes. These facilities have particulate matter and HCl emissions regulated by the local air pollutioncontrol districts and the Department of Health Services (49, 106, 108). These regional facilities manage nearly 75percent of the infectious waste incinerated in the State (8,700 tons per year of the 12,105 tons per year of infectious
l~ter tie a&ptiOn of t h e CARB con t r o l measur e, local air pollution contr ol districts have 120 da ys to pr opose a d 6 monti to adopt
a regulation at least as str ingent as th at a dopted by CARB (106, 108).
2~cordfig to Califofia law, a tOXiC fi con t i~t “an air pollutant which may cause or contribute to an increase in mortality or
an increase in serious illness, or which may pose a present or potential hazard to human health’ (California Health and Safety Code Section
39655).Continued on next page

8/14/2019 9018
http://slidepdf.com/reader/full/9018 53/82
44 q Finding the Rx for Managing Medical Wastes
wastes incinerated). The amount medical waste currently incinerated represents about 0.05 percent of the totalgeneral waste produced in California annually (49, 106, 108).
CARB emissions testing of eight California medical waste incinerators served as the basis for developing theATCM. The emission rate for dioxins from these eight facilities ranged from 0.0003 to 14,140 rig/kg of wasteburned. A multipathway risk assessment (which considered exposure to inhalation, dirt ingestion, dermalabsorption, and mother’s milk) estimated that the risk for dioxin is 1 to 246 chances of developing cancer permillion, with the lower end of the range reflecting controlled facilities. Based on these findings, CARB identifiedcontrol equipment that could reduce dioxin emissions by 99 percent or to 10 rig/kg and determined that wastedisposal alternatives to incineration are available (106, 108). The proposed control measure is expected to reducethe maximum individual risk by 90 to 99 percent, to 1 to 3 chances of developing cancer per million (49, 106, 108).
The proposed ATCM for dioxin of 99 percent reduction of dioxins or reduction to a level no greater than 10rig/kg of waste burned is considered to be BACT (the best available control technology). Although CARB firstidentified a dry scrubber and baghouse air pollution control system as the most effective in reducing dioxinemissions, it later tested and reported that a well-designed incinerator equipped with a Venturi wet scrubber
achieved the 99 percent reduction (i.e., the proposed emission limit for dioxins). The proposed control measure alsoincludes requirements to ensure combustion efficiency to minimize dioxin formation, These include a minimumtemperature of 1,4000 °F in the primary chamber of a multiple chamber unit and a minimum temperature of 1,800°Fin the secondary chamber of a multiple chamber unit or the primary chamber of a single chamber unit, with a onesecond gas residence time (106, 108).
In addition, a maximum temperature for flue gas at the outlet of the air pollution control equipment is specifiedas 300°F (unless an alternative temperature achieves equal or greater control). The control measure also specifiesrequirements regarding continuous record keeping for the operation of equipment and maintenance; reportingviolations, malfunctions, or upset conditions; annual source testing; operator training; and mandatory air districtpermits (106, 108).
The proposed measure became effective July 1991, and the compliance timetable is for installation of BACT
15 months after the local air district’s adoption or to cease operation 6 months after the district’s adoption. Thedioxin control measure is expected to increase waste treatment costs by approximately $0.10 to $0.35 per poundover current incinerator costs. In addition to the reduction in the risk to 1 to 3 chances of developing cancer permillion, the control measure is expected to produce other net environmental benefits (106, 108).
considered for permitting (e.g., wet scrubber sys- the wastes they burn may be most appropriate.10
terns). This provision was modified, however, to MSW incinerators tend to be large, mass-burnState performance standards (e.g., a 99 percentreduction requirement) without regard to the specifictechnology necessary to meet them. The proposedfinal standard became effective on July 12, 1990.Reported test results from one facility show a 99percent reduction and 10 rig/kg achievable with awell-operated incinerator equipped with a high-efficiency Venturi (wet) scrubber (107).
Given the large number of medical waste inciner-ators (on-site and off-site) operating in the country,separate regulation taking into account the specialcharacteristics of these incinerators and the nature of
incinerators (i.e., waste is burned as-it is received,not processed or sorted), which are typically one-
chamber combustion systems operating under con-ditions of excess air. Most medical wastes areburned in excess air or controlled air incinerators(sometimes referred to as starved air incinerators),which burn waste in two or more chambers underconditions of either excess oxygen or a deficiency of air, respectively (1 14, 45, 30, 40) (see figure 8).
11
As with MSW incineration, a trend may beemerging for medical waste incineration to recoverenergy and include front-end waste separation and
lo~e exact n um b e r of medic~ waste incinerators operatin g in the countr y is not known with certaint y. The St ate of California, Xt i 10 percent of
the U.S. population, r eports 146 medical waste incinera tors (49).
I I EpA finds, based on informa tion gathered in ~ Stat es, that approximately 40 percent of total nu mber of incinerators ar e ones operating u nderexcess air conditions a nd 35 percent a re st arved air units. These excess air incinerators ar e probably small incinerators u sed for pathologicrd wastes andhave limited or no ai r pollution control equipment. They are pr obably not required to meet most air qua lity standar ds due to th eir size unless th ey arein a Stat e (e.g., New York California) tbat h as r ecently adopted new air qu ality stan dards (141).
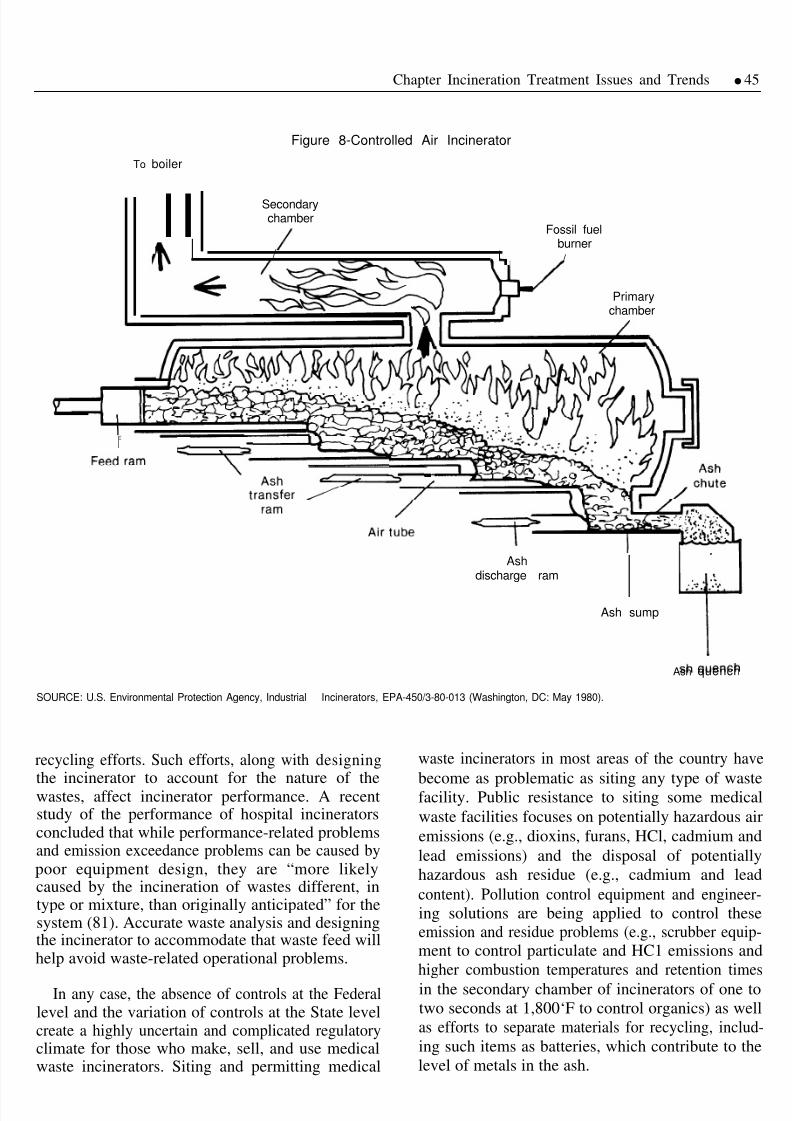
8/14/2019 9018
http://slidepdf.com/reader/full/9018 54/82
Chapter Incineration Treatment Issues and Trends q 45
Figure 8-Controlled Air Incinerator
To boiler
IISecondarychamber
Fossil fuel
Iburner
/ q /
Primarychamber
I
I
Ashdischarge ram
IAsh sump
Ash quench
SOURCE: U.S. Environmental Protection Agency, Industrial Incinerators, EPA-450/3-80-013 (Washington, DC: May 1980).
recycling efforts. Such efforts, along with designing
the incinerator to account for the nature of thewastes, affect incinerator performance. A recentstudy of the performance of hospital incineratorsconcluded that while performance-related problemsand emission exceedance problems can be caused bypoor equipment design, they are “more likelycaused by the incineration of wastes different, intype or mixture, than originally anticipated” for thesystem (81). Accurate waste analysis and designingthe incinerator to accommodate that waste feed willhelp avoid waste-related operational problems.
In any case, the absence of controls at the Federallevel and the variation of controls at the State levelcreate a highly uncertain and complicated regulatoryclimate for those who make, sell, and use medicalwaste incinerators. Siting and permitting medical
waste incinerators in most areas of the country have
become as problematic as siting any type of wastefacility. Public resistance to siting some medicalwaste facilities focuses on potentially hazardous airemissions (e.g., dioxins, furans, HCl, cadmium andlead emissions) and the disposal of potentiallyhazardous ash residue (e.g., cadmium and lead
content). Pollution control equipment and engineer-ing solutions are being applied to control theseemission and residue problems (e.g., scrubber equip-ment to control particulate and HC1 emissions andhigher combustion temperatures and retention timesin the secondary chamber of incinerators of one totwo seconds at 1,800‘F to control organics) as wellas efforts to separate materials for recycling, includ-ing such items as batteries, which contribute to thelevel of metals in the ash.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 55/82
46 q Finding the Rx for Managing Medical Wastes
CAPACITY, COSTS, AND RISKS
Capacity
The advent of stricter environmental controls forincinerators and the prospect of the resulting closureof many existing facilities has fueled concerns overwhether adequate incineration capacity for medicalwastes is available nationally. This discussion willfocus on capacity issues, which are driving trends intechnology and permitting, and will indirectly (qual-itatively) identify the general level to which a
capacity problem exists in this country.
It is extremely difficult to determine existingincineration capacity (or demand/need for capacity)on a national basis given the differences betweenon-site and off-site incinerator capacity parametersand the fact that the amount of medical waste(including nonhospital sources) requiring treatmentis not definitively known (104). It does appear,however, that the demand for capacity has outpacedits availability in some regions of the country,
especially where new, more stringent State require-ments lead to the closure of existing facilities andnewer facilities are not readily available (given thelengthy permitting process and the persistent sitingproblems).
The capacity problem is most likely to arise whenon-site incinerators shut down because they can nolonger meet regulations, when management prac-tices (e.g., universal precautions widely applied)increase the amount of waste requiring incineration,
or when increasing numbers of nonhospital genera-tors enter the market. If a large number of on-siteincinerators cease operation, for whatever reasons,in the same geographic region, a ‘‘capacity crunch’can occur (104). This capacity deficit can result ineither accelerated permitting or increased export(transfer) to other regions. In California, new re-gional incinerators are being permitted, which willprovide surplus capacity for medical waste, nolonger burned on-site (49). In New York State,increased out-of-State shipment is anticipated at
least in the short-term after new regulations takeeffect (94).
Increasingly, older, on-site units are being re-placed either with larger, on-site units that can beregional (accepting medical wastes from nearby
clinics and nursing homes) and/or co-incinerate thefacility’s medical and solid wastes, or with off-siteregional incineration. The customer base for re-gional incinerators continues to grow. Substantialgrowth in this industry is projected.
12Interestingly,
although total on-site and off-site capacity may beadequate to meet disposal needs, the regionalmarkets determine the fluctuations in availablecapacity in a given area. That is, the variedgeneration rates (in part related to regulatory trendsand shifts in management practices), the reluctance
of major regional incineration and autoclavingoperating companies to make capacity available tocompetitors when the need arises, and regionalregulatory trends create an unstable level of treat-ment capacity (104)0
The Southeast (centered in and around SouthCarolina), lower Midwest (centered in and aroundOklahoma), and the Ohio Valley area now appear tohave excess capacity for medical waste. Indeed,these areas have been magnets for the waste from
other parts of the country where capacity has becomesaturated. Wastes from locations on both coasts havebeen transported great distances to facilities in theseareas.
The uncertain outcome of the pending changes inthe Clean Air Act has slowed the pace of permitapplications in a number of States. In the Northeast,constraints on capacity have been driven by suchfactors as permit difficulties (e.g., the (now expired)moratorium on incineration activity in Pennsylva-
nia). In other areas, there may be permit activity(e.g., Texas, Illinois), but there is a lag between thetime when additional incineration and/or alternativetreatment capacity will be available in those marketsand the immediate capacity needs (104). This cannecessitate exporting medical waste out of the areafor treatment, at least until new treatment capacity isavailable. In some areas, a “capacity crunch” isbeing met by arrangements with local MSW incine-rators to accept medical wastes (68; see below). TheState of California, when adopting new air emission
standards for medical waste incinerators, examinedthe potential for a capacity shortfall. They concluded
1 2 ~ e S w e iS t ie for t ie entire ~e&c~ ~a~te ~Mgement indu s@y. ~cording t o on e s tudy, m e c~enfly es t ima ted $750 mdfion medical wast e
industry will expand to $1.5 billion by 1991 and grow to nearly to $5 billion by 1994 (cited in 75). Other studies project revenues to be even higher,reaching $10.7 billion by 1991, with expenditures estimated to grow from $970 million to $2.9 billion by 1991 (cited in 74).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 56/82
Chapter Incineration Treatment Issues and Trends q 47
that upgraded or new incinerators, or other treatmentalternatives, could be permitted within the timeframebefore existing facilities would be required to shutdown. Further, the relatively low volume of medical
waste incinerated could be landfilled at existingfacilities with little impact on their capacity accord-ing to CAB.
Changes in regulation of a waste stream can resultin short-term shortfalls of permitted treatment ca-pacity (e.g., the shortages of permitted MSW landfillcapacity experienced in some areas of the country asStates adopt more stringent landfill regulations,leading to closure of many existing facilities). Itappears that such temporary shortfalls of permitted
capacity can occur for medical wastes. Yet, if adoption of new regulations is coordinated withcareful planning and expedient permitting, suchshortfalls may be averted.
costs
The variable nature of the equipment design, size,and add-on pollution control equipment make itimpractical to identify the typical cost of treatingmedical waste by incineration (104, 54).
13Incinera-
tion costs can vary by more than 500 percent, and
OTA’s contractors independently identified widecost ranges from $0.07 per pound to over $0.50 perpound (104, 54). The California Air ResourcesBoard estimates that uncontrolled incineration costsare about $0.15 per pound and controlled incinera-tion costs about $0.50 per pound (108). It isgenerally believed that incineration is a more costlyalternative than most nonincineration treatmentalternatives; some estimates find autoclaving to be30 percent of the cost of incineration (104).
CARB also calculated the estimated cost toretrofit existing facilities to meet its proposedstandards to be an increase of $0.16 per pound of waste burned. If on-site incinerators are shut downand off-site incineration is used, costs are estimatedto increase by $0.35 per pound. If steam sterilizationis used, on-site, a $0.10 per pound cost is estimated,and if incinerators are shut down and off-site steam
sterilization is used, a cost of $0.17 per pound isexpected (108).
Risks
Relative health risks associated with the combus-tion of medical wastes continue to be debated as dataremains limited. A thorough examination of healthand environmental risks posed by different pollut-ants is beyond the scope of this effort; these risks areaddressed elsewhere (116, 66, 12, 108). The inten-tion here is to identify those pollutants of primaryconcern in medical waste incineration because of their potential human health and environmentalimpacts.
These pollutants include dioxins and furans (someof which are thought to be carcinogens), pathogens(entities with infection potential), metals (e.g.,cadmium, a neurotoxic chemical and thought to bea probable human carcinogen), acid gases (e.g.,hydrogen chloride (HC1), nitrogen oxides, and sulfurdioxides), which can cause acute effects such as eyeand respiratory irritation, can contribute to acid rain,and may enhance the toxic effects of heavy metals),and particulate emissions (which can absorb heavymetals and organics and 1odge in human lungs, and
serve as irritants possibly responsible for chronichealth effects). Their presence in either air emissionsor ash residue is a concern.
14
A large data base for dioxins and furans and theirpotential carcinogenicity makes them a particularsource of concern. It is presumed by regulators thatcontrolling emissions of these organics will controlemissions of other organics (PAHs), cadmium, andperhaps particulate matter and HC1.
15Emissions of
these organic compounds from medical waste inci-
nerators have been noted (see table 6 and figures 9,10, and 11). Barton et al., in a study for the EPA andCARB, hypothesize that dioxin and furan formationcan be minimized by controlling particle and traceorganic emission levels within the combustion zone,minimizing the time particles are held at tempera-tures that maximize dioxins and furan formation andmaximizing the destruction of precursors (both
13EPA, as p~of it s Nsps Pqram form~ic~ waste incinerators, is evaluating the capital and operating costs of various W pollution con t ro l devi~s
and incinerators; the preliminary results ar e expected in late 1990.
Idsee OTA, 1989 (1 16 ) for a discussion of fisks associated with MSW incinerator a ir emissions ~d ash r esidues, which m aY be simil~ t o ~“se
associated with some forms of medical waste incineration.
15~@scrubber systems (i.e., acid ga s r e m o v ~ pl US particulate removal), high removal of particulate matter gene~lY me~s ‘i@ ‘em ovd ‘f ‘ea ~
me t a l s (except possibly mercury) and moderate t o high con t ro l of dioxins~~s (~d other semi-volatile organics). I t appears that par ticulate mattercontrol is the key to controlling the pollutants no t ed here, because t h ey m e converted to a solid (particulate) form to facilitate their removal from thegas (20).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 57/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 58/82
Chapter 4-Incineration Treatment Issues and Trends q 49
Figure 9-Comparison of PCDD/PCDF Concentration in Medical and Municipal Wastes
c
100
10
Medical waste Municipal waste
SOURCE: R. Barton, G. Hassel, W. Lanier, and W. Seeker, State of the Art Assessment of Medical Waste Thermal Treatment, EPA Contract 68-03-3365 andARB Contract A832-155 (Irvine, CA: Energy& Environmental Research Corp., 1989).
Figure 10—Comparison of PCDD/PCDF Emissions From a Variety of Incinerators
Emitted PCDD/PCDF concentrations Medical
Municipal waste incineratorswaste
incinerators
12000 I
6000
Hazardouswaste
incinerator
ESP - Electrostatic precipitatorDI - Dry sorbent injectionFF - Fabric filterSD - Spray drierV - Venturi scrubberCYC - CycloneDS - Dry scrubberWS - Wet scrubber
*Note that ng/Ncm represents measurements normalized to standard concentration of 12% C0 2
SOURCE: R. Barton, G. Hassel, W. Lanier, and W. Seeker, State of the Art Assessment of Medical Waste Thermal Treatment, EPA Contract 68-03-3365 andARB ContractA832-155 (Irvine, CA: Energy& Environmental Research Corp., 1989).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 59/82
50 q Finding the Rx for Managing Medical Wastes
Figure n-Comparisons of Cadmium Emissions From a Variety of Incinerators
Cadmium
Municipal solid waste
Medical Hazardous
waste waste
- (,
0[
u
0.1
0.01
0001
0.0001
ESP = Electrostatic precipitator
DI = Dry sorbent Injection
FF = Fabric filter
SD = Spray drier
V = Venturi scrubber
CYC = CycloneDS = Dry scrubberWS = Wet scrubber
IWS = Ionizing wet scrubber
WSH = Water spray humidifier
PBS = Packed bed scrubber
A = Data not available
D = Metal below detection Iimit
dscf . dry standard cubic foot; 1 gr/dscf = 2.290 g/Ncm
SOURCE: R. Barton, G. Hassel, W. Lanier, and W. Seeker, State of the Art Assessment of Medical Waste Thermal Treatment, EPA Contract 68-03-365 andARB Contract A832-155 (Irvine, CA: Energy& Environmental Research Corp., 1989).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 60/82
Chapter 4-Incineration Treatment Issues and Trends q 51
levels are defined by standards.17
CARB, for exam-ple, reports that tests demonstrate high efficiencyVenturi wet scrubber systems, as well as dry
scrubber systems, at well-designed and operatedincinerators can reduce risks to acceptable levels,defined by their standards to one to three chances ina million (49, 108). It should be noted though that theheterogeneous nature of the medical waste streammakes it nearly impossible to conclude with cer-tainty what the emission levels of certain substanceswill be in any given unit. For example, two hospitalswith similar incineration systems can have highlydifferent emission test results largely due to thedifferences in their waste streams and charging
methods (104).
TRENDS IN AIR POLLUTIONCONTROL SYSTEMS
Until a few years ago when the first major studyof emissions from hospital incinerators was com-pleted and some localities set more stringent airemission standards, air pollution equipment associ-ated with these incinerators was minimal (126).
Today, some form of scrubbing system is considereda standard part of many new incineration systems,although most medical waste incinerators remainuncontrolled and pollution control equipment is notnecessarily a standard part of medical waste inciner-ation systems (41). Pollution control devices cur-rently in use on medical waste incinerators includewet or dry acid gas scrubbers (to remove/neutralizeacid gases, etc.), baghouses (fabric falters) or electro-static precipitators (to remove airborne particulatematter), hybrid dry/wet scrubbers, and afterburners
(sometimes used on excess air combustors to reducetoxic organic gases).
A fairly common list of toxic compounds andcriteria pollutants to be controlled has evolvedthrough the development of regulations and thepermitting process. These substances are: particu-late, hydrogen chloride, sulfur dioxide, carbonmonoxide, nitrogen oxides, dioxins, furans, mer-cury, arsenic, cadmium, chromium, nickel, zinc, andlead (104) (see table 7).
The selection of air pollution control systemsinvolves choosing between a wet or a dry scrubbersystem. A scrubber is an emission control device that
adds alkaline reagents to react with and neutralizeacid gases, with the resultant products collected formanagement of residue. For a dry scrubber this isusually done through the use of a baghouse (fabricfalter) to trap solid particles (dust), while for a wetscrubber byproducts are discharged as a slurry,possibly requiring treatment before discharge to thesewer. In the future, depending on the type of scrubber used and the sewage discharge standards inan area, wastewater treatment may also become amore common feature of medical waste incineration
systems. This could add significantly to the capitalcost of an incineration system utilizing wet scrub-bing (e.g., a wastewater treatment system can cost$150,000 (8)). However, a condensing wet scrubbersystem with zero liquid discharge, a technology usedfor hazardous waste incineration, is being adaptedfor application to medical waste incineration. Itappears that this could be an efficient and costeffective system for controlling emissions frommedical waste incinerators (2).
These scrubber systems can control dioxin andfuran emissions as well as particulate emissionsbecause dioxins and furans in flue gases condenseonto fly ash particles if the gases are cooled enough.They are then removed by the scrubber or particulatecontrol system (1 16). In MSW incinerators, thecombination of a dry scrubber and baghouse canremove 97 to 99 percent of total dioxins present inpostcombustion flue gases (1 16).
As noted, the proposed regulations in California
first identified a dry scrubber as BACT
18
Theincineration industry reported, however, that the dryscrubber/baghouse combination is not suitable forall medical waste incinerators, although this appearsto be primarily based on cost considerations. As onestudy concluded, “Venturi [wet] scrubbers, due totheir lower capital costs and greater flexibility, arethe best choice for smaller and medium size hospitalincinerators’ and dry scrubbers, while ‘‘not as pop-ular or as proven in the field, ” are cost competitivefor larger facilities (12 tons per day or more) (26).
17This is me ~ess Zt iO risk is re@red, which no technology---or waste management praCtiCC-Can ac~eve.
lsc~ifornia used EPA data on d r y scrubbers u sed for MSW incinerators (usually a spray atomizer-baghouse s y s t em) to medicd w*te incin~ators.Medical waste incinerators which do use dry scrubbers usually have dr y inj@ion baghou s e systems with injection of a dry alkaline substance into theflue gas, which reacts with pollutant s and is then captured in th e baghou s e (41).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 61/82
52 q Finding the Rx for Managing Medical Wastes
Table 7—Performance Data of Medical Waste Incinerators With Pollution Control Equipment
“Typical”average of Lowest
Emission measured three samples reported Units of measurement1.
2.
3.
4.
5.
6.
8.
9.
10.11.12.13.14.15.16.
17.
Particulate including Method 5 impinger catch, 0.028 0.018
without CHEAF installed 69.2 44.589.0
Particulate including Method 5 impinger catch, 0.014 0.008
with CHEAF installed
HCI (hydrogen chloride)
SO2 (sulfur dioxide)
CO (carbon monoxide)
HF (hydrogen fluoride)
As (arsenic)Be (beryllium)Cd (cadmium)Cr (chromium)Ni (nickel)Pb (lead)Hg (mercury)TCDD equivalent (dioxins)TCDF equivalent (furans)
34.6 19.897.3
9.2 0.9815.0 1.699.3
4.0 0.3111.4 0.8992.118.8 8.7
Note: Worst case reported is 68 ppm (voI) dry basis @770020.08 Not detected0.094 —
95.6 —
<0.05 —
<0.25 —
1.02 0.960.045 0.030.112 0.06
10.74 5.822.96 1.860.0311 0.02640.1088 0.0967
Total TCDD & TCDF as TCDD equivalent 0.1399 0.1231
Opacity 2 0
Grain/sdcf @7%02mg/Nm
3dry @7% O2
% RemovalGrain/sdcf@7?4002mg/Nm
3dry @7% O2
% Removalppm (voI) dry basis @7% O2
mg/Nm 3 dry @7%O 2
% Removalppm (voI) dry basis@7Y002mg/Nm 3 dry@7% O 2
% Removalppm (voI) dry basis @7% O2
ppm (voI) dry basis @7% O2
mg/Nm 3 dry @7% O2
% Removalmg/Nm
3dry@ 7Y002
fg/Nm3dry@ 7% O2
fg/Nm3dry@ 7% O2
fg/Nm3dry @7%O 2
fg/Nm3dry@ 7Y002
fg/Nm3dry@ 7?4002
fg/Nm3dry@ 7 %O 2
fg/Nm3dry@ 7%02
fg/Nm3dry@ 7 %O 2
fg/Nm3dry@ 7 %O 2
PercentNOTE: These data were collected from over 20 installations of medical waste incinerators with scrubbers in the United States in the period from Jan. 1,1988
through Apr. 1, 1990. They do not necessarily represent the best performance which can be achieved, but do represent “typical” performance whichcan be expected from the equipment and systems reviewed b y the study. Some data are supported b y ove r 100 sepa rate samplings, while some
(including the detailed metals and dioxin information) are based on only one or two installations with three samplings each. Nm3represents
normalization of measurements to standard 70/. 02conditions. 1fg=10 -15 grams.
SOURCE: Anderson 2000 Inc., Technical Description, Performance Information, Material Balance and Flowsheet Data, Typical Guarantees and TurnkeyInstalled Pricing for a 16.2 MM BTU/HR (1700#/HR) State-of-the-Art Medical Waste Incinerator With Wet Scrubber Emission Controls, Document#1-5670-W (Peachtree City, GA: Anderson 2000 Inc., 1990).
EPA reports that there are no technical reasonswhy a dry injection system or a spray dryer systemcannot be applied to medical waste incinerators (41).
Reports that the baghouse in medical waste incinera-tor applications is susceptible to corrosion becauseof the intermittent operation, which can result inholes in the bag, should not occur if the system isproperly designed and operated (41, 49). Further, dryscrubbers do not have any associated waste waterproblems.
Wet scrubbers can remove about 95 to 99 percentof HC1 and 85 to 95 percent of sulfur dioxideemissions in MSW incinerator applications (116,
45). Wet scrubbers can achieve 90 percent HClremoval with plain water in medical waste incine-
rators, but lime slurries or caustic soda solutions canresult in 99 percent or better hydrochloric acidremoval (139, 126). The California Air Resources
Board reports 85 percent particulate removal, 99percent hydrogen chloride removal and O to 75percent cadmium removal by wet scrubber systemsfor a medical waste incinerator (108). Reheating theflue gases may be necessary to ensure adequatedispersion from the stack and compliance withambient air quality regulations, although it is notclear that any medical waste incinerators have had todo this (41).
19
The WCEI maintains that advanced (versus con-
ventional Venturi) wet scrubbing systems can attainhigh removal efficiencies for fine particulate, acid
ls7’hat is , we t scrubbing COOLS t ie flue gases to the water sat eration temperatur e which can be as low as 120OF . AS a result, p l umes l eav ing t h e s@ckdo not rise very h igh which can increase ground level concent rat ions of polluta nt s (1 16).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 62/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 63/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 64/82
Chapter G-incineration Treatment Issues and Trends . 55
ered. Another strategy is to use dedicated incine-rators for medical wastes at sites permitted for MS Wincineration (104). Sweden and the Federal Republicof Germany take a similar approach. In addition topermitting the use of high-volume MSW incine-rators for medical waste, these governments allowco-locating infectious waste incinerators with MSWincinerators and channeling their flue gases throughthe high efficiency air pollution control equipmentof the larger incinerator (57).
A variation of co-incineration is a demonstrationproject sponsored by the Department of Energy-Morgantown Energy Technology Center and Penn-sylvania Energy Development Authority whichco-fires medical waste with coal in a circulatingfluidized bed with steam recovery (27). Suggestionshave also been made that medical waste regionalfacilities configured as hazardous waste incinerators(which burn at extremely high temperatures) couldbe efficient enough to cofire hazardous or other“problem wastes” with medical wastes. Wastetypes suggested for co-incineration with medicalwastes include: household hazardous waste, scraptires, and some commercial waste (66). To date nosuch co-incineration facility exists.
There are plans for a hazardous waste (rotary kilnincinerator) facility in California to burn medical aswell as hazardous waste. This facility is in the permitprocess and has an expected start date in 1992 (104).In some European countries, MSW and medicalwaste facilities are sometimes designed as hazard-ous waste incinerators (57).
25
Regional Incineration
Regional facilities for medical waste managementmay be privately owned and/or operated, or may becooperatively owned and/or operated by a number of generators. It is also conceivable that, as with MSWincineration, some of these facilities might be run bya municipality or by a municipality in conjunctionwith a private company and/or a number of genera-tors (31). Regional incineration of medical waste ona commercial basis began in earnest in 1986, whenthe demand for services was high, capacity wasscarce, and permit requirements for air emissionscontrols were simple and uniform (104).
In the four short years since then, the aggressivepursuit of permits and development of facilities bywaste management companies have made greatercapacity available, even though the regulatory cli-mate for permitting such incineration has becomecomplicated and variable. Indeed, the more compli-cated regulatory situation for incineration of medicalwastes is one reason the demand for off-site treat-ment has remained high. At this point, hospitals andlarge generators in at least two metropolitan areas,Baltimore and New York City, are cooperativelyplanning a regional facility, usually as part of abroader planning effort for a regional waste manage-ment strategy. This section discusses these differentapproaches to off-site, regional incineration of medical waste: commercial (privately run) regionalincineration and generator-run regional incineration.
Commercial Regional Incineration
The two largest waste management companies inthe United States, Waste Management, Inc. andBrowning-Ferris Industries, have aggressively de-veloped medical waste incineration sites on anational basis; a number of other smaller companies(e.g., Medigen, Atwoods, and Incendere) have done
the same on a more regional basis (104). As theconditions for permitting these facilities have be-come more problematic, closer scrutiny is beinggiven to the size, type, and location of the regionalsites. The waste management industry has called fora ‘ ‘leveling of the playing field, ” i.e., for uniformperformance standards on a national basis in orderthat companies operating in more than one State willhave similar requirements to meet. In addition,on-site and off-site incinerators would be subject tothe same requirements; a state of affairs which can
favor a larger scale operation (104).
Permitting is a long, difficult process for anyfacility—an-site or off-site—whether it be for medi-cal wastes, MSW, hazardous wastes, or low-levelradioactive wastes. Yet, for medical waste incinera-tion, it is probably more difficult to permit an off-sitethan an on-site facility, although the on-site facilitymight operate quite similarly to the off-site facility(e.g., accept wastes from other generators). On-siteincineration has the benefit of possible waste heatutilization and reduced transportation of waste.Indeed, some waste companies have attempted tolocate on the site of a hospital or large generator.
MA f;lcl[lfy LIIa[ buns MSW :{nd mcdlc~ WaSkX In Stroud, Oklabom~ is ah equipped m a way Sh ih 1 0 a h z = d o u s wa s t e facili~.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 65/82
56 q Finding the Rx for Managing Medical Wastes
Three significant hurdles in the siting and permittingof off-site, commercial incinerators are: addressingpublic concerns over potential risks posed by
incineration, meeting zoning permit requirementsand addressing transportation issues (e.g., the ‘ ‘im-portation’ of wastes for the facility).
26
The lengthy and difficult nature of the permittingprocess has had a dramatic impact on the economicsassociated with the construction of a regionalmedical waste incinerator. Permitting a site can takeup to two years or more to complete beforeconstruction of a facility. This can encourage theconstruction of larger facilities or multiple facilities
on a site.Other factors can favor siting smaller units. For
example, some communities are willing to accept asmaller facility that will manage their own commu-nity’s or local region’s medical waste, but areopposed to a facility that acts like a magnet for theimportation of wastes from great distances. Also,depending on the service needs of an area, havingseveral facilities rather than one large unit willprovide convenient backup capacity when a unit isdown for maintenance or repairs (104). It appears
that a mixture of large and small facilities will beconstructed depending upon the type of companyoperating each, the scope of intended service, andreceptivity of the local community (104). It is likelythat the developmental trend of regional incinerationfacilities for medical waste incinerators will mirrorsomewhat the ups and downs of the regulatoryclimate, at least until that becomes more uniform andcertain in nature.
Nonprofit/Generator Regional Incineration
Although the number of cooperative arrange-ments between hospitals and other medical wastegenerators within regions is not as high as somemight have predicted a few years ago, several sucharrangements are being developed in different areasof the country. Examples include: the Baltimore areamedical waste project; the Greater New York Hospital Association plans for a facility for metro-politan New York, and the facility planned by theNassau-Suffolk Regional Council on Long Island,
New York.
The Baltimore regional facility is designed some-what like a utility, A number of factors led to theparticular regional approach taken in this area.
Hospitals were responding to a dramaticallychanged climate for medical waste managementbrought on by the media coverage of washups of syringes in the Baltimore area and related publicconcern, new State and local regulations that re-sulted, and consequent concerns over the viability of present management practices by various facilities(given, for example, a newly instituted ban of medical wastes by a local MSW incinerator, amoratorium in one county on incinerator construc-tion, etc.).
The Maryland Hospital Association at the requestof its members then solicited bids for a long-termsolution to the medical waste management needs of the area hospitals (25).
27These efforts were soon
re-directed when a newly organized corporation, theMedical Waste Associates (MWA), presented aproposal to develop a privately-owned medicalwaste disposal facility. Eventually, to secure a freedcost for financing the facility, ‘‘tax exempt’ statuswas obtained for the $24 million bond issue. The
central features of the arrangements between MWAand the individual hospitals are that participatinggenerator facilities will sign ‘ ‘put or pay’ contracts(i.e., each hospital agrees to pay for the disposal of a minimum number of tons of waste per year) for 20years (with renewal options every 4 years), andMWA will charge a flat rate of $300/ton ($0.15/ pound) for their disposal privilege. A rebate arrange-ment exists to share the profits of ‘excess’ capacitysold to others, and MWA will pay the ‘‘founding’hospitals 50 percent of any net profits earned fromcogeneration activities (e.g., sale of byproducts suchas steam, ash, etc.) (25).
The facility will have a 160-tons-per-day capacityin two incineration units; 120 tons are reserved forthe participating hospitals. This facility will acceptonly medical wastes, including wastes from officesof doctors on the staffs of a participating hospital.Hospitals find it attractive that the facility willaccept nonsegregated medical wastes, but this fea-ture and the ‘‘put or pay’ nature of the contractcreate little incentive for reduction and recycling
~sl%bhc concern over the siting of medcal waste facilities and the importance of public involvement in the permitting and siting processes are topicsbeyond the scope of this effort. Public concerns and the impacts of participation are net dissimilar to those expressed for MSW facilities that are discussedin OTA, 1989, see especially, chapter 8 (1 16).
27Cmley ~d Born (25) provide a more detailed account of the development of the Baltimore rewond medic~ wrote facfli~.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 66/82
Chapter 4-Incineration Treatment Issues and Trends q 57
efforts. There are 31 hospitals in the region to beserviced by the facility (as restricted by a special cityordinance). Construction began on the facility in thespring of 1990; it is expected to open in 1991.
The Greater New York Hospital Association hasformed a cooperative to build a state-of-the-artfacility to service the participating hospitals in themetropolitan New York area. Citizen and environ-mental interests, unions, waste companies, and cityand State officials, as well as the generator interests,are involved in the planning of this facility as part of their development of a broader medical wastemanagement plan. The New York City Health &Hospitals Corp. initiated a related but separate effortfor a comprehensive waste management study toevaluate the potential of waste reduction and recy-
cling opportunities for area hospitals before deter-mining the most appropriate type of regional incin-erator. The Natural Resources Defense Councilhosted an initial meeting of interested parties in theirNew York office, November 30, 1989, to discusssome of the initial study plans for developing theregional medical waste management plan.
This plan also sets targets to reduce the volume of medical waste, explores toxicity reduction efforts,
and identifies feasible recycling opportunities forhospitals. A critical feature of the planning isensuring that the sizing of regional incineratorfacilities factors in the impacts that reduction andrecycling efforts might have on capacity needs in anarea.
The Nassau-Suffolk Hospital Council, Inc. repre-sents 22 nonprofit hospitals on Long Island, NewYork and also has been in the process of establishinga nonprofit corporation for a regional disposalfacility, This regional planning effort, as with the
metropolitan New York effort, includes efforts toimplement reduction and recycling services in thehospitals. At this point, the council has adopted aninterim strategy that involves use of autoclave/ compaction units (see ch. 3) by the hospitals on-siteand then shipment to several existing communityMSW incinerators with excess capacity. A regionalmedical waste incinerator is still planned for thefuture, and sites for it are being investigated now(68).
Community involvement in the development of plans such as these is key to their acceptability. Forexample, the disinfection of wastes prior to shipment
to the off-site incinerator can allay community
concern over the transportation of the wastes. Theentire load of waste (which is mixed in the compac-
tion process with nonregulated medical wastes) is
manifested to meet the requirements of MWTA. Asnoted above, there are no technical reasons to
preclude the burning of medical waste in MSW
incinerators. The pollution equipment on a state-of-
the-art facility should adequately control emissions
from the medical wastes. Adjustments can be made
to facilitate safe handling of the wastes to minimizeworker contact and any risks associated with expo-
sure. In the case of the Long Island hospitals,
pathological wastes and sharps will not be sent to the
MSW incinerators, but instead sent to an upgradedhospital incinerator. This interim plan allows the
closure of 11 older incinerators, which would notmeet New York in 1992 (68).
State new standards taking effect
SUMMARY
Incineration of medical waste is likely to remain,
at least for the next decade, the cornerstone of management methods for medical wastes in much
the same way landfilling is for MSW managementefforts. Yet, as has already occurred with MSWmanagement, this necessary and appropriate treat-
ment option for certain wastes can be effectively
supplemented by other treatment technologies (e.g.,autoclaving, chemical/mechanical disinfection, etc.).The size, type, and nature of pollution control
equipment will continue to change as the regulatory
issues evolve. There is general agreement amongregulators and the regulated community that devel-
opment of uniform regulatory standards for air
emissions and site permitting would help stabilize
the regulatory climate for medical waste manage-ment and assist in the further identification andassessment of risks associated with incineration. Inaddition, regulatory determinations r e g a r d i n g t h emanagement of incinerator ash are necessary toaccurately project costs for ash management and
facilitate decision making by health-care facilitiesregarding the attractiveness of the incinerationalternative on the basis of costs.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 67/82
Chapter 5
Special Treatment Issues
A number of management issues associated withpackaging, handling, and disposal practices inter-face with decisions regarding treatment methods formedical waste. This chapter examines m a n a g e m e n tdevelopments for a number of such treatment issues:sharps management, small generator management,sewer use, and shredding.
SHARPS MANAGEMENT
Special attention is given to the management of sharps (e.g., hypodermic needles and syringes; alsoscalpels, broken glass, etc.) because of both theoccupational and general public risks they pose.Sharps, specifically syringes, are generated by bothhouseholds (e.g., in-home health-care) and health-care facilities. They are therefore part of both thegeneral MSW and medical waste stream. In Wash-ington State’s survey of occupational exposure of waste industry workers to infectious waste (with 438of the 940 workers surveyed responding), 21 percentof the respondents reported having sustained aneedlestick injury on the job from both medical andresidential sources (139).
1The ATSDR, based on its
literature survey and study, estimates that 500 to7,300 medical waste-related sharp injuries occurannually to solid waste workers (93). Surveys of health-care workers, including housekeeping staff,usually indicate much higher incidence of needle-stick injuries.
2Sharps cause concern not only
because of their infectious potential, but also be-cause of the direct prick or stab type of injury thatcan result from them (114; see also 96). It is in partfor this reason that EPA included unused sharps inits definition of regulated waste types under MWTA.
Most of the concern over the management of sharps has focused on the packaging of used sharps,the integrity of which is critical to containing thesharps during their collection, storage, and transpor-tation to the treatment or disposal site. Currently,puncture-resistant containers are the preferred han-
dling package for sharps (122, 118, 120, 121). Yet,a number of new techniques for containing sharps,particularly needles and syringes, continue to emerge(e.g., encapsulation).
Education of health-care and refuse workers, aswell as the general public, about the proper disposalof sharps will facilitate their safe handling andmanagement. Segregation of sharps and their sepa-rate collection and management without compactionis key to reducing the risk of injury associated withtheir management. In King County, Washington(Seattle area), there is a local requirement that allsharps be segregated and disposed of in leakproof,impermeable plastic containers with tight lids forseparate, uncompacted collection and transportationto a landfill. This management strategy greatlyreduces the risk of human contact with the sharpsand the potential of needlestick injuries (111).
Manufacturing
Some of the efforts to ensure the safer handling of sharps have been made at the manufacturing stage.The attempt by manufacturers of sharps is toincorporate into the syringe a mechanism which willrender it “nonsharp’ immediately after it has beenused. One method for achieving this is a sheatharound the barrel of the syringe that will slide uparound the needle when used while the barrel part is
held. This makes it impossible for a needlestick injury to occur and the end product can be disposedof in a bag with other regulated waste items (unlessthe facility’s protocol dictates otherwise) (104).These syringes are costly, however, restricting theiruse to date to high-risk areas of health care. Theirpotential as a feasible and practical method of protection in the home health-care setting seemsapparent, although this application has not yetoccurred, presumably due to their higher cost (104).Tests of the performance and reliability of thesesyringes were not identified by OTA.
lhte~s~ly, 32 percent of the respondents reported direct conta ct with wast e blood on t heir clothin g or shoes and l’g percent repofled Mving
received oc cupa t i on r d cuts an d scratches (139). Need l e s t i c k injuries while prevalent are not necessarily the most common type of occupational hazardfor wast e workers (e.g., back stra in an d other types of injuries ar e more prevalent ).
@ne survey by a local union of the Service Employees I n t e rm t i o n a l Union (the Nation’s I arges t health -care u nion) of its hospital workers in the Sa nFrancisco area, found that 62 percent reported accidental ne ed l e s t i c k injuries on the job (100; see also 91).
–59–

8/14/2019 9018
http://slidepdf.com/reader/full/9018 68/82
60 q Finding the Rx for Managing Medical Wastes
Mechanical/Chemical
Although grinding, clipping, and other practices
are no longer used for sharps management, primarilydue to their potential for worker injury or exposurethrough aerosolization of microorganisms duringthe procedure, new techniques have appeared, e.g.,chemical treatment and shredding of sharps. Theprimary alternative method of sharps managementof this sort is the mechanical/chemical disinfectionprocess discussed in chapter 3. In another processthe needle part of the syringe is placed in a box whileholding the barrel part. The needle completes anelectrical circuit that melts it and leaves only the
barrel in need of disposal. This process is a bit timeconsuming given the individual treatment of eachsharp, but it does probably meet the “treated anddestroyed” criteria of MWTA (141). Again, it maybe a process for which the appgenerator settings is most practica
Encapsulation
Another process introduced with
ication to small(104).
in the last couple
of years that is experiencing some success isencapsulation of sharps. This process involves use of a phenolic solution to disinfect sharps and thenintroduction of an oxidizing agent as a catalyst toencapsulate the waste in a polymer matrix, i.e., asolid block-like material. This material can then bedisposed of as solid waste without risk to theworkers handling it (114, 104). It does not, however,meet the ‘‘treated and destroyed’ criteria of MWTAregulations (141).
This system is also expensive, currently four tofive times higher than the cost of comparablecontainers for sharps (104). This factor makes itsapplication for high-volume generators largely im-practical, but the process could facilitate handlingsharps for the small generators and home health caresince it both disinfects and immobilizes the sharps,allowing for their disposal with other solid waste.
Some States (such as California, where smallgenerators are required to manage their medicalwastes in an approved reamer) have endorsed theprocess and in some cases permitted its use as analternative treatment technology. Until more Statesendorse this process, it is unlikely that it will gainwidespread adoption (104).
Concern has been expressed over potential im-pacts of these blocks of encapsulated sharps to thesolid waste stream, in particular over what signifi-
cance (if any) incinerating them with other wasteswould have. Where landfilling of the “blocks” isnot allowed, the encapsulated sharps are in somecases shipped via the United Parcel Service (UPS) toa manufacturer of the process in Georgia (see below)(104).
Mail Shipment for Disposal
The mail shipment of wastes for disposal is anincreasingly common practice. As noted above,encapsulated sharps are sometimes shipped by UPS.
Apparently, they are one of the few types of wastethat nonpostal shipping companies will acceptbecause they are rendered noninfectious prior toshipment.
A number of companies now operating werecreated primarily to cater to the needs of small orrural generators for viable disposal options. Theyoperate out of several States and accept wasteshipments from generators and then transport thewastes to treatment facilities. A contractor to OTA
identified such operations in four States: Indiana,New Jersey, Oklahoma, and Texas (104). One of these firms claims over 30,000 clients nationwideand transfers the material to an incinerator in yetanother State (104).
Most States authorizing waste by mail mandatethat their State requirements be met, even if thewaste is being mailed out of the State. For example,California authorizes out-of-state shipment only if the waste is rendered noninfectious prior to disposal.
International shipment is allowed also if the waste istreated frost in-state (104). Under MWTA, genera-tors in States covered by the demonstration programare allowed through an exemption in the regulationsto ship medical waste sharps through the mail,provided they meet the specified packaging require-ments (40 CFR 259). This exemption is intended toencourage small quantity generators (e.g., doctors’offices) to dispose of medical wastes properly (141).
For the most part, most of the medical wastesshipped are sharps. Some tissues and laboratoryspecimens are mailed to laboratories for diagnosticpurposes. Historically, laboratory samples, etiologicagents, and other medical items have been shippedthrough the postal service. Some basic postalpackaging requirements exist and the practices have

8/14/2019 9018
http://slidepdf.com/reader/full/9018 69/82
Chapter Special Treatment Issues q 61
been the subject of congressional hearings (e.g., 54Federal Register 1197(.)).
Concerns have been raised not only about the
potential hazard or at least negative perceptionassociated with handling medical wastes and house-hold mail through the same postal system, but alsoover the operation of these waste mail companiesthat essentially operate as transfer stations (104).The scope of current regulation does not cover suchoperations. These practices warrant further investi-gation, particularly over the adequacy of currentregulations governing the shipment of wastesthrough the mail and the desirability of such systemsfor small generators and rural health-care facilities.
SMALL GENERATOR -MANAGEMENT
The amount of medical wastes generated nation-ally from non-hospital settings is not known (al-though EPA will reportedly be including suchestimates in its first report to Congress). These smallgenerators include such sources of medical wastes
as: home health-care patients, doctors’ offices (in-cluding dental and veterinarian), and rural health-care settings. Although some States are includingsome small generators of medical wastes, such asdoctor and dental offices, in their regulatory pro-grams for medical wastes, most exclude households.
The equity of including some and not all genera-tors of medical wastes under regulations is hotlydebated.
3It is widely recognized that the same types
of controls are not feasible for both large and small
generators. The focus of the debate is over wheretodraw the regulatory line between generators to beincluded or excluded from regulation and over howlarge the gulf should be between the level of scrutinyand degree of requirements for large versus smallsources of medical wastes.
In the area of medical waste policy, the demandfor a comprehensive scope for controls is beinggrappled with from the beginning of regulatoryefforts. EPA issued guidelines for home health-care
disposal shortly after it promulgated its standards forMWTA (130). Other guidelines are being developed
and discussed in response to the increased attention
to wastes from these sources and their infectiouspotential (102; see also 82, 83).
The need for developing feasible and economical
treatment and disposal options for small generators
is widely acknowledged. Few advocate including
households under medical waste regulations, but
concerns over solid waste worker safety are real. The
need for viable disposal options for rural hospitals,
small laboratories, and different types of doctors’
offices are also real. Some technologies have already
been adapted for nonhospital sources. For example,for a number of years a mobile sterilization system
has been used in Berlin, West Germany, to collectdoctor office and nursing home medical wastes.
There are plans by a hospital council on Long Island,New York, to attempt to bring this technology to the
United States (68).
For small generators, the most promising of the
emerging treatment methods discussed in this report
are the nonincineration treatment methods and the
newer management methods for sharps. These
options may provide safe and economically feasibleon-site treatment alternatives for small generators.
Off-site incineration is also an option, since somemedical waste companies will contract to pick up
and transport to their incinerator medical wastes
from doctor and dental offices and other small
generator sources.
Careful and creative management strategies will
be key to ensuring effective handling and treatment
of these wastes. Limited information and assistance
are available to households, small and rural hospi-tals, and other smaller generators to help them devise
effective medical waste management plans andsystems. Education efforts are clearly important butto date are limited to an EPA brochure for house-holds, to be distributed by health-care providers or
others (130).
qclemly, mWlatiom are usually adopted not beeau s e they are permived as “fair,’ but rather beeau s e they a re n ecessary to achieve some social oreconomic goal of the greater public. That regulations be “rea.somble” maybe di f . fku l t to define, but a legitimate standard by which to judge them. Inmost areas of environmental policy, regulatory attention is first focused on the largest generators of the problem. Later, refinements are made to theregulations and their scope broadened to include other s ign i t3can t sources.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 70/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 71/82
Chapter 5--Special Treatment Issues . 63
required to achieve nonrecognizability. This lack may account for the apparent reluctance to applyshredding technology to emerging treatment meth-ods.
8The necessity for criteria or standards for this
and other treatment and destruction methods willperhaps best be evaluated after the completion of MWTA demonstration program.
Yet other factors, such as the difficulty existingshredding systems have with the heterogeneity of the medical waste stream and the high maintenance
associated with shredders, may account for their
limited application to date. It may be that improve-
ments and refinements to shredding technologies
will occur, particularly if the nonrecognizabilitycriterion is more widely incorporated into medicalwaste regulations, and the use of shredders is
increased. In any case, disinfection of infectious
medical wastes before shredding to minimize poten-tial aerosolization of pathogens is desirable.
%teresfigly, me r e a r e specific shredding sta nda rds for document destr uction by the Depart ment of Defense for confidentiality (1~).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 72/82
Chapter 6
Comparisons of Treatment Alternatives
However great the achievements of reduction andrecycling efforts, there will continue to be a need foreffective treatment and disposal for wastes thatcannot be recycled. Although incineration remains,and is likely to continue to remain, a primarytreatment method for medical wastes for the foresee-able future, a number of other treatment alternativesare available and will supplement incinerationtechnology. As concerns over the cost, safety, andpermitting/siting of incineration facilities continue,so too will the favorable climate for emerging
nonincineration technologies. New variations of autoclave, mechanical/chemical, radiation, and mi-crowave treatment methods are now commerciallyviable. Other emerging technologies are in thetesting or even conceptual stages. Currently, Statesplay the critical role in evaluating and approvingalternative treatment technologies. Inconsistenciesexist among the States and increasingly Federalguidance on evaluation and approval of treatmentalternatives is suggested as necessary and desirable(e.g., suggestions of participants at the OTA Medical
Waste Workshop, 1990).
An important given when comparing alternativesis that whatever treatment alternative is used, someform of additional solid waste disposal must occur.In all cases, ultimately, some degree of dependencyon landfills remains. For medical waste incineration,the ash becomes a waste product requiring landfill-ing. For autoclaving, microwaving, and irradiationeither incineration and/or landfilling is necessary.The residue from the chemical/mechanical treatment
alternative will be discharged to the sewer orlandfilled. The difficulty of landfilling even treatedmedical wastes, given refusals by some landfilloperators, remains a significant obstacle for man-agement in some areas of the country. Interstateshipment and international exportation of solidwaste, including medical wastes, is an emergingenvironmental and political issue nationally (1 16).
Valid comparisons of various treatment alter-natives for medical wastes are problematic be-cause different types of treatment goals areserved by different technologies (e.g., the goal canbe treatment to render wastes noninfectious; ornoninfectious and nontoxic; or noninfectiousnonrecognizable, and/or nontoxic). This means
that different techniques may be appropriate fordifferent waste types. Treatment alternatives willdiffer in the nature of the emissions that warranttest protocols, control measures and operatingparameters specific to each technology.
Obviously, costs and risks associated with thealternatives will vary. Further, a number of considerations concerning liabilities and costsinfluence generator decisions about on-site ver-sus off-site treatment. Treatment alternatives are
more easily scaled to various types and sizes of facilities. Comparisons between off-site and on-site applications of various alternatives can alsobe problematic. With all of these differences,clearly, comparisons of the treatment technolo-gies must be made carefully. Such comparisonsare imprecise, but helpful in highlighting thevarious features and considerations associatedwith the alternative treatment technologies.
CAPABILITIES AND RISKS
Table 8 compares the various treatment technolo-gies discussed in chapters 3 and 4. All of thesetreatment alternatives can effectively managemost infectious wastes; the only ones that areusually used to treat pathological waste are theincineration and mechanical/chemical disinfec-tion systems. Depending on the type of incineratorand the nature of its controls, incineration is the onetreatment alternative that could manage all of ahealth-care facility’s wastes, i.e., pathological and
other infectious, hazardous (possibly, depending onthe design and controls of the incinerator), adminis-trative, food, and other non-patient wastes.
From other perspectives, nonincineration al-ternatives may have advantages over incinera-tion. In general, there are more serious emissionsconcerns associated with incineration than mostalternatives. Yet, it is true that because incinerationis a more established technology, emission concernshave been more clearly identified. The human healthand environmental risks may be presumed to be lessfrom nonincineration treatment alternatives but ad-ditional study, particularly of water effluents fromsome of the systems, is necessary. Generally, healthrisks associated with the various treatment technolo-
-65-

8/14/2019 9018
http://slidepdf.com/reader/full/9018 73/82
66 q Finding the Rx for Managing Medical Wastes
Table 8—Comparison of Treatment Technologies
Costs (approximate)d
“Regulated medical Operating or per pound
wastes” appropriate for charges (not including Capital (equipmenttreatment method to render Volume reduction labor; depreciation; profit/ and installation)
Treatment technology wastes non-infectious (%) return) ($/lb./hr.) ($ K)
Steam autoclave . . . . . . . . All, except pathological o $0.05-$0.07 $100 K (on-site)Autoclave with
compaction . . . . . . . . . . Ail, except pathological 60-80% $0.03-$0.10 $100 KMechanical/chemical . . . . . All 60-907. $0.06 $40-350 KMicrowave
(with shredder) . . . . . . . Alla 60-907. $0.07-$0.10 b $500 K
Irradiation(with grinder) . . . . . . . . . All, except pathological 60-90% $0.15 Not available
incineration . . . . . . . . . . . . Allc 90-95% $0.07-$0.50 $1,000 K (on-site)
apathologi~l ~a~te~ are usu~ly nottreat~ by rnicrowavedue to esthetic reasons, Cytotoxical Orothertoxic Chemicals cannot IM adequately treated to dUCe
their hazardous nature.b[n~~ing an energy cost of $0.07/kWh.cAlthough separation of noncombustibles ad items with problematic ~ns t i tuen ts improves combustion efficiency (See ch. 3).dReiiable Cmt information is difficult to obtain and verify. Further, valid comparisons are diff icul t t o m~e given the different circumstances under which VariOUS
technologies operate (e.g., amount of waste treated and its effect on costs, etc.)
SOURCE: Office of Technology Assessment, 1990.
gies have not been thoroughly studied. Presumably,pollution controls could adequately control pollut-ants of concern for both nonincineration and inciner-ation alternatives. Of course, the more pollutioncontrols necessary, generally, the more expensivethe treatment.
The concerneconomic state
jeopardized by
COSTS
that the already generally precariousof the health-care industry could befurther regulation of medical waste
management warrant s examination. Presently, theexact amount a health-care facility spends onmedical waste management is often not known withcertainty even by the facility’s management. Theadditional cost that new controls, alternative treat-
ment technologies, or management practices mightentail can not be accurately assessed unless currentcosts can be understood with some certainty.
Available cost estimates for various treatmenttechnologies indicate that on-site incinerationcan be comparable or significantly higher in coststhan other on-site alternatives (30; 104). Whilecosts for on-site alternatives can be estimated fairlyconstantly, the same is not true for off-site alterna-tives. OTA contractors found from informal discus-sions with generators of medical wastes and opera-tors of medical waste services throughout thecountry that the price charged for any type of off-sitetreatment is never determined solely on the basis of costs, but rather by ‘‘what the market will bear. ’Given that it is a highly competitive industry, this
does not necessarily mean that off-site waste facili-ties reap an unusually high profit, but, as noted inchapter 3, the medical waste industry is healthy.
It appears that hospitals and other health-carefacilities eligible to receive Medicare reimburse-
ment can theoretically be reimbursed for someon-site medical waste management costs. Althoughthere is no specific category for waste managementreporting, some percentage of capital costs and someoperating costs could be covered (54). In the State of New York the eligibility of health-care facilities forMedicare reimbursements for some on-site medicalwaste costs (and regional utilization of an on-sitehospital treatment facility) is explicitly addressed bythe Department of Health (85). Although no hospi-tals have been known to request Medicare reim-
bursement to date, it was part of the New York Statelegislative debate over increasing the reimburse-ment rates for hospitals (80).
Other types of grants offered by some Stateenergy offices, such as those that will cover someportion of the capital costs for waste-to-energyfacilities, may also reduce a facility’s share of costsfor this type of incineration (31). For example, inNew York State, a proposed Environmental bondissue, which will be on the ballot in November 1990,will provide $50 million in State assistance forregulated medical waste projects. The grant programwould be administered by the State Department of Health and would provide funding for up to 50percent of the project costs. To be eligible, a facilitymust participate in a waste audit and must develop

8/14/2019 9018
http://slidepdf.com/reader/full/9018 74/82
Chapter 6-Comparisons of Treatment Alternatives and Policy Issues for Federal Action . 67
a plan for recycling, product reuse, and wastereduction (94).
The volume of waste handled by a treatment unit
and its effect on the operating cost of the unit ishighly variable, but generally costs are lower foron-site incineration and nonincineration alterna-tives. The capital costs associated with incinerationare significantly higher than those for most alterna-tive treatment technologies. Yet, heat recovery (and,as noted, programs that will reimburse up to half thecapital costs for waste-to-energy facilities) andefficient operation (e.g., including recycling inconjunction with incineration) may reduce incinera-tion costs to the facility and result in a more
favorable cost comparison of incineration to theother technologies (31). Nonetheless, the potentiallyhigh cost of disposal of incinerator ash, if it isclassified as a hazardous waste, is also a potentialsignificant cost factor associated with incinerationthat must be considered. Other factors that affectcosts, such as reduced cost of transportation, reduceddisposal costs, and reduced liability, are relevant toa decision to manage wastes on-site v. off-site.
Costs, even so, are only one of a number of factors(e.g., nonrecognizability, liability, and ability to
render wastes non-infectious) that health-care facili-ties consider when deciding what type of treatmentalternative to use and whether to manage wasteson-site or off-site. Clearly, a facility may be able toreduce its costs and liability and have greater controlby managing wastes on-site; however, on-site man-agement also represents a major institutional com-mitment of resources to waste management, which
is not the primary function of the health-care facility.As has been noted throughout this report, a numberof factors favor off-site treatment as well.
Ultimately, each generating facility must weighthe various factors and determine which wastereduction and management alternatives are mostappropriate for its circumstances. Public policiesshould recognize and not preclude the variablesolutions necessary to meet individual generators’waste management needs. In addition, medicalwaste policies shouldsort of protocols toreliability and safetytives.
help through the use of somereduce uncertainty over theof various treatment alterna-
It remains to be seen what direction Congress andFederal agencies, and the medical and health-careindustry and community will define for medicalwaste management. It will be important, though, thatany legislative or regulatory activity acknowledgesand appropriately addresses the variety of manage-ment issues and available treatment technologiesdiscussed in this report. Experiences with manage-ment of other components of our society’s wastesindicate that effective waste management is basedon a recognition that there are a variety of viable
management options available and appropriate tomeet particular site-specific circumstances, andprevention or reduction and recycling efforts areincluded in these options. Adopting a more compre-hensive approach to medical waste policy may offerthe greatest prospect for adoption of a program thatwill ensure the safe, cost-effective management of medical wastes.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 75/82

8/14/2019 9018
http://slidepdf.com/reader/full/9018 76/82
70 qFinding the Rx for Managing Medical Wastes
Box D—The Medical Waste Tracking Program
EP A established th e 2-year pilot F ederal tr acking program au thorized by MWTA by publishing its “Stan dard s for theTracking and Management of Medical Waste; Interim F inal Rule and Request for Commen ts ‘‘ in the Federal Register in March
1989, which took effect in June 1989. 1 The tr acking system for m edical wast es designates r ecordkeeping requiremen ts forfacilities that gen erat e over 50 pounds a m onth of medical waste an d requir es the u se of a four -part form for an y off-she shipmen t
of medical wastes. EP A and t he St ate m ust be notified if a generat or does not receive a copy of th e ma nifest form from th e fina l
dest ination faci li ty. Generators of medical waste t hat produce less than 50 pounds a re su bject to the same h andling requirements,
except instead of using the tracking form they must maintain a log (i.e., as a reporting requirement).
EP A has au th ority to assess civil pena lties of up t o $25,000 per day for each violation, criminalp e n a l t i e s o f u p t o $ 5 0 , 0 0 0
per da y per violation, and jail term s of up to 5 years may be imposed in States implementing the tracking system (sec. 11005).
Sta tes ha ve the au th ority to conduct inspections a nd t ake en forcement a ctions a s well. The MSWTA does not specify wheth er th eEPA or the States has lead enforcement authority and the EPA regulations do not specify enforcement roles, but the Agency
prepa red an enforcement str ategy which encour ages Sta te implemen tat ion. Flexibility is given to the St at es to develop a var iety
of approaches t o compliance an d en forcement (134). EP A restricts its role to encour aging volun ta ry compliance th rough its
various education efforts and by providing States with guidance and assistance when needed (e.g., when a violation involves
wastes from or t ran sported to a nonpar t icipating State).
EPA, also as part of the MWTA demonstrat ion program, issued requirements tha t generat ors of waste m ust follow beforemedical wastes leave the site to be shipped to authorized treatment or disposal facilities. Under the demonstration program,
generat ors include institu tional and commercial sources of wastes in th e part icipating St ates a nd t erritories. Of course, any
treatment facilities accepting regulated medical wastes may be subject to other Federal, State, and local laws and regulations.
The MWTA does not consider r esidential sources of medical waste to be regulat ed generat or sources, nor does it addr ess problems
with the disposal of wastes associated with illegal drug use. EPA issued guidance information on proper home medical waste
disposal and states in its pamphlet describing the MWTA that drug enforcement, Clean Water Act programs, and citizen litter
cont rol projects will help elimin at e ‘‘flagr an t du mpin g of wastes. ’ (130)
According to the MWTA requirements, generators must separate regulated medical wastes from general refuse, meet storage
requirements (if such wastes are stored before treatment), and package regulated wastes in labelled, rigid, leak-resistant
containers. In addition, special separation and packaging requirements are specified for both sharps and fluids. To help ensure
that packages retain their integrity during handling and transportation, secondary packaging (i.e., a rigid outer container) is
genera lly requir ed for sh ipping. This secondar y packaging can be reu sed if th oroughly cleaned. The pa ckage labels must iden tifythe content , generator, and t ran sporter of the wastes.
Medical wast es incinera ted on-site, or t reat ed by other meth ods (e.g., some t ype of disinfection un it) tha t m eet both
regulatory criteria of treatment and destruction (i.e., waste is ‘‘processed by a means to reduce levels of infectious agents” and
waste is “no longer generally recognizable as medical waste”), do not need to be tracked under the demonstration program, but
instea d generat ors mu st subm it a report t o EPA. The position of th e EPA is that if th e biological and ph ysical hazar d of th e waste,
as well as t heir ‘visually offensive nat ur e, “ is altered they can be managed according to regulations applicable to solid waste.
The required report must be a summary of the volumes and types of medical waste treated on-site during the first 6-month period
of the program; a second report covers the 13 to 18 months of the program.
I since t h i s t ie , t h e Agency h a s issued a n umber of guides for the public, generators and tra nsporters about t ie Fede~ ~ program(128).
improved management of medical waste will need to beevaluated independently. GAO (134) has evaluated theefforts to date of the EPA and States to implementMWTA. For this reason, their implementation activity isnot evaluated here. Apparently, despite early controversyover the listing of wastes by the Agency to be tracked andconcerns over compliance costs, as well as the initial typeof confusion usually associated with new regulatoryprograms, the implementation of MWTA demonstrationprogram has been rather smooth. EPA reports that most
of the early violations were minor in nature (e.g., errors incompleting manifest forms, etc.), although fines havebeen levied against responsible parties for such violationsas incomplete record keeping and failing to lock storageareas (88).
A number of issues that EPA and ATSDR are required
by MWTA to address (e.g., health effects of medical
waste, generation information, cost implications, small-
quantity generator issues) also is not discussed exten-
sively in this study. The focus of this effort is on availableand emerging management methods, including waste
reduction and recycling possibilities. This emphasis onthe evaluation of treatment technologies is intended to
alleviate immediate concerns over the nature, availability,
and tradeoffs of various treatment methods and tostimulate a broader consideration of management alterna-
tives for medical waste than is currently typical.
8/14/2019 9018
http://slidepdf.com/reader/full/9018 77/82
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
Adelstein, J. and McKusick, K., ” ‘Not in My Back
Yard’: Low-Level Radioactive Waste and Health,”The Harvard Medical School Health Letter, April1986.Advanced Concepts Inc., Ultra High Eficiency
&roLiquidDischar-ge Hot Gas Scrubbers lnfonna-
tion Packet (San Diego, CA: 1990).Allen, R., Brenniman, G., Logue, R. and Strand, V.,Bacterial Emissiom From Incineration of HospitalWaste, ILENR/RE-AQ-88/17 (Springfield, IL: Illi-nois Department of Natural Resources, July 1988).American Diabetes Association, Position State-ment: Insulin Administration (Alexandria, VA:
ADA, National Service Center, 1990).American Hospital Association, TechnicaZ Docu-ment Series, Infectious Waste (Chicago, IL: 1989).
American Society of Mechanical Engineers, “Pro-posal to Develop a Training Course for Operators of Medical Waste Incinerators” (Washington, DC: nodate).
Anderson 2000 Inc., Technical Description, Per-
formanceInforrnation, A4aterialBalance andFlow-sheet Data, Typical Guarantees and Turnkey In-
stalled Pricing for a 16.2 MM BTUIHR (1700#iHl?)State-of-the-Art Medical Waste Incinerator With
Wet ScrubberEmission Controls, Document #I-5670-W (Peachtree City, GA: 1990).
Ashworth, R., “The Modem Medical Waste Incin-eration Facility, ’ paper presented at the Incinera-tion Conference of 1990, University of California,Irvine, and Co-Sponsor, San Diego, CA, May14-18, 1990.
Associated Press Newswire, “Hospital ReportedlyNot Good at Recycling,” June 27, 1990.Axness, C., “Management of Biomedical Waste atRefuse-Derived Fuel Facilities,’ manuscript (New-port and Elk River, MN: Northern States Powerco.).
Baram, M., “Hospital Management of MedicalWaste: Legal Framework and Policy Issues,” Ch.Vl: Perspectives on Medical Wastes (Albany, NY:The Nelson A. Rockefeller Institute of Gover-
nment, State University of New York, 1989).Barton, R., Hassel, G., Lanier, W. and Seeker, W.,State of the Art Assessment of Medical WasteTher-maZ Treatment, EPA Contract 68-03-3365 andARB Contract A832-155 (Irvine, CA: Energy andEnvironmental Research Corp., 1989).
Battelle, “MEDPAK; Products, Packaging, andProcesses: Improved Management of Solid &Infectious Wastes, ” A Multiclient Proposal (Co-lumbus, OH: 1990).
14.
15.
16.
17.
18.
19.
20.
21.
21a.
22.
23.
24.
25.
26.
Bayfront Medical Center, “Recycle & Reclaim
Waste-to-Energy Project,” pamphlet (St. Peters-burg, FL: 1990).Becker, A., Physicians Health Insurance Co., per-sonal communication, June 1990.
Belkin, N. L., “Do Reusable or Disposable GownsGive Better Protection Against Infection?” Laun-dry News 8(2):10,17-18, 1982.
Bernstein, R., General Medical Corp., personalcommunication, June 1990.
131enkham, D. B., ‘‘The Journal of Infection ControlNursing--On the Right Track” Nursing Times
83(22):64-68, 1987.
Brill, D., Allen, E.W., Lutzker, L., et al., “Disposalof Imw-bvel Radioactive Waste: Impact on theMedical Profession,” Journal of the AmericanMedical Association 254(17):2449-2451.
Bma, T., U.S. Environmental Protection Agency,Research Triangle Park, NC, personal communica-tion, June 1990.Campbell, D., “Hospital Waste Management inCanada,” Proceedings of the National Workshopson Hospital Waste Incineration and Hospital Sterili-zation, U.S. Environmental Protection Agency, SanFrancisco, CA, May 1988.
Carey, L., “Linen Poses Higher Infection Risk toLaundry Worker than Patient” Laundry News,February 1982, p. 10, 13.Church, T, Cooper, P. and Nakamura, R., “ThePolitical and Regulatory Environment of MedicalWaste: Formulation and Implementation of theMedical Waste Tracking Act,” Report to theMedical Waste Policy Committee (a public policyproject administered by the Nelson A. RockefellerInstitute of Government, State University of NewYork, Albany) (Albany, NY: State University of New York, 1989).Collins, B.J., et al., “Safety of Reusing DisposablePlastic Insulin Syringes,” Lancet 1(8324):559-61,1983.
Cooley, L., Radiation Safety Office, University of Maryland, Baltimore, personal communication, June1990.
Cooley, L., and Born, C., “Development of aRegional Medical Waste Facility: A Case Study,”draft manuscript, University of Maryland at Balti-more, 1990.Corbus, D., “A Comparison of Air Pollution
Control Equipment for Hospital Waste Incine-rators,” paper presented to the 83rd Air and WasteManagement Association Annual Meeting, Pitts-burgh, PA, June 24-29, 1990.
–71–

8/14/2019 9018
http://slidepdf.com/reader/full/9018 78/82
72 qFinding the Rx for Managing Medical Wastes
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
3’7.
38.
39.
40.
Coulthard, E., Donlee Technologies, Inc., personalcommunication, June 1990.
Council on the Environment of New York City,
“Waste Paper Recycling Program: Feasibility Study,Beth Israel Hospital,” Office Paper RecyclingService (New York, NY: October 1988).
Cross, F., “The Case for Regional Incineration of Hospital Waste,” Proceedings of the First NationalSymposium on Incineration of Infectious Waste,Washington, DC, May 1988.
Cross, F., “Evaluation of Alternative TreatmentTechniques for the Treatment of Solid MedicalWastes,’ ch. IV, Perspectives on Medical Wastes,(Albany, NY: The Nelson A. Rockefeller Instituteof Government, State University of New Yorlq
1989).Cross, F., Crossflessitore & Associates, Inc., per-sonal communication, May 1990.
Cross, F., Incineration for Hospital and MedicalWastes for Incinerator Operators (Mataway, NJ:SciTech Publishers, Inc., 1990).Curtis, F., “Testing for Medical Waste IncineratorDestruction Efficiency for Surrogate Indicator Or-ganisms,” paper presented to the 83rd Air andWaste Management Association Annual Meeting,Pittsburgh, PA, June 24-29, 1990.
Cusak, J., Combustion Engineering, personal com-munication and microwave information packet,NOV. 14, 1989.Cusa.k, J., ABB Environmental Services, Inc.,personal communication at Medical Waste ReviewPanel, May 29, 1990.Cuthbertson, B., and Petruska, M., “RegulatedMedical Waste and the Medical Waste TrackingAct,” Plant, Technology & Safety Series, The JointCommission on Accreditation of Healthcare Organ-izations, 1989 series, 4:7-1 1.
Daschner, F. D., “Practical Aspects for Cost Reduc-tion in Hospital Infection Control,” Infection Con-trol 5(1):32-35, 1984.
Dhooge, P., and Rogers, T., “Infectious Wasteprocessing With an Electiocatalytic Oxidation Sys-tem,’ paper presented to the Hazwaste Expo Atlant89 Conference (Albuquerque, NM: Delphi Re-search, Inc., 1989).
Doucet, Lawrence G., Infectious Waste Treatmentand Disposal Alternatives (Peekskill, NY: Doucet& Mainka, P. C., 1989).
Doucet, L., “Institutional Waste Incineration,”
presentation at the Environmental ManagementWorkshop: An Integrated Approach to HazardousWaste Management, sponsored by the AmericanSociety for Hospital Engineers of the AmericanHospital Association (Peekskill, NY: Doucet &Mainka, P. C., 1987).
41.
42.
43,
44,
45.
46.
47.
48,
49.
50.
51.
52.
53.
54.
54a.
Eddinger, J., U.S. Environmental Protection Agency,Research Triangle Park, NC, personal communica-tion, May 1990.
Electric Power Research Institute, “T’he PlasmaTorch: Revolutionizing the Foundry Fire,” EPRZ
Journal, October 1986, pp. 12-19.Emmerrnan, J., Waste Management, Inc., personalcommunication, May 1990.Engelbrecht, R., and Amirhor, P., “Inactivation of Enteric Bacteria and Viruses in Sanitary LandfillLeachate,” NTXVPB0252 973/AS (Springfield, VA:National Technical Information Service, 1975).Etter, R., (written) Testimony and Supplement forthe Hearing on the Clean Air Act Amendments of 1989, Subcommittee on Environmental Protection,
Committee on Environment and Public Works,Sept. 21, 1989, U.S. Senate, S. Hrg. 101-331, Pt. 1(Washington, DC: U.S. Government Printing Of-fice, 1989).Forder, A. A., “Infection Risks in the Re-Use of Disposable,” Nursing RSA 4(2):4245, 1989.
Forshey, R., San-I-P~ personal communicationand information packet, October 1989.Forshey, R., San-I-Pak, personal communication,June 1990.Fry, B., California Air Resources Board, personalcommunication, and presentation, “Air Toxics andMedical Waste Incinerators,” Incineration Confer-ence, University of California, Irvine and Co-Sponsors, San Diego, CA, May 14-18, 1990.Garibaldi, R.A., et al., ‘‘Comparison of Nonwovenand Woven Gown and Drape Fabric to PreventIntraoperative Wound Contamination and Postop-erative Infection,” American Journal of Surge~152(5):505-509, 1986.
Glasser, H., and Chang, D., “Analysis of the Stateof California’s Biomedical Waste Incinerator Base,’paper presented to the 83rd Air and Waste Manage-
ment Association Annual Meeting, Pittsburg, PA,June 24-29, 1990.Greenough, A., et al., “Disposable Syringes forInsulin Injedioq’’B&hMedicalJournal 1(6176):1467-
8, 1979.
Griffith, N. C., and Schell, R.E., “NosocomialInfections, ’’American Family Physician 35(6):179-
186, 1987.
Guttman, R., “Survey and Analysis of Costs of Disposing of Medical Wastes,” OTA contractreport, (Beverly, MA: Robert A. Guttman, Esq.,1990).
Hagenmaier, H., Kraft, M., Brunner, H., and Haag,R., “Catalytic Effects of Fly Ash From WasteIncineration Facilities on the Formation and Decom-position of Polychlorinated Dibenzo-p-dioxins andPolychlorinated Dibenzofurans,” Environ. Sci. Tech-nol. 21(1 1):1080-1084, 1987.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 79/82
References q 73
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
Harwood, S., Occupational Safety and Health Ad-ministration, personal communication, June 1990.
Hedrick, E., ‘What Is ‘Infectious Medical Waste’?”Plant, Technology & Safety Series, The JointCommission on Accreditation of Healthcare Organ-izations, 1989 series, 4:24-28.
Hershkowitz, A., ‘‘Incinerating Infectious Waste inthe United States: A Critical Comparison WithSwitzerland, the Federal Republic of Germany, andSweden,” Plant, Technology & Safety Series, TheJoint Commission on Accreditation of HedthcareOrganizations, 1989 series, 4:29-35.
“Infectious Waste: International Concerns, ” PanelDiscussion, The 1989 Incineration Conference,Knoxville, TN, May 1-5, 1989.
Jackson, M. M., “Rituals Without Reason: Updat-ing the Curriculum in Infection Control,’ NLNPublications 15(2154):171-188, 1986.
Jacobson, J. A., “Fever, Chills, and HypotensionFollowing Cardiac Catheterization With Single-andMultiple-Use Disposable Catheters,” Catherizationand Cardiovascular Diagnosis 9(1):3946, 1983.
Jacques, L., et al., ‘‘Bacteriological Study of Handsand the Use of Soap in the Hospital Environment,”Biomedicine and Pharmacotherapy 37(9- 10):415-418, 1983.
Jordan, W., Waste Tech, personalMay 1990.
Jordan, W., Waste Tech, personalJune 1990.
Klein, B. S., et al., “Reduction
communication,
communication,
of NosocomialInfection During Pediatric Intensive Care by Protec-tive Isolation,” New England Journal of Medicine320(26):1714-21, 1989.
Knack, R., as quoted in News Release, IroquoisHealthcare Consortium, “Healthcare EmployeesRecycle, Reduce, Reuse,” Albany, NY, June 15,1990.
Lauber, J., and Drum, D., “Best Controlled Tech-nologies for Regional Biomedical Waste Incinera-tion,” paper to be presented at the 83rd AnnualMeeting of the Air and Waste Management Associ-ation, Pittsburgh, PA, June 27, 1990.
Lopez, H., Beth Israel Hospital, New York, NY,personal communication, May 4, 1990.
Lord, J., Nassau-Suffolk Hospital Council, Inc.,New Yorlq NY, personal communication, May 9,1990.
Marriot Food & Service Management, “Marriott,
Standard Textile to Provide Recyclable, ProtectiveSurgical Packs,” The F&SM Bulletin, Apr. 20,1990.
McCabe, G., Battel.le Human Affairs, personalcommunication, June, 1990.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
McGrane, J., New York City Health HospitalsCorp., New York, N , personal communication,May 8, 1990.
Malina, J., and Sgik, B., eds., Virus Survival inWater and Wastewater Systems, Water ResourcesSymposium Number Seven, Center for Research inWater Resources (Austin, TX: University of Texasat Austin, 1974).Meaney, J., and Cheremisihoff, P., “Medical WasteStrategy,” Pollution Engineering, October 1989,pp. 92-106.Medical Waste News, “Money Matters,” 2(5):33,
Mar. 7, 1990.
Medical Waste News, “Study Predicts BiomedicalWaste Business will Boom in 1990s,” 2(7):51, Apr.
4, 1990.Medical Waste News, “Ozone Watch,” 2(9):65,May 2, 1990.
Medical Waste Policy Committee, Perspectives onMedicaZ Waste, A Report of the Nelson A. Roeker-feller Institute of Government, State University of New York, Albany) (Albany, NY: State Universityof New York, 1989).
Miejer, R., Winfield, personal communication, July1990.
Milbum, T., “Biomedical Waste Incineration BA~
Application Considerations,” Proceedings of the
Third National Symposium on Infectious WasteManagement, Chicago, IL, April 1989.
Miller, M., “Miller Urges More Money for Hospi-tals,’ ‘ News Release from Speaker Mel Miller,Albany, ~, Jan. 30, 1990.
Mineo, R., and Rosenthal, A., “Start-Up andTesting of a Hospital Waste Incinerator,” paperpresented to the 83rd Air and Waste ManagementAssociation Annual Meeting, Pittsburg, PA, June24-29, 1990.
National Committee for Clinical Laboratory Stan-dards,
“Clinical Laboratory Waste,” ProposedGuideline, NCCLS Document GP5-P, vol. 6,N0. 15(Villanova, PA: September 1986).
National Committee for Clinical Laboratory Stan-dards, “Protection of Laboratory Workers FromInfectious Disease Transmitted by Blood and Tis-sue, Proposed Guideline, NCCLS Document M29-P, vol. 7, No. 9 (Villanova, PA: November 1987).
Nenonen, L., RACORSE Network, Oakland, CA,personal communication, May 9, 1990.
New York State Department of Health, A StatewidePlan for Treatment and Disposal of Regulated
Medical Waste (Albany, NY: State Hospital Reviewand Planning Council, August 1989). .
Onel, S., “The Medical Waste Tracking Act of 1988: Will It Protect Our Beaches?” VirginiaEnvironmental Law Journal 9(1):225-247, fdl 1989.

8/14/2019 9018
http://slidepdf.com/reader/full/9018 80/82
74 qFinding the Rx for Managing Medical Wastes
8-7.
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.
98.
99.
100.
Penberthy Electromelt International, Inc., “Hospi-tal Wastes Destroyed in Penberthy Molten GlassFurnace,” Seattle, WA, 1990.
Petruska, M., U.S. Environmental Protection Agency,personal communication, Dec. 21, 1989.Petruska,M., U.S. Environmental Protection Agency,personal communication, May 7, 1990.Poteet, G.W., et al., “Outcome of Multiple Usage of Disposable Syringes in the Insulin-Requiring Dia-betic,” Nursing Research 36(6):350-352, 1987.Research Triangle Institute, “Review and Evalua-tion of Existing Literature on Generation, Manage-ment, and Potential Health Effects of MedicalWaste,” prepared for the Health Assessment Sec-tion, Technical Assessment Branch, Office of Solid
Waste, U.S. Environmental Protection Agency(Research Triangle Park, NC: November 1988).Research Triangle Institute, ‘‘Medical Waste Treat-ment Techniques, ’ draft final report, prepared for(under subcontract to Dynamac Corp., Rockville,MD) EPA Contract No. 68-01-7266 (ResearchTriangle Park, NC: October 1989).Rodenbeck, S., Agency for Toxic Substances andDisease Regnstery, personal communication, July1990.
Rounds, C., Albany Medical Center, personal com-munication, and “New York State Department of Environmental Conservation Medical Waste Incin-erator Operator Taskforce, ” paper presented at theIncineration Conference, University of California,Irvine, and Co-Sponsor, San Diego, CA, May14-18, 1990.Rutala, W., Odette, W., and Sarnsa, G., “Manage-ment of Infectious Waste by U.S. Hospitals, ”Journal ofAmerican MedicalAssociation 262:1635-1640, 1989.
Rutala, W. and F. Sarubbi, ‘Management of Infec-tious Waste From Hospitals,” Infectious Waste
Management 4(4):198-203, 1983.Rutala, William, et al., ‘Decontamination of Micro-biological Waste by Steam Sterilization,” AppliedEnvironmental Microbiology, vol. 33, 1982.
Ryan, P., “Questions and Answers From the 4thNational Conference on the Expanding Importanceof Central Service in Infection Control, HospitalTopics 56(5):6-8, 1978.
Santolevi, J., and Kraftz, R., “Medical WasteIncineration Requirements for System Design Mod-ifications, ’ Proceedings of the Third NationalSymposium on Infectious Waste Management,
Chicago, IL, April, 1989.Service Employees International Union, AFL-CIO,CLC (SEIU), Local 250, “Needlestick SurveyResults: San Francisco Area Private, Non-ProfitHospitals” (Washington, DC: SEIU, December1987).
101.
102.
103.
104.
105.
106.
107.
108.
109.
110.
111.
112.
113.
114.
Sharp, James, Vice President, Stencycle, personalcommunication, May 1990.
Simmons, B., Trussler, M., Roccaforte, J., Smith, P.,
and Scott, R., “Infection Control for HomeHealth,” draft manuscript (Memphis, TN: Method-ist Health System, 1990).
Sobsey, M., “Field Survey of Enteric Viruses inSolid Waste,” American Journal of Public Health68:858-863.
Spurgin, R., Spurgin & Associates, Medical WasteTreatment Technologies, contract report for theOffice of Technology Assessment, Mar. 16, 1990.
Starkey, D.H., and Hirnmelsbach, C.K., “InfectionControl-Central Service: On the Avoidance of
Failures in Sterilization,” Hospitals 48(13):143-52,1974.
State of California Air Resources Board, TechnicalSupport Document to Proposed Dioxins and Cad-mium Control Measure for Medical Waste Incine-rators, prepared by Toxic Air Contaminant ControlBranch, Stationary Source Division, California AirResources Board, May 23, 1990.
State of California Air Resources Board, DrafiSummary of State Mealcal Waste Regulations,prepared by Toxic Air Contaminant ControlBranch, Stationary Source Division, California Air
Resources Board, June 1990.State of California Air Resources Board, ProposedDioxins Control Measure for Medical Waste Inci-nerators, State Report, Stationary Source Division(Sacramento, CA: May 25, 1990).
Sulmer, P., “Defining and Managing InfectiousWaste,” Plant, Technology & Safety Series, TheJoint Commission on Accreditation of HealthcareOrganizations, 1989 series, 4:17-23.
Tbrnberg, W., “An Examination and Risk Evalua-tion of Infectious Waste in King County, Washing-
ton” (Seattle, WA: Seattle-King County Depart-ment of Public Health, Mar. 18, 1988).
Thrnberg, W., Washington State Department of Ecology, personal communication, May-June 1990.
U.S. Congress, Office of Technology Assessment,Technologies and Management Strategies for Haz-ardous Waste Control, OTA-M-196 (Washington,DC: U.S. Government Printing Office, March1983).
U.S. Congress, Office of Technology Assessment,Serious Reduction of Hazardous Waste, OTA-ITE-
317 (Washington, DC: U.S. Government PrintingOffice, September 1986).
U.S. Congress, Office of Technology Assessment,Issues in Medical Waste Management--BackgroundPaper, OTA-BP-O-49 (Washington, DC: U.S. Gov-ernment Printing Office, October 1988).

8/14/2019 9018
http://slidepdf.com/reader/full/9018 81/82
References . 75
115. U.S. Congress, Office of Technology Assessment,“Medical Wastes on Our Coasts: Issues and Im-pacts, ” staff paper, April 1989, presented at theSecond International Conference on Marine Debris,
April 2-7, 1989, Honolulu, HI and the 1989Conference on the State of Our Coastal and OceanResources, May 10-12, 1989, New York, NY.
116. U.S. Congress, Office of Technology Assessment,Facing America’s Trash: What Next for Municipal
Solid Waste? OTA-O-425 (Washington, DC: U.S.Government Printing Office, October 1989).
117. U.S. Congress, Office of Technology Assessment,Partnerships Under Pressure: Managing hw-
Level Radioactive Waste, OTA-0426 (Washing-ton, DC: U.S. Government Printing Office, Novem-ber 1989).
118. U.S. Department of Health and Human Services,Centers for Disease Control/National Institutes of Health, “Biosafety in Microbiological and Bi-omedical Laboratories” (Atlanta, GA: 1984).
119. U.S. Department of Health and Human Services,Centers for Disease Control, ‘Guidelines for Hand-washing and Hospital Environmental Control”(Atlanta, GA: 1985a).
120. U.S. Department of Health and Human Services,Centers for Disease Control, “Guidelines for thePrevention of Surgical Wound Infections’ (Atlanta,GA: 1985b).
121. U.S. Department of Labor and U.S. Department of Health and Human Services, “Protection AgainstOccupational Exposure to Hepatitis B Virus (HBV)and Human Immunodeficiency Virus (HIV), JointAdvisory Notice, Oct. 19, 1987.
122. U.S. Environmental Protection Agency, Guiak forInfectious Waste Management, EPA/530-SW-86-
014 (Washington, DC: May 1986).123. U.S. Environmental Protection Agency, Proceed-
ings of the Meeting on Medical Wastes, Annapolis,MD, NOV. 14-16, 1988, (EPA)F-89-~PF-FFFFF-48.
124. U.S. Environmental Protection Agency, ‘The Su-
perfund Innovative Technology Evaluation Pro-gram: Technology Profiles,” EP~540/5-88/033(Washington, DC: 1988).
125. U.S. Environmental Protection Agency, Office of Solid Waste, ‘Tracking Medical Wastes,’ EPA/530-SW-89-020 (Washington, DC: March 1989).
126. U.S. Environmental Protection Agency, ControlTechnology Center, Operation and Maintenance of HospitalMedical Waste Incinerators, EPA450/3-89-
002 (Research Triangle Park, NC: March 1989).127. U.S. Environmental Protection Agency, Control
Technology Center, Hospital Incinerator OperatorTraining Course: Volumes 1 and H, EPA-450/3-89-
003 and EPA-450/3 -89-O04 (Research TrianglePark, NC: March 1989).
128. U.S. Environmental Protection Agency, Managingand Trach”ng Medical Wates, (includes “A Guideto the Federal Program for Generators,” “A Guideto the Federal Program for Transporters,” and “A
Guide to the Federal Program for Treatment,Destruction, and Disposal Facilities,’) Solid Wasteand Emergency Response, EPW530-SW-89-021 to023 (Washington, DC: September 1989).
129. U.S. Environmental Protection Agency, ‘Costs andBenefits of Phasing Out Production of CFCS andHalons in the United States,’ review draft, Office of Air and Radiation (Washington, DC: November1989).
130. U.S. Environmental Protection Agency, “DisposalTips for Home Health Care,” Solid Waste andEmergency Response, EP~530-90-014A (Wash-
ington, DC: January 1990a).131. U.S. Environmental Protection Agency, Handbook~
Operation and Maintenance of Hospital MedicalWaste Incinerators, Office of Air Quality Planningand Standards, EPA/625/689/024 (Research Trian-gle Park, NC: January 1990).
132. U.S. Environmental Protection Agency, Methods toManage and Control Plastic Wastes, Office of SolidWaste and Emergency Response, EPN530-SW-89-051 (Research Triangle Park, NC: Feburary 1990).
133. U.S. General Accounting Office, Infectious Waste:Federal Health Care Facilities’ Handling and
Disposal Practices, GAO/HRD-89-84 (Washing-ton, DC: May 1989).
134. U.S. General Accounting Office, Medical WasteRegulation: Health and Environmental Risks NeedTo Be Fully Assessed, GAO/RCED-90-86 (Wash-ington, DC: March 1990).
135. U.S. NuclearRegulatory Commission, BeZow Regu-latory Concern; Policy Statement, Washington,DC: June 27, 1990
136. University of California, Irvine, Low-Level Radio-active Waste Management in Medical and Biomedi -
cal Research Institutions, Low-Level RadioactiveWaste Management Handbook Series, U.S. Depart-ment of Energy Contract Nos. DE-AC07-761D01570 and C85-1OO675 (Idaho Falls, ID:EG&G Idaho, hlC,, March 1987).
137. Wagner, K., “The Federal Role in Medical WasteManagement,’ Plant, Technology & Safe~ Series,The Joint Commission on Accreditation of Healthcare Organizations, 1989 series, 4:12-16.
138. Ware, S., “A Survey of Pathogen Survival DuringMunicipal Solid Waste and Manure TreatmentProcesses,’ EpA-600/8-80-034 (Cincinnati, OH:
U.S. Environmental Protection Agency, August1980).
139. Washington State Department of Ecology, Solidand Hazaxdous Waste program, Report to theLegislature: Washington State Infectious Waste

8/14/2019 9018
http://slidepdf.com/reader/full/9018 82/82
76 qFinding the Rx for Managing Medical Wastes
Project and Attachments (Olympia, WA: Dec. 30, field, VA: National Technical Information Service,1989). July 1986).
140. Weir, G., “Characteristics of Medically RelatedLow-Level Radioactive Waste,” U.S. Depmtment 141. Wilson, M., U.S. Environmental ProtectionAgency,
of ~ergy Cmtract No. DIWG07-851D12605 (Spring- personal communication, May 1990.





























