Embed Size (px)
Citation preview

1403
□ CASE REPORT □
A Case of Adult-onset Adrenoleukodystrophy with FrontalLobe Dysfunction: A Novel Point Mutation in the
ABCD1 Gene
Shinichiro Inoue 1, Seishi Terada 1, Tadashi Matsumoto 2, Hiroshi Ujike 1 and Yosuke Uchitomi 1
Abstract
We report the case of a 48-year-old man with adult-onset adrenoleukodystrophy (ALD) who developed de-
mentia with subacute onset. He was abulic, indifferent to his surroundings, and without insight with regards
to his own disease. An elevated plasma very long chain fatty acid level and a novel point mutation IVS3+2t>
g in the ABCD1 gene confirmed the diagnosis of ALD. Diffusion-weighted MRI revealed a high intensity
area in the white matter of the frontal lobes. Severe brain hypoperfusion in the frontal lobes was revealed.
We believe that this is a rare case of adult-onset adrenoleukodystrophy with predominant frontal lobe dys-
function.
Key words: adrenoleukodystrophy, diffusion-weighted MRI, frontal lobe dysfunction, MR spectroscopy, sin-
gle photon emission CT (SPECT)
(Intern Med 51: 1403-1406, 2012)(DOI: 10.2169/internalmedicine.51.6899)
Introduction
X-linked adrenoleukodystrophy (X-ALD) is a rare inher-
ited metabolic disease caused by an enzyme deficiency lead-
ing to accumulation of saturated very long chain fatty acid
(VLCFA). Its prevalence is currently estimated at 1:17,000
males in the USA (1), 1:20,000 males in France (2), and 1:
30,000 to 50,000 males in Japan (3). The disease phenotype
varies widely. The most frequent phenotypes are the infan-
tile cerebral form, which often has a fatal course during the
first decade of life due to the extensive demyelination of the
cerebral hemispheres, and adult adrenomyeloneuropathy,
which leads to slowly evolving spastic paraparesis (2-5).
The less frequently described forms include those observed
in heterozygous women, pure Addisonian forms, and adoles-
cent ALD and adrenomyeloneuropathy (AMN) with some
signs of cerebral involvement (5). Adult cerebral disease (X-
ALD presenting with adult-onset dementia) is the least fre-
quently observed phenotype, occurring in 2-3% of cases in
Western countries (5, 6). In Japan, the adult cerebral form is
reported to be more common (21.4%) (3). Neuroradiological
studies of adult-onset ALD have only rarely been re-
ported (7-9). Adult-onset ALD is often characterized by
psychotic-like features, ataxia, spasticity and extensive white
matter demyelination as revealed by MRI. In this report, the
clinical, neuropsychological, and neuroimaging findings of a
patient with genetically and biochemically confirmed X-
ALD who developed dementia with subacute onset in the
fifth decade of life are presented.
Case Report
The patient is a 48-year-old man with a negative family
history of hereditary diseases, and with normal psychologi-
cal development and education. He has two siblings, was
married at the age of 29, and has three children. There were
no particular findings in his history.
In May 2004, he became slightly irritable. In June, he
was confused and got on the wrong trains several times and
also went to work on a holiday by mistake. His family
pointed out his mistake to him, but he showed no concern
1Department of Neuropsychiatry, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Japan and 2Depart-
ment of Nursing, Nagasaki University School of Medicine, Japan
Received for publication November 8, 2011; Accepted for publication February 8, 2012
Correspondence to Dr. Seishi Terada, [email protected]
Intern Med 51: 1403-1406, 2012 DOI: 10.2169/internalmedicine.51.6899
1404
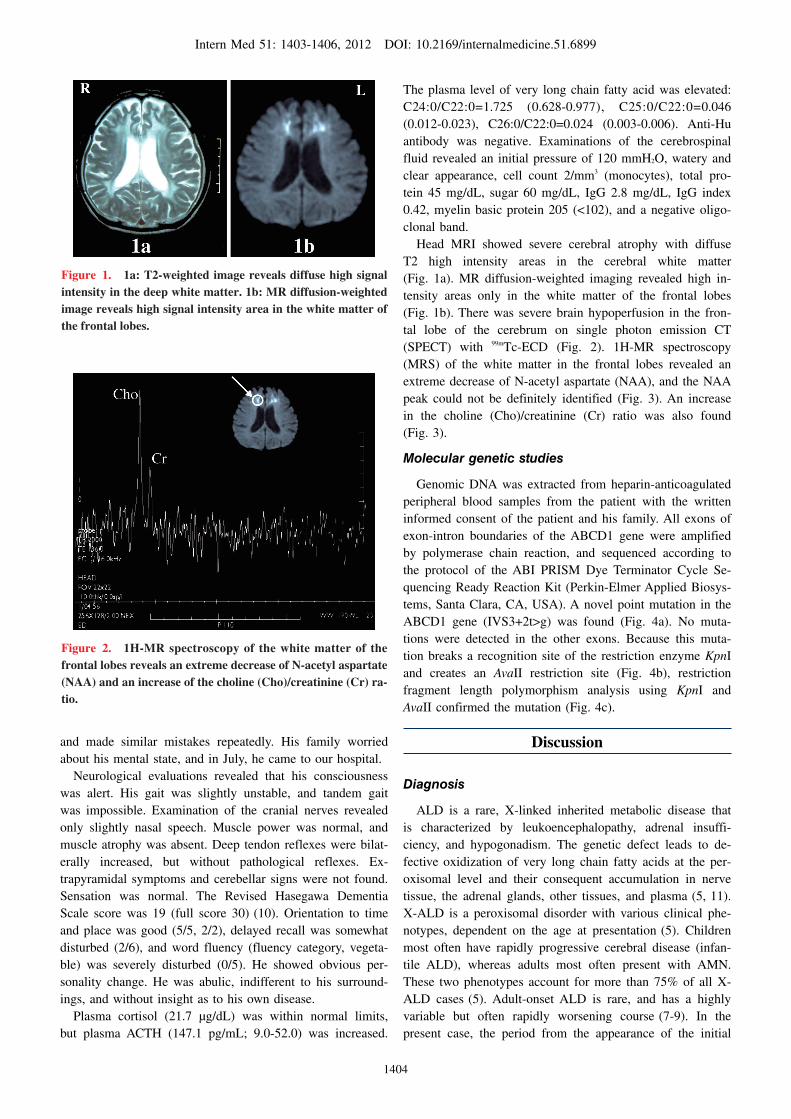
Figure 1. 1a: T2-weighted image reveals diffuse high signal intensity in the deep white matter. 1b: MR diffusion-weighted image reveals high signal intensity area in the white matter of the frontal lobes.
Figure 2. 1H-MR spectroscopy of the white matter of the frontal lobes reveals an extreme decrease of N-acetyl aspartate (NAA) and an increase of the choline (Cho)/creatinine (Cr) ra-tio.
and made similar mistakes repeatedly. His family worried
about his mental state, and in July, he came to our hospital.
Neurological evaluations revealed that his consciousness
was alert. His gait was slightly unstable, and tandem gait
was impossible. Examination of the cranial nerves revealed
only slightly nasal speech. Muscle power was normal, and
muscle atrophy was absent. Deep tendon reflexes were bilat-
erally increased, but without pathological reflexes. Ex-
trapyramidal symptoms and cerebellar signs were not found.
Sensation was normal. The Revised Hasegawa Dementia
Scale score was 19 (full score 30) (10). Orientation to time
and place was good (5/5, 2/2), delayed recall was somewhat
disturbed (2/6), and word fluency (fluency category, vegeta-
ble) was severely disturbed (0/5). He showed obvious per-
sonality change. He was abulic, indifferent to his surround-
ings, and without insight as to his own disease.
Plasma cortisol (21.7 μg/dL) was within normal limits,
but plasma ACTH (147.1 pg/mL; 9.0-52.0) was increased.
The plasma level of very long chain fatty acid was elevated:
C24:0/C22:0=1.725 (0.628-0.977), C25:0/C22:0=0.046
(0.012-0.023), C26:0/C22:0=0.024 (0.003-0.006). Anti-Hu
antibody was negative. Examinations of the cerebrospinal
fluid revealed an initial pressure of 120 mmH2O, watery and
clear appearance, cell count 2/mm3 (monocytes), total pro-
tein 45 mg/dL, sugar 60 mg/dL, IgG 2.8 mg/dL, IgG index
0.42, myelin basic protein 205 (<102), and a negative oligo-
clonal band.
Head MRI showed severe cerebral atrophy with diffuse
T2 high intensity areas in the cerebral white matter
(Fig. 1a). MR diffusion-weighted imaging revealed high in-
tensity areas only in the white matter of the frontal lobes
(Fig. 1b). There was severe brain hypoperfusion in the fron-
tal lobe of the cerebrum on single photon emission CT
(SPECT) with 99mTc-ECD (Fig. 2). 1H-MR spectroscopy
(MRS) of the white matter in the frontal lobes revealed an
extreme decrease of N-acetyl aspartate (NAA), and the NAA
peak could not be definitely identified (Fig. 3). An increase
in the choline (Cho)/creatinine (Cr) ratio was also found
(Fig. 3).
Molecular genetic studies
Genomic DNA was extracted from heparin-anticoagulated
peripheral blood samples from the patient with the written
informed consent of the patient and his family. All exons of
exon-intron boundaries of the ABCD1 gene were amplified
by polymerase chain reaction, and sequenced according to
the protocol of the ABI PRISM Dye Terminator Cycle Se-
quencing Ready Reaction Kit (Perkin-Elmer Applied Biosys-
tems, Santa Clara, CA, USA). A novel point mutation in the
ABCD1 gene (IVS3+2t>g) was found (Fig. 4a). No muta-
tions were detected in the other exons. Because this muta-
tion breaks a recognition site of the restriction enzyme KpnI
and creates an AvaII restriction site (Fig. 4b), restriction
fragment length polymorphism analysis using KpnI and
AvaII confirmed the mutation (Fig. 4c).
Discussion
Diagnosis
ALD is a rare, X-linked inherited metabolic disease that
is characterized by leukoencephalopathy, adrenal insuffi-
ciency, and hypogonadism. The genetic defect leads to de-
fective oxidization of very long chain fatty acids at the per-
oxisomal level and their consequent accumulation in nerve
tissue, the adrenal glands, other tissues, and plasma (5, 11).
X-ALD is a peroxisomal disorder with various clinical phe-
notypes, dependent on the age at presentation (5). Children
most often have rapidly progressive cerebral disease (infan-
tile ALD), whereas adults most often present with AMN.
These two phenotypes account for more than 75% of all X-
ALD cases (5). Adult-onset ALD is rare, and has a highly
variable but often rapidly worsening course (7-9). In the
present case, the period from the appearance of the initial

Intern Med 51: 1403-1406, 2012 DOI: 10.2169/internalmedicine.51.6899
1405
Figure 3. Single photon emission CT (SPECT) with 99mTc-ECD shows hypoperfusion in the frontal lobes.
Figure 4. 4a: Sequence analysis in the border zone of exon 3 and intron 3 in the ABCD1 gene. A novel point mutation in the ABCD1 gene (IVS3+2t>g; 1224+2t>g) was detected. 4b: This mutation breaks a recognition site of the restriction en-zyme KpnI and creates an AvaII restriction site. 4c: Restric-tion fragment length polymorphism analysis of intron 3 of the ABCD1 gene using KpnI and AvaII restriction enzymes. KpnI digestion produced two bands in the control, whereas no di-gestion was observed in the patient. AvaII digestion produced two bands in the control because the PCR product has a com-mon AvaII recognition site. A longer band after AvaII diges-tion was cleaved into two in the patient’s analysis, resulting in three bands.
symptom (irritability) to the first consultation was only
about two months, and the progression of symptoms was
rapid (12). The elevated plasma level of very long chain
fatty acids was confirmed, and diffuse leukoencephalopathy
was obvious. A novel point mutation in the ABCD1 gene
(IVS3+2t>g) was found. The mutation produces a donor
splice variant and incorporation of 23 novel amino acids af-
ter the end of exon 3 with an early termination. Therefore,
he was diagnosed with X-ALD presenting with adult-onset
dementia.
Clinical symptoms
Kitchin et al. reviewed 109 cases of ALD, most of them
with onset before the age of 21, and found that the present-
ing symptom was exclusively psychiatric in 17%, while psy-
chiatric symptoms appeared during the course of the disease
in 56% (13). Typical ALD with an onset at 21 years or
older presented with some psychiatric problems in four of
six cases (67%) and with only psychiatric problems in one
of six cases (17%) (13). The most common psychiatric
manifestation was dementia, followed by learning difficul-
ties, behavioral changes, and schizophrenia-like symp-
toms (5, 13, 14). Luda and Barisone reported that the over-
all neuropsychological picture of patients with adult-onset
ALD was subcortical dementia, but that the alterations in
symbolic functions indicate the involvement of some cortical
areas, especially the frontal cortex (15). We suppose that the
present case with abulia and indifference also suffered from
frontal lobe dysfunction.
Neuroradiological findings
Neuroradiological findings of sixty boys with infantile
cerebral form of ALD revealed that predominantly frontal
and mixed locations of cerebral disease were 13% (8/60)
and 5% (3/60), respectively (16). Kumar et al. found three
cases of adult cerebral ALD among 54 adult male ALD
cases (most cases were adrenomyeloneuropathy) (17). Those
three cases showed parieto-occipital dominant white matter
lesions without frontal lobe lesions (17). Two cases of adult
cerebral ALD with frontal dominant lesion were re-
ported (7, 8). Loes et al. examined 206 boys and men with
cerebral ALD (18) and found the frontal dominant type in
15.5% (32/206) and combined but separate involvement type
of frontal and parieto-occipital white matter in only 2.5%
(5/206). Diffuse global white matter involvement was ob-
served only in 2.5% (5/206) and it was thought to represent
a late stage of the disease (18). The present case showed
diffuse white matter lesions from frontal to occipital lobes
on T2-weighted images at the initial evaluation. The diffuse
white matter involvement observed at the initial evaluation
in our case is thought to be a relatively rare pattern.
Diffusion-weighted brain MR imaging of patients with
adult onset ALD has not been reported. Ito et al. examined
11 boys with ALD and described three patterns of white
matter lesions on T2-weighted and isotropic diffusion-
weighted images: one was both isotropic diffusion and T2
high, the second was isotropic diffusion high and T2 not
very high, and the last was isotropic diffusion not very high
and T2 high lesions (9). They stated that isotropic diffusion
not very high and T2 high lesions were rare (9). Both iso-
tropic diffusion and T2 high lesions were reported to be
found in core areas, and isotropic diffusion high and T2 not
very high lesions spread in peripheral areas (9). Core areas
correspond to the third zone of Shaumburg and without any

Intern Med 51: 1403-1406, 2012 DOI: 10.2169/internalmedicine.51.6899
1406
evidence of an active process (19), whereas peripheral areas
correspond to the first and second zones of Shaumburg and
with active processes (19). Ito et al. made use of diffuson
tensor MRI. Therefore, their classification could not be di-
rectly applied to the present case. In our case, the T2 high
white matter lesion was diffuse from frontal to occipital
lobes, and the diffusion high lesion was only found in the
frontal lobe.
It has been reported that on MRS in ALD, a decrease in
NAA reflects neuronal damage or loss and that an increase
in Cho corresponds to active demyelination and glial prolif-
eration (20, 21). In recent reports, an obvious decrease of
NAA and increase of Cho were also reported in the cerebral
white matter of patients with ALD (infantile cerebral
form) (20-22). In the present case, proton MRS revealed an
obvious decrease of NAA and increase of Cho in the white
matter of the frontal lobe. These results suggest that axons
as well as myelin sheaths are involved in the pathological
process in ALD (20-22).
Brain hypoperfusion in cases with ALD have been re-
ported, but the pattern of hypoperfusion varies. In a boy
with ALD, markedly reduced blood flow in the occipital,
parietal, and temporal cortical gray matter was reported (23),
whereas in another report, extremely decreased values of ap-
proximately 28 and 10 mL/100 g/min in bilateral frontal
cortex and white matter, respectively, were recorded (24). In
the present case, obvious frontal hypoperfusion was present
on SPECT. In both diffusion tensor MR imaging and
SPECT, severe damage in the frontal lobe was suggested,
and the clinical symptoms of abulia or indifference suggest
frontal lobe dysfunction. It is suggested that the severe dam-
age in the frontal lobe shown by diffusion-weighted MR im-
aging and SPECT caused the frontal symptoms in this case.
Conclusion
We reported a case of adult-onset adrenoleukodystrophy
with predominant frontal lobe dysfunction. Diffusion-
weighted MR imaging and SPECT were useful to detect le-
sions in ALD.
The authors state that they have no Conflict of Interest (COI).
References
1. Bezman L, Moser AB, Raymond GV, et al. Adrenoleukodystro-
phy: incidence, new mutation rate, and results of extended family
screening. Ann Neurol 49: 512-517, 2001.
2. Moser HW, Mahmood A, Raymond GV. X-linked adrenoleukodys-
trophy. Nat Clin Pract Neurol 3: 140-151, 2007.
3. Takemoto Y, Suzuki Y, Tamakoshi A, et al. Epidemiology of X-
linked adrenoleukodystrophy in Japan. J Hum Genet 47: 590-593,
2002.
4. Ferrer I, Aubourg P, Pujol A. General aspects and neuropathology
of X-linked adrenoleukodystrophy. Brain Pathol 20: 817-830,
2010.
5. Berger J, Gärtner J. X-linked adrenoleukodystrophy: clinical, bio-
chemical and pathogenetic aspects. Biochim Biophys Acta 1763:
1721-1732, 2006.
6. Moser HW. Adrenoleukodystrophy: phenotype, genetics, patho-
genesis and therapy. Brain 120: 1485-1508, 1997.
7. Larner AJ. Adult-onset dementia with prominent frontal lobe dys-
function in X-linked adrenoleukodystrophy with R152C mutation
in ABCD1 gene. J Neurol 250: 1253-1254, 2003.
8. Sutovský S, Petrovic R, Chandoga J, Turcáni P. Adult onset cere-
bral form of X-linked adrenoleukodystrophy with dementia of
frontal lobe type with new L160P mutation in ABCD1 gene. J
Neurol Sci 263: 149-153, 2007.
9. Ito R, Melhem ER, Mori S, Eichler FS, Raymond GV, Moser HW.
Diffusion tensor brain MR imaging in X-linked cerebral adreno-
leukodystrophy. Neurology 56: 544-547, 2001.
10. Hosokawa T, Yamada Y, Isagoda A, Nakamura R. Psychometric
equivalence of the Hasegawa Dementia Scale-Revised with the
Mini-Mental State Examination in stroke patients. Percept Mot
Skills 79: 664-666, 1994.
11. Kemp S, Wanders R. Biochemical aspects of X-linked adreno-
leukodystrophy. Brain Pathol 20: 831-837, 2010.
12. Suzuki Y, Takemoto Y, Shimozawa N, et al. Natural history of X-
linked adrenoleukodystrophy in Japan. Brain Dev 27: 353-357,
2005.
13. Kitchin W, Cohen-Cole SA, Mickel SF. Adrenoleukodystrophy:
frequency of presentation as a psychiatric disorder. Biol Psychiatry
22: 1375-1387, 1987.
14. Gothelf D, Levite R, Gadoth N. Bipolar affective disorder herald-
ing cerebral demyelination in adreno-myelo-leukodystrophy. Brain
Dev 22: 184-187, 2000.
15. Luda E, Barisone MG. Adult-onset adrenoleukodystrophy: a clini-
cal and neuropsychological study. Neurol Sci 22: 21-25, 2001.
16. Miller WP, Rothman SM, Nascene D, et al. Outcomes after allo-
geneic hematopoietic cell transplantation for childhood cerebral
adrenoleukodystrophy: the largest single-institution cohort report.
Blood 118: 1971-1978, 2011.
17. Kumar AJ, Kohler W, Kruse B, et al. MR findings in adult-onset
adrenoleukodystrophy. Am J Neuroradiol 16: 1227-1237, 1995.
18. Loes DJ, Fatemi A, Melhem ER, et al. Analysis of MRI patterns
aids prediction of progression in X-linked adrenoleukodystrophy.
Neurology 61: 369-374, 2003.
19. Schaumburg HH, Powers JM, Raine CS, Suzuki K, Richardson EP
Jr. Adrenoleukodystrophy. A clinical and pathological study of 17
cases. Arch Neurol 32: 577-591, 1975.
20. Sener RN. Atypical X-linked adrenoleukodystrophy: new MRI ob-
servations with FLAIR, magnetization transfer contrast, diffusion
MRI, and proton spectroscopy. Magn Reson Imaging 20: 215-219,
2002.
21. Oz G, Tkác I, Charnas LR, et al. Assessment of adrenoleukodys-
trophy lesions by high field MRS in non-sedated pediatric pa-
tients. Neurology 64: 434-441, 2005.
22. Eichler FS, Itoh R, Barker PB, et al. Proton MR spectroscopic and
diffusion tensor brain MR imaging in X-linked adrenoleukodystro-
phy: initial experience. Radiology 225: 245-252, 2002.
23. al Suhaili AR, Hertecant J, Sztriha L. Adrenoleukodystrophy: cor-
tical hypoperfusion demonstrated with 99mTc-HMPAO SPECT. J
Child Neurol 9: 284-286, 1994.
24. Matsuda H, Uesugi H, Kamata K, et al. Regional cerebral blood
flow measurement using Tc-99m HMPAO SPECT in a patient
with adrenoleukodystrophy. Clin Nucl Med 20: 52-54, 1995.
Ⓒ 2012 The Japanese Society of Internal Medicine
http://www.naika.or.jp/imindex.html





























