Embed Size (px)
Citation preview
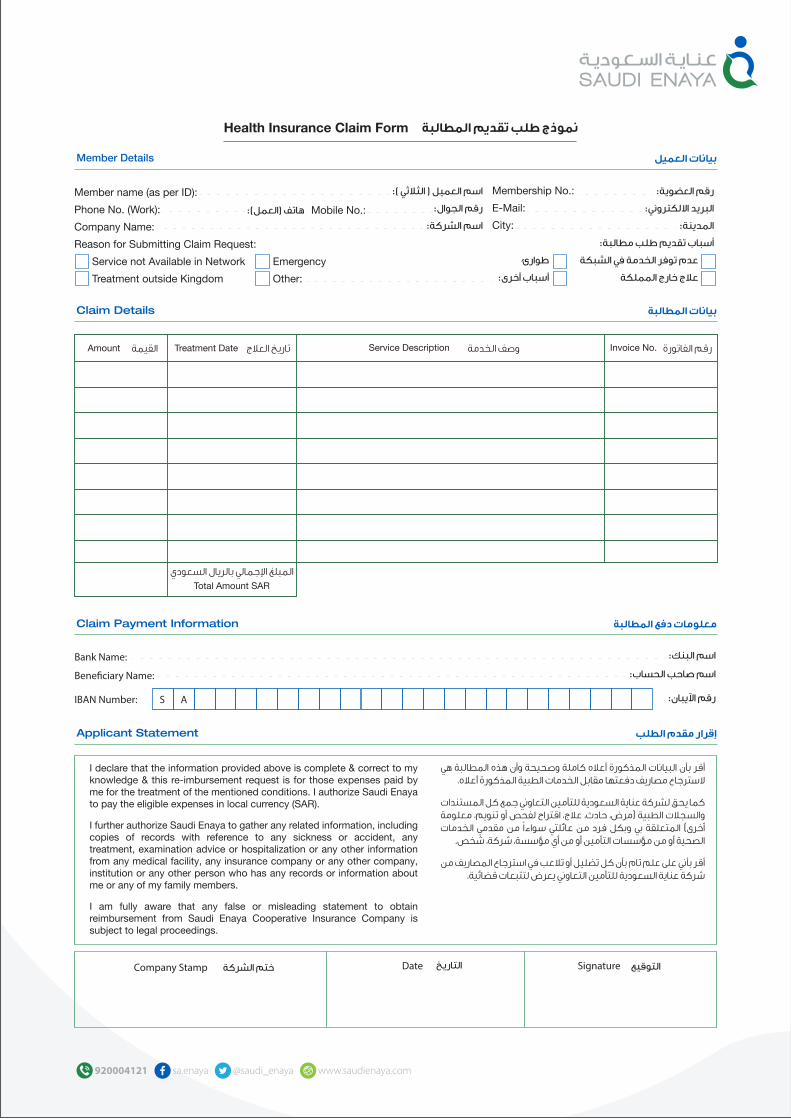
نموذج طلب تقديم المطالبة
بيانات العميل
ختم الشركةالتاريخ
Health Insurance Claim Form
Member name (as per ID):
Phone No. (Work):
Company Name:
Reason for Submitting Claim Request:
Service not Available in Network Emergency
Treatment outside Kingdom Other:
Member Details
Claim Detailsبيانات المطالبة
Claim Payment Informationمعلومات دفع المطالبة
Applicant Statementإقرار مقدم الطلب
I declare that the information provided above is complete & correct to my knowledge & this re-imbursement request is for those expenses paid by me for the treatment of the mentioned conditions. I authorize Saudi Enaya to pay the eligible expenses in local currency (SAR).
I further authorize Saudi Enaya to gather any related information, including copies of records with reference to any sickness or accident, any treatment, examination advice or hospitalization or any other information from any medical facility, any insurance company or any other company, institution or any other person who has any records or information about me or any of my family members.
I am fully aware that any false or misleading statement to obtain reimbursement from Saudi Enaya Cooperative Insurance Company is subject to legal proceedings.
Bank Name:
Bene�ciary Name:
IBAN Number:
DateCompany Stamp Signature
Membership No.:
E-Mail:
City:
Invoice No.Amount Service Description
اسم العميل ( الثالثي ):رقم الجوال:
اسم الشركة:
رقم العضوية:البريد االلكتروني:
المدينة:أسباب تقديم طلب مطالبة:
طوارئ عدم توفر الخدمة في الشبكة أسباب أخرى: عالج خارج المملكة
هاتف (العمل): Mobile No.:
القيمة Treatment Date تاريخ العالج
Total Amount SAR
المبلغ ا�جمالي بالريال السعودي
وصف الخدمة رقم الفاتورة
اسم البنك:
اسم صاحب الحساب:
رقم ا�يبان:
التوقيع
المطالبة هي المذكورة أعاله كاملة وصحيحة وأن هذه البيانات بأن أقر السترجاع مصاريف دفعتها مقابل الخدمات الطبية المذكورة أعاله.
كما يحق لشركة عناية السعودية للتأمين التعاوني جمع كل المستندات والسجالت الطبية (مرض، حادث، عالج، اقتراح لفحص أو تنويم، معلومة الخدمات مقدمي من سواءا عائلتي من فرد وبكل بي المتعلقة أخرى)
الصحية أو من مؤسسات التأمين أو من أي مؤسسة، شركة، شخص.
أقر بأني على علم تام بأن كل تضليل أو تالعب في استرجاع المصاريف من شركة عناية السعودية للتأمين التعاوني يعرض لتتبعات قضائية.
S A
General Instructions
Kindly use a separate form for each Saudi Enaya Member as well as separate forms for each new Provider. A new form can be downloaded from www.saudienaya.com or may be obtained from any Saudi Enaya branch.
Please read the form carefully and make sure that the form is filled out completely. Saudi Enaya will not be able to process any Reimbursement Claim Forms which are incomplete & lack proper supporting documents.
Supporting Documents Required:1. ID / Iqama (mandatory).
2. Saudi Enaya Insurance Card.
3. Claim Form filled out completely signed by member and stamped by policy holder. “Original”.
4. Itemized payment invoices and receipts. “Original”.
5. Medical prescription from the treating doctor. “Signed by doctor”.
6. Investigation results/reports. For example: laboratory and imaging.
7. Medical Report mentioning the complaint, diagnosis, and treatment.
8. For Dental Services: Please specify the tooth Number.
9. For Inpatient and Day-Case Services: Prior approval / Authorization Letter from Saudi Enaya, together with discharge Summary stamped and signed by the treating Doctor.
Note: Please retain copies of receipts and documents enclosed with your claim, as Saudi Enaya will not return the original documents.
For any pending claims, missing documentation must be received within your submission period, with a Grace Period of 10 Days; otherwise the claim will be automatically rejected.
All reimbursement claims should be submitted to Saudi Enaya from the last treatment date as mentioned below:
• Services availed within Saudi Arabia: 30 Days.
• Services availed outside Saudi Arabia: 60 Days.
The Claim documents are to be submitted as follows:
At company premises:
Jeddah: Saudi Enaya Cooperative Insurance Company
Mohammed Bin Abdulaziz Road (Tahliya Road)
Ahmed Ghalib Al Esayi Building, 1st floor
Jeddah, Saudi Arabia
Riyadh: Rabi Plaza, Thumamah Road, Ar Rabi District, Riyadh
Or via Mail at:Saudi Enaya Claims Department
P.O Box: 3528Jeddah 21481
Saudi Arabia.
Once you have completed your claim submission, it will be processed by Saudi Enaya. Processing time is 14 working days from date of receipt. Your claim will first be evaluated & the amount will then be reimbursed to you accordingly as per your Table of Benefits.
You will be notified with an SMS once your claim has been processed.
If you have any query or need assistance in filling this form, Please call:
Inside kingdom: 800 30 100 30
Outside Kingdom:+966 920 004 122
Or via email: [email protected]
توجيهات عامة
يرجى استعمال نموذج مطالبة منفصل لكل مؤمن وكذلك بالنسبة لكل مقدم خدمة صحية كما يمكن تحميل نموذج مطالبة استرجاع المصاريف الطبية من لشركة فرع أي من إقتناءه أو www.saudienaya.com ا�لكتروني الموقع
عناية السعودية للتأمين التعاوني.
يرجى قراءة النموذج بشكل دقيق مع ا�دالء بجميع المعلومات المطلوبة فيها. غير مطالبة وسداد دراسة التعاوني للتأمين السعودية عناية لشركة يمكن ال
موثقة وغير كاملة وشاملة.
الوثائق المؤيدة للمطالبة:١ - نسخة من بطاقة الهوية أو رخصة ا�قامة (إلزامي).
٢ - نسخة من بطاقة التأمين.ع من العميل ومختوم من حامل الوثيقة ٣ - نموذج المطالبة معبأ بالكامل، موق
( ا«صل).٤- أصل الفواتير وإيصاالت الدفع المفصلة.
٥ - نسخة من الوصفة الطبية موقعة من الطبيب المعالج.٦ - نسخة من تقارير ونتائج الفحوصات، مثل التحاليل وا«شعات.
٧ - نسخة من التقرير الطبي موضحا ا«عراض والتشخيص والعالج.٨ - ولخدمات ا«سنان يرجى تحديد رقم السن أو الضرس موضع العالج.
٩ - ولخدمات التنويم ومعالجات اليوم الواحد، يجب الحصول على موافقة مسبقة من ومختوما موقعا الخروج ملخص إرفاق ويرجى السعودية، عناية شركة من
الطبيب المعالج.
االحتفاظ يرجى لذا ا«صلية، الوثائق تعيد ال السعودية عناية شركة إن مالحظة: بنسخ عن ا�يصاالت وجميع الوثائق المرفقة مع الطلب.
الوثائق تسليم فينبغي مكتملة، الغير أو المعلقة المطالبات وبخصوص المطلوبة خالل فترة التقديم الخاصة بك، مع فترة سماح مدتها ١٠ أيام وإال سيتم
رفض المطالبة تلقائيا.
يجب تقديم المطالبات لشركة عناية السعودية خالل:داخل بها المنتفع للخدمات بالنسبة عالج يوم آخر تاريخ من يوم ٣٠ خالل •
المملكة.خارج بها المنتفع للخدمات بالنسبة عالج يوم آخر تاريخ من يوم ٦٠ خالل •
المملكة.
يتم تقديم المطالبات كما يلي:
في مقر الشركة على العنوان التالي:جدة: شركة عناية السعودية للتأمين التعاوني
شارع ا«مير محمد بن عبد العزيز ( شارع التحلية)مبنى أحمد غالب العيسائي - الدور ا«ول
المملكة العربية السعودية - جدةالرياض: مجمع الربيع، طريق الثمامة، حي الربيع، الرياض
أو عبر البريد التالي:عناية السعودية قسم المطالبات
ص.ب ٣٥٢٨ جدة ٢١٤٨١المملكة العربية السعودية
كامال الطلب تقديم تاريخ من عمل يوم ١٤ خالل الطلب وتنفيذ دراسة سيتم حسب جدول المنافع.
حين االنتهاء من تنفيذ الطلب سوف يتم إرسال رسالة نصية على هاتفك الجوال.
�ي مساعدة أو استفسار، يرجى االتصال على ا�رقام التالية:
من داخل المملكة: ٨٠٠٣٠١٠٠٣٠
من خارج المملكة:٩٦٦٩٢٠٠٠٤١٢٢+
[email protected] :أو عبر البريد ا�لكتروني




![EMPLOYEES’ PROVIDENT FUND ORGANISATION M obile Number Composite Claim ... - HR … · 2019. 3. 23. · Insurance [EDLI] ( ) 2 र्֦तक सदस्य का िार्](https://img.pdfslide.tips/doc/110x75/608fa77127d9820c4b6d351f/employeesa-provident-fund-organisation-m-obile-number-composite-claim-hr.jpg)










![Services agreement—one–off supply—pro-customer · Web viewpublic liability insurance for not less than £[insert amount] in respect of each claim; ... absolutely with full title](https://img.pdfslide.tips/doc/110x75/5e3f7be19611b550da57fb16/services-agreementaoneaoff-supplyapro-customer-web-view-public-liability-insurance.jpg)













