Embed Size (px)
Citation preview

ATCEWL
O
M
R
C
Ittstocacrw
FvPaS
vE
©A
Basic and Translational Science
doptive Transfer of Tumor-Reactiveransforming Growth Factor-�–Insensitiveytolytic T Cells for Treatment ofstablished Mouse Renca Tumorseijun Qin, Feng Tian, Fuli Wang, Bin Song, He Wang, Qiang Zhang, Borko Jovanovic,
ili Liang, Yinglu Guo, Norm Smith, and Chung Lee
BJECTIVES To test, using a mouse renal cancer, Renca, whether adoptive transfer of tumor-reactivetransforming growth factor (TGF)-�–insensitive cytolytic T cells can inhibit tumor progression.
ETHODS Cytolytic T cells were isolated from the spleen of male Balb/c mice repeatedly primed withirradiated Renca cells. They were expanded ex vivo and were rendered TGF-�–insensitive byinfecting with a retrovirus containing dominant negative TGF-� type II receptor.
ESULTS These tumor reactive TGF-�–insensitive cytolytic T cells showed a specific and robust tumorkilling activity against Renca cells, but not irrelevant cells, using an in vitro cytotoxic assay.Adoptive transfer of cytolytic T cells was performed in mice 10 days after they were challengedwith Renca cells (5 � 105) by tail vein injection. At 30 days after the adoptive transfer,the pulmonary tumor counts in mice who had received TGF-�–insensitive cytolytic T cells(mean � standard deviation 130 � 140) was significantly less than those in mice that hadreceived TGF-�–sensitive cytolytic T cells (305 � 60) or in mice had received naive cytolyticT cells (375 � 50; P � .01). Kaplan-Meier survival analysis indicated that mice that hadreceived adoptive transfer of TGF-�–insensitive cytolytic T cells had a significantly greater rateof survival (75%) compared with mice that had received TGF-�–sensitive cytolytic T cells(35%) or naive cytolytic T cells (15%), respectively (P � .05).
ONCLUSIONS These results suggest that adoptive transfer of tumor-reactive TGF-�–insensitive cytolytic T cellscan warrant consideration for renal cell cancer immunotherapy. UROLOGY 72: 943–947, 2008.
© 2008 Elsevier Inc.5tsag
isncicefosttIa
n the United States alone, 50 000 people are diag-nosed with renal cell carcinoma (RCC) and �12 000die annually.1 Although the medical field is able to
reat early-stage localized RCC, metastatic cases remaino be a major medical challenge. RCC that has metasta-ized is invariably fatal and does not respond to conven-ional radiotherapy or chemotherapeutic drugs. Becauseccasional spontaneous remissions of advanced renalancer occur, it has been suggested that immune mech-nisms might have played a role in the natural diseaseourse of RCC.2 Currently, several nonspecific cytokineegimens are used in the treatment of metastatic RCCith an overall response rate of approximately 15%, with
rom the Department of Urology, Xijing Hospital, the Fourth Military Medical Uni-ersity, Xi’an, Shanxi Province, China; the Department of Urology, the First Hospital,eking University, Beijing, China; Departments of Urology and Preventive Medicine,nd Robert H. Lurie Comprehensive Cancer Center, Northwestern University Feinbergchool of Medicine, Chicago, Illinois
Reprint requests: Chung Lee, Ph.D., Department of Urology, Northwestern Uni-ersity Medical School, 303 East Chicago Avenue, Tarry 11, Chicago, IL 60611.
w-mail: [email protected]: January 14, 2008, accepted (with revisions): April 9, 2008
2008 Elsevier Inc.ll Rights Reserved
% of patients showing complete responses.3 However,he toxicity profile of these cytokine regimens remains aignificant concern.4 The development of an effectivend safe immunotherapeutic strategy is, therefore, ur-ently needed.
Transforming growth factor (TGF)-� represents a fam-ly of pleiotropic growth factors with diverse functions,uch as embryonic development, wound healing, immu-omodulation, and cancer progression.5 Cancer cells areharacterized by an increased production of TGF-�,6
ncluding RCC.7 An elevated TGF-� level in cancerells will facilitate tumor invasion, metastasis, angiogen-sis, and evasion of host immune surveillance.8 There-ore, the use of TGF-�–insensitive immune cells mightffer a potential tool for cancer therapy. In previoustudies, we have successfully used the adoptive transfer ofumor reactive, TGF-�–insensitive cytolytic T cells forhe treatment of mouse prostate cancer (TRAMP-C2).9
t remains unclear whether the same approach can bepplied to a different tumor system. In the present study,
e used a mouse renal cancer, Renca, as an experimental0090-4295/08/$34.00 943doi:10.1016/j.urology.2008.04.017

mtct
M
RTs1i�
GGcIwacktgRba
GCRTsericcvTc
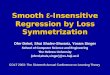
FoMctTcv enase used as reference for leading control.
FcaaTcfi�cs
9
odel, and we reported the successful use of the adoptiveransfer of tumor reactive TGF-�–insensitive cytolytic Tells into recipient mice for the treatment of Rencaumors.
ATERIAL AND METHODS
enca Cellshe Renca cells were provided by T. Ratliff of Purdue Univer-
ity and were maintained in Roswell Park Memorial Institute-640 (Gibco, Grand Island, NY) supplemented with 10% heat-nactivated fetal bovine serum, 100 U/mL penicillin, and 100g/mL streptomycin.
eneration of Tumor Reactive Cytolytic T Cellseneration of tumor-reactive TGF-�–insensitive cytolytic T
ells was performed according to a previously described method.9
n brief, male Balb/c mice (6 weeks old) were vaccinated 3 timesith irradiated Renca cells (5 � 106/mice at 50 Gy) at 10 dayspart. Two weeks after the last boosting, splenic cytolytic Tells were isolated by using murine T cell CD8 subset columnit (R&D Systems, Minneapolis, MN) and were expanded inhe presence of Renca lysates (1 � 106) and irradiated autolo-ous splenocytes (1 � 106/mL, 50 Gy) in medium containingoswell Park Memorial Institute-1640 medium with 10% fetalovine serum, interleukin-2 (50 U/mL), anti-CD3 monoclonalntibody (30 ng/mL, R&D Systems).
eneration of Tumor Reactive TGF-�–Insensitiveytolytic T Cells With Murine Stem Celletroviral Vectorumor-reactive cytolytic T cells were infected with the murine
tem cell retroviral vector (MSCV) retrovirus containing thexpression vectors of the dominant negative TGF-� type IIeceptor (T�RIIDN) and the green fluorescent protein (GFP)n bicistronic sites.9 In this manner, we generated 3 types ofytolytic T cells. The first type was tumor-reactive cytolytic Tells infected with the virus containing the T�RIIDN-GFPector and was designated as the T�RIIDN cytolytic T cells.hese cells are tumor reactive, TGF-�–insensitive cytolytic T
igure 1. Characterization of tumor-reactive TGF-�–insensitf murine tumor reactive cytolytic T cells transfected with (1 is GFP-negative population. M2 is GFP-positive populati
ells allowed the performance of adoptive transfer directlyypes of cytolytic T cells probing for total Smad2 (T-Samd2GF-�, p-Smad2 was observed in naive cytolytic T cells (naontrol vector (GFP lane) but not in tumor-reactive cytolyticector (T�RIIDN lane). Glyceraldehyde phosphate dehydrog
ive cytolytic T cells. Fluorescence-activated cell sorter analysisA) T�RIIDN vector (87.4%) and (B) GFP control vector (89.5%).on. High efficiency of infection of viral transgene into cytolytic Twithout need for sorting. (C) Western blot analysis of different) and phosphorylated Smad2 (p-Smad2). After treatment withive lane) and tumor-reactive cytolytic T cells infected with GFPT cells infected with dominant negative TGF-� type II receptor
ells. The second type was tumor-reactive cytolytic T cells b
44
A. Renca cells CTL assay
B. EMT-2 cells CTL assay
igure 2. Chromium-51 release assay performed usingonventional CTL assay of cytolytic T cells. In vitro CTLssay performed using conventional chromium-51 releasessay (see “Material and Methods” section). Naive cytolyticcells, GFP, and T�RIIDN-transfected cytolytic T cells were
o-cultured with chromium-51-labeled targets at the speci-ed Effector cell: Target cell (E:T) ratios. (A) Renca cells (5
104) used as targets. (B) Irrelevant mice breast cancerells, EMT-6, used as negative control. Each point repre-ents average observations obtained from 8 wells. Vertical
ars denote standard deviation.UROLOGY 72 (4), 2008

idrns
ITTtac
ITFrb(eubttw
SFatdeft
R
IMTTM8(TdT
ITTiCcalc
ITiWvsahFlttmTmTairwphtsre
CTsrbmai�pshmitataf
iTatasdi
U
nfected with the virus containing the GFP control vector andesignated as GFP cytolytic T cells. These cells are tumoreactive, TGF-�–sensitive cytolytic T cells. The third type wasaive cytolytic T cells, which were freshly isolated from thepleen of untreated naive donor mice.
n Vitro Specificity of Tumor-Reactive CytolyticCells—Cytotoxic T Lymphocyte Assay
he specificity of these 3 types of cytolytic T cells was inves-igated using the conventional cytotoxic T lymphocyte (CTL)ssay against Renca cells. An irrelevant mouse breast cancerell line, EMT-6, was used as a negative control.
n Vivo Antitumor Activity of Tumor-ReactiveGF-�–Insensitive Cytolytic T Cellsor the in vivo antitumor test, male Balb/c mice (6-8 weeks old)eceived a single injection of 5 � 105 Renca cells intravenouslyy way of the tail vein. Adoptive transfer of cytolytic T cells2 � 106) was performed 10 days after tumor cell injection. Thexperiment was terminated 30 days after the adoptive transfer,sing 20 mice in each treatment group. The status of the tumorurden in each mouse was evaluated by counting the number ofumor nodules in an hematoxylin-eosin–stained histologic sec-ion from the middle of each lung and by measuring the totaleight of the lung.
tatistical Analysisisher’s exact test and the log-rank test were used for differencesmong surviving record and Kaplan-Meier survival cure, respec-ively. Numeric data are expressed as the mean � standardeviation. Because of the large variation in tumor counts withinach treatment group, logarithmic transformation was per-ormed, followed by analysis of variance and the multiple rangeest. Differences were considered significant, if P � .05.
ESULTS
nfection of Tumor-Reactive Cytolytic T Cells withSCV Retrovirus Containing T�RIIDN and Test of
GF-� Sensitivityhe infection rate of cytolytic T cells was 87% for theSCV retrovirus containing the T�RIIDN vector and
9% for the virus containing the GFP control vectorFig. 1A,B). The reduced TGF-� sensitivity of the�RIIDN cytolytic T cells was confirmed by the lack ofetection of Smad2 phosphorylation after treatment withGF-�1 (10 ng/mL, Fig. 1C).
n Vitro CTL Test for Specificity of Tumor ReactiveGF-�–Insensitive Cytolytic T Cellshe specificity of cytolytic T cell against Renca cells was
nvestigated using the conventional chromium-51 releaseTL assay (Fig. 2). Tumor-reactive TGF-�–insensitive
ytolytic T cells showed a specific in vitro CTL activitygainst Renca cells (Fig. 2A). As expected, they hadittle specificity against the irrelevant mice breast cancer
ells, EMT-6 (Fig. 2B). fROLOGY 72 (4), 2008
n Vivo Antitumor Test of Adoptive Transfer ofumor-Reactive TGF-�–Insensitive Cytolytic T Cellsn Tumor-Bearing Mice
hen the Renca cells were injected into the mice intra-enously, they metastasized to the lung.10 In the presenttudy, because adoptive transfer was initiated 10 daysfter the injection of the tumor cells, the Renca tumorsad established in the lung before the adoptive transfer.igure 3A shows representative histologic sections of theung tissue at the conclusion of the experiment. Theumor burden was determined by counting the number ofumor foci in the middle section of the lung from eachouse (Fig. 3B). Again, the mice that had received�RIIDN cytolytic T cells had a significantly lower tu-or count than those of the other 2 groups (P � .01).he results of the tumor count were supported by theverage weight of the lung, which was used as anotherndication of the relative tumor burden (Fig. 3C). Ourecords indicated that all mice with the lung tissueeighing �1.30 g died before the 30-day observationeriod because of the heavy tumor burden. The mice thatad received T�RIIDN cytolytic T cells had the lowestumor burden, which was supported by the Kaplan-Meierurvival curve (Fig. 3D), and 75% of the mice that hadeceived T�RIIDN cytolytic T cells were living at thend of the experimental period.
OMMENThe results of the present study have demonstrated a
uccessful antitumor effect by adoptive transfer of tumoreactive TGF-�–insensitive cytolytic T cells in miceearing Renca tumors. Renca cells are different from theouse prostate cancer cell line, TRAMP-C2, in that they
re insensitive to TGF-�.11 The present results havendicated that adoptive transfer of tumor-reactive TGF-–insensitive cytolytic T cells is able to control therogression of both TGF-�–sensitive and TGF-�–insen-itive tumors. These results are encouraging because theyave not only confirmed our previous studies with theouse prostate cancer model,9 but they have also exhib-
ted a remarkable similarity in the antitumor efficacy ofhese tumor-reactive TGF-�–insensitive cytolytic T cellsgainst 2 completely different tumor systems. Together,hese combined findings allow us to speculate that suchn immunotherapy approach might be applicable to dif-erent tumor types.
A significant part of tumor immunology has been thedentification of tumor-specific antigens and the cytolytic-cells specific for these peptides.12 Adoptive T-cell ther-py using antigen-specific cytolytic T cells for cancerreatment has been attempted with encouraging results13
nd seems to be an advantage over the transfer of non-pecific T cells.14 The results of the present study haveemonstrated that, by superimposing TGF-� insensitivitynto tumor-reactive cytolytic T cells in an adoptive trans-
er platform, the antitumor efficacy was further enhanced945

9
A. Representative H&E staining of histological sections of the lung
B. Average number of tumor nodules in the middle section of the lung
C. Average weight of the lung (g)
D. Kaplan-Meier survival curve
0 10 20 30 400
10
20
30
40
50
60
70
80
90
100
days
% s
urvi
val
TBRIIDNGFPNaive
adoptive transfer
46 UROLOGY 72 (4), 2008

ae
tmsqdtidecmsa
CTtciTtt
R
1
1
1
1
1
1
4Fsr�ltivtl P �
U
nd was able to specifically inhibit the progression ofstablished tumors.
The critical issue in immunotherapy thus far has beenhe tumor-derived immunosuppressive effect, which re-ains unresolved. TGF-� is a potent immunosuppres-
ant.6 Immune cells, including cytolytic T cells, are ex-uisitely sensitive to the inhibitory effect of tumor-erived TGF-�.15 By introducing the dominant negativeype II TGF-� receptor into cytolytic T cells, thesemmune cells were given a reduced sensitivity to tumor-erived TGF-� and were able to elicit a robust antitumorfficacy. The present study has provided a proof of prin-iple to suggest that in this experimental renal cancerodel adoptive transfer of tumor-reactive TGF-�–insen-
itive cytolytic T cells is able to inhibit tumor progressionnd prolong the survival of recipient mice.
ONCLUSIONShe results of the present study have demonstrated that
he growth stimulatory effect of TGF-� on Renca tumorells can be mediated through host factors, which, at leastn part, involve TGF-� inhibition of cytolytic T cells.hese results suggest that immunotherapy using adoptive
ransfer of immune cells is a promising approach for thereatment of different tumor types.
eferences1. Jemal A, Siegel R, Ward E, et al. Cancer statistics. CA Cancer
J Clin. 2007;57:43-66.2. Gleave ME, Elhilali M, Fradet Y, et al., for the Canadian Urologic
™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™igure 3. Tumor burden in 3 treatment groups. (A) Repections of lung tissue from mice that had received adoptiveactive cytolytic T cells (B,E), and T�RIIDN-transfected tum100 for D-F. (B) Average number of tumor sites in mid-sec
ess in T�RIIDN group than those in other 2 groups (Pransformation of original data). (C) Average weight of lungndication of tumor burden and was significantly smaller inariance). Vertical bars denote standard deviation. Eachumor-bearing mice that had received adoptive transfer of naine), and T�RIIDN-transfected cytolytic T cells (black line).
Oncology Group. Interferon gamma-1b compared with placebo in
ROLOGY 72 (4), 2008
metastatic renal-cell carcinoma. N Engl J Med. 1998;338:1265-1271.
3. Gitlitz BJ, Figlin RA. Cytokine-based therapy for metastatic renalcell cancer. Urol Clin North Am. 2003;30:589-600.
4. Bleumer I, Oosterwijk E, De Mulder P, et al. Immunotherapy forrenal cell carcinoma. Eur Urol. 2003;44:65-75.
5. Derynck R, Akhurst RJ, Balmain A. TGF-� signaling in tumorsuppression and cancer progression. Nat Genet. 2001;29:117-129.
6. Pinkas J, Teicher BA. TGF-� in cancer and as a therapeutic target.Biochem Pharmacol. 2006:l72:523-529.
7. Gomella LG, Sargent ER, Wade TP, et al. Expression of transform-ing growth factor � in normal adult kidney and enhanced expres-sion of transforming growth factors � and �1 in renal cell carci-noma. Cancer Res. 1989;49:6972-6975.
8. Wakefield LM, Roberts AB. TGF-� signaling: Positive and nega-tive effects on tumorigenesis. Curr Opin Genet Dev. 2002;12:22-29.
9. Zhang Q, Yang X, Pins M, et al. Adoptive transfer of tumor reactiveTGF-� insensitive CD8� T cells: Eradication of autologous mouseprostate cancer. Cancer Res. 2005;65:1761-1769.
0. Liu VC, Wong LW, Jang T, et al. Tumor evasion of the immunesystem by converting CD4�CD25� T cells into CD4�CD25� Tregulatory cells: Role of tumor-derived TGF-�. J Immunol. 2007;178:2883-2892.
1. Zhang Q, Rubenstein JN, Liu VC, et al. Restoration of expressionof transforming growth factor-� type II receptor in murine renalcell carcinoma (Renca) cells by 5-aza-2=-deoxycytidine. Life Sci.2005;76:1159-1166.
2. van den Eynde BJ, van der Bruggen P. T cell defined tumorantigens. Curr Opin Immunol. 1997;9:684-693.
3. Morgan RA, Dudley ME, Wunderlich JR, et al. Cancer regressionin patients after transfer of genetically engineered lymphocytes.Science. 2006;314:126-129.
4. Zeh HJ III, Perry-Lalley D, Dudley ME, et al. High avidity CTLs fortwo self-antigen demonstrate superior in vitro and in vivo antitu-mor efficacy. J Immunol. 1999;162:989-994.
5. Wojtowicz-Praga S. Reversal of tumor-induced immunosuppresion
™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™ntative histologic features of hematoxylin-eosin–stainednsfer of naive cytolytic T cells (A,D), GFP-transfected tumoractive cytolytic T cells (C,F). Magnification: �40 for A-C andof lung from each mouse. Tumor counts were significantly.01 according to analysis of variance after logarithmicues of 3 groups of mice. Lung weight used as additionalIIDN groups than in other 2 groups (P � .01, analysis of
p contained 20 mice. (D) Kaplan-Meier survival curve ofytolytic T cells (light gray line), GFP control vector (dark gray.05 according to log-rank test among all groups.
™™™resee traor-retion�tissT�R
grouive c
by TGF-� inhibitors. Invest New Drugs. 2003;21:21-32.
947