Embed Size (px)
DESCRIPTION
Adrenergic Agonists (Sympathomimetics). Characteristics of Adrenergic Agonists. Most of adrenergic agonists are β -phenylethylamine derivatives. Substitution on either the benzene ring or on the ethylamine side chain give a great variety of compounds which can be divided into: Catecholamines - PowerPoint PPT Presentation
Citation preview
Adrenergic Agonists(Sympathomimetics)
Characteristics of Adrenergic Agonists
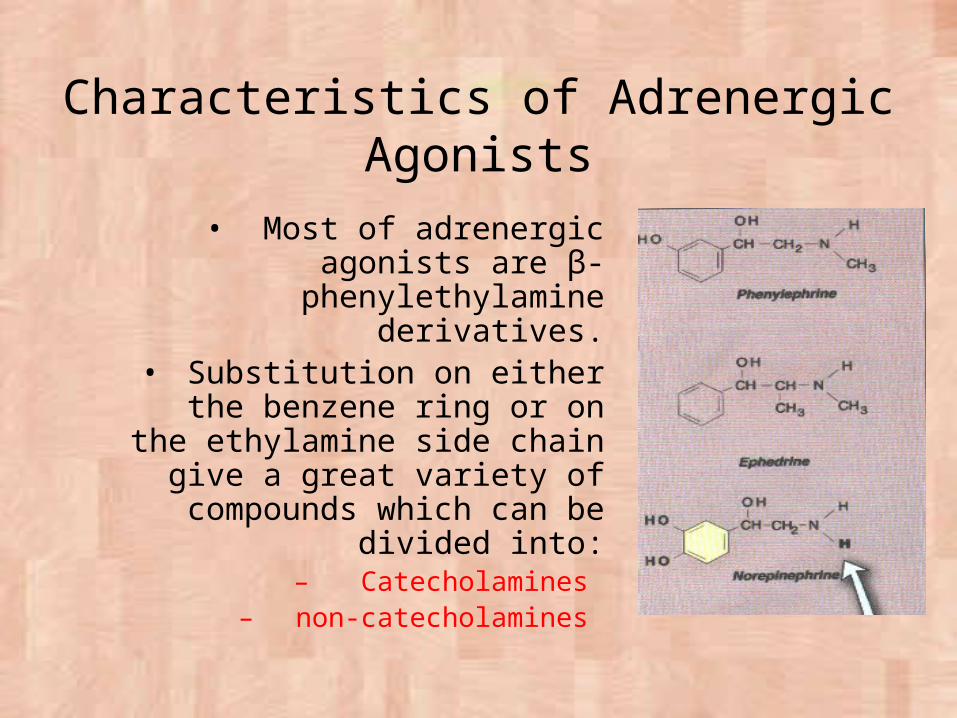
• Most of adrenergic agonists are β-phenylethylamine
derivatives.• Substitution on either the
benzene ring or on the ethylamine side chain give a great variety of compounds
which can be divided into:– Catecholamines
– non-catecholamines
Catecholamines
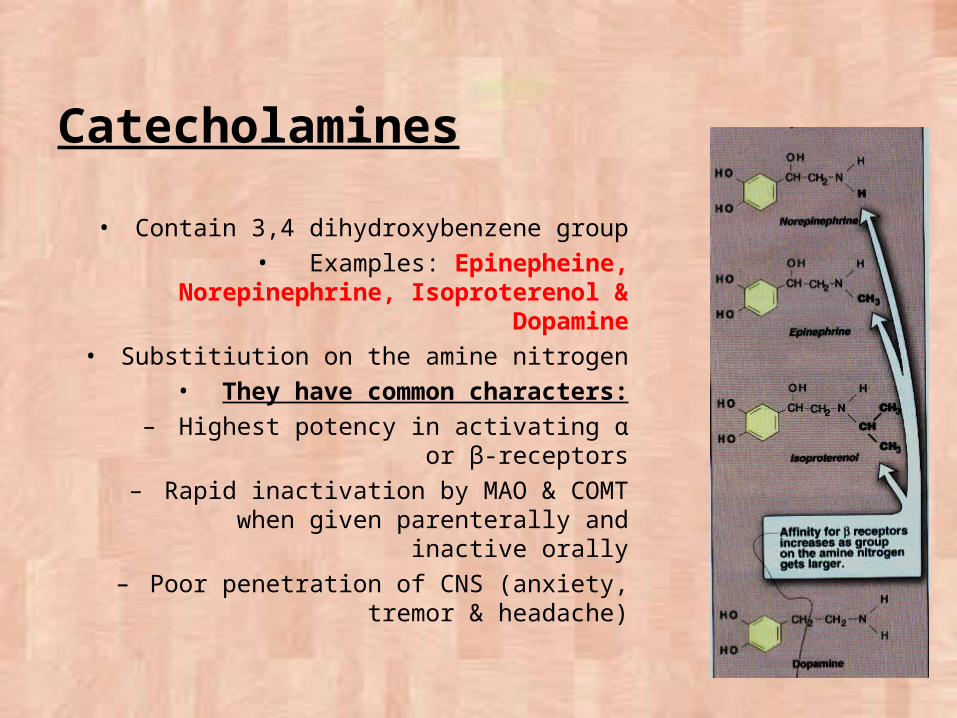
• Contain 3,4 dihydroxybenzene group• Examples: Epinepheine, Norepinephrine,
Isoproterenol & Dopamine• Substitiution on the amine nitrogen• They have common characters:
– Highest potency in activating α or β-receptors
– Rapid inactivation by MAO & COMT when given parenterally and inactive
orally– Poor penetration of CNS (anxiety,
tremor & headache)
Noncatecholamines
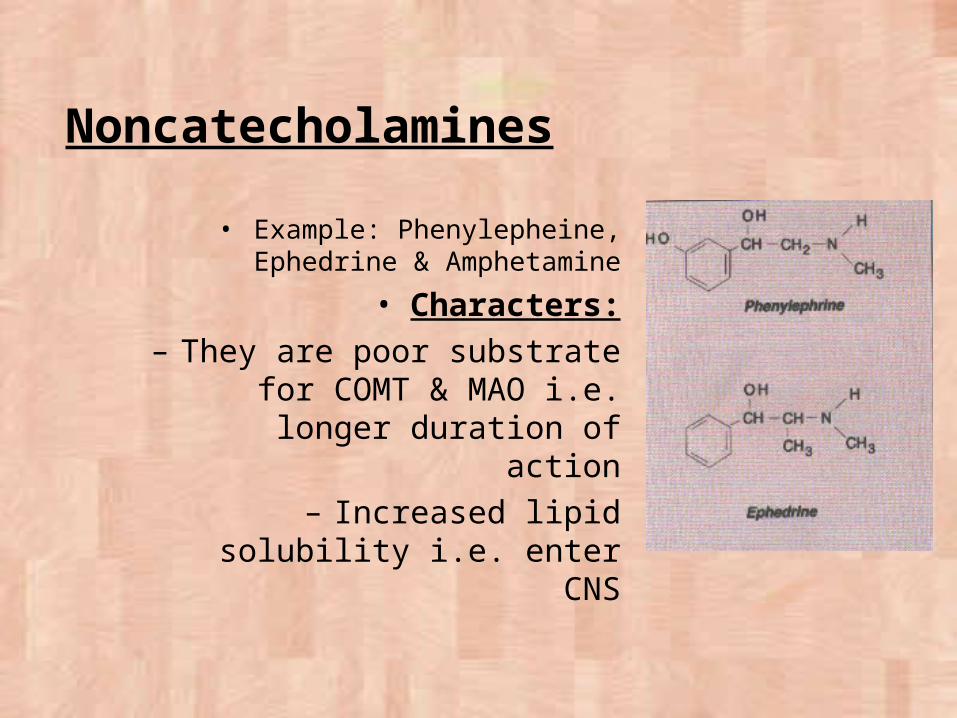
• Example: Phenylepheine, Ephedrine & Amphetamine
• Characters:– They are poor substrate for
COMT & MAO i.e. longer duration of action
– Increased lipid solubility i.e. enter CNS
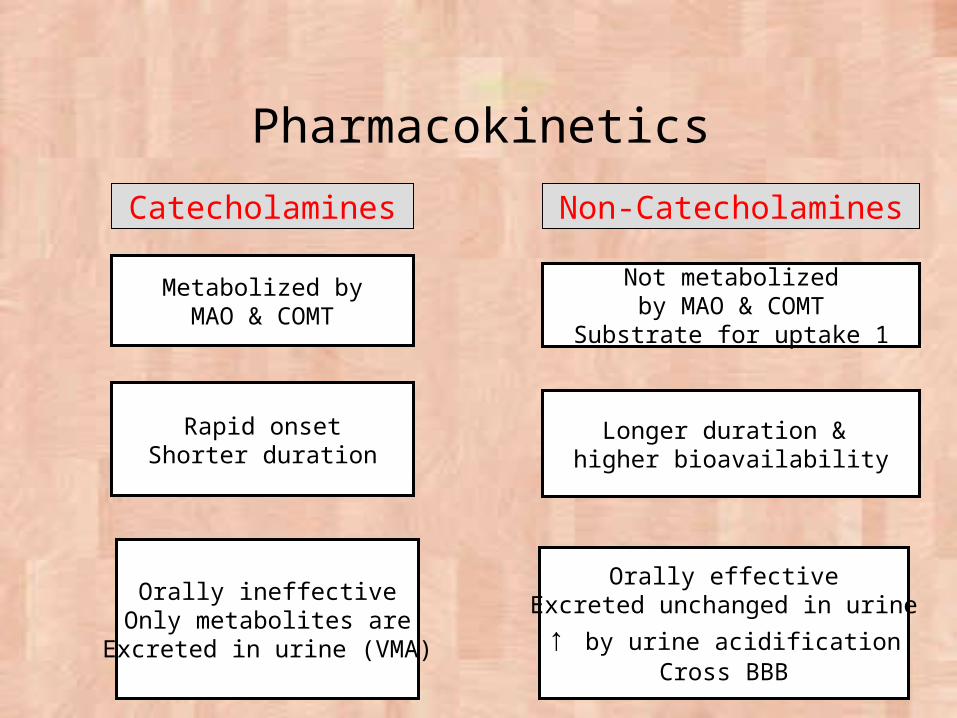
Pharmacokinetics
Catecholamines Non-Catecholamines
Rapid onsetShorter duration
Longer duration & higher bioavailability
Orally ineffectiveOnly metabolites are
Excreted in urine (VMA)
Orally effectiveExcreted unchanged in urine
↑ by urine acidificationCross BBB
Metabolized byMAO & COMT
Not metabolizedby MAO & COMT
Substrate for uptake 1
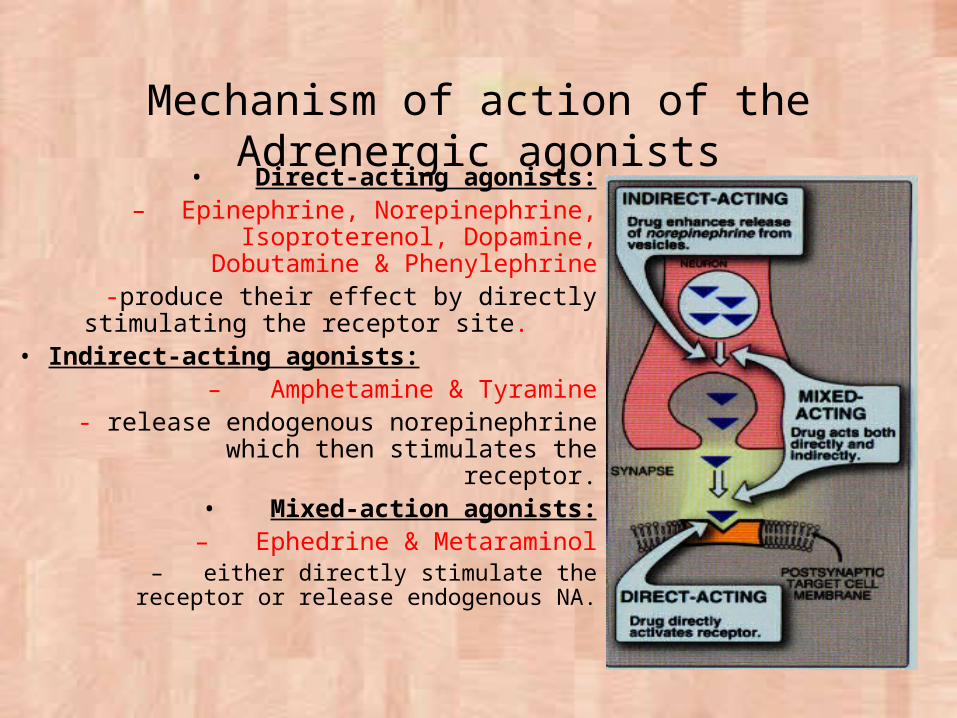
Mechanism of action of the Adrenergic agonists• Direct-acting agonists:
– Epinephrine, Norepinephrine, Isoproterenol, Dopamine, Dobutamine
& Phenylephrine -produce their effect by directly
stimulating the receptor site.• Indirect-acting agonists:
– Amphetamine & Tyramine- release endogenous norepinephrine
which then stimulates the receptor.• Mixed-action agonists:– Ephedrine & Metaraminol
– either directly stimulate the receptor or release endogenous NA.
Direct-Acting Agonist: e.g. Phenylephrine (α1)
Clonidine (α2) (sympathomimetic ?)
Isoprenaline & Dobutamine (β1)
Salbutamol & Terbutaline (β2)
Effects of Adrenergic Agonists
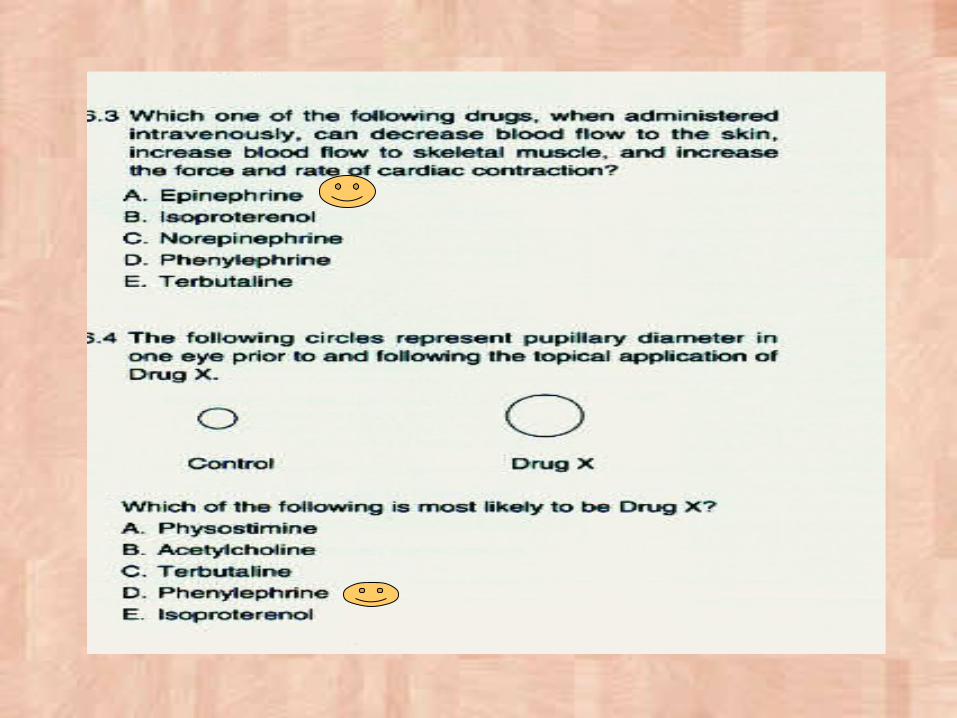
• Cardiovascular: Heart: ↑HR, contractility » ↑CO + O2 consumption
↑Conductivity (atria, AV node & ventricles)↑Excitability » arrhythmia
BV: VD or VC depending on the selective activity of drug and the anatomic site of vessels
e.g. Skin, Splanchnic, Sk.M., renal BV
BP: Depends on effect on heart, PR & venous return
The effect of α-agonist is different from β-agonist
CVS Effect of α-agonist
• Vasoconstriction leading to rise in PR & BP
• ↑ Systolic & diastolic BP (abolished by α-blocker)
• Baroreceptor reflex causing ↑ vagal supply to the heart leading to bradycardia (blocked by atropine)
• CO is not decreased in proportion to the decrease in HR because the venous return increase the stroke
volume
CVS Effect of β-agonist
β1 : +ve chronotropic effect (↑ HR)
•+ve inotropic effect (↑ force of contraction)
•↑ CO and so ↑ systolic BP
β 2: Dilation of arterioles of Sk.M. (↓PR) and so ↓both of systolic & diastolic BP•No vasoconstriction
•Slightly ↑ of systolic BP & ↓ diastolic BP

Summary– Adrenalin (α & β): ↑ systolic BP & slight ↓diastolic BP
– NA: (α & β1) ↑ systolic & diastolic BP + Reflex bradycardia
– Isoproterenol (β-agonist): slight ↑ systolic BP & ↓diastolic BP
– Indirect acting sympathomimetics: ↑ BP (hypertensive crisis)
– Dopamine: ↑ D receptors (renal vasculature VD) + ↑ β1 (heart) + ↑ α1 at high doses (VC)
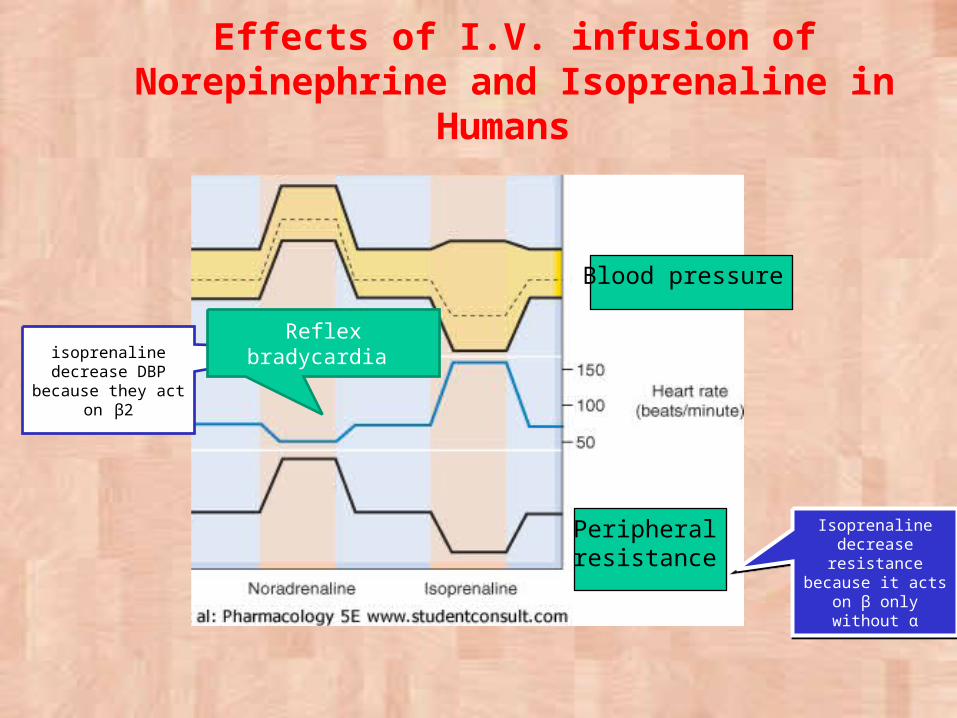
Effects of I.V. infusion of Norepinephrine and Isoprenaline in
Humans
isoprenaline decrease DBP
because they act on β2
Reflex bradycardia
Isoprenaline decrease resistance because it acts on β
only without α
Isoprenaline decrease resistance because it acts on β
only without α
Blood pressure
Peripheral resistance

Effects of Adrenergic Agonists
• Smooth Muscles: Bronchi: bronchodilation (β2) & ↓ bronchial secretion (α1) GIT: relax wall & contract sphincter (constipation) Urinary Bladder: relax wall & contract sphincter (urinary
retention) Eye: Ciliary muscle (β2) Vasoconstriction of conjunctival BV (decongestion) Active mydriasis (α1)
Effects of adrenergic agonists (cont.)
METABOLISM• Hyperglycemia:
– Increase liver glycogenolysis (β2)– Increase glucagon release (β2)– Decrease insulin release (α2)
• Lipolysis:– Increase hydrolysis of TG into free fatty acids &
glycerol (β3)
cAMP
Central Nervous System (CNS)•These drugs produce CNS excitation or alertness•Higher doses produce anxiety, apprehension, restlessness, and tremors.
Dopamine
• Immediate precursor of NE• Occurs in
– CNS (act as neurotransmitter)– Adrenergic nerve ending
– Adrenal medulla
• Activates: – α1(at high doses)
– β1 (at small doses)– D1(occurs in renal vascular bed)
– D2 (occurs in presynaptic adrenergic neurons)
Pharmacological Effects of Dopamine
• CVS:– +ve chronotropic & inotropic effects– At high doses: VC of BV
• Renal & visceral:– VD of renal and splanchnic arterioles– Effective in treatment of shock (the drug of choice
taken by continuous infusion)
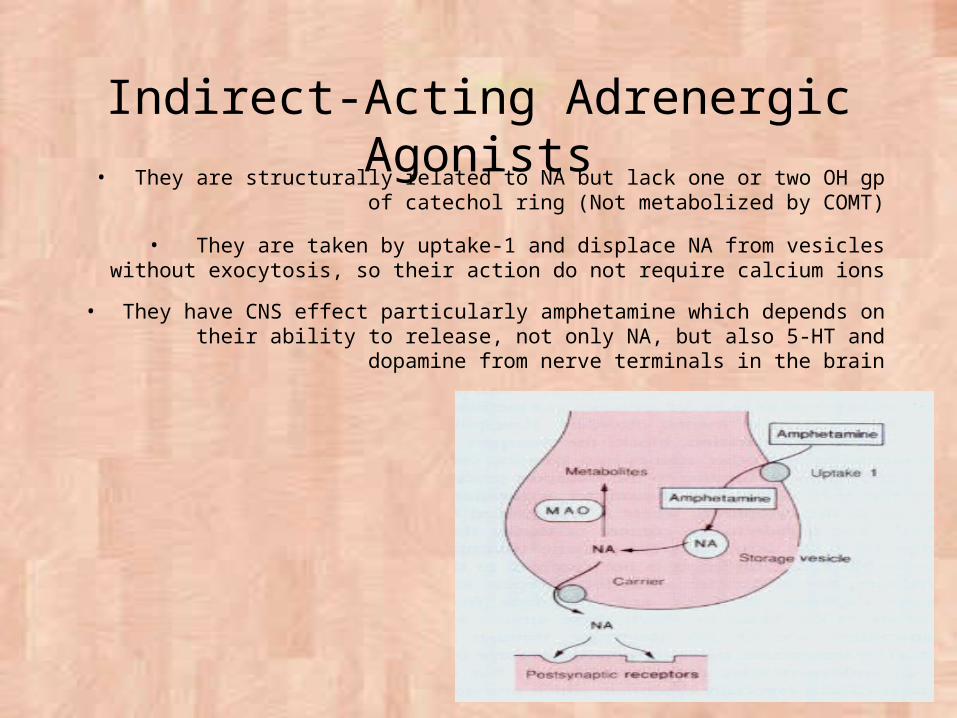
Indirect-Acting Adrenergic Agonists• They are structurally related to NA but lack one or two OH gp of catechol
ring (Not metabolized by COMT)
• They are taken by uptake-1 and displace NA from vesicles without exocytosis, so their action do not require calcium ions
• They have CNS effect particularly amphetamine which depends on their ability to release, not only NA, but also 5-HT and dopamine from nerve
terminals in the brain
• Tachyphylaxis
Indirect-Acting Adrenergic Agonists (cont.)
• Drug Interactions Reserpine: Abolishing their effect
Depleting the stored vesicles
MAOI: Potentiation
They inhibit the metabolism of released NA & also tyramine
TCA: Interfere with their effect
Uptake-1 inhibitor
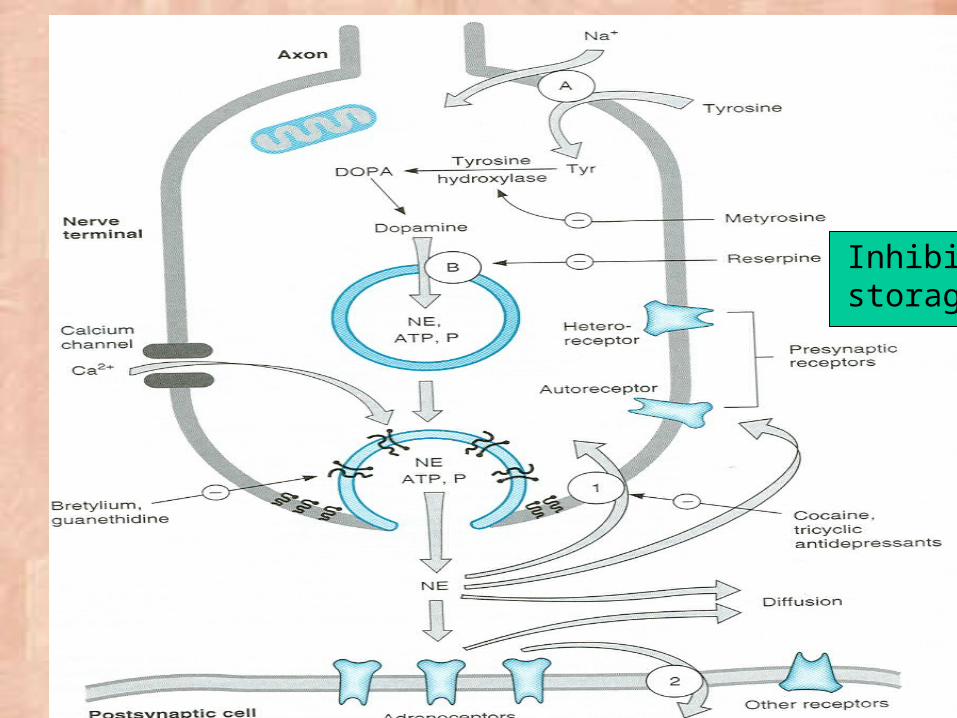
Inhibit storage
Ephedrine
• Plant origin, synthetic compound• Mixed-action acting drug
• It is not a catechol and is a poor substrate for COMT and MAO
• Pharmacological effects:– ↑ systolic & diastolic BP by VC and cardiac stimulation
– Bronchodilation (slowly and less than EP & isoproterenol), so used as prophylactic in chronic asthma (not acute)
– Mild CNS stimulation (↑ alertness, ↓ fatigue & prevent sleep)– Improve athletic performance
– Nasal decongestant
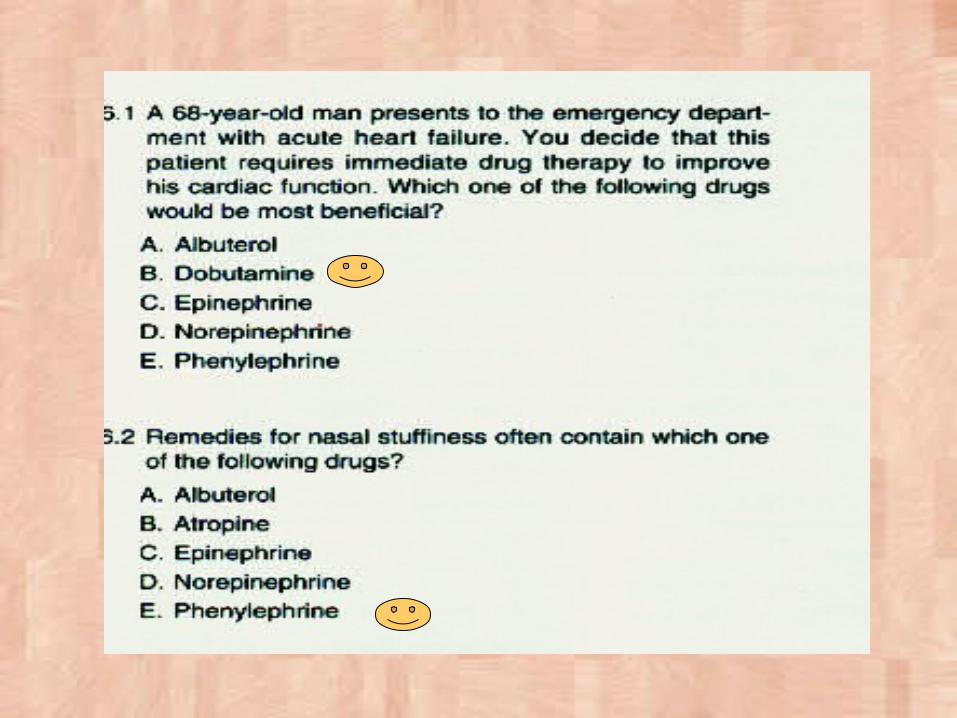
Clinical Uses of Adrenergic Agonists
• Cardiovascular: Cardiogenic Shock, Cardiac arrest:
β agonist: Adrenaline, dobutamine or dopamine Dopamine is clinically more useful in the treatment of shock, in
which significant increase in sympathetic activity might compromise renal function and worsens the peripheral circulation
Malignant hypertension: α2 agonist: ClonidineHYPOTENSION: α1 agonist phenylephrineHeart block : β agonist: isoprenaline
It’s only used now to reverse the block which is produced by overdoses of β – blockers
• N.B. cardiac arrest means : complete cessation of heart’s activity.
• While heart block means : partial or complete inhibition of the spread of conduction of the electrical impulse from the atria to the ventricles
• Anaphylactic reactions:• Ad is the first line of treatment for
bronchoconstriction & CV collapse• Both β and α agonist required.• We use EP with steroid and antihistamine to
cause Bronchodilation, Increase BP
Clinical Uses of Adrenergic Agonists (cont.)
• Respiratory: Asthma and premature labor contractions: For treatment »
Isoprenaline (β agonist), Salbutamol, Terbutalin & Salmeterol (selective β2 is preferred)
For prophylaxis » Salmeterol & FormoterolNorepinephrine is NOT used in treatment of asthma Nasal Decongestion: Ephedrine Haemostatic in epistaxis: Adrenaline & Ephedrine
• Miscellaneous: Mydriatic: Ephedrine Glaucoma: Adrenaline decrease IOP in open angel glaucoma,
decrease aqueous humor production by VC of ciliary body BV. Depression: Amphetamine
ritordine
With local anesthetics: Adrenaline & NA•These drugs are used in dentistry because of their vasoconstrictive actions on blood vessels. •They are added to local anesthetics because they prolong the action of the local anesthetic, reduce the risk for systemic toxicity, and help to create a dry field.
Central Nervous System Stimulation•These medications are used for the treatment of attention deficit hyperactivity disorder, narcolepsy, and as diet aids.
Adverse Effects
– CNS disturbance: anxiety, fear, tension, headache & tremors
– Cerebral hemorrhage
– Tachycardia & Cardiac arrhythmias
– Tachyphylaxis occurs with indirectly acting drugs
Contraindications to use of adrenergics
• Cardiac dysrhythmias, angina pectoris• Hypertension• Hyperthyroidism• Cerebrovascular disease• Distal areas with a single blood supply such
as fingers, toes, nose and ears• Renal impairment use caution
Toxicity of adrenergics in critically ill patients
• Affects renal perfusion• Can induce cardiac dysrhythmias• Increases myocardial oxygen consumption• May decrease perfusion of liver• Tissue necrosis with extravasation
PhenylephrineClinical uses:
• As a mydriatic agent to examine the fundus of the eye– It acts on α1 – receptors in the radial dilator pupillary muscle
• As a decongestant – Used as nasal drops to cause VC in the nasal blood vessels
& relief congestion • As a vasopressor agent in case of hypotension
– α1 stimulation causes VC leading to increase BP
Clinical use of Amphetamine-like drugs
• To suppress appetite – In very obese persons Amphetamine can act centrally
on the hunger center in the hypothalamus to suppress appetite
• In narcolepsy– Narcolepsy is irresistible attacks of sleep during the
day in spite of enough sleep at night – Amphetamine stimulates the CNS & makes the patient
awake • In ADHD “Attention Deficit Hyperactivity Disease”
EphedrineClinical uses:
• Pressor agent (used to increase BP) • Decongestant • It is no longer used to treated bronchial
asthma. (because it’s less potent + slow onset of action)
Pseudoephedrine:
• Has similar pharmacological activities to ephedrine
• It is not controlled : OTC (over the counter)• It is commonly used as a decongestant
Phenylpropranolamine:
• Again it is similar to pseudoephedrine, and was used as decongestant, but it was stopped because it may cause cerebral hemorrhage
Dobutamine: • It is direct acting β 1 – selective agonist• Given only parenterally (not orally) • It causes increases in CO • Uses: Inotropic agent for Heart Failure; in septic and
cardiogenic shock.
Salbutamol:
• It is β2 – selective agonist• Can be used orally, IV and by inhalation• Formulations: (Tablets; Syrup; Injection;
solution and Inhalation)• Clinical Uses
– bronchial asthma by β2 stimulation, which leads to relaxation of bronchial smooth muscle and bronchodilation.
– Treatment of refractory hyperkalemia (I.V)
Salmetrol and Formoterol:
– These selective beta agonists, have longer duration of action as compared to Salbutamole.
– Uses: As inhalors for bronchial Asthma
Clonidine:
• It is a selective α2 – agonist • Mechanism of action : (Acts centrally as a central sympatholytic
drug.) – Clonidine is Lipid – soluble, so, it freely passes BBB & reaches
CNS to stimulate α2 – receptors in medulla and pons causing decreased sympathetic tone and finally decrease BP
• It act by it self not like Methyldopa • Clinical use include:
– Treatment of mild to moderate hypertension – Treatment of morphine withdrawal symptoms – As analgesic during labour
• The dose = 1.25 ug/day • It can be given I.M
• Adverse affects of Clonidine– Depression – Dizziness, insomnia, & nightmares – Impotence – Alopecia الشعر تساقط– Urticaria – Weight gain – Fluid retention – Sudden withdrawal leads to rebound hypertension
Metyldopa and the comparison between it and clonidine are in the lecture (adrenergic antagonists)
3. Apraclonidine
• Like clonidine it is selective α2 adrenoceptor agonist, however, main uses as adjuvant therapy for glaucoma via decrease of aqueous humour formation.