Embed Size (px)
Citation preview
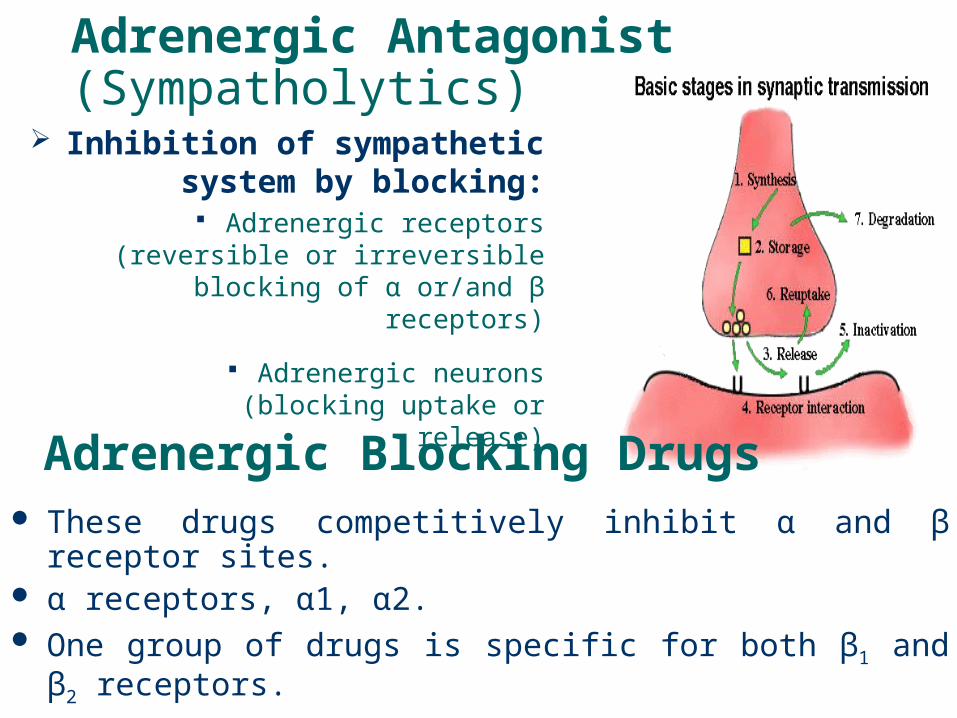
Adrenergic Antagonist (Sympatholytics)
Inhibition of sympathetic system by blocking:
Adrenergic receptors (reversible or irreversible blocking of α
or/and β receptors)
Adrenergic neurons (blocking uptake or release)
These drugs competitively inhibit α and β receptor sites. α receptors, α1, α2. One group of drugs is specific for both β1 and β2 receptors. One group is specific for β2 receptors. One group is specific for both α and β receptors.
Adrenergic Blocking Drugs
Adrenergic Receptor Antagonist
α-Blockers:- Non selective: Phenoxybenzamine & Phentolamine
- α1-Blocker: Prazosin, Terazosin, Doxazosin & Tamsulosin
- α2-Blocker: Yohimbine (Sympatholytic ?)
β-Blockers:- Non selective: Propranolol, Timolol & Nadolol
- β1-Blocker: Atenolol, Metoprolol & Esmolol
- β1-Blocker with partial β2 agonist activity: Acebutolol & Pindolol
α & β Blocker: Labetalol & carvidilol
Effects of α-adrenoceptor Antagonists The most important effect is CVS effect
They block α1 receptors causing decrease in peripheral resistance and
consequently BP The resultant hypotension provokes reflex
tachycardia For non selective α-antagonists, the main differences between phenoxybenzamine and phentolamine are:
Phenoxybenzamine is a prodrug that takes few hrs for biotransformation while phentolamine is not a prodrug
Phenoxybenzamine bind covalently (irreversible binding) to α receptors and so the activity last for about 28 hrs. On the other hand, phentolamine is competitive blocker (reversible binding),
so the activity last for 4hr.
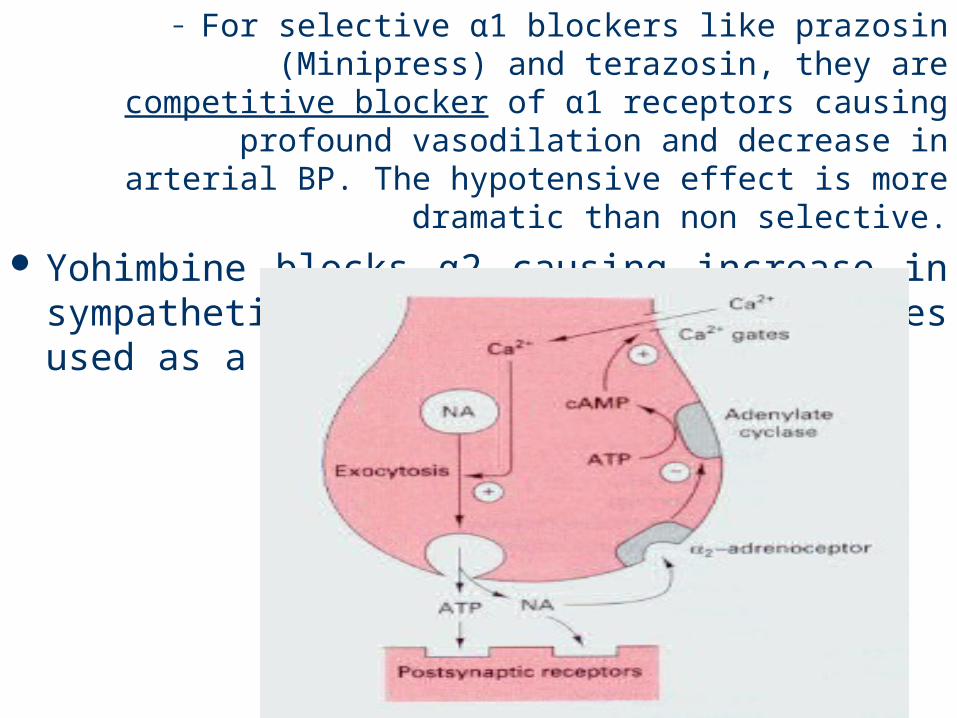
– For selective α1 blockers like prazosin (Minipress) and terazosin, they are competitive blocker of α1
receptors causing profound vasodilation and decrease in arterial BP. The hypotensive effect is
more dramatic than non selective. Yohimbine blocks α2 causing increase in
sympathetic flow and so BP. is sometimes used as a sexual stimulant.
Clinical uses of α-adrenoceptor antagonists
Hypertension: α1 selective blockers are more preferred e.g. prazosin. They are used alone or in
combination with other antihypertensive drugs
Phaeochromocytoma: A combination of α- and β- receptor antagonists is the most effective way of
controlling the BPe.g. phenoxybenzamine and atenolol
Flomax (tamsulosin). Used in BPH. Produces smooth muscle relaxation of prostate gland and bladder neck. Minimal orthostatic hypotension.
Priscoline (tolaxoline) used for Pulmonary hypertension in newborn.
Adverse effects of α-adrenoceptor antagonists
1st dose effect: syncope. With alpha 1 blockers, first dose syncope may occur from hypotension. Give low starting dose and at hs.
Postural hypotension
Tachycardia (α1-selective produce less tachycardia because they do not increase NA release from
sympathetic nerve terminal)
Prazosin may cause sodium & water retention, therefore it is frequently used with a diuretic
Orthostatic hypotension dentistry Orthostatic hypotension is a problem with prazosin
analogs and to a lesser extent tamsulosin. Significantly, orthostatsis is a problem that can be seen with any vasodilator that affects the tone on venous smooth muscle.
This would include, organic nitrates, hydralazine, clonidine, minixodil and the many drugs.
Orthostatic hypotension or postural hypotension occurs when systemic arterial blood pressure falls by more than 20 mmHg upon standing.
In this situation, cerebral perfusion falls and an individual may become light headed, dizzy or fatality may occur.
In changing from the supine to the standing position, gravity tends to cause blood to pool in the lower extremities. However, several reflexes, including sympathetically mediated venoconstriction minimize this pooling and maintain cerebral perfusion. If these reflex actions do not occur, then orthostatic hypotension could result.
By blocking the alpha1-receptors associated with venous smooth muscle, prazosin-like drugs, inhibit the sympathetically mediated vasoconstriction associated with postural changes. Hence, orthostatic hypotension can occur.
Drugs like clonidine cause orthostasis due to its CNS actions that block the sympathetic reflexes.
Vasodilators such as nitrates, minoxidil, hydralazine or impotence medications cause orthostasis because of their actions directly on the vasculature.

β-adrenoceptor antagonists They are all competitive blocker, most of them are nonselective or β1 blocking activity (cardioselective)
β-Blockers:- Non selective: Propranolol, Timolol & Nadolol
- β1-Blocker: Acebutolol, Atenolol, Metoprolol & Esmolol
- β1-Blocker with partial β2 agonist activity: Acebutolol & Pindolol
Beside β blocking activity, some blockers may possess one or more of the following properties:
Intrinsic Sympathetic Activity (ISA): i.e. they have the ability to stimulate the occupied receptors, hence
known as partial agonist e.g. pindolol Membrane stabilizing activity: i.e. inhibit
depolarization of excitable membrane (by blocking Na+ channels) and so they have antiarrhythmic and local
anaesthetic action e.g. propranolol
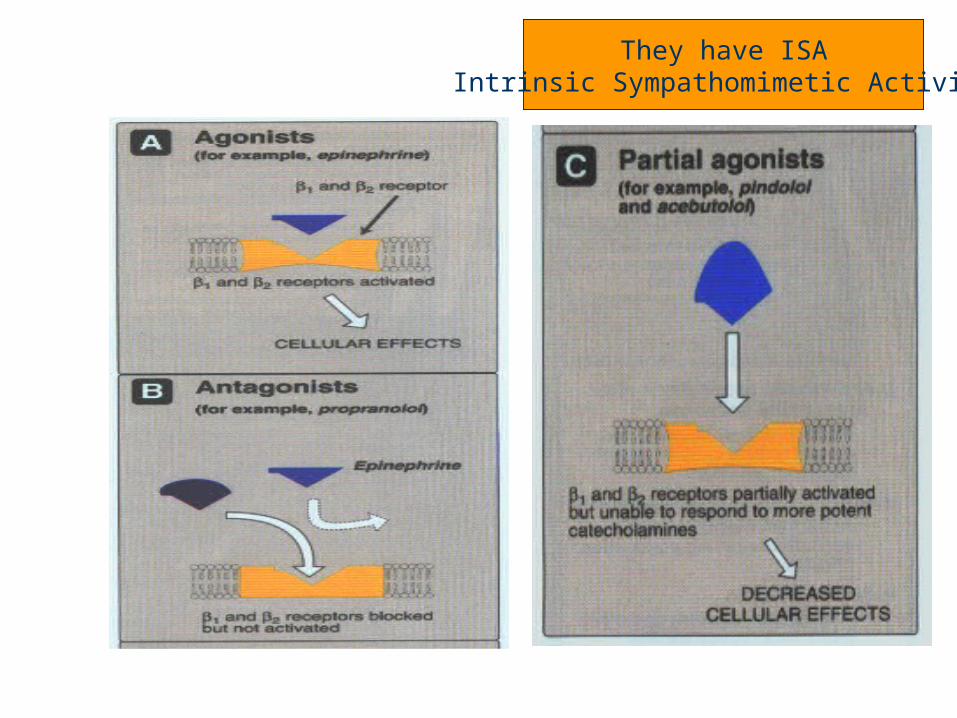
They have ISAIntrinsic Sympathomimetic Activity
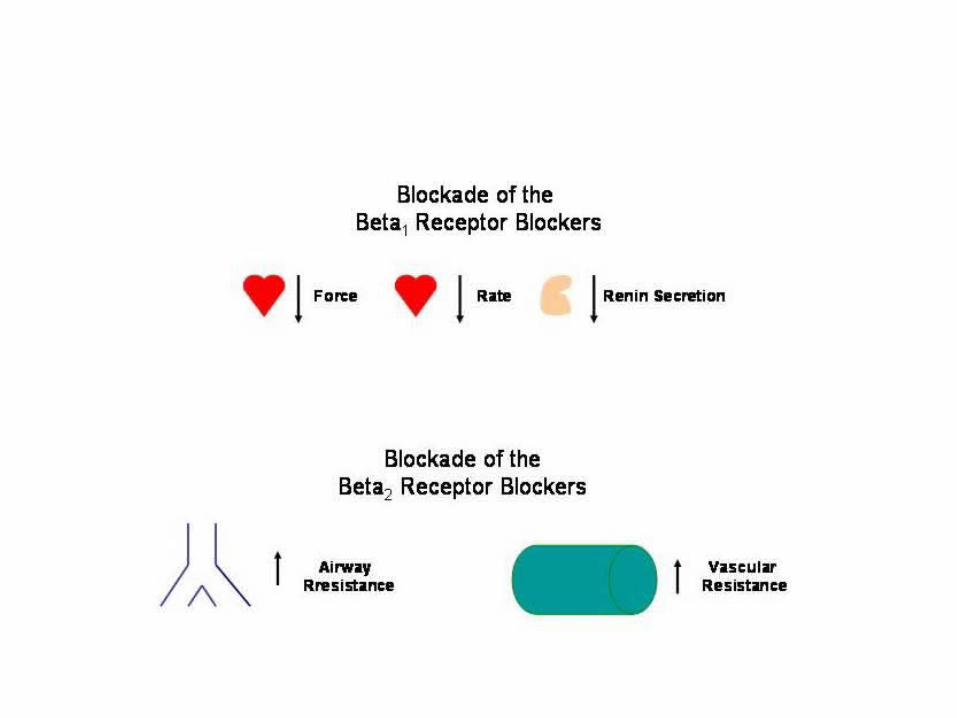
Effects of β-adrenoceptor antagonists
Cardiovascular: – Heart:
-ve chronotropic & inotropic (↓CO, O2 consumption & HR)
↓excitability (antiarrhythmic effect) ↓Conductivity (heart block in large dose)
– BV: Block β2 mediated VD No postural hypotension (No α effect) Reflex VC due to ↓CO & BP and so ↓ blood flow to the
periphery– BP: ↓ with no reflex tachycardia
• Reduction in CO• Reduction in renin release
Effects of β-adrenoceptor antagonists
Bronchial smooth muscles:• In asthma & obstructive pulmonary disease, they can cause
severe bronchoconstriction. This danger is less with β1 selective blocker
Metabolism:• Inhibition of glycogenolysis (Caution with insulin treatment?)
• Inhibition of glucagon release• Hypertriglyceridemia & hypercholesterolemia
Decreased production of aqueous humor in eye
May increase VLDL and decrease HDL Diminished portal pressure in clients with
cirrhosis Decreased renin production.
Receptor selectivity
Acetutolol, atenolol, betaxolol, esmolol, and metoprolol are relatively cardioselective
These agents lose cardioselection at higher doses as most organs have both beta 1 and beta 2 receptors.
esmolol is the most rapidly acting, short t ½ (8 minutes), given only IV for management of arrhythmia.
Non-Receptor selectivity
Carteolol, levobunolol, metipranolol, nadolol, propranolol, sotalol and timolol are all non-selective
Can cause bronchoconstriction, peripheral vasoconstriction and interference with glycogenolysis
Combination selectivity
Labetalol and carvedilol (Coreg) block alpha 1 receptors to cause vasodilation and beta 1 and beta 2 receptors which affect heart and lungs
Both alpha and beta properties contribute to antihypertensive effects
May cause less bradycardia but more postural hypotension
Less reflex tachycardia
Intrinsic sympathomimetic activity
Have chemical structure similar to that of catecholamines
Block some beta receptors and stimulate others
Cause less bradycardia Agents include: acebutolol, penbutolol and
pindolol
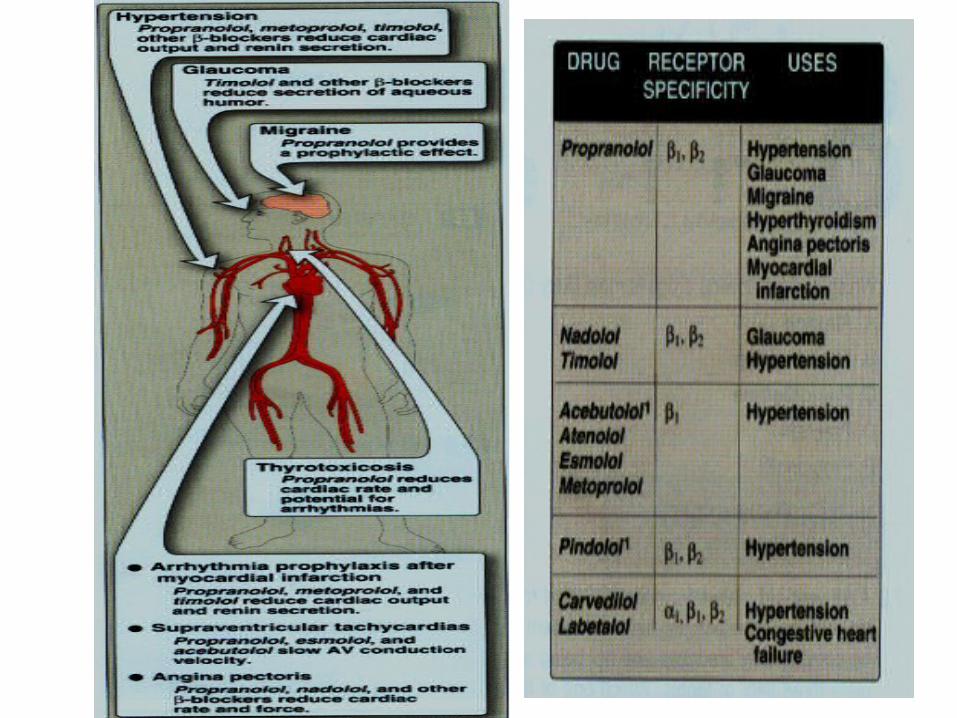
Clinical Uses of β-adrenoceptor antagonists
Cardiovascular:
• Hypertension: • They are used alone or in combination.
• Mixed α & β blocker, labetalol, is often used in preeclamptic toxaemia (a form of hypertension occurring late in pregnancy)
• Angina pectoris• ↓ Cardiac work & O2 consumption by decreasing rate, BP and contractility
• Chronic management of stable angina (not acute treatment)
• Cardiac arrhythmias
• Following myocardial infarction:• It is preferred to give β-blocker immediately following a myocardial
infarction to reduce infarct size by blocking the action of circulating catecholamines
Useful in pheochromocytoma in conjunction with alpha blockers (counter catecholamine release)
Clinical Uses of β-adrenoceptor antagonists (cont.)
• Glaucoma: Open angel • Particularly timolol, used as eye drops
• ↓ secretion of aqueous humor by the ciliary body• They do not affect the ability of eye to focus for near vision or pupil
size
• Hyperthyroidism : • Preoperatively in thyrotoxicosis by blocking sympathetic
stimulation that occurs in hyperthyroidism, particularly cardiac arrhythmia
• Migraine: • as prophylaxis by blocking catecholamine-induced VD in the brain
vasculature
Specific condtions-beta blockers
With significant bradycardia, may need medication with ISA such as pindolol and penbutolol
Patient with asthma, cardioselectivity is preferred
For MI, start as soon as patient is hemodynamically stable
Special conditions—beta blocers
Should be discontinued gradually. Long term blockade results in increase receptor sensitivity to epinephrine and norepinephrine. Can result in severe hypertension. Taper 1-2 weeks.
Adverse effects of β-adrenoceptor antagonists
Bronchoconstriction
Cardiac failure (large dose), May worsen condition of heart failure as are negative inotropes
Hypoglycemia (with reduced awareness of hypoglycemia in patients receiving insulin)
Physical fatigue (due to reduced cardiac output and reduced muscle perfusion in exercise)
Cold extremities
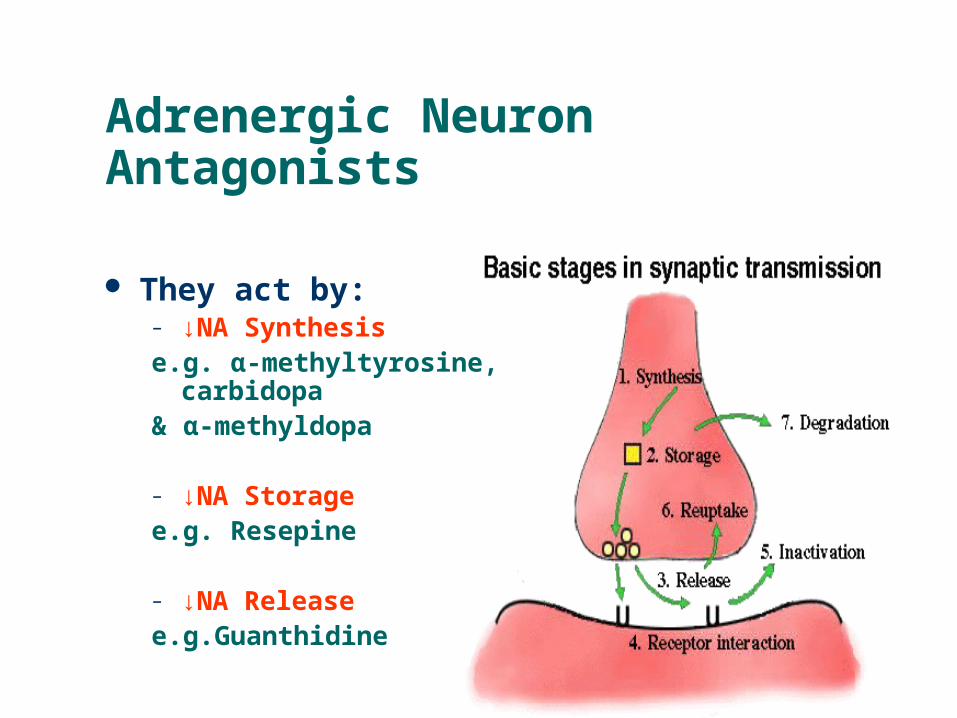
Adrenergic Neuron Antagonists
They act by:– ↓NA Synthesis e.g. α-methyltyrosine, carbidopa & α-methyldopa
– ↓NA Storage e.g. Resepine
– ↓NA Release e.g.Guanthidine
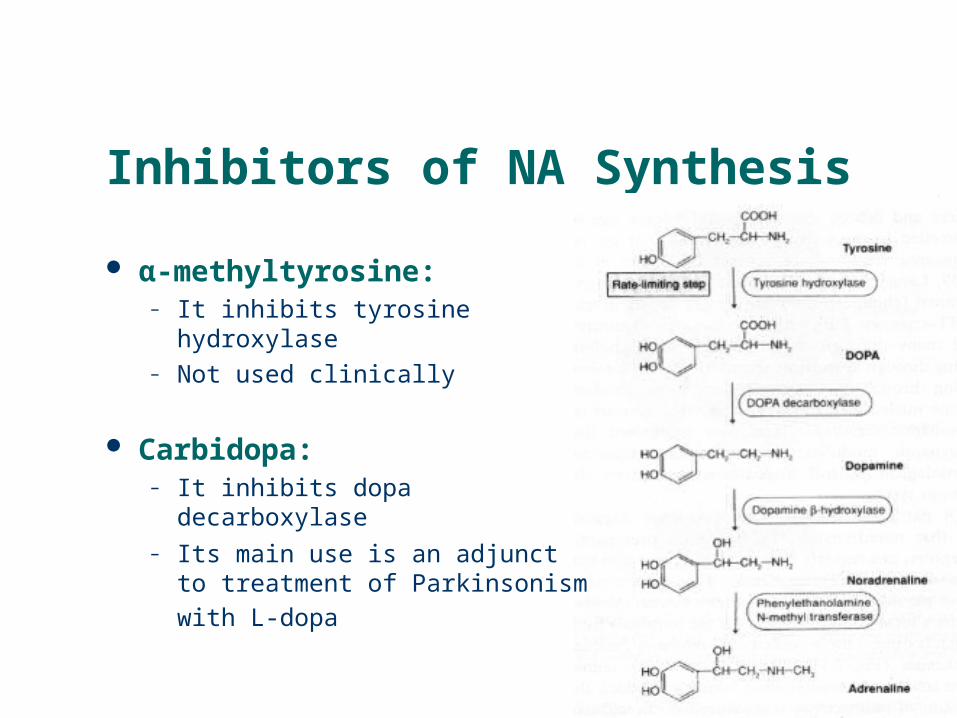
Inhibitors of NA Synthesis
α-methyltyrosine: – It inhibits tyrosine hydroxylase– Not used clinically
Carbidopa: – It inhibits dopa decarboxylase– Its main use is an adjunct to
treatment of Parkinsonism with L-
dopa
Inhibitors of NA Synthesis
α-methyldopa: It is taken up by noradrenergic neurons, where it is
decarboxylated and hydroxylated to form the false transmitter, α-methyl-nor-adrenaline
The false transmitter is released in the same way as NA but differ in two points:
- It is less active than NA on α1 receptors and thus it is less effective in causing vasoconstriction
- It is more active on presynaptic α2 receptors and so stimulates autoinhibitory feedback mechanism
It is used in treatment of hypertension
Inhibitors of NA Storage
Reserpine a plant alkaloid
It acts by blocking ATP-dependent transport of NA and other amines (e.g. 5-HT & dopamine) into synaptic
vesicles, apparently by binding to the transport protein → depletion of NA from the adrenergic neurons
It induces a gradual decrease in BP with concomitant slowing of heart rate. It has slow onset and longer
duration of action (persist for many days after stopping)
Used for hypertension resistant to other treatment
Inhibitors of NA Release
Guanthidine Overall, the principle action of guanthidine involves
its accumulation by the synaptic vesicles, which are then unable to fuse with the cell membrane in the
normal way, so the exocytosis is prevented i.e. Stop the release
It induce transient increase in BP because guanthidine displace NA in its storage sites
At large doses, it causes structural damage of noradrenergic neurons
It is no longer used clinically