Embed Size (px)
Citation preview

UNIVERSIDADE ESTADUAL DE CAMPINAS
FACULDADE DE ODONTOLOGIA DE PIRACICABA
Jessica Montenegro Fonseca
ALTERAÇÕES DO COMPLEXO DENTINA-POLPA EM CÁRIE CONVENCIONAL
E CÁRIE RELACIONADA À RADIAÇÃO: UM ESTUDO COMPARATIVO.
DENTIN-PULP COMPLEX REACTIONS IN CONVENTIONAL AND RADIATION-
RELATED CARIES: A COMPARATIVE STUDY.
Piracicaba
2017

Jessica Montenegro Fonseca
ALTERAÇÕES DO COMPLEXO DENTINA- POLPA EM CÁRIE CONVENCIONAL
E CÁRIE RELACIONADA À RADIAÇÃO: UM ESTUDO COMPARATIVO.
DENTIN-PULP COMPLEX REACTIONS IN CONVENTIONAL AND RADIATION-
RELATED CARIES: A COMPARATIVE STUDY.
Dissertação apresentada à Faculdade de
Odontologia de Piracicaba da Universidade
Estadual de Campinas como parte dos
requisitos exigidos para a obtenção do título de
Mestra em Estomatopatologia, na Área de
Estomatologia.
Dissertation presented to the Piracicaba Dental
School of the University of Campinas in
partial fulfilment of the requirements for the
degree of Master in Pathology, in Stomatology
area.
Orientador: Prof. Dr. Mario Fernando De Goes
Coorientador: Prof. Dr. Alan Roger Dos Santos Silva
ESTE EXEMPLAR CORRESPONDE À VERSÃO FINAL DA DISSERTAÇÃO DEFENDIDA PELA ALUNA JESSICA MONTENEGRO FONSECA E ORIENTADA PELO PROFº. DRº MARIO FERNANDO DE GOES.
Piracicaba
2017

Agência(s) de fomento e nº(s) de processo(s): CAPES, 758/2012
ORCID: http://orcid.org/0000-0002-1217-7298
Ficha catalográfica
Universidade Estadual de Campinas
Biblioteca da Faculdade de Odontologia de Piracicaba
Marilene Girello - CRB 8/6159
Fonseca, Jessica Montenegro, 1991-
F733a Alterações do complexo dentina-polpa em cárie convencional e cárie
relacionada à radiação : um estudo comparativo / Jessica Montenegro
Fonseca. – Piracicaba, SP : [s.n.], 2017.
Orientador: Mario Fernando de Goes.
Coorientador: Alan Roger dos Santos Silva.
Dissertação (mestrado) – Universidade Estadual de Campinas, Faculdade
de Odontologia de Piracicaba.
1. Câncer. 2. Radioterapia. 3. Cárie dentária. 4. Dentes. 5. Polpa dentária.
I. Goes, Mario Fernando de,1954-. II. Santos-Silva, Alan Roger,1981-. III.
Universidade Estadual de Campinas. Faculdade de Odontologia de Piracicaba.
IV. Título.
Informações para Biblioteca Digital
Título em outro idioma: Dentin-pulp complex reactions in conventional and radiation-
related caries : a comparative study
Palavras-chave em inglês:
Cancer
Radiotherapy
Dental caries
Teeth
Dental pulp
Área de concentração: Estomatologia
Titulação: Mestra em Estomatopatologia
Banca examinadora:
Alan Roger dos Santos Silva [Coorientador]
José Flávio Affonso de Almeida
Karina Morais Faria
Data de defesa: 17-07-2017
Programa de Pós-Graduação: Estomatopatologia

UNIVERSIDADE ESTADUAL DE CAMPINAS
FACULDADE DE ODONTOLOGIA DE
PIRACICABA
A Comissão Julgadora dos trabalhos de Defesa de Dissertação de Mestrado, em sessão
pública realizada em 17 de Julho de 2017, considerou a candidata JESSICA MONTENEGRO
FONSECA aprovada.
PROF. DR. ALAN ROGER DOS SANTOS SILVA
PROFª. DRª. KARINA MORAIS FARIA
PROF. DR. JOSÉ FLÁVIO AFFONSO DE ALMEIDA
A Ata da defesa com as respectivas assinaturas dos membros encontra-se no processo de vida
acadêmica do aluno.

DEDICATÓRIA
Dedico este trabalho aos meus pais Jane Montenegro Fonsêca e Ruy Leal Fonsêca,
que por amor e altruísmo abdicaram dos próprios caminhos, para acompanhar-me nos meus;
À minhas irmãs, Taís Montenegro Fonsêca e Elaine Montenegro Fonsêca por igual
apoio.

AGRADECIMENTOS
À Deus por sua presença em mim, todos os dias, na forma de fé, dando- me saúde e
força para superar as dificuldades;
À Universidade Estadual de Campinas, na pessoa do Magnífico Reitor, Prof. Dr.
Marcelo Knobel;
À Faculdade de Odontologia de Piracicaba, na pessoa do seu Diretor Prof. Dr.
Guilherme Elias Pessanha Henriques, e seu Diretor Associado, Prof. Dr. Francisco Haiter
Neto;
Ao Professor Doutor Márcio Ajudarte Lopes, coordenador do Programa de Pós
Graduação em Estomatopatologia, pela atenção com cada um dos alunos do programa e por
todas as oportunidades cedidas;
Ao Professor Doutor Alan Roger dos Santos Silva, pela orientação acadêmica e
profissional e por todo o cuidado e atenção do início ao fim do meu mestrado, sempre
incentivando a criar novos conhecimentos e sendo exemplo de ética e profissionalismo;
Aos Professores Doutores, Oslei Paes de Almeida, Pablo Agustin Vargas, Jacks Jorge
Júnior, Edgard Graner e Ricardo Della Coletta, da Área de Patologia da Faculdade de
Odontologia de Piracicaba, pelo apoio, dedicação e oportunidades de aprendizado;
Aos profissionais do OROCENTRO, em especial ao Rogério de Andrade Elias,
Elisabete, Maria Aparecida Campion, Daniele Cristina Castelli Morelli, pelo apoio, bom
convívio e aprendizado profissional;
Aos profissionais do Laboratório de Patologia Oral, da Faculdade de Odontologia de
Piracicaba, em especial ao Adriano Luís e Fabiana Casarotti, por todo suporte, atenção e
também pelo aprendizado;
À Thaís Bianca Brandão, chefe do serviço de Odontologia Oncológica do Instituto do
Câncer do Estado de São Paulo (ICESP) por ter cedido o material biológico que viabilizou a
execução desta Dissertação e por todo o suporte que tem oferecido ao Programa de Pós
Graduação em Estomatopatologia da FOP - UNICAMP;
À Fundação Brasileira de Coordenação de Aperfeiçoamento de Pessoal de Nível
Superior (CAPES) pelo apoio financeiro, através da concessão da bolsa de mestrado no
período de Agosto de 2015 à Julho de 2017;
À professora Doutora Águida Cristina Gomes Henriques Leitão, minha orientadora de
iniciação científica, pelo apoio e incentivo contínuo desde a minha graduação até hoje;

Aos colegas Wagner Gomes, Mariana Paglioni e Karina Morais pela colaboração na
minha pesquisa e nos experimentos;
À minha turma de mestrado, Gleyson Amaral, Natália Palmier, Rodrigo Soares, Lígia
Miyahara e Camila Weissheimer pela amizade, união, cumplicidade e por todo o apoio
profissional e pessoal;
Aos meus companheiros de moradia Daniel Chan, Lara Caponi, Lucas Del Vigna,
Thaís Tavares, Jordana Carvalho, Rebeca Barros e Bruno Mariz pela irmandade e carinho
durante toda a minha estadia em Piracicaba, facilitando a minha jornada longe de casa;
Por fim a todos os meus colegas e amigos da Faculdade de Odontologia, pelo bom
convívio, troca de experiências e apoio durante o período do meu mestrado.

EPÍGRAFE
“Sempre que houver alternativas, tenha cuidado. Não opte pelo conveniente, pelo
confortável, pelo respeitável, pelo socialmente aceitável, pelo honroso.
Opte pelo que faz o seu coração vibrar. Opte pelo que gostaria de fazer, apesar de todas as
consequências.”
(Osho)

RESUMO
Os carcinomas espinocelulares de cabeça e pescoço são diagnosticados
predominantemente em estadios clínicos avançados da doença e, consequentemente, tratados
por meio de protocolos multimodalidade, incluindo quimiorradioterapia (QRDT). Apesar dos
avanços tecnológicos, protocolos contemporâneos de radioterapia (RDT) atingem, além do
tumor primário, tecidos sadios adjacentes ao tumor, gerando toxicidades agudas e crônicas em
pele, mucosas, glândulas salivares, ossos e dentes, entre outros. A cárie relacionada à
radioterapia (CRR) é uma toxidade crônica que afeta aproximadamente 25% dos pacientes
submetidos à RDT na região de cabeça e pescoço, podendo gerar destruição generalizada dos
dentes, perda de eficiência mastigatória, infecção crônica e risco aumentado para o
desenvolvimento da osteorradionecrose. A inclusão dos dentes no campo de radiação dos
tumores de cabeça e pescoço (CCPs) sugere que a CRR resulta da destruição radiogênica do
esmalte, da junção amelodentinária e do complexo dentina-polpa. Desta forma, é imperioso
compreender se sua patogênese é consequência direta ou indireta da RDT. O objetivo deste
estudo foi comparar padrões microscópicos de resposta do complexo dentina-polpa à
progressão da cárie convencional e da CRR a fim de testar a hipótese de que a RDT é capaz
de modificar diretamente as respostas micromorfológicas do complexo dentina-polpa à
progressão da CRR. Foram utilizados 22 dentes extraídos de pacientes com CCPs, divididos
entre grupo controle (cárie convencional) e grupo estudo (CRR). Os espécimes dos dois
grupos foram pareados por grupo anatômico dental, padrões clínicos de progressão da cárie
[“Post-Radiation Dental Index” (PRDI)] e profundidade de invasão microscópica das lesões de cárie.
As amostras foram desmineralizadas e analisadas por meio da microscopia de luz óptica e da
histomorfometria a fim de investigar a hierarquia tecidual da polpa e padrões microscópicos
da resposta do complexo dentina-polpa à progressão da cárie. Todos os eventos avaliados
neste estudo foram semelhantes entre os grupos, incluindo PRDI (CRR=3.8 vs. controle=3.2),
profundidade de invasão microscópica (CRR=1,056.89 μm vs. controle=1,158.58 μm; p=
0.79), evidência de fibrose pulpar (p=0.9), calcificação pulpar (p=0.34), necrose pulpar
(p=1.0), inflamação pulpar (p= 0.28) e deposição de dentina reacional (p=0.28). Em
conclusão, o presente estudo identificou preservação da hierarquia tecidual da polpa em
ambos os grupos, rejeitando a hipótese de que a RDT é capaz de modificar diretamente as
respostas micromorfológicas do complexo dentina-polpa à progressão da CRR.
Palavras-chave: Câncer; Radioterapia, Cárie Relacionada à Radiação, Dentes, Polpa

ABSTRACT
Head and neck squamous cell carcinomas are mainly diagnosed in late stages, which
consequently increases the necessity for multimodality treatment protocols, such as
chemoradiotherapy (CRT). Although the technological improvement in radiotherapy (RT)
treatment protocols, radiation still damage not only the tumour site but also adjacent healthy
tissues leading to the development of acute and chronic toxicities on the skin and mucosal
tissues, salivary glands, bones, teeth, among others. Radiation-related caries (RRC) is a
chronic toxicity that affects about 25% of the patients who have undergone head and neck RT
(HNRT), and it can lead to generalized tooth breakdown, loss of masticatory efficiency,
recurrent infections and increased risk for the development of osteoradionecrosis. The
inclusion of the teeth inside the radiation field of head and neck tumours (HNC) suggests that
RRC results of a radiogenic destruction of enamel, dentin-enamel junction (DEJ) and dentin-
pulp complex. Therefore, it`s of great importance to further understand if it’s the direct or
indirect influence of RT on the pathogenesis of RRC. The aim of the present study was to
compare microscopic patterns of the dentin-pulp complex response to the progression of
conventional caries lesions and RRC, testing the null hypothesis that the RT is able to directly
modify the micromorphological response of the dentin-pulp complex facing RRC
progression. Twenty-two teeth extracted from HNC patients were divided into control
(conventional caries) and study (RRC) groups. The samples from both groups were paired
matched by anatomic dental group, clinical patterns of caries progression [“Post-Radiation
Dental Index” (PRDI)] and depth of microscopic invasion of caries lesions. Samples were
demineralized and analysed by means of light microscopy and histomorphometry in order to
investigate the pulp tissue hierarchy and microscopic patterns of the dentin-pulp complex
response to caries. The results found in the present study were similar between the groups,
including PRDI (Control= 3.2 vs RRC= 3.8), depth of microscopic invasion (Control=
1,158.58 μm vs RRC= 1,056.89 μm; p=0.79), pulp fibrosis evidence (p=0.9), pulp
calcification (p=0.34), pulp necrosis (p=1.0), pulp inflammation (p=0.28) and tertiary dentin
deposition (p=0.28). In conclusion, the present study observed preservation of pulp tissue
hierarchy in both groups rejecting the null hypothesis that the RT is able to directly modify
the micromorphological response of the dentin-pulp complex facing RRC progression.
Key Words: Cancer; Radiotherapy, Radiation-Related Caries, Teeth, Pulp.

SUMÁRIO
1 INTRODUÇÃO 12
2 ARTIGO: Dentin-Pulp Complex Reactions In Conventional And
Radiation-Related Caries: A Comparative Study
17
3 CONCLUSÃO 35
REFERÊNCIAS 36
ANEXOS
Anexo 1: Parecer Consubstanciado do CEP 40
Anexo 2: Certificado de submissão ao periódico: Clinical Oral
Investigations
41

12
1 INTRODUÇÃO
A incidência do câncer aumentou de modo exponencial nos últimos anos em todo o
mundo, e passou a apresentar um grande desafio no cenário de políticas em saúde pública.
Estima-se que, até 2030, 27 milhões de casos novos serão diagnosticados no mundo. No
Brasil, para 2017, foram estimados 596 mil novos casos de câncer (INCA, 2016). Neste
contexto, o câncer de cabeça e pescoço (CCP) representa 6% de todas as neoplasias malignas,
afetando frequentemente os tecidos moles e duros da boca, lábios, faringe, laringe, glândulas
salivares menores e maiores, cavidade nasal e seios paranasais (Sloan et al., 2017). Entre
todos os casos de câncer de cabeça e pescoço, 90% correspondem a carcinomas
espinocelulares (CECs) de boca orofaringe (Rodrigues et al., 2014; Sloan et al., 2017).
Indivíduos do gênero masculino, idosos, tabagistas e etilistas de longa data e grande
intensidade representam o principal perfil clínico para o câncer de boca e orofaringe (Pelucchi
et al., 2008; Neville et al., 2016). Recentemente, outro grupo composto por pacientes mais
jovens (menos de 40 anos de idade) e sem fatores de risco comumente associados ao câncer
de boca foi identificado (Ribeiro et al., 2009). A infecção pelo papiloma vírus humano (HPV),
principalmente o genótipo 16 e 18, também é atualmente considerada fator de risco para o
CEC de orofaringe e, ao que tudo indica, está associada ao comportamento sexual (sexo oral)
(Sloan et al., 2017) .
Em adição à problemática da alta frequência dos CECs bucais e de orofaringe, é
importante esclarecer que a maior parte destes tumores é diagnosticada tardiamente, em
estadiamentos clínicos avançados da doença, o que torna seu tratamento desafiador e
associado a baixas taxas de sobrevida em cinco anos. Os protocolos de tratamento
contemporâneos do CEC de boca e orofaringe costumam envolver a cirurgia, a quimioterapia
(QT) e a radioterapia (RDT) associadas ou, mais frequentemente, combinadas (Huang e
O´sullivan, 2013; Marta et al., 2015).
A radiação ionizante atua diretamente sobre as células tumorais durante o ciclo celular,
produzindo espécies reativas de oxigênio que interagem, por sua vez, com o DNA, o RNA e
as enzimas celulares de forma a desorganizar seus nucleotídeos e danificar seu material
genético de modo que não consegue ser reparado pelos mecanismos regulatórios de células
malignas, gerando apoptose, morte celular e diminuição da capacidade proliferativa do tumor
(Huber e Terezhalmy, 2003).

13
A dose de RDT é expressa pela quantidade de energia absorvida pelo tecido irradiado.
A unidade que padroniza a dose absorvida pelo tecido é conhecida como Gray (Gy = 1J/Kg)
(Huber; Terezhalmy, 2003; Rolim; Costa; Ramalho, 2011). Com o objetivo de minimizar
toxicidades ao paciente, a RDT em cabeça e pescoço costuma ser administrada ao longo de 5
a 7 semanas com frações diárias de 2 Gy, 5 vezes por semana com intervalos de dois dias (aos
finais de semana) a fim de que os tecidos sadios adjacentes ao tumor possam se recuperar
(Vissink et al., 2003; Kielbassa et al., 2006).
A QT também cumpre papel importante no tratamento dos CECs bucais e de
orofaringe e tem sido associada à RDT (quimiorradioterapia - QRDT) de forma a elevar as
chances de sucesso terapêutico, podendo ser aplicada antes (indução), simultaneamente
(neoadjuvante) ou após o tratamento radioterápico (adjuvante). Desta forma, a QRDT atua
reduzindo o tamanho do tumor primário, potencializando a atividade citotóxica do tratamento
e reduzindo o risco de metástases (Bucheler et al., 2012). No entanto, esta modalidade pode
intensificar as toxicidades bucais que comumente geram dor intensa, necessidade de
interrupção dos protocolos de tratamento oncológico, redução nas taxas de sucesso do
tratamento e aumento dos custos globais de tratamento do câncer (Seiwert et al., 2007).
O tratamento radioterápico associado ou não à QT para os CCPs promove reações aos
tecidos sadios adjacentes ao campo irradiado, incluindo os dentes. De acordo com Cooper et
al. (1995), a região de cabeça e pescoço é complexa do ponto de vista anatômico, onde
estruturas muito distintas do ponto de vista biológico reagem de uma maneira muito variável à
radiação. Neste cenário, as principais toxicidades da RDT incluem mucosite, disgeusia,
disfagia, hipossalivação, infecções oportunistas, osteorradionecrose, CRR e trismo, entre
outros (Vissink et al., 2003; Lobo; Martins, 2009). Estas toxicidades podem se manifestar
logo no início (agudas) ou após meses da conclusão da RDT (crônicas), sendo que as últimas
podem apresentar duração permanente aos pacientes que sobreviverem (Vissink et al., 2003).
Nesta problemática, a CRR é uma toxicidade crônica que surge após aproximadamente
12 meses da conclusão do tratamento radioterápico e afeta cerca de 25% dos pacientes
tratados por RDT em cabeça e pescoço. Interessantemente, os padrões clínicos de início,
desenvolvimento e progressão da CRR são distintos aos da cárie convencional (Hong et al.,
2010). O início da CRR geralmente afeta as áreas cervical e incisal dos dentes anteriores
(Kielbassa et al., 2006), gerando primariamente perda do brilho e translucidez do esmalte da
coroa dental seguida por alteração da coloração da coroa que passa a assumir tom
esbranquiçado que, se não tratado, progride para marrom escuro em associação a trincas e
fraturas nas superfícies livres de esmalte. Posteriormente, o esmalte sofre o fenômeno de

14
“delaminação” caracterizado pelo desprendimento de grandes áreas de esmalte que acaba
expondo a dentina (tecido mais frágil) ao ambiente bucal dos pacientes irradiados, marcado
por alto potencial cariogênico e que permitirá rápida deterioração das coroas dentárias que
acabam amputadas da raiz, expondo o canal radicular ao meio bucal, tornando-se fácil acesso
para entrada de microrganismos nos tecidos periapicais. (Frank et al., 1965; Schweyen et al.,
2012). Caso não seja instituído um protocolo de prevenção ou tratamento à CRR, pode
ocorrer destruição generalizada dos dentes de pacientes oncológicos, representando um
grande risco para o desenvolvimento de focos de infecção crônica e, consequentemente, de
osteorradionecrose (Vissink et al., 2003; Silva et al., 2009). Geralmente, a deterioração dos
tecidos dentais relacionada à CRR não está associada a queixa de dor espontânea, ou
estimulada, por parte dos pacientes (Schweyen et al., 2012).
O conjunto de sinais e eventos clínicos “atípicos” descritos acima, no contexto da
CRR, acaba por estimular clínicos e pesquisadores a atribuir o início e a progressão da CRR a
danos radiogênicos diretos sobre a microestrutura dentária. Esta eventual destruição
radiogênica seria responsável pela perda gradual da vitalidade pulpar e consequente retração
dos processos odontoblásticos, gerando fragilidade na junção amelodentinária (JAD)
(Dahllöf et al., 1994; Grötz et al., 2001). Outros autores sugeriram que alterações radiogênicas
diretas alterariam o fluxo vascular da polpa e reduziriam a condução nervosa dos nociceptores
pulpares, permitindo que a CRR progredisse de modo mais rápido na ausência dos
mecanismos protetores de dor nos pacientes oncológicos irradiados (Knowles et al., 1986;
Schweyen et al., 2012). Ainda no campo da vascularização pulpar, estudos clínicos
demonstraram que os níveis de oxigenação da polpa diminuem durante a radioterapia para
tumores de cabeça e pescoço. Contudo, o mesmo grupo de autores, em outro estudo mais
recente, demonstrou níveis normais de oxigenação da polpa após 4 a 6 anos da conclusão do
tratamento radioterápico, sugerindo que a radioterapia provavelmente não tem influência a
longo prazo na vitalidade da polpa (Kataoka et al., 2011; Kataoka et al., 2016).
Os estudos supramencionados validam evidências sobre o fato de que a patogênese da
CRR permanece controversa e incerta, especialmente no que se refere à capacidade da RDT
em gerar efeitos diretos na estrutura dentária. Uma série de pesquisadores e especialistas
acreditam que a CRR não deve ser atribuída aos efeitos diretos da RDT sobre os dentes; ao
contrário, seria resultado de um “agrupamento de sintomas bucais” representados por efeitos
indiretos da radiação que se desenvolvem em pacientes com CCPs submetidos à RDT, como
as alterações quantitativas (hipossalivação) e qualitativas (microbiota bucal) da saliva que são

15
notoriamente atribuídas ao aumento do risco de cárie (Kielbassa et al., 2006; Sciubba et al.,
2006). Tais alterações na quantidade e na composição salivar alteram a microbiota oral,
estimulando o desenvolvimento de microrganismos acidófilos com patogenicidade aumentada
como Streptococcus mutans, Lactobacillus e espécies de Cândida (Al-Nawas et al., 2006;
Kielbassa et al., 2006).
O “agrupamento de sintomas orais” é ainda composto por alterações na dieta do
paciente com CPP submetido à RDT. O déficit nutricional típico deste perfil de pacientes
oncológicos é compensado por meio da ingestão de alimentos mais calóricos, de consistência
pastosa ou líquida, ricos em carboidratos, em porções pequenas e frequentes, o que favorece a
adesão à superfície dental de um ambiente sem saliva e aumenta a predisposição à cárie
rampante (Deng et al., 2015). Além disso, esta população enfrenta um desafio no controle da
placa dental devido a um curto intervalo de tempo entre as refeições e também à dor
relacionada à mucosite (induzida pela QRDT) que afeta diretamente o estímulo à higiene oral
e a capacidade de remoção mecânica do biofilme dental (Vissink et al., 2003; Kielbassa et al.,
2006; McGuire et al., 2014; Brennan et al., 2010).
Adicionalmente a esta teoria multifatorial acerca da patogênese da CRR, a hipótese do
dano radiogênico direto para os tecidos dentários permanece latente na literatura científica.
Estudos anteriores utilizando modelos experimentais animais ou técnicas de RDT já em
desuso defendem a ideia de alterações pulpares em dentes submetidos a altas doses de
radiação (Meyer et al., 1962; Hutton et al., 1974; Vier –Pelisser et al., 2007). Do mesmo
modo, pesquisas in vitro, sustentam a existência de alterações na estrutura mineralizada de
dentes irradiados (Pioch et al., 1992; Springer et al., 2005; De Barros da Cunha et al., 2017).
Springer et al., (2005), concluiu em um estudo que a radiação é capaz de causar dano direto
ao colágeno presente na polpa dental, não ocorrendo em tecido mineralizado devido a
concentração relativamente baixa desta proteína na dentina e esmalte.
Contrariamente a estes resultados, estudos recentes de nossa equipe de pesquisadores -
baseados em dentes irradiados in vivo- indicam que os efeitos diretos da radiação não são
capazes de causar alterações micromorfológicas nos tecidos dentários. Em outras palavras, é
pouco provável que a radiação ionizante dos protocolos oncológicos de RDT em cabeça e
pescoço represente um fator de risco independente para o início e a progressão da CRR (Silva
et al., 2009; Faria et al., 2014; Gomes-Silva et al., 2017).

16
A despeito dos resultados mencionados, tornou-se imperioso aprimorar o
conhecimento do impacto da RDT sobre o complexo dentina-polpa e sua habilidade de
responder à progressão da CRR, tendo em vista os resultados de pesquisas sugerindo que os
efeitos diretos da radiação limitariam a resposta do complexo dentina-polpa e justificariam a
rápida progressão clínica da CRR (Springer et al., 2005; El-Faramawy et al., 2013; McGuire
et al., 2014).
Portanto, o presente estudo se propôs a comparar os padrões microscópicos de
resposta do complexo dentina-polpa à progressão da cárie convencional e da CRR, com a
finalidade de testar a hipótese de que a RDT é capaz de modificar diretamente as respostas
micromorfológicas do complexo dentina-polpa à progressão da CRR.

17
2 ARTIGO
Este trabalho foi realizado no formato alternativo, conforme Informação
CCPG/001/2015, da Comissão Central de Pós-Graduação (CCPG) da Universidade Estadual
de Campinas.
Dentin-pulp complex reactions in conventional and radiation-related caries: A
comparative study.
Jéssica Montenegro Fonsêcaa
Wagner Gomes Silvaa,b
Natalia Rangel Palmiera
Pablo Agustin Vargasa
Mario Fernando De Goesc
Marcio Ajudarte Lopesa
João Victor Salvajolid
Ana Carolina Prado Ribeiroa,b
Thais Bianca Brandãoa,b
Alan Roger Santos-Silvaa,b
a Oral Diagnosis Department, Semiology and Oral Pathology Areas, Piracicaba Dental School,
University of Campinas (UNICAMP), Piracicaba, São Paulo, Brazil.
b Dental Oncology Service, Instituto do Câncer do Estado de São Paulo (ICESP), Faculdade
de Medicina da Universidade de São Paulo, São Paulo, Brazil.
c Department of Dental Materials, Piracicaba Dental School, Av. Limeira, 901, Piracicaba, SP
13414-903, Brazil.
d Radiotherapy Service, Instituto do Câncer do Estado de São Paulo (ICESP), Faculdade de
Medicina da Universidade de São Paulo, São Paulo, Brazil.
Corresponding Author
Alan Roger Santos-Silva DDS, MSc, PhD
Department of Oral Diagnosis, Semiology Area
Piracicaba Dental School, University of Campinas (UNICAMP)
Av. Limeira, 901, Bairro Areão, Piracicaba-SP, Brasil. CEP 13414-903
[email protected] Telephone: +55 19 21065320

18
ACKNOWLEDGMENTS
The authors would like to gratefully acknowledge the financial support of the São
Paulo Research Foundation (FAPESP) processes numbers 2013/18402-8 and 2012/06138-1 as
well as The Coordination for the Improvement of Higher Education Personnel
(CAPES/PROEX process number 758/2012). The authors also thank Fabiana Facco
Cassarotti and Adriano Luis Martins who provided technical support and contributed to the
experimental development of the study.

19
ABSTRACT
Introduction: radiation-related caries (RRC) is one of the most significant oral toxicities of
head and neck radiotherapy (HNRT); however, the potential of radiation to directly cause
harmful dentin and pulpal effects and impair response to caries progression is controversial.
Therefore, the aim of this study was to characterize the reactions of the dentin-pulp complex
in teeth affected by RRC. Methods: twenty-two carious teeth extracted from 22 head and neck
cancer patients were divided into control (conventional caries; n=11) and irradiated (RRC;
n=11) groups and matched by dental homology, clinical patterns of caries progression
following the Post-Radiation Dental Index (PRDI) and microscopic depth of carious invasion
(1,158.58µm control vs. 1,056.89µm irradiated; p=0.79). Optical light microscopy and
histomorphometry descriptively investigated histopathological characteristics based on
morphological hierarchy and cell populations of dental pulp, including blood vessels, neural
elements, extracellular matrix components, presence of inflammation, patterns of carious
invasion and reactionary dentin presence. Results: pulp histopathological changes and dentin
reaction patterns were similar between groups and varied according to the PRDI scores and
carious lesions depth. Conclusions: dentin and pulp reactions to RRC are highly preserved.
Clinical relevance: direct effects of radiation therapy may not be directly injurious to the pulp
to the extent of impairing the response to caries progression.
Key Words: Cancer; Caries; Radiotherapy, Radiation-Related Caries, Teeth, Pulp.

20
INTRODUCTION
Head and neck cancer (HNC) represent 6% of all human malignancies and
approximately 650,000 new cases are diagnosed annually worldwide. Treatment protocols
often involve the combination of surgery, chemotherapy, and head and neck radiotherapy
(HNRT). Although considered highly effective in the locoregional control of cancer, HNRT
results in a myriad of acute and chronic toxicities to non-targeted tissues, including oral
mucositis, hyposalivation, oral opportunistic infections, trismus, radiation-related caries
(RRC) and osteoradionecrosis, among others [1, 2].
RRC, also known as “radiation caries”, is a chronic side effect of HNRT that affects
up to 25% of patients who underwent HNRT. Its hallmark is a high potential for generalized
dentition destruction and clinical patterns of progression that differ from conventional caries,
being characterized by widespread cervical demineralization, incisal edges and cusp tips
lesions and diffuse brownish to black discoloration of the smooth surface of enamel. RRC
rapidly progresses causing enamel cracks, delamination and amputation of teeth crowns,
leading to teeth destruction. In addition, it can increase the risk for the development of
osteoradionecrosis and negatively impact the overall oral function as well as the quality of life
of cancer survivors [3, 4].
One of the most controversial topics in the scenario of HNRT side effects is the ability
of ionizing radiation to cause direct radiogenic destruction to the teeth. Although many
studies have suggested direct radiogenic damage to the dentin and pulp that would lead to
RRC [5, 6, 7], others have linked the increased risk of caries in post-HNRT patients with the
indirect effects of radiation therapy. These would include hyposalivation, oral microbiota
alterations, impaired self-cleaning properties, poor oral health status prior to and after
treatment, increased dietary intake of carbohydrates, and insufficient fluoride exposure, which
form a cluster of oral symptoms that predisposes patients to rampant caries regardless of the
direct effect of radiation on teeth [8, 9, 10].
Hence, considering that HNRT is routinely used in more than 90% of all HNC patients
[2], it is paramount to precisely understand its impact on the reactions of dentin and pulp to
caries progression. To date, no study has been conducted to investigate biological evidence
that radiation therapy could be directly injurious to the dentin-pulp complex and impair
response to caries progression. Therefore, this study aimed to evaluate if in vivo irradiated

21
human teeth affected by RRC have microscopically discernible effect on dentin and pulp
responses when compared to conventional caries teeth samples.
PATIENTS AND METHODS
Patients and specimen collection
This study was approved by the local Ethics Committee (protocol number 023/2015)
and was conducted in accordance with the Declaration of Helsinki. Carious teeth (n=22) from
HNC patients were collected independently of the particulars of the study. Dental extractions
were performed due to advanced caries or periodontal disease in both teeth groups (control
and irradiated). Immediately after the extractions, teeth were identified, placed in plastic
containers with 10% buffered formalin solution and fixed for at least 72 h at 4 °C [3].
Eleven teeth affected by RRC were extracted from 11 patients with head and neck
squamous cell carcinomas (SCC) who were subjected to clinical radiation protocols with
tridimensional conformal HNRT in 6-mV linear accelerators on the Synergy Platform (Elekta
AB, Stockholm, Sweden) with cumulative doses that ranged from 60 to 70 Gy (2 Gy/day, five
days per week). The tridimensional HNRT plan of the patients was retrieved from the CMS
system XiO version 4.60 (Elekta CMS software, St. Louis, MS, USA) to study the radiation
field and the total dose directed to the teeth [11]. Eleven carious non-irradiated teeth
specimens were extracted from 11 head and neck SCC patients before radiation treatment
during mouth conditioning protocols.
For clinical characterization of the patients, the electronic medical record system was
consulted and the following data were collected: age, gender, tumor topography, alcohol
consumption and smoking habit, tumor histological type, clinical cancer stage (according the
American Joint Committee on Cancer), total radiation dose prescribed to tumor treatment
(Gy), anatomic origin of extracted teeth, and time between the end of HNRT and teeth
extraction.
Macroscopic analysis
All twenty-two carious teeth samples were divided into two groups: control
(conventional caries; n=11) and irradiated (RRC; n=11), cataloged and subjected to
photographic documentation. Teeth samples from both groups were classified and matched by

22
dental homology (anatomic group), clinical patterns of caries progression established by the
Post-Radiation Dental Index (PRDI) [12] and microscopic depth of carious invasion (refer to
microscopy analysis).
Demineralization and histological preparation
All specimens were cleaned up with manual periodontal curettes to remove residual
soft tissues and decalcified in Ana Morse’s solution (equal volumes of 20% sodium citrate
and 50% formic acid) at 4 °C for three weeks, with changes every two days. The
decalcification was monitored and confirmed by weekly periapical radiographs. Specimens
were sectioned along the longitudinal teeth axis through the center of the deepest carious
lesions with the aid of a histologic disposable razor. The samples were embedded in Paraplast
Plus® (Leica Biosystems Richmond, Inc., Richmond, IL, USA) to produce 5-µm-thick
sections on a microtome (Leica, Nussloch, Germany) in silanized slides for hematoxylin and
eosin (H&E) morphological evaluation.
Optical light microscopy analysis
An optical light microscope (OLM) (DM4000 B Leica, Wetzlar, Germany) was used
for the micromorphological study of the cell populations of dental pulp, including blood
vessels, neural elements, extracellular matrix components, inflammation, depth of carious
invasion and reactionary dentin presence. Three demineralized histological sections of each
specimen were analyzed and illustrative microscopic images were captured.
Two previously calibrated oral pathologists analyzed the slides. A descriptive analysis
was performed for the morphologic criteria [13,14] regarding microscopic dentin and pulp
reactions to caries progression, which were evaluated in a semi-quantitative way and
compared between groups: presence and preservation of hierarchy of the dental pulp;
presence and preservation of blood vessels; pulp extracellular matrix components (fibrosis,
calcification, necrosis or inflammation) and the presence of reactionary dentin. Examiners
were instructed to come to a consensus in discordant cases. Results were analyzed by using
descriptive statistics, absolute values, and percentages.
Mean microscopic depth of caries invasion was quantitatively determined by
measuring the distance from the surface of the demineralized dentin to the deepest point of

23
caries-affected dentin in three demineralized histological sections of each specimen, in both
groups, which was obtained in microns (µm) by using the software LAS version 4.2.0 (Leica
Microsystems, Switzerland).
Statistical analysis
Morphological outcomes were descriptively analyzed and the results generated were
analyzed by using descriptive statistics (Fisher's exact test), absolute values, and percentages.
Mean values of microscopic depth of caries invasion for each specimen were compared
between both groups using the Student’s t-test for independent samples. The software IBM
SPSS Statistics for Windows version 22.0 (Armonk, NY, USA) was used with the
significance level set at α=0.05.
RESULTS
Demographic features and clinicopathological data obtained from the 22 patients are
described in Table 1. The control and irradiated groups consisted of 6 molars (54.54%), 3
pre-molars (27.27%), 1 incisor (9.09%) and 1 canine (9.09%) each. The mean time for teeth
extraction following HNRT was 33 months, ranging from 4 to 62 months. The mean dose
received by each tooth sample was 53.47 Gy, ranging from 38.79 to 69.33 Gy (Table 1).
Mean PRDI scores were 3.2 for the control group and 3.8 for the irradiated group, with
values ranging from 2 to 5 in both groups. The dentin demineralization patterns were similar
between the groups and marked by triangular demineralization with the base at the tooth
surfaces and the apex pointing towards the pulp. Demineralization depth due to caries
progression was controlled during specimens’ selection, leading to a mean depth of 1,158.58
μm (ranging from 471,57 to 2,498.48 μm) in the control group and 1,056.89 μm (ranging
from 750,75 to 1,407.54 μm) in the irradiated group (p=0.79).
All pulp specimens presented well-preserved polarized odontoblastic layers arranged
in palisade, subodontoblastic cell-poor layers of Weil and central zones with prominent
normal blood vessels, fibroblasts, and neural bundles. The microscopic analysis revealed the
presence and the preservation of the pulp cellular layers hierarchy in 8 (72.7%) cases for the
control group and 8 (72.7%) cases of the irradiated group (p=0.28) (Figures 1A and 1B). In
the other cases of both groups, the presence and the preservation of the pulp cellular layers

24
hierarchy was changed because of calcification, diffuse chronic inflammation and necrosis
associated to bacterial invasion. Blood vessels presence and vascular architectural
preservation was observed in all (100%) samples of both groups.
All samples from both groups (100%) presented well-preserved subodontoblastic
layers, which were closely related to well-preserve odontoblasts layers. Odontoblasts from all
samples were characterized by tall columnar cells arranged in palisade and located at the
periphery of the dental pulp. Cell processes arising from the odontoblasts' cell body could be
observed penetrating into the dentin and in close contact between fibroblasts of all studied
samples (Figures 2A and 3A).
Superficial caries-infected dentin composed of disorganized dentin and bacterial
colonies, as well as an inner demineralized layer with affected, but not disrupted, dentin was
consistently observed in all studied specimens of both groups (Figures 2B and 3B). Pulp
extracellular matrix components were similarly detected in both groups and characterized by
focal areas of fibrosis: 8 (72.7%) control cases vs. 7 (63.6%) irradiated cases (p=0.9);
calcification: 5 (45,5%) cases in each studied group (p = 0.34); necrosis: 4 (36.4%) control
cases vs. 3 (27.3%) irradiated cases (p=1.00); and chronic inflammation: 7 (63.6%) control
cases vs. 6 (55,5%) irradiated cases (p=0.28) (Figures 2C and 3C). Reactionary dentin
formation was detected underlying caries demineralization fronts. The presence of reactionary
dentin was observed in 6 (55,5%) cases of the control group and 5 (45,5%) cases of the
irradiated group (p=0.28) (Figures 2D and 3D).
No significant difference was encountered between irradiated and non-irradiated
groups in any of the analyzed parameters. No evidence of abnormal cellular components or
architecture could be detected.
DISCUSSION
The potential of HNRT to cause direct harmful dentin and pulpal effects that could
impair the response of the dentin-pulp complex to caries progression is controversial. In this
context, Kataoka et al. [15] showed that the levels of pulp oxygenation are decreased during
radiotherapy for malignant intraoral and oropharyngeal tumors. More recently, the same
group of authors [16] demonstrated normal pulp oxygenation levels after 4 to 6 years of the
conclusion of HNRT, suggesting that radiation therapy may not have a long-term influence on

25
pulp vitality. Influenced by their results, we decided to perform a study to investigate
microscopic evidence that radiation therapy could be directly injurious to the pulp and impair
response to caries progression by using teeth extracted after a mean time of 33 months
following the conclusion of HNRT (ranging from 4 to 62 months).
The clinicopathological profile of patients enrolled in this study is in accordance with
the traditional features of oral and oropharyngeal SCC patients observed worldwide [17, 18],
which is marked by elderly male individuals, smokers and drinkers with poor oral health
status who were diagnosed at late stages of tumor progression [19, 20, 21].
The clinical aggressiveness and the potential for generalized dental destruction have
been well documented in RRC patients and predominately linked to post-radiation
hyposalivation [9, 22, 23]. However, observations based on in vitro studies proposed that the
direct effects of HNRT on tooth-mineralized structure might also be a significant causal factor
for RRC [5, 7, 12, 24].
Although the potential benefits in terms of reducing treatment-associated toxicities,
the intensity-modulated radiotherapy (IMRT) technology is not available in many centers of
the world, where tridimensional conformal radiotherapy (3DRT) is still routinely used [25,
26, 27]. In this context, 3DRT was the technology used in all of the patients investigated in
the present study and its use is still widely accepted because no overall survival benefits have
been observed in HNC patients treated with IMRT [28]. Most importantly, high doses of
radiation were directed to the irradiated group samples of the current study (mean dose of
53.47Gy) and the influence of the radiation technique should not be considered an issue in
terms of radiogenic effects, especially because a collaborative study recently demonstrated
that IMRT and 3DRT deliver similar doses of radiation to the teeth of HNC patients [29].
One of the limitations of the current study was the small number of teeth specimens
analyzed; wherein larger sample sizes would probably lead to more robust results. However, it
is important to clarify that this limitation was a consequence of the strict methodological
design used, which was based on a paired-matched sampling approach by teeth anatomic
origin, clinical stage of RRC progression and microscopic depths of caries invasion. In
addition, this study relied on human in vivo irradiated teeth (which are seldom collected
because of the risk of osteoradionecrosis) rather than in samples irradiated in vitro.
Comparisons between studies that evaluated in vivo and in vitro effects of radiotherapy on
dental pulp should be carefully established because in vitro simulated radiotherapy does not

26
represent real clinical conditions concerning the cariogenic microenvironment or the
dosimetric standards for HNRT [11].
From a microscopic point of view, patterns of dentin demineralization presented
normal architecture [13,14] and varied according to the PRDI in both groups. The
microscopic analysis found homogeneous results between the groups, showing no statistical
difference to the criteria of presence and preservation of hierarchy of the dental pulp; presence
and preservation of blood vessels; pulp extracellular matrix components (fibrosis,
calcification, necrosis or inflammation) and the presence of reactionary dentin. Apparently,
this was the first study to compare RRC and conventional caries specimens by using matched-
paired teeth groups.
Previous studies based on animal experimental models or with an obsolete technique
of radiotherapy, also investigated pulpal reactions related to radiation, but not to caries
progression, and concluded that only teeth subjected to high doses of radiation (more than 50
Gy) showed alterations in the dental pulp tissue, including fibrotic and inflammatory
degenerations [30, 31]. Conversely, a recent study failed to detect morphological changes or
altered patterns of immunohistochemical expression of proteins related to vascularization
(CD34 and smooth muscle actin), innervation (S-100, NCAM/CD56, and neurofilament), and
extracellular matrix (vimentin) in dental pulp after in vivo HNRT, showing broad preservation
of the microvascular and neural pulp components following high doses of radiation [32].
In conclusion, the present study rejected the hypothesis that HNRT is able to impair
the micromorphological pulp reactions to RRC progression. Therefore, direct effects of
radiation may not be regarded as an independent factor to explain the rapid onset and
aggressive clinical patterns of RRC progression.

27
COMPLIANCE WITH ETHICAL STANDARDS
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
- Research Foundation (FAPESP) processes numbers 2013/18402-8 and
2012/06138-
- Coordination for the Improvement of Higher Education Personnel
(CAPES/PROEX) process number 758/2012.
Ethical approval
All procedures performed in studies involving human participants were in accordance
with the ethical standards of the institutional and/or national research committee and with the
1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.

28
REFERENCES
1. Merlano MC, Monteverde M, Colantonio I, Denaro N, Lo Nigro C, Natoli G,
Giurlanda F, Numico G, Russi E (2012) Impact of age on acute toxicity induced
by bio- or chemo-radiotherapy in patients with head and neck cancer. Oral Oncol
48:1051-Doi:10.1016/j.oraloncology.2012.05.001
2. Buglione M, Cavagnini R, Di Rosario F, Sottocornola L, Maddalo M, Vassalli L.
et al (2016) Oral toxicity management in head and neck cancer patients treated
with chemotherapy and radiation: Dental pathologies and osteoradionecrosis (Part
1) literature review and consensus statement. Crit Rev Oncol Hematol 97:131-42.
doi: 0.1016/j.critrevonc.2015.08.010.
3. Silva ARS, Alves FA, Antunes A, Goes MF, Lopes MA (2009) Patterns of
Demineralization and Dentin Reactions in Radiation-Related Caries. Caries
Research 43:43-9. doi: 10.1159/000192799
4. Hong CH, Napeñas JJ, Hodgson BD, Stokman MA, Mathers-Stauffer V, Elting
LS, Spijkervet FK, Brennan MT (2010) Dental Disease Section, Oral Care Study
Group, Multi-national Association of Supportive Care in Cancer
(MASCC)/International Society of Oral Oncology (ISOO) A systematic review of
dental disease in patients undergoing cancer therapy. Support Care Cancer
18:1007-21. doi: 10.1007/s00520-010-0873-2
5. Pioch T, Golfels D, Staehle HJ (1992) An experimental study of the stability of
irradiated teeth in the region of the dentino enamel junction. Endod Dent
Traumatol 8:241-244. doi: 10.1007/s00520-010-0873-2
6. Kielbassa AM, Beetz I, Schendera A, Hellwig E (1997) Irradiation effects on
microhardness of fluoridated and non-fluoridated bovine dentin. Eur J Oral Sci
105:444-7.
7. Springer IN, Niehoff P, Warnke PH, Bocek G, Kovács G, Suhr M, Wiltfang J,
Açil Y (2005) Radiation caries – radiogenic destruction of dental collagen. Oral
Oncol 41:723–728. doi: 10.1016/j.oraloncology.2005.03.011
8. Brennan MT, Elting LS, Spijkervet FK (2010) Systematic reviews of oral
complications from cancer therapies, Oral Care Study Group, MASCC/ISOO:
methodology and quality of the literature. Support Care Cancer 18:979-84. doi:
10.1007/s00520-010-0856-3

29
9. Kielbassa AM, Hinkelbein W, Hellwig E, Meyer-Lückel H (2006) Radiation-
related damage to dentition. Lancet Oncol 7:326-35. doi: 10.1016/S1470-
2045(06)70658-1
10. Santos-Silva AR, Feio Pdo S, Vargas PA, Correa ME, Lopes MA (2015) cGVHD-
Related Caries and Its Shared Features with Other 'Dry-Mouth'-Related Caries.
Braz Dent J 26:435-40. doi: 10.1590/0103-6440201300200
11. Morais-Faria K, Menegussi G, Marta G, Fernandes PM, Dias RB, Ribeiro AC,
Lopes MA, Cernea CR, Brandão TB, Santos-Silva AR (2015) Dosimetric
distribution to the teeth of patients with head and neck cancer who underwent
radiotherapy. Oral Surg Oral Med Oral Pathol Oral Radiol 120:416-9. doi:
10.1016/j.oooo.2015.05.009
12. Walker MP, Williams KB, Wichman B (2008) Post-radiation dental index:
development and reliability. Support Care Cancer 16:525-30. doi:
10.1007/s00520-007-0393-x
13. Bjørndal L (2008) The caries process and its effect on the pulp: the science is
changing and so is our understanding. Pediatr Dent 30:192-6.
14. Bjørndal L, Mjör IA (2001) Pulp-dentin biology in restorative dentistry. Part 4:
Dental caries-characteristics of lesions and pulpal reactions. Quintessence Int
32:717-36.
15. Kataoka SH, Setzer FC, Gondim-Junior E, Pessoa OF, Gavini G, Caldeira CL
(2011) Pulp Vitality in patients with intraoral and oropharyngeal malignant tumors
undergoing radiation therapy assessed by pulse oximetry. J Endod 37:1197-200.
doi: 10.1016/j.joen.2011.05.038
16. Kataoka SH, Setzer FC, Gondim-Junior E, Fregnani ER, Moraes CJ, Pessoa
OF,Gavini G, Caldeira CL (2016) Late Effects of Head and Neck Radiotherapy on
Pulp Vitality Assessed by Pulse Oximetry. J Endod 42:886-9. doi:
10.1016/j.joen.2016.02.016
17. Kowalski LP, Carvalho AL, Priante AVM, Magrin J (2005) Predictive factors for
distant metastasis from oral and oropharyngeal squamous cell carcinoma. Oral
Oncol 41:534–41. doi: 10.1016/j.oraloncology.2005.01.012
18. Rodrigues PC, Miguel MC, Bagordakis E, et al (2014) Clinicopathological
prognostic factors of oral tongue squamous cell carcinoma: a retrospective study of
202 cases. Int J Oral Maxillofac Surg 43:795-801. doi: 10.1016/j.ijom.2014.01.014
19. Pelucchi C, Gallus S, Garavello W, Bosetti C, La Vecchia C (2008) Alcohol and

30
tobacco use, and cancer risk for upper aerodigestive tract and liver Eur J Cancer
Prev 17:340-4. doi: 10.1097/CEJ.0b013e3282f75e91
20. Bonan PRF, Lopes MA, Pires FR, Almeida OPD (2006) Dental management of
low socioeconomic level patients before radiotherapy of the head and neck with
special emphasis on the prevention of osteoradionecrosis. Braz Dent J 17:336–342.
21. Jham BC, Reis PM, Miranda EL, et al (2008) Oral health status of 207 head and
neck cancer patients before, during and after radiotherapy. Clin Oral Investig
12:19–24. doi: 10.1007/s00784-007-0149-5
22. Lăcătuşu S, Frâncu L, Frâncu D (1996) Clinical and therapeutical aspects of
rampant caries in cervico-facial irradiated patients. Rev Med Chir Soc Med Nat
Iasi 100:198-202.
23. Vissink A, Jansma J, Spijkervet FK, Burlage FR, Coppes RP (2003) Oral sequelae
of head and neck radiotherapy. Crit Rev Oral Biol Med. 2003;14:199-212.
24. Kalnins V (1954) The indirect effect of x-ray irradiation on the dental pulp of the
dog. J Dent Res 33:389-99. doi: 10.1177/00220345540330031201
25. Jonhston M, Clifford S, Bromley R, Back M, Oliver L, Eade T (2011) Volumetric
modulated arc therapy in head and neck radiotherapy: a planning comparison using
simultaneous integrated boost for nasopharynx and oropharynx carcinoma. Clin
Oncol 23:503–11. doi: 10.1016/j.clon.2011.02.002
26. Miles EA, Clark CH, Urbano MT, Bidmead M, Dearnaley DP, Harrington KJ,
A'Hern R, Nutting CM (2005) The impact of introducing intensity modulated
radiotherapy into routine clinical practice. Radiother Oncol 77:241-6. doi:
10.1016/j.radonc.2005.10.011
27. Marta GN, Silva V, de Andrade Carvalho H, de Arruda FF, Hanna SA, Gadia R,
da Silva JL, Correa SF, Vita Abreu CE, Riera R (2014) Intensity-modulated
radiation therapy for head and neck cancer: systematic review and meta-analysis.
Radiother Oncol 110:9-15. doi: 10.1016/j.radonc.2013.11.010
28. Karmiol M, Walsh RF (1975) Dental caries after radiotherapy of the oral regions. J
Am Dent Assoc 91:838-45.
29. Fregnani ER, Parahyba CJ, Morais-Faria K, Fonseca FP, Ramos PA, de Moraes
FY, da Conceição Vasconcelos KG, Menegussi G, Santos-Silva AR, Brandão TB
(2016) IMRT delivers lower radiation doses to dental structures than 3DRT in
head and neck cancer patients. Radiat Oncol 11:116. doi: 10.1186/s13014-016-
0694-7

31
30. Meyer I, Shklar G, Turner J (1962). A comparison of the effects of 200 kV
radiation and cobalt-60 radiation on the jaws and dental structure of the white rat:
a preliminar report. Oral Surg Oral Med Oral Pathol 15:1098–108.
31. Vier-Pelisser FV, Figueiredo MAZ, Cherubini K, Braga-Filho A, Figueiredo JA
(2007) The effect of head-fractioned teletherapy on pulp tissue. Int Endod J 40:
859–65. doi:10.1111/j.1365-2591.2007.01294.x
32. Faria KM, Brandão TB, Ribeiro AC, Vasconcellos AF, de Carvalho IT, de Arruda
FF, Castro Junior G, Gross VC, Almeida OP, Lopes MA, Santos-Silva AR (2014)
Micromorphology of the dental pulp is highly preserved in cancer patients who
underwent head and neck radiotherapy. J Endod 40:1553-9. doi:
10.1016/j.joen.2014.07.006

32
TABLES
Table 1. Clinicopathological profile of studied patients
Irra
dia
ted
Gro
up
Patient Age Gender Tobacco Alcohol Site T N M CH RDT Dose Dental Dose
1 58 M Yes Yes Tongue 3 0 0 Yes 3D 70 Gy 67.83 Gy
2 65 M Yes Yes Oropharynx 4 3 0 Yes 3D 70 Gy 38.79 Gy
3 52 F Yes Yes Tongue 4 2 0 No 3D 70 Gy 59.35 Gy
4 54 M Yes Yes Tongue 2 3 0 Yes 3D 70 Gy 46.71 Gy
5 56 F No No Nasopharynx 4 1 0 Yes 3D 70 Gy 63.83 Gy
6 65 F Yes Yes Tongue 3 0 0 No 3D 60 Gy 40.04 Gy
7 65 F Yes Yes Tongue 4 0 0 No 3D 70 Gy 69.33 Gy
8 66 M Yes Yes Tongue 4 2 0 Yes 3D 70 Gy 46.71 Gy
9 62 M Yes Yes Oropharynx 2 2 0 Yes 3D 70 Gy 53.11 Gy
10 47 M Yes Yes Oropharynx 1 2 0 Yes 3D 70 Gy 51.81 Gy
11 54 M Yes Yes Oropharynx 4 1 0 Yes 3D 70 Gy 51.81 Gy
Con
trol
Gro
up
1 52 M Yes Yes Nasopharynx 3 3 0 - - - -
2 68 M Yes No Larynx 4 3 0 - - - -
3 76 M Yes Yes Submandibular gland 3 2 0 - - - -
4 55 M Yes Yes Hypopharynx 1 2 0 - - - -
5 60 M Yes Yes Larynx 4 3 0 - - - -
6 53 M Yes Yes Oral Cavity 4 2 0 - - - -
7 55 M Yes Yes Tongue 2 0 0 - - - -
8 61 M Yes Yes Soft Palate 4 0 0 - - - -
9 51 F Yes Yes Tongue 4 1 0 - - - -
10 48 M Yes Yes Oral Cavity 1 2 0 - - - -
11 61 M Yes Yes Soft Palate 1 2 0 - - - -
M: Male; F: Female; CH: Chemotherapy; RDT: Radiotherapy; 3D: Tridimensional conformal radiotherapy; Dental Dose: mean radiation dose
delivered to each tooth.

33
FIGURES
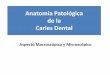
Figure 1. Microscopic overview of irradiated teeth crowns showing preservation of the dental
pulp layers hierarchy (Hematoxylin and Eosin-stained sections, 2X magnification). A.
Irradiated molar sample. B. Irradiated premolar sample.
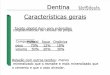
Figure 2. Control group samples exhibiting preservation of the dental pulp layers hierarchy
(Hematoxylin and Eosin-stained sections). A. Dentin (D), predentin (PD), odontoblasts (O)
and pulp central region (C). B. Patterns of bacterial invasion of the dentin. C. Chronic

34
inflammation affecting irradiated pulp tissue. D. Preservation of the dental pulp
micromorphology and dentin-pulp complex reactions to caries. Dentin (D), reactionary dentin
(RD), predentin (PD), odontoblastic layer (O), cell-poor zone (CP), cell-rich zone (CR) and
central region (C) with preserved fibroblasts, and vascular bundles.
Figure 3. Irradiated group samples exhibiting preservation of the dental pulp layers hierarchy
(Hematoxylin and Eosin-stained sections). A. Presence of preserved neural vascular bundles,
dystrophic calcification, and hyperemia in irradiated pulp tissue. Dentin (D), predentin (PD),
odontoblasts (O) and pulp central region (C). B. Superficial caries-infected dentin composed
of bacterial colonies and disorganized dentin. Inner demineralized layer with affected dentin
showing normal patterns of bacterial invasion of the irradiated dentin. C. Chronic
inflammation affecting irradiated pulp tissue. D. Preservation of the dental pulp layers
hierarchy and dentin-pulp complex reactions to caries. Reactionary dentin (RD), cell-poor
zone (CP), cell-rich zone (CR), central region (C), odontoblasts (O), predentin (PD), and
dentin (D). Note the presence of preserved fibroblasts and neural vascular bundles.

35
3 CONCLUSÃO
Não foram identificadas diferenças microscópicas significativas entre os padrões de
resposta do complexo dentina-polpa entre dentes afetados por cárie convencional e
CRR.
Este estudo rejeitou a hipótese de que a RDT é capaz de modificar diretamente as
respostas micromorfológicas do complexo dentina-polpa à progressão da CRR.

36
REFERÊNCIAS1
Al-Nawas B, Grotz KA. Prospective study of the long term change of the oral flora after
radiation therapy. Support Care Cancer. 2006; 14 (3): 291-6.
Brennan MT, Elting LS, Spijkervet FK. Systematic reviews of oral complications from cancer
therapies, Oral Care Study Group, MASCC/ISOO: methodology and quality of the literature.
Support Care Cancer. 2010 Aug;18(8):979-84.
Bucheler BM, Ehnes A, Kavsadze M, Langenberg S, Wilhelm-Buchstab T, Zipfel M, et al.
Quality of life after treatment of head and neck tumors: Longitudinal comparison after
operation and adjuvant radio(chemo)therapy. HNO. 2012; 60 (12): 1053–9.
Cooper JS, Fu K, Marks J, Silverman S. Late effects of radiation therapy in the head and neck
region. Int J Radiat Oncol Biol Phys. 1995; 31(5):1141-64.
Dahllöf G, Rozell B, Forsberg CM, Borgström B. Histologic changes in dental morphology
induced by high dose chemotherapy and total body irradiation. Oral Surg Oral Med Oral
Pathol. 1994 Jan;77(1):56-60.
De Barros da Cunha SR, Fonseca FP, Ramos PAMM, Haddad CMK, Fregnani ER, Aranha
ACC. Effects of different radiation doses on the microhardness, superficial morphology, and
mineral components of human enamel. Arch Oral Biol. 2017 Apr 10;80:130-135.
Deng J, Jackson L, Epstein JB, Migliorati CA, Murphy BA. Dental demineralization and
caries in patients with head and neck cancer. Oral Oncol. 2015 Sep;51(9):824-31.
El-Faramawy N, Ameen R, El-Haddad K, El-Zainy M. Effects of gamma radiation on hard
dental tissues of albino rats: investigation by light microscopy. Radiat Environ Biophys. 2013
Aug;52(3):375-87.
Frank RM, Herdly J, Philippe E. Acquired Dental Defects and Salivary Gland Lesions After
Irradiation For Carcinoma. J Am Dent Assoc. 1965 Apr;70:868-83.
1 De acordo com as normas da UNICAMP/FOP, baseadas na padronização do International
Committee of Medical Journal Editors - Vancouver Group. Abreviatura dos periódicos em
conformidade com o PubMed.

37
Faria KM, Brandão TB, Ribeiro AC, Vasconcellos AF, de Carvalho IT, de Arruda FF, Castro
Junior G, Gross VC, Almeida OP, Lopes MA, Santos-Silva AR. Micromorphology of the
dental pulp is highly preserved in cancer patients who underwent head and neck radiotherapy.
J Endod. 2014 Oct;40(10):1553-9.
Gomes-Silva W, Prado-Ribeiro AC, Brandão TB, Morais-Faria K, de Castro Junior G, Mak
MP, Lopes MA, Rocha MM, Salo T, Tjäderhane L, de Goes MF, Santos-Silva AR.
Postradiation Matrix Metalloproteinase-20 Expression and Its Impact on Dental
Micromorphology and Radiation-Related Caries. Caries Res. 2017 Mar 31;51(3):216-224.
Grötz KA, Riesenbeck D, Brahm R, Seegenschmiedt MH, al-Nawas B, Dörr W, Kutzner J,
Willich N, Thelen M, Wagner W. [Chronic radiation effects on dental hard tissue (radiation
caries). Classification and therapeutic strategies]. Strahlenther Onkol. 2001 Feb;177(2):96-
104.
Hong CH, Napeñas JJ, Hodgson BD, Stokman MA, Mathers-Stauffer V, Elting LS, Spijkervet
FK, Brennan MT. Dental Disease Section, Oral Care Study Group, Multi-national Association
of Supportive Care in Cancer (MASCC)/International Society of Oral Oncology (ISOO). A
systematic review of dental disease in patients undergoing cancer therapy. Support Care
Cancer. 2010;(18):1007-21.
Huang S-H, O´sullivan B. Oral cancer: Current role of radiotherapy and chemotherapy. Med
Oral Patol Oral Cir Bucal Mar Mar Med Oral S L CIF B Med Oral Patol Oral Cir Bucal Mar.
2013;1181818(12):233–40.
Huber MA, Terezhalmy GT. The head and neck radiation oncology patient.Quintessence Int.
2003; 34 (9): 693–717.
Hutton MF, Patterson SS, Mitchell DF, et al. The effect of cobalt-60 radiation on the dental
pulps of monkeys. Oral Surg Oral Med Oral Pathol 1974;42:2581–90.
Instituto Nacional de Cancer José Alencar Gomes da Silva. Estimativa 2016 - Incidência de
Câncer no Brasil [Internet]. Ministério da Saúde Inst. Nac. Cancer José Alencar Gomes da
Silva. Rio de Janeiro; 2016; 124.
Recuperadode:http://www.inca.gov.br/estimativa/2016/estimativa-2016-v11.pdf

38
Kataoka SH, Setzer FC, Gondim-Junior E, Pessoa OF, Gavini G, Caldeira CL. Pulp vitality in
patients with intraoral and oropharyngeal malignant tumors undergoing radiation therapy
assessed by pulse oximetry. J Endod. 2011 Sep;37(9):1197-200
Kataoka SH, Setzer FC, Gondim-Junior E, Fregnani ER, Moraes CJ, Pessoa OF, Gavini G,
Caldeira CL. Late Effects of Head and Neck Radiotherapy on Pulp Vitality Assessed by Pulse
Oximetry. J Endod. 2016 Jun;42(6):886-9.
Kielbassa AM, Hinkelbein W, Hellwig E, Meyer-Lückel H. Radiation-related damage to
dentition. Lancet Oncol. 2006 Apr;7(4):326-35.
Knowles JC, Chalian VA, Shidnia H. Pulp innervation after radiation therapy. J Prosthet
Dent. 1986 Dec;56(6):708-11.
Lobo ALG, Martins G B. Consequências da radioterapia na região de cabeça e pescoço: uma
revisão de literatura. Revista Portuguesa de Estomatologia. 2009; 50( 4): 251-255.
Marta GN, William WN, Feher O, Carvalho AL, Kowalski LP. Induction chemotherapy for
oral cavity cancer patients: Current status and future perspectives. Oral Oncol. Elsevier Ltd;
2015;51(12):1069–75.
McGuire JD, Mousa AA, Zhang BJ, Todoki LS, Huffman NT, Chandrababu KB, et al.
Extracts of irradiated human tooth crowns contain MMP-20 protein and activity. J Dent.
2014; 42 (5): 626-35.
Meyer I, Shklar G, Turner J. A comparison of the effects of 200 kV radiation and cobalt-60
radiation on the jaws and dental structure of the white rat. A preliminary report. Oral Surg
Oral Med Oral Pathol. 1962;15: 1098-108.
Neville WD, Damm DD, Allen CM, Bouquot JE. Patologia Oral e Maxilo Facial, Quarta
Edição, 2016.
Pelucchi C, Gallus S, Garavello W, Bosetti C, La Vecchia C. Alcohol and tobacco use, and
cancer risk for upper aerodigestive tract and liver. Eur J Cancer Prev. 2008;17(4):340-4.
Pioch T, Golfels D, Staehle HJ. An experimental study of the stability of irradiated teeth in
the region of the dentino enamel junction. Endod Dent Traumatol. 1992;8:241-244.

39
Ribeiro AC, Silva AR, Simonato LE, Salzedas LM, Sundefeld ML, Soubhia AM. Clinical and
histopathological analysis of oral squamous cell carcinoma in young people: a descriptive
study in Brazilians. Br J Oral Maxillofac Surg. 2009;47(2):95-8.
Rodrigues PC, Miguel MC, Bagordakis E, et al. Clinicopathological prognostic factors of oral
tongue squamous cell carcinoma: a retrospective study of 202 cases. Int J Oral Maxillofac
Surg. 2014; 43(7): 795-801.
Rolim Ana Emília Holanda, Costa Lino João da, Ramalho Luciana Maria Pedreira.
Repercussões da radioterapia na região orofacial e seu tratamento. Radiol Bras [Internet].
2011 Dec [cited 2017 Mar 01] ; 44( 6 ): 388-395.
Seiwert TY, Salama JK, Vokes EE. The chemoradiation paradigm in head and neck cancer.
Nat Clin Pract Oncol. 2007; 4 (3): 156-71.
Sciubba JJ, Goldenberg D. Oral complications of radiotherapy. Lancet Oncol. 2006; 7 (2):
175-83.
Silva ARS, Alves FA, Antunes A, Goes MF, Lopes MA. Patterns of Demineralization and
Dentin Reactions in Radiation-Related Caries. Caries Research 2009;43:43-9.
Sloan P, Gale N, Hunter K, Lingen MW, Nylander K, Reibel J, et al. Malignant surface
epithelial tumours. In: El-Naggar AK, Chan JK, Grandis Jennifer R, Takata T, Slootweg PJ,
organizers. WHO Classif Head Neck Tumours. Fourth. 2017;109–11.
Schweyen, R., Hey, J., Fränzel, W. et al. Strahlenther Onkol. 2012; 188 - 21.
Springer IN, Niehoff P, Warnke PH, Bocek G, Kovács G, Suhr M, Wiltfang J, Açil Y:
Radiation caries – radiogenic destruction of dental collagen. Oral Oncol 2005; 41:723–728.
Vier-Pelisser FV, Figueiredo MAZ, Cherubini K, Braga-Filho A, Figueiredo JA. The effect of
head-fractioned teletherapy on pulp tissue. Int Endod J. 2007;40: 859–65.
Vissink A, Jansma J, Spijkervet FK, Burlage FR, Coppes RP. Oral sequelae of head and neck
radiotherapy. Crit Rev Oral Biol Med. 2003;14(3):199-212.

40
ANEXOS
Anexo 1 – Parecer Consubstanciado do CEP

41
Anexo 2 - Certificado de submissão ao periódico