Embed Size (px)
Citation preview

Alzheimerkrankheit – Ursachen, Diagnostik und Behandlungsmöglichkeiten
Linz, 2017
Alzheimer Austria
Prim. Dr. Andreas Winkler, MSc
Facharzt für Neurologie & Geriatrie
Ärztlicher Direktor der Klinik Pirawarth
Vorstand der Abteilung für Neurologische Rehabilitation
Vizepräsident Alzheimer Austria
Klinik Pirawarth
Neurologische Rehabilitation
Orthopädische Rehabilitation
Psychosomatische Rehabilitation
Klinik Pirawarth
Neurologische Rehabilitation
Orthopädische Rehabilitation
Psychosomatische Rehabilitation
Herausforderung Demenz
• 46 Millionen weltweit (WHO 2015) und 130.000 Menschen in Österreich
leiden an einer Demenzerkrankung
• Weitere 500.000 Personen in Österreich zeigen Symptome einer leichten
kognitiven Beeinträchtigung (MCI)
• Zahl der Demenzpatienten wird sich bis 2050 auf bis zu 270.000 erhöhen
• Alzheimer ist die häufigste Ursache einer Demenz (~ 70 %)
• Ist die häufigste Einzelursache für Pflegebedürftigkeit im Alter
• Ist die häufigste und folgenschwerste Erkrankung im höheren
Lebensalter
• Demenz ist eine vorzeitig zum Tod führende Erkrankung (3-4 fach
erhöhte Mortalität)
WHO 2015
Alzheimer Austria 2013
BD James et al., Neurology 2014
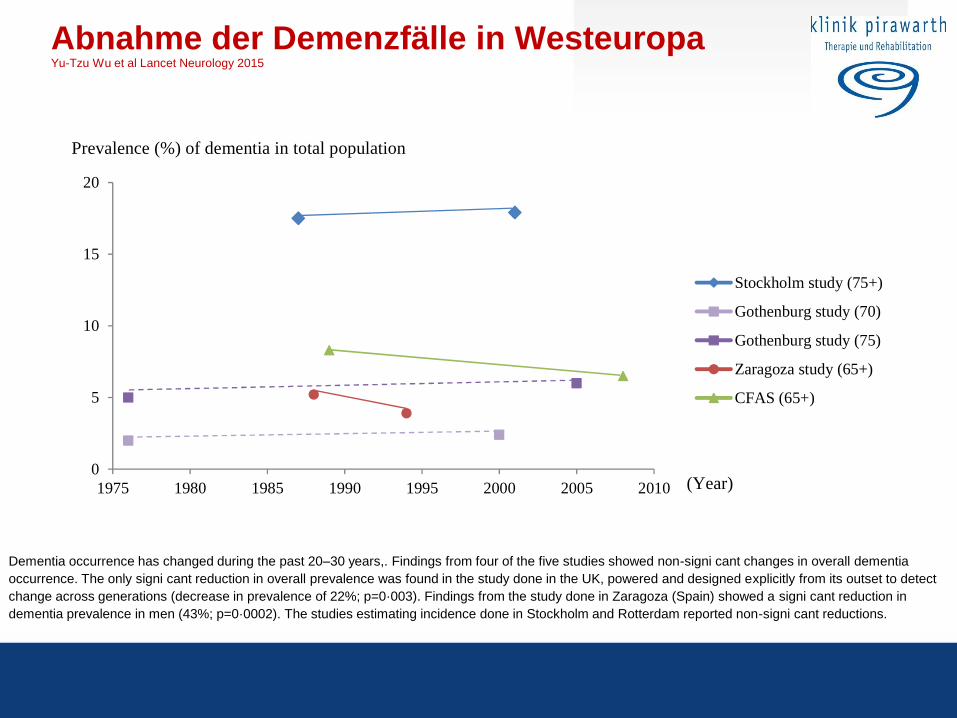
Abnahme der Demenzfälle in Westeuropa Yu-Tzu Wu et al Lancet Neurology 2015
Dementia occurrence has changed during the past 20–30 years,. Findings from four of the five studies showed non-signi cant changes in overall dementia
occurrence. The only signi cant reduction in overall prevalence was found in the study done in the UK, powered and designed explicitly from its outset to detect
change across generations (decrease in prevalence of 22%; p=0·003). Findings from the study done in Zaragoza (Spain) showed a signi cant reduction in
dementia prevalence in men (43%; p=0·0002). The studies estimating incidence done in Stockholm and Rotterdam reported non-signi cant reductions.
Figure 3 Age-adjusted prevalence of dementia by the year of investigation
Prevalence (%) of dementia in total population
Prevalence (%) of dementia in men
Prevalence (%) of dementia in women
0
5
10
15
20
1975 1980 1985 1990 1995 2000 2005 2010
Stockholm study (75+)
Gothenburg study (70)
Gothenburg study (75)
Zaragoza study (65+)
CFAS (65+)
0
5
10
15
20
1975 1980 1985 1990 1995 2000 2005 2010
Stockholm study (75+)
Gothenburg study (70)
Gothenburg study (75)
Zaragoza study (65+)
CFAS (65+)
0
5
10
15
20
1975 1980 1985 1990 1995 2000 2005 2010
Stockholm study (75+)
Gothenburg study (70)
Gothenburg study (75)
Zaragoza study (65+)
CFAS (65+)
(Year)
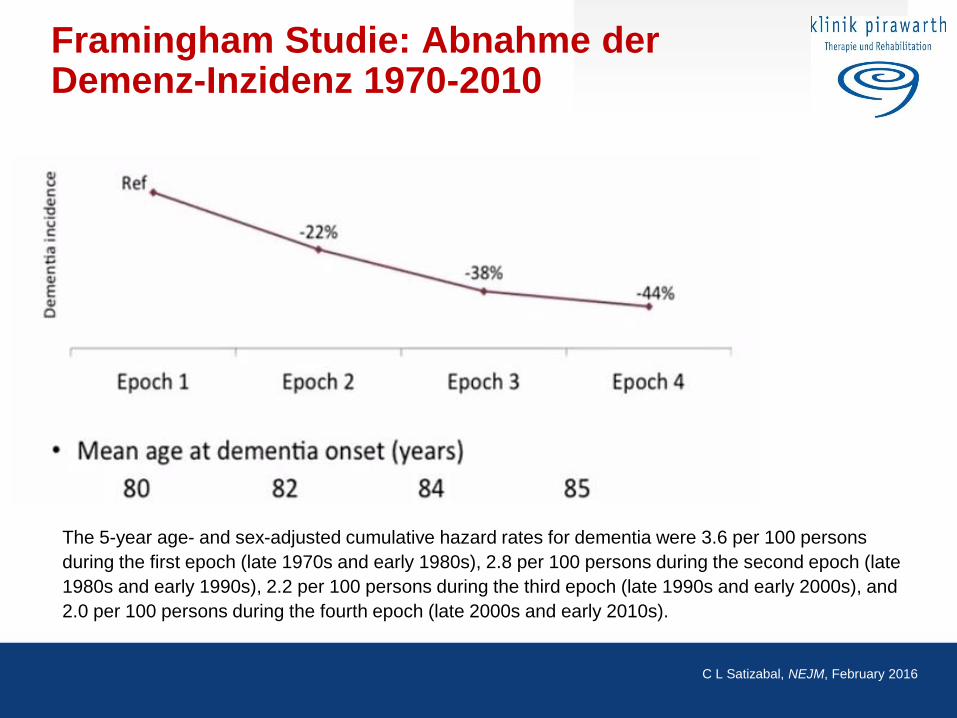
Framingham Studie: Abnahme der Demenz-Inzidenz 1970-2010
The 5-year age- and sex-adjusted cumulative hazard rates for dementia were 3.6 per 100 persons
during the first epoch (late 1970s and early 1980s), 2.8 per 100 persons during the second epoch (late
1980s and early 1990s), 2.2 per 100 persons during the third epoch (late 1990s and early 2000s), and
2.0 per 100 persons during the fourth epoch (late 2000s and early 2010s).
C L Satizabal, NEJM, February 2016
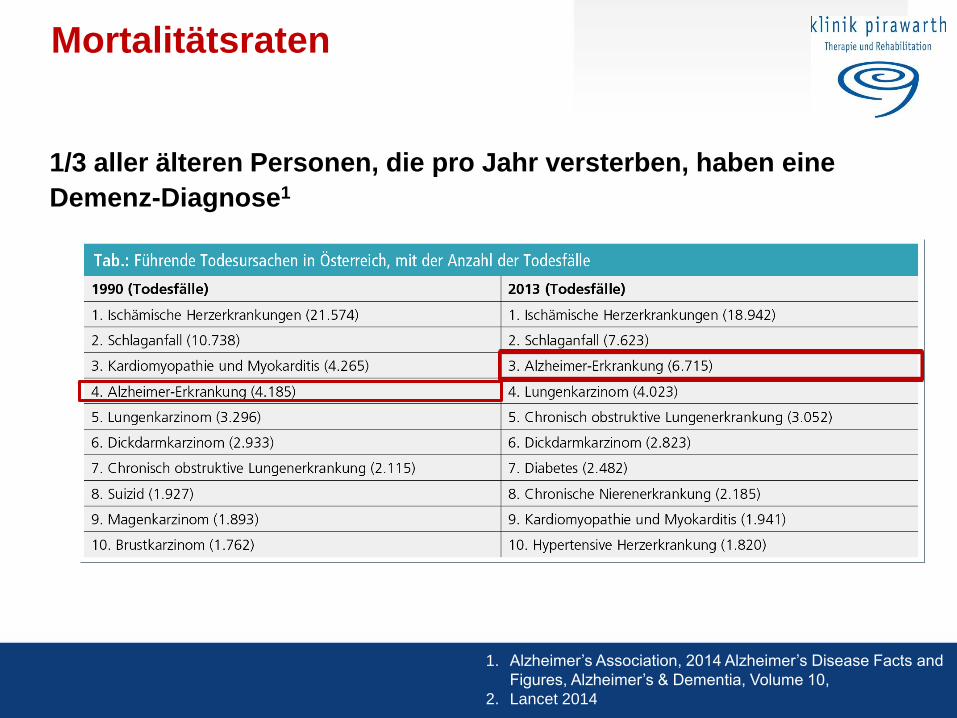
Mortalitätsraten
1/3 aller älteren Personen, die pro Jahr versterben, haben eine
Demenz-Diagnose1
1. Alzheimer’s Association, 2014 Alzheimer’s Disease Facts and
Figures, Alzheimer’s & Dementia, Volume 10,
2. Lancet 2014
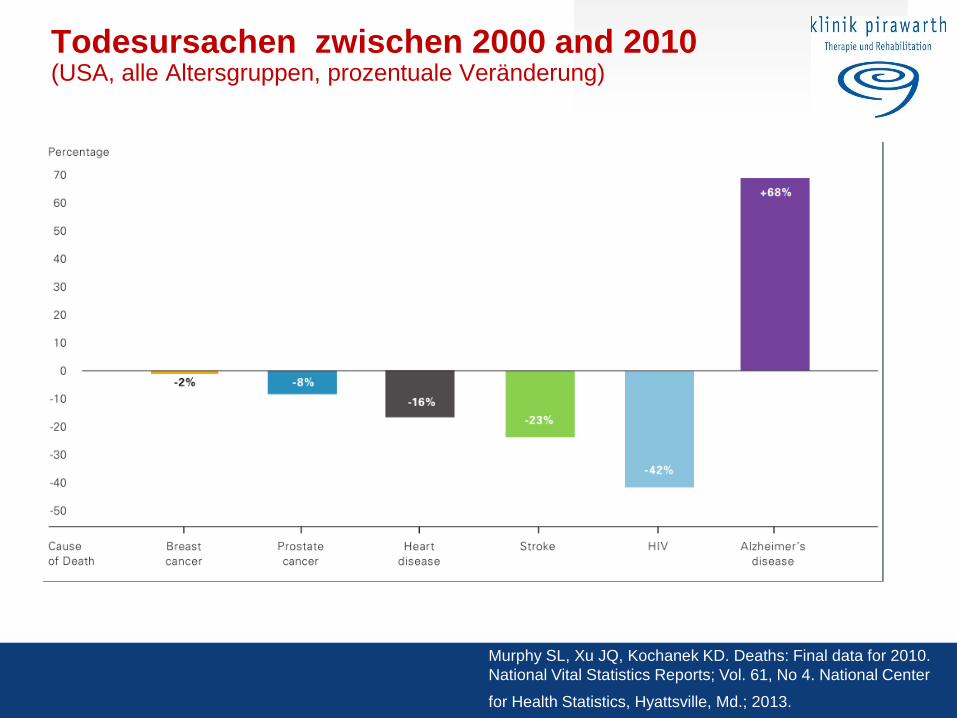
Todesursachen zwischen 2000 and 2010 (USA, alle Altersgruppen, prozentuale Veränderung)
Murphy SL, Xu JQ, Kochanek KD. Deaths: Final data for 2010.
National Vital Statistics Reports; Vol. 61, No 4. National Center
for Health Statistics, Hyattsville, Md.; 2013.
Herausforderung Demenz
Alzheimer EUROPE:
• Ein zunehmender Mangel an Demenz-Spezialisten gefährdet
Forschungsfortschritt
• 5x mehr Wissenschafter entscheiden sich für onkologische
Themen als für Demenz
• 70% aller Demenz-Experten (mit PhD) verlassen das Forschungsgebiet
innerhalb von 4 Jahren
• Es besteht bereits heute ein kritischer Mangel an spezialisierten
Pflegfachkräften und Experten mit Demenz-Schwerpunkt
S. Marjanovic et al.; 2015; http://www.alzheimers.org.uk/researchreport2015
Alzheimerkrankheit - Demenz Vergesslichkeit - Alzheimer
Obst
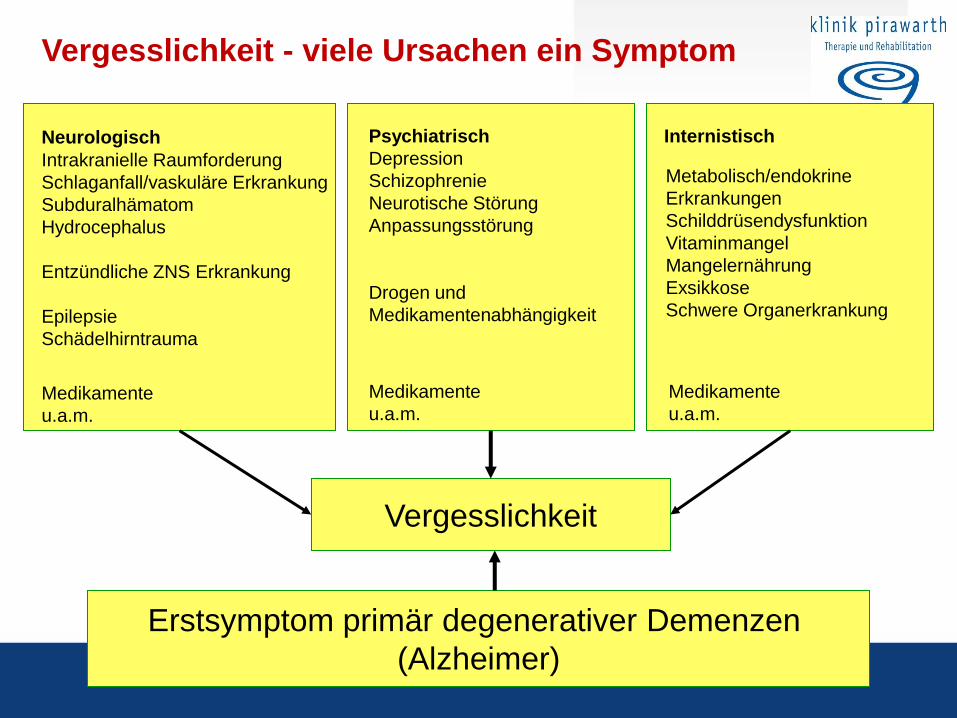
Neurologisch Psychiatrisch
Depression
Schizophrenie
Neurotische Störung
Anpassungsstörung
Drogen und
Medikamentenabhängigkeit
Internistisch
Vergesslichkeit - viele Ursachen ein Symptom
Erstsymptom primär degenerativer Demenzen
(Alzheimer)
Vergesslichkeit
Intrakranielle Raumforderung
Schlaganfall/vaskuläre Erkrankung
Subduralhämatom
Hydrocephalus
Entzündliche ZNS Erkrankung
Epilepsie
Schädelhirntrauma
Metabolisch/endokrine
Erkrankungen
Schilddrüsendysfunktion
Vitaminmangel
Mangelernährung
Exsikkose
Schwere Organerkrankung
Medikamente
u.a.m.
Medikamente
u.a.m.
Medikamente
u.a.m.
20
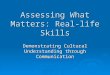
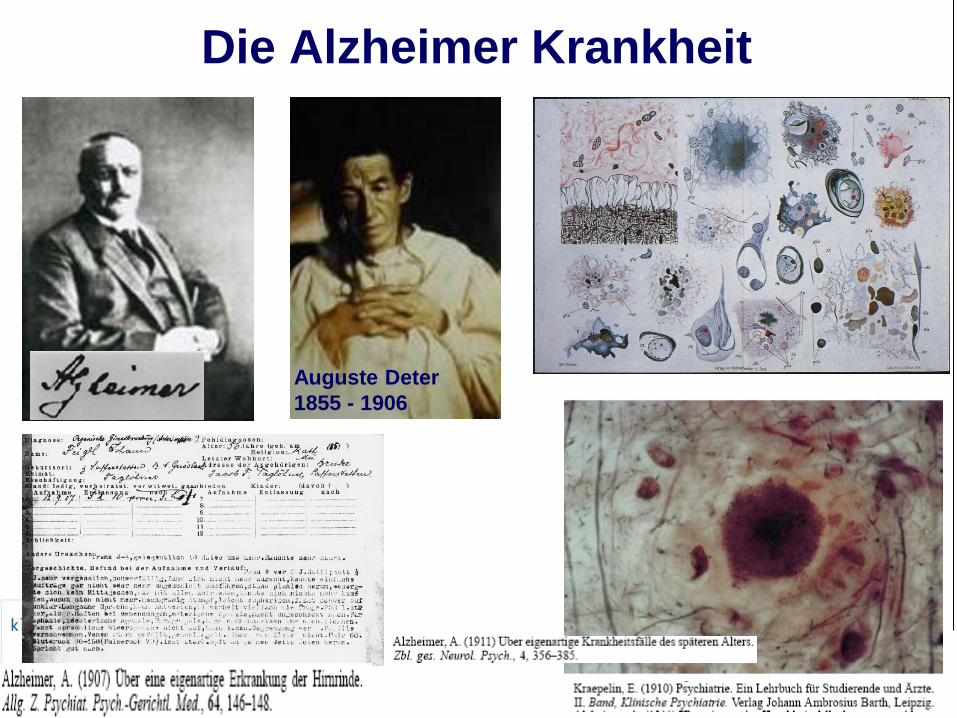
Die Alzheimer Krankheit
Auguste Deter
1855 - 1906
22
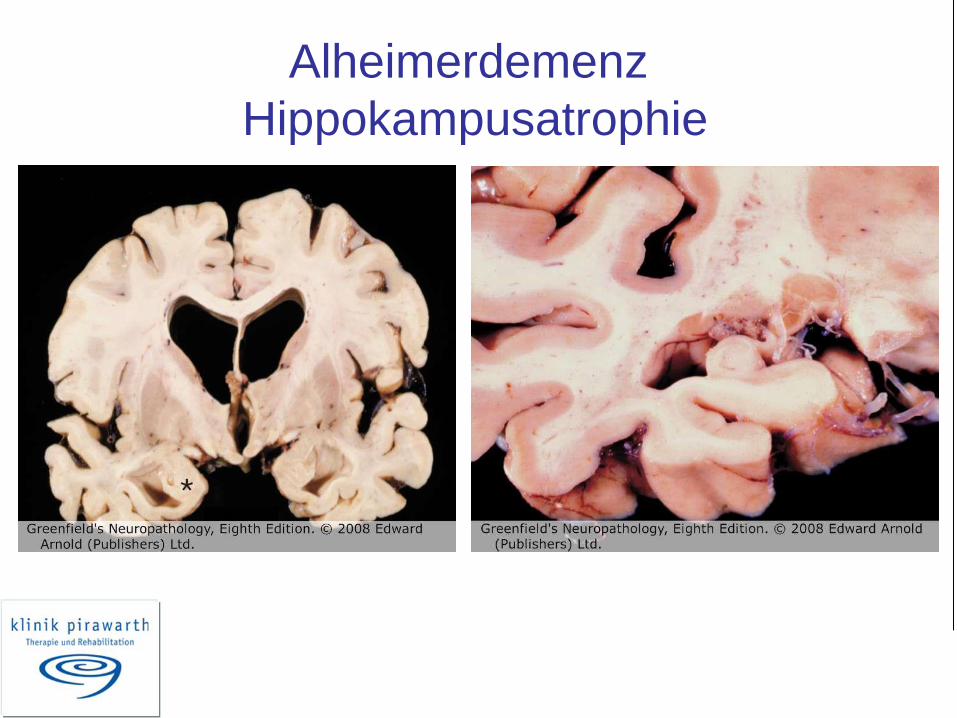
Alheimerdemenz
Hippokampusatrophie
23
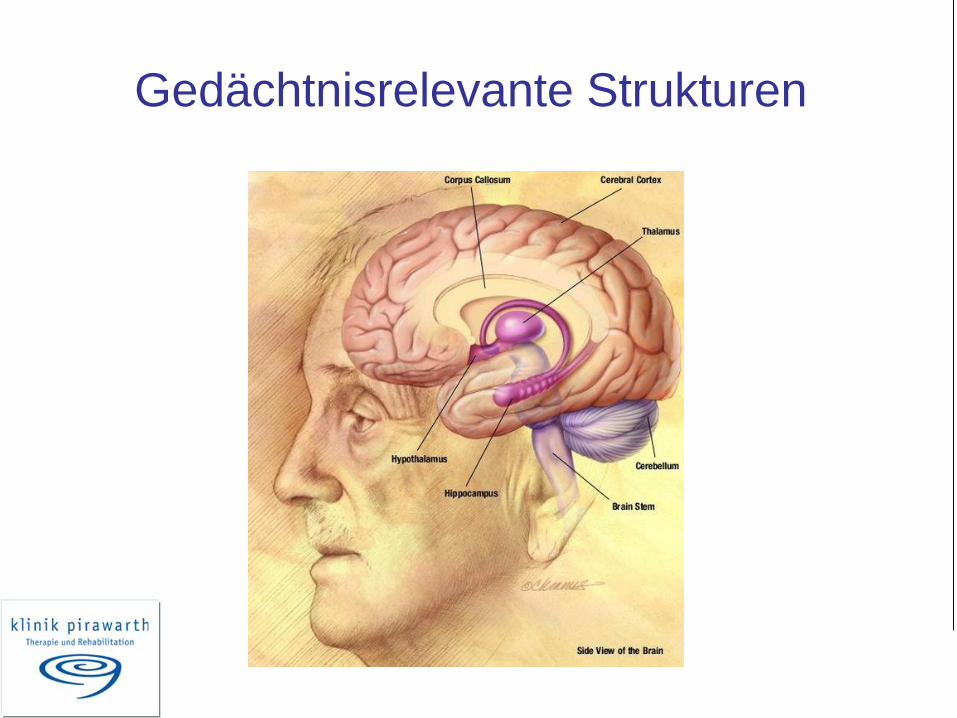
Gedächtnisrelevante Strukturen
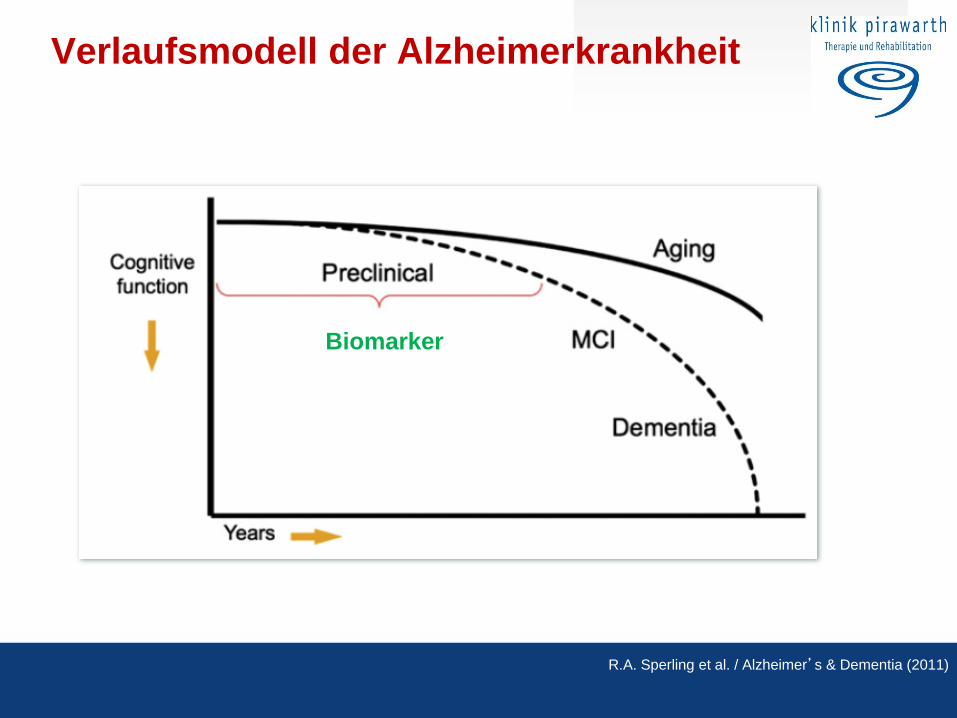
Verlaufsmodell der Alzheimerkrankheit
R.A. Sperling et al. / Alzheimer’s & Dementia (2011)
Biomarker
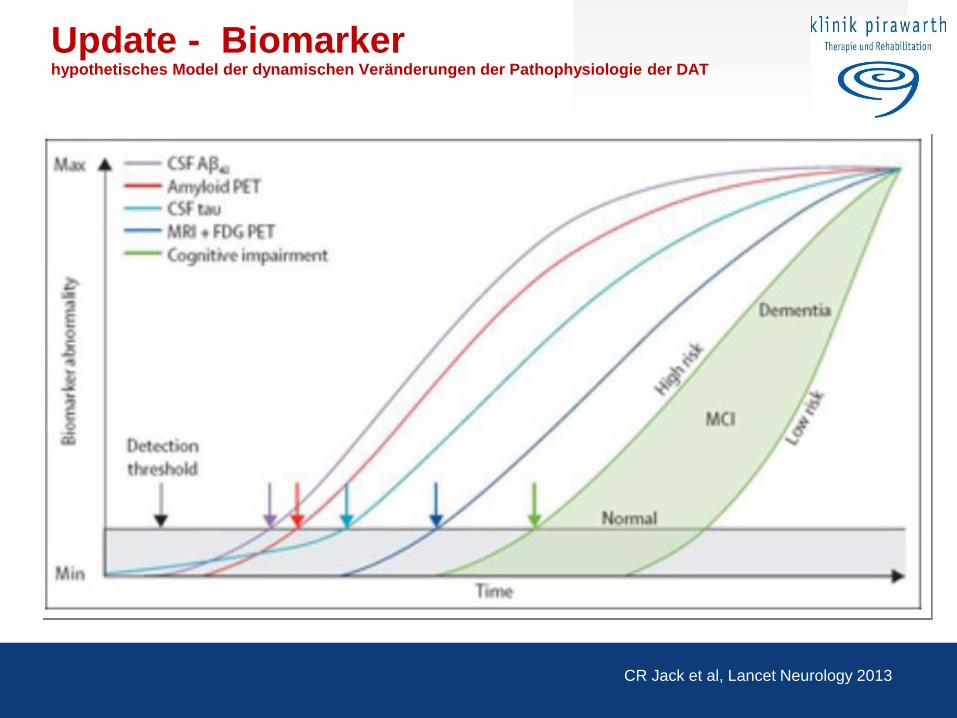
Update - Biomarker hypothetisches Model der dynamischen Veränderungen der Pathophysiologie der DAT
CR Jack et al, Lancet Neurology 2013
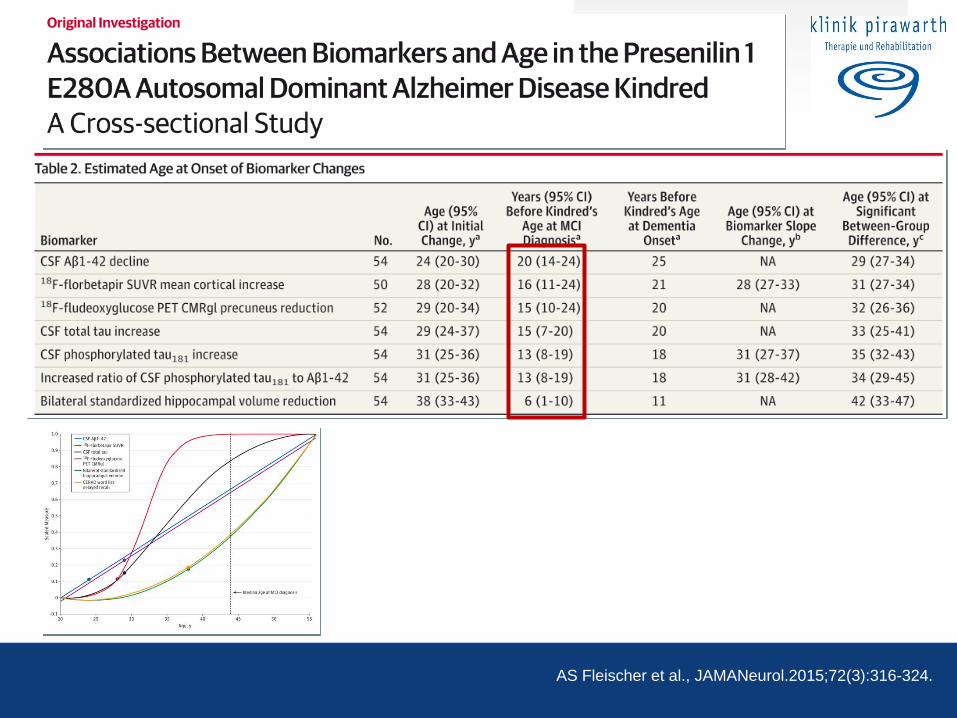
AS Fleischer et al., JAMANeurol.2015;72(3):316-324.
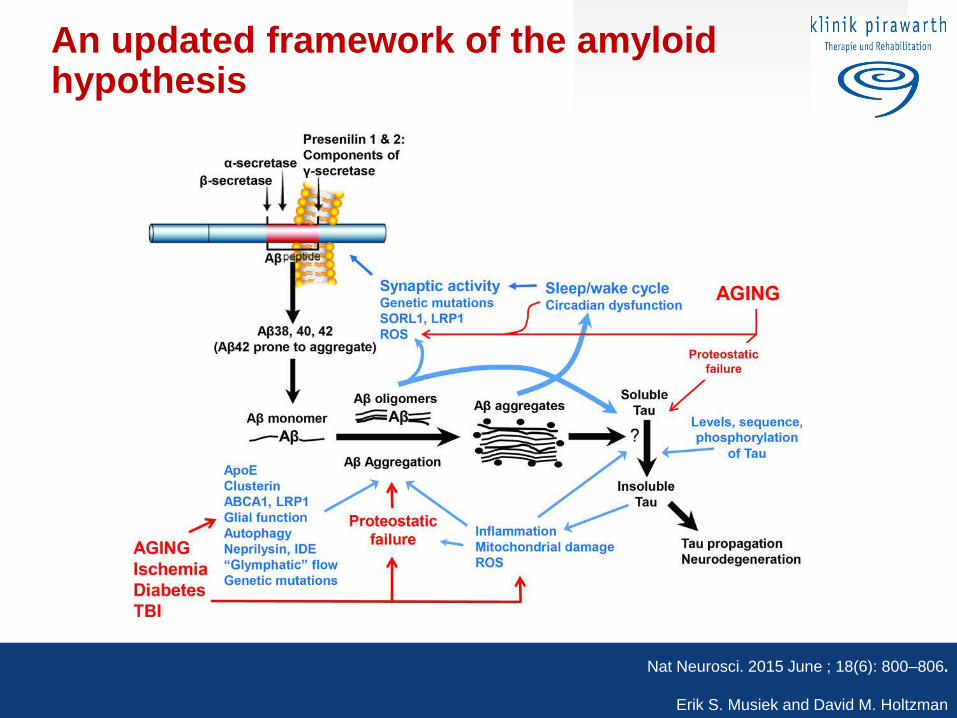
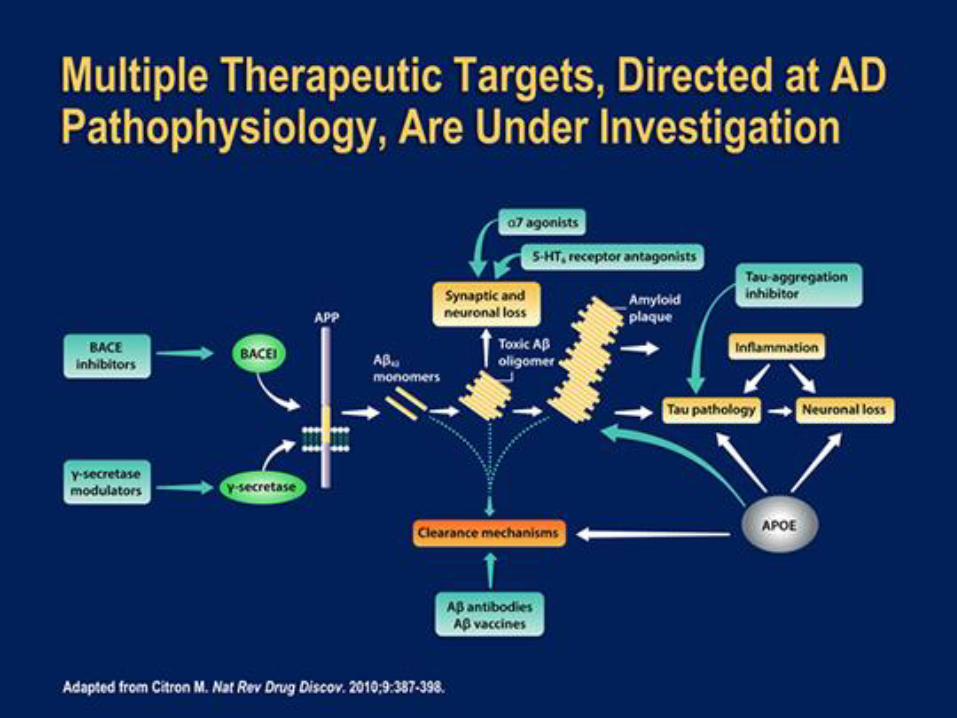
An updated framework of the amyloid hypothesis
Nat Neurosci. 2015 June ; 18(6): 800–806.
Erik S. Musiek and David M. Holtzman
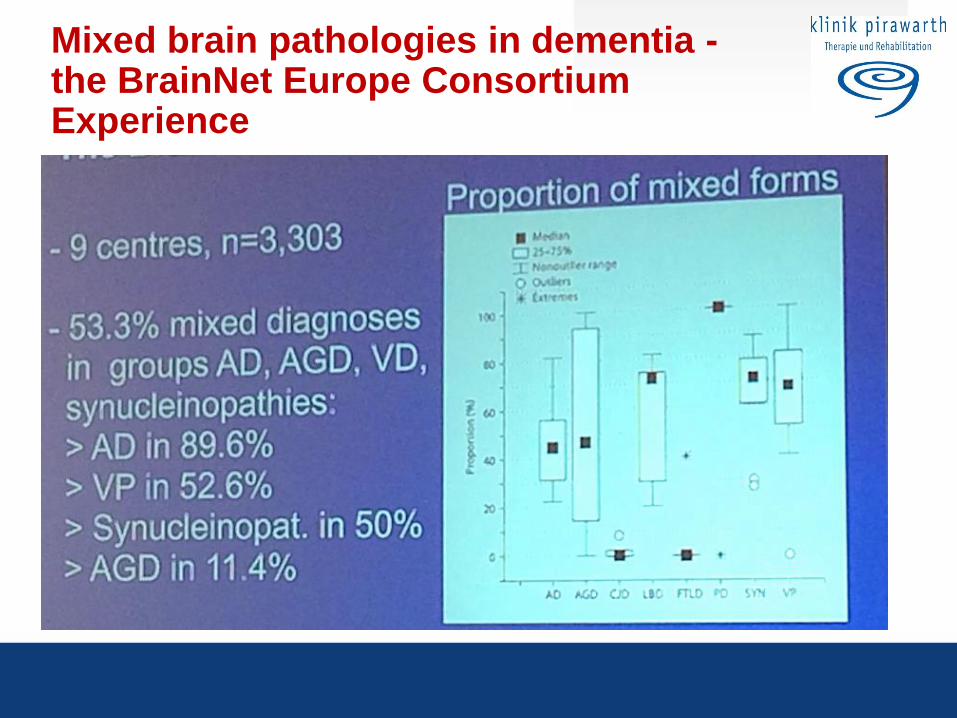
Mixed brain pathologies in dementia - the BrainNet Europe Consortium Experience
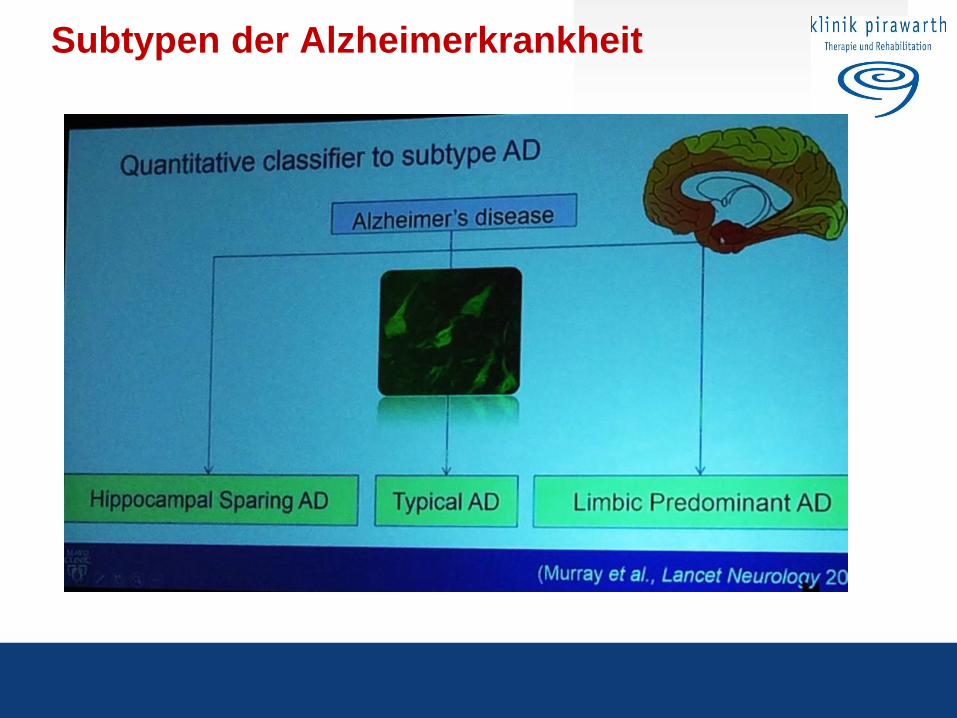
Subtypen der Alzheimerkrankheit
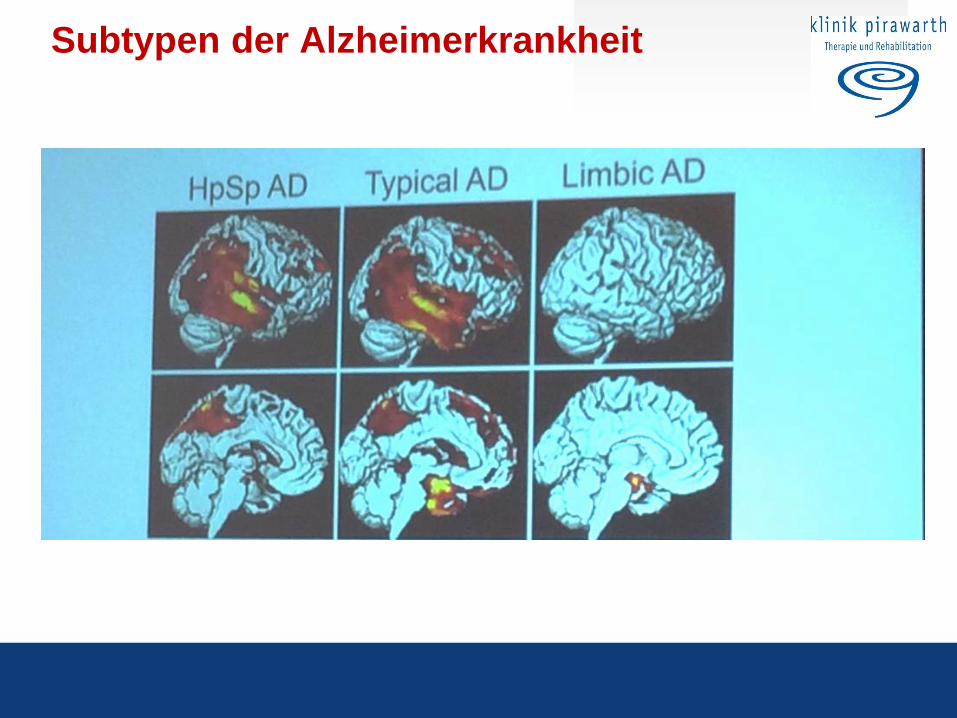
Subtypen der Alzheimerkrankheit
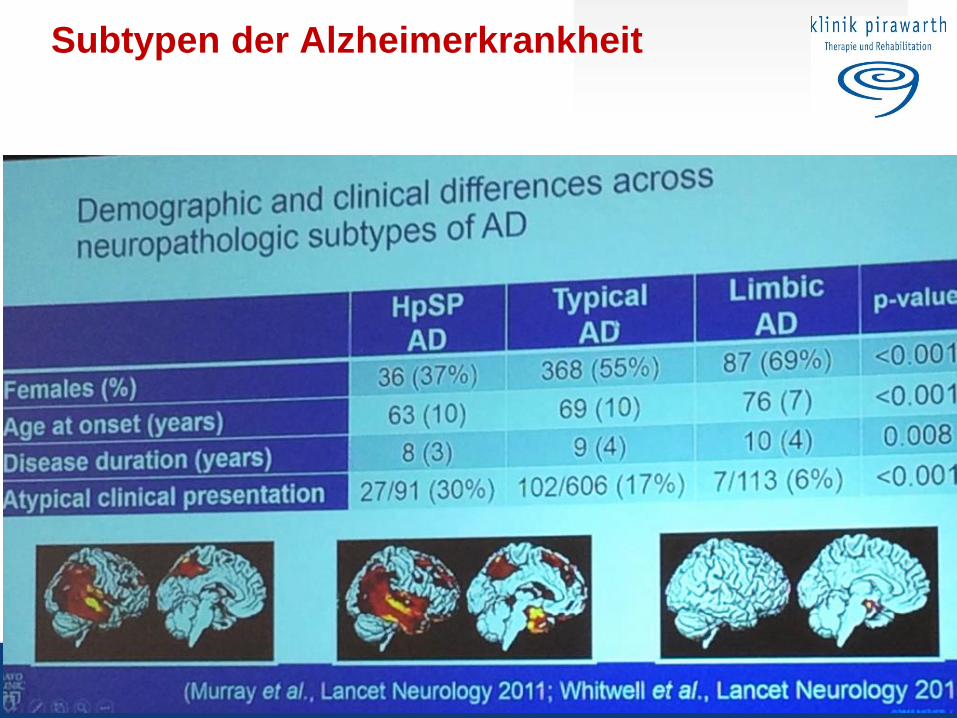
Subtypen der Alzheimerkrankheit
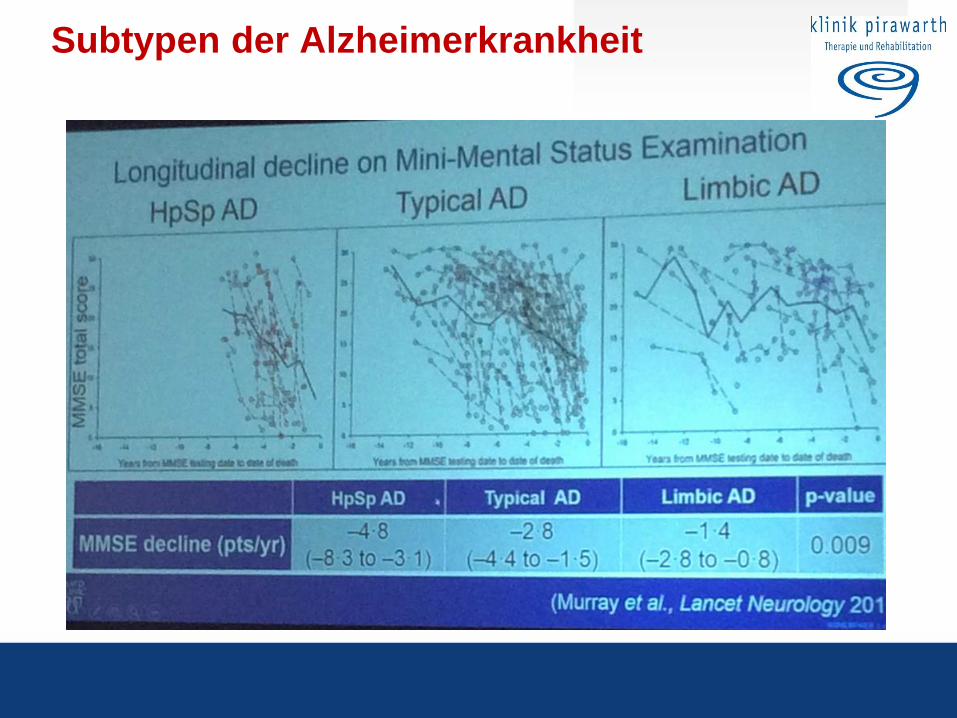
Subtypen der Alzheimerkrankheit
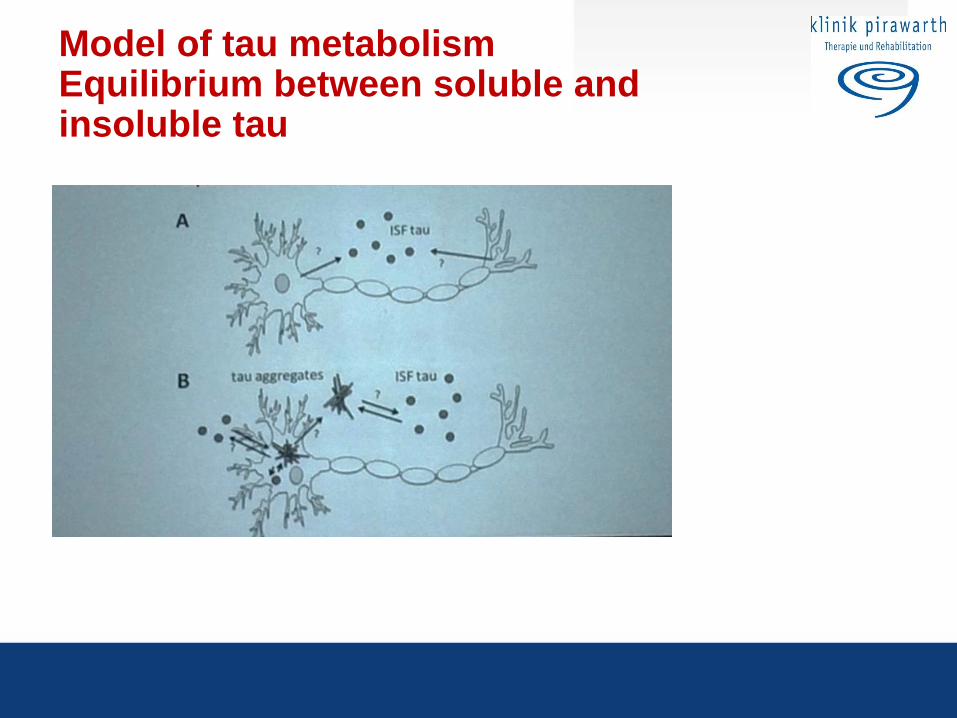
Model of tau metabolism Equilibrium between soluble and insoluble tau
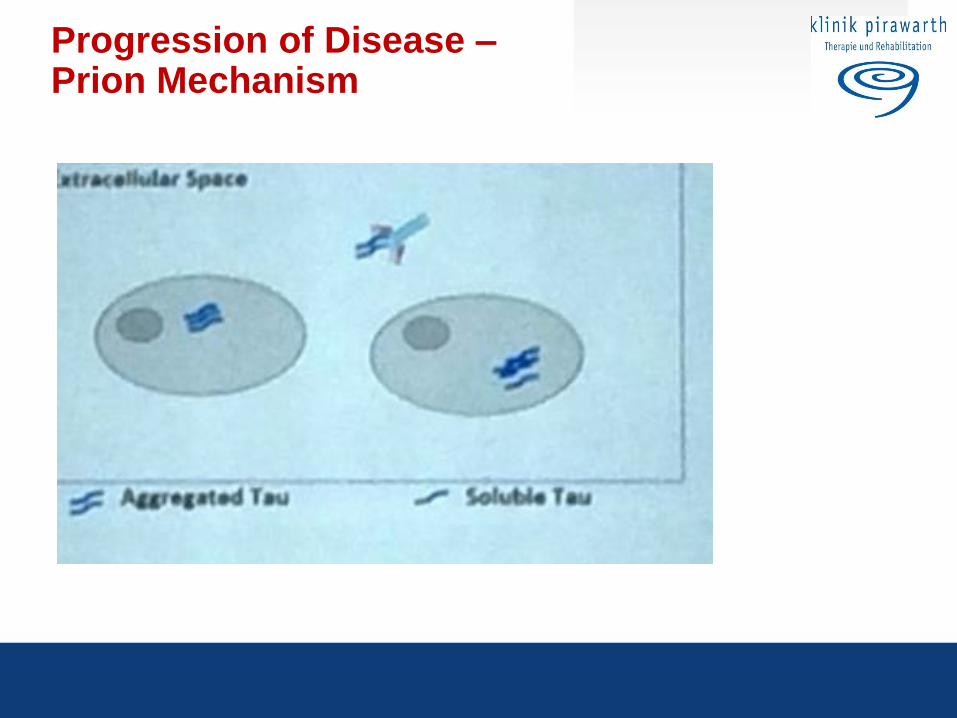
Progression of Disease – Prion Mechanism
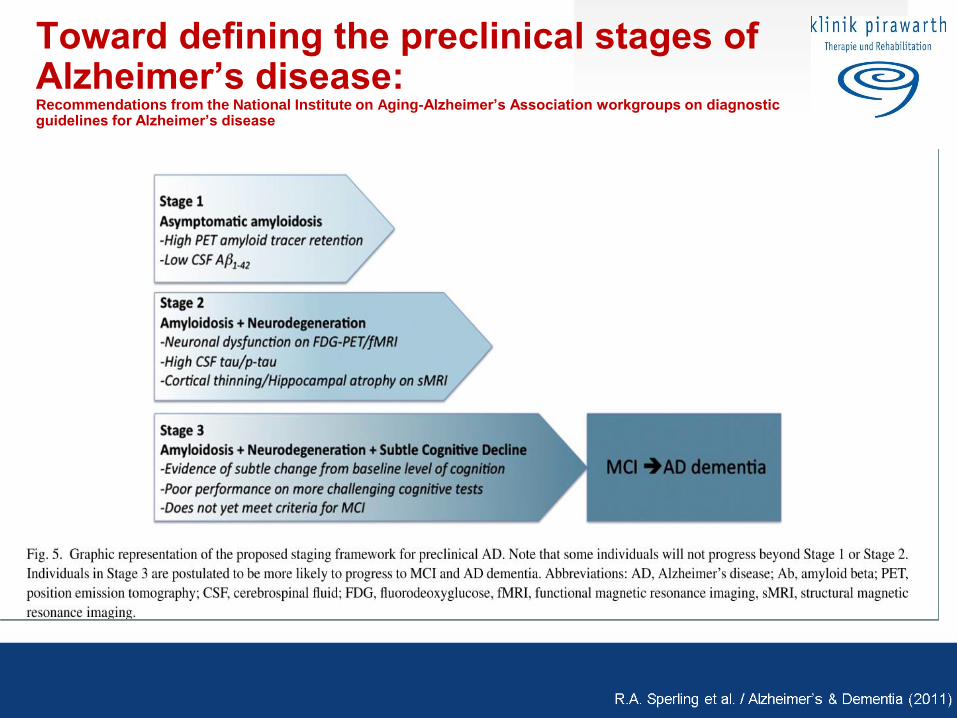
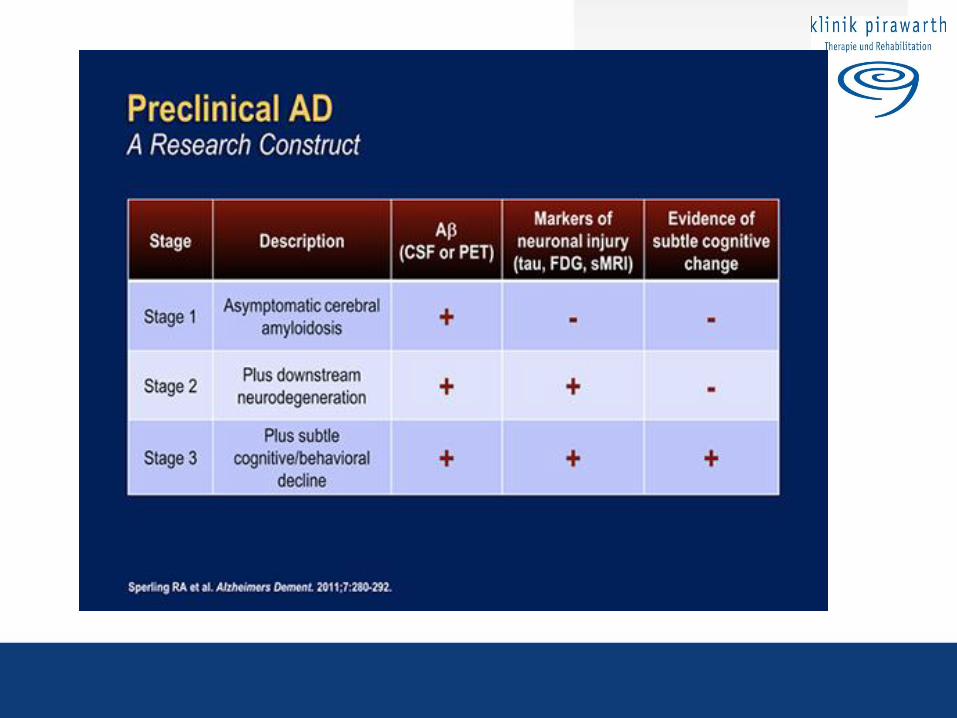
Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease
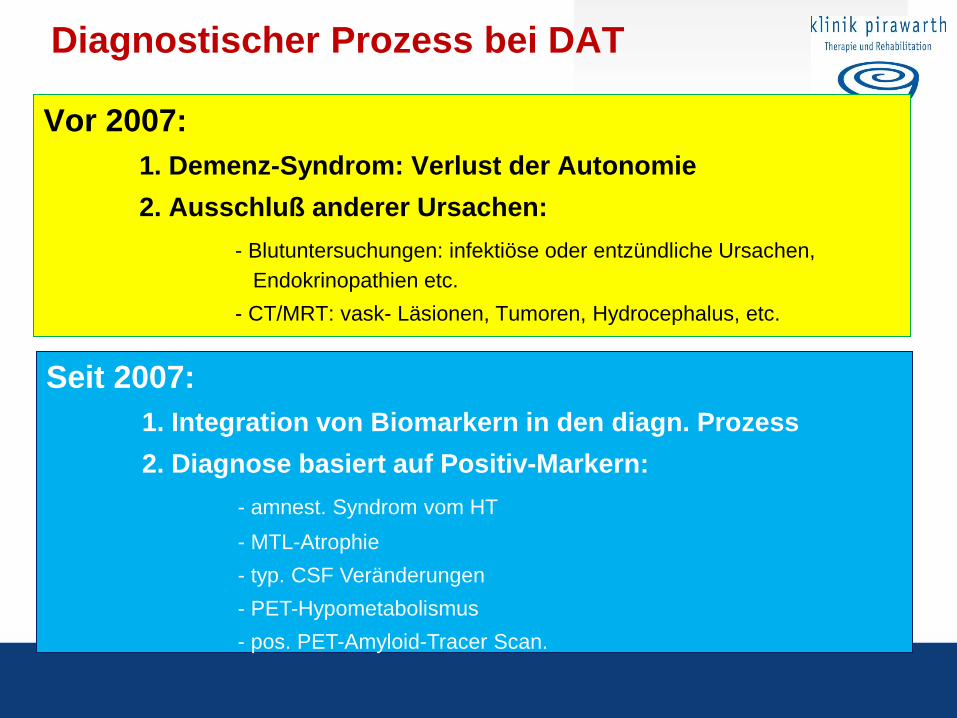
Diagnostischer Prozess bei DAT
Vor 2007:
1. Demenz-Syndrom: Verlust der Autonomie
2. Ausschluß anderer Ursachen:
- Blutuntersuchungen: infektiöse oder entzündliche Ursachen,
Endokrinopathien etc.
- CT/MRT: vask- Läsionen, Tumoren, Hydrocephalus, etc.
Seit 2007:
1. Integration von Biomarkern in den diagn. Prozess
2. Diagnose basiert auf Positiv-Markern:
- amnest. Syndrom vom HT
- MTL-Atrophie
- typ. CSF Veränderungen
- PET-Hypometabolismus
- pos. PET-Amyloid-Tracer Scan.
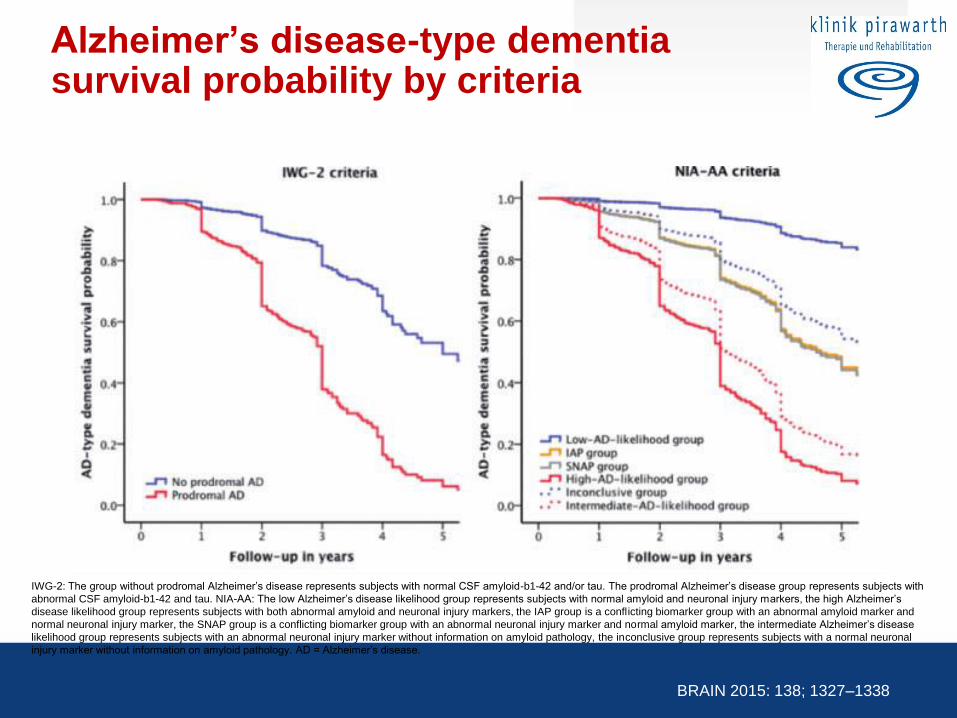
Alzheimer’s disease-type dementia survival probability by criteria
IWG-2: The group without prodromal Alzheimer’s disease represents subjects with normal CSF amyloid-b1-42 and/or tau. The prodromal Alzheimer’s disease group represents subjects with
abnormal CSF amyloid-b1-42 and tau. NIA-AA: The low Alzheimer’s disease likelihood group represents subjects with normal amyloid and neuronal injury markers, the high Alzheimer’s
disease likelihood group represents subjects with both abnormal amyloid and neuronal injury markers, the IAP group is a conflicting biomarker group with an abnormal amyloid marker and
normal neuronal injury marker, the SNAP group is a conflicting biomarker group with an abnormal neuronal injury marker and normal amyloid marker, the intermediate Alzheimer’s disease
likelihood group represents subjects with an abnormal neuronal injury marker without information on amyloid pathology, the inconclusive group represents subjects with a normal neuronal
injury marker without information on amyloid pathology. AD = Alzheimer’s disease.
BRAIN 2015: 138; 1327–1338
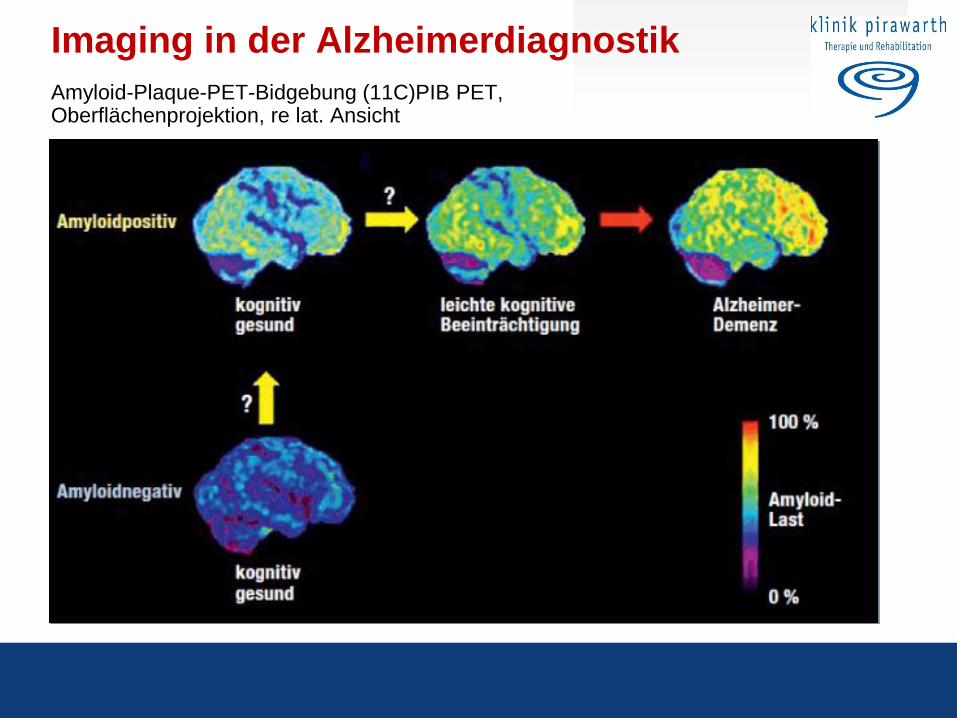
Imaging in der Alzheimerdiagnostik
Amyloid-Plaque-PET-Bidgebung (11C)PIB PET, Oberflächenprojektion, re lat. Ansicht
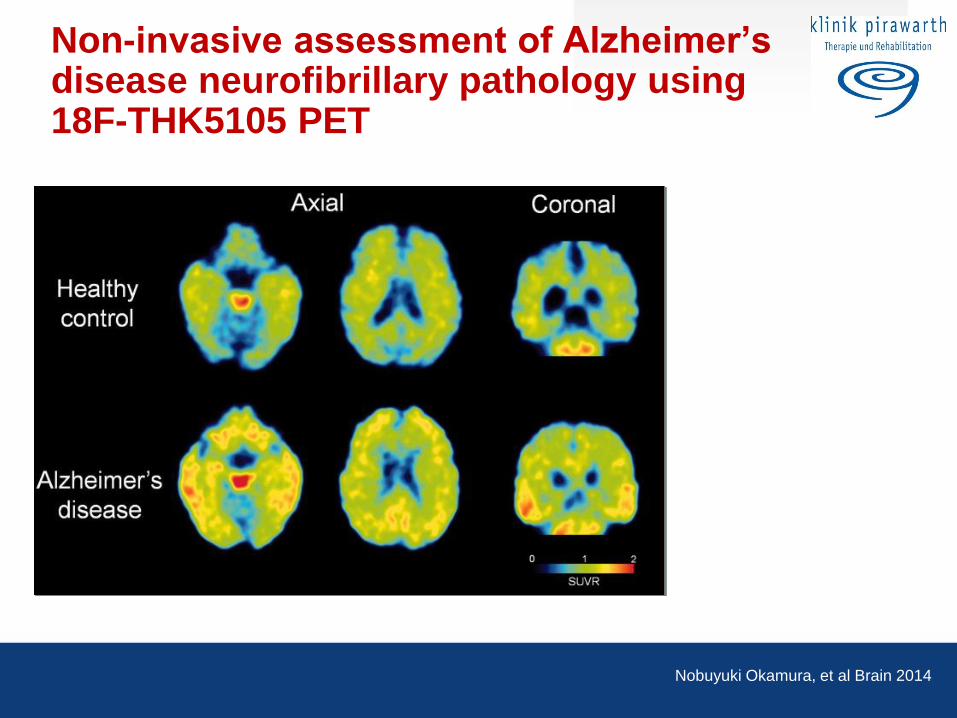
Non-invasive assessment of Alzheimer’s disease neurofibrillary pathology using 18F-THK5105 PET
Nobuyuki Okamura, et al Brain 2014
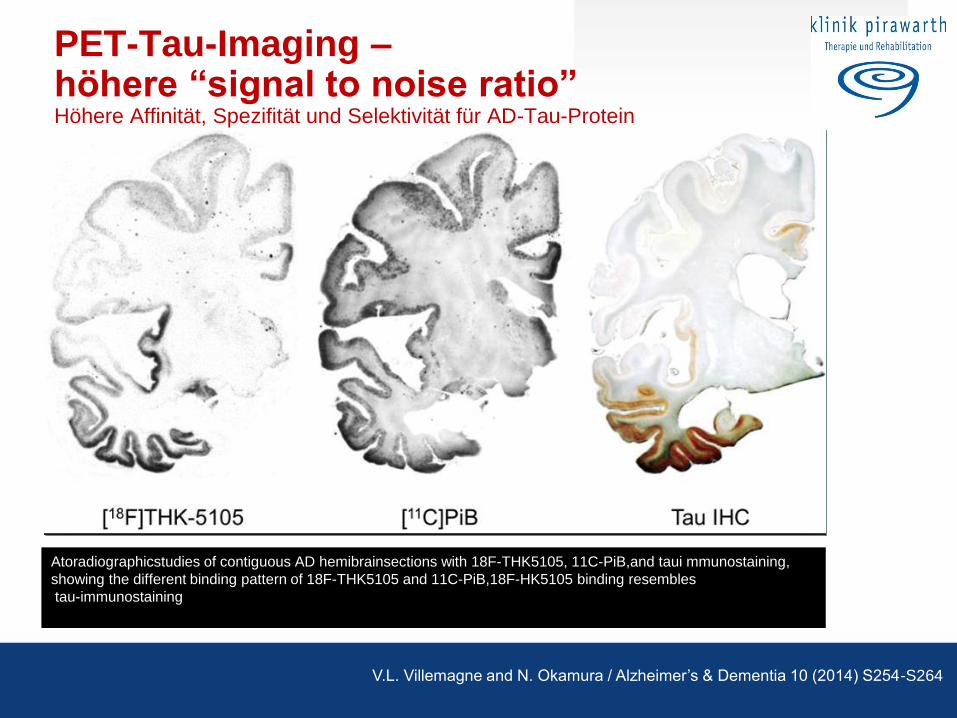
PET-Tau-Imaging – höhere “signal to noise ratio” Höhere Affinität, Spezifität und Selektivität für AD-Tau-Protein
Atoradiographicstudies of contiguous AD hemibrainsections with 18F-THK5105, 11C-PiB,and taui mmunostaining,
showing the different binding pattern of 18F-THK5105 and 11C-PiB,18F-HK5105 binding resembles
tau-immunostaining
V.L. Villemagne and N. Okamura / Alzheimer’s & Dementia 10 (2014) S254-S264
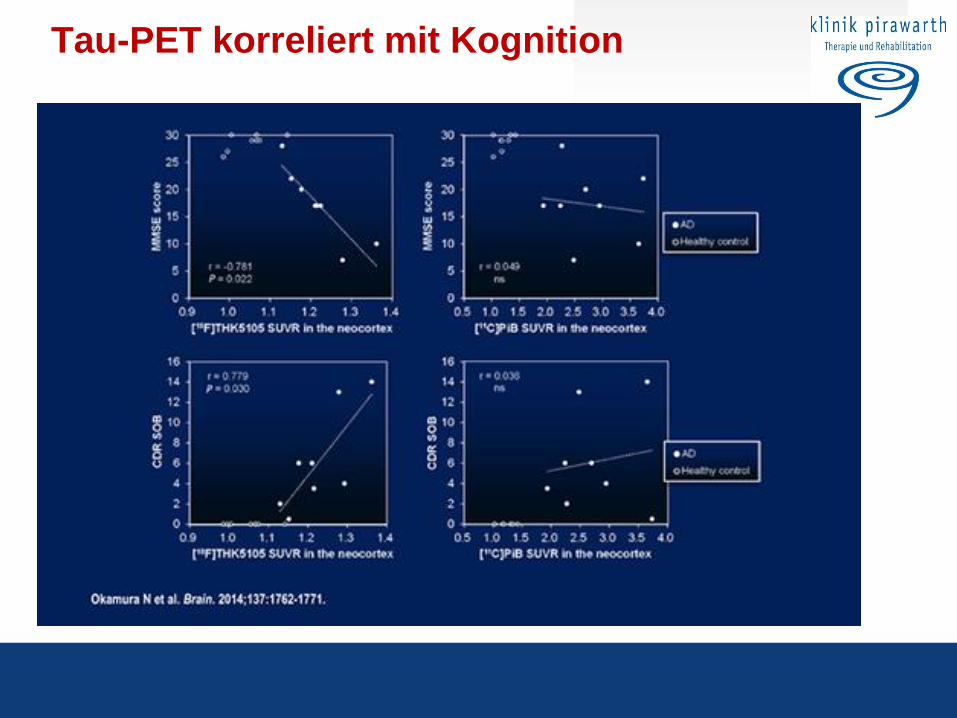
Tau-PET korreliert mit Kognition
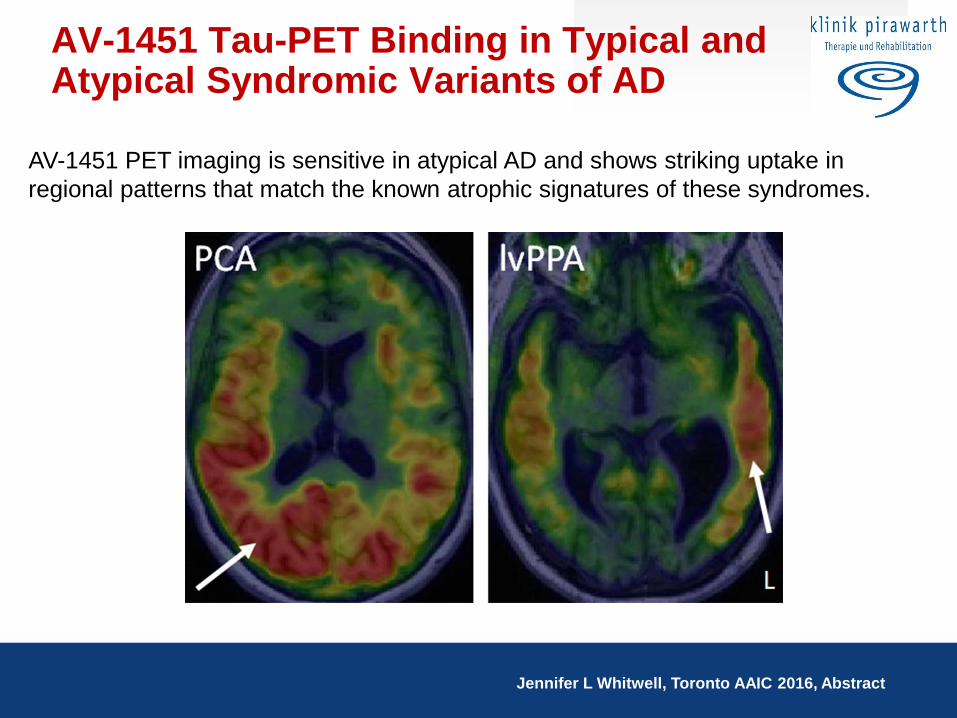
AV-1451 Tau-PET Binding in Typical and Atypical Syndromic Variants of AD
AV-1451 PET imaging is sensitive in atypical AD and shows striking uptake in
regional patterns that match the known atrophic signatures of these syndromes.
Jennifer L Whitwell, Toronto AAIC 2016, Abstract
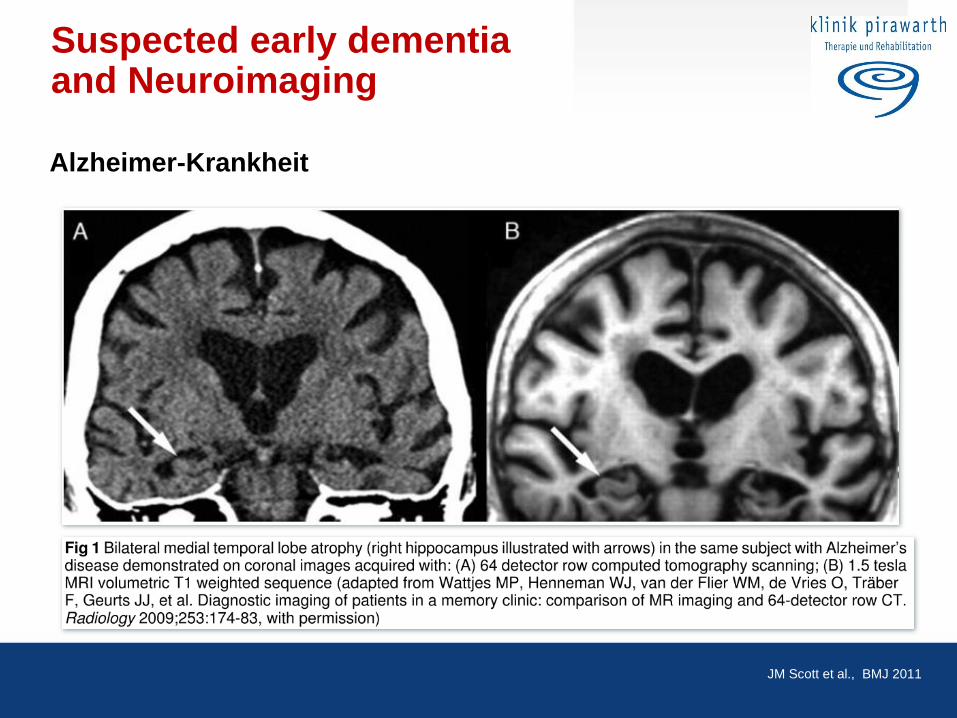
Suspected early dementia and Neuroimaging
Alzheimer-Krankheit
JM Scott et al., BMJ 2011
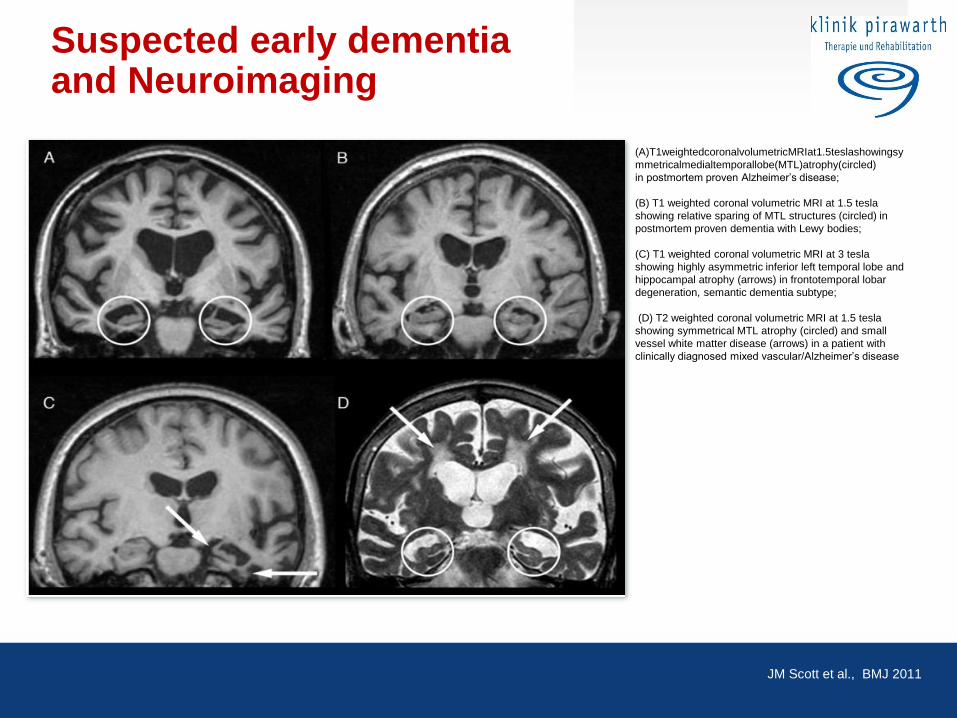
Suspected early dementia and Neuroimaging
JM Scott et al., BMJ 2011
(A)T1weightedcoronalvolumetricMRIat1.5teslashowingsy
mmetricalmedialtemporallobe(MTL)atrophy(circled)
in postmortem proven Alzheimer’s disease;
(B) T1 weighted coronal volumetric MRI at 1.5 tesla
showing relative sparing of MTL structures (circled) in
postmortem proven dementia with Lewy bodies;
(C) T1 weighted coronal volumetric MRI at 3 tesla
showing highly asymmetric inferior left temporal lobe and
hippocampal atrophy (arrows) in frontotemporal lobar
degeneration, semantic dementia subtype;
(D) T2 weighted coronal volumetric MRI at 1.5 tesla
showing symmetrical MTL atrophy (circled) and small
vessel white matter disease (arrows) in a patient with
clinically diagnosed mixed vascular/Alzheimer’s disease
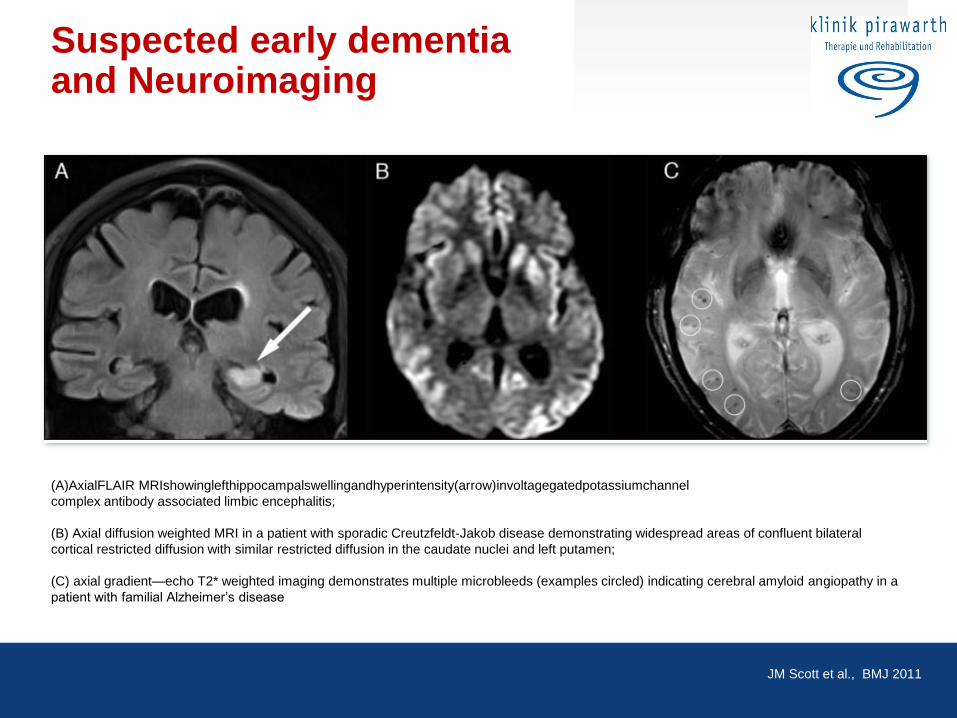
Suspected early dementia and Neuroimaging
JM Scott et al., BMJ 2011
(A)AxialFLAIR MRIshowinglefthippocampalswellingandhyperintensity(arrow)involtagegatedpotassiumchannel
complex antibody associated limbic encephalitis;
(B) Axial diffusion weighted MRI in a patient with sporadic Creutzfeldt-Jakob disease demonstrating widespread areas of confluent bilateral
cortical restricted diffusion with similar restricted diffusion in the caudate nuclei and left putamen;
(C) axial gradient—echo T2* weighted imaging demonstrates multiple microbleeds (examples circled) indicating cerebral amyloid angiopathy in a
patient with familial Alzheimer’s disease
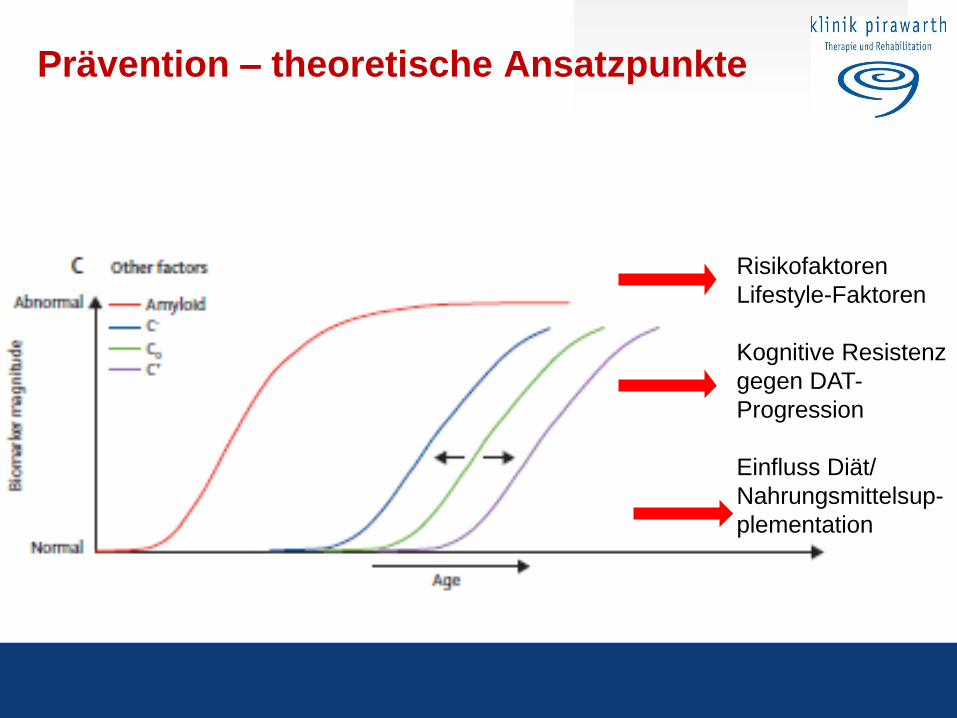
Prävention – theoretische Ansatzpunkte
Risikofaktoren
Lifestyle-Faktoren
Kognitive Resistenz
gegen DAT-
Progression
Einfluss Diät/
Nahrungsmittelsup-
plementation
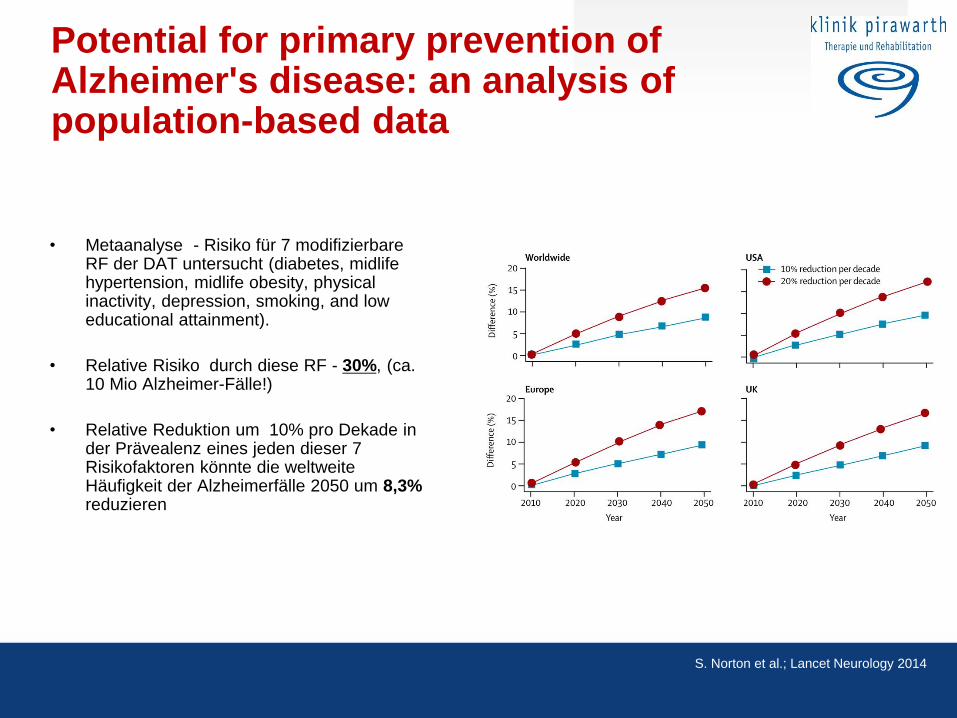
Potential for primary prevention of Alzheimer's disease: an analysis of population-based data
• Metaanalyse - Risiko für 7 modifizierbare RF der DAT untersucht (diabetes, midlife hypertension, midlife obesity, physical inactivity, depression, smoking, and low educational attainment).
• Relative Risiko durch diese RF - 30%, (ca. 10 Mio Alzheimer-Fälle!)
• Relative Reduktion um 10% pro Dekade in der Prävealenz eines jeden dieser 7 Risikofaktoren könnte die weltweite Häufigkeit der Alzheimerfälle 2050 um 8,3% reduzieren
S. Norton et al.; Lancet Neurology 2014
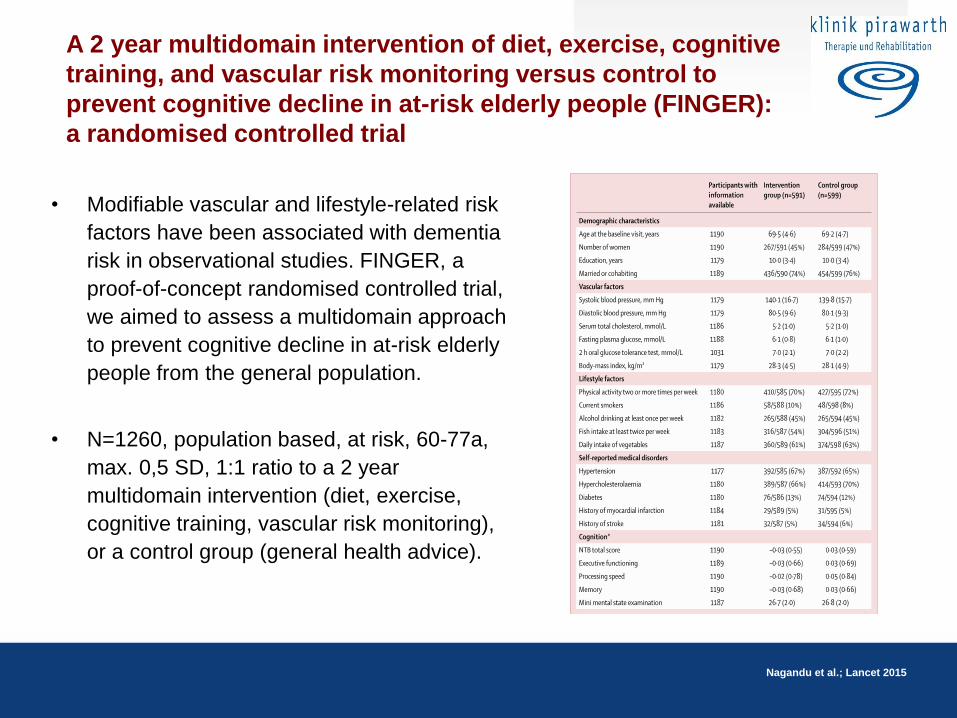
A 2 year multidomain intervention of diet, exercise, cognitive
training, and vascular risk monitoring versus control to
prevent cognitive decline in at-risk elderly people (FINGER):
a randomised controlled trial
Nagandu et al.; Lancet 2015
• Modifiable vascular and lifestyle-related risk
factors have been associated with dementia
risk in observational studies. FINGER, a
proof-of-concept randomised controlled trial,
we aimed to assess a multidomain approach
to prevent cognitive decline in at-risk elderly
people from the general population.
• N=1260, population based, at risk, 60-77a,
max. 0,5 SD, 1:1 ratio to a 2 year
multidomain intervention (diet, exercise,
cognitive training, vascular risk monitoring),
or a control group (general health advice).
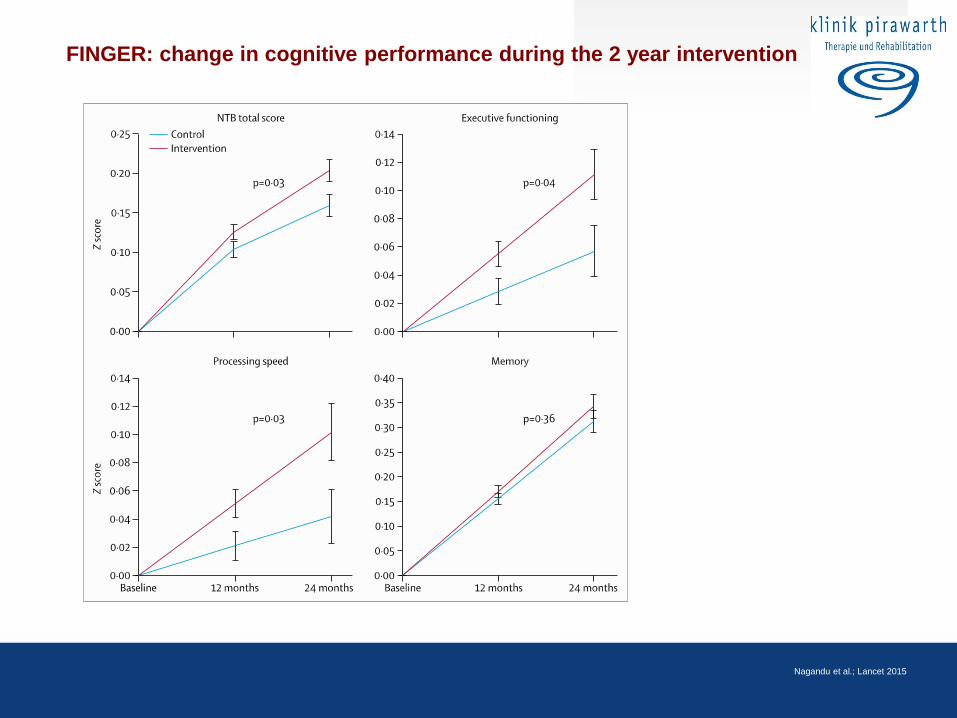
FINGER: change in cognitive performance during the 2 year intervention
Nagandu et al.; Lancet 2015
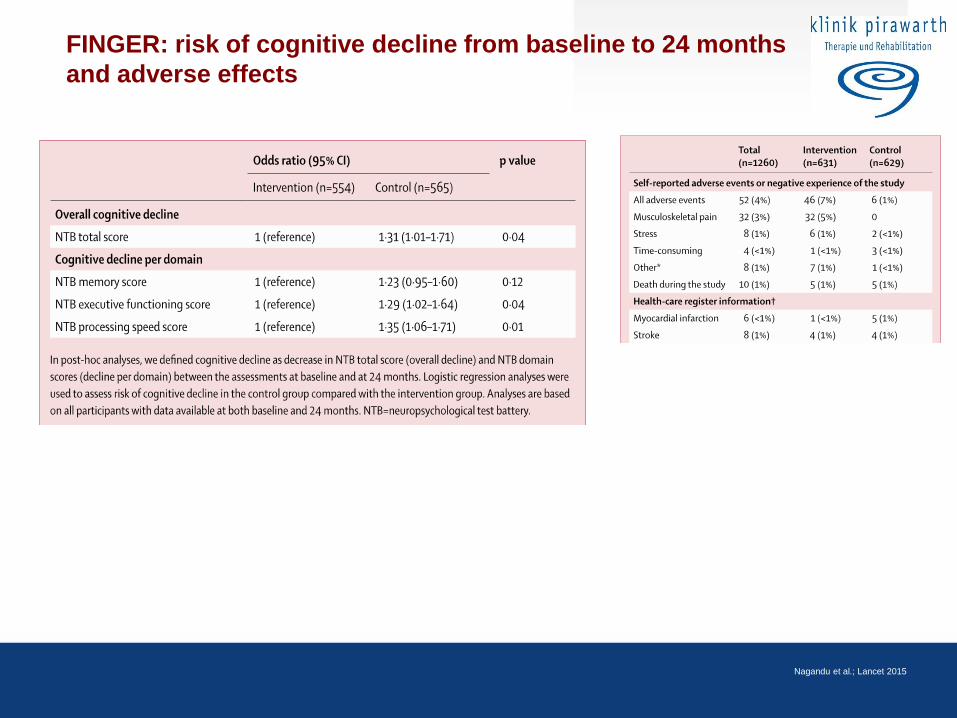
FINGER: risk of cognitive decline from baseline to 24 months
and adverse effects
Nagandu et al.; Lancet 2015

Aktuelle Therapie der Alzheimerdemenz und Perspektiven
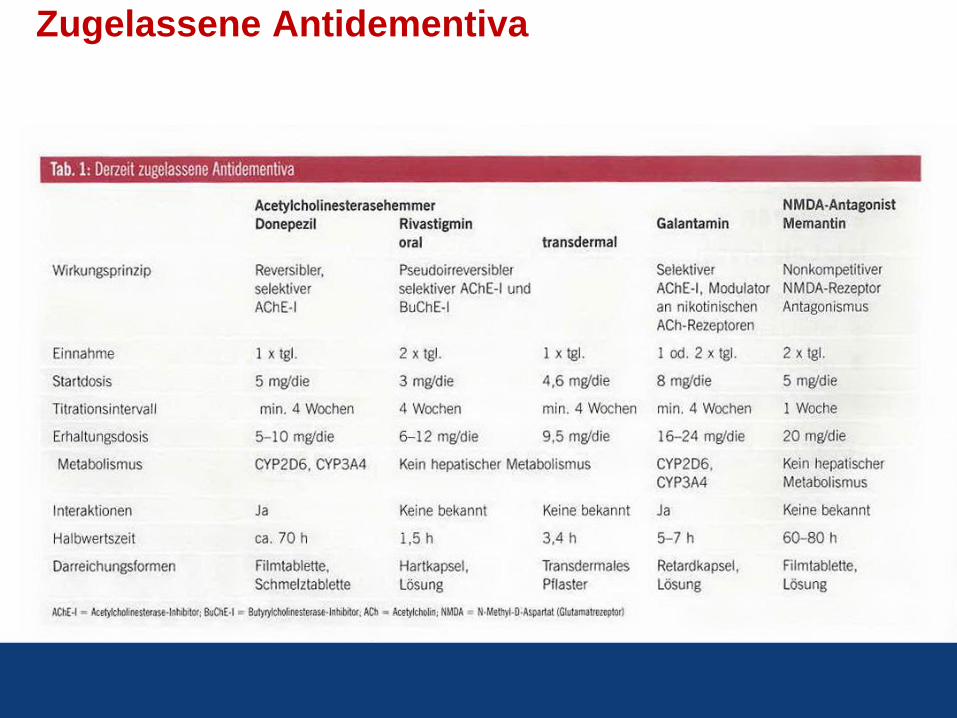
Zugelassene Antidementiva
Zusammenfassung I • Was haben wir bislang nicht erreicht?
- Heilung der Erkrankung/ keine Kausal wirksamen Therapien
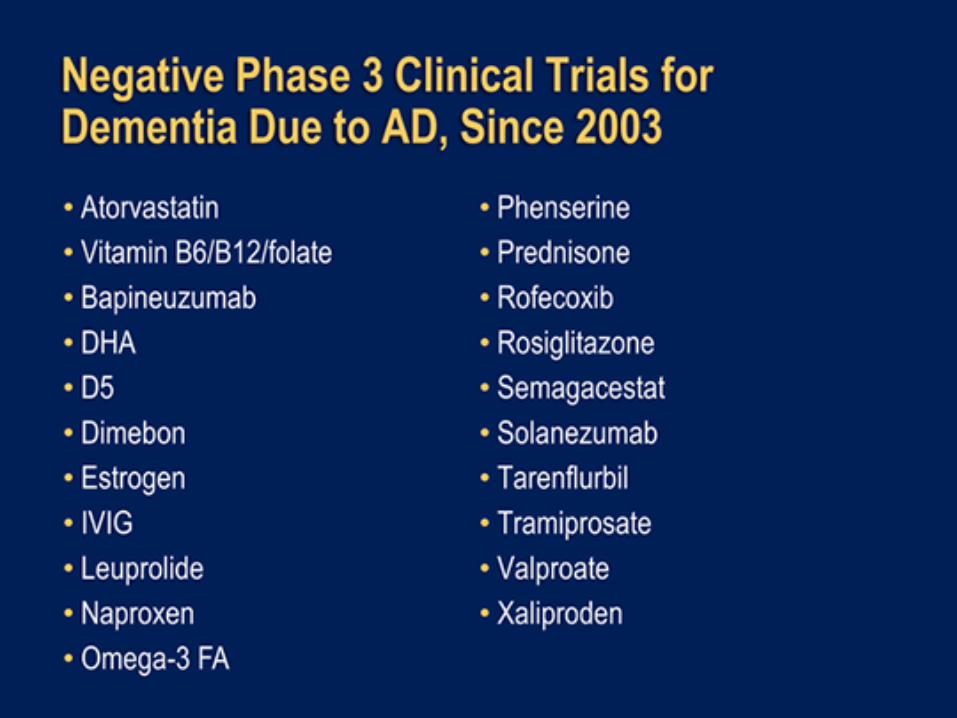
- zahlreiche Studien-Medikamente haben nicht den Weg in die klinische
Anwendung gefunden
- Frühe Diagnose: nur 20-50% erhalten eine Diagnose (weltweit nur ca.75%)
- Kontinuierliche Behandlung – nach einem Jahr nehmen nur mehr maximal 1/5
der Pat. ihre Medikamente (AChEH) ein!
- Eine adäquate Unterstützung der Betroffenen und Angehörigen (Pflegegeld,
Entlastungs- und Urlaubsangebote, soziale Einbindung, Demenzfreundliche
Krankenhäuser ....)
Zusammenfassung II • Was haben wir bislang bereits erreicht?
- Eine symptomatische Behandlung der Erkrankung. Mehrere wirksamen
Therapien stehen heute in der Routine zur Verfügung
- Frühe Diagnose: mit neuen Diagnoseverfahren ist eine zuverlässige und
frühzeitige Diagnostik möglich
- Das Auftreten neuer Demenzfälle scheint sich zu reduzieren
- Prävention ist wirksam und kann Gedächtnisleistung erhalten/Verbessern
- Kontinuierliche Behandlung – Medikamente sind in zahlreichen
patientenfreundlichen Formulierungen vorhanden (z.B. Pflaster)
- Eine Österreichischer Demenzplan ist im Entstehen
Vielen Dank für Ihre Aufmerksamkeit
Prim. Dr. Andreas Winkler, MSc
Klinik Pirawarth
Rehabilitationszentrum für Neurologie, Orthopädie u. Psychosomatik [email protected]
www.klinik-pirawarth.at