Embed Size (px)
Citation preview

Amori, R. E. et al. JAMA 2007;298:194-206.
Efficacy and Safety of Incretin Therapy in Type 2 Diabetes
Systematic Review and Meta-analysis
亀田総合病院 1年目初期研修医
大野 真紀

Amori, R. E. et al. JAMA 2007;298:194-206.
■ Background:<50% of Type2DM reach HbA1c<7.0% ・ ineffective implementation of therapy ・ efficacy of therapy diminishes as disease progresses and beta cell function declines ・ therapy limited by adverse effect
target the decline in beta cell function without weight gain with minimal adverse effects

Amori, R. E. et al. JAMA 2007;298:194-206.
□ incretin:・ augment glucose-stimulated insulin secretion by intestinally derived peptides → released with glucose in the gut
・ action depends on glucose concentration → cease glucose < 55mg/dL

Amori, R. E. et al. JAMA 2007;298:194-206.
□ incretin:・ GIP (glucose-dependent insulinotropic polypeptide) GLP-1 (glucagonlike peptide 1)
・ inactivated by DPP4 (dipeptidyl peptidase 4)

Amori, R. E. et al. JAMA 2007;298:194-206.
□ exenatide (Byetta):・ GLP-1 receptor analogue・ injection
□ sitagliptin・ selective DPP4 inhibitor・ oral・ for monotherapy or with metformin or thiazolidinedione

Amori, R. E. et al. JAMA 2007;298:194-206.
■ Objective:To assess the efficacy and safety of incretin-based therapy (GLP-1 analogues and DPP4 inhibitors) in type2 DM

Amori, R. E. et al. JAMA 2007;298:194-206.
■ Methods:□ Data source:・ MEDLINE and Cochrane for English RCT involving incretin therapy・ search prescribing information, relevant Web, reference and citation, abstracts at recent conferences

Amori, R. E. et al. JAMA 2007;298:194-206.
□ Study selection:inclusion: ・ RCT ・ compare incretin therapy with placebo or other medication ・ report HbA1c in nonpregnant adults with type 2 DM
exclusion: ・ < 12 weeks in duration

Amori, R. E. et al. JAMA 2007;298:194-206.
□ Data extraction:・ two independent reviewers・ resolved by consensus・ meta-analyses for efficacy and safety
baseline characteristics (Table1)

Table1. Characteristics of Randomized Controlled Trials of Glucagonlike Peptide 1 Analogues and Dipeptidyl Peptidase 4 Inhibitors Included in the Systematic Review
Amori, R. E. et al. JAMA 2007;298:194-206.

Amori, R. E. et al. JAMA 2007;298:194-206.

Amori, R. E. et al. JAMA 2007;298:194-206.

Amori, R. E. et al. JAMA 2007;298:194-206.
・ efficacy: primary: baseline HbA1c secondary: fasting PG, postprandial PG, proportion of patients achieving HbA1c<7% (body weight and lipid profile if available)
・ safety: hypoglycemia, all adverse events, antibodies to incretin analogue
・ quality: baseline characteristic, allocation concealment, ITT analysis, dropout rate

Amori, R. E. et al. JAMA 2007;298:194-206.
□ Data synthesis and analysis ・ continuous variable (HbA1c, fasting PG, weight): weighted mean difference, 95% CIs
・ dichotomous variable (HbA1c < 7%, hypoglycemia, adverse events): risk ration, 95% CIs
・ subgroup analyses

Amori, R. E. et al. JAMA 2007;298:194-206.
□ Data synthesis and analysis: ・ dose-dependent outcomes: data from approved maximum dose only ・ adverse event outcomes: data from all available doses ・ postprandial PG, lipid, antibody: no meta-analyses ・ meta-analyses: random-effects model ・ I-2 statistic for heterogeneity

Amori, R. E. et al. JAMA 2007;298:194-206.
■ Results:□ Search results (Figure1)

Amori, R. E. et al. JAMA 2007;298:194-206.
Figure1. Study Design

Amori, R. E. et al. JAMA 2007;298:194-206.
■ Results:□ Study characteristics (Table1):29 articles >30weeks: 3 articles
GLP-1 analogue: 8 trials long-acting GLP-1 analogue: 1 trial DPP4 inhibitor vs placebo: 13 trials DPP4 inhibitor vs medication: 4 trials DPP4 inhibitor only for certain meta-analyses: 3 abstracts

Amori, R. E. et al. JAMA 2007;298:194-206.
□ Methodological quality:・ double blind: all but for involving insulin・ eligibility: clearly reported・ concealment allocation: only 3 trials・ balanced baseline characteristic: few
・ withdrawal %: 19% in GLP-1 analogue, 18% in DPP4 inhibitor・ withdrawal reason: loss of efficacy in placebo GI adverse effects in exenatide・ all funded by pharmaceutical companies
Amori, R. E. et al. JAMA 2007;298:194-206.
□ incretin mimetics (GLP-1 analogue):・ glycemic: exenatide HbA1c decline: placebo: significant (Figure 2) insuline: no difference % of HbA1c<7%: placebo: significant (Table 2) insuline: no difference

Amori, R. E. et al. JAMA 2007;298:194-206.
Figure2. Weighted Mean Difference in Change in Hemoglobin A1c Percentage Value for GLP-1 Analogues vs Control in Adults With Type 2 Diabetes

Amori, R. E. et al. JAMA 2007;298:194-206.
□ incretin mimetics (GLP-1 analogue): fasting and postprandial PG placebo: significant (Table 2) insuline: postprandial PG reduced more in exenatide no difference in fasting PG mixed-meal testing: dose-dependent postprandial PG decrease
Amori, R. E. et al. JAMA 2007;298:194-206.
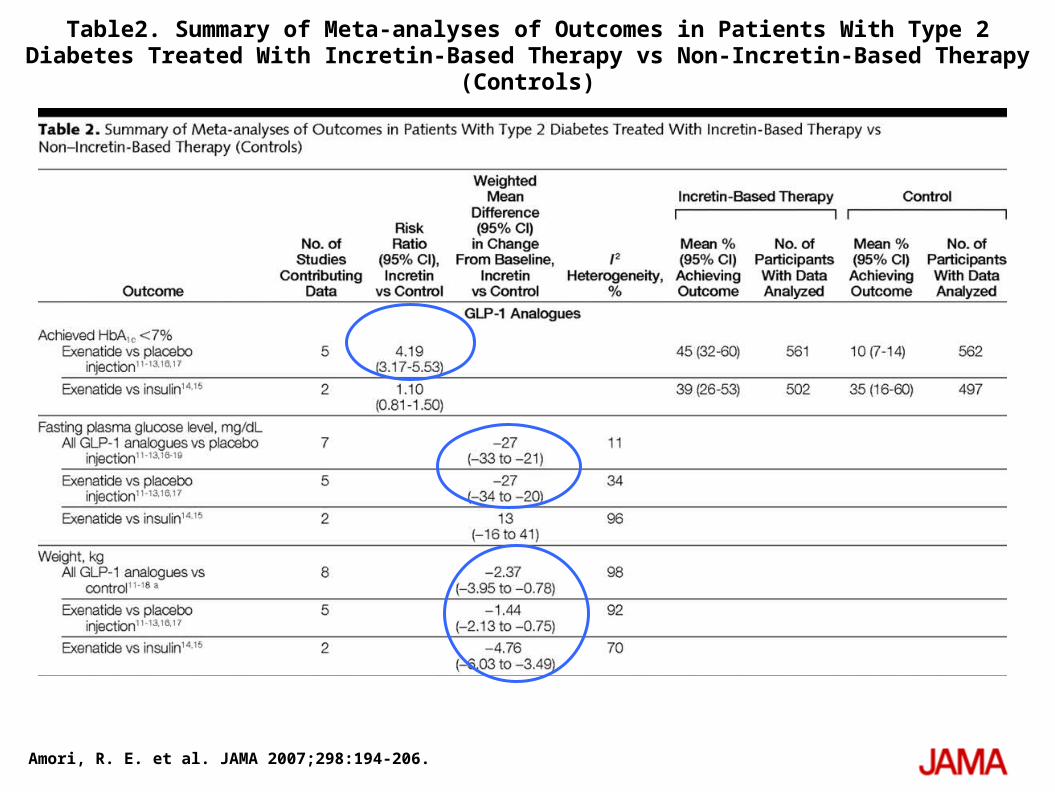
Table2. Summary of Meta-analyses of Outcomes in Patients With Type 2 Diabetes Treated With Incretin-Based Therapy vs Non-Incretin-Based Therapy (Controls)

Amori, R. E. et al. JAMA 2007;298:194-206.
□ incretin mimetics (GLP-1 analogue):・ nonglycemic: Weight : significant loss, more pronounced loss when compared with insulin progressive, dose-dependednt, without plateau trend– greater reduction with nausea Lipids: no significant change HDL better than insulin LDL better than placebo

Amori, R. E. et al. JAMA 2007;298:194-206.
□ incretin mimetics (GLP-1 analogue):・ Adverse events: hypoglycemia: mild to moderate, with SU during initiation of therapy similar with insulin Others: nausea and vomit: dose-dependent, mild to moderate, initial 8 weeks diarrhea antibodies: high, up to 67%

Amori, R. E. et al. JAMA 2007;298:194-206.
Table3. Summary of Adverse Events in Patients With Type 2 Diabetes Treated With Incretin-Based vs Non-Incretin-Based Therapy

Amori, R. E. et al. JAMA 2007;298:194-206.
□ incretin enhancers (DPP4 inhibitor1)・ glycemic: HbA1c decline: placebo: significant (Figure 3) other hypoglycemic agents: slightly less effective
% of HbA1c<7%: placebo: significant (Table2)

Amori, R. E. et al. JAMA 2007;298:194-206.
Weighted Mean Difference in Change in Hemoglobin A1c Percentage Value for DPP4 Inhibitors vs Control in Adults With Type 2 Diabetes

Amori, R. E. et al. JAMA 2007;298:194-206.
Table2 (cont.)Summary of Meta-analyses of Outcomes in Patients With Type 2 Diabetes Treated With Incretin-Based Therapy vs Non-Incretin-Based Therapy (Controls)

Amori, R. E. et al. JAMA 2007;298:194-206.
□ incretin enhancers (DPP4 inhibitor1)fasting and postprandial PG placebo: significant (Table 2) sitagliptin > vildagliptin
mixed-meal testing: dose-dependent postprandial PG decrease
Amori, R. E. et al. JAMA 2007;298:194-206.
□ incretin enhancers (DPP4 inhibitor1)・ nonglycemic: Weight : small increase sitagliptin: better than glipizide vildagliptin: better than thiazolidinediones
Lipids: no consistent change some improvements in TG, LDL, HDL

Amori, R. E. et al. JAMA 2007;298:194-206.
□ incretin enhancers (DPP4 inhibitor1)・ Adverse events: hypoglycemia: severe in 2 patients mild to moderate, no difference Others: no GI effects, very well tolerated nasopharyngitis, UTI, headache

Amori, R. E. et al. JAMA 2007;298:194-206.
Table3 (cont.) Summary of Adverse Events in Patients With Type 2 Diabetes Treated With Incretin-Based vs Non-Incretin-Based Therapy

Amori, R. E. et al. JAMA 2007;298:194-206.
Summary of Adverse Events in Patients With Type 2 Diabetes Treated With Incretin-Based vs Non-Incretin-Based Therapy

Amori, R. E. et al. JAMA 2007;298:194-206.
■ Conclusion:incretin-based therapy:・ moderate effectiveness in glycemia・ greater reductions in postprandial PG・ favorable (GLP-1) or neutral (DPP4) effects on weight
・ adverse effects GLP-1: GI adverse effects DPP4 inhibitor: infection and headache

Amori, R. E. et al. JAMA 2007;298:194-206.
□ moderate effectiveness in glycemia :・ relatively low baseline HbA1c (~8%)・ greater reduction in higher HbA1c
□ greater reductions in postprandial PG:・ postprandial reduction > fasting reduction・ alternative for targeting postprandial glycemia・ noninferior to others, except for metformin superior to vildagliptin

Amori, R. E. et al. JAMA 2007;298:194-206.
□ favorable (GLP-1) or neutral (DPP4) effects on weight:・ continuous loss without plateau・ may or may not due to nausea・ weight loss medication ?: exenatide・ DPP4 better than SU, thiazolidinediones

Amori, R. E. et al. JAMA 2007;298:194-206.
□ adverse effects:・ low hypoglycemia: glucose dependent, may occur with insulin secretagogues
・ GI adverse effects: develop tolerance, withdrawal 4% dose escalation protocol to minimize effects

Amori, R. E. et al. JAMA 2007;298:194-206.
□ adverse effects:・ infection and headache: ubiquitous cell-membrane protein, concerns about long-term immune function, relative risk 1.5 → significant burden
・ headache: not related to hypoglycemia

Amori, R. E. et al. JAMA 2007;298:194-206.
□ Limitation: < less than 30 weeks: long-term data needed race or ethnicity: white dominant children not included not used intention-to-treat analyses: may overestimate glycemic efficacy

Amori, R. E. et al. JAMA 2007;298:194-206.
□

Amori, R. E. et al. JAMA 2007;298:194-206.
□