-
1591
ORIGINAL ARTICLE
An Open-label Longitudinal Study on the Efficacy ofSwitching
from Insulin Glargine or Detemir to Degludec
in Type 2 Diabetes Mellitus
Ippei Kanazawa 1, Masakazu Notsu 1, Ken-ichiro Tanaka 1, Nobuaki
Kiyohara 1,Yuko Tada 2 and Toshitsugu Sugimoto 1
Abstract
Objective Insulin degludec (IDeg), a new long-acting basal
insulin, and FlexTouch, a new injection device,recently became
available in Japan. The efficacy and usefulness of IDeg and
FlexTouch, compared with insu-lin glargine or detemir, were
assessed in patients with type 2 diabetes mellitus.Methods We
performed an open-label longitudinal trial in 20 patients. After
informed consent was ob-tained, all subjects recorded their
self-monitoring data of the blood glucose (BG) level; thereafter,
basal insu-lin was replaced by an IDeg-prefilled FlexTouch with the
same dose and duration of time (2 weeks). Afterusing FlexTouch, the
patients were provided a device-specific questionnaire.Results The
patients were divided into two groups according to the dose of
basal insulin (10 U and
-
Intern Med 54: 1591-1598, 2015 DOI:
10.2169/internalmedicine.54.3993
1592
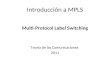
Figure1.Study protocol. Basal insulin treatment was switched to
insulin degludec for 2 weeks. In the week indicated by the
asterisk, self-monitored blood glucose levels were recorded every
day before breakfast and just before basal insulin injection.
0
*
Insulin degludec
1 2 3 4 5
* *
weeks
Insulin glargine/detemir Insulin glargine/detemir
Recently, insulin degludec (IDeg), a new, long-acting ba-sal
insulin preparation, has been made commercially avail-able. IDeg is
reported to have a terminal half-life of ap-proximately 25 hours,
which is two times longer than insu-lin glargine, and a duration of
action of more than 42hours (2, 3). In addition, IDeg provides a
smaller peak ef-fect compared with traditional basal insulin (4)
and thusmay be an ideal basal insulin to achieve the stable control
ofthe BG levels.As insulin devices have developed, it has become
easier
to initiate insulin therapy than before. It has become easierto
teach diabetic patients how to use insulin injection
pens;therefore, the use of these pens is widespread. Owing
tocontinuous improvements in the injection-system technology,a
prefilled injection device, FlexTouch, was newly generatedby Novo
Nordisk A/S (Kobenhavn, Denmark). It has beenreported that more
insulin-treated pen-naive patients withtype 1 and type 2 diabetes
mellitus preferred FlexTouch interms of the ease of use, insulin
injection, diabetes manage-ment, and overall preference (5). In
2013, the IDeg-prefilledFlexTouch became available in Japan;
however, the efficacyof IDeg or the usefulness of FlexTouch has not
yet beenclinically evaluated in patients with type 2 diabetes.
Weherein evaluate the BG levels and their fluctuations in Japa-nese
patients with type 2 diabetes during the use of tradi-tional basal
insulin and IDeg and determine the usefulnessof FlexTouch via
interview forms when the previous injec-tion device was switched to
FlexTouch.
Materials and Methods
Subjects
Twenty participants with type 2 diabetes (mean age, 67.1years;
65% men) were recruited in this open-label longitudi-nal study to
evaluate the efficacy of IDeg compared withtraditional basal
insulin. At the study enrollment, the demo-graphic data, clinical
characteristics, and current diabetestreatments were recorded. The
numbers of patients who hadbeen taking sulfonylurea, metformin,
dipeptidyl peptidase-4inhibitors, and alpha-glucosidase inhibitors
were 1, 4, 9, and2, respectively. During the follow-up period, no
prescribedmedications except for basal insulin were changed, and
norestrictions were imposed on the patients lifestyle, exceptthat
they were encouraged to adhere to an appropriateweight-control
program, including proper nutrition control
and regular exercise.This study was in compliance with the
Declaration of
Helsinki and was approved by the Institutional ReviewBoard of
the Shimane University Faculty of Medicine. Allsubjects agreed to
participate in the study and gave informedconsent.
Study protocol
After informed consent was obtained, all subjects contin-ued
receiving insulin glargine or detemir once per day;thereafter,
basal insulin was replaced by the same dose ofIDeg for the same
duration of treatment (2 weeks). The pa-tients were requested to
record their self-monitoring data ofthe fasting BG (FBG) before
breakfast and the BG level justbefore injection of basal insulin
(BG-I) for the week imme-diately prior to the switch to IDeg and
for the second weekafter the switch to IDeg (Fig. 1). The means of
the BG lev-els and standard deviation (SD) were calculated. The
pa-tients were also asked to record their symptoms when theglucose
level was
-
Intern Med 54: 1591-1598, 2015 DOI:
10.2169/internalmedicine.54.3993
1593
Table1.Background Data of the Subjects.
Number of subjects (male/female) Age (years) Duration of
diabetes (years) Duration of insulin treatment (years) Preparation
of basal insulin Glargine Detemir Dose of basal insulin (units)
Basal and 3 mealtime rapid-acting insulin Basal and 1 or 2
rapid-acting insulin Basal without bolus insulin BMI (kg/m2) Grip
power (kg) ALT (U/L) Serum creatinine (mg/dL) Mean of FBG (mg/dL)
SD of FBG Mean of BG-I (mg/dL)SD of BG-I HbA1c (%)
67.1 15.9
7.3
12
25.3 28.9
240.82 134
17158
287.3
20 (13/7)
164120 8
Data are mean SD. BMI: body mass index, ALT: alanine
aminotransferase, FBG: fasting blood glucose, SD: standard
deviation, BG-I: blood glucose before injection of basal insulin,
HbA1c: hemoglobin A1c
8.9 10.7 7.5
8
4.2 9.8 140.21 271548180.9
using the paired Students t-test. Students t-test and the 2test
were used in univariate analyses. All the analyses wereperformed
using the statistical computer program StatView(Abacus Concepts,
Berkeley, USA) and statistical signifi-cance was considered to
exist at p value
-
Intern Med 54: 1591-1598, 2015 DOI:
10.2169/internalmedicine.54.3993
1594
Table2.Chronological Changes in the Parameters of Blood Glucose
in All Subjects.
Mean of FBG (mg/dL) SD of FBG Mean of BG-I (mg/dL) SD of
BG-I
13417
15828
Baseline
27154818
13516
15022
32105213
13318
16426
25176518
Degludec After Mean change 95% CI p
0.8-1.4 -7.7 -5.5
-9.4 - 10.9-6.4 - 3.6 -19.1 - 3.7 -11.7 - 0.7
0.879 0.566 0.174 0.078
Data are mean SD. FBG: fasting blood glucose, SD: standard
deviation, BG-I: blood glucose before injection of basal insulin,
CI: confidential interval Statistical significance was determined
using paired Students t test compared to baseline data.
Table3.Comparison of Various Parameters between Patients with
Decreased BG-I and with Increased BG-I.
Age (years) Duration of diabetes (years) Duration of insulin
treatment (years) Dose of basal insulin (units) Dose of basal
insulin / body weight Basal with 3 bolus/basal without bolus BMI
(kg/m2)Grip power (kg) ALT (U/L) Serum creatinine (mg/dL)Mean FBG
(mg/dL)SD of FBG Mean of BG-I (mg/dL)SD of BG-I HbA1c (%)
66.3 17.0
4.2 7
0.12
22.5 34.3
200.81 132
14150
267.2
3/4
7.3 13.4 4.3 6 0.08
3.2 9.4 8 0.23 228 54200.8
Number of subjects 767.5 15.4
9.0 14
0.22
26.9 26.8
260.82 135
19162
297.3
5/8
10.0 9.5 8.5 8 0.13
3.9 9.5 160.20 301847180.9
13Increased Decreased
0.774 0.745 0.186 0.053 0.075 0.7830.022 0.156 0.400 0.974 0.850
0.539 0.613 0.813 0.839
p
Data are mean SD. BMI: body mass index, ALT: alanine
aminotransferase, FBG: fasting blood glucose, SD: standard
deviation, BG-I: blood glucose before injection of basal insulin,
HbA1c: hemoglobin A1c
Table4.Chronological Changes in the Parameters of Blood Glucose
in Patients Treated with Less than or More than 10 Units of Basal
Insulin.
Dose of basal insulin < 10 units (n=9)
Dose of basal insulin 10 units (n=11)
Mean of FBG (mg/dL)SD of FBG Mean of BG-I (mg/dL)SD of BG-I
14322
16432
Baseline
27184517
14318
14422
34104010
14322
15832
28144516
Degludec After Mean change 95% CI p
0.5 -3.5 -19.6 -10.4
-17.9 - 19.0 -13.0 - 5.9 -30.2 - 9.0 -19.5 - 1.2
0.949 0.423 0.002 0.031
Data are mean SD.FBG: fasting blood glucose, SD: standard
deviation, BG-I: blood glucose before injection of basal insulin,
CI: confidential interval Statistical significance was determined
using paired Students t test compared to baseline data.
Mean of FBG (mg/dL) SD of FBG Mean of BG-I (mg/dL) SD of
BG-I
12311
15022
Baseline
247 5419
12412
15723
269 6617
12214
15118
23157315
Degludec After Mean change 95% CI p
1.0 1.2 6.9 0.4
-9.3 - 11.3 -1.3 - 3.7
-13.0 - 26.7 -7.5 - 8.4
0.828 0.295 0.4460.901
Discussion
In this study, neither parameter was significantly changed
after switching to IDeg when the glucose levels and SDswere
examined in all the subjects. These findings suggestthat switching
from traditional basal insulin to IDeg may notbe useful for all
patients with type 2 diabetes. However,
-
Intern Med 54: 1591-1598, 2015 DOI:
10.2169/internalmedicine.54.3993
1595
Figure2.Percent changes in the blood glucose parameters before
basal insulin injection. The sub-jects were divided into two groups
according to the dose of basal insulin (10 U and
-
Intern Med 54: 1591-1598, 2015 DOI:
10.2169/internalmedicine.54.3993
1596
Figure3.The subjects comparison assessments via a
device-specific questionnaire on FlexTouch and the previously used
device. The black bars indicate the number of subjects rating
FlexTouch with the higher score; gray bars indicate the number of
subjects rating the other device with the higher score; and white
bars indicate the number of subjects who gave both the devices the
same rating.
4
6
5
2
1
2
5
5
6
7
8
3
3
1
11
8
8
10
16
18
12
19
9
3
4
4
3
2
4
5
5
1
3
7
12
11
15
17
15
2
2
1
1
5
2
1
1
3
13
16
20
19
18
16
20
9 9 2
Pen Preparation before injectionEase of reading dose scale
Q1
Ease of hearing clicks while setting dose Q2 Ease of feeling
clicks while setting dose Q3
Ease of turning dose selector Q4 Confidence of setting correct
dose Q5
Ease of attaching needle Q6 Confidence correctly performing air
shot Q7
Speed of preparing pen for injection Q8
Insulin injection with PenEase of pushing injection button
Q9
Ease of holding pen stable during injection Q10 Ease of
determining if full dose is injected Q11
Ease of injecting in different places on body Q12 Painlessness
of self-injection Q13
Fit in hand during injection Q14
General opinion about the PenConfidence in injecting correct
amount of insulin Q15
Usefulness of color coding to indicate insulin type Q16 Comfort
in managing daily injections Q17
Comfort in controlling blood glucose levels Q18 Pen is discreet
to use in public Q19
Convenience of pen size Q20 Easy to learn how to use Q21
Overall
FlexTouch Previous Pen Both Preference
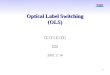
Figure4.The subjects comparison assessments via a
device-specific comparative preference ques-tionnaire on FlexTouch
and the previously used device. The black bars indicate the number
of sub-jects rating FlexTouch with the higher score; gray bars
indicate the number of subjects rating the other device with the
higher score; and white bars indicate the number of subjects who
gave a similar rating for both devices.
FlexTouch Previous Pen Both Preference
Easier to prepare before injection Q1
Easier to injection dose Q2
Easier to depress button for injection Q3
More suitable length when injecting maximum dose Q4
Simpler to use Q5
Easier to use Q6
Trust more to accurately deliver insulin Q7
Safer to operate Q8
1
5
9
4
5
3
3
4
8
7
1
4
5
6
5
15
7
4
19
12
10
11
12
tween the effect of IDeg and the residual capacity of
insulinsecretion as well as the dose of basal insulin in type 2
dia-betes.Conversely, the FBG levels remained unchanged after
the
switch to IDeg. Phase 2 and 3 trials have shown similar re-sults
to the present study. The lowering effects of IDeg andglargine on
the FBG and HbA1c levels were not different inthe patients with
type 2 diabetes (7, 8). However, it has
-
Intern Med 54: 1591-1598, 2015 DOI:
10.2169/internalmedicine.54.3993
1597
Table6.Comparison of Various Parameters between the Preference
of Insulin Device.
Age (years) Male/female Duration of diabetes (years) Duration of
insulin treatment (years) Dose of basal insulin (units) Basal with
3 bolus/basal without bolus BMI (kg/m2)Grip power (kg) Mean FBG
(mg/dL)SD of FBG Mean of BG-I (mg/dL)SD of BG-I HbA1c (%) Changes
in mean FBG (mg/dL)Changes in SD of FBG Changes in mean of BG-I
(mg/dL)Changes in SD of BG-I
7 / 2
3 / 6
Number of subjects
6 / 3
8 / 1
FlexTouch Previous Pen p
Data are mean SD. BMI: body mass index, ALT: alanine
aminotransferase, FBG: fasting blood glucose, SD: standard
deviation, BG-I: blood glucose before injection of basal insulin,
HbA1c: hemoglobin A1c
65.4
10.3 4.6 13
25.9 31.6 123
13151
257.2
8 0
-13-4
9.8
7.5 5.6 10
3.7 8.2 278 48151.0 249 1210
67.2
21.2 10.2
10
24.9 29.1 149
23173
347.5 -2 -3 0
-8
7.6
11.9 8.9 6
5.3 10.7 222050200.8 18143317
0.674 0.599 0.0340.140 0.490 0.016 0.648 0.611 0.039 0.198 0.352
0.308 0.446 0.3190.588 0.268 0.633
9 9
been previously reported that the events of nocturnal
hypo-glycemia were significantly reduced in the patients
treatedwith IDeg compared with those treated with insulinglargine
(8). The glucose-lowering effects of insulin glargineand detemir
last a maximum of approximately 4 and 7hours, respectively, after
injection and then decrease gradu-ally (9). The peak effects of
glargine and detemir may causenocturnal hypoglycemia. In contrast,
the glucose-loweringeffects of IDeg are reported to be flat and
stable over 24hours when measured by the euglycemic glucose
clampmethod (4). Therefore, switching from conventional
basalinsulin to IDeg may be beneficial even if the FBG andHbA1c
levels do not change. Because no hypoglycemicevents were reported
in the present short-term study of rela-tively poorly controlled
patients, further studies are neededto examine this point in the
future.The stability effect of IDeg is clinically useful for
control-
ling daily BG levels. If a patients BG levels are
constantlyfluctuating, it is difficult to change the insulin
administrationdose. In contrast, adjusting the insulin dose becomes
easierif the BG levels are stabilized. Previous studies have
shownthat the BG fluctuation improved after replacing
insulinglargine with IDeg (10). As described previously, the
stabil-ity of IDegs action leads to a stable BG. In the
presentstudy, the SD value of BG-I was significantly decreased
af-ter switching from basal insulin to IDeg in the patientstreated
with a higher dose; thereafter, it returned to the base-line level.
Therefore, these findings confirm the stableglucose-lowering effect
of IDeg in the patients with type 2diabetes.Previous studies
demonstrated that FlexTouch accurately
and consistently delivered insulin (11). Moreover, FlexTouchis
currently the only prefilled pen that has a push button thatdoes
not extend at any dose (as opposed to the traditional
prefilled pens which require more thumb or finger pressurefor
injection). This may make it easier for patients to injectinsulin.
In the present study, we evaluated the preference forFlexTouch when
the insulin device was exchanged for 2weeks. Half of the patients
preferred FlexTouch comparedwith the previous device they used and
half did not. In addi-tion, the patients with a shorter duration of
diabetes, singleinsulin injection, and lower FBG levels tended to
preferFlexTouch compared with their previous insulin device.
Inother words, the patients with a longer duration of
diabetesreceiving basal and three bolus mealtime rapid-acting
insulintreatments may have become more accustomed to the
insulindevice they were using. However, the insulin device
prefer-ence made no difference in the glucose-lowering effect
ofIDeg.There are some limitations associated with the present
study. First, the sample size was not large enough to
makedefinite conclusions. A large-scale study ought to be
con-ducted to confirm the present findings. However, we
chrono-logically evaluated the BG levels and SDs after
switchingfrom IDeg to the previous insulin and found that the
pa-rameters evaluated returned to the baseline levels.
Thesefindings support the effectiveness of IDeg. Second, we
ana-lyzed only subjects who accepted the study protocol;
there-fore, we are not able to exclude potential selection
bias.Third, due to the limited number of subjects, we could
notseparately assess insulin glargine and detemir. Fourth, theBMIs
in the present populations were lower than those ob-served in
Western populations, and the capacity of insulinsecretion and
degree of obesity in Asian populations areknown to differ from
Western populations (12). Thus, large-scale longitudinal studies
should be performed in othercountries. In contrast, previous
studies showed no differ-ences in the BG levels between IDeg and
glargine (7, 8).
-
Intern Med 54: 1591-1598, 2015 DOI:
10.2169/internalmedicine.54.3993
1598
We found that the BG-lowering effects of high-dose IDegmay be
more favorable than traditional basal insulin. Thecontradictory
results between the previous studies and thepresent study may be
due to the differences in the studyprotocol, basal insulin doses,
and insulin injection devices.In conclusion, replacing basal
insulin with IDeg is useful
for the stable and accurate control of the BG levels in
thepatients with type 2 diabetes receiving higher doses of
basalinsulin. The patients with a short duration of diabetes
re-ceiving a single injection of insulin preferred switching
fromtheir device to FlexTouch.This manuscript has been registered
with an approved IC-
MJE clinical trial registry ID (UMIN000011333).
The authors state that they have no Conflict of Interest
(COI).
References
1. UKPDS Group. U.K. prospective diabetes study 16. Overview of6
years therapy of type II diabetes: a progressive disease.
U.K.Prospective Diabetes Study Group. Diabetes 44: 1249-1258,
1995.
2. Heise T, Pieber TR. Towards peakless, reproducible and
long-acting insulins. An assessment of the basal analogues based
onisolycaemic clamp studies. Diabetes Obes Metab 9:
648-659,2007.
3. Heise T, Hvelmann U, Nosek L, Bttcher S, Granhall C, HaahrH.
Insulin degludec has a two-fold longer half-life and a
moreconsistent pharmacokinetic profile than insulin glargine.
Diabetes60 (Suppl 1): LB11, 2011.
4. Heise T, Nosek L, Bttcher SG, Hastrup H, Haahr H.
Ultra-long-acting insulin degludec has a flat and stable
glucose-lowering ef-fect in type 2 diabetes. Diabetes Obes Metab
14: 944-950, 2012.
5. Garg S, Bailey T, DeLuzio T, Pollom D. Preference for a new
pre-filled insulin pen compared with the original pen. Cerr Med
ResOpin 27: 2323-2333, 2011.
6. Yamada K, Nakayama H, Sato S, et al. A randomized
crossoverstudy of the efficacy and safely of switching from insulin
glargineto insulin degludec among patients with type 1 diabetes.
DiabetolInt 5: 74-77, 2014.
7. Zinman B, Fulcher G, Rao PV, et al. Insulin degludec, an
ultra-long-acting basal insulin, once a day or three times a week
versusinsulin glargine once a day in patients with type 2 diabetes:
a 16-week, randomized, open-label, phase 2 trial. Lancet 377:
924-931,2011.
8. Rodbard HW, Cariou B, Zinman B, et al. Comparison of
insulindegludec with insulin glargine in insulin-nave subjects with
type2 diabetes: a 2-year randomized, treat-to-target trial. Diabet
Med30: 1298-1304, 2013.
9. Porcellati F, Rossetti P, Busciantella NR, et al. Comparison
ofpharmacokinetics and dynamics of the long-acting insulin
analogsglargine and detemir at steady state in type 1 diabetes: a
double-blind, randomized, crossover study. Diabetes Care 30:
2447-2452,2007.
10. Ogawa S, Nako K, Okamura M, Senda M, Sakamoto T, Ito
S.Compared with insulin glargine, insulin degludec narrows the
day-to-day variability in the glucose-lowering effect rather than
lower-ing blood glucose levels. J Diabetes Mellitus 3: 244-251,
2013.
11. Wielandt JO, Niemeyer M, Hansen MR, Bucher D, Thomsen
NB.FlexTouch: a prefilled insulin pen with a novel injection
mecha-nism with consistent high accuracy at low-(1 U), medium-(40
U),and high-(80 U) dose settings. J Diabetes Sci Technol 5:
1195-1199, 2011.
12. Torrens JI, Skurnick J, Davidow AL, et al. Ethnic
differences ininsulin sensitivity and beta-cell function in
premenopaulsa or earlyperimenopausal women without diabetes: the
Study of WomensHealth Across the Nation (SWAN). Diabetes Care 27:
354-361,2004.
2015 The Japanese Society of Internal
Medicinehttp://www.naika.or.jp/imonline/index.html