Embed Size (px)
Citation preview

Surg Today (2003) 33:873–878DOI 10.1007/s00595-003-2602-7
Appleby Operation for Pancreatic Body-Tail Carcinoma:Report of Three Cases
Koji Yamaguchi, Kenji Nakano, Kiichiro Kobayashi, Yasuhiro Ogura, Hiroyuki Konomi, Atsushi Sugitani,and Masao Tanaka
Department of Surgery and Oncology, Graduate School of Medical Sciences, Kyushu University, 3-1-1 Maidashi, Higashi-ku,Fukuoka 812-8582, Japan
Key words Appleby operation · Pancreatic body-tailcarcinoma · Total pancreatectomy
Introduction
Despite recent advances in diagnostic and therapeuticmodalities, the clinical outcome of patients with pancre-atic carcinoma remains dismal.1 The resectability is stillvery limited and long-term survival after surgery israre.2,3 Moreover, pancreatic body-tail carcinoma isoften found at a later stage than pancreatic head carci-noma. This is because pancreatic head carcinoma causesobstructive jaundice, resulting in relatively earlier de-tection, whereas pancreatic body and tail carcinoma isfound in the late phase as a huge mass causing backpain. Anatomically, the distal pancreas is thin, and can-cerous invasion to the retropancreatic structures occurseasily. The major reasons for unresectability are me-tastases to other organs and cancerous invasion ofmajor vessels such as the common hepatic, splenic, andceliac arteries, and to the retroperitoneum. Hence,patients often have no symptoms until the cancerinfiltrates the neural plexus around these vessels, andtumors remain in the retroperitoneal aspect after con-ventional distal pancreatectomy.
In Western countries, the resectability of carcinomaof the body and tail of the pancreas and the 5-yearsurvival rate are both about 10%.4,5 On the otherhand, resectability is relatively high in Japan, at34% (4 597/13 498) according the Pancreatic CancerRegistration Committee of the Japan Pancreas Society.6
The 3- and 5-year survival rates are also relativelyhigh, at 23% and 18%, respectively. This differencemay be attributable to the fact that extended radicalresection with extensive clearance of the lymph nodesand retroperitoneal tissue is widely performed inJapan.
AbstractThe clinical course of patients with carcinoma of thepancreas, especially of the body-tail, remains dismaldespite recent advances in diagnostic and therapeuticprocedures. We present three case reports to evaluatethe role of the Appleby operation in the treatment ofpancreatic body-tail cancer. Care 1 was a 55-year-oldJapanese woman who underwent the Appleby opera-tion for mucinous cystadenocarcinoma of the body andtail of the pancreas invading the stomach, celiac axis,superior mesenteric and splenic arteries, and thesplenic, superior mesenteric, and portal veins. Localrecurrence and peritoneal dissemination with malignantascites were found 7 months later and she died 10months after the operation. Case 2 was a 61-year-oldJapanese man who underwent the Appleby operationwith 20 Gy radiation therapy for invasive ductal carci-noma of the body of the pancreas involving the celiacaxis, common hepatic, splenic, and left gastric arteries,and the splenic vein. Peritoneal dissemination with ma-lignant ascites was evident 5 months later and he died 14months after the operation. Case 3 was a 50-year-oldJapanese man who underwent the Appleby operationwith 20 Gy radiation therapy for invasive ductal carci-noma of the body of the pancreas invading the stomach,splenic artery, celiac axis, and splenic vein. Multiplehepatic metastases were found 2 months later and thepatient died 8 months after the operation. Based on ourexperience of these three cases, we conclude that theindications for the Appleby operation to treat locallyadvanced pancreatic body carcinoma are still limitedbecause it does not improve quality of life or clinicaloutcome.
Reprint requests to: K. YamaguchiReceived: May 28, 2002 / Accepted: March 11, 2003

874 K. Yamaguchi et al.: Appleby Operation for Pancreas Cancer
The Appleby operation was first described byAppleby,7 a Canadian surgeon, in 1953. It was originallydevised for complete clearance of the lymph nodes,especially those along the celiac axis in a patient withgastric carcinoma. In 1976, Nimura et al.8 first adoptedthis operation for a patient with carcinoma of the bodyand tail of the pancreas to achieve complete retroperito-neal clearance. To our knowledge, this procedure hasbeen used to treat 11 cases of carcinoma in the body andtail of the pancreas with invasion of the common he-patic, splenic, or celiac arteries, which were thought tobe unresectable.8–15 We report our experience of treat-ing three cases of pancreatic body and tail carcinomawith the Appleby operation, and review the total 14cases reported in the literature, including ours.
Case Reports
Case 1: Invasive Mucinous Cystadenocarcinomaof the Body and Tail of the Pancreas
A 55-year-old Japanese woman presented to our hospi-tal with back pain. Her serum levels of carbohydrateantigen (CA) 19-9 and carcinoembryonic antigen(CEA) were 2054.2 U/ml and 0.5 ng/ml, respectively.Ultrasonography (US) showed a multicystic lesion, 6 �4.5cm, in the body and tail of the pancreas. Computedtomography (CT) demonstrated a multicystic tumor ofthe body-tail of the pancreas invading the retroperito-neal tissue, including the celiac, left gastric, inferiorphrenic, splenic, and dorsal pancreatic arteries, and thesplenic vein, producing localized portal hypertension.The gastroduodenal and superior mesenteric arteriesand portal vein were spared. Endoscopic retrogradecholangiopancreatography (ERCP) showed completeobstruction of the main pancreatic duct at the body ofthe pancreas. Cytology of the pancreatic juice revealedatypical cells suggestive of malignancy.
Laparotomy was done under the tentative diagnosisof mucinous cystadenocarcinoma of the body and tail ofthe pancreas invading the celiac axis. The patient wasfully informed of the disease and the operative risksbefore surgery. On opening the abdomen, no peritonealdissemination was seen, but the pancreatic body massinvaded the stomach and transverse colon. TheAppleby operation, which consisted of total gastrec-tomy, subtotal pancreatectomy, and splenectomy, wasdone with partial resection of the transverse colon. Fol-lowing Kocher’s maneuver, the superior mesenteric ar-tery was taped and hepatic arterial flow was confirmedin the hepatoduodenal ligament after transient clamp-ing of the common hepatic artery. The celiac artery wasligated and cut at the root. Reconstruction was doneusing the double tract method. The histopathologic
diagnosis was invasive mucinous cystadenocarcinoma ofthe body and tail of the pancreas. The surgical margin atthe retroperitoneal aspect was invaded by malignantcells. Lymph node metastasis was evident around thesplenic vein. The patient had an uneventful postopera-tive course and was discharged on postoperative day 76.She was able to lead a normal and active life until herserum levels of CEA and CA19-9 both became elevatedagain, with increasing back pain, 7 months after theoperation. Follow-up CT showed local recurrence andperitoneal dissemination with ascites. Cytology of theascites showed malignant cells. She died of local recur-rence and peritoneal dissemination 10 months after theoperation.
Case 2: Invasive Ductal Carcinoma of the Bodyof the Pancreas
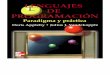
A 61-year old Japanese man presented to a local hospi-tal with a 3-month history of abdominal pain and bodyweight loss of 7kg. CT scan showed a low-density massin the body of the pancreas and the patient was referredto our hospital for surgery. On admission, a hard mass,the size of a man’s first, was palpated in the left hypo-chondrium. Serum chemistry was within normal limits,including the serum levels of CEA and CA19-9. A 75gglucose tolerance test (GTT) showed a diabetic pattern,and CT showed a low-density mass, 3cm in diameter, inthe body of the pancreas with obstructive pancreatitis inthe distal pancreas (Fig. 1). Angiography showed en-casement of the celiac axis, and left gastric and commonhepatic arteries, but the superior mesenteric artery and
Fig. 1. Computed tomography showed a low-density mass(arrow) in the body of the pancreas invading the commonhepatic and splenic arteries and celiac axis

875K. Yamaguchi et al.: Appleby Operation for Pancreas Cancer
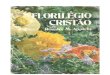
portal vein were free from encasement. ERCP showedcomplete obstruction of the main pancreatic duct in thebody of the pancreas. Cytology of the pancreatic juicerevealed adenocarcinoma. A laparotomy was doneunder the tentative diagnosis of ductal carcinoma of thebody of the pancreas invading the celiac axis (Fig. 2).Before surgery, the patient was fully informed of hiscondition and of the operative risks.
On opening the abdomen, no peritoneal dissemina-tion or hepatic metastasis were found. FollowingKocher’s maneuver, the superior mesenteric artery wastaped and the hepatic arterial flow was confirmed in thehepatoduodenal ligament after transient clamping ofthe common hepatic artery. The Appleby operation wasperformed with intraoperative radiation (20Gy) deliv-ered to the retroperitoneal aspect. Histopathologicexamination of the resected specimen showed well tomoderately differentiated adenocarcinoma of the bodyof the pancreas. The splenic vein was invaded by thecarcinoma, but the arteries were spared microscopi-cally. The surgical margin at the retroperitoneal aspectwas invaded by malignant cells. A lymph node fromaround the splenic vein (No. 11) was metastasized bycarcinoma cells, but the other lymph nodes dissectedwere free from metastases (Nos. 3, 4, 10, 16).
The patient had an uneventful postoperative courseand was discharged on postoperative day 27. He had anormal life until abdominal distension with ascitesdeveloped 5 months after the operation. Back painalso developed and his serum CA19-9 levels increased.CT revealed peritoneal dissemination with ascites,the cytology of which showed malignant cells. He diedof peritoneal dissemination 14 months after theoperation.
Case 3: Invasive Ductal Carcinoma of the Bodyof the Pancreas
A 60-year-old Japanese man who was being followed upfor hepatitis C was found to have a pancreatic bodymass on US and CT. His serum levels of CEA andCA19-9 were 6.7 ng/ml and 73U/ml, respectively. Noabnormal physical findings were evident on admission.Laboratory data showed glucose intolerance and mildliver dysfunction. US, CT, and magnetic resonance im-aging (MRI) showed a mass in the body of the pancreas,3cm in diameter, and chronic obstructive pancreatitisdistal to the mass. The mass was close to the splenicartery and vein and celiac axis, but there was no encase-ment of the vessels on angiography. ERP showed com-plete obstruction of the main pancreatic duct in thebody of the pancreas, and cytology of the pancreaticjuice revealed malignant cells. An upper gastrointesti-nal X-ray series showed compression of the stomach bythe pancreatic tumor. A laparotomy was done under thediagnosis of pancreatic body carcinoma. The patientwas fully informed of the disease and operative risks.
At laparotomy, the pancreatic mass was adherent tothe celiac axis, common hepatic artery, and splenicvessels. Following Kocher’s maneuver, the celiac arteryand superior mesenteric artery were taped and satisfac-tory hepatic arterial flow was confirmed by palpation ofthe hepatoduodenal ligament after transient clampingof the common hepatic artery. The Appleby operation,which consisted of total gastrectomy, subtotal pancre-atectomy, and splenectomy, was performed, and intra-operative radiation (20 Gy) was delivered toward thepancreatic bed. The postoperative histopathologic diag-nosis was well to moderately differentiated adenocarci-noma of the body of the pancreas. The splenic vein wasinvaded by the carcinoma, but the celiac, commonhepatic, and splenic arteries were free of invasion. Theretroperitoneal surgical margin was positive for malig-nant cells. Three lymph nodes around the splenic veinwere metastasized by the adenocarcinoma.
The patient suffered from pneumonia postopera-tively, but recovered with medical treatment and wasdischarged on postoperative day 85. He returned homeand was followed up in the outpatient department everyweek for 6 months after the operation. About 3 monthsafter surgery, CT revealed multiple liver metastases,and the serum levels of CEA and CA19-9 were alsoincreased. He did not complain of any abdominal orback pain, but died of liver metastases 8 months afterhis operation.
Discussion
The purpose of the Appleby operation is to controlretroperitoneal invasion of pancreatic cancer by dis-
Fig. 2. Computed tomography showed a celiac axis stump(arrow). The body and tail of the pancreas were notrecognized

876 K. Yamaguchi et al.: Appleby Operation for Pancreas Cancer
secting the celiac, common hepatic, and splenic arteries.The indications for this operation in the treatment ofcarcinoma of the body and tail of the pancreas are asfollows:
1. The tumor is confined to the body and tail of thepancreas without invasion to the head
2. There is no invasion to the proper hepatic artery orsuperior mesenteric artery
3. The celiac axis can be resected at the root and thecommon hepatic artery can be resected before thebranching point of the gastroduodenal artery
4. Complete retroperitoneal clearance of the carci-noma is possible
5. Pulsation of the proper hepatic artery is verifiedintraoperatively after clamping the common hepaticartery
When retroperitoneal invasion is extensive, even if theceliac axis is divided, not only macroscopic, but alsomicroscopic cancer cells remain in the retroperitonealaspect, which are difficult to control, as in our threepatients. Therefore, the retroperitoneal margin shouldbe examined by preoperative imaging and intraopera-tive frozen section. The retroperitoneal surgical marginwas positive for malignant cells in all of our three pa-tients. Two patients had peritoneal dissemination withmalignant ascites and the other one had multiple livermetastases after the operation. Therefore, completeclearance of the retroperitoneum seems to be very diffi-cult, even with this radical operation. Ozaki et al.13 pro-posed that giving radiation therapy during and after theoperation, which might help to prevent tumor recur-rence, should be considered for patients with advancedpancreatic carcinoma. In the present series, two patientsreceived intraoperative radiation therapy for the retro-peritoneal aspect, but they died 8 and 14 months post-operatively, respectively.
To our knowledge, the Appleby operation has beenreformed for pancreatic body-tail carcinoma in 14 pa-tients, including our 3 (Table 1).8–15 These 14 patientsconsisted of 7 men and 7 women with an average age of58.1 years (range 43–74 years). The vessels involvedwere the celiac axis in 7 patients, the common hepaticartery in 10, the splenic artery in 12, and the SMA in 3.The portal vein was invaded by tumors in 3 patients, 4patients had gastric invasion, and 2 patients had co-existing gastric carcinomas. Portal vein resection wasperformed in 3 patients. The histologic diagnosis wasadenocarcinoma in 9 patients, mucinous cystadenocar-cinoma in 2, and unknown in the other 3. Four patientssurvived for periods ranging from 1 month to 13 yearsafter the operation, the average survival period being50.5 � 35.2 months, and 8 patients died from 21 daysto 12 months after the operation, the average survivalperiod being 5.7 � 1.5 months. The clinical outcome was
not documented for the other 2 cases. Thus, the clinicalcourse of patients with pancreatic body-tail carcinomaremains poor even after the Appleby operation.
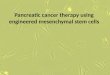
At the time of the Appleby operation, proper hepaticarterial flow after resection of the celiac axis should besupplied by the superior mesenteric artery. However, insome patients, hepatic arterial flow becomes very weakafter resection of the celiac axis. This abrupt reductionin hepatic arterial blood flow can cause postoperativecomplications, such as severe liver dysfunction or gall-bladder necrosis. Therefore, confirmation of hepaticarterial flow after ligation of the common hepatic arteryis mandatory to prevent such ischemic events. A bal-loon occlusion test under angiographic guidance hasbeen proposed. During balloon occlusion of the com-mon hepatic artery, superior mesenteric angiography isperformed to confirm the presence of hepatic arterialflow via the pancreatoduodenal arcade from the supe-rior mesenteric artery (Fig. 3). This method may help toconfirm hepatic artery flow after ligation of the commonhepatic artery perioperatively. On the other hand,Kondo et al.16 proposed preoperative coil embolizationof the common hepatic artery, to improve the hepaticblood collateral and increase the resectability of theAppleby operation. In the present series, the commonhepatic artery was clamped with a bulldog clamp andthe hepatic flow was confirmed by palpation of thehepatoduodenal ligament during the operation. Therewere no complications related to ischemia of the liver orgallbladder.
Some modifications of the Appleby operations havebeen reported.17–19 Nagino et al.17 preserved the stomachin the Appleby operation in patients without direct
Table 1. Summary of the 14 reported cases of the Applebyoperation for pancreatic body-tail carcinoma
Age (years) 43–74 (58.1 � 2.4)M/F 7/7Invasion
Stomach 4/14CHA 10/14CA 7/14SpA 12/14SMA 3/14PV 3/14SMV 2/14
Combined resection PV: 3, SMV: 1, CHA: 1Histology Adenocarcinoma: 9
Cystadenocarcinoma: 2Not available: 3
Prognosis Alive: 4 (1 month–13 years)Dead: 8 (21 days–12 months)Not available: 2
CHA, common hepatic artery; CA, celiac artery; SpA, splenic artery;SMA, superior mesenteric artery; PV, portal vein; SMV, superiormesenteric vein

877K. Yamaguchi et al.: Appleby Operation for Pancreas Cancer
invasion to the stomach. Takenaka et al.18 reported amodified Appleby procedure with direct anastomosis ofthe stumps of the celiac axis and common hepatic ar-tery, which made the procedure safer. Hishinuma et al.19
also reported the cases of two patients with pancreaticcarcinoma who underwent distal pancreatectomy com-bined with resection of the celiac artery and preserva-tion of the stomach, emphasizing the importance ofpreserving the stomach to improve quality of life. Thesestomach-preserving modifications should be differen-tiated from the conventional Appleby operation. Re-cently, Johnson et al.20 emphasized that carcinoma ofthe body is more likely to encroach on the pancreaticneck, and recommended total pancreatectomy forsuch lesions if the patient is in good general condi-tion. Matsumoto et al.21 reported a high incidence ofdiabetes mellitus after the Appleby operation forgastric cancer, with increasing occurrence year afteryear. Therefore, patients who undergo the Applebyoperation should be carefully followed up long after theoperation.
We conclude that the indications for the Applebyoperation to treat locally advanced pancreatic bodycarcinoma are limited because the clinical outcomeremains dismal after this operation. On the other hand,quality of life and outcome after chemoradiation haveimproved.
Fig. 3. A balloon occlusion test showed that the commonhepatic artery was occluded by the balloon (arrow). A supe-rior mesenteric arteriography showed hepatic arterial flow viathe pancreatoduodenal arcade from the superior mesentericartery
References
1. Tsiotos GG, Farnell MB, Sarr MG. Are the results of pancreate-ctomy for pancreatic cancer improving? World J Surg 1999;23:913–9.
2. Yamaguchi K, Enjoji M. Carcinoma of the pancreas: a clinico-pathologic study of 96 cases with immunohistochemical observa-tions. Jpn J Clin Oncol 1989;19:14–22.
3. Yamaguchi K, Shimizu S, Yokohata K, Noshiro H, Chijiiwa K,Tanaka M. Pancreatic carcinoma: reappraisal of surgicalexperiences in one Japanese University Hospital. Hepato-Gastroenterology 1999;46:3257–62.
4. Sohn TA, Yeo CJ, Cameron JL, Koniaris L, Kaushal S, AbramsRA, et al. Resected adenocarcinoma of the pancreas — 616 pa-tients: results, outcomes, and prognostic indicators. J GastrointestSurg 2000;4:567–79.
5. Lillemoe KD, Kaushal S, Cameron JL, Sohn TA, Pitt HA,Yeo CJ. Distal pancreatectomy: indications and outcomes in 235patients. Ann Surg 1999;229:693–8.
6. The Pancreatic Cancer Registration Committee of the JapanPancreas Society. The present status of pancreatic cancer regis-tration. Gann Monogr Cancer Res 1995;43:107–16.
7. Appleby L. The coeliac axis in the expansion of the operation forgastric carcinoma. Cancer 1953;6:704–7.
8. Nimura Y, Hattori T, Miura K, Nakashima N, Hibi M. Resectionof advanced pancreatic body-tail carcinoma by Appleby’s opera-tion. (in Japanese). Shujutu 1976;30:885–9.
9. Wada T, Konishi T. Application of Appleby’s operationfor double cancer of the stomach and the pancreatic body (inJapanese). Gekashinryou 1977;19:1299–301.
10. Hishida Y. Combined resection of the major vessels — pancreaticresection and retroperitoneal clearance (in Japanese). Geka1979;41:319–23.
11. Imaizumi T, Nakamura M, Takada T, Fukushima Y, Suzuki S,Yoshikawa T, et al. A case of pancreatic body and tail carcinomaresected by Appleby’s operation (in Japanese). Geka 1979;41:532–7.
12. Fujita T, Imaizumi T, Yoshikawa T, Miyagawa S, Hanyu H. Aresected pancreatic body and tail carcinoma by Appleby’s opera-tion with portal vein resection (in Japanese with English abstract).Suizo 1987;2:122–8.
13. Ozaki H, Kinoshita T, Kosuga T, Yamamoto J, Shimada K,Inoue K, et al. An aggressive therapeutic approach to carcinomaof the body and tail of the pancreas. Cancer 1996;77:2240–5.
14. Kimura W, Han I, Furukawa Y, Sunami E, Futakawa N,Inoue T, et al. Appleby operation for carcinoma of the bodyand tail of the pancreas. Hepato-Gastroenterology 1997;44:387–93.
15. Yamamori H, Tasiro A, Morisima T, Otsubo Y, Sugiura T, HayaiE, et al. Dissection of lymph nodes of no. 14 and no. 16 in thecarcinoma of the tail of the pancreas (in Japanese). Proc 23rdNihon Suisetu Kenkyukai 1996:118–9.
16. Kondo S, Katoh H, Shimizu T, Omi M, Hirano S, Ambo Y, et al.Preoperative embolization of the common hepatic artery inpreparation for radical pancreatectomy for pancreas body cancer.Hepato-Gastroenterology 2000;47:1447–9.
17. Nagino M, Nimura Y, Hayakawa N, Kamiya J, Kondo S.Appleby’s operation for pancreas cancer (in Japanese). Tan to Sui1991;12:1361–8.
18. Takenaka H, Iwase K, Ohshima S, Hiranaka T. A new techniquefor the resection of gastric cancer: modified Appleby procedurewith reconstruction of hepatic artery. World J Surg 1992;16:947–51.
19. Hishinuma S, Ogata Y, Matusui J, Ozawa I, Inada T, Shimizu H,et al. Two cases of cancer of the pancreatic body undergoinggastric preservation with distal pancreatectomy combined withresection of the celiac axis (in Japanese with English abstract).Nippon Shoukaki Geka Gakkai Zasshi 1991;24:2782–6.

878 K. Yamaguchi et al.: Appleby Operation for Pancreas Cancer
20. Johnson C, Schwall G, Flechtenmacher J, Trede M. Resection foradenocarcinoma of the body and tail of the pancreas. Br J Surg1993;80:1177–9.
21. Matsumoto H, Miwa K, Tsugawa K, Segawa M, Fushida S,Yonemura Y, et al. Evaluation regarding effect and quality of
life after distal pancreatectomy combining total gastrectomy(in Japanese). Nippon Geka Gakkai Zasshi 1993;94:1244–8.