Embed Size (px)
Citation preview
Author(s):PatrickCarter,DanielWachter,RockefellerOteng,CarlSeger,2009-2010.License:Unlessotherwisenoted,thismaterialismadeavailableunderthetermsoftheCreativeCommonsAttribution3.0License:http://creativecommons.org/licenses/by/3.0/
WehavereviewedthismaterialinaccordancewithU.S.CopyrightLawandhavetriedtomaximizeyourabilitytouse,share,andadaptit.Thecitationkeyonthefollowingslideprovidesinformationabouthowyoumayshareandadaptthismaterial.Copyrightholdersofcontentincludedinthismaterialshouldcontactopen.michigan@umich.eduwithanyquestions,corrections,orclarificationregardingtheuseofcontent.Formoreinformationabouthowtocitethesematerialsvisithttp://open.umich.edu/education/about/terms-of-use.Anymedicalinformationinthismaterialisintendedtoinformandeducateandisnotatoolforself-diagnosisorareplacementformedicalevaluation,advice,diagnosisortreatmentbyahealthcareprofessional.Pleasespeaktoyourphysicianifyouhavequestionsaboutyourmedicalcondition.Viewerdiscretionisadvised:Somemedicalcontentisgraphicandmaynotbesuitableforallviewers.
CitationKeyformoreinformationsee:http://open.umich.edu/wiki/CitationPolicy
Use+Share+Adapt
MakeYourOwnAssessment
CreativeCommons–AttributionLicense
CreativeCommons–AttributionShareAlikeLicense
CreativeCommons–AttributionNoncommercialLicense
CreativeCommons–AttributionNoncommercialShareAlikeLicense
GNU–FreeDocumentationLicense
CreativeCommons–ZeroWaiver
PublicDomain–Ineligible:WorksthatareineligibleforcopyrightprotectionintheU.S.(USC17§102(b))*lawsinyourjurisdictionmaydiffer
PublicDomain–Expired:Worksthatarenolongerprotectedduetoanexpiredcopyrightterm.
PublicDomain–Government:WorksthatareproducedbytheU.S.Government.(USC17§105)
PublicDomain–SelfDedicated:Worksthatacopyrightholderhasdedicatedtothepublicdomain.
FairUse:UseofworksthatisdeterminedtobeFairconsistentwiththeU.S.CopyrightAct.(USC17 § 107)*lawsinyourjurisdictionmaydifferOurdeterminationDOESNOTmeanthatallusesofthis3rd-partycontentareFairUsesandweDONOTguaranteethatyouruseofthecontentisFair.Tousethiscontentyoushoulddoyourownindependentanalysis todeterminewhetherornotyourusewillbeFair.
{Contentthecopyrightholder,author,orlawpermitsyoutouse,shareandadapt.}
{ContentOpen.Michiganbelievescanbeused,shared,andadaptedbecauseitisineligibleforcopyright.}
{ContentOpen.MichiganhasusedunderaFairUsedetermination.}
Advanced Emergency Trauma Course
GhanaEmergencyMedicineCollaborativePatrickCarter,MD∙DanielWachter,MD∙RockefellerOteng,MD∙CarlSeger,MD
Shock
Presenter:CarlSeger,MD
Overview Introduction• Definition• Physiology
InitialPatientAssessment• Recognize
TypesofShock ClassesofHemorrhagicShock TreatingHemorrhagicShock• Fluid/BloodResuscitation• EvaluatingtreatmentofShock
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Introduction
Inordertotreatshockappropriately,itmustfirstberecognized,thenidentifythecause
Inordertorecognizeit,itisimportanttounderstandsomeofthephysiologyofthediseaseprocess
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Definition Aphysiologicalstatethatresultsininadequateorganperfusionandtissueoxygenation Downwardspiralofimpairedperfusionleadingtoimpairedfunction
Resultsinmultipleorganfailureanddeath
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Basic Physiology OxygenDelivery=COxarterialcontentofO2 CardiacOutput=HRxStrokeVolume StrokeVolumeisafunction• Preload• Afterload• MyocardialContractility
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Pathophysiology
Bloodloss• Releaseofendogenouscatecholamines
Increasecardiacoutput• Increaseheartrate• Vasoconstrictionoflessvitalorgans
skin,muscle ResultsinhigherdiastolicBP(narrowPP)
Continuetoperfusevitalorgansaslongaspossible(brain,heart,kidney)
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Initial Patient Assessment
RecognitionofShock• Clinicalsignsandsymptomsdependsontheseverityoftheshock• Earlymanifestationsincludetachycardiaandcutaneousvasoconstriction
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Clinical Pathophysiology of Shock
General/Vitalsigns Cardiovascular-tachycardia Skin-vasoconstrictionvs.vasodilation Respiratory-increasedRR Urinary-decreaseurineoutput Neurologic-confusion,agitation Extremities-coldvs.warm
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Clinical Endpoints of Shock
END-STAGE SHOCK Bradycardia Arrythmias
Death
DECREASED BLOOD FLOW TO BRAIN AND HEART Restless, agitated, confused, lethargy
Hypotension Tachycardia Tachypnea
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Classifying Shock Hypovolemic• Hemorrhagic
Distributive/Vasogenic• Sepsis,Anaphylactic
Cardiogenic Neurogenic• Spinalcordinjury
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
SIRS Systemic Inflammatory Response Syndrome -SIRS
• Defined by the presence of two or more of the following: Body temp < 36 °C (97 °F) or > 38 °C (100 °F) Heart Rate > 90 bpm RR > 20 bpm WBC < 4,000 cells/mm3 or > 12,000 cells/mm3 (<
4 × 109 or > 12 × 109 cells/L), or greater than 10% band
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Sepsis and Septic Shock
Sepsis-DefinedasSIRSinresponsetoaconfirmedinfectiousprocess.
Septicshock-Definedassepsiswithrefractoryarterialhypotensionorhypoperfusionabnormalitiesinspiteofadequatefluidresuscitation.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourseGhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Septic Shock Abloodborneinfectionwidelydisseminatedtomanyareasofthebody
Commonfeaturesarehighfever,vasodilatation(especiallyinaffectedtissues)
Sludgingoftheblood,andRBCagglutinationresultinginDIC
http://en.wikipedia.org/wiki/File:Staphylococcus_aureus_Gram.jpg
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Anaphylactic Shock AnIgEmediatedeventthattriggersmassivereleaseofimmuneresponsemediators
Resultsinwidespreadperipheralvasodilation,bronchialsmoothmusclecontraction,andlocalvasculardilatation
JustinBeck(flickr)
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Cardiogenic Shock Keyelementsarehypotension(SBP<90)andhypoperfusionwithpulmonarycongestion
Mortalityis50-80%beforereperfusiontherapy Acutemyocardialischemiaismostcommoncause
PatrickJ.Lynch,medicalillustrator;C.CarlJaffe,MD,cardiologist(Wikipedia)GhanaEmergencyMedicineCollaborative
AdvancedEmergencyTraumaCourse
Neurogenic Shock Resultofspinalcordinjury Lossofsympathetictone Decreasedvasomotortone Resultsinhypotensionandbradycardia
Patientsmayremainalert,warm,anddrydespitethehypotension
PhotoofChristopherReevetakenbygunkyboy(Wikipedia)
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Case 1 29y/omale,PVAwhilecrossingthestreet,awake,complainingofseverebackpain,andinabilitytomoveorfeelhislegs HR45RR25BP100/45Sa0298%T34.0
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

What do we do next?
Maintain ventilation
Enhance perfusion
Treat underlying cause
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
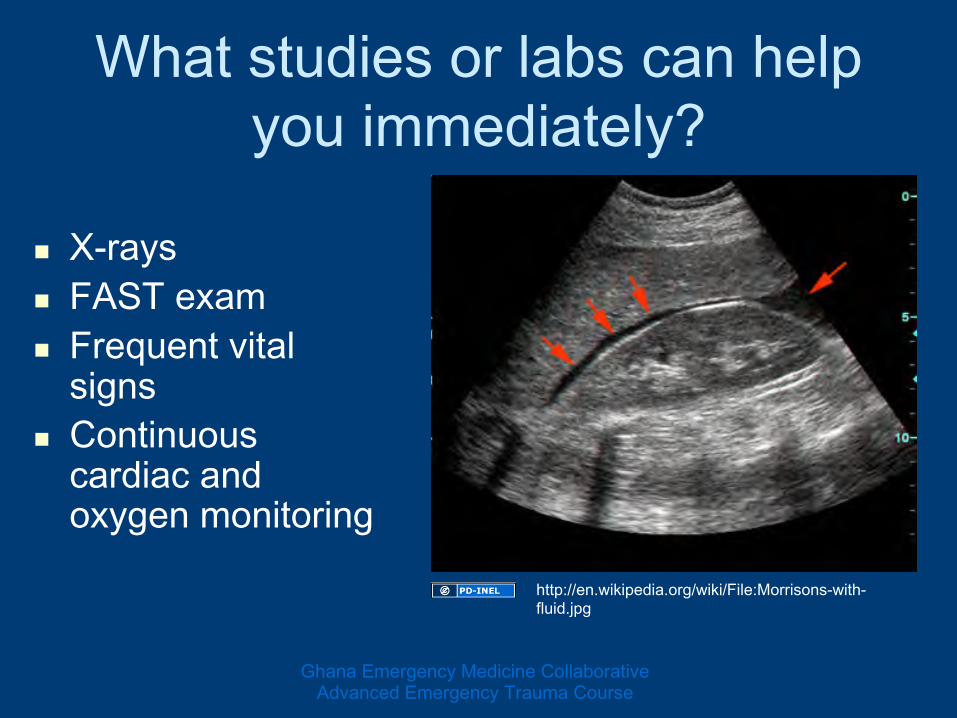
What studies or labs can help you immediately?
X-rays FASTexam Frequentvitalsigns
Continuouscardiacandoxygenmonitoring
http://en.wikipedia.org/wiki/File:Morrisons-with-fluid.jpg
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
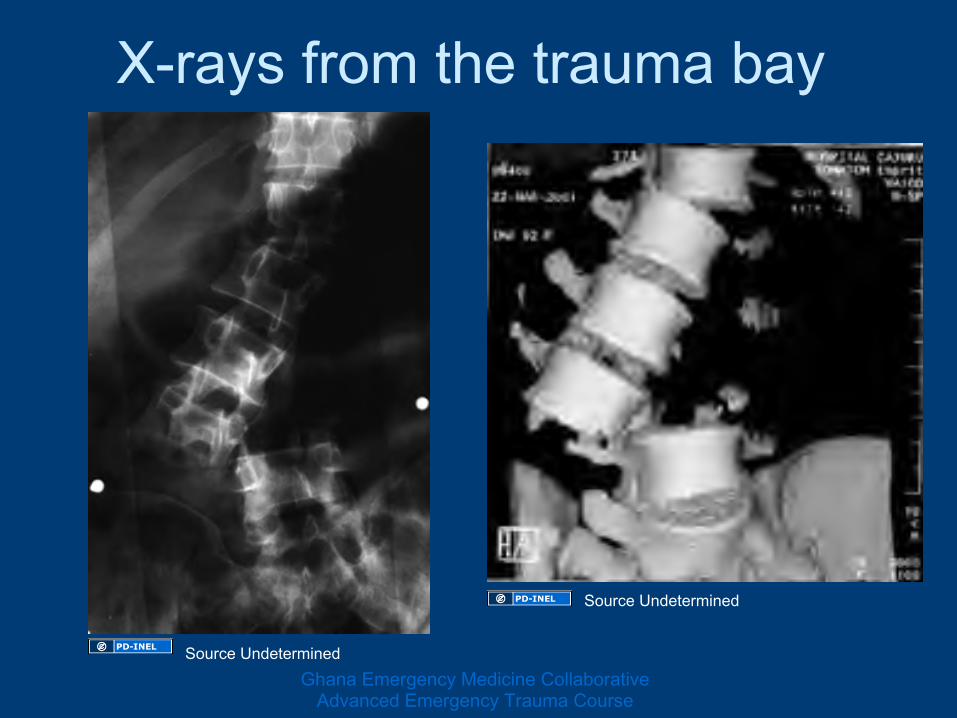
X-rays from the trauma bay
SourceUndetermined
SourceUndeterminedGhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Neurogenic Resuscitation
Adequateoxygenation Assessbreathing Maximizecirculation• IVfluidsorblood• Pressorsifnecessary
Supportheartrateifneeded• Atropine
PreparefortheOR
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Hypovolemic
Hemorrhagic• Mostlytraumatic• Focusoftoday
Severeburn GIlosses• vomitinganddiarrhea
Urinary• DKA
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
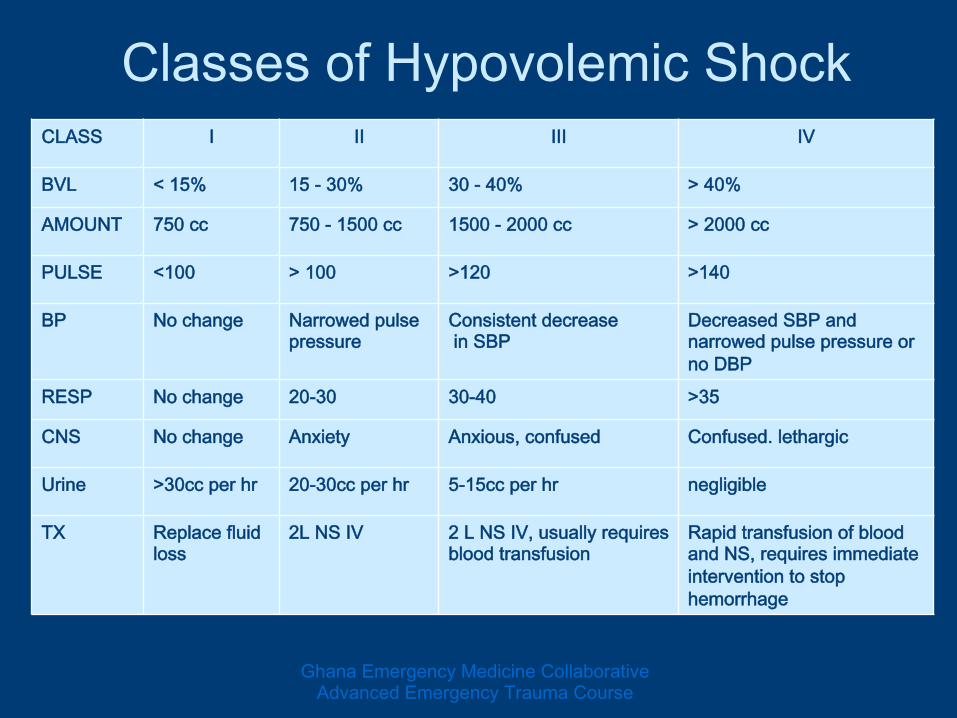
Classes of Hypovolemic Shock CLASS I II III IV
BVL <15% 15-30% 30-40% >40%
AMOUNT 750cc 750-1500cc 1500-2000cc >2000cc
PULSE <100 >100 >120 >140
BP Nochange Narrowedpulsepressure
ConsistentdecreaseinSBP
DecreasedSBPandnarrowedpulsepressureornoDBP
RESP Nochange 20-30 30-40 >35
CNS Nochange Anxiety Anxious,confused Confused.lethargic
Urine >30ccperhr 20-30ccperhr 5-15ccperhr negligible
TX Replacefluidloss
2LNSIV 2LNSIV,usuallyrequiresbloodtransfusion
RapidtransfusionofbloodandNS,requiresimmediateinterventiontostophemorrhage
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Treating Hemorrhagic Shock
AsalwaysABC’s• AirwayandBreathing
WouldpreferO2satgreaterthan95% PlacingO2onthepatient
• Circulation HemorrhageControl VascularAccess,LargeboreIVx2
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Monitoring Continuousmonitoring OxygenSaturation Urineoutput
LRHopson,2005
SourceUndetermined
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Treating Hemorrhagic Shock
Identify&reversethecause Restoretissueperfusion Restoreorganfunction
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Initial Fluid Therapy AdultwithnormalCardiacFunction• 1to2LitersofLRorNSrapidly
Pediatric• 20ml/kgofLRorNSrapidly
Evaluatepatientsresponsetofluid
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Evaluation of Treatment Assessorganperfusion• Urinaryoutput• MentalStatus• Skinexam• Vitals
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
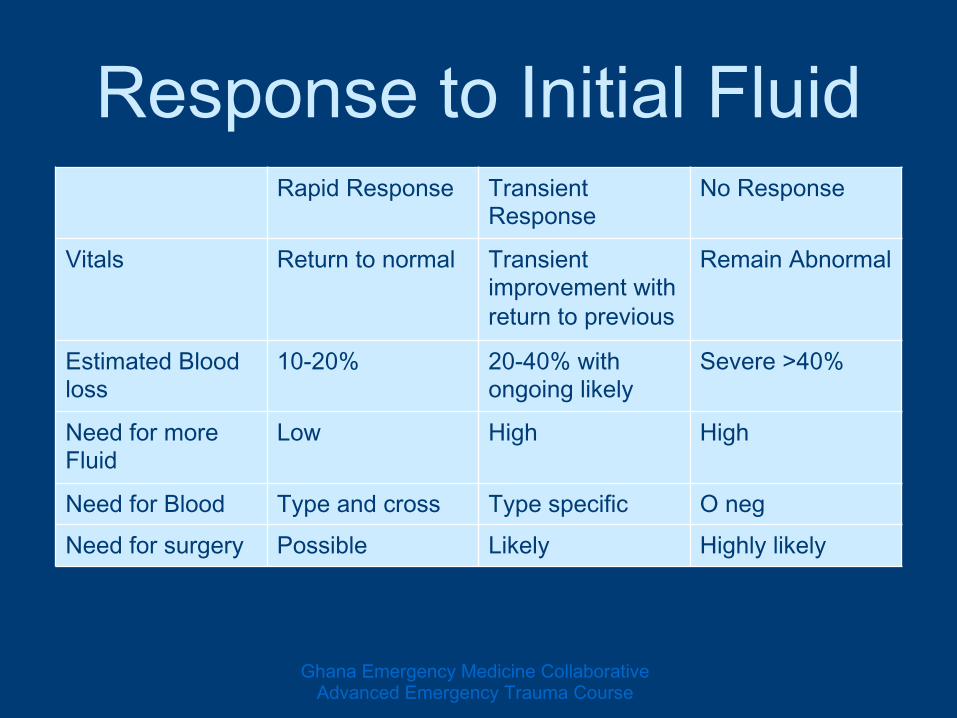
Response to Initial Fluid RapidResponse Transient
ResponseNoResponse
Vitals Returntonormal Transientimprovementwithreturntoprevious
RemainAbnormal
EstimatedBloodloss
10-20% 20-40%withongoinglikely
Severe>40%
NeedformoreFluid
Low High High
NeedforBlood Typeandcross Typespecific OnegNeedforsurgery Possible Likely Highlylikely
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Case 2 25yearoldmaleinaheadonmotorvehicleaccident.HehassustainedobviouschestandabdominaltraumaandhasaGCSof13.
VS:HR125RR28BP100/50T36.0Sa0293%on100%
Patientisagitatedandconfused.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
What class of Shock? ClassIII ABC IVAccess 2litersofNS
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Case #2 cont
PatientsVitalsafter2liters:• HR95RR25BP110/70
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Case #3 17y/omalecutshisinnerthighwithasickle• Presentshemorrhagingfromleftgroinarea• AwakeandAlert• VS:BP120/60HR120RR30Sat98%onRA• PthaspulsedistallyinLtLeg
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
What to do?
ABC• DirectPressuretobleedingarea• IVAccess• 2LitersNS
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Case #3 After2Liters• Havingdifficultycontrollingbleeding• VitalSigns
HR130BP85/60RR30Sat100%onNC
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Case #3
WhatNext?• MoreFluid• Blood• Surgeon?
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
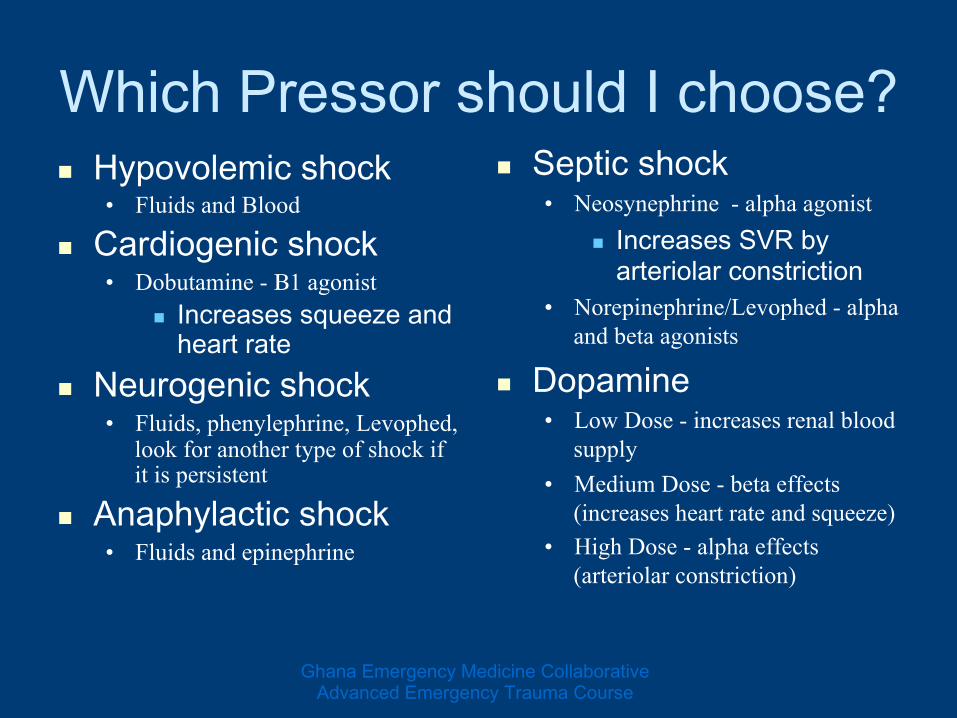
Which Pressor should I choose? Hypovolemicshock
• Fluids and Blood
Cardiogenicshock• Dobutamine - Β1 agonist
Increasessqueezeandheartrate
Neurogenicshock• Fluids, phenylephrine, Levophed,
look for another type of shock if it is persistent
Anaphylacticshock• Fluids and epinephrine
Septicshock• Neosynephrine - alpha agonist
IncreasesSVRbyarteriolarconstriction
• Norepinephrine/Levophed - alpha and beta agonists
Dopamine• Low Dose - increases renal blood
supply • Medium Dose - beta effects
(increases heart rate and squeeze) • High Dose - alpha effects
(arteriolar constriction)
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Overview Introduction• Definition• BasicPhysiology
InitialPatientAssessment• Recognize
TypesofShock ClassesofHemorrhagicShock TreatingHemorrhagicShock• Fluid/BloodResuscitation• EvaluatingtreatmentofShock
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Questions?
Dkscully(flickr)
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
References Rivers,E.,Otero,R.,Nguyen,H.Approachtothepatientinshock,inEmergencyMedicine:AComprehensiveGuide.Tintinalli,Editor.2004,McGraw-Hill.p.219-225.
Manning,J.FluidandBloodResuscitation,inEmergencyMedicine:AComprehensiveGuide.Tintinalli,Editor.2004,McGraw-Hill.p.225-231.
Jui,J.SepticShock,inEmergencyMedicine:AComprehensiveGuide.Tintinalli,Editor.2004,McGraw-Hill.p.231-242.
Peacock,W.,Weber,J.CardiogenicShock,inEmergencyMedicine:AComprehensiveGuide.Tintinalli,Editor.2004,McGraw-Hill.p.242-247.
Rowe,B.,Carr,S.,AnaphylaxisandAcuteAllergicReactions,inEmergencyMedicine:AComprehensiveGuide.Tintinalli,Editor.2004,McGraw-Hill.p.242-252.
Euerle,B.,Scalea,T.NeurogenicShock,inEmergencyMedicine:AComprehensiveGuide.Tintinalli,Editor.2004,McGraw-Hill.p.219-255.
AmericanCollegeofSurgeons.Shock,inAdvancedTraumaLifeSupportforDoctors7thedition.2004.p.62-102.
Mills,T.TraumaResuscitation,inEmergencyMedicine.Adams,Editor.2008,SaundersElsevier.p.77-84





























