Embed Size (px)
Citation preview
BASICS PHYSICS, TECHNICAL ASPECTS
AND RADIOTHERAPY OBJECTIVES OF
PROTON THERAPY
Author: Dr. Kovács Árpád, Simon Mihály
Lecturer: Dr. Kovács Péter

© Dr. Kovács Árpád, Simon Mihály – 2021
The textbook was made with the support of the following tender:
EFOP-3.4.3-16-2016-00005 Korszerű egyetem a modern városban: Értékközpontúság, nyitottság és
befogadó szemlélet egy 21. századi felsőoktatási modellben
ISBN: 978-963-429-658-4
Publisher: Pécsi Tudományegyetem Egészségtudományi Kar
Pécs, 2021.
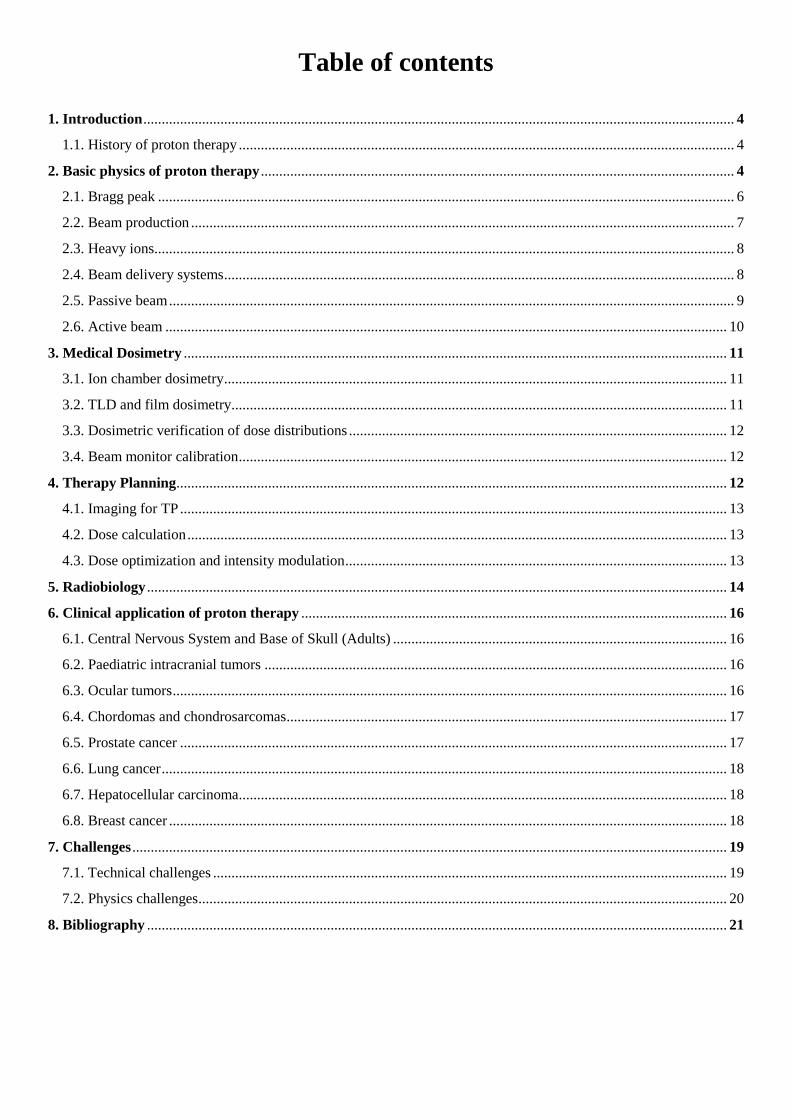
Table of contents
1. Introduction ................................................................................................................................................................. 4
1.1. History of proton therapy ....................................................................................................................................... 4
2. Basic physics of proton therapy ................................................................................................................................. 4
2.1. Bragg peak ............................................................................................................................................................. 6
2.2. Beam production .................................................................................................................................................... 7
2.3. Heavy ions .............................................................................................................................................................. 8
2.4. Beam delivery systems ........................................................................................................................................... 8
2.5. Passive beam .......................................................................................................................................................... 9
2.6. Active beam ......................................................................................................................................................... 10
3. Medical Dosimetry .................................................................................................................................................... 11
3.1. Ion chamber dosimetry ......................................................................................................................................... 11
3.2. TLD and film dosimetry....................................................................................................................................... 11
3.3. Dosimetric verification of dose distributions ....................................................................................................... 12
3.4. Beam monitor calibration ..................................................................................................................................... 12
4. Therapy Planning ...................................................................................................................................................... 12
4.1. Imaging for TP ..................................................................................................................................................... 13
4.2. Dose calculation ................................................................................................................................................... 13
4.3. Dose optimization and intensity modulation ........................................................................................................ 13
5. Radiobiology .............................................................................................................................................................. 14
6. Clinical application of proton therapy .................................................................................................................... 16
6.1. Central Nervous System and Base of Skull (Adults) ........................................................................................... 16
6.2. Paediatric intracranial tumors .............................................................................................................................. 16
6.3. Ocular tumors ....................................................................................................................................................... 16
6.4. Chordomas and chondrosarcomas ........................................................................................................................ 17
6.5. Prostate cancer ..................................................................................................................................................... 17
6.6. Lung cancer .......................................................................................................................................................... 18
6.7. Hepatocellular carcinoma..................................................................................................................................... 18
6.8. Breast cancer ........................................................................................................................................................ 18
7. Challenges .................................................................................................................................................................. 19
7.1. Technical challenges ............................................................................................................................................ 19
7.2. Physics challenges ................................................................................................................................................ 20
8. Bibliography .............................................................................................................................................................. 21

4
1. Introduction
1.1. History of proton therapy
According to the Big Bang Theory roughly 13.4
billion years ago hydrogen was the first element to
form in the Universe. The existence of proton was
demonstrated by Ernest Rutherford in 1919.
Robert Wilson 1946, published an article in 1946
proposing that accelerated protons should be
considered for radiation therapy, he explained the
biophysical rationale for proton therapy. (Wilson
1946). 1954 was the year of the first application of
a proton beam treating a human by UC Lawrence
Berkeley Laboratory, (Lawrence et al 1958).
In the following years a number of techniques,
e.g. proton radiosurgical techniques for brain
tumors developed at the Gustaf-Werner Institute
in 1957 and radiosurgery of small intercranial
targets at Harvard Cyclotron Laboratory
(Kjellberg et al 1962), had been developed.
The process of developing further key
technologies for radiotherapy continued, such as
accelerators, magnetically scanned beams,
computed tomographic imaging and magnetic
resonance imaging. In the 70s-80s several physics
facilities, including PSI in Switzerland, started to
treat patients with proton.
In 1989 the world`s first hospital based proton
beam therapy facility opened in Clatterbridge
Cancer Centre UK with low energy proton beams.
The first high-energy proton beam therapy facility
opened in Loma Linda University Medical Center,
California in 1990.
Based on Particle Therapy Cooperative group
(PTCOG) data in 2018 71 specialized proton
therapy center had been registered worldwide and
the total number of patients treated by this
modality reached 149345 by the end of 2016.
The rationale of proton therapy is strongly related
to radiobiology (Jackel 2009), the possibility of
concentrating the proton beam to the cancer cells
while avoiding or minimizing the radiation effect
to the surrounding normal tissues is called dose
conformation. (Weber et. el 2009) defines the
rationale of proton therapy in its superior spatial
dose distribution in the patient, Weber also found
that the advantage of proton to photon namely
providing highly conformal and uniform dose to
the cancer cells has been wildly lessened by
advances in photon therapy.
However, studies indicates, that the advantage of
proton therapy in normal tissue sparing never been
more apparent or important (Valdivieso et al
2012), approximately 65% of adults and 80% of
children survive 5 years after their cancer
diagnosis.
2. Basic physics of proton therapy
As mentioned before the very first element formed
in the universe was hydrogen and the proton is the
nucleus of the hydrogen atom. It carries the unit of
5
positive charge (1.6 x 10-19
Coulombs) and has a
mass of 1.6 x 10-27
kg which is ~ 1840 times the
mass of one electron.
Given the charge of the protons as they pass
through medium they interact with atomic
electrons and atomic nuclei through Coulomb
force. Nuclear reactions are also possible, but
those are very rare. Interactions based on
Coulomb force can be inelastic collisions with
atomic electrons or elastic scattering. In an
inelastic collision protons lose part of their kinetic
energy to generate ionization and excitation of
atoms.
Proton beams have sharp lateral distribution due
to the fact that heavier charged particles scatter
through much smaller angles, compared to an
electron beam.
1. figure: Schematic illustration of proton interaction mechanisms: (a) energy loss
via inelastic Coulombic interactions, (b) deflection of proton trajectory by repulsive Coulomb elastic
scattering with nucleus, (c) removal of primary proton and creation of secondary particles via non-
elastic nuclear interaction (p: proton, e: electron, n:neutron, γ: gamma rays), (Wayne et al, 2015)
Mass stopping power (energy loss per unit path
length in g/cm2) for protons is greater in low
atomic-number (Z) materials than in high-Z
materials. On a per g/cm2 basis, low-Z materials
are more effective in slowing down protons while
high-Z materials scatter protons through larger
angles than the low-Z materials. Accordingly,
scattering foils should be made of high Z materials
to scatter protons with minimal energy loss and
consequently low z materials should be used when
6
energy decrease is desired with minimal
scattering. A combination of high-Z and low-Z
materials can help to control scattering and
reduction in beam energy. Collisions with nuclei
to produce nuclear reactions are rare. The products
of such collisions are excited nuclei, secondary
protons, neutrons, and, in some cases, α particles.
2.1. Bragg Peak
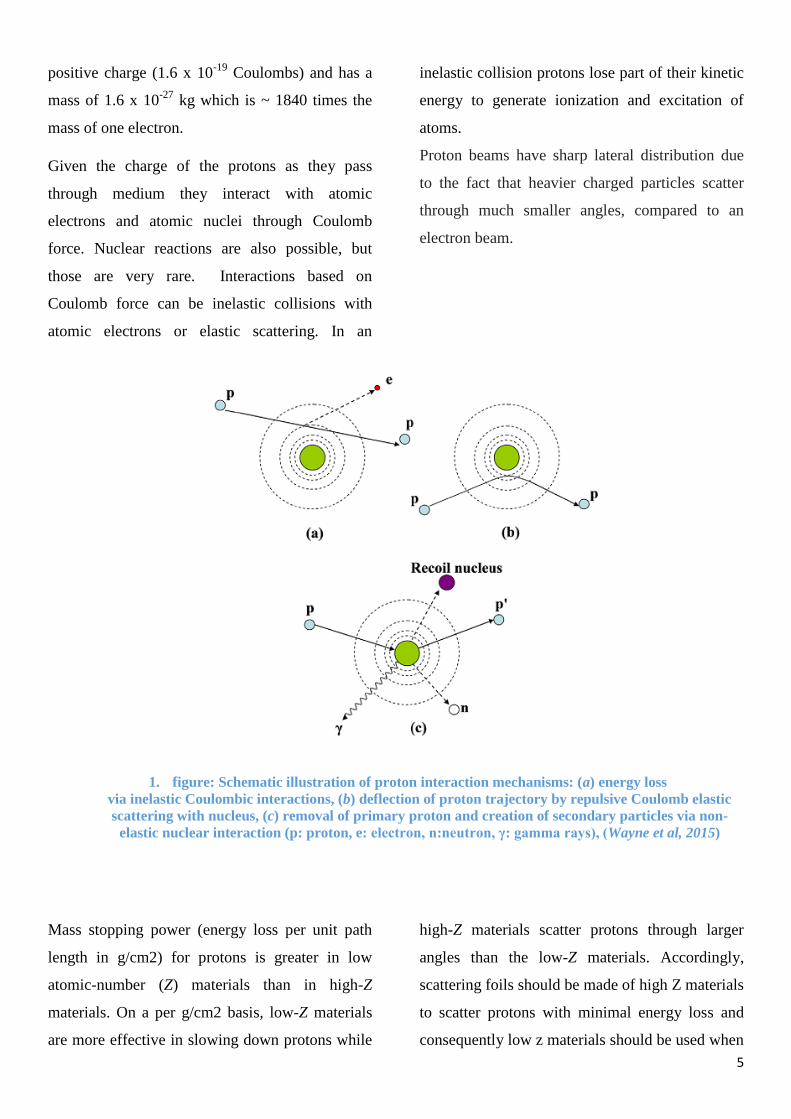
The stopping power is the average rate of energy
loss of a particle per unit path length in a medium.
The linear stopping power is measured in MeVcm-
1. This simply means how much energy is
deposited per cm in the medium by a given
particle. This often referred as the Linear Energy
Transfer (LET) of the particle. The biological
effectiveness of radiation is strongly correlates
with LET.
The rate of energy loss due to ionization of a
charged particle is proportional to the square of
the charge and inversely proportional to the square
of its velocity. In practice as a particle passes
through medium it deposits energy on its` path
and as the velocity of the particle approaches zero
the rate of energy loss becomes maximum. The
depth dose distribution follows this rate of energy
loss.
2. figure: Typical dose deposition as a function of depth for a proton beam
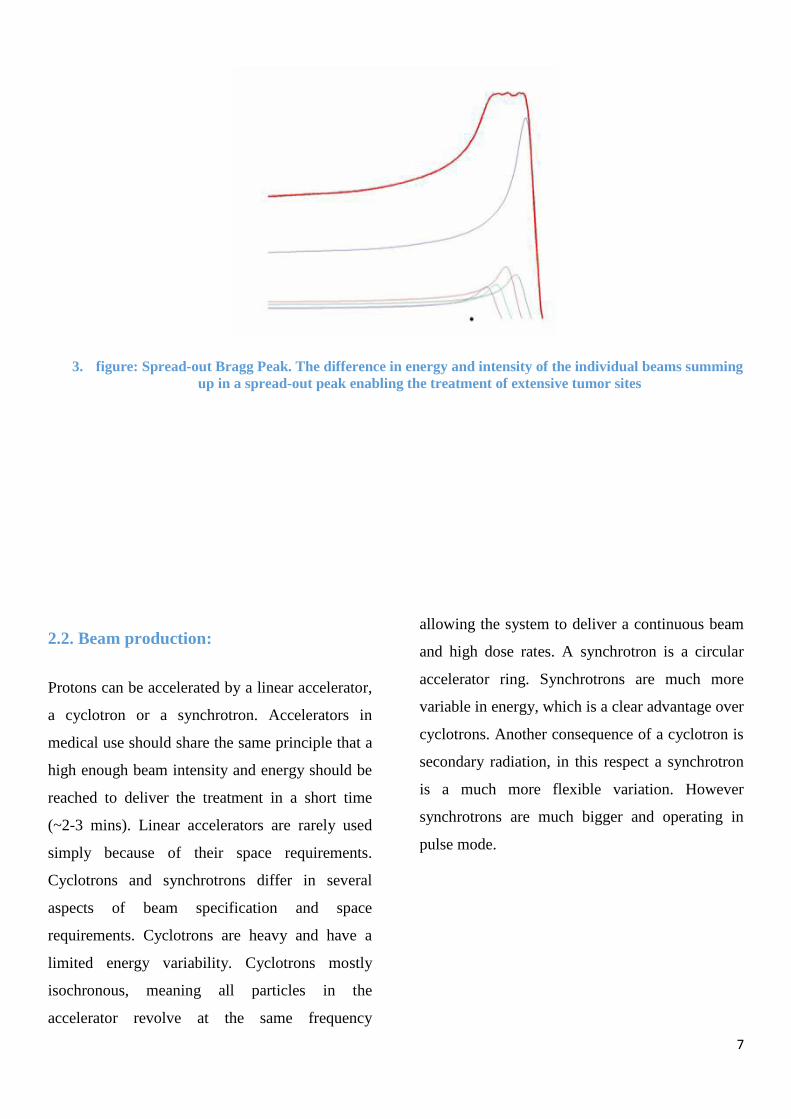
It can be easily seen that a single mono-energetic
proton beam is not capable to cover a treatment
site given the sharp Bragg peak. By adding
weighted proton beams with different energies the
Bragg peaks summing up and create a Spread Out
Bragg Peak (SOBP).
7
3. figure: Spread-out Bragg Peak. The difference in energy and intensity of the individual beams summing
up in a spread-out peak enabling the treatment of extensive tumor sites
2.2. Beam production:
Protons can be accelerated by a linear accelerator,
a cyclotron or a synchrotron. Accelerators in
medical use should share the same principle that a
high enough beam intensity and energy should be
reached to deliver the treatment in a short time
(~2-3 mins). Linear accelerators are rarely used
simply because of their space requirements.
Cyclotrons and synchrotrons differ in several
aspects of beam specification and space
requirements. Cyclotrons are heavy and have a
limited energy variability. Cyclotrons mostly
isochronous, meaning all particles in the
accelerator revolve at the same frequency
allowing the system to deliver a continuous beam
and high dose rates. A synchrotron is a circular
accelerator ring. Synchrotrons are much more
variable in energy, which is a clear advantage over
cyclotrons. Another consequence of a cyclotron is
secondary radiation, in this respect a synchrotron
is a much more flexible variation. However
synchrotrons are much bigger and operating in
pulse mode.
8
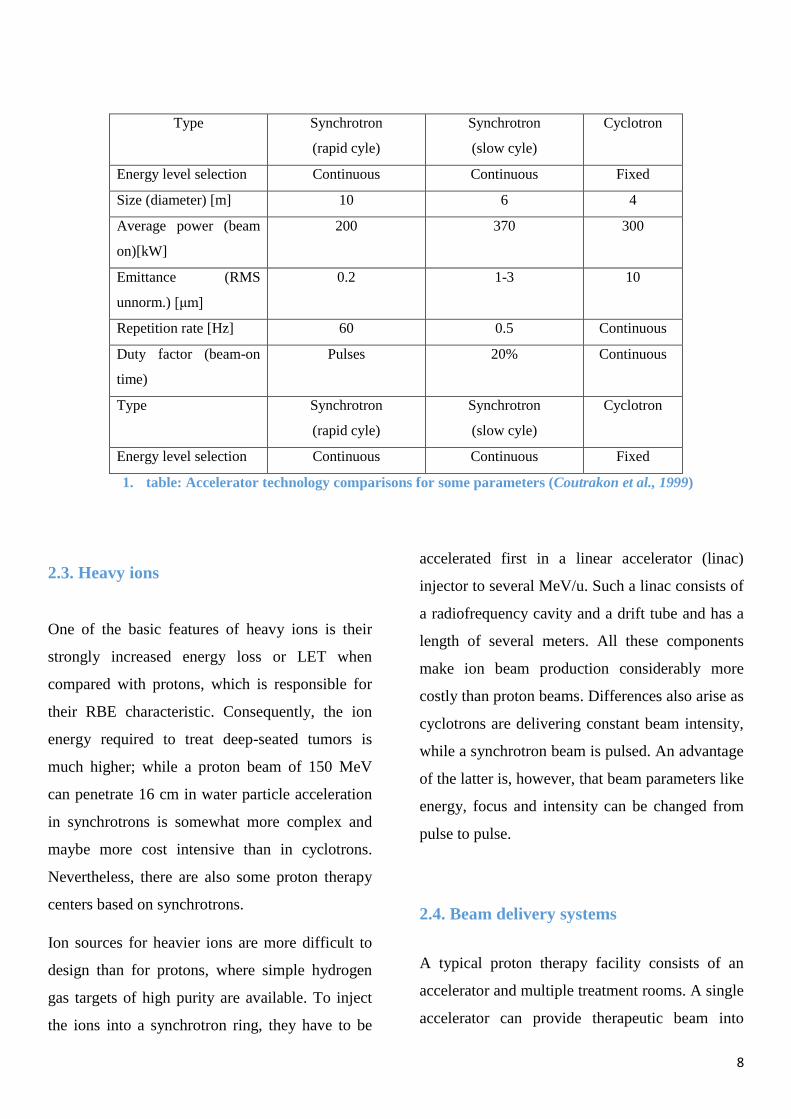
Type Synchrotron
(rapid cyle)
Synchrotron
(slow cyle)
Cyclotron
Energy level selection Continuous Continuous Fixed
Size (diameter) [m] 10 6 4
Average power (beam
on)[kW]
200 370 300
Emittance (RMS
unnorm.) [μm]
0.2 1-3 10
Repetition rate [Hz] 60 0.5 Continuous
Duty factor (beam-on
time)
Pulses 20% Continuous
Type Synchrotron
(rapid cyle)
Synchrotron
(slow cyle)
Cyclotron
Energy level selection Continuous Continuous Fixed
1. table: Accelerator technology comparisons for some parameters (Coutrakon et al., 1999)
2.3. Heavy ions
One of the basic features of heavy ions is their
strongly increased energy loss or LET when
compared with protons, which is responsible for
their RBE characteristic. Consequently, the ion
energy required to treat deep-seated tumors is
much higher; while a proton beam of 150 MeV
can penetrate 16 cm in water particle acceleration
in synchrotrons is somewhat more complex and
maybe more cost intensive than in cyclotrons.
Nevertheless, there are also some proton therapy
centers based on synchrotrons.
Ion sources for heavier ions are more difficult to
design than for protons, where simple hydrogen
gas targets of high purity are available. To inject
the ions into a synchrotron ring, they have to be
accelerated first in a linear accelerator (linac)
injector to several MeV/u. Such a linac consists of
a radiofrequency cavity and a drift tube and has a
length of several meters. All these components
make ion beam production considerably more
costly than proton beams. Differences also arise as
cyclotrons are delivering constant beam intensity,
while a synchrotron beam is pulsed. An advantage
of the latter is, however, that beam parameters like
energy, focus and intensity can be changed from
pulse to pulse.
2.4. Beam delivery systems
A typical proton therapy facility consists of an
accelerator and multiple treatment rooms. A single
accelerator can provide therapeutic beam into

9
several rooms, beam transport is controlled by
magnets to selectively drive a proton beam into
the desired room. The particle beam is focused
and its diameter is kept as small as possible during
the transport, only when it enters the room is
spread out to the required cross section.
4. figure: Schematic drawing of a complex proton beam therapy facility at UCLH
There are two basic methods to shape the beam and to tailor the dose to the target volume
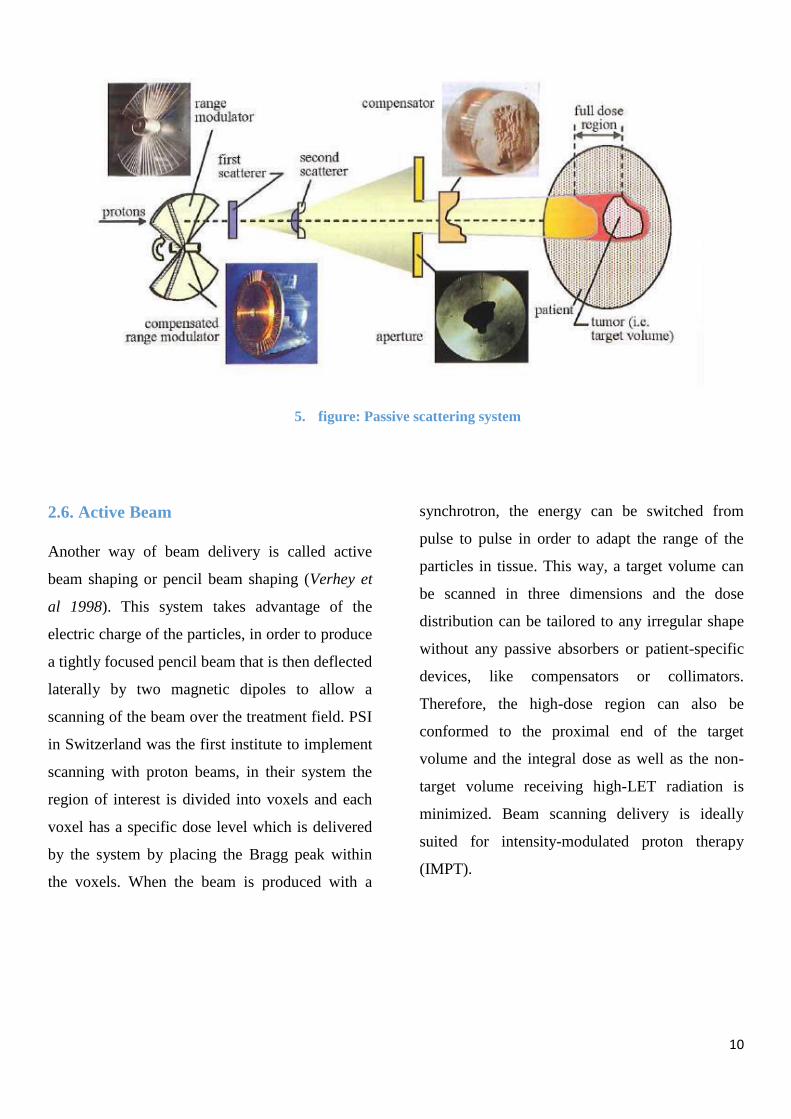
2.5. Passive beam
Passive beam delivery techniques use double-
scattering systems or wobbling magnets in
combination with scatterers to produce large
particle fields (Hug, 2001). The particle field is
then confined to the tumor cross section by
individually manufactured collimators or multileaf
collimators. To generate the SOBP, a rotating
modulator wheel is inserted into the beam. This
device introduces material of varying thickness
into the beam that results in a periodical
modulation of the range. Alternatively, a static
filter of varying thickness may be applied. This
so-called ridge-filter uses bar-ridge energy
absorbers to produce a homogeneous range
modulation over the lateral extension of the
treatment field. Each modulator wheel or ridge
filter is connected to a specific SOBP and is
selected according to the extension of the tumor in
depth. To adjust the SOBP to the distal edge of the
tumor, range shifters are used.
Finally, compensators manufactured for the
individual field of each patient can be used to
adjust the dose distribution to the distal edge of
the tumor. As the extension of the SOBP remains
constant over the tumor cross section, the dose
conformation at the distal edge is connected to
high doses in the normal tissue at the proximal
edge of the tumor (Khan, 2014).
10
5. figure: Passive scattering system
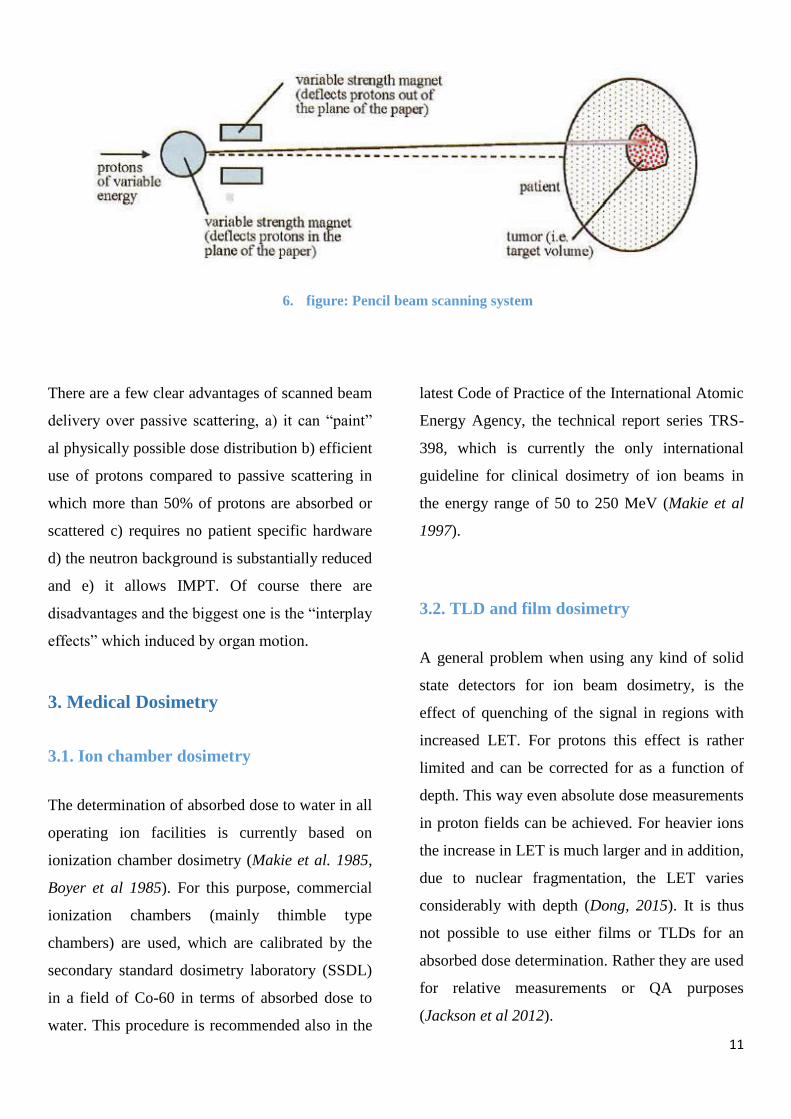
2.6. Active Beam
Another way of beam delivery is called active
beam shaping or pencil beam shaping (Verhey et
al 1998). This system takes advantage of the
electric charge of the particles, in order to produce
a tightly focused pencil beam that is then deflected
laterally by two magnetic dipoles to allow a
scanning of the beam over the treatment field. PSI
in Switzerland was the first institute to implement
scanning with proton beams, in their system the
region of interest is divided into voxels and each
voxel has a specific dose level which is delivered
by the system by placing the Bragg peak within
the voxels. When the beam is produced with a
synchrotron, the energy can be switched from
pulse to pulse in order to adapt the range of the
particles in tissue. This way, a target volume can
be scanned in three dimensions and the dose
distribution can be tailored to any irregular shape
without any passive absorbers or patient-specific
devices, like compensators or collimators.
Therefore, the high-dose region can also be
conformed to the proximal end of the target
volume and the integral dose as well as the non-
target volume receiving high-LET radiation is
minimized. Beam scanning delivery is ideally
suited for intensity-modulated proton therapy
(IMPT).
11
6. figure: Pencil beam scanning system
There are a few clear advantages of scanned beam
delivery over passive scattering, a) it can “paint”
al physically possible dose distribution b) efficient
use of protons compared to passive scattering in
which more than 50% of protons are absorbed or
scattered c) requires no patient specific hardware
d) the neutron background is substantially reduced
and e) it allows IMPT. Of course there are
disadvantages and the biggest one is the “interplay
effects” which induced by organ motion.
3. Medical Dosimetry
3.1. Ion chamber dosimetry
The determination of absorbed dose to water in all
operating ion facilities is currently based on
ionization chamber dosimetry (Makie et al. 1985,
Boyer et al 1985). For this purpose, commercial
ionization chambers (mainly thimble type
chambers) are used, which are calibrated by the
secondary standard dosimetry laboratory (SSDL)
in a field of Co-60 in terms of absorbed dose to
water. This procedure is recommended also in the
latest Code of Practice of the International Atomic
Energy Agency, the technical report series TRS-
398, which is currently the only international
guideline for clinical dosimetry of ion beams in
the energy range of 50 to 250 MeV (Makie et al
1997).
3.2. TLD and film dosimetry
A general problem when using any kind of solid
state detectors for ion beam dosimetry, is the
effect of quenching of the signal in regions with
increased LET. For protons this effect is rather
limited and can be corrected for as a function of
depth. This way even absolute dose measurements
in proton fields can be achieved. For heavier ions
the increase in LET is much larger and in addition,
due to nuclear fragmentation, the LET varies
considerably with depth (Dong, 2015). It is thus
not possible to use either films or TLDs for an
absorbed dose determination. Rather they are used
for relative measurements or QA purposes
(Jackson et al 2012).
12
3.3. Dosimetric verification of dose
distributions
In the case of a passive beam delivery technique,
the dosimetric verification of a beam of protons or
ions is practically identical to conventional (non-
IMRT) RT. Here the treatment field can be
measured, e.g. by scanning a single ion chamber
through the treatment field in a water phantom. If
active beam delivery is used, the scanning of ion
chambers is not possible and hence multichannel
dosimetry systems are needed in order to do
efficient dosimetric verification. For this purpose,
dedicated systems have been developed which
allow, for instance, positioning a set of many
individual ion chambers in a water phantom and
measure doses at various points in the field
simultaneously (Sisterson J. 2005). Another
possibility is to use multichannel detectors like for
instance, segmented ion chamber arrays (e.g.
PTW 729). Although a quantitative dose
determination in not possible with film detectors,
they are still important to check geometric
parameters of the treatment fields.
3.4. Beam monitor calibration
Like the dosimetric verification, also the
calibration of beam monitors for passive systems
can be performed in the same way as in
conventional RT. This typically includes an
individual calibration of eachtreatment field in
terms of monitor units at the reference point. If
proper modelling of the beam line is performed,
also an empirical calibration for each combination
of beam shaping elements can be achieved (Kooy
et. al 2003). If a scanning system is used together
with an energy selection system, the monitor
calibration typically has to be done energy
specific, i.e. a calibration of all beam energies has
to be done in order to achieve a proper treatment
field. In this case, the reference point may be
chosen to lie in the entrance region of the
individual Bragg peaks, rather than in the SOBP
as in the case of passive systems (Jackel et. Al
2004).
4. THERAPY PLANNING
For the active beam shaping system, a research
therapy planning system (TPS) was developed
(Kramer et. al 2000, Jackel et al 2001), which
fulfils the needs of the beam scanning system.
While a modulator for passive beam shaping is
designed to achieve a prescribed homogeneous
biologically effective dose for a single field. A 3D
scanning system can produce nearly arbitrary
shapes of the spread-out Bragg peak (SOBP).The
shape of the SOBP therefore has to be optimized
separately for every scan point in the irradiation
field. The introduction of a 3D scanning system,
thus, has some important consequences for the
TPS:
The particle number at every scan point
and the energy has to be optimized
separately.
The capability for intensity modulated RT
with ions should be taken into account.
13
All fields of a treatment plan are applied
on the same day to avoid uncertainties in
the resulting dose due to set-up errors.
The dose per fraction should be variable
for every patient.
The scanner control data (energy, beam
position, particle number at every beam
spot) have to be optimized for each field of
every patient.
An RBE model that allows the calculation
of a local RBE at every point in the patient
has to be implemented.
4.1. Imaging for TP
While it is a common standard to use CT and MR
images to outline the tumor and organs at risk,
CT data is still the only quantitative source of
electron density needed to calculate the range of
the ions in tissue. A calibration of CT numbers to
ion ranges relative to water is needed. These
relations are usually empirical and are only valid
for a certain well defined imaging protocol (Jakel
et al. 2000).
4.2. Dose calculation
The dose calculation for active beam shaping
systems relies on measured data for the depth–
dose curves, instead of the measured depth–dose
data for the SOBP resulting from the modulators,
data for single energies needed. If the applied dose
is variable, it is necessary to base the calculation
of absorbed dose on absolute particle numbers
rather than on relative values. For the calculation
of the absorbed dose, the integral data including
all fragments are sufficient. Before the actual dose
calculation starts, the target volume is divided into
slices of equal radiological depth (Here the same
empirical methods of range calculation as for
passive systems are used). Each slice then
corresponds to the range of ions at certain energy
of the accelerator. The scan positions of the raster
scanner are then defined as a quadratic grid for
each energy. In the last step, the particle number
at each scan point is optimized iteratively until a
predefined dose at each point is reached.
4.3. Dose optimization and intensity
modulation
The most straightforward optimization of
(biological effective) dose is a technique which
may be called single field uniform dose
optimization. In the case of passive systems, this
is achieved by an optimization of the design of the
range modulator. In the case of protons a
homogeneous absorbed dose throughout the depth
modulation is produced. For heavier ions the
increase of RBE with LET and thus depth
necessitates a decrease of the absorbed dose
(Kempe et al 2007).
In the case of scanning systems, much more
flexibility introduced into the possible
optimization of a single field. The additional
degree of freedom of depth–dose modulation
enables several
techniques, like the individual biological modeling
of RBE (see below) and the use of intensity
14
modulated particle therapy (IMPT) (Sarfehnia et
al 2010). IMPT can be achieved by various
approaches as follows: an IMRT-like optimization
of dose in 2D (keeping the depth modulation
fixed), a 2+1 2D optimization (with an additional,
but fixed depth–dose modulation
throughout the field) or a real 3D optimization of
all individual scan spots. The more degrees of
freedom are used, the more it becomes important
to have additional dose constraints in order not to
produce degenerated solutions of the optimization
process (Lomax A. J. 2008).
5. Radiobiology
Relative biologic effectiveness (RBE) of any
radiation is the ratio of the dose of 250-kVp x-rays
to produce a specified biologic effect to the dose
of the given radiation to produce the same effect.
The specified biologic effect may consist of cell
killing, tissue damage, mutations, or any other
biologic endpoint. The reference radiation for
RBE comparison is sometimes chosen to be
cobalt-60 g rays or megavoltage x-rays for which
the RBE has been determined to be about 0.85 ±
0.05 (relative to 250-kVp x-rays) (Khan, 2014).
The RBE value of protons beams can`t be fixed,
but for 70 – 250 MeV protons range typically
from 0.9 to 1.9, with an accepted 'generic' value of
1.1 in clinical proton therapy. Consequently, the
equivalent 60
Co photon dose is the proton dose
multiplied by 1.1. This calculated dose is defined
as the Cobalt Gray Equivalent (CGE) dose and
this is used to calculate and compare doses
between modalities (Weber et al., 2006).
Nuclear interactions are of importance for proton
radiation therapy for three reasons. First, they
contribute to the total absorbed dose. Second, they
may have high-LET values causing an increase of
the beam’s relative biological effectiveness
(RBE). Third, they produce secondary neutrons
leading to dose deposition outside the target
volume (Paganetti, 2002).
The common analytical methods of proton dose
calculation in radiation therapy involve
approximations that may be reflected in
uncertainties in the predicted absorbed dose.
Besides the dose from electromagnetic
interactions (Petti 1992), part of the total dose in
proton therapy is due to secondary protons,
deuterons, tritons, 3 He and α-particles liberated in
nuclear interactions (and due to nuclear recoils). A
dose build-up effect in the entrance region of a
Bragg curve (i.e. the spatial pattern of dose as a
function of depth) interpreted as being due to
secondary particle dose was first confirmed by the
measurements in a 185 MeV proton beam
(Carlsson 1977). In analytical pencil-beam
algorithms, the influence of nuclear interactions is
usually assumed to be small and they are included
only through their (measured) contribution to the
depth–dose distribution (Hong et al 1996, Russell
et al 1995).
Heavy ions exhibit a strong increase of LET in the
Bragg peak region when compared with the
entrance region (Sandison et al 1997). This
increase is due to the track structure as explained
15
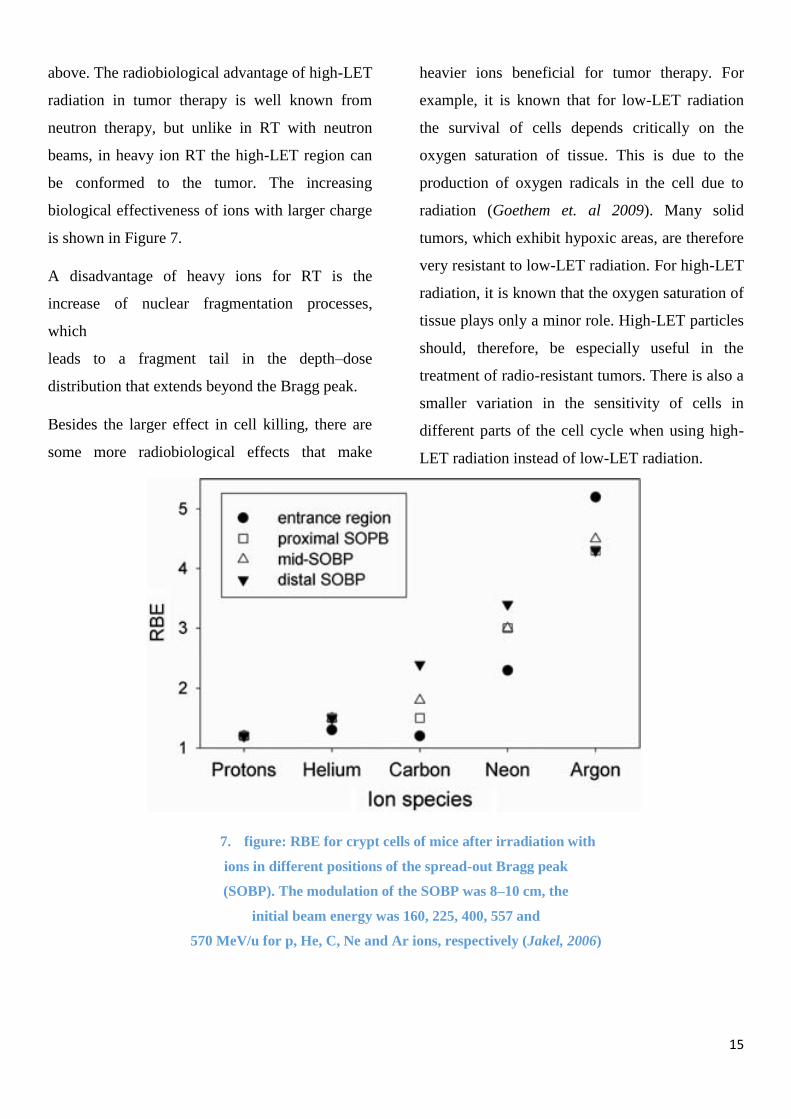
above. The radiobiological advantage of high-LET
radiation in tumor therapy is well known from
neutron therapy, but unlike in RT with neutron
beams, in heavy ion RT the high-LET region can
be conformed to the tumor. The increasing
biological effectiveness of ions with larger charge
is shown in Figure 7.
A disadvantage of heavy ions for RT is the
increase of nuclear fragmentation processes,
which
leads to a fragment tail in the depth–dose
distribution that extends beyond the Bragg peak.
Besides the larger effect in cell killing, there are
some more radiobiological effects that make
heavier ions beneficial for tumor therapy. For
example, it is known that for low-LET radiation
the survival of cells depends critically on the
oxygen saturation of tissue. This is due to the
production of oxygen radicals in the cell due to
radiation (Goethem et. al 2009). Many solid
tumors, which exhibit hypoxic areas, are therefore
very resistant to low-LET radiation. For high-LET
radiation, it is known that the oxygen saturation of
tissue plays only a minor role. High-LET particles
should, therefore, be especially useful in the
treatment of radio-resistant tumors. There is also a
smaller variation in the sensitivity of cells in
different parts of the cell cycle when using high-
LET radiation instead of low-LET radiation.
7. figure: RBE for crypt cells of mice after irradiation with
ions in different positions of the spread-out Bragg peak
(SOBP). The modulation of the SOBP was 8–10 cm, the
initial beam energy was 160, 225, 400, 557 and
570 MeV/u for p, He, C, Ne and Ar ions, respectively (Jakel, 2006)

16
6. Clinical application of proton therapy
Clinical use of proton beam therapy (PBT) has
become a major focus of health policy debate in
the (Mark V. Mishra et.al 2016). The rationale for
the use of proton beams in radiotherapy is the
increased tumor control probability (TCP) by
delivering higher doses to the tumor. Like other
highly conformal therapy techniques, proton
therapy is of particular interest for tumors located
close to serial organs. Data are grouped according
to anatomic region.
6.1. Central Nervous System and Base of
Skull (Adults)
In the beginning of 90’s, proton therapy was used
to treat brain metastases and AVM’s at Loma
Linda University, United States (Slater, 2006). At
Harvard Cyclotron Laboratory the investigations
reported long-term success with stereotactic
proton radiosurgery for pituitary adenomas
(Ronson et al 2005), Reporting on patients treated
during the period from 1963 to 1990, they
observed that 98% of 581 patients with
acromegaly had hormone normalization at 20
years post treatment. In a group of 36 patients
with Nelson’s syndrome and 180 patients with
Cushing’s disease, 85% achieved hormone
normalization at 20 years (Kjellberg et al 1990). A
radio-surgical application of protons has been
implemented in the treatment of AVMs (Kjellberg
et al. 1983).
6.2. Paediatric intracranial tumors
The use of proton therapy for paediatric
intracranial tumors has not been widely studied,
there are some publications and ongoing studies,
Most studies are case series with a limited number
of patients included (<30). Benk et al. studied
Base of skull and cervical spine chordomas in
children treated by high-dose irradiation (Benk, V.
et al 1995), another study done by (Habrand, J.L.
1999) was Proton beam therapy (PT) in the
management of CNS tumors in childhood. , Hug
et al studied the Conformal proton radiation
therapy for pediatric low-grade astrocytoma’s
(Hug et al 2002). These studies were
heterogeneous with respect to diagnosis, stage and
treatment. Proton therapy was given as part of a
primary treatment, or as treatment for recurrence.
In most studies an aggressive treatment had been
administered, and local control rates were high.
6.3. Ocular tumors
Proton therapy has emerged as an alternative to
enucleation or ocular brachytherapy in the
treatment of ocular tumors, Seddon et al compared
cancer control rates for patients with uveal
melanomas following proton therapy versus
enucleation (Seddon, 1985). Patients treated with
proton therapy were younger, had smaller tumors
and different locations compared patients on the
control arm treated with surgery. Five year overall
survival was 81% in the proton therapy group and
17
68% in the enucleation group. Cox regression
analysis adjusted for prognostic variables found
no difference in overall survival, RR 1.2 (95% CI
0.9–1.2), or disease free survival, RR 1.0 (95% CI
0.7–1.4) (Olsen et al 2007).
A study analyzed medical records for patients
with choroidal melanoma treated with proton
therapy or brachytherapy. Local recurrence,
mortality and visual acuity were analyzed, but the
model was not appropriately adjusted for possible
confounders (only basal tumor diameter). Patients
treated with proton therapy had a higher mortality
rate (9.4%) compared to patients given
brachytherapy (3.7% and 5.0% for 125
I or 106
Ru,
respectively), but a lower rate of local recurrence
(5.2%), compared with 4.2% and 10.7% for 125
I
or 106
Ru, respectively (Wilson, M.W. and
Hungerford, J.L. 1999) and (Olsen et al 2007).
6.4. Chordomas and chondrosarcomas
Chordomas and chondrosarcomas in the head and
neck region are usually treated with surgery
and/or radiotherapy. Conventional radiotherapy
with doses of 50–55 Gy do not provide sufficient
cancer control, but higher doses may be offset by
toxic effects on surrounding neurological tissues.
A study randomized 96 patients with chordomas
and chondrosarcomas of the skull base to receive
66.6 or 72 CGE with a combination of proton and
photons by (Santoni,et al 1998) The only
publication identified from this study reported
temporal lobe damage without analyzing patents
by initial allocation group, and was not able to
relate temporal lobe damage to treatment strategy.
Overall temporal lobe damage was 7.6% at 2
years and 13.2% after 5 years.
Nine case-series reported results for around 500
patients treated with proton therapy alone or as a
supplement to conventional radiotherapy, Proton
therapy was given as part of primary treatment or
for recurrence. Five and 10 year survival was 94%
and 86%, respectively, for the whole population
(Debus et al. 1997). Two studies reported lower
overall survival for chordomas compared with
chondrosarcomas, at 3 year follow up 87–88% and
94–100%, respectively (Hug et al. 1999 and Noel
et al. 2002).
6.5. Prostate cancer
Men with prostate cancer comprise approximately
65% of all patients treated with protons at Loma
Linda University Medical Center; this population
represents the largest series of patients treated
with protons for prostate cancer anywhere in the
world. A series of reports from LLURM
investigators, and a multi-institutional randomized
controlled study, have demonstrated that proton
radiation enables delivery of effective doses of
ionizing energy to the desired prostatic CTV while
limiting radiation exposure of nearby tissues, thus
yielding few or no side effects in most patients
treated. Initial studies used total doses that were
10% greater than was typical at the time, and
18
preliminary results were encouraging (Slater,
Rossi, et al 1999).
6.6. Lung cancer
Based on the American society of oncology, there are
170,000 new lung cancer cases every year in United
States, previous researchers at Loma Linda
University Hospital encouraging the use of proton
therapy for stage one lung cancer (Bush et al
1999), and a later report indicated that excess
pulmonary toxicity did not occur when higher-
than-conventional doses of radiation at a higher-
than- conventional dose per fraction were
delivered via conformal radiation techniques with
protons (Bonnet et al 2001).
A study, investigating the role of PT in NSCLC
therapy, conducted for 68 patients, all of them
with stage one non-small-lung cancer were treated
with multi-beam proton radiation therapy. The
delivered treatment was 51 GyE in 10 fractions
over two weeks to the first 22 patients; the
subsequent 46 patients received 60 GyE in 10
fractions over two weeks., all 68 patients data
were analyzed and reported No symptomatic
radiation pneumonitis or late esophageal or
cardiac toxicity were seen; the 3-year local control
and disease-specific survival rates were 74% and
72%, respectively. There was significant
improvement in local tumor control in T1 vs. T2
tumors (87% vs. 49%), with a trend toward
improved survival (Bush et al 2004). In addition
to proton therapy treatment of lung tumours,
controlling tumour displacements remains one of
the biggest challenges (Kovács, et al 2007, 2007,
2009)
6.7. Hepatocellular carcinoma
A study conducted to determine the role of proton
therapy for treating Hepatocellular carcinoma with
34 patients had completed treatment and had been
followed for at least six months (median follow-
up, 20 months). The average tumor size was 5.7
cm. Two-year actuarial data showed a 75% local
tumor control rate and an overall survival rate of
55%. Of patients with an elevated pretreatment
alpha-fetoprotein (AFP), 85% were found to have
declining AFP levels, from a pretreatment mean of
1,405 to 35 at six months after treatment. Six
patients underwent liver transplantation several
months after radiotherapy was completed; two of
these individuals demonstrated no evidence of
residual carcinoma within the explanted liver.
Post-treatment toxicity was minimal and included
a small but significant decline in albumin levels
and increased total bilirubin; three patients
experienced duodenal or colonic bleeding when
bowel was immediately adjacent to the treated
tumor (Bush et al 2004).
6.8. Breast cancer
At present, the role of radiotherapy in the
multidisciplinary management of breast cancer is
well established (Coates et al 2015), Postoperative
irradiation reduces breast and lymph node
recurrences, and improves survival, mainly in

19
high-risk population. Treatment of local or loco-
regional breast areas with conventional radiation
techniques can include a significant amount of
normal tissue and organs at risk in the irradiated
volume, with the risk of treatment-related normal
tissue injury and worsening quality of life (Brown
et al 2015).
Recently, proton therapy has been also explored in
breast cancer treatment. This indication is not
recommended for routine referral because of
insufficient evidence, but inclusion in clinical
studies or treatment of individual cases should be
considered in a multidisciplinary setting (Patel et
al 2014). The potential of protons for coverage of
target tissues and sparing of normal structures has
been evaluated in several dosimetric studies, in
silico planning studies (Orecchiaa et al 2015),
several studies investigated the dose distribution
of protons in left-sided breast cancer, evaluating
the dose reduction to the heart. A comparative
treatment planning on 20 left-sided breast cancer
patients, with increasingly complex loco-regional
volumes including the internal mammary chain,
showed that IMPT allowed the best target
coverage and lowest dose to neighboring organs.
Cardiac dose lowered by a factor of above 20
when compared to IMRT, potentially reducing the
risk of cardiovascular toxicity (Ares et al 2010),
another study on five patients after mastectomy
and bilateral breast implants compared IMPT
versus three-dimensional (3D) conformal photons
(Jimenez et al 2013).
7. Challenges
7.1. Technical challenges
Proton beams for radiation therapy are generated
by using a particle accelerator, either a cyclotron
or a synchrotron. Both have their pros and cons.
Cyclotrons are smaller in size, but generally allow
the extraction of only one fixed beam energy. This
means that energy changes have to be achieved by
placing absorber material in the beamline,
typically right at the exit of the beam from the
cyclotron. A synchrotron produces a significantly
smaller beam (in cross-section) and can switch
energy on sub-second timescales. On the other
hand, its pulsed beam delivery makes it less
flexible for some modulation techniques.
Currently most proton therapy accelerators are
large, such that they are sited outside of the
treatment room. In fact, a proton accelerator will
typically feed several treatment rooms, with a
significant amount of space needed to transport
the beam from the accelerator using magnets for
bending, steering and focusing. In contrast, photon
LINACS, including all beam shaping and
monitoring devices, easily fit into a single room.
Proton facilities are therefore typically larger than
photon treatment facilities, not least because a
complete radiation delivery system also contains a
gantry to rotate the entire treatment head around
the patient. Most proton gantries have diameters
of several meters, owing to the magnetic field

20
strength required to bend the beam path of protons
with energies of up to 250 MeV. The cost of a
proton delivery system is also higher than that of a
photon machine, in part because of room
requirements when using a 360° gantry. A number
of studies have assessed the need for a full
rotational gantry and whether specific beam
angles might be sufficient. A full 360° gantry
might not be required for most treatments, for
example, with the use of a robotic couch with six
degrees of freedom and with patients being treated
in a lying or seated position.
7.2. Physics challenges
Dose uncertainties: When prescribing and
delivering dose we rely on the dose distributions
shown by the treatment planning program after
optimization. However, there is always
uncertainty when predicting the dose and the dose
distribution may not be delivered precisely as
planned. In radiation therapy, the aim is to deliver
the dose to within 2.5% of the prescribed dose.
This value was suggested by international
regulatory bodies.
Dose calculations are routinely performed using
analytical algorithms that are fast enough to allow
treatment optimization in minutes. While these
techniques are typically sufficiently accurate in
the photon world, they have significant
shortcomings in proton therapy. The steeper dose
gradients present in particle fields expose the
approximations in analytical algorithms, in
particular with respect to scattering of protons at
interfaces such as bone and soft tissue. While too
slow to be used in the clinic in the past, dose
calculations based on particle-track simulations
(‘Monte Carlo’) have recently achieved
efficiencies that make them suitable for use in
treatment planning. Monte Carlo codes offer
superior dose calculations to analytical algorithms
and are considered the gold standard.
Uncertainties can have more severe consequences
in proton therapy versus photon therapy because
of the finite range and the impact of proton
scattering in an inhomogeneous patient geometry.
Understanding uncertainties in proton therapy is
therefore vital when making treatment planning
decisions.
21
8. Bibliography
1. Wilson, R. R. Radiological use of Fast
Protons. Radiology 47, 487-491 (1946).
2. Lawrence, J. H., Tobias, C. A., Born, J. L.
Hypophysectomy for Advanced Breast
Cancer Using High Energy Particle Beams
3. Kjellberg, R. N., Sweet, W. H., Preston,
W. M., Koehler, A. M. The Bragg Peak of
a Proton Beam in Intracranial Therapy of
Tumors. Trans. Am. Neurol. Assoc. 87,
216-218 (1962).
4. Newhauser W.D. and Zhang R. 2015 Phys.
Med. Biol. 60 R155)
5. Shipley WU, Prout GR, Jr, Coachman
NM, McManus PL, Healey EA, Althausen
AF, Heney NM, Parkhurst EC, Young HH,
2nd, Shipley JW, et al. Radiation therapy
for localized prostate carcinoma:
experience at the Massachusetts General
Hospital (1973-1981). NCI
Monogr. 1988;(7):67–73.[PubMed]
6. Jardins M, Houde M, Gagnon E
(2005) Phagocytosis: the convoluted way
from nutrition to adaptive
immunity. Immunol Rev 207: 158–
165 [PubMed]
7. Zietman, A. L., Bae, K., Slater, J. D.,
Shipley, W. U., Efstathiou, J. A., Coen, J.
J., . . . Rossi, C. J. (2010). Randomized
trial comparing conventional-dose with
high-dose conformal radiation therapy in
early-stage adenocarcinoma of the
prostate: Long-term results from proton
radiation oncology group/American
college of radiology 95-09. Journal of
Clinical Oncology, 28, 1106-1111.
8. Oliver Jäkel; Medical physics aspects of
particle therapy, Radiation Protection
Dosimetry, Volume 137, Issue 1-2, 1
November 2009, Pages 156–
166, https://doi.org/10.1093/rpd/ncp192
9. Weber D C et al 2009 RapidArc, intensity
modulated photon and proton techniques
for recurrent prostate cancer in previously
irradiated patients: a treatment planning
comparison study Radiat. Oncol. 4 34
10. Valdivieso M, Kujawa A M, Jones T and
Baker L H 2012 Cancer survivors in the
United States:a review of the literature and
a call to action Int. J. Med. Sci. 9 163–73
11. Faiz M. Khan , The physics of proton
therapy, 2014
12. Hug, E. B., Nevinny-Stickel, M., Fuss, M.,
Miller, D. W., Schaefer, R. A., Slater, J. D.
Conformal Proton Radiation Treatment for
Retroperitoneal Neuroblastoma:
Introduction of a Novel Technique. Med.
Pediatr. Oncol. 37, 36-41 (2001)
13. Verhey, L. J., Smith, V., Serago, C. S.
Comparison of Radiosurgery Treatment
Modalities Based on Physical Dose
Distributions. Int. J. Radiat. Oncol. Biol.
Phys. 40, 497-505 (1998).
22
14. Mackie TR, Scrimger JW, Battista JJ. A
convolution method of calculating dose for
15 MV x-rays. Med Phys. 1985;12:188-
196.
15. Dong L. Clinical commissioning of proton
beam Principles and Practice of Proton
Beam Therapy (Medical Physics
Monograph No. 37, 2015)
16. Boyer AL, Mok EC. A photon dose
distribution model employing convolution
calculations. Med Phys. 1985;12:169-177.
17. FM, Gerbi BJ, eds. Treatment Planning in
Radiation Oncology. Philadelphia, PA:
Lippincott Williams & Wilkins; 2012.
18. Kooy, H. M., Schaefer, M., Rosenthal, S.
and Bortfeld, T. Monitor unit calculations
for range-modulated spread-out Bragg
peak fields. Phys. Med. Biol. 48, 2797–
2808 (2003).
19. Jäkel, O., Hartmann, G. H., Karger, C. P.,
Heeg, P. and Vatnitsky, S. A calibration
procedure for beam monitors in a scanned
beam of heavy charged particles. Med
Phys. 2004 May;31(5):1009-13.
20. Jäkel, O., Kramer, M., Karger, C. P. and
Debus, J. Treatment planning for heavy
ion radio-therapy: clinical implementation
and application. Phys. Med. Biol. 46,
1101–1116 (2001).
21. Jäkel, O., Hartmann, G. H., Karger, C. P.
and Heeg, P. Quality assurance for a
treatment planning system in scanned ion
beam therapy. Med. Phys. 27, 1588–1600
(2000).
22. Jäkel, O., Jacob, C., Schardt, D., Karger,
C. P. and Hartmann, G. H. Relation
between carbon ions ranges and X-ray CT
numbers. Med. Phys. 28(4), 701–703
(2001).
23. van Goethem M J, van der Meer R, Reist
H W and Schippers J M 2009 Geant4
simulations of proton beam transport
through a carbon or beryllium degrader
and following a beam line. Phys Med Biol.
2009 Oct 7;54(19):5831-46.
24. Paganetti, H. et al. Relative biological
effectiveness (RBE) values for proton
beam therapy. Int. J. Radiat. Oncol. Biol.
Phys. 53, 407–421 (2002).
25. Carlsson C A and Carlsson G A 1977
Proton dosimetry with 185 MeV protons.
Dose buildup from secondary protons and
recoil electrons Health Phys. 33 481–4
26. Hong L, Goitein M, Bucciolini M,
Comiskey R, Gottschalk B, Rosenthal S,
Serago C and Urie M 1996 A pencil beam
algorithm for proton dose calculations
Phys. Med. Biol. 41 1305–30
27. Russell K R, Grusell E and Montelius A
1995 Dose calculations in proton beams:
range straggling corrections and energy
scaling Phys. Med. Biol. 40 1031–43
28. Sandison G A, Lee C-C, Lu X and Papiez
S 1997 Extension of a numerical algorithm
to proton dose calculations: I.
Comparisons with Monte Carlo
simulations Med. Phys. 24 841–9
29. Kjellberg R N, Hanamura T, Davis K R,
Lyons S L and Adams R D 1983 Bragg-
23
peak proton-beam therapy for
arteriovenous malformations of the brain
N. Engl. J. Med. 309 269–74
30. Kempe J, Gudowska I and Brahme A 2007
Depth absorbed dose and LET
distributions of therapeutic 1H, 4He, 7Li,
and 12C beams Med. Phys. 34 183–92
31. Sarfehnia A, Clasie B, Chung E, Lu H M,
Flanz J, Cascio E, Engelsman M, Paganetti
H and Seuntjens J 2010 Direct absorbed
dose to water determination based on
water calorimetry in scanning proton beam
delivery Med. Phys. 37 3541–50
32. Lomax, A. J. Intensity modulated proton
therapy and its sensitivity to treatment
uncertainties 1: the potential effects of
calculational uncertainties. Phys. Med.
Biol. 53, 1027–1042 (2008)
33. Lippitz B, Lindquist C, Paddick I,
Peterson D, O’Neill K, Beaney R (2014)
Stereotactic radiosurgery in the treatment
of brain metastases: the current evidence.
Cancer Treat Rev 40:48–59
34. Lindquist, C., Paddick, I. The Leksell
Gamma Knife Perfexion and comparisons
with its
predecessors. Neurosurgery. 2007;61:130–
140 ([discussion 40–1]).
35. Steven D. Chang, William Main, David P.
Martin, Iris C. Gibbs, M. Peter Heilbrun;
An Analysis of the Accuracy of the
CyberKnife: A Robotic Frameless
Stereotactic Radiosurgical
System, Neurosurgery, Volume 52, Issue
1, 1 January 2003, Pages 140–147,
36. Murphy, M. J. and Cox, R. S. (1996), The
accuracy of dose localization for an image‐
guided frameless radiosurgery system.
Med. Phys., 23: 2043-2049.
37. Verellen, D., Linthout, N., Bel, A., Soete,
G., Van Den Berge, D., D' Haens, J.,
Storme, G. Assessment of the uncertainties
in dose delivery of a commercial system
for linac-based stereotactic radiosurgery
(1999) International Journal of Radiation
Oncology Biology Physics, 44 (2), pp.
421-433.
38. Lippitz B, Lindquist C, Paddick I,
Peterson D, O’Neill K, Beaney R (2014)
Stereotactic radiosurgery in the treatment
of brain metastases: the current evidence.
Cancer Treat Rev 40:48–59
39. Lucien A. Nedzi, Hanne M. Kooy, Eben
Alexander, Gösran K. Svensson, Jay S.
Loeffler, Dynamic field shaping for
stereotactic radiosurgery: A modeling
study, International Journal of Radiation
Oncology*Biology*Physics, Volume 25,
Issue 5, 1993, Pages 859-869, ISSN 0360-
3016,
40. Kubo, H.D., Wilder, R.B., Pappas, C.T.E.
Impact of collimator leaf width on
stereotactic radiosurgery and 3D
conformal radiotherapy treatment plans
(1999) International Journal of Radiation
Oncology Biology Physics, 44 (4), pp.
937-945.
41. Simonová G.,Roman L. Radiosurgery in
the treatment of malignant brain tumors,
24
Expert Review of Anticancer
Therapy, 2014, 3:6, 879-890,
42. Nataf, F., Schlienger, M., Liu, Z.,
Foulquier, J.N., Grès, B., Orthuon, A.,
Vannetzel, J.M., (...), Touboul, E.
Radiosurgery With or Without A 2-mm
Margin for 93 Single Brain Metastases
(2008) International Journal of Radiation
Oncology Biology Physics, 70 (3), pp.
766-772.
43. Benk, Veronique, et al. "Base of skull and
cervical spine chordomas in children
treated by high-dose
irradiation." International Journal of
Radiation Oncology• Biology• Physics31.3
(1995): 577-581.
44. Habrand, Jean-Louis, et al. "The role of
radiation therapy in the management of
craniopharyngioma: a 25-year experience
and review of the literature." International
Journal of Radiation Oncology• Biology•
Physics 44.2 (1999): 255-263.
45. Hug, E. B., Muenter, M. W., Archambeau,
J. O., DeVries, A., Liwnicz, B., Loredo, L.
N., ... & Slater, J. D. (2002). Conformal
proton radiation therapy for pediatric low-
grade astrocytomas. Strahlentherapie und
Onkologie, 178(1), 10-17
46. Seddon JM,et al. Comparison of survival
rates for patients with uveal melanoma
after treatment with proton beam
irradiation or enucleation. American
journal of ophthalmology 99.3 (1985):
282-290.
47. Wilson, Matthew W., and John L.
Hungerford. "Comparison of episcleral
plaque and proton beam radiation therapy
for the treatment of choroidal
melanoma." Ophthalmology 106.8 (1999):
1579-1587.
48. Dag Rune O. et al. "Proton therapy–a
systematic review of clinical
effectiveness." Radiotherapy and
oncology 83.2 (2007): 123-132.
49. Santoni R. et al. "Temporal lobe (TL)
damage following surgery and high-dose
photon and proton irradiation in 96
patients affected by chordomas and
chondrosarcomas of the base of the
skull." International Journal of Radiation
Oncology• Biology• Physics 41.1 (1998):
59-68.
50. Hug, EB., et al. "Proton radiation therapy
for chordomas and chondrosarcomas of the
skull base." Journal of neurosurgery 91.3
(1999): 432-439.
51. Slater, JD. et al. "Conformal proton
therapy for early-stage prostate
cancer." Urology 53.5 (1999): 978-983.
52. Bush, D. A., Dunbar, R. D., Bonnet, R.,
Slater, J. D., Cheek, G. A., Slater, J. M.
Pulmonary Injury From Proton and
Conventional Radiotherapy as Revealed by
CT. Am. J. Roentgenol. 172, 735-739
(1999).
53. Bonnet, R. B., Bush, D., Cheek, G. A.,
Slater, J. D., Panossian, D., Franke, C.,
Slater, J. M. Effects of Proton and
Combined Proton/Photon Beam Radiation
25
on Pulmonary Function in Patients with
Resectable but Medically Inoperable Non-
small Cell Lung Cancer. Chest 120, 1803-
1810 (2001).
54. Bush, D. A., Slater, J. D., Shin, B. B.,
Cheek, G., Miller, D. W., Slater, J. M.
Hypofractionated Proton Beam
Radiotherapy for Stage I Lung Cancer.
Chest 126, 1198-1203 (2004).
55. Bush, D. A., Hillebrand, D. J., Slater, J.
M., Slater, J. D. High-dose Proton Beam
Radiotherapy of Hepatocellular
Carcinoma: Preliminary Results of a Phase
II Trial. Gastroenterology. 127, S189-s193
(2004).
56. Kovács A, Hadjiev J, Lakosi F et al. A
tumormozgások jelentőségének
sokszeletes-CT-alapú képfúziós vizsgálata
tüdődaganatos betegek sugárkezelésénél
[Tumor movements detected by multi-slice
CT-based image fusion in the radiotherapy
of lung cancer patients]
MAGYAR ONKOLÓGIA 51 : 3 pp. 219-
223. , 5 p. (2007)
57. Kovács A, Hadjiev J, Lakosi F et al.
Thermoplastic patient fixation: influence
on chest wall and target motion during
radiotherapy of lung cancer
STRAHLENTHERAPIE UND
ONKOLOGIE (0179-7158 1439-099X):
183 5 pp 271-278 (2007)
58. Kovács A, Hadjiev J, Lakosi F et al.
Dynamic MR based analysis of tumor
movement in upper and mid lobe localized
lung cancer
PATHOLOGY AND ONCOLOGY
RESEARCH (1219-4956 1532-2807): 15
2 pp 269-277 (2009)
59. Coates AS, Winer EP, Goldhirsh A, et al.
Tailoring therapies: improving the
management of early breast cancer: St
Gallen International Expert Consensus on
the primary therapy of early breast cancer
2015. Ann Oncol 2015; 26:1533–1546.
60. Brown LC, Muteer RW, Halyard MY.
Benefits, risk, and safety of external beam
radiation therapy for breast cancer. Int J
Womens Health 2015; 24:449–458.
61. Patel S, Kostaras X, Parliament M, et al.
Recommendations for the referral of
patients for proton-beam therapy, an
Alberta Health Services report: a model for
Canada? Curr Oncol 2014; 21:251–262
62. Roberto Orecchiaa,b,c, Piero Fossatia,b,c,
Stefano Zurridaa , and Marco Krenglib,d,
New frontiers in proton therapy:
applications in breast cancer, 2015
Nov;27(6):427-32.
63. Ares C, Khan S, Macartain AM, et al.
Postoperative proton radiotherapy for
localized and locoregional breast cancer:
potential for clinically relevant
improvements? Int J Radiat Oncol Biol
Phys 2010; 76:685–697.
64. Jimenez RB, Goma C, Nyamwanda J, et
al. Intensity modulated proton therapy for
postmastectomy radiation of bilateral
implant reconstructed breasts: a treatment
26
planning study. Radiother Oncol 2013;
107:213–217
65. Weber DC, Ares, C, Lomax AJ, Kurtz JM
Radiation therapy planning with photons
and protons for early and advanced breast
cancer: an overview, Radiation Oncology
2006 1:22




























![On the scattering power of radiotherapy protons - arXiv · arXiv:0908.1413v1 [physics.med-ph] 10 Aug 2009 On the scattering power of radiotherapy protons Bernard Gottschalk ∗ August](https://img.pdfslide.tips/doc/110x75/5ae048917f8b9af05b8d7250/on-the-scattering-power-of-radiotherapy-protons-arxiv-09081413v1-10-aug-2009.jpg)