Embed Size (px)
Citation preview

¿Recomendado?
EAU BPH guidelines. Madersbacher S y cols. Eur Urol 2012
Tratamiento expectante
Alfa-bloqueantes
Inhibidores de la 5-alfa-reductasa (5ARI’s)
Tratamiento de combinación
Fitoterapia
Técnicas mínimamente invasivas
Cirugía
Tratamientos actuales HBP:
No?

Guías Europeas de Urología: Management of Male LUTS 2012
1º Fitoterapia:
• Cucurbita pepo (pumpkin seeds)• Hypoxis rooperi (South African star grass)• Pygeum africanum (bark of the African plum tree)• Secale cereale (rye pollen)• Serenoa repens (syn. Sabal serrulata; berries of the American dwarf palm, saw palmetto)• Urtica dioica (roots of the stinging nettle).
No reconocen afección de la esfera sexual por este tipo de terapias.
Sevilla 15 - 16 Nov. 2012

Guías Europeas de Urología: Management of Male LUTS 2012
2ºAntimuscarínicos:
• darifencacin hydrobromide (darifenacin);• fesoterodine fumarate (fesoterodine);• oxybutynin HCL (oxybutynin);• propiverine HCL (propiverine);• solifenacin succinate (solifenacin);• tolterodine tartrate (tolterodine);• trospium
No reconocen afección de la esfera sexual por este tipo de terapias.
Sevilla 15 - 16 Nov. 2012

Guías Europeas de Urología: Management of Male LUTS 2012
3º Alfabloqueantes:
• Alfuzosina•Terazosina
• Doxazosina•Tamsulosina•Silodoxina
Sevilla 15 - 16 Nov. 2012
Alfa bloqueantes y HBP:

Sevilla 15 - 16 Noviembre 2012
-Existen tres tipos de receptores α en el pene: 1A, 1B y 1D
-Teóricamente los receptores α= contracción muscular= detumescencia peneana
Fenilefrina: priapismo, PGE1
-Un αbloqueante debería favorecer la erección:
-Fentolamina oral vs placebo= mejoría de la erección.
Becker AJ, Stief CG, Machtens S, et al. Oral phentolamine as treatment for erectile dysfunction. J Urol 1998; 159: 1214-6
-La doxazosina mejora la respuesta del alprostadil Kaplan SA, Reis RB, Kohn IJ, et al. Combination therapy using oral alpha-blockers and intracavernosal injection in men with erectile dysfunction. Urology 1998; 52: 739-43
-Doxazosina mejora la respuesta en no respondedores Sildenafilo: De Rose AF, Giglio M, Traverso P, et al. Combined oral therapy with sildenafil and doxazosin for the treatment of
non-organic erectile dysfunction refractory to sildenafil monotherapy. Int J Impot Res 2002; 14: 50-3
-Estudios en animales sugieren que pueden tener un efecto pro-eréctil por acción nerviosa central
Chang AY, Huang CM, Chan JY, et al. Involvement of noradrenergic innervation from locus coeruleus to hippocampal formation in negative feedback regulation of penile erecetion in the rat. Hippocampus 2001; 11: 783-92

Sevilla 15 - 16 Noviembre 2012
-Pero en el ámbito de la clínica no se traduce:Implicación de bajada de TA?, involucras otras áreas cerebrales?
-Globalmente se acepta una DE alrededor del 3%
-Pacientes que abandonan el ttº por DE con Tamsulosina 0,2% y Terazosina 0,3% Narayan P, O’Leary MP, Davidai G. Early efficacy of tamsulosin versus Terazosin in the treatment of men with
benign prostatic hyperplasia: a randomized open-label trial. Urology 2001; 58: 953-9 Res 2005; 5: 237-45

Sevilla 15 - 16 Noviembre 2012
Comparación αbloqueantes vs placebo:
Alfuzosina vs placebo: 3RCT empeora FE y 4RCT no varía
Doxazosina vs placebo: 1RCT empeora FE y 2RCT no varía
Tamsulosina vs placebo: 1RCT empeora FE y 3RCT no varía
Terazosina vs placebo: 6RCT lo empeora y 2RCT no varía
Effects of α1-Adrenoceptor Antagonists on Male Sexual FunctionDrugs 2009; 66 (3): 287-301Marleen M. van Dijk,1 Jean J.M.C.H. de la Rosette1 and Martin C. Michel

Sevilla 15 - 16 Noviembre 2012
Comparación αbloqueantes entre ellos:
Alfuzosina 2.5 mgr/8h vs tamsulosina 0,4: no diferencias
Alfuzosina 10mgr/24h vs tamsulosina 0,4: no diferencias
Alfuzosina 10mgr/24h vs doxazosina 8mgr: peor no significativo alfuzosina
Effects of α1-Adrenoceptor Antagonists on Male Sexual FunctionDrugs 2009; 66 (3): 287-301Marleen M. van Dijk,1 Jean J.M.C.H. de la Rosette1 and Martin C. Michel

Sevilla 15 - 16 Noviembre 2012
Conclusiones Alfa bloqueantes y HBP:
-En el ttº de HBP la DE secundaria a αbloq es un evento poco frecuente
-El porcentaje de pacientes que abandonan el ttº por DE es insignificante
-Ningún αbloq parece ser superior al resto en términos de DE
-No está claro el mecanismo por el cual producen DE

4.2.4 Tolerability and safety
The most relevant adverse effects of 5a-reductase inhibitors are related to sexual function and include reduced libido, erectile dysfunction and, less frequently, ejaculation disorders, such as retrograde ejaculation, ejaculation failure, or decreased semen volume (3,10,13). The incidence of sexual dysfunction and other adverse events is low and even decreased with trial duration. Gynaecomastia (breast enlargement with breast or nipple tenderness) develops in approximately 1-2% of patients.
Sevilla 15 - 16 Noviembre 2012
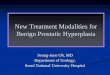
5ARIS y HBP:
Guías Europeas de Urología: Management of Male LUTS 2012:

Roehrborn CG y cols. Urology 2002; 60: 434–441
Efectos adversos relacionados con el fármaco*
412 (19)158 (7) 91 (4) 48 (2) 50 (2)
13 (<1)
303 (14)86 (4)46 (2)
17 (<1) 16 (<1)
33 (2)
Todos los EA relacionados con el fármacoDisfunción eréctilAlteración (disminución) de la libidoTrastornos de la eyaculaciónGinecomastiaMalestar y astenia
Dutasterida
(n=2167)
n (%)
Placebo
(n=2158)
n (%)
Efecto adverso
*>1% de los pacientes
5ARIS y HBP:

3
6
1,21,7
2,8
1,4
0,4 0,4
0
1
2
3
4
5
6
7
8
9
10%
de p
aci
ente
s
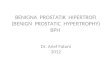
Año 1 Año 2 Año 3 Año 4
Placebo/Dutasterida n = 2158 1736 1152 968
Dutasterida/Dutasterida n = 2167 1744 1188 1041
Debruyne F y cols. Eur Urol 2004; 46: 488−495
Inicio de los AA relacionados con el fármaco: Disfunción Erectil
Años de tratamiento
Doble ciego Fase abierta
Placebo 2 años
Dutasterida 4 años
Dutasterida en fase abierta después de placebo

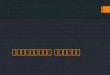
Debruyne F y cols. Eur Urol 2004; 46: 488−495
Doble ciego Fase abierta
1,9
3,7
0,3 0,6
2,4
0,4 0,2 0,1
0
1
2
3
4
5
6
7
8
9
10
% d
e p
aci
ente
s
Año 1 Año 2 Año 3 Año 4
Años de tratamiento
Placebo 2 años
Dutasterida 4 años
Dutasterida en fase abierta después de placebo
Placebo/Dutasterida n = 2158 1736 1152 968
Dutasterida/Dutasterida n = 2167 1744 1188 1041
Inicio de los AA relacionados con el fármaco: Disminución de la líbido

Primeros estudios de tratamiento combinado a corto plazo
Estudio n Duración Fármacos
Veterans Affairs Cooperative Study (VA Coop)Lepor (1996) 1229 1 año Fin, Ter, Fin + Ter, PlaLepor (1998)
PREDICTKirby (1999) a, b 1089 1 año Fin, Dox, Fin + Dox, PlaRoehrborn (2000) a, bKirby (2003)
ALFINDebruyne (1998) 1051 6 meses Fin, Alf, Fin +Alf

Estudios a Largo PlazoMTOPS


Comparación de los estudios CombAT y MTOPs
CombAT1 MTOPs2
Grupos de tratamiento
Monoterapia con dutasterida
Monoterapia con tamsulosina
Tratamiento combinado con dutasterida y tamsulosina
Monoterapia con finasterida
Monoterapia con doxazosina
Tratamiento combinado con finasterida y doxazosina
Placebo
n 4844 3047
Localización Internacional Sólo EEUU
Criterios inclusiónEdadVP (cc)PSA (ng/ml)IPSS
≥50≥30 ≥1,5 y ≤10≥12
≥50Ninguno≤108–30
Crit. de val. princ.2 años4 años
Mejoría puntuación IPSSReducción del riesgo de RAO / cirugía
NingunoCrit. de val. de progresión clínica de la HBP
1Siami et al. Contemp Clin Trials, 2007;28:770–92McConnell et al. NEJM 2003; 349: 2387–98

Tamsulosina 0.4mgTamsulosina 0.4mg
Dutasterida 0.5 mgDutasterida 0.5 mg
Combinacion
PlaceboRun in
4 semanas
SeguimientoSeguridad
Scre
enin
g
Pre-screen
Cribado Inicio M48 Seguimiento (Final del Tto + 16
semanas)
Simple-ciego Doble ciego
Visitas cada 3 mM24
IPSS RAOCirugía
Objetivos primarios
Diseño del estudio CombAT
Siami et al. Contemp Clin Trials, 28 (2007); 770-779

CombAT dutasteride and tamsulosin 5ARI αblocq Combinado
Decreased libido 3 2 4
ED 7 5 9
Semen volume decreased < 1 < 1 2
Retrograde ejaculation < 1 1 4
MTOPS finasteride and doxazosin
Decreased libido 2.36 1.56 2.51
ED 4.53 3.56 5.11
EjD (abnormal ejaculation) 1.78 1.10 3.0
Sevilla 15 - 16 Noviembre 2012
El % de abandonos es similar para monoterapia y terapia combinada

Inhibidores de la 5αreductasa y HBP:
-La incidencia de alteraciones sexuales de ambos fármacos es similar
-Se desconoce el mecanismo fisiopatológico por el que se produce:¿Inhibición de la expresión NO andrógeno-dependiente?
Hellstrom WJG, Giuliano F, Rosen RC. Ejaculatory dysfunction and its association with lower urinary tract symptoms of benign prostatic hyperplasia and
BPH treatment. Urology 2009; 74: 15–21.
-Los eventos sexuales nuevos disminuyen con el paso del tiempoFinasteride vs placebo: la DE sólo aparece y empeora durante el 1er año de ttº. Posteriormente se estabiliza.
Wessells H, Roy J, Bannow J et al. Incidence and severity of sexual adverse experiences in finasteride and placebo-treated men with benign prostatic hyperplasia. Urology 2003; 61: 579–84.
Lo mismo se ha demostrado para DutasterideSchulman C, Pommerville P, Ho¨fner K, Wachs B. Long-term therapy with the dual 5alpha-reductase nhibitor dutasteride is well
tolerated in men with symptomatic benign prostatic hyperplasia. BJU Int 2005; 97: 73–80.
-La literatura sitúa en torno a un 7-25% la aparición de DE con ambos fármacos.
Sevilla 15 - 16 Noviembre 2012

-PDE5-I alone versus placebo included 2250 patients
PDE5-Is significantly ameliorateIPSS (2.8 [3.6 to 2.1]; p < 0.0001)IIEF score (+5.5 [+4.1 to +6.9]; p < 0.0001) but not Qmax (0.0 ml/s [0.6 to 0.6]
-αblockers alone vs a-blockers and PDE5-I included 107 patients
The combination of the two medications significantly improved IPSS (1.8 [3.7 to 0.0]; p = 0.05)IIEF score (+3.6 [+3.1 to +4.1]; p < 0.0001)Qmax (+1.5ml/s [+0.9 to +2.2]; p < 0.0001)
Sevilla 15 - 16 Noviembre 2012
A Systematic Review and Meta-analysis on the Use of Phosphodiesterase 5 Inhibitors Alone or in Combinationwith a-Blockers for Lower Urinary Tract Symptoms Due to Benign Prostatic Hyperplasia. Mauro Gacci a,*, Giovanni Corona b,c, Matteo Salvi a, Linda Vignozzi c, Kevin T. McVary d, Steven A. Kaplan e, Claus G. Roehrborn f, Sergio Serni a, Vincenzo Mirone g, Marco Carini a,Mario Maggi c. Eur Urol 2012

Sevilla 15 - 16 Noviembre 2012
2 RCT comparando RTUp vs WW:
1) Wasson et al:
Seguimiento de 2,8 años
DE: 19% vs 21%. No diferencias signifcativasWasson JH, Reda DJ, Bruskewitz RC, et al. A comparison of transurethral surgery with watchful
waiting for moderate symptoms of benign prostatic hyperplasia. The Veterans Affairs CooperativeStudy Group on Transurethral Resection of the Prostate. New Engl J 2002;324:1059–1061.
2) Brookes et al:340 participants.
Before treatment ED: 70% TURP and 67% WW.
After surgery DE: 55%TURP vs 72% WW
The odds ratio TURP vs WW was 0.37 (95% CI: 0.19–0.74). RTUp PROTEGE!!!
Brookes ST, Donovan JL, Peters TJ, Abrams P, Neal DE. Sexual dysfunction in men after treatment for lower urinary tractsymptoms: evidence from randomized controlled trial. BMJ. Med 1995 Jan;332(2):75-9

Metanalisis RTUp: 29 estudios incluidos
DE en 6,5%
La aparición de DE tras RTUp parece responder a factores de confusión más que a la propia técnica en si.
Madersbacher S, Marberger M. Is transurethral resection of the prostate still justified? Br J Urol 1999
Feb;83(3):227-37.

A total of 390 holmium laser vs 370 TURP.
The average follow-up in the studies was 21 months.
Of the eight studies, six provided data pertaining to erectile function without using any validated questionnaires
-DE: Holep 7.5% (3.9% - 11.2%) vs 7.7% RTUp(0% - 17%)
-Mejora la Función eréctil: Holep 7.1% (1.7%-20%) vs RTUp 6.2% (0%-19%)
RTUp vs Laser Holmium:
Asian Journal of Andrology (2010) 12: 500–508

KTP laser vs TURP:
Two studies used the validated questionnaires
127 men KTP laser group and 125 men TURP group.
The follow-up interval ranged from 6 to 36 months.
No new development of ED was reported?
Hamann MF, Naumann CM, Seif C, van der Horst C, Junemann KP, et al. Functional outcome following photoselective vaporization of the prostate (PVP): urodynamic findings within 12 months follow-up. Eur Urol 2008; 54: 902–10.

Sevilla Nov. 15-16 2012
The only randomized control trial comparing the thulium laser
52 patients thulium laser vs 48 patients TURP
Follow-up of 12 months.
They did not address erectile function
Xia SJ, Zhuo J, Sun XW, Han BM, Shao Y, et al. Thulium laser versus standard transurethral resection of the prostate: a randomized prospective trial. Eur Urol 2008; 53: 382–90.
Laser Thulium vs RTUp:

TUMT versus TURP
Four comparative studies
190 patients TUMT vs 148 patients TURP.
The length of follow-up 3 to 60 months.
Two studies used the validated questionnaires to evaluate sexual function [24, 27].
Collectively, TUMT had less adverse effects on sexual function.
ED : TUMT 8.7% (0%-18.2%) vs TURP 19.3% (14.3%-26.5%)
Improve EF: TUMT 15.2% vs 20.4% TURP.
Mattiasson A, Wagrell L, Schelin S, Nordling J, Richthoff J, et al. Five-year follow-up of feedback microwave thermotherapy versus TRUP for clinical BPH: a prospective randomized multicenter study. Urology 2007; 69: 91–6.
Norby B, Nielsen HV, Frimodt-Moller PC. Transurethral nterstitial laser coagulation of the prostate and transurethral microwave thermotherapy vs.transurethral resection or ncision of the prostate: results of a randomized, controlled study in patients with symptomatic benign prostatic hyperplasia. BJU Int 2002; 90: 853–62.

Three randomized control trials and one cohort study
Collectively, 198 patients TUNA vs 200 patients underwent TURP
The follow-up 3 to 60 months.
Two studies used validated questionnaires to evaluate erectile function
ED: 5.8% TUNA (0%-20%) vs TURP 18.2% (12%-26.5%).
Inprove EF: 7.9% TUNA vs 20.4% TURP.
TUNA vs TURP
Arai Y, Aoki Y, Okubo K, Maeda H, Terada N, et al. Impact of interventional therapy for benign prostatic hyperplasia onquality of life and sexual function: a prospective study. J Urol 2000; 164: 1206–11.

The variability that exists between studies and their heterogeneous design prevents firm conclusions concerning the risk of sexual dysfunction following prostate surgery.
Exists a high prevalence of ED amongst candidates for prostatic surgery for BPH.
A significant improvement in the IIEF EF domain scores can be found amongst prostate surgery candidates reporting ED preoperatively.
EF will improve in an important percentage of these patients postoperatively.
Exists an important risk of deterioration of EF following surgery, especially if EF is normal preoperatively.
Factors related to surgical effects on ED are unclear.
CONCLUSIONES:
Impact of Benign Prostatic Hyperplasia Surgery on Erectile FunctionJosé M. Martínez-Jabaloyas Rafael Villamón-Fort Manuel Gil-Salom Pascual Chuan-NuezUrol Int 2010;84:407–412