Embed Size (px)
Citation preview
Are Current DES the Final Answer?BioFreedomTM: the Polymer-Free Biolimus A9TM Coated Stent
Biosensors Lunch Symposium
25th April 2013
Prof. Stephen WL Lee, JP 李偉聯MD FRCP(Lon. Edin. Glas.) FHKCP FHKAM FACC FSCAI
Chief of Cardiology, Professor & Senior Consultant
Department of Medicine, Queen mary Hospital, University of Hong Kong

Speaker’s name: Stephen Wai-luen LEE
(Queen Mary Hospital, University of Hong Kong)
I have the following potential conflicts of interest to report:
Research contracts
Consulting
Employment in industry
Stockholder of a healthcare company
Owner of a healthcare company
Other(s)
I do not have any potential conflict of interest to declare
Potential conflicts of interest
x
The stents were provided by Biosensors as investigational devices.
The Core Laboratory Charges are supported by Biosensors.

PCI objective = purely for achieving revascularization
= without complicated issues of
• Acute failure
• Restenosis
• Stent thrombosis
• Prolonged DAPT
• BleedingBut many DES still show Poor Stent Healing :-drug cytotoxicity, polymer hypersensitivity, local inflammatory reactions, loss endothelial and vasomotor functions
• Stent thrombosis
• MACE
All current DES = can achieved neointimal suppression

Is stent thrombosis genuine ?
• Most powerful histological predictor of stent thrombosis = endothelial coverage• Most powerful surrogate indicator of endothelialization = neointimal coverage• Best morphometric predictor of LST = ratio of uncovered to total stent struts
Finn et al. Circulation 2007;115;2435-2441

Pooled Analysis of Data Comparing SES With BMSEstimated 4-year cumulative incidence of
stent thrombosis, death, MI, and TLR
2.0
1.5
1.0
0.5
0.00 1 2 3 4
Years Since Procedure
Ste
nt
Th
rom
bo
sis
(%
)
Sirolimus stent (1.2%)
Bare-metal stent (0.6%)
P=.20
10
6
4
2
00 1 2 3 4
Years Since Procedure
Sirolimus stent (6.4%)
Bare-metal stent (6.2%)
P=.86
8
Myo
card
ial In
farc
tio
n (
%)
30
20
10
00 1 2 3 4
Years Since Procedure
Bare-metal stent (23.6%)
P<.001
25
5
15T
arg
et-
Lesio
n
Reva
sc
ula
rizati
on
(%
)
Sirolimus stent (7.8%)
Years Since Procedure
10
6
4
2
00 1 2 3 4
Sirolimus stent (6.7%)
Bare-metal stent (5.3%)
P=.23
8
Death
(%
)
Stone et al. N Engl J Med. 2007;356:998-1008
2.0
1.5
1.0
0.5
0.00 1 2 3 4
Years Since Procedure
Ste
nt
Th
rom
bo
sis
(%
)
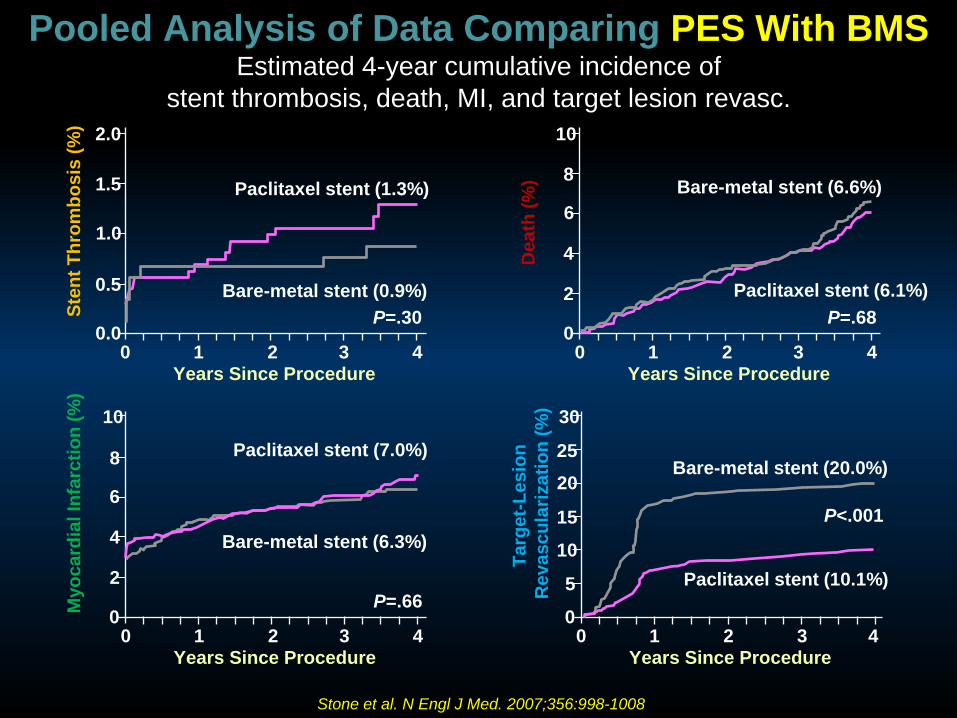
Paclitaxel stent (1.3%)
Bare-metal stent (0.9%)
P=.30
Pooled Analysis of Data Comparing PES With BMSEstimated 4-year cumulative incidence of
stent thrombosis, death, MI, and target lesion revasc.
10
8
6
2
00 1 2 3 4
Years Since Procedure
De
ath
(%
)
Paclitaxel stent (6.1%)
Bare-metal stent (6.6%)
P=.68
4
10
8
6
2
00 1 2 3 4
Years Since Procedure
Myo
card
ial In
farc
tio
n (
%)
Paclitaxel stent (7.0%)
Bare-metal stent (6.3%)
P=.66
4
30
25
20
5
00 1 2 3 4
Years Since Procedure
Targ
et-
Lesio
n
Reva
sc
ula
rizati
on
(%
)
Paclitaxel stent (10.1%)
Bare-metal stent (20.0%)
P<.00115
10
Stone et al. N Engl J Med. 2007;356:998-1008
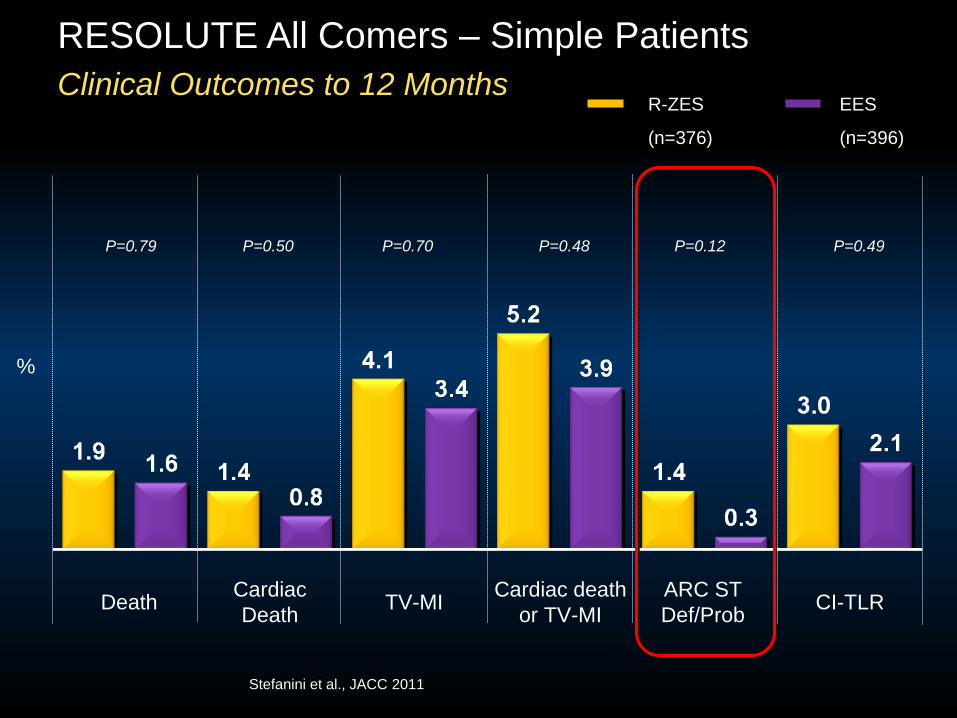
Cardiac
DeathTV-MI CI-TLRDeath
Cardiac death
or TV-MI
ARC ST
Def/Prob
RESOLUTE All Comers – Simple Patients
Clinical Outcomes to 12 MonthsR-ZES EES
(n=376) (n=396)
P=0.79 P=0.50 P=0.70 P=0.48 P=0.12 P=0.49
%
Stefanini et al., JACC 2011

Cardiac
DeathTV-MI CI-TLRDeath
ARC ST
Def/Prob
%
RESOLUTE All Comers – Complex Patients
Clinical Outcomes to 12 Months
P=0.02 P=0.24 P=0.90 P=0.58 P=0.26 P=0.80
R-ZES EES
(n=764) (n=756)
Cardiac death
or TV-MI
Stefanini et al., JACC 2011Resolute-US Trial: similar results between the 2 stents

Biolimus-A9™ Eluting Stent
• Biolimus is a semi-synthetic sirolimus analogue with 10x higher lipophilicity and similar potency as sirolimus.
• Biolimus is immersed at a concentration of 15.6 g/mm into a biodegradable polymer, polylactic acid, and applied solely to the abluminal stent surface by a fully automated process.
• Biolimus is co-released with polylactic acid and completely desolves into carbon dioxide and water after a 6-9 months period.
• The stainless steel stent platform has a strut thickness of 120 m with a quadrature link design.
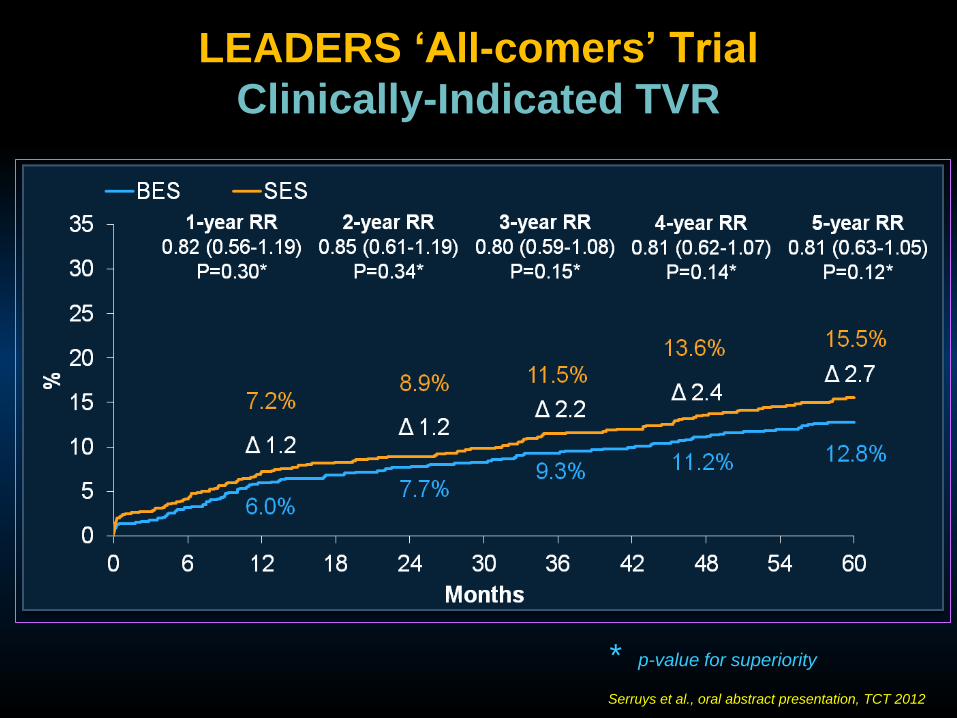
LEADERS ‘All-comers’ Trial
Clinically-Indicated TVR
* p-value for superiority
Serruys et al., oral abstract presentation, TCT 2012

LEADERS ‘All-comers’ Trial
Biomatrix (n=850) versus Cypher (n=850).DAPT = 12 months. 81% off-label use.
1o endpoint: MACE: Cardiac death, MI, clinically-indicated TVR (9 months)
5 years data available. Better outcomes than Cypher at 5 years.
Patie
nt O
rie
nte
d E
ndp
oin
ts (
Dea
th, M
I, T
LR
, T
VR
)

P for interaction=0.022
* p-value for superiority
Serruys et al., oral abstract presentation, TCT 2012
Definite ST (ARC)
Landmark Analysis @ 1 Year
LEADERS ‘all-comers’ Trial


ESC guidelines 2010
Wijns et al., Eur Heart J. 2010; 31(20): 2501-55.
But these are guidelines based on clinical outcomes.
Is there any more scientific approach:-
(In-vivo assessment of stent healing guiding of DAPT duration)

Biomatrix (Biolimus-A9™ PLA) DES
Polymer-free drug elution via porous surface
Biofreedom (Biolimus-A9™) DCS
Potential Advantages
• Reduced late adverse effects due to polymer
hypersensitivity
• Improved surface integrity with no polymer to be
sheared or peeled away from the stent struts
• Possible shorter DAPT with better healing without
polymer and inner BMS surface
11
Highest lipophilicity of the common limus drugs
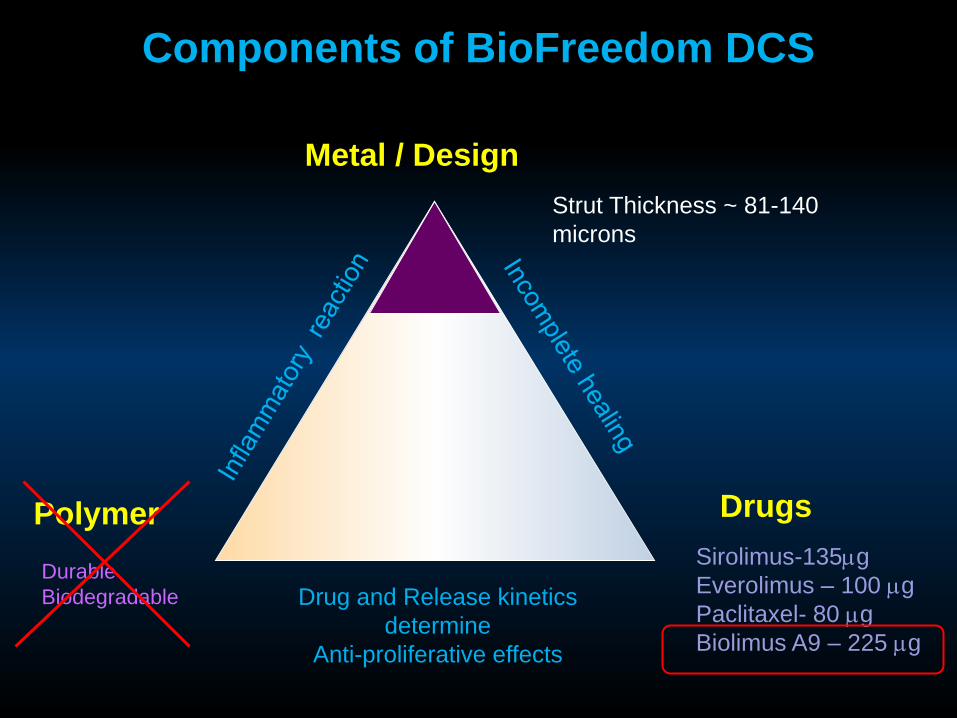
Components of BioFreedom DCS
Metal / Design
Polymer Drugs
Drug and Release kinetics
determine
Anti-proliferative effects
Sirolimus-135g
Everolimus – 100 g
Paclitaxel- 80 g
Biolimus A9 – 225 g
Strut Thickness ~ 81-140
microns
Durable
Biodegradable
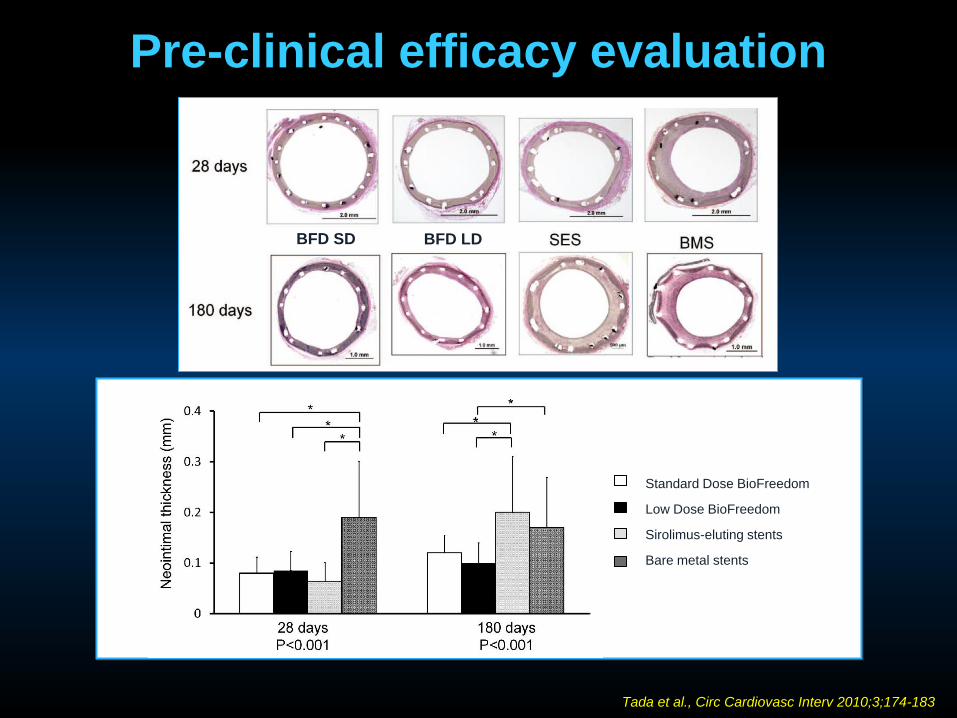
Tada et al., Circ Cardiovasc Interv 2010;3;174-183
Pre-clinical efficacy evaluation
Standard Dose BioFreedom
Low Dose BioFreedom
Sirolimus-eluting stents
Bare metal stents
BFD LDBFD SD

BioFreedom FIM design
BioFreedom FIM182 patients
12 Month Angio FU107 patients
BioFreedom
standard
dose
(BFD SD)
N=35
BioFreedom
low
dose
(BFD LD)
N=36
TAXUS®
Liberté ®
N=36
Second Cohort
Enrollment Period
Jan 2009 – Jun 2009
BioFreedom
standard
dose
(BFD SD)
N=25
BioFreedom
low
dose
(BFD LD)
N=26
TAXUS®
Liberté ®
N=24
4 Month Angio FU75 patients
First Cohort
Enrollment Period
Sept 2008 – Jan 2009
Angio FU 92%
12 Month Clinical FU 99%
Angio FU 92%
1o End-point: In-stent Late Lumen Loss at 4 months (LD) and 12 months (Standard Dose)
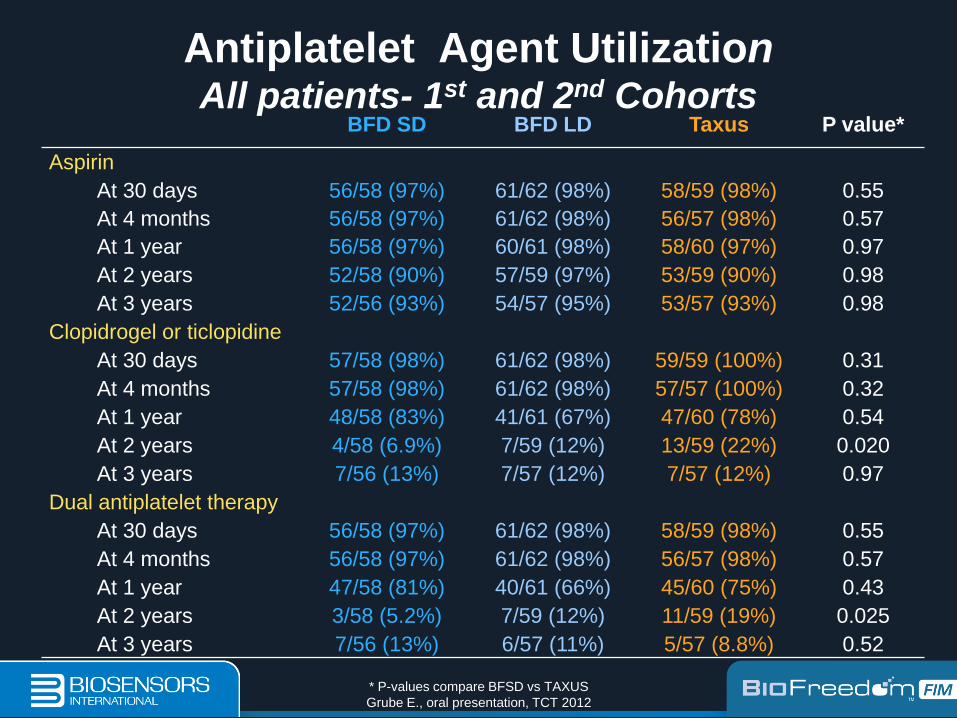
Antiplatelet Agent UtilizationAll patients- 1st and 2nd Cohorts
* P-values compare BFSD vs TAXUS
Grube E., oral presentation, TCT 2012
BFD SD BFD LD Taxus P value*
Aspirin
At 30 days 56/58 (97%) 61/62 (98%) 58/59 (98%) 0.55
At 4 months 56/58 (97%) 61/62 (98%) 56/57 (98%) 0.57
At 1 year 56/58 (97%) 60/61 (98%) 58/60 (97%) 0.97
At 2 years 52/58 (90%) 57/59 (97%) 53/59 (90%) 0.98
At 3 years 52/56 (93%) 54/57 (95%) 53/57 (93%) 0.98
Clopidrogel or ticlopidine
At 30 days 57/58 (98%) 61/62 (98%) 59/59 (100%) 0.31
At 4 months 57/58 (98%) 61/62 (98%) 57/57 (100%) 0.32
At 1 year 48/58 (83%) 41/61 (67%) 47/60 (78%) 0.54
At 2 years 4/58 (6.9%) 7/59 (12%) 13/59 (22%) 0.020
At 3 years 7/56 (13%) 7/57 (12%) 7/57 (12%) 0.97
Dual antiplatelet therapy
At 30 days 56/58 (97%) 61/62 (98%) 58/59 (98%) 0.55
At 4 months 56/58 (97%) 61/62 (98%) 56/57 (98%) 0.57
At 1 year 47/58 (81%) 40/61 (66%) 45/60 (75%) 0.43
At 2 years 3/58 (5.2%) 7/59 (12%) 11/59 (19%) 0.025
At 3 years 7/56 (13%) 6/57 (11%) 5/57 (8.8%) 0.52

0.17[0.09, 0.39]
0.22[0.17, 0.66]
0.35[0.22, 0.57]
0.0
0.1
0.2
0.3
0.4
0.5
BFD SD BFD LD TAXUS
2nd Cohort – PRIMARY ENDPOINT
P = 0.001* (p=0.11**)
P = 0.21* (p=0.55**)
(mm
)
N = 31 N = 31N = 35
*Non-inferiority tests based on the mean. **Superiority tests.
All values are presented as median [IQR].
Grube E., oral presentation, TCT 2010
In-stent Late Lumen Loss (12 months)

EVENT BFD SD
N = 60
BFD LD
N = 62
TAXUS
N = 60
MACE
(All Death, MI, Emergent Bypass
or TLR)
3 (5.1%) 7 (11.5%) 3 (5.0%)
All Death 1 (1.7%) 0 (0.0%) 0 (0.0%)
MI 1 (1.7%) 1 (1.6%) 0 (0.0%)
Q Wave MI 0 (0.0%) 0 (0.0%) 0 (0.0%)
Non-Q Wave MI 1 (1.7%) 1 (1.6%) 0 (0.0%)
Emergent Bypass 0 (0.0%) 0 (0.0%) 0 (0.0%)
TLR 1 (1.7%) 6 (9.8%) 3 (5.0%)
Definite/probable stent
thrombosis (ARC)0 (0.0%) 0 (0.0%) 0 (0.0%)
All patients – 1st and 2nd Cohorts (98.9%)
All P values are non-significant.
Tests were performed for BFD SD vs. TAXUS and BFD LD vs. TAXUS.
Grube E., oral presentation, TCT 2010
BioFreedom 12-Month Outcomes

EVENT BFD SD
N = 60
BFD LD
N = 62
TAXUS
N = 60
MACE (All Death, MI, Emergent
Bypass or TLR)7(11.9%) 11(18.1%) 6(10.0%)
All Death 3(5.1%) 2(3.3%) 1(1.7%)
MI 1(1.7%) 2(3.4%) 1(1.7%)
Q Wave MI 0(0.0%) 0(0.0%) 0(0.0%)
Non-Q Wave MI 1(1.7%) 2(3.4%) 1(1.7%)
Emergent Bypass 0(0.0%) 0(0.0%) 0(0.0%)
TLR 3(5.2%) 8(13.2%) 4(6.7%)
Definite/probable stent
thrombosis (ARC)0(0.0%) 0(0.0%) 0(0.0%)
All patients – 1st and 2nd Cohorts (96.1%)
All P values are non-significant. Tests were performed for BFD SD vs. TAXUS and BFD LD vs. TAXUS
Grube E , TCT 2012
BioFreedom 36-Month Outcomes
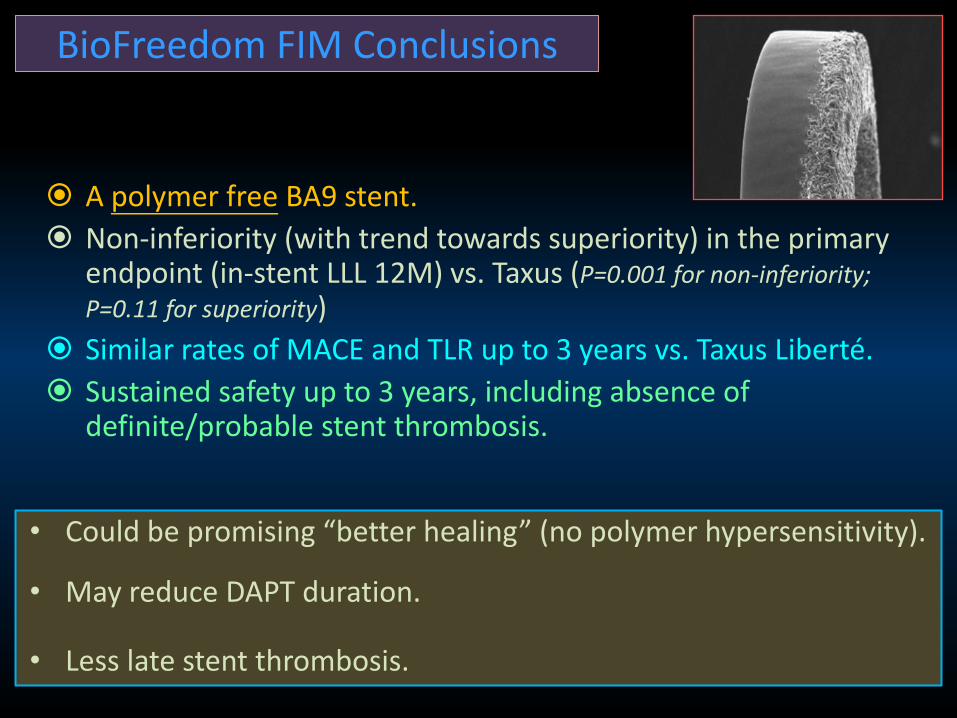
A polymer free BA9 stent.
Non-inferiority (with trend towards superiority) in the primary endpoint (in-stent LLL 12M) vs. Taxus (P=0.001 for non-inferiority;
P=0.11 for superiority)
Similar rates of MACE and TLR up to 3 years vs. Taxus Liberté.
Sustained safety up to 3 years, including absence of definite/probable stent thrombosis.
BioFreedom FIM Conclusions
• Could be promising “better healing” (no polymer hypersensitivity).
• May reduce DAPT duration.
• Less late stent thrombosis.

Leaders Free Trial
• Biosensors BioFreedom™ BA9 Drug-Coated Coronary Stent (DCS)
• Biosensors Gazelle™ Bare Metal Coronary Stent (BMS)
Two stents
• ASA 100-160 mg OD, indefinitely
• 1 month DAPT (Clopidogrel 75 mg OD or another P2Y12 inhibitor)
One DAPT regimen
Randomise, double-blind, 1:1 control study.
60+ centres world-wide 2400+ patients with high risk of bleeding.
FU for 2 years.
Co-Primary Endpoints(1) Safety (non-inferiority) – MACE (Death, MI, Stent Thrombosis)
(2) Efficacy (superiority) - clinically-driven TLR
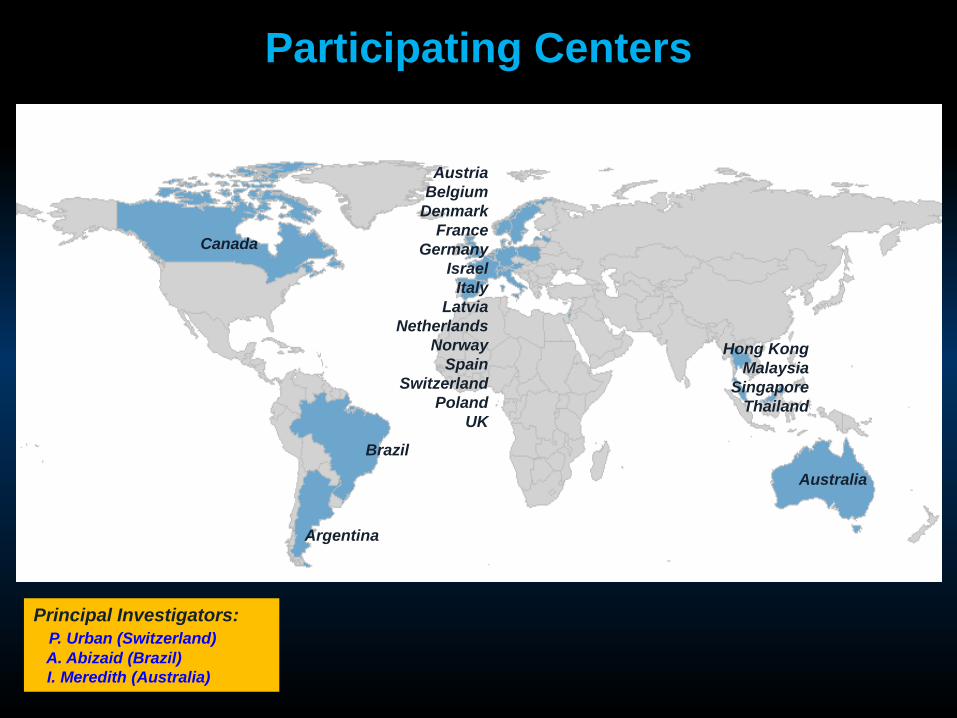
Brazil
Canada
Australia
Argentina
Hong Kong
Malaysia
Singapore
Thailand
Austria
Belgium
Denmark
France
Germany
Israel
Italy
Latvia
Netherlands
Norway
Spain
Switzerland
Poland
UK
Participating Centers
Principal Investigators:
P. Urban (Switzerland)
A. Abizaid (Brazil)
I. Meredith (Australia)

Primary Endpoint: OCT % strut coverage from 1 to 6 months.
Secondary Endpoints: Clinical Endpoints (MACE)
QCA & OCT Findings at 9 months
Drug therapy: ASA and clopidogrel (per guidelines for 9 months)
Clinical Follow up: 30d, 6mo, 9mo, 12mo, 1yr, 2yr.
N = 100 patients Single Center
Initial PCI procedure angiogram (baseline OCT)Randomly assigned to 6 FU groups at 1,2,3,4,5 & 6 months (OCT)Final restudy angiogram & OCT at 9 months
1mo 9 mo
OCT
Clinical
Endpoint
BioFreedom DCS Stent
Real World, All Comers
With symptomatic coronary artery disease
3mo 4mo 5mo 6mo 12mo 24moBaseline 2mo
1st Angiographic & OCT FU 2nd OCT FU
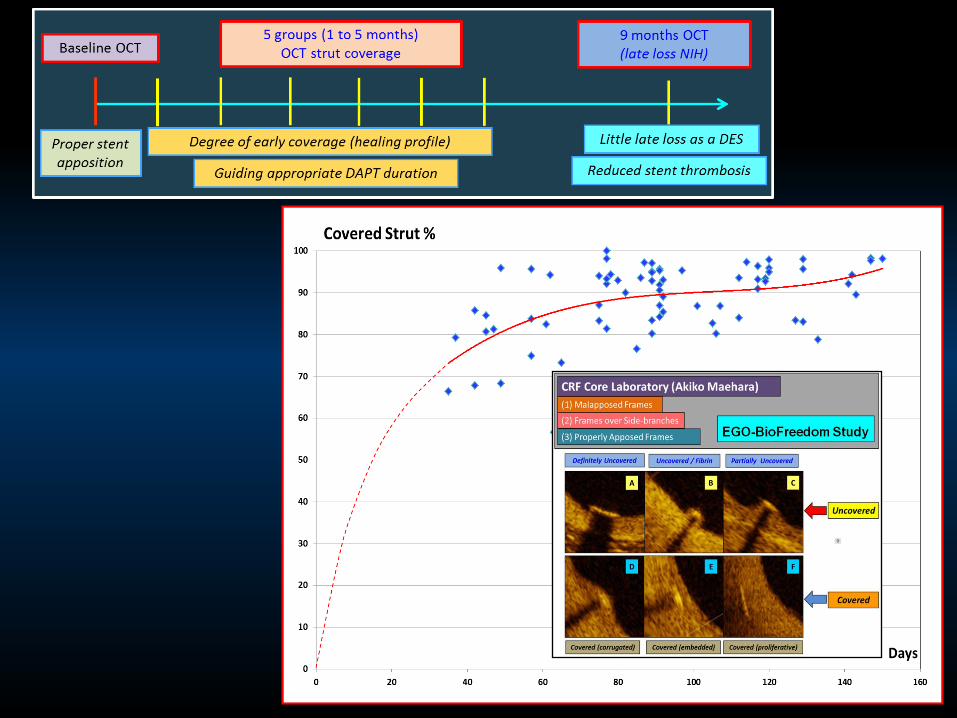
EGO-BioFreedom Study
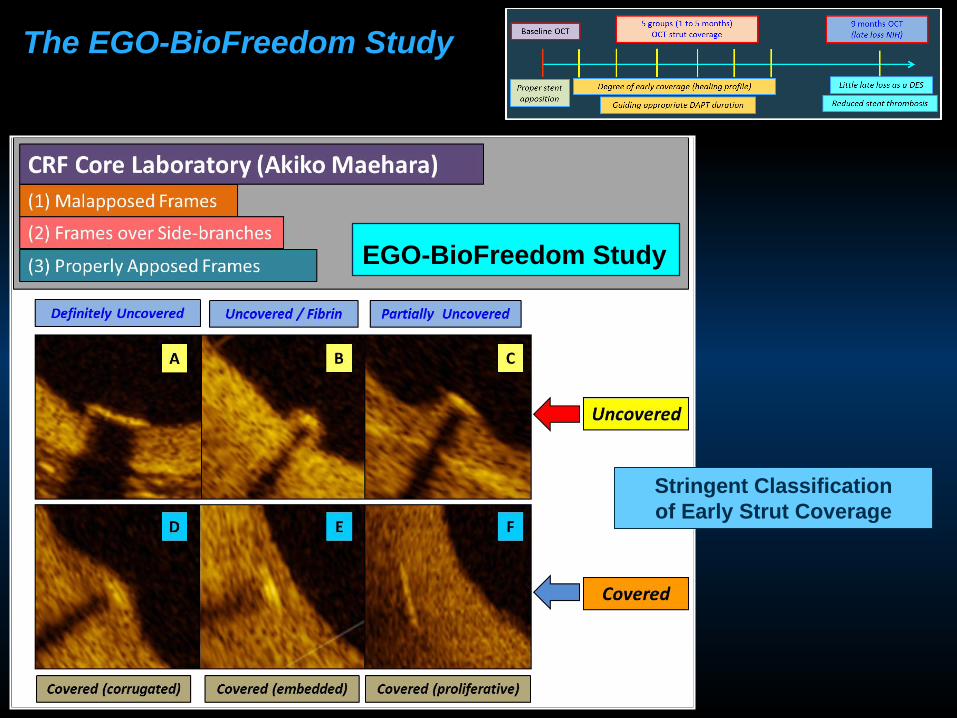
EGO-BioFreedom Study
The EGO-BioFreedom Study
Stringent Classification
of Early Strut Coverage
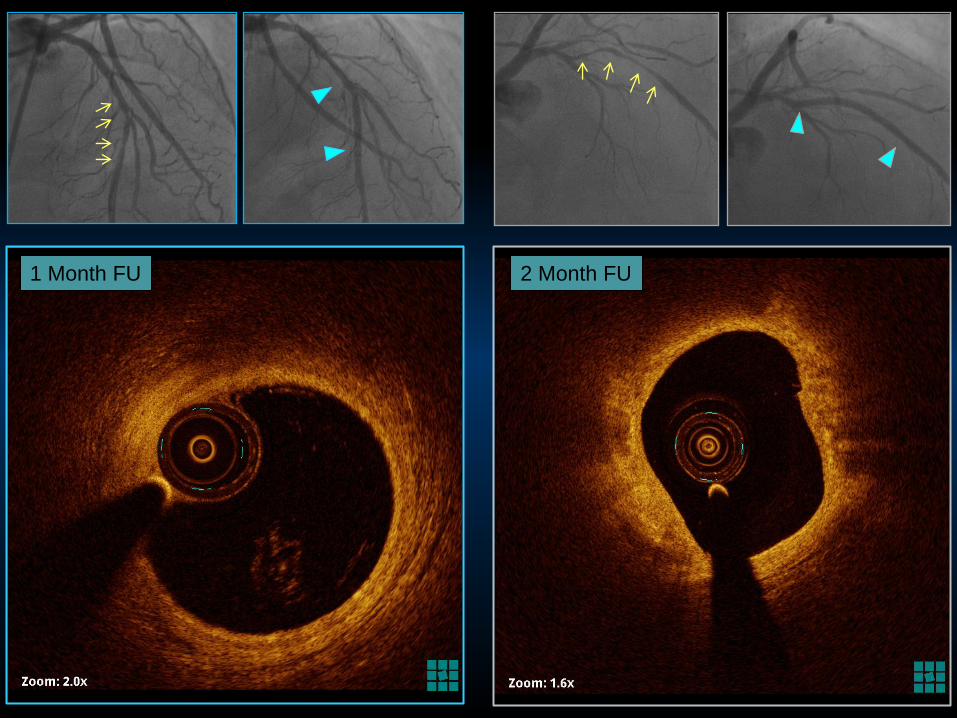
1 Month FU 2 Month FU
A B C
D E F
Very stringent strut coverage classification
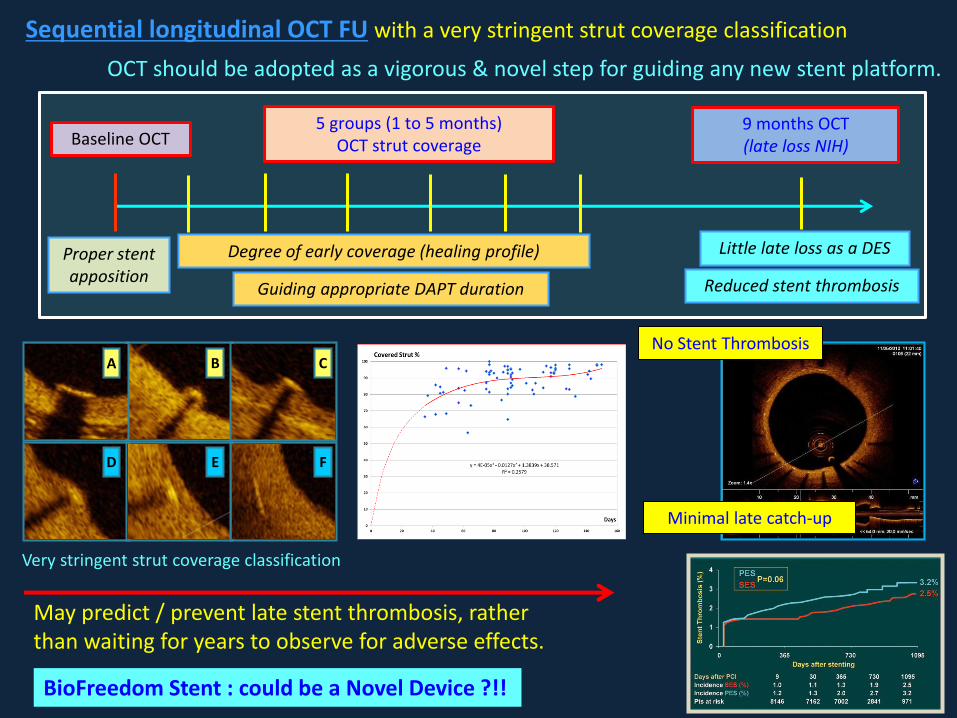
Sequential longitudinal OCT FU with a very stringent strut coverage classification
May predict / prevent late stent thrombosis, ratherthan waiting for years to observe for adverse effects.
OCT should be adopted as a vigorous & novel step for guiding any new stent platform.
BioFreedom Stent : could be a Novel Device ?!!
No Stent Thrombosis
Minimal late catch-up
Baseline OCT9 months OCT(late loss NIH)
5 groups (1 to 5 months)OCT strut coverage
Degree of early coverage (healing profile)
Guiding appropriate DAPT duration Reduced stent thrombosis
Little late loss as a DES Proper stent apposition
The Leaders-Free & EGO-Biofreedom Study
Thank you

PCI objective = purely for achieving revascularization
= without complicated issues of
• Acute failure
• Restenosis
• Stent thrombosis
• Prolonged DAPT
But many DES still show poor Stent Healing =
drug cytotoxicity, polymer hypersensitivity, local inflammatory reactions, loss endothelial and vasomotor functions
• Stent thrombosis
• MACE
BMS vs. DES
All current DES = can achieved neointimal suppression