Embed Size (px)
Citation preview
Bone: Normal Physiology and Response to Injury
Wongworawat
August 3, 2010
Structure
• Cortical vs. Trabecular
• Woven vs. Lamellar
• Vascular supply– Nutrient artery—intramedullary– Periosteal– Periarticular plexus
Extracellular Matrix
• Mineral: 2/3– Hydroxyapatite Ca10(PO4)6(OH)2
• Organic– Type I collagen: 90%– Noncollagenous protein: 10%
• Osteocalcin, most abundant
• Proteoglycans
• Others
Collagen Problems
• OI: Type I collagen
• Scurvy: Ascorbic acid dependent prolyl hydroxylase and lysyl hydroxylase
• Ehlers-Danlos: Lysyl oxidase for crosslinking
• Urinary detection of turnover: pyridinoline, telopeptide, and hydroxyproline
Bone Cells
• Osteoblasts– Receptor for PTH– Roles
• Form bone
• Regulate osteoclasts
– Lipoprotein receptor-related protein 5 (LRP5)• Transmembrane protein for osteoblast proliferation
regulation
• Signaling important for maintenance of bone mass
Bone Cells
• Osteoblast differentiation– Stem cell– Mesenchymal stem cell– Osteoprogenitor– Pre-osteoblast– Mature osteoblast– Osteocyte– Cell deth
Osteoblastic Problems
• Fibrodysplasia ossificans progressiva– Activating mutation in BMP receptor ACVR1
• Cleidocranial dysostosis– Loss of runx 2 gene (formerly CBFA 1)
– Runx 2: transcription factor, “master regulator” of osteoblast differentiation
Osteoclasts
• Lineage: related to hematopoietic cells, macrophages
• Receptors– Calcitonin– RANKL, (osteoprotegrin)– Integrin
• Half-life: 10 days
Form and Function
• Remodeling– Trabecular– Cortical
• Molecular coupling– PTH– RANKL– BMP
Mechanical Regulation
• Wolff’s Law
Mechanical Properties
• Anisotropic– Stronger in compression than tension
• Viscoelastic– Higher stiffness and strength at higher loading
rates
Aging
• Osteoporosis: 2.5 SD < young standard
• Increase in both inner and outer diamters
• More anisotropy
Bone Injury and Repair
• Osteonecrosis
• Fracture
• Fixation
• Adjunctive therapies
Osteonecrosis
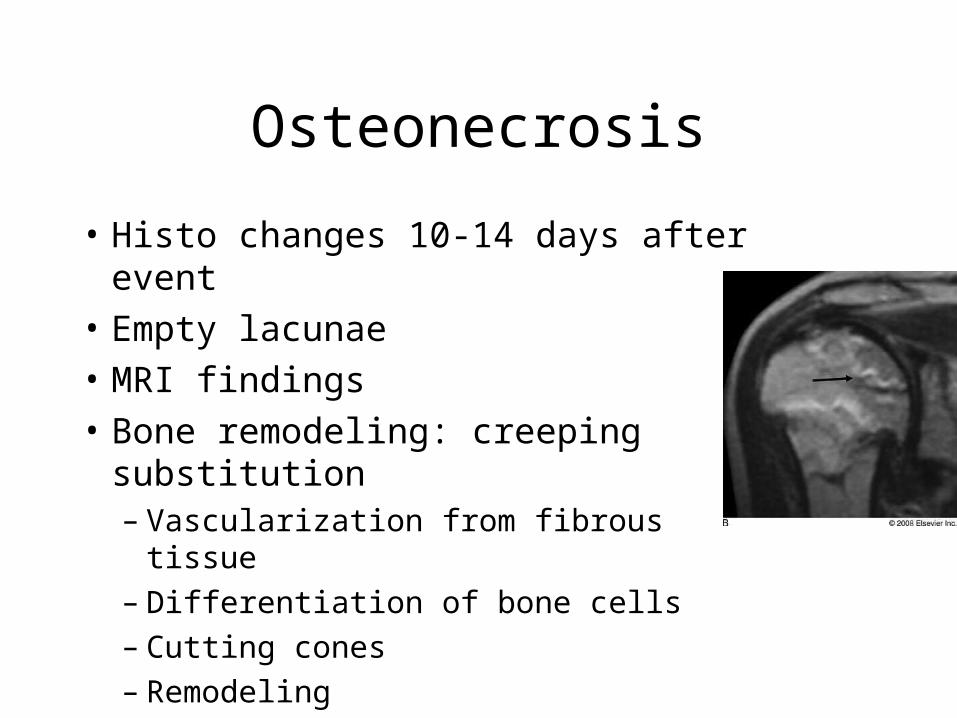
• Histo changes 10-14 days after event
• Empty lacunae
• MRI findings
• Bone remodeling: creeping substitution– Vascularization from fibrous tissue– Differentiation of bone cells– Cutting cones– Remodeling
Fracture Healing
• External factors– Micromotion: endochondral ossification– Rigid fixation: direct intramembranous
ossification
Fracture Healing
• Inflammatory response
• Cell differentiation– sox9 upregulates cartilage genes (col2)– Hypertrophic chondrocytes: type X collagen
• Ossification
• Remodeling
Chondrogenesis Pathology
• Camptomelic dysplasia: sox9 mutation
• Cleidocranial dysplasia: runx2 mutation
• Multiple epiphyseal dysplasia (MED): cartilage oligomeric matrix protein (COMP)
• Diastrophic dysplasia: sulfate transport protein
Fixation Biomechanics
• Intramedullary device
• Plates– Rigidity: thickness3
• External fixation– Rigidity
• Pin diameter, number, bone to rod distance, pin group separation, ½ pins separated 45°
Bone Grafts
• Osteoconductive
• Osteoinductive
• Osteogenic
• Gold Standard: Autograft
Allograft
• Structural
• Particulate
• Demineralized
Minerals and Other
• Calcium sulfate
• Tricalcium phosphate ceramics
• Calcium phosphate cements
• Polymers
BMP
• TGF- β family
• Bind cell curface receptors– Serine/threonine kinase receptors
• Phosphorylate SMADs
• SMADs translocates into nucleus to activate genes for osteoblast differentiation
Adjunctive Therapies
• Inductive coupling (magnetic)– Upregulation TGF-β1, FGF-2, BMP
• Capacitative coupling (electrodes)– Transmembrane calcium translocation– Upregulation of TGF- β1, BMP
• Ultrasound– Increased TGF- β1, PGE2, PDGF