Embed Size (px)
Citation preview

By
Hussam A.S. Murad and Khaled A. MahmoudDepartment of Pharmacology and Therapeutics
Faculty of Medicine , Ain Shams University
By
Hussam A.S. Murad and Khaled A. MahmoudDepartment of Pharmacology and Therapeutics
Faculty of Medicine , Ain Shams University
Does a Combination of Rosiglitazone and
Fenofibrate (Peroxisome Proliferator Activated
Receptor (PPAR) γ and α agonists respectively)
Achieve More Beneficial Effects than
Rosiglitazone (a PPAR γ agonist) in
Diabetic Rats ?
Does a Combination of Rosiglitazone and
Fenofibrate (Peroxisome Proliferator Activated
Receptor (PPAR) γ and α agonists respectively)
Achieve More Beneficial Effects than
Rosiglitazone (a PPAR γ agonist) in
Diabetic Rats ?
Type II diabetes mellitus is characterized by impaired glucose tolerance and insulin resistance. It is associated with hyperglycemia, dyslipidemia, obesity and vascular complications, leading to impaired life quality and increased mortality. None of the clinically used drugs has proved sufficiently effective in restoring normal glucose metabolism alone or in combination therapy as the disease progresses.
Thiazolidinediones (PPAR agonists) improve glucose metabolism by increasing peripheral insulin sensitivity, in addition, they decrease serum triglycerides.
Fibrates (PPAR α agonists) are hypolipidemic drugs acting mainly in the liver and skeletal muscle regulating intracellular lipid homeostasis.
Type II diabetes mellitus is characterized by impaired glucose tolerance and insulin resistance. It is associated with hyperglycemia, dyslipidemia, obesity and vascular complications, leading to impaired life quality and increased mortality. None of the clinically used drugs has proved sufficiently effective in restoring normal glucose metabolism alone or in combination therapy as the disease progresses.
Thiazolidinediones (PPAR agonists) improve glucose metabolism by increasing peripheral insulin sensitivity, in addition, they decrease serum triglycerides.
Fibrates (PPAR α agonists) are hypolipidemic drugs acting mainly in the liver and skeletal muscle regulating intracellular lipid homeostasis.
The present study was conducted to compare effects of rosiglitazone (a PPAR agonist) with those of a combination of rosiglitazone and fenofibrate (PPAR and agonists respectively) on fasting blood glucose, lipids, insulin and glycosylated hemoglobin in type 2 diabetic rats.
The present study was conducted to compare effects of rosiglitazone (a PPAR agonist) with those of a combination of rosiglitazone and fenofibrate (PPAR and agonists respectively) on fasting blood glucose, lipids, insulin and glycosylated hemoglobin in type 2 diabetic rats.
(A) Induction of type 2 DM by streptozotocin under nicotinamide protection in rats:
Rats were administered nicotinamide (290 mg/kg) by intraperitoneal injection 15 minutes before streptozotocin (60 mg/kg) by intravenous injection . Fasting blood glucose, lipids, insulin and glycosylated hemoglobin levels were determined before and 3 days after injection of streptozotocin. Rats having blood glucose levels below 150 mg/dl were considered non-diabetic.
(B) Effects of rosiglitazone versus rosiglitazone plus fenofibrate on blood glucose, lipids, insulin and glycosylated hemoglobin levels in STZ-NA diabetic rats:
3 groups (6/group) were used which received the following by gastric gavage for 4 weeks: Group I (Control group): 0.5 ml D.W. Group II (Rosiglitazone group): Rosiglitazone 3mg /kg/ day. Group III (Rosiglitazone and Fenofibrate group): Rosiglitazone 3mg /kg/ day and
fenofibrate 95 mg/kg/day After 4 weeks , blood was collected for measurement of :
(I) Fasting glucose level : Using the enzymatic method
(II) Lipids levels (cholesterol , triglycerides, high density lipo-proteins (HDL) cholesterol and low density lipoproteins (LDL)) : Using the enzymatic methods
(III) Insulin level : Using ELISA
(IV) Glycosylated hemoglobin level : Using haemolysate.
(A) Induction of type 2 DM by streptozotocin under nicotinamide protection in rats:
Rats were administered nicotinamide (290 mg/kg) by intraperitoneal injection 15 minutes before streptozotocin (60 mg/kg) by intravenous injection . Fasting blood glucose, lipids, insulin and glycosylated hemoglobin levels were determined before and 3 days after injection of streptozotocin. Rats having blood glucose levels below 150 mg/dl were considered non-diabetic.
(B) Effects of rosiglitazone versus rosiglitazone plus fenofibrate on blood glucose, lipids, insulin and glycosylated hemoglobin levels in STZ-NA diabetic rats:
3 groups (6/group) were used which received the following by gastric gavage for 4 weeks: Group I (Control group): 0.5 ml D.W. Group II (Rosiglitazone group): Rosiglitazone 3mg /kg/ day. Group III (Rosiglitazone and Fenofibrate group): Rosiglitazone 3mg /kg/ day and
fenofibrate 95 mg/kg/day After 4 weeks , blood was collected for measurement of :
(I) Fasting glucose level : Using the enzymatic method
(II) Lipids levels (cholesterol , triglycerides, high density lipo-proteins (HDL) cholesterol and low density lipoproteins (LDL)) : Using the enzymatic methods
(III) Insulin level : Using ELISA
(IV) Glycosylated hemoglobin level : Using haemolysate.
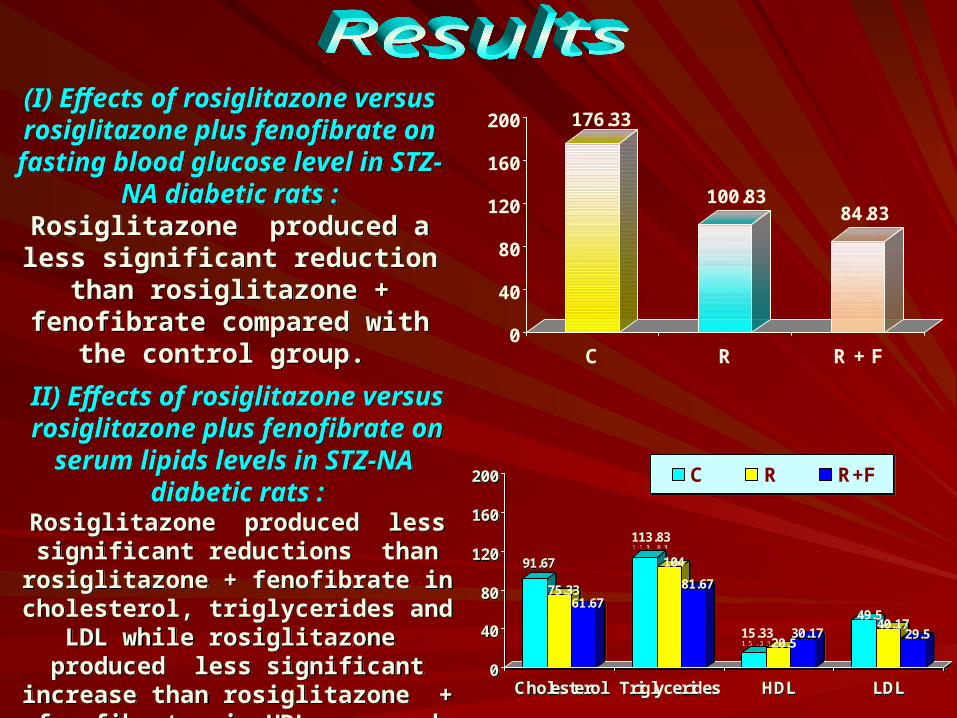
(I) Effects of rosiglitazone versus rosiglitazone plus fenofibrate on
fasting blood glucose level in STZ-NA diabetic rats :
Rosiglitazone produced a less significant reduction than
rosiglitazone + fenofibrate compared with the control group.
(I) Effects of rosiglitazone versus rosiglitazone plus fenofibrate on
fasting blood glucose level in STZ-NA diabetic rats :
Rosiglitazone produced a less significant reduction than
rosiglitazone + fenofibrate compared with the control group.
176.33
100.8384.83
0
40
80
120
160
200
C R R + F
II) Effects of rosiglitazone versus rosiglitazone plus fenofibrate on
serum lipids levels in STZ-NA diabetic rats :
Rosiglitazone produced less significant reductions than rosiglitazone + fenofibrate in cholesterol, triglycerides and LDL while
rosiglitazone produced less significant increase than rosiglitazone + fenofibrate
in HDL compared with the control groups
II) Effects of rosiglitazone versus rosiglitazone plus fenofibrate on
serum lipids levels in STZ-NA diabetic rats :
Rosiglitazone produced less significant reductions than rosiglitazone + fenofibrate in cholesterol, triglycerides and LDL while
rosiglitazone produced less significant increase than rosiglitazone + fenofibrate
in HDL compared with the control groups
91.67
75.3361.67
113.83
104
81.67
15.3320.5
30.1749.5
40.1729.5
0
40
80
120
160
200
Cholesterol Triglycerides HDL LDL
C R R+F
91.67
75.3361.67
113.83
104
81.67
15.3320.5
30.1749.5
40.1729.5
0
40
80
120
160
200
Cholesterol Triglycerides HDL LDL
C R R+F
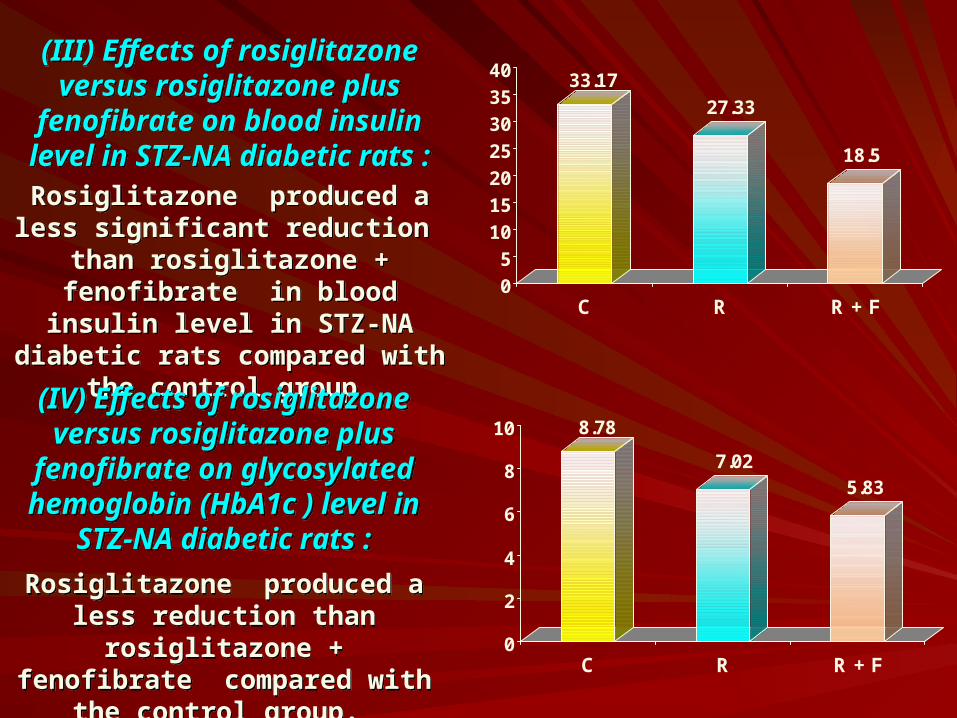
(III) Effects of rosiglitazone versus rosiglitazone plus
fenofibrate on blood insulin level in STZ-NA diabetic rats :
Rosiglitazone produced a less significant reduction than
rosiglitazone + fenofibrate in blood insulin level in STZ-NA diabetic rats
compared with the control group
(III) Effects of rosiglitazone versus rosiglitazone plus
fenofibrate on blood insulin level in STZ-NA diabetic rats :
Rosiglitazone produced a less significant reduction than
rosiglitazone + fenofibrate in blood insulin level in STZ-NA diabetic rats
compared with the control group
33.17
27.33
18.5
0
5
10
15
20
25
30
35
40
C R R + F
(IV) Effects of rosiglitazone versus rosiglitazone plus
fenofibrate on glycosylated hemoglobin (HbA1c ) level in
STZ-NA diabetic rats :
Rosiglitazone produced a less reduction than rosiglitazone + fenofibrate compared with the
control group.
(IV) Effects of rosiglitazone versus rosiglitazone plus
fenofibrate on glycosylated hemoglobin (HbA1c ) level in
STZ-NA diabetic rats :
Rosiglitazone produced a less reduction than rosiglitazone + fenofibrate compared with the
control group.
8.78
7.025.83
0
2
4
6
8
10
C R R + F
PPAR- is highly expressed in adipose tissue, with low expression in nonadipose tissues. PPAR- is highly expressed in nonadipose tissues and it regulates intracellular lipid homeostasis through upregulation of fatty acid oxidative enzymes mainly in the liver and skeletal muscle. Also it increases insulin sensitivity and reduces lipid accumulation in skeletal muscle.
Combination of rosiglitazone and fenofibrate have many advantages over rosiglitazone alone. Fenofibrate prevents pancreatic islets hypertrophy and atrophy while rosiglitazone does not affect islet hypertrophy at earlier stages but prevents ß-cell atrophy at later stages. Also fenofibrate decreases while rosiglitazone increases body weight. Despite the opposite effects on adiposity, both drugs improve insulin actions in skeletal muscle and decrease triglyceride content in muscle and pancreatic islets.
Coactivation of PPAR and induces the expression of genes in the peroxisomal -oxidation pathway while these genes are unaffected by rosiglitazone. For all genes tested, the maximum degree of increase by coactivation of PPAR and is about 20% higher than that with rosiglitazone.
PPAR- is highly expressed in adipose tissue, with low expression in nonadipose tissues. PPAR- is highly expressed in nonadipose tissues and it regulates intracellular lipid homeostasis through upregulation of fatty acid oxidative enzymes mainly in the liver and skeletal muscle. Also it increases insulin sensitivity and reduces lipid accumulation in skeletal muscle.
Combination of rosiglitazone and fenofibrate have many advantages over rosiglitazone alone. Fenofibrate prevents pancreatic islets hypertrophy and atrophy while rosiglitazone does not affect islet hypertrophy at earlier stages but prevents ß-cell atrophy at later stages. Also fenofibrate decreases while rosiglitazone increases body weight. Despite the opposite effects on adiposity, both drugs improve insulin actions in skeletal muscle and decrease triglyceride content in muscle and pancreatic islets.
Coactivation of PPAR and induces the expression of genes in the peroxisomal -oxidation pathway while these genes are unaffected by rosiglitazone. For all genes tested, the maximum degree of increase by coactivation of PPAR and is about 20% higher than that with rosiglitazone.
Thiazolidinediones reduce fat accumulation in skeletal muscle, heart and pancreatic ß-cells (preventing their apoptosis) and improve insulin action in muscle. This is through sequestering lipids in adipose tissue or increasing production of adiponectin (an adipocytokine that increases insulin sensitivity). Fenofibrate prevents the development of diabetes in diabetes-prone rats by reducing adiposity, improving peripheral insulin action and preventing ß-cell destruction.
Insulin resistance and hyperinsulinemia improve in various models of type 2 DM upon activation of PPAR and PPAR through effects on fatty acid and glucose homeostasis. Activation of PPAR reduces hepatic glucose production, improves glucose disposal to muscle and adipose tissue and lowers circulating fatty acids due to sequestering into adipose tissue and decreasing lipolysis leading to secondary beneficial effects on muscle and/or liver. Activation of PPAR mediates catabolism of fatty acids mainly through hepatic fatty acid oxidation.
Thiazolidinediones reduce fat accumulation in skeletal muscle, heart and pancreatic ß-cells (preventing their apoptosis) and improve insulin action in muscle. This is through sequestering lipids in adipose tissue or increasing production of adiponectin (an adipocytokine that increases insulin sensitivity). Fenofibrate prevents the development of diabetes in diabetes-prone rats by reducing adiposity, improving peripheral insulin action and preventing ß-cell destruction.
Insulin resistance and hyperinsulinemia improve in various models of type 2 DM upon activation of PPAR and PPAR through effects on fatty acid and glucose homeostasis. Activation of PPAR reduces hepatic glucose production, improves glucose disposal to muscle and adipose tissue and lowers circulating fatty acids due to sequestering into adipose tissue and decreasing lipolysis leading to secondary beneficial effects on muscle and/or liver. Activation of PPAR mediates catabolism of fatty acids mainly through hepatic fatty acid oxidation.
New class of drugs for treatment of type 2 diabetes called the non-thiazolidinedione or the "glitazar" class are PPAR and agonists under investigation, showed lower levels of blood triglycerides, free fatty acids, glucose and insulin and improved polyuria after four weeks of treatment in diabetic mice. Ragaglitazar reduced circulating insulin, improved insulin sensitivity and reduced Hb A1c to a greater extent than rosiglitazone alone. Muraglitazar improved glycemic control and dyslipidemia associated with type 2 diabetes and this may reduce the risk of cardiovascular complications. The dual PPAR / agonist LY-465608 completely restored euglycemia in diabetic rats during treatment in the early diabetic period (8-12 week of age) without increase in body weight.
New class of drugs for treatment of type 2 diabetes called the non-thiazolidinedione or the "glitazar" class are PPAR and agonists under investigation, showed lower levels of blood triglycerides, free fatty acids, glucose and insulin and improved polyuria after four weeks of treatment in diabetic mice. Ragaglitazar reduced circulating insulin, improved insulin sensitivity and reduced Hb A1c to a greater extent than rosiglitazone alone. Muraglitazar improved glycemic control and dyslipidemia associated with type 2 diabetes and this may reduce the risk of cardiovascular complications. The dual PPAR / agonist LY-465608 completely restored euglycemia in diabetic rats during treatment in the early diabetic period (8-12 week of age) without increase in body weight.
A combination of rosiglitazone and fenofibrate (PPAR γ and α agonists respectively) achieves more beneficial effects than rosiglitazone (a PPAR γ agonist) alone in diabetic rats. Consequently, this combination may be more useful therapeuticlly in treatment of type 2 diabetic patients.
A combination of rosiglitazone and fenofibrate (PPAR γ and α agonists respectively) achieves more beneficial effects than rosiglitazone (a PPAR γ agonist) alone in diabetic rats. Consequently, this combination may be more useful therapeuticlly in treatment of type 2 diabetic patients.