Embed Size (px)
Citation preview

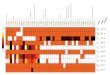
Hei
ght
W
eigh
t
Hea
ring
(R /
L)
Vi
sion
(R /
L)
D
enta
l / B
ite
R
espi
rato
ry
C
ardi
ac
BP
Her
nia
E
xtre
miti
es
G
enita
ls
S
kin
Chec
k th
ose
that
app
ly:
Life
Thr
eate
ning
Con
ditio
ns
Con
tact
Len
ses
Ear
Ach
es /
Infe
ctio
n
G
yn P
robl
ems
Poi
son
Ivy,
Oak
, Sum
ac
Rhe
umat
ic F
ever
S
tom
ach
Prob
lem
s
S
ore
Thro
at
Abs
ence
of a
pai
red
orga
n
W
hoop
ing
Cou
gh
Sin
us P
robl
ems
Cur
rent
orth
odon
tic
Mon
onuc
leos
is in
the
past
12
appl
ianc
e
mon
ths
Ski
n P
robl
ems
(Acn
e,
Rec
ent I
llnes
s / I
nfec
tions
E
czem
a)
HB
P
C
oncu
ssio
n / H
ead
Inju
ry
Bon
e / J
oint
Inju
ries
Oth
er C
hron
ic C
ondi
tion
Ope
ratio
ns
Oth
er
Ast
hma
Dia
bete
s
E
pile
psy
/ Sei
zure
s
H
eart
Con
ditio
ns /
Mur
mur
Fo
od A
llerg
ies
(spe
cify
)
M
edic
atio
n Al
lerg
ies
(spe
cify
)
O
ther
Alle
rgie
s ~
inse
ct s
tings
, ha
y fe
ver,
anim
al
Oth
er (P
leas
e de
tail)
C
amp
Cod
e:
(com
plet
ed b
y st
aff)
Imm
uniz
atio
n an
d Ph
ysic
al fo
rm fr
om s
choo
l / p
hysi
cian
may
be
subm
itted
in li
eu o
f co
mpl
etin
g th
e im
mun
izat
ion
and
phys
ical
exa
min
atio
n se
ctio
n be
low
.
Send
a c
opy –
and
also
brin
g th
e or
igin
al fo
rms
to c
amp!
PL
EASE
CO
MPL
ETE
ENTI
RE
FORM
St
uden
t Nam
e
Ag
e at
cam
p
Bi
rth
Date
:
/ /
Gen
der:
M
F Ad
dres
s:
City
St
ate:
Zi
p:
Phon
e Nu
mbe
r (Da
y): (
)
(E
ve):
( )
In
Cas
e of
Em
erge
ncy
and
pare
nt /
guar
dian
can
not b
e re
ache
d:
Cont
act:
Rel
atio
nshi
p:
Ph
one:
(
)
Pare
nt/G
uard
ian
Auth
oriz
atio
ns: T
his
heal
th h
isto
ry is
cor
rect
and
com
plet
e. T
he p
erso
n he
rein
des
crib
ed h
as p
erm
issi
on to
eng
age
in a
ll ca
mp
activ
ities
exc
ept a
s no
ted.
I he
reby
giv
e pe
rmis
sion
to th
e ca
mp
to p
rovi
de ro
utin
e he
alth
care
and
see
k em
erge
ncy
med
ical
tre
atm
ent i
nclu
ding
ord
erin
g x-
rays
or r
outin
e te
sts.
I ag
ree
to th
e re
leas
e of
any
reco
rds
nece
ssar
y fo
r tre
atm
ent,
refe
rral
, bill
ing,
or
insu
ranc
e pu
rpos
es. I
giv
e pe
rmis
sion
to th
e ca
mp
to a
rrang
e ne
cess
ary
rela
ted
trans
porta
tion
for m
e/m
y ch
ild. I
n th
e ev
ent I
can
not b
e re
ache
d in
an
emer
genc
y, I
here
by g
ive
perm
issi
on to
the
Dire
ctor
of S
occe
rPlu
s C
amps
or t
heir
desi
gnee
to s
ecur
e an
d ad
min
iste
r tre
atm
ent,
incl
udin
g ho
spita
lizat
ion,
for t
he p
erso
n na
med
abo
ve.
In
dem
nific
atio
n: T
he u
nder
sign
ed p
aren
t/gua
rdia
n of
the
regi
stra
nt, f
or a
nd in
furth
er c
onsi
dera
tion
of S
occe
rPlu
s C
amps
’ ac
cept
ing
sai
d re
gist
rant
, her
eby
agre
es to
sav
e an
d in
dem
nify
and
kee
p ha
rmle
ss th
e sa
id S
occe
rPlu
s C
amps
, its
age
nts,
and
spo
nsor
s ag
ains
t any
and
all
liabi
lity,
cla
ims,
judg
men
ts, o
r dem
ands
aris
ing
as a
resu
lt of
any
cou
rse
of in
stru
ctio
n or
act
ivity
giv
en th
e re
gist
rant
by
Soc
cerP
lus
Cam
ps.
Si
gnat
ure
of P
aren
t/Gua
rdia
n
Imm
uniz
atio
ns
Imm
uniz
atio
ns
Date
Bo
oste
rs
Dta
p/TD
/Tda
p
Po
lio (3
)
H
epat
itis
B (3
)
MM
R (2
)
TD
(val
id 1
0 y)
H
aem
ophi
lus
Influ
enza
Typ
e B
Imm
uniz
atio
ns o
r pro
of o
f illn
ess
Date
Va
ricel
a or
pro
of o
f Chi
cken
Pox
Ill
ness
(if a
pplic
able
) Da
te
Mea
sles
Ger
man
mea
sles
Mum
ps
H
epat
itis
A
H
epat
itis
C
Ph
ysic
al E
xam
inat
ion:
- Va
lid fo
r 365
Day
s O
nly
and
to B
e Co
mpl
eted
by
a L
icen
sed
Heal
th C
are
Prof
essi
onal
ONL
Y!
Pr
inte
d Na
me
M
edic
al In
sura
nce
Com
pany
(REQ
UIRE
D)
Ins.
Co.
Date
Polic
y #
G
roup
#
In
sure
d Em
ploy
er
We
reco
mm
end
that
a p
hoto
copy
(fro
nt a
nd b
ack)
of h
ealth
insu
ranc
e ca
rd b
e at
tach
ed to
this
form
. H
ealth
His
tory
:
* * *
Det
ails
of a
bove
to b
e co
mpl
eted
on
addi
tiona
l she
et *
* *
Indi
vidu
aliz
ed O
rder
For
m fo
r ALL
med
icat
ions
MU
ST
also
be
com
plet
ed.
REST
RICT
IONS
, LIM
ITAT
IONS
(INC
LUDI
NG
DIE
T):
RECO
MM
END
ATIO
NS:
The
abov
e na
med
per
son
is in
sat
isfa
ctor
y co
nditi
on a
nd m
ay e
ngag
e in
all
cam
p ac
tiviti
es e
xcep
t as
note
d:
Dat
e:
Ex
amin
ing
phys
icia
n:
Te
leph
one:
(
)
Pr
int p
hysi
cian
’s n
ame:
Stat
e lic
ense
d in
:
L
icen
se #
:
Ad
dres
s:
Plea
se s
ubm
it at
leas
t 30
days
prio
r to
cam
p an
d al
so b
ring
orig
inal
s to
cam
p:
Subm
it Fo
rm E
lect
roni
cally
to:
info
@so
ccer
plus
.org
/Fax
888
-891
.447
4 So
ccer
Plus
has
gon
e pa
perle
ss. W
e w
ill no
long
er a
ccep
t pap
er c
opie
s vi
a m
ail.

Authorization for the Self-Administration of Medications
CAMPER: DATE OF BIRTH: / / WEIGHT: lbs
This person takes NO medications on a routine basis.
The following form must be completed and signed by the child’s physician if your child: Needs to take any Over the Counter Medication “as needed” provided by the parent /guardian, while at camp. (Part I)
Over-The-Counter medication must be in the original container and labeled with the child’s name. Needs to take any routine Prescription Medications, provided by the parent /guardian, while at camp. (Part II). Prescription
medications must be in pharmacy-prepared containers and labeled with the name of the child, name of the drug, strength, dosage, frequency, physician’s or dentist’s name and date of the original prescription.
ALL MEDICATIONS AT CAMP ARE TO BE SELF-ADMINISTERED, BUT KEPT BY THE MEDICAL STAFF WHILE ON SITE.
Part I - Over-the-Counter Medications
Drug Name Route Dosage Indications Physician Order Comments Tylenol
(EXAMPLE) Liquid or Tabs
(EXAMPLE) Per Label (EXAMPLE)
Pain or Fever (EXAMPLE)
Yes No (EXAMPLE)
Part II - Prescription Medications Drug Name Controlled
Substance Route Dosage / Time of Administration
Indications Physician Order
Comments / Relevant Side Effects
Y / N
Y / N
Y / N
Y / N
Y / N
Y / N
If there are Relevant Side Effects listed above, please provide plan for management for each substance.
Date: Examining physician: Print physician’s name: Telephone: ( ) State licensed in: License #:
Authorization by Parent/Guardian for the administration of the above medication: To nurse, first aider, director, alternate director or youth camp counselor: I hereby request that the above medication, ordered by the physician/dentist for my child , be administered by the nurse, first aider, director, alternate director or youth camp counselor. I understand that I must supply the Youth Camp with the prescribed medication in the original container dispensed and properly labeled by a physician or pharmacist. Over-the-counter medication shall be in the original container labeled by the parent with the child’s name. I understand that this and all medication will be destroyed if it is not picked up on the last day of camp following termination of the order.
Name of Parent or Guardian Signature
(Print Name) Street Address City/Town State Phone ( )
Relationship to child: Date: / /

Tel– 800.KEEPER.1 Fax 888-891-4474 soccerplus.org
Individual Information
Last Name First Name
Birthdate Gender: Male / Female (circle one) Grade
Address (Street, City, State, zip)
Home Phone Mother Cell Phone Father Cell Phone
AMATEUR ATHLETIC WAIVER AND RELEASE OF LIABILITY
In consideration of being allowed to participate in any way and/or enter upon, use and/or engage in sports activities by SoccerPlus Companies: SoccerPlus Camps, Inc, including participation in practices, training, programs and/or other events and activities, the undersigned:
1. Agrees that prior to participating, he/she will inspect the facilities and equipment to be used, and if he/she believes an ything is unsafe, he/she will immediately advise a representative of SoccerPlus of such condition(s) and refuse to participate;
2. Acknowledge and fully understand that each participant will be engaging in activities that involve risk of serious injury, including permanent disability and death, and severe social and economic losses which might result not only from their own actions, inactions or negligence of others, the rules of play, or the condition of the premises or of any equipment used. Further, that there may be other risks not known to us or not reasonably foreseeable at this time;
3. Assume all the foregoing risks and accept personal responsibility for the damages following such injury, permanent disability or death;
4. Release, waive, discharge and covenant not to sue SoccerPlus, or their affiliated clubs, their respective members, administrators, directors, coaches and other employees of said organizations, participants, sponsoring agencies, sponsors, advertisers, and, if applicab le, owners and lessees of premises used to conduct the event, all of which are hereinafter referred to as “releasees”, from demand, losses or damages on account of injury, including death or damage to property, caused or alleged to be caused in whole or in part by the negligenc e of the releasees or otherwise;
5. Shall defend, indemnify, and hold SoccerPlus Companies: SoccerPlus Camps, Inc., its officers, employees, and agents harmless from and against any and all liability, loss, expense, including reasonable attorneys’ fees, or claims for injury or damages arising out of the performance of this Agreement but only in proportion to and to the extent such liability, loss, expense, attorneys’ fees, or claims for inj ury or damages are caused by omissions of the individual or group obtaining services from the SoccerPlus Companies, its officers, agents or employees;
6. Agrees to allow SoccerPlus to utilize the likeness and image of the participant in the form of photographs and/or video for the purposes of marketing and/or promotions.
THE UNDERSIGNED HAVE READ AND ACKNOWLEDGE THAT HE/SHE IS ENTERING INTO THE ABOVE WAIVER AND RELEASE, UNDERSTANDING THAT THEY HAVE GIVEN UP SUBSTANTIAL RIGHTS BY SIGNING IT AND SIGN IT VOLUNTARILY. WITHOUT LIMITING THE GENERALITY OF THE FOREGOING, IT IS MY INTENTION ON BEHALF OF MYSELF OR MY MINOR CHILD TO SPECIFICALLY RELEASE AND SOCCERPLUS CAMPS, INC. FROM ANY AND ALL CLAIMS ARISING FROM THEIR OWN NEGLIGENCE. I AGREE TO INDEMNIFY, DEFEND AND HOLD HARMLESS SOCCERPLUS CAMPS, INC. FROM ANY LIABILITIES, LOSSES, DAMAGES, SETTLEMENTS, CLAIMS, EXPENSES AND COSTS ARISING FROM MY OR MY CHILD’S PARTICIPATION IN THE DESCRIBED ACTIVITY, SAID INDEMNITY TO INCLUDE COURT COSTS AND REASONABLE ATTORNEY’S FEES.
Individual Signature (18 or over) _Date
Guardian Signature (if minor) Date

Tel– 800.KEEPER.1 Fax 888-891-4474 soccerplus.org
RULES & REGULATIONS: Please read, review and understand all content on these two pages. It is your responsibility to abide by all rules and regulations at all times.
Roommates: Roommates must each request each other by full name for the request to be considered (student A requests student B and vice- versa). Once at site, no one can change room assignments without permission of the director. Some sites only offer only multiple beds per room. We will do everything that we can to honor roommate requests. There are circumstances outside of control that may limit our ability to fulfill the request.
Travel Arrangements: SoccerPlus will pick up and drop off students only during select times from only the designated airport. To arrange for the shuttle service: please call ATP International Travel Service at 1-800-243-1806 or 203-772-0060 and ask for “The Soccer Desk.” This is the only way a student can reserve a spot with this shuttle service. They can make your flight arrangements, coordinate the arrival and departure times and schedule your shuttle with SoccerPlus for a $50 fee. If you book the flights by yourself you must provide the student's itinerary to ATP and not the SoccerPlus Office, so they can add the student to the camp itinerary. Reservations for shuttle must be made at least 15 days prior to the start of camp. Reservations made within 15 days of the camp may be subject to an additional charge. Driving directions to camp will be included in your pre-camp e-mail, sent approximately one week before the camp start date. Campers may not arrive earlier than the first day of camp at 3:00 PM and must leave on the closing day by noon.
Medical Policies: 1. Detailed Medical documentation policies and other policies (health care, discipline, and grievance) are available upon request [MA 430.215] by sending a self-addressed stamped envelope to the SoccerPlus Administrative Office. 2. All medications will be self-administered at camp, but kept by the staff certified athletic trainer (ATC) in a lockbox. 3. All medication use MUST accompany an Authorization for the Self- Administration of Medications form, available from our website or from our office. This must be completed and signed by physician PRIOR to the start of the program. 4. If you’ve had a recent physical and would like to attach a copy of your signed and dated physical form to our form, you may as long as you fill out the left-hand side of our health form as well. These forms are acceptable as long as the physician’s signature and date are less than one year old on the last day of camp.
OUR PURPOSE AND YOUR INTENTIONS ARE TO DEVELOP YOUR SOCCER SKILLS. THE FOLLOWING RULES HAVE BEEN ESTABLISHED TO HELP US BOTH REACH OUR GOALS. THEY WILL BE ENFORCED. 1. Specific campus rules must be adhered to. Remember we are guests of the particular school and must respect their property and regulations. 2. Students that drive to camp must turn in their keys to the director, and inform camp personnel of the location of the vehicle. Use of the car will be forbidden during the camp week. 3. Students are not allowed in campus areas held off limits to SoccerPlus Camps. IMMEDIATE DISMISSAL MAY RESULT! No one is allowed to leave campus grounds without the permission of the director of SoccerPlus. 4. POSSESSION OF ALCOHOLIC BEVERAGES, DRUGS INCLUDING TOBACCO, FIREARMS, OR ANY ITEM DANGEROUS TO OTHER STUDENTS WILL RESULT IN IMMEDIATE DISMISSAL AND POSSIBLE CRIMINAL PROSECUTION. 5. Tampering with fire safety equipment, electrical wiring or any campus property may result with dismissal. 6. Rooms must be kept clean and neat. Students are responsible for broken or damaged items. Before dismissal at end of camp rooms will be inspected. 7. Students must secure their valuables. SoccerPlus is not responsible for any lost valuables. 8. No student is allowed in another student’s room without an invitation. 9. Girls’ dormitory hallways and rooms are off limits to all males and vice- versa. Violators will be IMMEDIATELY DISMISSED. 10. The daily schedule of the program is to be adhered to, including all meeting times, meal times and wake-up and lights out. 11. Shinguards are mandatory at all training sessions. 12. An athletic trainer will be available at all camp locations. If special treatment is necessary, SoccerPlus must be informed in writing prior to the first training session. All injuries must be reported to the athletic trainer or camp director. 13. Any student dismissed from camp for disciplinary reasons will not be entitled to any refund. Refund Policy: The deposit of $250 is non-refundable. Any monies paid beyond the deposit amount are completely refundable until 30 days prior to the start of the program. At 30 days prior to start of programs, no refunds will be issued, only credit to future programs. Credits are transferable to immediate family members. All refund requests must be made in writing and can be emailed to [email protected]. We reserve the right to handle all refunds on an individual basis.
OUR ADVICE: Concentrate on soccer and the SoccerPlus Camp experience will be worthwhile, rewarding and enjoyable. If you have any questions please call our office at 1.800.533.7371 Monday through Friday 10am to 5pm eastern time or email us anytime at [email protected]

Tel– 800.KEEPER.1 Fax 888-891-4474 soccerplus.org
What to Bring:
Attending SoccerPlus Camps this summer will benefit anyone who is looking to improve their game. It is an experience unlike any other which will change your life on and off the field. However, to make the most of your camp experience, you need to be fully prepared. Here are some tips that will help.
1. BE PHYSICALLY PREPARED Come to camp in your best physical condition to get the most out of the time at camp. Every moment at camp is a valuable learning experience so be fit enough to participate. You want to be able to seize every opportunity to practice and learn. Our ability to pay attention decreases when we are tired. Our ability to train is reduced with a pulled muscle. The bottom line is that to take full advantage of everything that is offered at camp you must be in good physical shape. 2. THE RIGHT EQUIPMENT Bringing the right equipment is crucial to having a successful camp. Please make sure that you bring: A lanyard for your dorm keys and cafeteria pass (optional but recommended) Cleats that are already broken in. Don’t buy a new pair of shoes to wear at camp unless you have enough time to break them in. New shoes can give you blisters. Indoor/flat shoes for possible indoor sessions and casual evening wear. Sometimes because of bad weather sessions will be conducted indoors. A ball. One can be reserved for you by prepaying $25 at least 2 weeks prior to camp. Call 800-533-7371 or e-mail [email protected] to reserve a camp ball. Shinguards. Note: Please bring your own athletic tape if you need to hold your socks up. Our athletic trainer’s tape is for injuries only. A warm-up suit/sweats. You don’t want to get cold on your way to the evening lecture. Plenty of t-shirts, shorts, socks and underwear. SoccerPlus dress code forbids mid-drift tops or sleeveless shirts, for both boys and girls. Sheets (standard twin), blankets, pillow and towel(s). Bathroom items e.g. soap, shampoo, toothbrush, toothpaste, deodorant, etc. Sandals for the shower. Laundry detergent – Laundry is optional, but available. A bathing suit Some camps have access to a swimming pool. An alarm clock. All meals and meetings are mandatory. A fan. Not all rooms are air-conditioned. A notebook and pen for evening workshops. Bug spray and sun screen. A calling card or cell phone so you can call home. Spending money for evening snacks, laundry or the camp store. Sorry, there is no camp bank. The camp store does accept credit cards. A water bottle of your own which can be refilled from our coolers on the fields. This is a must. An address book. The friendships you make can last a lifetime. A disposable camera to get photos with your new friends. GOALKEEPERS: In addition to the above also bring: Extra goalkeeper jerseys. We recommend 4 or more. Long sleeve t-shirts also work well. At least one pair of goalkeeper gloves. Long goalkeeper pants for breakaway sessions. Skids or compression shorts work well but we suggest long pants for breakaway training.
There may be some other things you can think of but if you bring all of the above you will be in good shape. Don’t forget, there will be a camp store at each site with a great selection of equipment. 3. TAKE GOOD NOTES Evening workshops are designed to present students with information which time does not permit during the day. Most students are pretty tired by the end of the day but this is not the time to zone out or doze off. If you take good notes it will help you to pay attention and you will have a valuable asset to review when camp is over. It is also a good idea to jot down some of the exercises you did during the day. By the end of the week it will be hard to remember all that you have done. 4. TALK TO THE COACHES Most coaches were students at some time in the past. They can relate to a lot of issues which concern you. Never be shy about talking with coaches. They are there to help you. Many students develop lifelong relationships with their staff coaches. Exchange phone numbers, emails and addresses so you can stay in touch during the season. 5. STAY POSITIVE A week can be a long time when you are training with intensity. There will be some high and low points. It is important that you minimize your low points and get back on track quickly. Ultimately, you will learn more and have more successes with a positive state of mind. 6. BE A SPONGE Probably the most important thing you can bring to camp is an open mind. You are about to be inundated with all types of technical, tactical, psychological and physiological information. No matter how good you are or how many successes you have enjoyed remember why you decided to go to camp...to get better by learning from the best. Camp is a learning environment like school. You are presented with a whole lot of information and then it is up to you to decide what to do with it. Your goal should be to absorb as much information as possible and then fit what you can into your game. You may not agree with everything but you owe it to yourself to open your mind and try new things. Remember why you signed up for camp. 7. THE NEVER ENDING CAMP Camp does not end at the end of the week. The improvement will continue throughout the year if you continue to apply what you learned at camp. Remember the exercises you did (hope you took good notes), the intensity level at which you worked, the discipline you showed on and off the field and the words of wisdom you picked up from the staff. Every time you step on the practice field you should relive your week at camp. You have been given the tools to make yourself a better player. By the end of the week you will be a better player, but why should the improvement stop there. Enjoy your time at camp this summer. Strive to make the most of it as humanly possible and you will reap the rewards for the rest of your life . Please remember that registration begins at 3 pm. The first meal served at camp will be dinner. Try to eat lunch prior to registration so you will have the energy for our first field session. (If you are flying in, bring a bagged lunch, if you are driving in, pack a lunch or pick up something locally when you arrive).
“This Program is tough and intense. Those who attend our school become part of a very special family. The skills, friendships and self-respect you gain here will last a lifetime.” – Tony DiCicco
![0.9V Drive Nch + Nch MOSFET - Rohmrohmfs.rohm.com/.../discrete/transistor/mosfet/em6k34.pdf... [m ] T a = 125 C a = 75 T a = 25 C T a = 25 C T a = 125 C T = 75 C T = 25 C T = 25 C](https://img.pdfslide.tips/doc/110x75/5ac81aaf7f8b9acb688c30cb/09v-drive-nch-nch-mosfet-m-t-a-125-c-a-75-t-a-25-c-t-a-25-c.jpg)