-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
1/11
Reawakening Reective Capacity in the Psychotherapyof
Schizophrenia: A Case Study
Rebecca Bargenquast, Robert D. Schweitzer, and Suzanne Drake
Queensland University of Technology
Disturbed sense of self has long been identied as a common
experience among people suffering withschizophrenia. More recently,
metacognitive decits have been found to be a stable and
independentfeature of schizophrenia that contributes to disturbed
self-experience and impedes recovery. Individualpsychotherapy
designed to target poor metacognition has been shown to promote a
more coherentsense of self and enhanced recovery in people with
schizophrenia. We provide a report of a 2-yearindividual
psychotherapy with a patient suffering with chronic schizophrenia.
Progress was assessedover the course of treatment using the
Metacognition Assessment Scale and the Brief Psychiatric
RatingScale. The patient experienced improved metacognitive
capacity and reduced symptom severity overthe course of therapy.
Implications for clinical practice are discussed. C 2015 Wiley
Periodicals, Inc. J.
Clin. Psychol.: In Session 71:136–145, 2015.
Keywords: schizophrenia; psychotherapy; metacognition;
narrative; recovery
Loss of self is, arguably, at the core of the psychopathology in
people suffering from psychosis.People diagnosed with schizophrenia
are observed as suffering from a profound sense of beingcutoff from
themselves and the outside world, with the disorder having been
dened as an“I am illness–one that may overtake andredene the
identity of theperson” (Estroff,1989,p. 189).Although the symptoms
of schizophrenia are heterogeneous, disturbed sense of self has
longbeen identied as a common experience among sufferers, with some
arguing that schizophreniais fundamentally a self disorder
(Davidson, 2003; Jacobson, 2002; Lysaker & Lysaker, 2008;Roe
& Ben-Yishai, 1999; Sass & Parnas, 2003; Stanghellini,
2004). Recent advances in the eldhave linked disturbed
self-experience in people diagnosed with schizophrenia with
impairedmetacognitive capacity, that is, the ability to think
meaningfully about one’s own thoughts andfeelings and the thoughts
and feelings of others (Lysaker, Buck, Taylor, & Roe,
2008).
Metacognition is a multifaceted construct that comprises a range
of functions, from discreteacts of reection to more complex acts
involving the integration of multiple perceptions (Lysakeret al.,
2011). Metacognition involves operations such as recognizing and
differentiating ouremotions, making links between our mental states
and our behavior, recognizing that our beliefsabout ourselves and
others are subjective and others may see things differently,
identifying thereasons behind others mental states and behavior,
and using our understanding of our mentalstates to implement
strategies to manage distress. Metacognition is related to concepts
such astheory of mind, reective functioning, mind-mindedness,
empathy, and mentalization. Decitsin metacognitive functions are a
stable feature of schizophrenia and contribute to
sufferers’difculties with drawing plausibleconclusions about the
origins of internal states and the motivesof others (Frith, 1992;
Lysaker, Dimaggio, Buck, Carcione, & Nicolo, 2007).
Metacognitive decits have also been linked to difculties in
developing meaning from ex-periences, severity of delusions, poor
insight, trouble constructing coherent and meaningfulnarratives,
and diminished sense of self, all of which are barriers to recovery
(Harrington,Langdon, Siegert, & McClure, 2005; Lysaker,
Carcione, et al., 2005).
Recent research has suggested that we may conceive of
metacognitive capacity in terms of the following abilities: (a)
understanding one’s own mind, which is the capacity to
recognize,
Please address correspondence to: Robert Schweitzer, School of
Psychology and Counselling, QueenslandUniversity of Technology,
Kelvin Grove QLD, Australia. E-mail: [email protected]
JOURNAL OF CLINICAL PSYCHOLOGY: IN SESSION , Vol. 71(2), 136–145
(2015) C 2015 Wiley Periodicals, Inc.Published online in Wiley
Online Library (wileyonlinelibrary.com/journal/jclp). DOI:
10.1002/jclp.22149
-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
2/11
Reawakening Reective Capacity 137
Table 1Levels of Metacognitive Capacity Using the Metacognition
Assessment Scale
Understanding one’s own mind (nine levels)
1. Acknowledges having mental functions.2. Represents self as a
person with autonomous thoughts and feelings.3. Denes and
distinguishes own cognitive operations.4. Denes and distinguishes
own emotional states.5. Recognizes the subjectivity and fallibility
of representations of self and the world6. Recognizes the limited
impact thoughts and wishes have on reality.7. Recognizes that their
behavior may be determined by their thoughts and feelings.8.
Constructs complete description of their mental state
differentiating between thoughts
and feelings.9. Integrates different modes of cognitive and
emotional functioning into a coherent and
complex narrative.
Understanding others’ minds (seven levels)
1. Acknowledges others have mental functions.2. Represents
others as persons with autonomous thoughts and feelings.3. Denes
and distinguishes others’ cognitive operations.4. Denes and
distinguishes others’ emotional states.5. Makes plausible
inferences about others’ mental states.6. Constructs a complete
description of others’ mental states differentiating between
cognitive and emotional factors.7. Integrates others’ different
modes of cognitive, emotional, and relational functioning
into a coherent narrative.
distinguish, and integrate one’s own mental states; (b)
understanding others’ minds, which isthe capacity to understand
others’ mental states and form integrated representations of
otherpeople; (c) decentration, which is the capacity to recognize
that one is not at the center of others’ lives; and (d) mastery,
which is the capacity to use metacognitive knowledge to cope
withpsychological problems (Semerari et al., 2003).
Based on these constructs, the Metacognitive Assessment Scale
(MAS) was developed, andlater adapted in an abbreviated form
(MAS-A), to measure metacognitive capacity in peoplediagnosed with
schizophrenia spectrum disorders (Lysaker, Carcione, et al., 2005;
Semerari,
et al., 2003). The MAS-A measures metacognitive capacity along a
continuum from less tomore complex acts (see Table 1). These
constructs both inform and increase our insight andunderstanding of
the primary decits in schizophrenia and have, in part, guided the
developmentof Metacognitive Narrative Psychotherapy.
Metacognitive Narrative Psychotherapy
Drawing upon the conception of schizophrenia outlined above, the
proposed treatment model,Metacognitive Narrative Psychotherapy,
involves patients “developing a renewed sense of theirillness,
identity, agency, and worth within their life stories” (Lysaker
& Buck, 2006, p. 233). Theapproach, developed by Lysaker and
colleagues (Lysaker et al., 2011), draws upon a psychother-
apeutic approach developed for the treatment of personality
disorders (Dimaggio, Semerari,Carcione, Nicol ¯ o, & Procacci,
2007). Metacognitive Narrative Psychotherapy aims to addressthe
subjective aspects of the recovery process by offering a
therapeutic framework that helpspeople with schizophrenia recover
richer experiences of themselves by improving capacities
formetacognition and facilitating the development of more coherent,
richer narratives within aninterpersonal context.
-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
3/11
138 Journal of Clinical Psychology: In Session, February
2015
Metacognitive Narrative Psychotherapy has been described as an
approach that prioritizescollaboration, enables reection,
encourages the exploration of strengths and difculties, andassists
in the making of connections between the past, present, and future.
The approach offerspatients opportunities to practice acts of
metacognition (e.g., think about their own thinkingand feelings,
and the thinking and feelings of others) and, as such, strengthen
their ability to
perform more complex metacognitive functions within therapy
sessions and in their life outsideof treatment (Lysaker et al.,
2011; Lysaker, Glynn, Wilkniss, & Silverstein, 2010).
Interventionsmay involve reecting upon the metacognitive function
patients are engaging in, “You areremembering playing with your
sister as a child,” which targets level 3 of understanding one’sown
mind (see Table 1), or gently challenging them to engage in more
complex metacognitiveacts, “How does it feel to talk to me about
this?” which targets level 4 of understanding one’sown mind (see
Table 1).
The approach takes into account that capacities for
metacognition vary between people, withsome able to perform only
very basic acts and others able to perform more complex acts.
Forexample, a person may be able to dene and distinguish his or her
own cognitive operations,recognizing the difference between
thinking, remembering, and planning, but struggle to dene
and distinguish his or her own emotional states in a nuanced
way. To ensure appropriate inter-ventions, the therapist is
required to actively assess the patient’s metacognitive capacities
withineach session to ensure interventions are in line with the
patient’s abilities in the moment. Thiscan be done with reference
to the MAS-A.
Metacognitive Narrative Psychotherapy also targets narrative
coherence and richness in peo-ple with schizophrenia, recognizing
the interdependent relationship between metacognitive
ca-pacityandabilityfor coherent storytelling. “Withoutmetacognitive
capacity it shouldbe difcultto evolve a complex storied
understanding of one’s life, and without a sense that one’s life is
worthtelling a story about, there should be little need for complex
acts of metacognition” (Lysakeret al., 2010, p. 82). Storytelling,
and, in turn, capacity to reect upon mental states, is
furtherfacilitated by emphasizing the rst-person experience of the
patient, recognizing the patient as a
protagonist in the stories told, reecting on the therapist as
audience to the stories told, assistingthe patient to remember,
link and lter information, and identifying stories that remain
untold(Lysaker, Buck, & Hammoud, 2007; Lysaker, Buck, &
Roe, 2007; Lysaker & Lysaker, 2011).
A principle-based manual for the approach was developed by
Bargenquast and Schweitzer(2013b). The manual outlines ve phases of
treatment: (a) developing a therapeutic relation-ship, (b)
eliciting narratives, (c) enhancing metacognitive capacity, (d)
enriching narratives, and(e) living enriched narratives.
Progression through the phases of Metacognitive Narrative
Psy-chotherapy is related to patients’ developing richer life
stories, more fullling connections withothers, an enhanced sense of
coherence, improved volition and agency, a belief that they
arevalued by others, and a more complex, coherent sense of
self.
Evidence Base
A series of case studies of peoplewith schizophrenia spectrum
disordershasshown that Metacog-nitive Narrative Psychotherapy is
connected to improvements over time in metacognitive capac-ity,
narrative richness and coherence, and ability to portray oneself as
an active agent with socialconnections and value (Buck &
Lysaker, 2009; Lysaker, Buck, & Ringer, 2007; Lysaker, Davis,et
al., 2005; Lysaker, Davis, Jones, Strasburger, & Beattie, 2007;
Lysaker & Gumley, 2010). Inconjunction with metacognitive and
narrative improvements, case studies have also revealedimprovements
in social and emotional functioning, including increased
independence, improvedrelationships with family and friends,
increased insight, and a reduction in positive and negativesymptoms
(Lysaker, Buck, & Hammoud, 2007; Lysaker, Davis, et al., 2007;
Salvatore et al.,
2009).More recently, a pilot study of 11 people diagnosed with
schizophrenia investigated theeffectiveness of the manualized
version of Metacognitive Narrative Psychotherapy over thecourse of
11 to 26 months (Bargenquast & Schweitzer, 2013a). Results
showed that patientsdemonstrated signicant improvement in
subjective recovery and self-reectivity over the courseof
treatment. The ndings highlighted the potentially important role of
psychological treatment
-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
4/11
Reawakening Reective Capacity 139
in the recovery process for people diagnosed with psychotic
spectrum disorders. Althoughevidence supporting the approach
developed and described by Lysaker and colleagues is growingand a
multisite randomized controlled trial is underway (Van Donkersgoed
et al., 2014), thegeneralizability of the model across settings
continues to be unknown. An in-depth case studyapproach is often
the rst priority in developing a novel intervention, with a view to
gaining
a better understanding of the mechanisms of change involved in
the implementation of theapproach.
Case Illustration
Presenting Problem and Client Description
Clancy was an unemployed male in his 60s. He had never been
married and was living aloneon a disability pension. He had a
40-year history of psychosis, experiencing his rst psychoticepisode
and psychiatric hospitalization in mid-adolescence. His mental
health difculties wereassociated with at least 10 inpatient
admissions, poor vocational functioning, and profound
social disconnection. At the beginning of psychotherapy, he had
not had a psychiatric hospital-ization for about 20 years, although
he regularly presented to emergency services with akathisiaand
apparent anxiety.
He initially presented with negative symptoms and an array of
unusual persecutory andgrandiose ideas including extreme
suspiciousness regarding the motives of others, concernsregarding
the Catholic Church, and a belief he was being scouted for the
Olympic runningteam. Beliefs were not tenaciously held but
represented attempts to make sense of seeminglyconfusing and
conicting internal and external experiences. During the rst
session, Clancyexpressed signicant feelings of anxiety and fear and
evidenced a marked lack of personalagency. He reported a vast array
of somatic complaints that seemed to have little
physiologicalbasis. The stories he told lacked major details and a
sense of being placed in time, making
them difcult to follow. Clancy had limited awareness of his own
mental states, especially hisemotional experiences, and he
struggled to understand others’ behavior. His pretreatment ratingon
the Brief Psychiatric Rating Scale (BPRS; Lukoff, Liberman, &
Nuechterlein, 1986) placedhim in the “markedly ill” range (Leucht
et al., 2005).
Clancy was born into an Irish Catholic family and was one of ve
children. He was unsure of any family history of mental illness.
However, he alluded to his mother experiencing emotionaldifculties
during his childhood. His parents remained married throughout their
lives and hadpassed away 15 years prior to Clancy commencing
treatment. He continued to have intermittentcontact with three of
his sisters, who provided some nancial and social support. He
frequentedan art group for people with mental illness. Clancy often
experienced social interaction asconfusing and threatening, and he
reported a long history of never tting in. He had never been
married, had no children, and denied any history of romantic
relationships. In his youth, heachieved well academically until he
became unwell and had to drop out of high school. In
lateadolescence Clancy completed his Year 12 equivalency and worked
intermittently throughouthis 20s. At the beginning of therapy
Clancy had not worked for over 20 years.
Case Formulation
Clancy met diagnostic criteria for chronic schizophrenia,
characterized by negative symptomsand nonbizarre delusions. There
was no evidence of personality disorder. He suffered fromakathisia
due to long-term antipsychotic medication use. He was deaf in one
ear due to a geneticcondition for which he wore a hearing aid.
Initially, Clancy presented with little to say about his history
and the people in his life at thattime. He would merely repeat
sparse details of his daily activities with little expression of
histhoughts and feelings. It was near impossible to gain a sense of
who he was as a person. Hisstories were barren, representing an
inner world characterized by a sense of emptiness and, attimes,
nonexistence (Lysaker & Lysaker, 2002). We understood that the
development of a morestable sense of self was interrupted by the
onset of psychosis during his adolescence, in which
-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
5/11
140 Journal of Clinical Psychology: In Session, February
2015
Clancy’s awareness of his and others’ mental states appeared to
be greatly effected. Decades of social isolation, difculties
understanding his internal experiences, and an ever present sense
of threat had left Clancy with little sense of who he was apart
from being “schizophrenic.” Formany years the only story he had
been hearing was “You have schizophrenia and you need totake
medication,” leaving his inner world depleted.
Early assessments suggested Clancy experienced poor
metacognitive capacity, which meantthat he struggled to make sense
of his internal experiences and the motives of others leading toa
chronic sense of fear and persecution. Internal stimuli such as a
painful memory or a feelingof loneliness triggered immense
confusion and subsequent poor attempts to make sense of
hisexperiences. In the absence of meaningful self-reection, Clancy
used somatic complaints ordelusional beliefs to understand
affective experiences. In this sense, we believed Clancy’s
psy-chiatric symptoms, such as somatizing and delusional ideation,
served an important functionalpurpose by providing him with a
meaningful sense of who he was and warding off an
otherwiseoverwhelming sense of confusion and nothingness. We
conceived of his psychotic experiences asboth compensating for and
maintaining his impaired metacognitive capacity.
Course of Treatment
Clancy’s treatment was part of a larger pilot study of the
effectiveness of Metacognitive NarrativePsychotherapy. The outcomes
of this trial are published elsewhere (Bargenquast &
Schweitzer,2013a). His psychiatrist referred him to the research
project. During the duration of his psy-chotherapy, Clancy was
prescribed an antipsychotic medication and benzodiazepine to use
asneeded for sleep and anxiety. This was the rst time Clancy was
given the opportunity to engagein individual psychotherapy, having
been managed primarily on medication.
Psychotherapy sessions were weekly and lasted 45 minutes for the
course of 26 months. Clancyattended 97% of his scheduled sessions,
totaling 88 sessions. The end of treatment coincided withthe end of
the larger research project and, as such, was a forced termination.
The psychotherapist
(RB) was a novice psychologistcompleting her research
dissertationon psychotherapy for peoplediagnosed with
schizophrenia. Treatment was supervised by an experienced clinical
psychologistand psychotherapist (RS).
Clancy’s treatment was guided by the treatment manual
Metacognitive Narrative Psychother-apy: Guiding Principles and
Practice (Bargenquast & Schweitzer, 2013b). The manual
providedthe therapist with a set of general principles to guide the
psychotherapy sessions. While a manualwas used to guide practice,
sessions were not conducted prescriptively. Instead, the process of
change was considered unpredictable and unique to the patient.
Psychotherapy rarely followed alinear path. Improvements were often
followed by setbacks, which were then followed by
furtherprogress.
Early phase of treatment: Developing a therapeutic relationship
and eliciting narra-tives. The early sessions, drawing upon phases
1 and 2 of the manual, focused on the develop-ment of a shared
partnership between Clancy and his therapist. The therapist worked
hard topromote a sense of safety, with Clancy initially presenting
to sessions as confused and suspicious.Clancy had always found
social interaction perplexing, which meant his therapist needed to
bevery specic about the aims of the sessions, her role in relation
to Clancy’s treatment, and themotives that informed her
interventions during sessions. Questions would often include
caveatssuch as, “I’m asking about your experience of our session
today because it can be helpful for meto have feedback from you to
make sure we are working well together.”
The therapeutic process was made as explicit as possible.
External boundaries such as the timeand place of sessions were made
clear and remained consistent as much as possible throughout
the treatment. Clancy often expressed his surprise and
appreciation of sessions starting andending on time. It seemed that
attention to boundaries offered a sense of predictability that
wasvery comforting and potentially therapeutic.
The therapist adopted a reective, not-knowing stance. Space was
created, within the contextof the therapeutic relationship, to
think about Clancy’s internal experiences. For instance, “Let
ustake some time to think about what was going on for you when you
felt like everyone was talking
-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
6/11
Reawakening Reective Capacity 141
about you.” Interventions largely involved reecting upon small,
concrete fragments of Clancy’sself-experience. He often spoke about
his daily activities to which the therapist responded
withstatements emphasizing his rst person experience, “ You went
grocery shopping today,”
Although Clancy showed some awareness of his cognitive
operations during this early phaseof treatment, his reections were
sparse and inexible. He displayed little capacity to elaborate
upon his thinking processes. For instance, when describing
incidents that were confusing orthreatening to him, he often
stated, “I thought it was strange.” However, he was not able
toexpand upon his experience of strangeness , struggling with
therapist questions such as “Whenyou say strange what do you mean?”
or “What about it felt strange ?” So the therapist optedinstead for
gentler reections consistent with Clancy’s reective capacity at the
time, for instance,“Things didn’t feel quite right to you.”
During this phase of treatment, Clancy displayed signicant
difculties understanding andexpressing emotional experiences.
Painful emotions tended to trigger somatic concerns or perse-cutory
ideation, which often derailed the therapy dialogue. In a bid to
reduce Clancy’s sense of threat and maintain dialogue, the
therapist avoided emotion-laden questions and reections inthe
initial stages of treatment. Avoiding affect-laden probes appeared
to assist Clancy to reveal
parts of himself at a pace that was nonthreatening.
Seven months into treatment: Enhancing metacognitive capacity
and enrichingnarratives. Despite notable metacognitive decits,
glimpses of Clancy’s desire to better un-derstand his difculties
were evident during this phase of the intervention (phases 3 and 4
of the manual). Around 7 months into the treatment (session 23),
Clancy began to reveal somemore complex affective experiences, and
a clearer narrative around his experience of his illnessstarted to
form. Specically, Clancy spoke of feeling like a “guinea pig” and
“experimentedupon” when receiving hospital treatment for his
psychosis. He acknowledged for the rst timethat the therapy
sessions and relationship with the therapist were important to
him.
The rst year of psychotherapy (43 sessions) was very much a
process of trial and error, in
which the therapist was carefully testing the effectiveness of
her interventions and adjusting herapproach in response to Clancy’s
demonstrated reective capacity. The challenging nature of this
stage of treatment cannot be overstated, and it may account for
some clinicians’ reluctanceto engage in longer term therapy with
people with psychosis.
The therapist reported feelings of hopelessness, frustration,
and intense boredom that, in turn,led to some self-recrimination.
That is, the experience of working with Clancy was quite
differentthan the experience of working with people with a range of
more common adjustment problems.She would also frequently nd
herself with literally nothing to say in response to Clancy’s
stories.Her internal dialogue would cease and her mind would be
blank. This experience was potentiallyproblematic as a therapist
with nothing to say is rarely effective. However, the experience
wasalso informative.
Through supervision the therapist was able to reect on what it
must be like to have a de-pleted inner world. With this
understanding, the therapist was able to use her own experiencesin
session to guide treatment, share aspects of her experience with
Clancy, and further pro-mote the therapy relationship and dialogue:
“Sometimes when we are talking I nd it hardto think of anything to
say. I wonder if you ever feel like this.” Clancy responded with,
“Yes!Before I come to session I think about the things I want to
talk about. But when I get inthe room it’s like it all goes away;
I’m blank.” Interventions such as this provided a sense of being in
it together, sharing the experience of “blankness.” This seemed to
provide Clancywith a strong sense of being understood and also
allowed him to further explore his innerexperiences.
As treatment progressed, Clancy’s capacity to reect upon his
mental states grew. Over time,
the therapist gained a better understanding of which
interventions facilitated reection andwhich triggered an increase
in psychotic material. Interventions that involved simple
reectionsof Clancy’s mental states and the therapy process in the
moment tended to be the most helpful;for example: “It’s hard for
you to think of anything to say to me today”; “You’re thinking
aboutX a lot at the moment. It is hard to think about anything
else”; and “You were worried that Iwouldn’t be at our appointment
today.” Open and vague questions, such as “How was that for
-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
7/11
142 Journal of Clinical Psychology: In Session, February
2015
you?” or “How did you feel about that?” rarely facilitated the
therapy dialogue and often leftClancy confused, resulting in
disorganized, tangential responses.
At 15 months into therapy, a pivotal point was reached. Clancy
revealed that his sibling wasdying of cancer. Contemplating the
loss of his sibling seemed to open the door to exploring
otherlosses and the associated painful affect. Over a series of
sessions, loss and loneliness emerged as
signicant themes.During session 67, Clancy revealed a greater
awareness of his illness experience and the effect
it has had on his life. He began demonstrating an increased
capacity to reect upon his mentalstates and the therapeutic
relationship. A more elaborate picture of who Clancy was in
relationto his illness and others was developing.
Clancy: What do you want me to talk about?Therapist: It’s hard
to think of something to talk about?
C: Yeah, I think that I’m having trouble. I’m thinking of the
past all the time, yeah,politics and things like wars and
things.
T: So things from the past have been on your mind a lot
recently.C: I don’t know why, you know, I think it links to . . .
oh, seeing as I’m 67 it’s pretty hard
to . . . ‘cause I’m single, never married. I don’t know other
people in this position.Someone at my age would’ve been married
long ago, you know. Since I’ve, I’m, youknow, I was sick all the
time . . . . Sometimes I get ideas in my mind . . . . Oh, rememberI
was talking to you about the Mormons a couple of weeks ago? Perhaps
that was abit too much, you know, to relate to.
T: You’re worried about sharing certain ideas with me.C: Yes.T:
That it’ll be too much.C: Well, they are schizophrenia, I suppose.
Aren’t they related to it? You gotta talk about
it. But I feel a bit strange telling you, you know.T: So when
you say you feel strange telling me, what’s that feeling like?C:
Once I start I’ve gotta keep going . . . . It seems like I imagine
a lot of it . . . . My
schizophrenia and my position . . . it’s dawning on me now, you
know. So that’s itfor everything, you know, just go to mass and
wait to die.
T: When you say it’s dawning on you, what’s dawning on you?C:
The effect, the isolation. That’s about all, you know . . . I had
jobs, weren’t very nice,
they were low paid jobs, you know.T: So the impact that
schizophrenia has had on your life is dawning on you.C: Yes, yes.T:
You said something interesting . . . you will just give up on
everything and just go to
mass and wait to die.C: [laughs] I said yeah but I don’t know. I
do painting. I exercise. Try to get as much
mental treatment as I can.
With the end in mind: Living enriched narratives. During the nal
phase of treatment(phase 5 of the manual), Clancy was encouraged to
take what he had learned within the therapyrelationship and apply
it to his everyday life. For instance, Clancy was encouraged to
exploreopportunities to connect with others in the community to
address his loneliness. As therapy wascoming to an end, Clancy
revealed that he would often recall the therapist’s voice
reassuring
and guiding him when he was feeling unsafe. It seemed that over
the course of treatment Clancyhad internalized the therapy
dialogue. It was clear that therapy had become an important partof
Clancy’s life. With this in mind, the end of therapy was carefully
planned and spoken aboutthroughout this phase of the treatment. The
nal session was surprising because Clancy seemedto have gained
condence and expressed overt anger towards the therapist about the
therapyending. At his request he was referred to a private
psychologist so he could continue therapy.
-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
8/11
Reawakening Reective Capacity 143
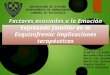
Figure 1. Changes in reective capacity and symptom severity over
the course of psychotherapy.
Outcome and Prognosis
Treatment progress was assessed using the MAS, BPRS, and
qualitative data. MAS and BPRSratings were completed for interviews
at pretreatment, 6 months, 12 months, and end of treat-ment
(Indiana Psychiatric Illness Interview; Lysaker, Clements,
Plascak-Hallberg, Knipscheer,& Wright, 2002). MAS ratings were
also completed for sessions 9, 23, 38, 45, 52, and 67. A grad-ual,
nonlinear improvement in Clancy’s metacognitive capacity over the
course of treatment wasevident (see Figure 1). A gradual reduction
in symptom severity overtime was also found, withClancy moving from
the “markedly ill” range to the ‘moderately ill’ range on the BPRS
(seeFigure 1).
Qualitatively, Clancy developed a more complex understanding of
himself and his experi-
ences over the course of therapy. Although he continued to
experience some symptoms andsocial isolation, he developed a
greater capacity to manage these experiences and was moreactively
pursuing a “social life.” He presented to emergency services far
less frequently for anx-iety and somatic concerns. We took the view
that Clancy would have beneted from ongoingpsychotherapy based upon
metacognitive narrative principles and the opportunity to
continueto develop his sense of self within a therapeutic
relationship.
Clinical Practices and Summary
The dominant models guiding the work with patients presenting
with schizophrenia draw uponbiological approaches citing evidence
of a genetic predisposition and biological correlates. Nev-
ertheless, antipsychotic medication is rarely sufcient to enable
patients with schizophrenia tofunction effectively and achieve
meaningful degrees of recovery. Psychological approaches arecrucial
in fostering recovery within this population. The current case
study provides practice-based evidence supporting a metacognitive
narrative approach to working with individuals whopresent with
symptoms of schizophrenia.
We outlined a framework for conceptualizing schizophrenia as
essentially a self-disorderand provided a basis for interventions
aimed at bolstering human capacities for reection,narration, and
meaning making. The implications to be drawn from the study are as
follows:(a) people diagnosed with schizophrenia are willing to
engage in a longer term psychotherapyand nd it benecial; (b)
treatments tailored to the whole person, taking into account
theirstrengths and decits, facilitate patient engagement; and (c)
psychological interventions targeting
metacognitive capacity promote recovery in people with
schizophrenia.By providing a therapeutic environment that is
supportive and engages with the subjectiveexperience of the person,
people with schizophrenia, in our experience, are enthusiastic
aboutengaging in psychotherapy. Our experience has taught us that
given the opportunity and a senseof openness on the part of the
therapist, patients are cautious but equally motivated to
engagewith others. A structured approach that is cognizant of the
unique needs of the patient provides
-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
9/11
144 Journal of Clinical Psychology: In Session, February
2015
a foundation for working psychotherapeutically with people with
schizophrenia. Within thisframe, we are able to learn about the
potential of the person to develop more integrated andcomplex ideas
about themselves and others over the course of a systematic therapy
process.The case of Clancy illustrates the potential of those most
disabled by psychosis to develop agreater awareness of themselves
and achieve meaningful degrees of recovery. It also points to
the
importance of a more open attitude to the role of psychological
interventions in the treatmentof people with chronic
schizophrenia.
A number of factors helped promote Clancy’s metacognitive
capacity and recovery over thecourse of therapy. First, the therapy
relationship was considered paramount. The therapist wasnot afraid
to focus on the intersubjective nature of the therapy and “deal
with” the relationship:“What is it like talking to me about these
ideas?” and “ You feel more comfortable with methan you used to.”
The relational aspects of the treatment were made explicit in a bid
todemystify social interactions and explore Clancy’s sense of
confusion in relation to others.Second, Clancy’s subjective
experiences were respected and given priority, with
interventionsdesigned to illuminate his inner world: “ You
think/wish/feel . . . ” and “What was that like for you?” The
therapist also used her own subjective experiences in sessions to
inform treatment.
Finally, the MAS-A was used regularly to assess changes in
Clancy’s metacognitive capacitywithin sessions and over the course
of treatment. Regular MAS-A ratings helped guide treatmentand
ensured interventions targeted specic areas of decit.
Although the early evidence for Metacognitive Narrative
Psychotherapy is promising, thereis a need to develop and implement
large-scale trials, which are designed in response to theneeds of
people suffering with psychotic disorders. There is also a need for
increased trainingand support for clinicians who are motivated to
provide longer term therapy for this patientgroup. We are hopeful
that, over time, we will gain increasing evidence for the
effectiveness of the intervention pioneered by Lysaker and
colleagues and be better able to assist people withschizophrenia
achieve meaningful degrees of recovery and live more enriched
lives.
Selected References and Recommended Readings
Bargenquast, R., & Schweitzer, R. D. (2013a). Enhancing
sense of recovery and self-reectivity in peoplewith schizophrenia:
A pilot study of Metacognitive Narrative Psychotherapy.
doi:10.1111/papt.12019
Bargenquast, R., & Schweitzer, R. D. (2013b). Metacognitive
Narrative Psychotherapy for people di-agnosed with schizophrenia:
An outline of a principle-based treatment manual. Psychosis,
1–11.doi:10.1080/17522439.2012.753935
Buck,K. D., & Lysaker, P. H. (2009). Addressing
metacognitive capacityin thepsychotherapy forschizophre-nia: A case
study. Clinical Case Studies, 8(6), 463–472.
doi:10.1177/1534650109352005
Davidson, L. (2003). Living outside mental illness: Qualitative
studies of recovery in schizophrenia. NewYork: New York University
Press.
Dimaggio, G., Semerari, A., Carcione, A., Nicol ¯ o, G., &
Procacci, M. (2007). Psychotherapy of personalitydisorders:
Metacognition, states of mind and interpersonal cycles. New York:
Routledge.
Estroff, S. E. (1989). Self, identity, and subjective
experiences of schizophrenia: In search of the
subject.Schizophrenia Bulletin, 15(2), 189–196.
doi:10.1093/schbul/15.2.189.
Geller, J. D., & Farber, B. A. (1993). Factors inuencing the
process of internalization in psychotherapy.Psychotherapy Research,
3, 166–180.
Lysaker, P. & Lysaker, J. (2002). A typology of narrative
impoverishment in schizophrenia: Implicationsfor understanding the
processes of establishing and sustaining dialogue in individual
psychotherapy.Counselling Psychology Quarterly, 19(1), 57–68. doi:
10.1080/09515070600673703.
Lysaker, P. & Lysaker, J. (2002). Narrative Structure in
Psychosis. Theory and Psychology, 12(2), 207–220.doi:
10.1177/0959354302012002630.
Lysaker, P. & Lysaker, J. (2008). Schizophrenia and the fate
of the self. Oxford: Oxford University Press.Lysaker, P., Buck, K.,
Taylor, A. & Roe, D. (2007). Associations of metacognition and
internalized stigma
with quantitative assessments of self-experience in narratives
of schizophrenia. Psychiatry Research, 157,31–38. doi:
10.1016/j.psychres.2007.04.023.
-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
10/11
Reawakening Reective Capacity 145
Lysaker, P., Dimaggio, G., Buck, K., Carcione, A. & Nicolo,
G. (2007). Metacognition within narrativesof schizophrenia:
Associations with multiple domains of neurocognition. Schizophrenia
Research, 93,278–287. doi: 10.1016/j.schres.2007.02.016.
Lysaker, P., Carcione, A., Dimaggio, G., Johannesen, J., Nicolo,
G., Procacci, M. & Semerari, A. (2005).Metacognition amidst
narratives of self and illness in schizophrenia: Associations with
insight, neu-
rocognition, symptom and function. Acta Psychiatrica
Scandinavica, 112, 64–71. doi:
10.1111/j.1600-0447.2005.00514.x.Lysaker, P., Glynn, S., Wilkniss,
S.& Silverstein, S.(2010). Psychotherapy and
RecoveryFromSchizophrenia:
A Review of Potential Applications and Need for Future Study.
Psychological Services, 7(2), 75–91. doi:10.1037/a0019115.
Lysaker, P., Buck, K. & Roe, D. (2007). Psychotherapy and
Recovery in Schizophrenia: A Proposal of Key Elements for an
Integrative Psychotherapy Attuned to Narrative in Schizophrenia.
PsychologicalServices, 4(1), 28–37. doi:
10.1037/1541–1559.4.1.28.
Lysaker, P. & Lysaker, J. (2011). Psychotherapy and Recovery
from Schizophrenia: A Model of Treatmentas Informed by a Dialogical
Model of the Self Experience in Psychosis. Journal of
ContemporaryPsychotherapy, 41, 125–133. doi:
10.1007/s10879-010-9157-x.
Lysaker, P., Davis, L., Eckert, G., Strasburger, A., Hunter, N.
& Buck, K. (2005). Changes in NarrativeStructure and Content in
Schizophrenia in Long Term Individual Psychotherapy: A Single Case
Study.Clinical Psychology and Psychotherapy, 12, 406–416. doi:
10.1002/cpp.457.
Lysaker, P., Clements, C., Plascak-Hallbert, C., Knipscheer, S.
& Wright, D. (2002). Insight and PersonalNarratives of Illness
in Schizophrenia. Psychiatry, 65(3), 197–206. doi:
10.1521/psyc.65.3.197.20174.
Lysaker, P. H., Buck, K. D., Carcione, A., Procacci, M.,
Salvatore, G., Nicol ò, G., & Dimaggio, G. (2011).Addressing
metacognitive capacity for self reection in the psychotherapy for
schizophrenia: A con-ceptual model of the key tasks and processes.
Psychology and Psychotherapy: Theory, Research andPractice, 84(1),
58–69. doi:10.1348/147608310x520436
Lysaker, P. H., Buck, K. D., & Hammoud, K. (2007).
Psychotherapy and schizophrenia: An anal-ysis of requirements of
individual psychotherapy with persons who experience manifestly
barrenor empty selves. Psychology and Psychotherapy: Theory,
Research and Practice, 80(3), 377–387.
doi:10.1348/147608306x159361Lysaker, P. H., Buck, K. D., &
Ringer, J. (2007). The recovery of metacognitive capacity in
schizophrenia
across 32 months of individual psychotherapy: A case study.
Psychotherapy Research, 17(6),
713–720.doi:10.1080/10503300701255932
Salvatore, G., Procacci, M., Popolo, R., Nicolo, G., Carcione,
A., Semerari, A., & Dimaggio, G. (2009).Adapted metacognitive
interpersonal therapy for improving adherence to intersubjective
contexts in aperson with schizophrenia. Clinical Case Studies,
8(6), 473–488. doi:10.1177/1534650109354916
Sass, L. A., & Parnas, J. (2003). Schizophrenia,
consciousness, and the self. Schizophr Bull, 29(3),
427–444.Semerari, A., Carcione, A., Dimaggio, G., Falcone, M.,
Nicol ò, G., Procacci, M., & Alleva, G. (2003). How
to evaluate metacognitive functioning in psychotherapy? The
metacognition assessment scale and itsapplications. Clinical
Psychology & Psychotherapy, 10(4), 238–261.
-
8/18/2019 Capacidad Reflexiva en Esquizofrenia
11/11
C o p y r i g h t o f J o u r n a l o f C l i n i c a l P s y c
h o l o g y i s t h e p r o p e r ti t s c o n t e n t m a y n o t
b e c o p i e d o r e m a i l e d t o m u l t i p l e s i t e s oc
o p y r i g h t h o l d e r ' s e x p r e s s w r i t t e n p e r m
i s s i o n . H o w e v e r , a r t i c l e s f o r i n d i v i d u
a l u s e .