Embed Size (px)
DESCRIPTION
Caspofungin. Breakthrough Treatment in the Management of Patients with Invasive Candidiasis. Overview: Growing Threat. Serious fungal infections are on the rise Invasive Candida infections 4th most common nosocomial bloodstream infection in the United States*. - PowerPoint PPT Presentation
Citation preview

Download from www.cancidas.ae
CaspofunginCaspofunginBreakthrough Treatment in the
Management of Patients with Invasive CandidiasisBreakthrough Treatment in the
Management of Patients with Invasive Candidiasis

Download from www.cancidas.ae
Overview: Growing ThreatOverview: Growing Threat
• Serious fungal infections are on the rise
• Invasive Candida infections– 4th most common nosocomial bloodstream infection in the
United States*
• Serious fungal infections are on the rise
• Invasive Candida infections– 4th most common nosocomial bloodstream infection in the
United States*
* In a 3-year (1995-1998) surveillance study of 49 hospitals in the United States.
Adapted from Edmond MB et al Clin Infect Dis 1999;29:239-244.
Andriole VT J Antimicrob Chemother 1999;44:151-162; Uzun O, Anaissie EJ Ann Oncol 2000;11:1517-1521; Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP Clin Infect Dis 1999;29:239-244.
* In a 3-year (1995-1998) surveillance study of 49 hospitals in the United States.
Adapted from Edmond MB et al Clin Infect Dis 1999;29:239-244.
Andriole VT J Antimicrob Chemother 1999;44:151-162; Uzun O, Anaissie EJ Ann Oncol 2000;11:1517-1521; Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP Clin Infect Dis 1999;29:239-244.
Coagulase-negative staphylococci 3908 31.9Staphylococcus aureus 1928 15.7Enterococci 1354 11.1Candida species 934 7.6
Coagulase-negative staphylococci 3908 31.9Staphylococcus aureus 1928 15.7Enterococci 1354 11.1Candida species 934 7.6
Pathogen No. of Isolates Incidence (%)Pathogen No. of Isolates Incidence (%)

Download from www.cancidas.ae
In an international surveillance study of bloodstream infections:
Species of Candida Most Commonly IsolatedIn an international surveillance study of bloodstream infections:
Species of Candida Most Commonly Isolated
Pfaller MA, Jones RN, Doern GV et al and The SENTRY Participant Group Antimicrob Agents Chemother 2000;44:747-751.Pfaller MA, Jones RN, Doern GV et al and The SENTRY Participant Group Antimicrob Agents Chemother 2000;44:747-751.
C. glabrata 16%
C. glabrata 16%
C. albicans 54%
C. albicans 54%C. parapsilosis
15%C. parapsilosis
15%
C. tropicalis 8%
C. tropicalis 8%
C. krusei 2%
C. krusei 2% other Candida
spp 5%other Candida
spp 5%
Adapted from Pfaller MA et al and The SENTRY Participant Group Antimicrob Agents Chemother 2000;44:747-751.Adapted from Pfaller MA et al and The SENTRY Participant Group Antimicrob Agents Chemother 2000;44:747-751.

Download from www.cancidas.ae
High Rate of Mortality Associated with Candidal Bloodstream InfectionsHigh Rate of Mortality Associated with Candidal Bloodstream Infections
Patients with candidal bloodstream infectionsPatients with candidal bloodstream infections
Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP Clin Infect Dis 1999;29:239-244.Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP Clin Infect Dis 1999;29:239-244.
00
55
1010
1515
2020
2525
3030
3535
4040
454540%40%
25%25%
Per
cent
age
of P
atie
nts
Per
cent
age
of P
atie
nts
Patients with bacterial (non-candidal)
bloodstream infections
Patients with bacterial (non-candidal)
bloodstream infections
In a 3-year surveillance study of nosocomial bloodstream infections in 49 US hospitals:In a 3-year surveillance study of nosocomial bloodstream infections in 49 US hospitals:

Download from www.cancidas.ae
Blumberg HM, Jarvis WR, Soucie JM et al and the NEMIS Study Group Clin Infect Dis 2001;33:177-186; Garber G Drugs 2001;61(suppl 1):1-12. National Epidemiology of Mycosis Survey (NEMIS) was a prospective, multicenter study conducted at 6 US sites from 1993-1995 to examine rates of risk factors for the development of candidal bloodstream infections (CBSIs) among patients in surgical and neonatal ICUs >48h. Among 4276 patients, 42 CBSIs occurred.
Blumberg HM, Jarvis WR, Soucie JM et al and the NEMIS Study Group Clin Infect Dis 2001;33:177-186; Garber G Drugs 2001;61(suppl 1):1-12. National Epidemiology of Mycosis Survey (NEMIS) was a prospective, multicenter study conducted at 6 US sites from 1993-1995 to examine rates of risk factors for the development of candidal bloodstream infections (CBSIs) among patients in surgical and neonatal ICUs >48h. Among 4276 patients, 42 CBSIs occurred.
Patients at High RiskPatients at High Risk
Potential risk factors include:
Non-Neutropenic
• Acute renal failure
• Parenteral nutrition
• Anti-anaerobic agents
• Prior vancomycin use
• Intralipid agents
• Prior surgery
• Indwelling triple-lumen catheters
Potential risk factors include:
Non-Neutropenic
• Acute renal failure
• Parenteral nutrition
• Anti-anaerobic agents
• Prior vancomycin use
• Intralipid agents
• Prior surgery
• Indwelling triple-lumen catheters
Neutropenic
• Cancer
• Transplantation
• Broad spectrum anti-anaerobic antibiotic use
• Prior vancomycin use
• Immunocompromised state
• Surgery
• Indwelling catheters
Neutropenic
• Cancer
• Transplantation
• Broad spectrum anti-anaerobic antibiotic use
• Prior vancomycin use
• Immunocompromised state
• Surgery
• Indwelling catheters

Download from www.cancidas.ae
Candidemia in Neutropenic Patients with Cancer: Clinical Characteristics* Candidemia in Neutropenic Patients with Cancer: Clinical Characteristics*
Broad-spectrum antibiotics in previous 2 weeks
Corticosteroids within previous 2 weeks
Chemotherapywithin previous 30 days
Abdominal surgerywithin previous 2 months
Intravenous hyperalimentationwithin previous 30 days
Concomitant infection within previous week
Central venous catheter (CVC) in place at time of positive
blood culture
Broad-spectrum antibiotics in previous 2 weeks
Corticosteroids within previous 2 weeks
Chemotherapywithin previous 30 days
Abdominal surgerywithin previous 2 months
Intravenous hyperalimentationwithin previous 30 days
Concomitant infection within previous week
Central venous catheter (CVC) in place at time of positive
blood culture
% with clinical characteristic% with clinical characteristic* Univariate analyses.
Adapted from Anaissie EJ et al Am J Med 1998;104:238-245.
Anaissie EJ, Rex JH, Uzun O, Vartivarian S Am J Med 1998;104:238-245.
* Univariate analyses.
Adapted from Anaissie EJ et al Am J Med 1998;104:238-245.
Anaissie EJ, Rex JH, Uzun O, Vartivarian S Am J Med 1998;104:238-245.
Neutropenic (n=217)Neutropenic (n=217)
00 1001005050
56%56%
3%3%
39%39%
63%63%
98%98%
90%90%
89%89%

Download from www.cancidas.ae
Candidemia in Non-Neutropenic Patients with Cancer: Clinical Characteristics*Candidemia in Non-Neutropenic Patients with Cancer: Clinical Characteristics*
* Univariate analyses.
Adapted from Anaissie EJ et al Am J Med 1998;104:238-245.
Anaissie EJ, Rex JH, Uzun O, Vartivarian S Am J Med 1998;104:238-245.
* Univariate analyses.
Adapted from Anaissie EJ et al Am J Med 1998;104:238-245.
Anaissie EJ, Rex JH, Uzun O, Vartivarian S Am J Med 1998;104:238-245.
Broad-spectrum antibiotics in previous 2 weeks
Corticosteroids within previous 2 weeks
Chemotherapywithin previous 30 days
Abdominal surgerywithin previous 2 months
Intravenous hyperalimentationwithin previous 30 days
Concomitant infection within previous week
Central venous catheter (CVC) in place at time of positive
blood culture
Broad-spectrum antibiotics in previous 2 weeks
Corticosteroids within previous 2 weeks
Chemotherapywithin previous 30 days
Abdominal surgerywithin previous 2 months
Intravenous hyperalimentationwithin previous 30 days
Concomitant infection within previous week
Central venous catheter (CVC) in place at time of positive
blood culture
% with clinical characteristic% with clinical characteristic
Non-Neutropenic (n=257)Non-Neutropenic (n=257)
00 1001005050
23%23%
29%29%
52%52%
61%61%
49%49%
80%80%
88%88%

Download from www.cancidas.ae
Kartsonis NA. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy. Kartsonis NA. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy.
Caspofungin: New Class of Drug Caspofungin: New Class of Drug
Nucleoside AnalogsNucleoside Analogs
-(1,3)-D-glucan-(1,3)-D-glucan
ErgosterolPolyenes
Azoles
ErgosterolPolyenes
Azoles
Phospholipid bilayerof the fungal cell
membrane
Phospholipid bilayerof the fungal cell
membrane
Fungal cell wallFungal cell wall
-(1,6)-glucan-(1,6)-glucan
-(1,3)-D-glucan synthaseGlucan Synthesis
Inhibitor
-(1,3)-D-glucan synthaseGlucan Synthesis
Inhibitor
nucleus
Breakthrough Mechanism of Action: Targets the Pathogen, Not the Patient Breakthrough Mechanism of Action: Targets the Pathogen, Not the Patient

Download from www.cancidas.ae
Caspofungin: Broad Spectrum of Activity Caspofungin: Broad Spectrum of Activity
Data on file, MSD; Bartizal K, Gill CJ, Abruzzo GK et al Antimicrob Agents Chemother 1997;41:2326-2332.Data on file, MSD; Bartizal K, Gill CJ, Abruzzo GK et al Antimicrob Agents Chemother 1997;41:2326-2332.
C. alb
ican
s
C. alb
ican
s
C. gla
brat
a
C. gla
brat
a
CANDIDA ALBICANSCANDIDA ALBICANS
C. par
apsil
osis
C. par
apsil
osis
C. tro
pica
lis
C. tro
pica
lisC. k
ruse
i
C. kru
sei
C. gui
llier
mon
dii
C. gui
llier
mon
dii
C. lip
olyt
ica
C. lip
olyt
ica
C. dub
linie
nsis
C. dub
linie
nsis
C. kef
yr
C. kef
yrC. l
usita
niae
C. lus
itani
aeC. r
ugos
a
C. rug
osa
A. fl
avus
A. fl
avus
A. fu
mig
atus
A. fu
mig
atus
A. te
rreu
s
A. te
rreu
sA.
nig
er
A. n
iger
A. n
idul
ans
A. n
idul
ans
CANDIDA NON-ALBICANS
CANDIDA NON-ALBICANS
ASPERGILLUSASPERGILLUS
Expanded Spectrum of In Vitro ActivityExpanded Spectrum of In Vitro Activity
C. pse
udot
ropi
calis
C. pse
udot
ropi
calis
Download from www.cancidas.ae
Unique Mechanism of Action (MOA) Offers Favorable Resistance Profile Unique Mechanism of Action (MOA) Offers Favorable Resistance Profile
• Active in vitro against fluconazole-, amphotericin B-, or flucytosine-resistant Candida
• Not cross-resistant with azoles or polyenes
• Not intrinsically resistant to Candida isolates
• Active in vitro against fluconazole-, amphotericin B-, or flucytosine-resistant Candida
• Not cross-resistant with azoles or polyenes
• Not intrinsically resistant to Candida isolates
Data on file, MSD; Graybill JR Int J Clin Pract 2001;55(9):633-638; Pfaller MA, Jones RN, Doern GV et al Diagn Microbiol Infect Dis 1999;35:19-25.Data on file, MSD; Graybill JR Int J Clin Pract 2001;55(9):633-638; Pfaller MA, Jones RN, Doern GV et al Diagn Microbiol Infect Dis 1999;35:19-25.

Download from www.cancidas.ae
Caspofungin: IndicationCaspofungin: Indication
• NEW: Invasive candidiasis including candidemia in neutropenic and non-neutropenic patients
In addition to:
• Invasive aspergillosis in patients who are refractory to or intolerant of standard therapies
• Esophageal candidiasis
• Oropharyngeal candidiasis
• NEW: Invasive candidiasis including candidemia in neutropenic and non-neutropenic patients
In addition to:
• Invasive aspergillosis in patients who are refractory to or intolerant of standard therapies
• Esophageal candidiasis
• Oropharyngeal candidiasis
Data on file, MSD.Data on file, MSD.
Download from www.cancidas.ae
Caspofungin: Proven Antifungal Efficacy against Invasive CandidiasisCaspofungin: Proven Antifungal Efficacy against Invasive Candidiasis
Clinical Trial: Protocol 014
Caspofungin vs. Amphotericin B Deoxycholate in the Treatment of Invasive Candidiasis in Neutropenic and Non-Neutropenic Patients
Clinical Trial: Protocol 014
Caspofungin vs. Amphotericin B Deoxycholate in the Treatment of Invasive Candidiasis in Neutropenic and Non-Neutropenic Patients
Data on file, MSD.Data on file, MSD.
Download from www.cancidas.ae
Protocol 014: ObjectiveProtocol 014: Objective
To compare the proportion of caspofungin acetate patients with both a favorable clinical response and a favorable microbiological assessment at the time of discontinuing IV antifungal therapy with that of amphotericin B patients
To compare the proportion of caspofungin acetate patients with both a favorable clinical response and a favorable microbiological assessment at the time of discontinuing IV antifungal therapy with that of amphotericin B patients
Data on file, MSD.Data on file, MSD.

Download from www.cancidas.ae
Protocol 014: DesignProtocol 014: Design
• Multicenter, randomized, double-blind, comparative study
• To compare the proportion of caspofungin patients with a favorable clinical response and a favorable microbiological assessment at the time of discontinuing IV antifungal therapy with that of amphotericin B patients
• Patients (18 years old) stratified by neutropenic status
• Multicenter, randomized, double-blind, comparative study
• To compare the proportion of caspofungin patients with a favorable clinical response and a favorable microbiological assessment at the time of discontinuing IV antifungal therapy with that of amphotericin B patients
• Patients (18 years old) stratified by neutropenic status
Caspofungin: Amphotericin B:114 pts (92 with candidemia) 125 pts (92 with candidemia)
— 50 mg/day — 0.7–1.0 mg/kg/day (70 mg loading dose on day 1) neutropenic patients
— 0.6–0.7 mg/kg/daynon-neutropenic patients
Caspofungin: Amphotericin B:114 pts (92 with candidemia) 125 pts (92 with candidemia)
— 50 mg/day — 0.7–1.0 mg/kg/day (70 mg loading dose on day 1) neutropenic patients
— 0.6–0.7 mg/kg/daynon-neutropenic patients
Data on file, MSD.Data on file, MSD.

Download from www.cancidas.ae
Study treatment course (at least 10 days of IV study therapy; switch to oral fluconazole possible after day 10)
Study treatment course (at least 10 days of IV study therapy; switch to oral fluconazole possible after day 10)
Protocol 014: Study Design Flow Chart Protocol 014: Study Design Flow Chart
Kartsonis NA. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy. Kartsonis NA. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy.
Start of IV study therapy
Start of IV study therapy
Positive culture
collected
Positive culture
collected
< 4 days < 4 days
Last positive culture
Last positive culture
End of treatment
course
End of treatment
course
2-week post-therapy
follow-up
2-week post-therapy
follow-up
6- to 8-week post-therapy
follow-up
6- to 8-week post-therapy
follow-up
14 days14 days
Day 10 of IV Rx
Day 10 of IV Rx
End of all antifungal Rx
End of all antifungal Rx
End of IV Study Rx
End of IV Study Rx
2-week follow-up2-week
follow-up6- to 8-week
follow-up6- to 8-week
follow-up
Primary Efficacy
Time Point Primary Efficacy
Time Point
Secondary Efficacy
Time Points Secondary Efficacy
Time Points

Download from www.cancidas.ae
Protocol 014: Efficacy Evaluation—Diagnostic CriteriaProtocol 014: Efficacy Evaluation—Diagnostic Criteria
• Favorable clinical response– Complete resolution of signs/symptoms of Candida
• Favorable microbiological response or presumptive eradication– Candida eradication from follow-up cultures
• Definition of comparability– 95.6% confidence interval (CI) difference
between groups
• Favorable clinical response– Complete resolution of signs/symptoms of Candida
• Favorable microbiological response or presumptive eradication– Candida eradication from follow-up cultures
• Definition of comparability– 95.6% confidence interval (CI) difference
between groups
Data on file, MSD.Data on file, MSD.
Download from www.cancidas.ae
Protocol 014: Primary Efficacy EndpointProtocol 014: Primary Efficacy Endpoint
• Proportion of patients with favorable overall response (favorable clinical and microbiological response) at end of IV therapy– Modified Intent-To-Treat (MITT): primary assessment
criteria• Patients received 1 day IV study therapy
– Evaluable Patients (EP): secondary assessment analysis• Patients met entry criteria, received IV study therapy 5
days, and had full efficacy evaluation at the end of IV study therapy
• Proportion of patients with favorable overall response (favorable clinical and microbiological response) at end of IV therapy– Modified Intent-To-Treat (MITT): primary assessment
criteria• Patients received 1 day IV study therapy
– Evaluable Patients (EP): secondary assessment analysis• Patients met entry criteria, received IV study therapy 5
days, and had full efficacy evaluation at the end of IV study therapy
Data on file, MSD.Data on file, MSD.

Download from www.cancidas.ae
Protocol 014: Caspofungin Demonstrates Comparable Efficacy Results in MITT Group Protocol 014: Caspofungin Demonstrates Comparable Efficacy Results in MITT Group
Caspofungin80/109
Caspofungin80/109
Perfect J. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy; Data on file, MSD.Perfect J. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy; Data on file, MSD.
00
1010
2020
3030
4040
5050
6060
7070
8080
9090
73.4%73.4%
61.7%61.7%
Amphotericin B71/115
Amphotericin B71/115
100100MITT (n=224)p=0.0861MITT (n=224)p=0.0861
Per
cent
age
Per
cent
age
Overall Response at End of IV Therapy (test of cure)Overall Response at End of IV Therapy (test of cure)

Download from www.cancidas.ae
Protocol 014: Caspofungin Appeared to Have Efficacy vs. Amphotericin B in Evaluable Patients Analysis*Protocol 014: Caspofungin Appeared to Have Efficacy vs. Amphotericin B in Evaluable Patients Analysis*
* Evaluable patients analysis was a secondary analysis.
Perfect J. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy; Data on file, MSD.
* Evaluable patients analysis was a secondary analysis.
Perfect J. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy; Data on file, MSD.
Caspofungin71/88
Caspofungin71/88
00
1010
2020
3030
4040
5050
6060
7070
8080
9090 80.7%80.7%
64.9%64.9%
Amphotericin B63/97
Amphotericin B63/97
100100P
erce
ntag
eP
erce
ntag
e
EP (n=185)p=0.0346EP (n=185)p=0.0346
Overall Response at End of IV Therapy (test of cure)Overall Response at End of IV Therapy (test of cure)

Download from www.cancidas.ae
Protocol 014: Caspofungin Demonstrates Similar Efficacy vs. Amphotericin B in Candidemia Protocol 014: Caspofungin Demonstrates Similar Efficacy vs. Amphotericin B in Candidemia
CaspofunginCaspofungin
Data on file, MSD.Data on file, MSD.
00
1010
2020
3030
4040
5050
6060
7070
8080
9090
72.5%72.5%
62.5%62.5%
Amphotericin BAmphotericin B
100100
Per
cent
age
of P
atie
nts
Per
cent
age
of P
atie
nts
n=92n=92
n=94n=94
Download from www.cancidas.ae
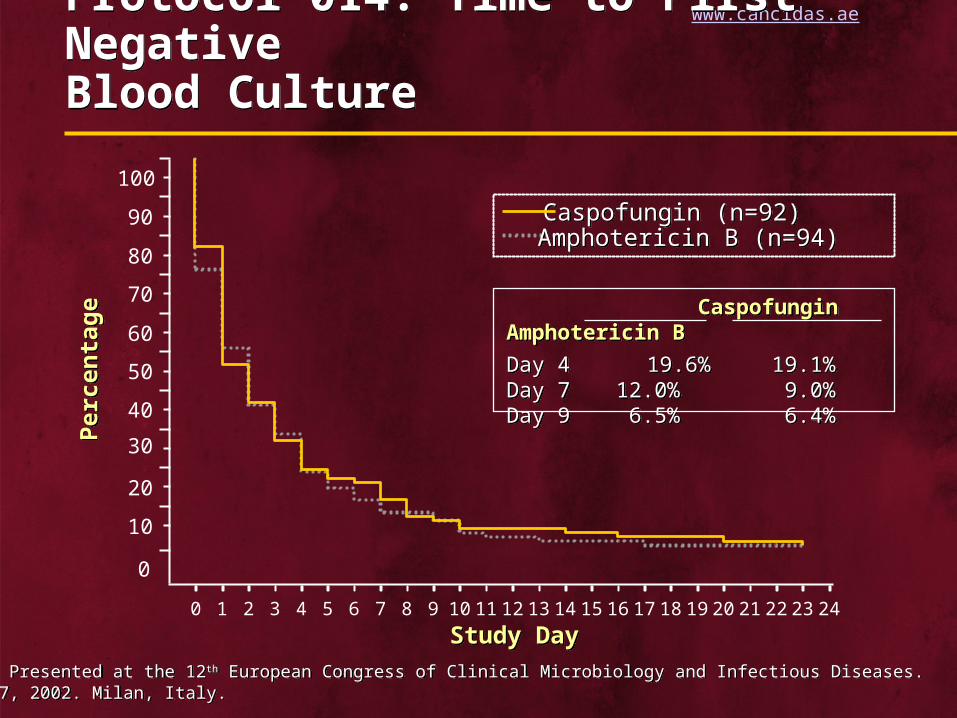
Protocol 014: Time to First Negative Blood Culture Protocol 014: Time to First Negative Blood Culture
Per
cent
age
Per
cent
age
Perfect J. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy.Perfect J. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy.
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
0
10
20
30
40
50
60
70
80
90
100
Study DayStudy Day
Caspofungin Amphotericin B
Day 4 19.6% 19.1%Day 7 12.0% 9.0%Day 9 6.5% 6.4%
Caspofungin Amphotericin B
Day 4 19.6% 19.1%Day 7 12.0% 9.0%Day 9 6.5% 6.4%
Caspofungin (n=92)Caspofungin (n=92)Amphotericin B (n=94)Amphotericin B (n=94)

Download from www.cancidas.ae
Protocol 014: Failure or Relapse Rates Protocol 014: Failure or Relapse Rates
Perfect J. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy.Perfect J. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy.
00
1010
2020
3030
4040
26.6%26.6%
6.4%6.4%
5050
Failure(End of IV
study therapy)
Failure(End of IV
study therapy)
38.2%38.2%
7.0%7.0%2.7%2.7%
16.5%16.5%
Relapse(6–8 weeks post-Rx)
Relapse(6–8 weeks post-Rx)
Toxicity requiring additional treatment
p=0.0277
Toxicity requiring additional treatment
p=0.0277
Caspofungin (n=109)70/50 mg
Amphotericin B (n=115)0.6–1.0 mg/kg
Caspofungin (n=109)70/50 mg
Amphotericin B (n=115)0.6–1.0 mg/kg
Download from www.cancidas.ae
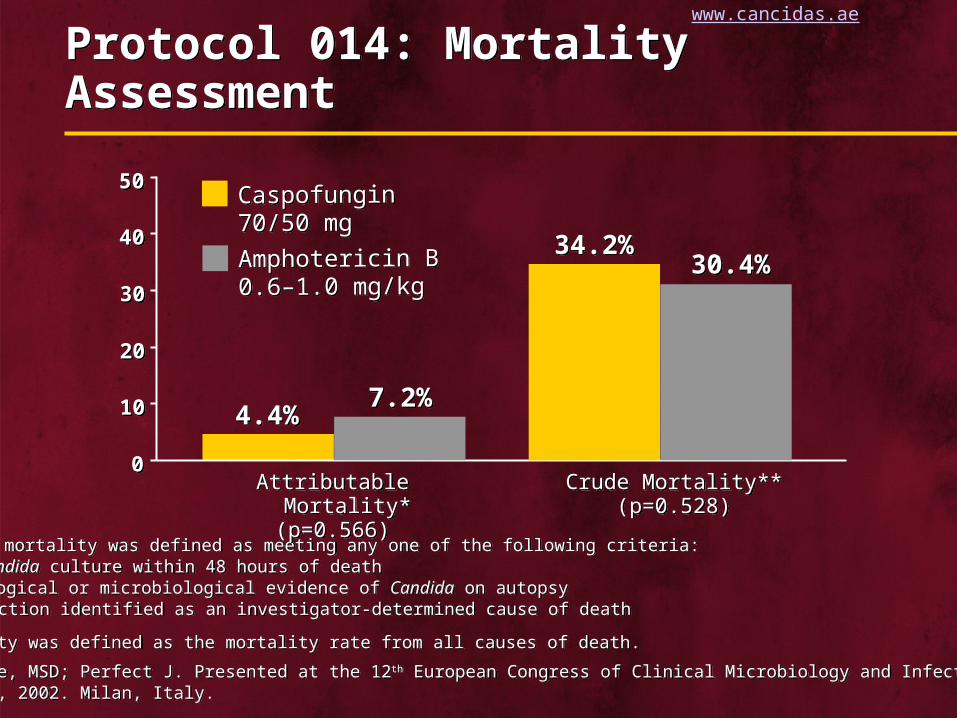
Protocol 014: Mortality Assessment Protocol 014: Mortality Assessment
* Attributable mortality was defined as meeting any one of the following criteria:— Positive Candida culture within 48 hours of death— Histopathological or microbiological evidence of Candida on autopsy— Candida infection identified as an investigator-determined cause of death
** Crude mortality was defined as the mortality rate from all causes of death.
Data on file, MSD; Perfect J. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy.
* Attributable mortality was defined as meeting any one of the following criteria:— Positive Candida culture within 48 hours of death— Histopathological or microbiological evidence of Candida on autopsy— Candida infection identified as an investigator-determined cause of death
** Crude mortality was defined as the mortality rate from all causes of death.
Data on file, MSD; Perfect J. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases. April 24-27, 2002. Milan, Italy.
Crude Mortality**(p=0.528)
Crude Mortality**(p=0.528)
00
1010
2020
3030
4040
4.4%4.4%
34.2%34.2%
5050
30.4%30.4%
7.2%7.2%
Caspofungin 70/50 mg
Amphotericin B 0.6–1.0 mg/kg
Caspofungin 70/50 mg
Amphotericin B 0.6–1.0 mg/kg
Attributable Mortality*(p=0.566)
Attributable Mortality*(p=0.566)
Download from www.cancidas.ae
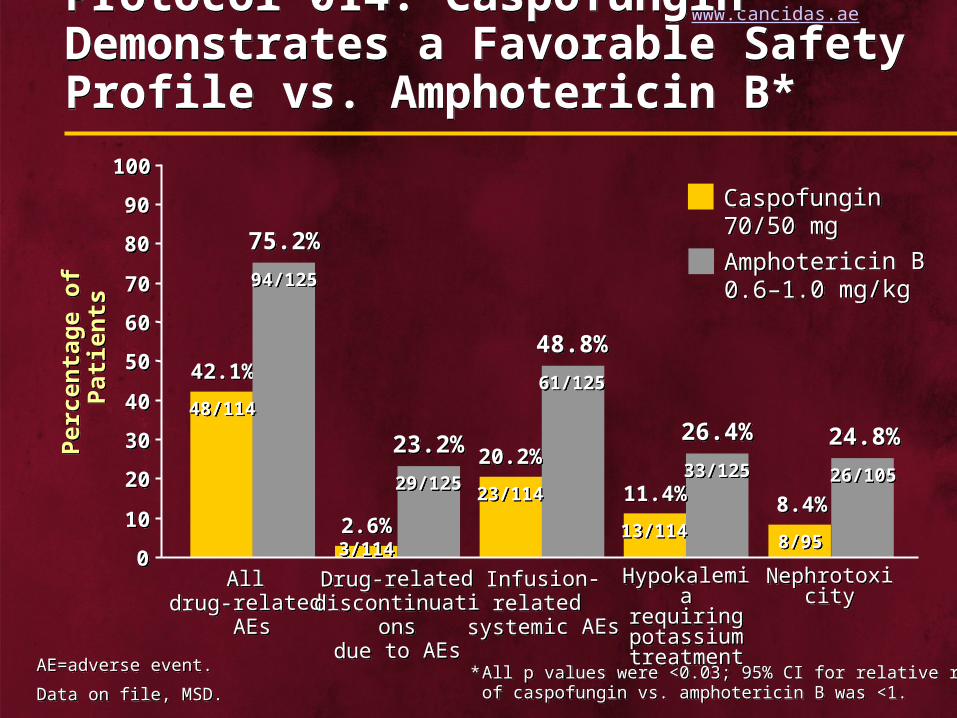
Protocol 014: Caspofungin Demonstrates a Favorable Safety Profile vs. Amphotericin B* Protocol 014: Caspofungin Demonstrates a Favorable Safety Profile vs. Amphotericin B*
AE=adverse event.
Data on file, MSD.
AE=adverse event.
Data on file, MSD.
00
1010
2020
3030
4040
5050
6060
7070
8080
9090
100100
Per
cent
age
of P
atie
nts
Per
cent
age
of P
atie
nts
42.1%42.1%
75.2%75.2%
2.6%2.6%
23.2%23.2%20.2%20.2%
48.8%48.8%
11.4%11.4%
26.4%26.4%
8.4%8.4%
24.8%24.8%
All drug-related
AEs
All drug-related
AEs
Infusion-related
systemic AEs
Infusion-related
systemic AEs
Drug-relateddiscontinuations
due to AEs
Drug-relateddiscontinuations
due to AEs
Hypokalemiarequiring potassium treatment
Hypokalemiarequiring potassium treatment
NephrotoxicityNephrotoxicity
48/11448/114
94/12594/125
3/1143/114
29/12529/12523/11423/114
61/12561/125
13/11413/114
33/12533/125
8/958/95
26/10526/105
* All p values were <0.03; 95% CI for relative riskof caspofungin vs. amphotericin B was <1.
* All p values were <0.03; 95% CI for relative riskof caspofungin vs. amphotericin B was <1.
Caspofungin 70/50 mg
Amphotericin B 0.6–1.0 mg/kg
Caspofungin 70/50 mg
Amphotericin B 0.6–1.0 mg/kg
Download from www.cancidas.ae
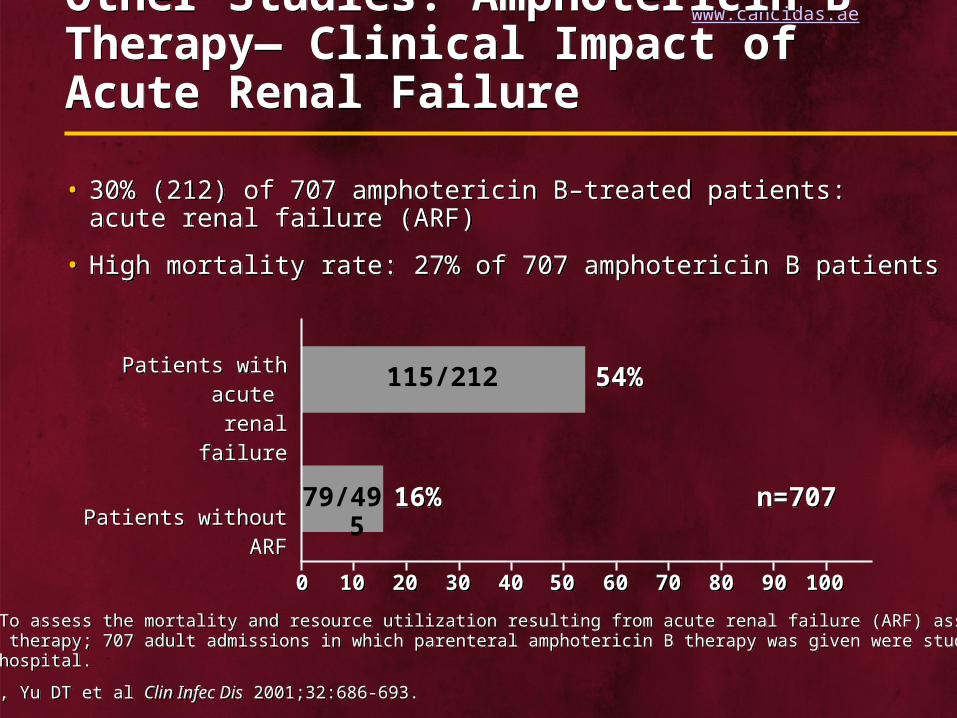
Other Studies: Amphotericin B Therapy— Clinical Impact of Acute Renal Failure Other Studies: Amphotericin B Therapy— Clinical Impact of Acute Renal Failure
• 30% (212) of 707 amphotericin B–treated patients: acute renal failure (ARF)
• High mortality rate: 27% of 707 amphotericin B patients
• 30% (212) of 707 amphotericin B–treated patients: acute renal failure (ARF)
• High mortality rate: 27% of 707 amphotericin B patients
Study Design: To assess the mortality and resource utilization resulting from acute renal failure (ARF) associated with amphotericin B therapy; 707 adult admissions in which parenteral amphotericin B therapy was given were studied at a tertiary-care hospital.
Bates DW, Su L, Yu DT et al Clin Infec Dis 2001;32:686-693.
Study Design: To assess the mortality and resource utilization resulting from acute renal failure (ARF) associated with amphotericin B therapy; 707 adult admissions in which parenteral amphotericin B therapy was given were studied at a tertiary-care hospital.
Bates DW, Su L, Yu DT et al Clin Infec Dis 2001;32:686-693.
Patients with acute renal failure
Patients with acute renal failure
16%16%
54%54%
5050404030302020101000 1001009090808070706060
Patients without ARFPatients without ARFn=707n=70779/495
115/212

Download from www.cancidas.ae
Other Studies: Caspofungin Maintains Favorable Safety/Tolerability ProfileOther Studies: Caspofungin Maintains Favorable Safety/Tolerability Profile
• Overall safety assessed in 876 patients
• 394 patients enrolled in Phase I studies
• Most patients with Candida infections had serious underlying medical conditions, including hematologic or other malignancy, recent major surgery, or HIV
• In a clinical study among patients with oropharyngeal or esophageal candidiasis, caspofungin (n=83) demonstrated a comparable tolerability profile vs. fluconazole (n=94)
• In a clinical study among patients with invasive candidiasis, caspofungin (n=114) demonstrated a superior tolerability profile to amphotericin B (n=125)
• In an open-label, noncomparative aspergillosis (n=69) study, caspofungin maintained its favorable profile
• Overall safety assessed in 876 patients
• 394 patients enrolled in Phase I studies
• Most patients with Candida infections had serious underlying medical conditions, including hematologic or other malignancy, recent major surgery, or HIV
• In a clinical study among patients with oropharyngeal or esophageal candidiasis, caspofungin (n=83) demonstrated a comparable tolerability profile vs. fluconazole (n=94)
• In a clinical study among patients with invasive candidiasis, caspofungin (n=114) demonstrated a superior tolerability profile to amphotericin B (n=125)
• In an open-label, noncomparative aspergillosis (n=69) study, caspofungin maintained its favorable profile
Data on file, MSD.Data on file, MSD.

Download from www.cancidas.ae
Caspofungin: Minimal Drug InteractionsCaspofungin: Minimal Drug Interactions
• Not a P450 (CYP) inhibitor
• No antagonistic interaction with amphotericin B or itraconazole
• Has been used with antirejection drugs tacrolimus and/or mycophenolate
• Not a P450 (CYP) inhibitor
• No antagonistic interaction with amphotericin B or itraconazole
• Has been used with antirejection drugs tacrolimus and/or mycophenolate
Data on file, MSD; Bartizal K et al Antimicrob Agents Chemother 1997;41:2326-2332.Data on file, MSD; Bartizal K et al Antimicrob Agents Chemother 1997;41:2326-2332.

Download from www.cancidas.ae
Caspofungin: Dosing/AdministrationCaspofungin: Dosing/Administration
• Once-daily dosing with 50 mg standard dose
• 70 mg loading dose on day 1 for aspergillosis and invasive candidiasis
• No premedication necessary
• Recommended infusion time: 1 hour
• No dosage adjustment in many cases*
• Once-daily dosing with 50 mg standard dose
• 70 mg loading dose on day 1 for aspergillosis and invasive candidiasis
• No premedication necessary
• Recommended infusion time: 1 hour
• No dosage adjustment in many cases*
* For patients with moderate hepatic insufficiency (Child-Pugh score 7-9), a dose adjustment to 35 mg daily is recommended. There is no clinical experience in patients with severe hepatic insufficiency (Child-Pugh score >9).
Data on file, MSD.
* For patients with moderate hepatic insufficiency (Child-Pugh score 7-9), a dose adjustment to 35 mg daily is recommended. There is no clinical experience in patients with severe hepatic insufficiency (Child-Pugh score >9).
Data on file, MSD.

Download from www.cancidas.ae
Conclusions: Caspofungin—The New Gold StandardConclusions: Caspofungin—The New Gold Standard
• Invasive candidiasis:– Caspofungin is comparable to amphotericin B
(MITT analysis)– Caspofungin appears to be superior to
amphotericin B (EP analysis)– Candidemia: Caspofungin is comparable to
amphotericin B
• Overall safety/tolerability profile:– Caspofungin has a favorable tolerability profile
• Invasive candidiasis:– Caspofungin is comparable to amphotericin B
(MITT analysis)– Caspofungin appears to be superior to
amphotericin B (EP analysis)– Candidemia: Caspofungin is comparable to
amphotericin B
• Overall safety/tolerability profile:– Caspofungin has a favorable tolerability profile
Data on file, MSD.Data on file, MSD.

Download from www.cancidas.ae
ReferencesReferences

Download from www.cancidas.ae
ReferencesReferences





