Embed Size (px)
Citation preview

LA FERTILITA’
DELLA DONNA
Vincent Castronovo, MD, PhD
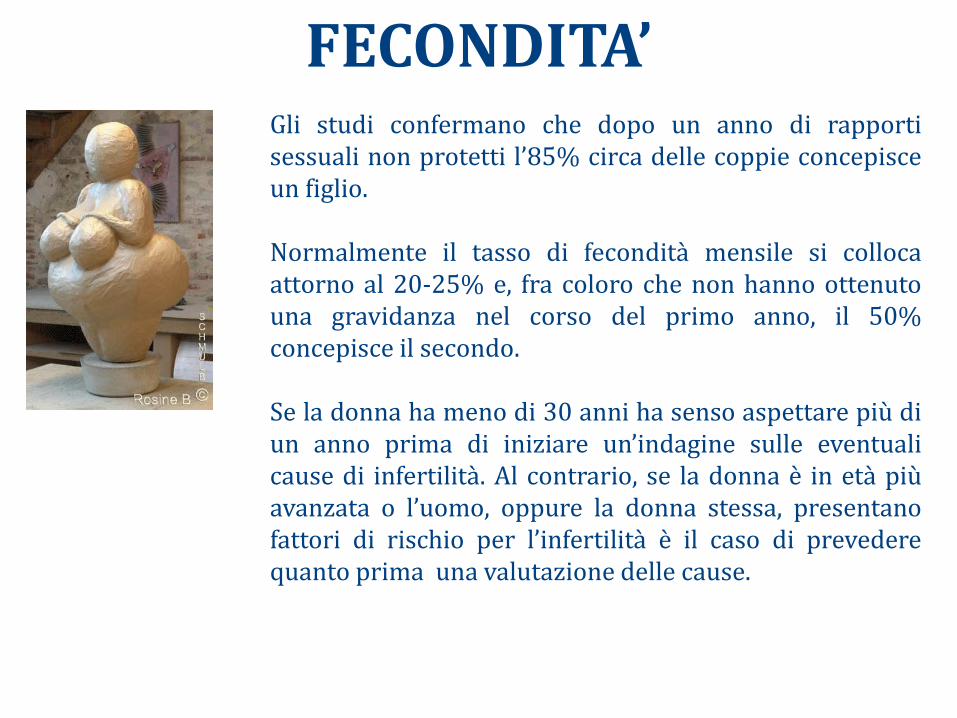
Gli studi confermano che dopo un anno di rapporti sessuali non protetti l’85% circa delle coppie concepisce un figlio. Normalmente il tasso di fecondità mensile si colloca attorno al 20-25% e, fra coloro che non hanno ottenuto una gravidanza nel corso del primo anno, il 50% concepisce il secondo. Se la donna ha meno di 30 anni ha senso aspettare più di un anno prima di iniziare un’indagine sulle eventuali cause di infertilità. Al contrario, se la donna è in età più avanzata o l’uomo, oppure la donna stessa, presentano fattori di rischio per l’infertilità è il caso di prevedere quanto prima una valutazione delle cause.
FECONDITA’

Il concepimento naturale richiede : Nell’uomo: Quantità sufficiente di spermatozoi normali. Gli spermatozoi devono passare nelle vie genitali maschili dove portano a termine la maturazione e acquisiscono la mobilità.
Nella donna: Crescita e maturazione dell’ovocita. Secrezioni del collo (muco) favorevoli alla sopravvivenza degli spermatozoi. L’apparato genitale consente l’incontro dei gameti. Cavità uterina anatomicamente normale e mucosa in grado di accogliere l’embrione.
FECONDITA’

Fertilità umana
• Il 30% delle coppie dichiara di avere avuto difficoltà a concepire
• Il 20% delle coppie si rivolge al medico per l’infertilità
• l ’eziologia dell’infertilità: • 1/3 di origine maschile
• 1/3 di origine femminile
• 1/3 di origine mista
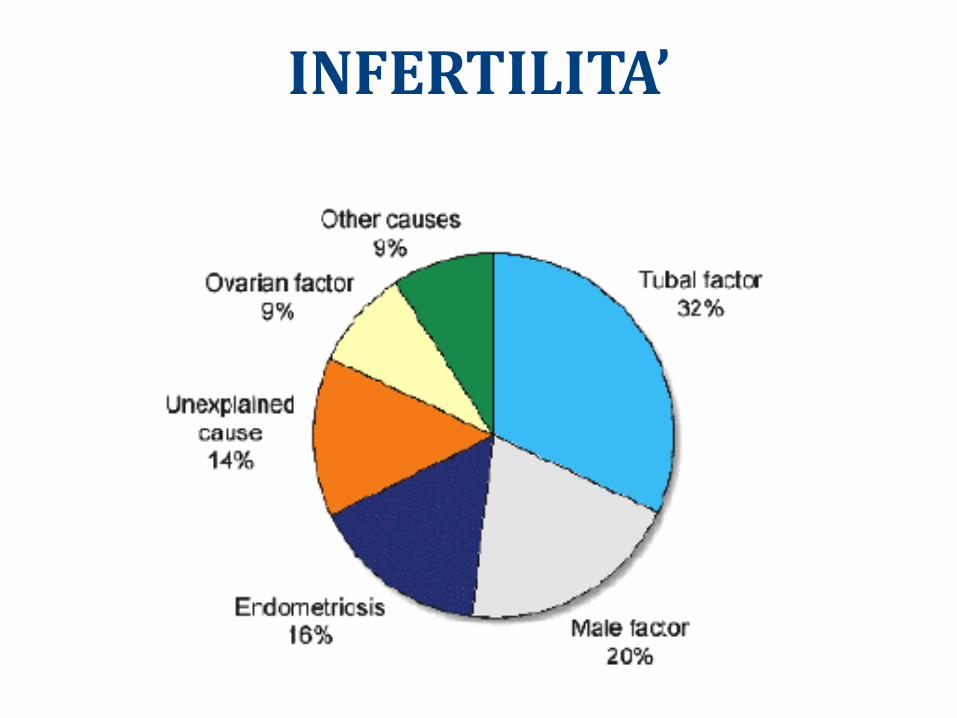
INFERTILITA’
Il consulto per l’infertilità
• Incontrare la coppia
• Anamnesi
– Antecedenti
– Sessualità
• Esame clinico
• Biologia nutrizionale e funzionale
• Indagini complementari
Infertilità: Anamnesi • Anomalie della sessualità di coppia
• Rapporti troppo distanziati
• donna: vaginismo
• uomo: impotenza, assenza di eiaculazione
Cause di infertilità
• Antecedenti uomo
– criptorchidismo
– orchite-torsione testicolo
– chemio-radioterapia
• Antedecenti donna
– Età del menarca
– salpingite- cisti ovariche
– chemio-radioterapia
Anamnesi
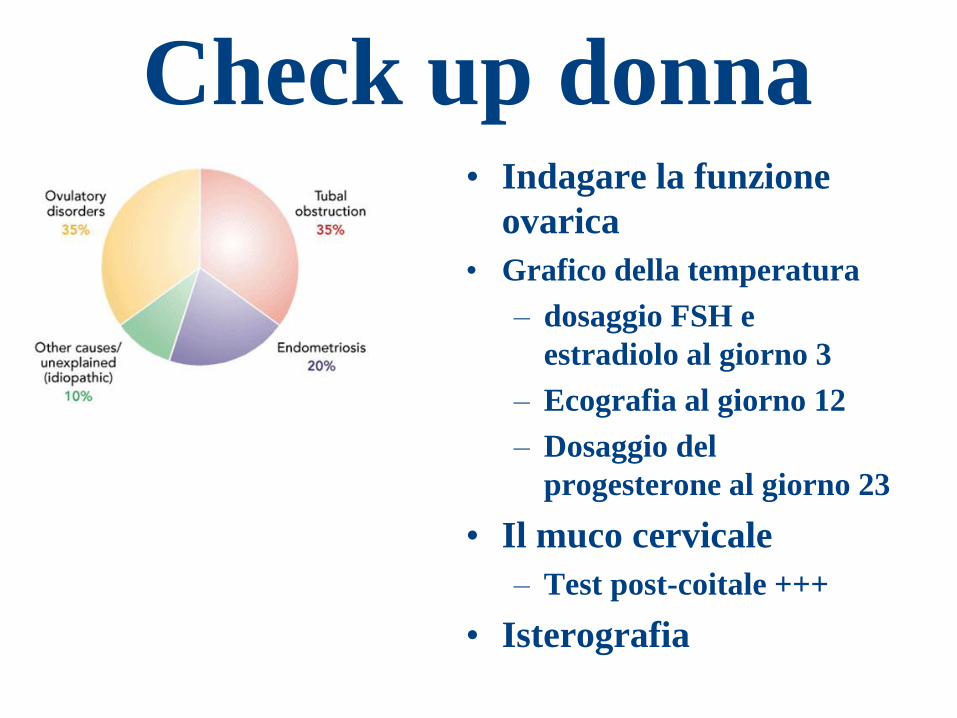
Check up donna • Indagare la funzione
ovarica
• Grafico della temperatura
– dosaggio FSH e
estradiolo al giorno 3
– Ecografia al giorno 12
– Dosaggio del
progesterone al giorno 23
• Il muco cervicale
– Test post-coitale +++
• Isterografia
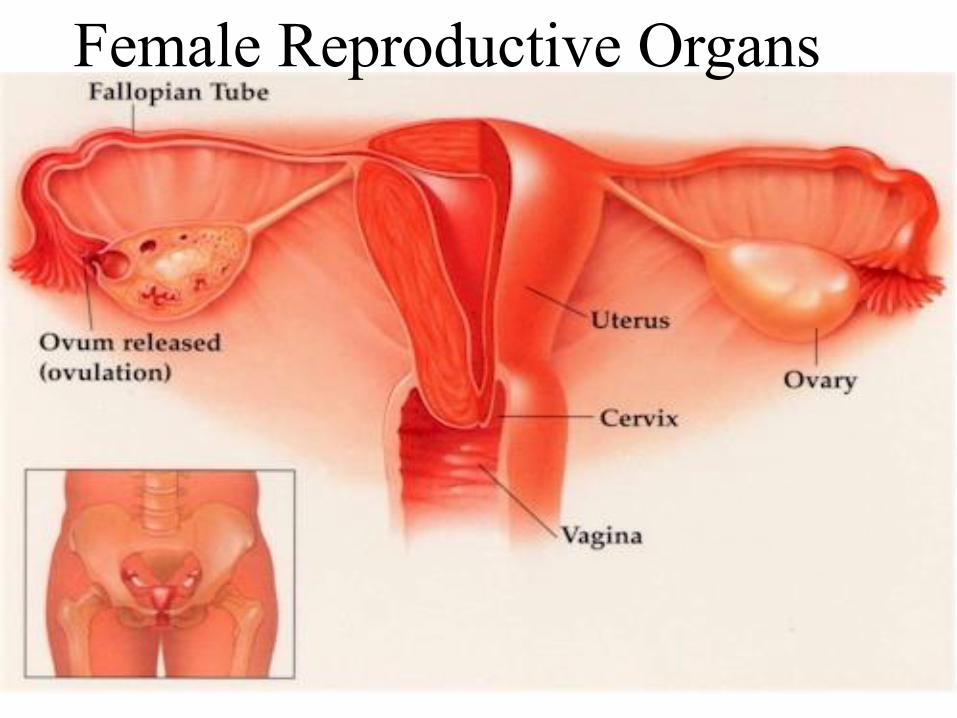
Female Reproductive Organs
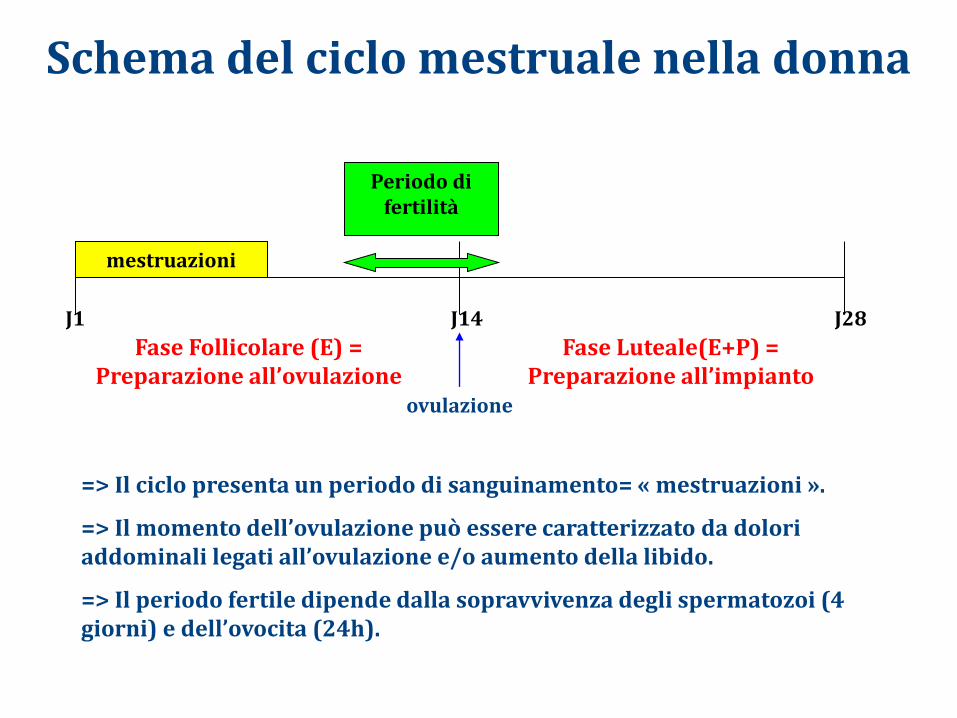
Schema del ciclo mestruale nella donna
J1 J14 J28
mestruazioni
Fase Follicolare (E) = Preparazione all’ovulazione
Fase Luteale(E+P) = Preparazione all’impianto
ovulazione
Periodo di fertilità
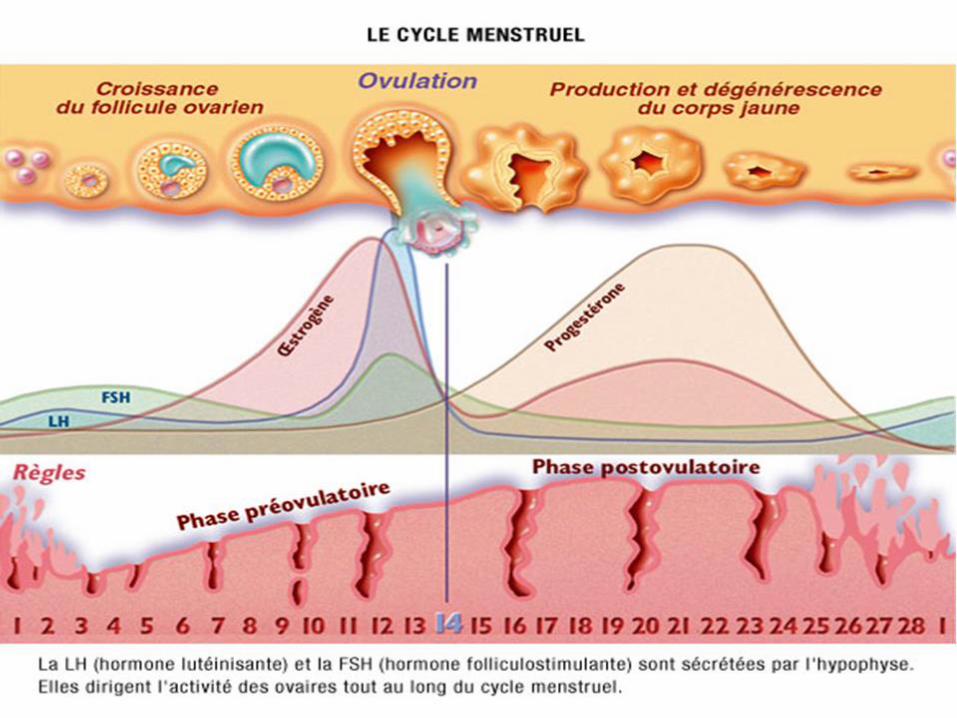
=> Il ciclo presenta un periodo di sanguinamento= « mestruazioni ».
=> Il momento dell’ovulazione può essere caratterizzato da dolori addominali legati all’ovulazione e/o aumento della libido.
=> Il periodo fertile dipende dalla sopravvivenza degli spermatozoi (4 giorni) e dell’ovocita (24h).
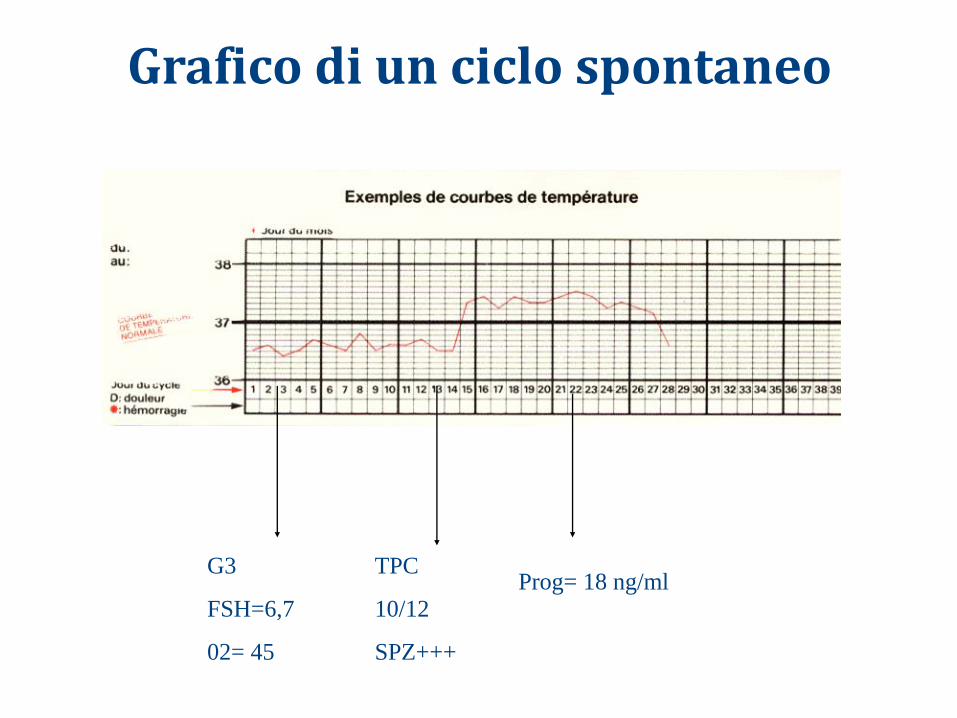
Grafico di un ciclo spontaneo
G3
FSH=6,7
02= 45
TPC
10/12
SPZ+++
Prog= 18 ng/ml
Anomalie della funzione ovarica
• FSH
• LH
• Prolattina
• Estradiolo
• Progesterone
• Testosterone
• SHBG
Funzione ovarica
• Età
– Diminuzione della riserva ovarica
– Diminuzione della fertilità
– Dosaggio FSH
• normale <10mUI:ml
Anomalie della funzione ovarica
• Disovulazione
• Anovulazione
• Amenorrea
Test post-coitale
• Su ciclo spontaneo
– Da 24 a 48h prima dell’ovulazione
• se TPC negativo con assenza di muco?
Anomalie della funzione ovarica
• Origine ipotalamo-ipofisaria
– funzionale: anoressia, stress (FSH basso)
– organica: adenoma da prolattina
• Sindrome dell’ovaio policistico
• Insufficienza ovarica (FSH alto)
– iniziale
– prematura: menopausa precoce

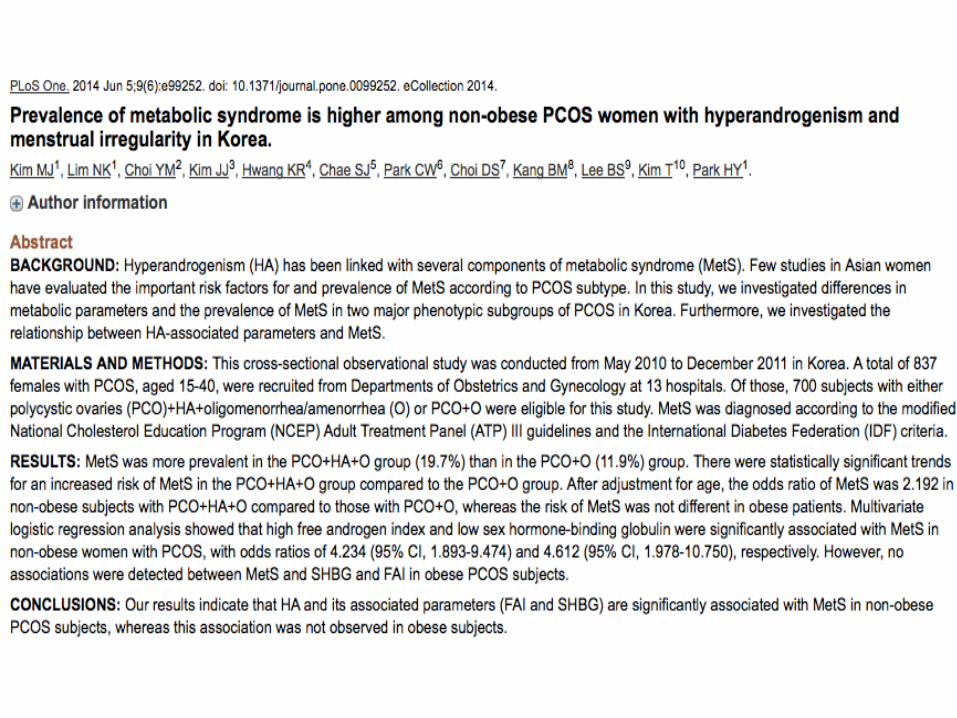
Sindrome dell’ovaio micropolicistico
• Descritto la prima volta da Stein e Leventhal nel 1935
• Caratterizzato da iperandrogenismo, Irregolarità mestruali, ovaio policistico e adiposità addominale
• Sindrome a eziologia multipla e a espressione clinica variabile
• La metà dei casi si presenta in modo non classico
Sindrome dell’ovaio micropolicistico
Epidemiologia
• Tra le cause più frequenti di infertilità femminile
• Tra le patologie endocrine più comuni nella donna
• Associazione con diabete di tipo II e diabete di tipo I
Sindrome dell’ovaio micropolicistico
Epid
em
iolo
gia
• Dal 4 al 10 % della popolazione femminile
• Il 50% ha obesità di tipo androide
• Il 32% è infeconda
• Il 36% ha iperandrogenismo con acne e irsutismo
• Il 29% presenta alterazioni mestruali
• L’1% scoperta casuale
Sindrome dell’ovaio micropolicistico
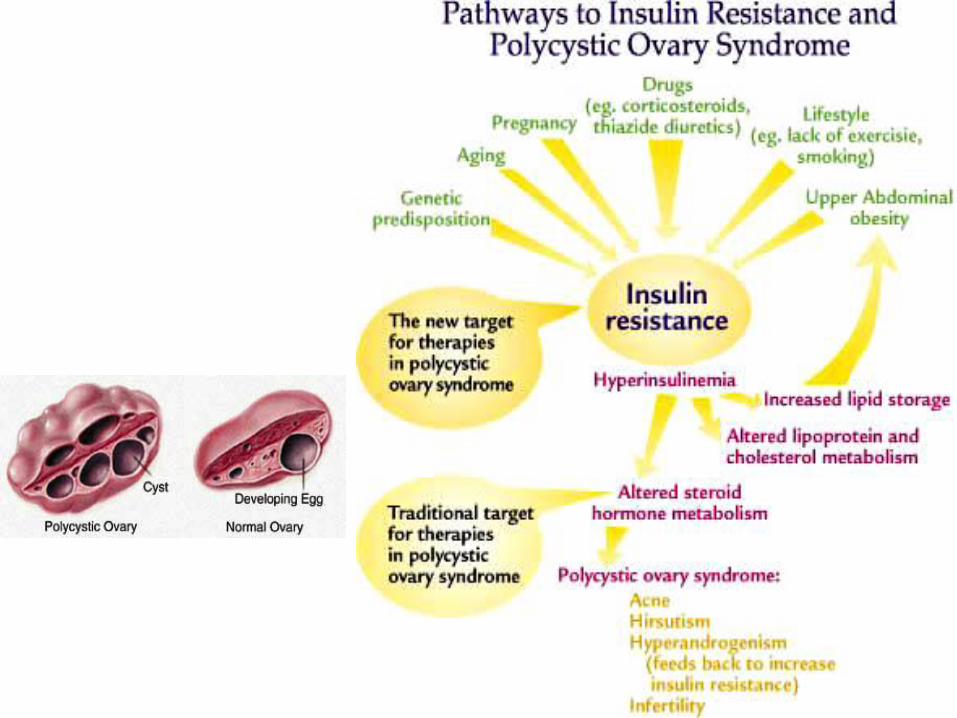
Pa
tog
en
esi
• Eccesso di androgeni intraovarici anovulazione e cisti ovariche multiple
• In discussione se anomalia della secrezione di gonadotropine ipofisarie (LH,FSH) o difetto della steroidogenesi ovarica/surrenale
Sindrome dell’ovaio micropolicistico
Eziologia
• Disordine genetico complesso
• Fattori ereditari e non ereditari
• Ipotesi attuale: genetica ovarica intrinseca che interagisce con fattori congeniti o ambientali nel causare disfunzionamento della steroidogenesi
• Studi sui geni che regolano l’asse ipotalamo-ipofisi- gonadi e la resistenza insulinica
Sindrome dell’ovaio micropolicistico
• Evidenza clinica e biochimica
• Acne, irsutismo, virilizzazione
• Irsutismo = distribuzione pilifera secondo il modello maschile (labbro superiore, mento, periareolare, medio sternale)
• Virilizzazione = aumento della massa muscolare, voce più profonda, clitoromegalia.
Ipe
ran
dro
ge
nis
mo
Sindrome dell’ovaio
micropolicistico
Ind
ag
ini
pa
racl
inic
he
pe
r la
M
icro
po
lici
sto
si o
va
rica
• Tassi elevati di LH incostanti
• FSH normale o basso (se tassi normali sono probabilmente sotto la soglia necessaria per il
normale sviluppo follicolare)
• Rapporto LH/FSH elevato PRL limite superiore
• Caduta della SHBG (con aumento del testosterone libero) prova di iperinsulinismo
• Androgeni: – testosterone e/o ∆4 androstenedione elevati
– DHEA…tasso variabile
– 170HP diagnosi differenziale
• Ecografia: – Ovaie voluminose, cistiche
– Follicoli multipli immaturi 10 follicoli/ovaio di uguali dimensioni ipertrofia dello stroma
Sindrome dell’ovaio micropolicistico
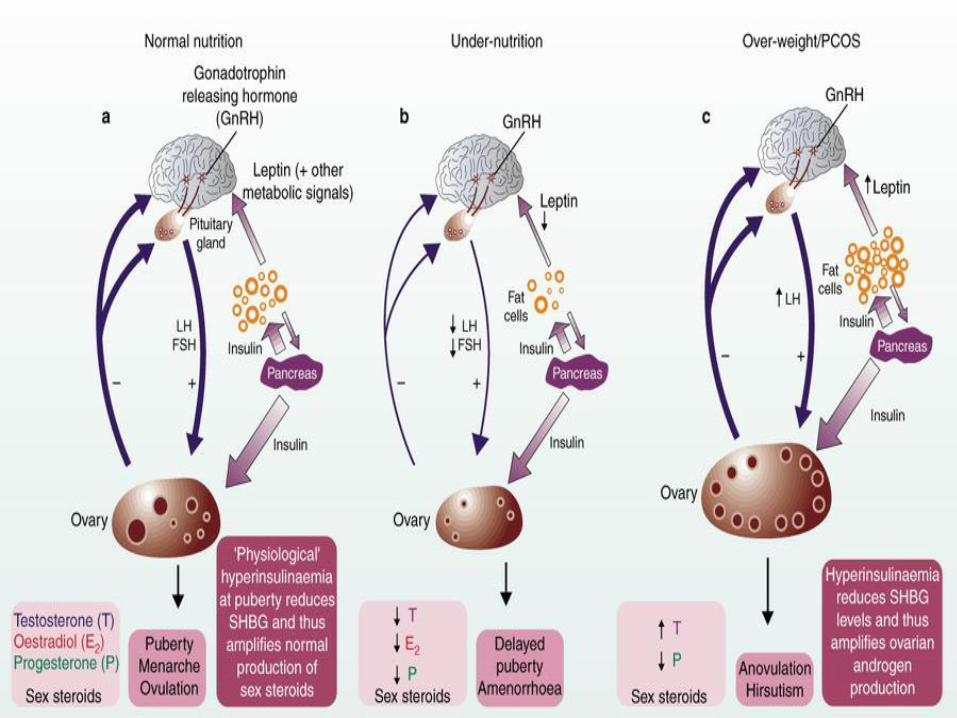
Iperinsulinismo
• Associato a resistenza insulinica
• Indipendente da obesità
• Effetto potenziante dell’LH sulle cellule tecali dell’ovaio
• Fattore chiave nella fisiopatologia della micropolicistosi ovarica
Sindrome dell’ovaio micropolicistico
Obesità • Dilemma a livello diagnostico
• Il 30-75 % delle pazienti con PCOS
• PCOS atipico : Pazienti obese con evidenza biochimica e/o clinica di iperandrogenismo senza irregolarità mestruali o policistosi ovarica
Sindrome dell’ovaio micropolicistico
• Forte associazione tra diabete di tipo II e PCOS
• La resistenza all’insulina influisce sulla steroidogenesi
• Il 10% circa delle donne con hanno DM di tipo II a 40 anni
• Il 1/3 delle donne con PCOS avranno un test di tolleranza al glucosio anormale
Sindrome dell’ovaio micropolicistico
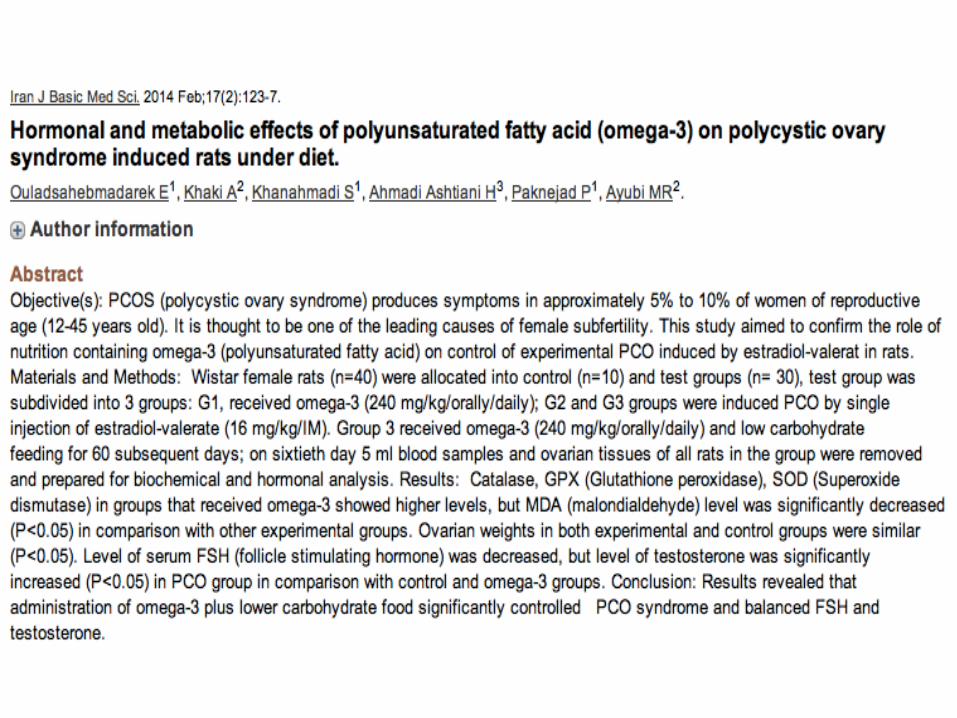
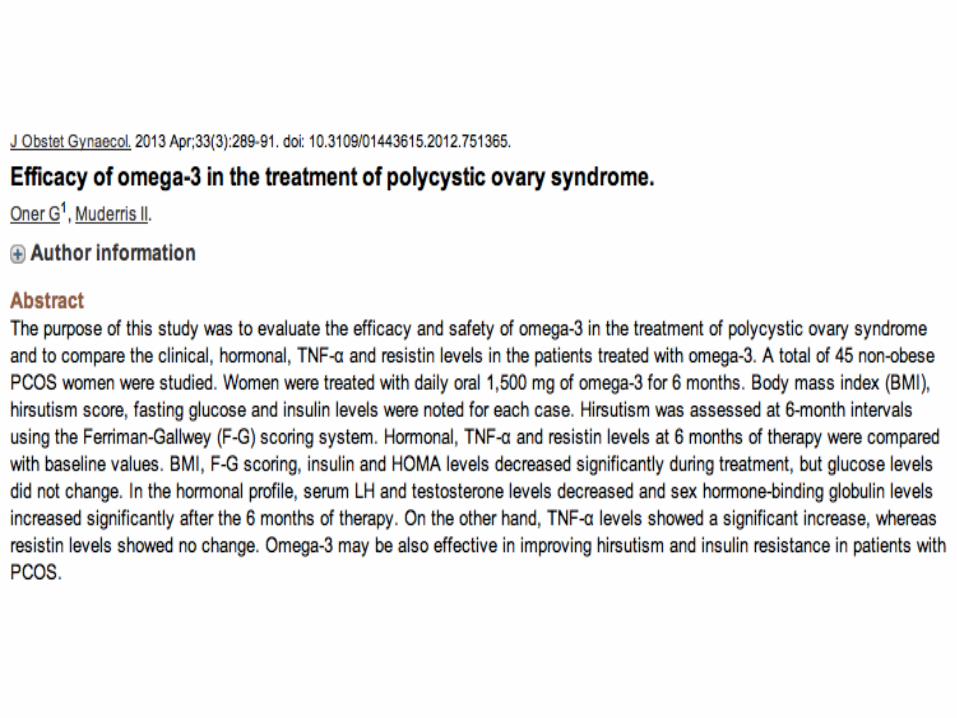
• Presa in carico della sindrome metabolica • Presa in carico dell’infiammazione patologica (leaky gut syndrome, immunizzazione alimentare,….) TR
ATT
AM
ENTO
Sindrome dell’ovaio
micropolicistico
Ipotiroidismo subclinico E infertilità nella donna
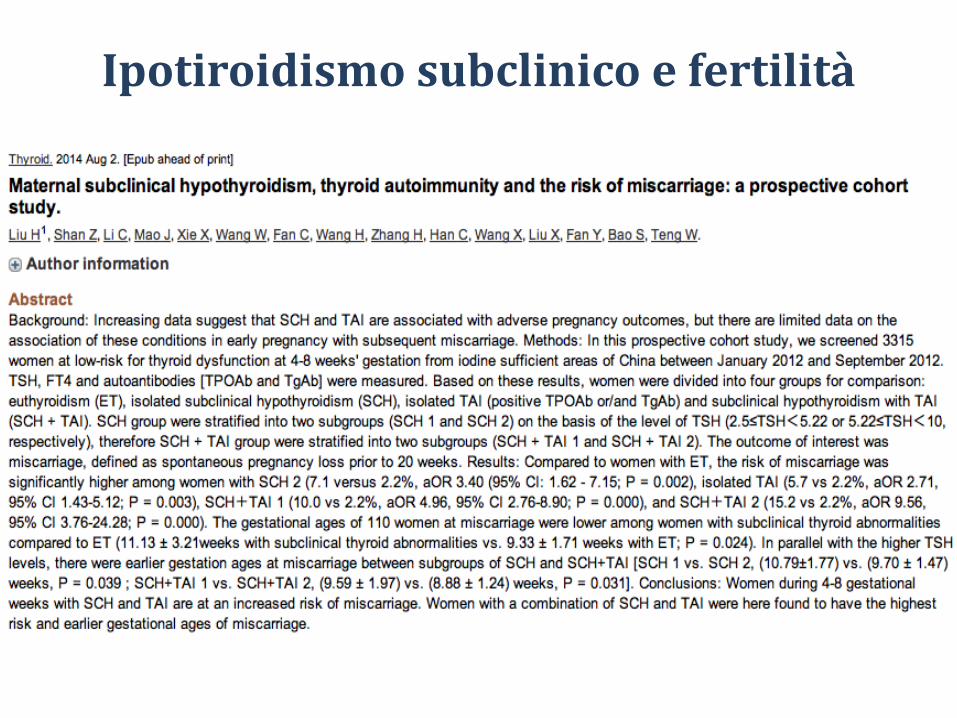
Ipotiroidismo subclinico e fertilità

L’ipotiroidismo subclinico è definito da un tasso di TSH > 4 mUI/l, confermato da un secondo dosaggio a 1 mese di distanza senza anomalie della concentrazione di T4L
Ipotiroidismo subclinico
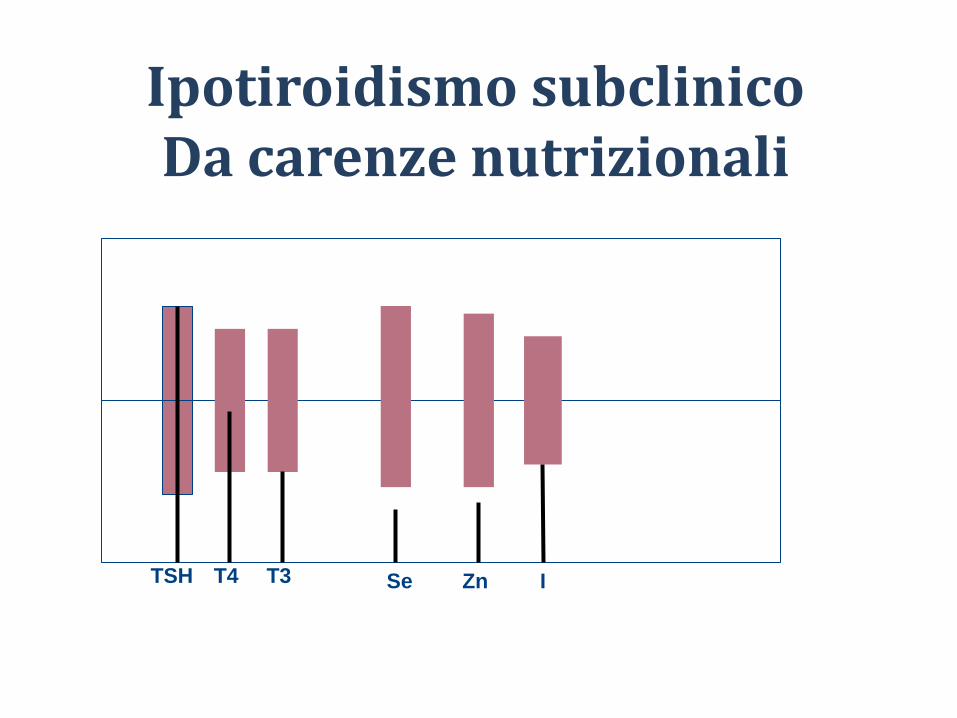
TSH T3 T4 Se Zn I
Ipotiroidismo subclinico Da carenze nutrizionali
TSH T3 T4 Se Zn I
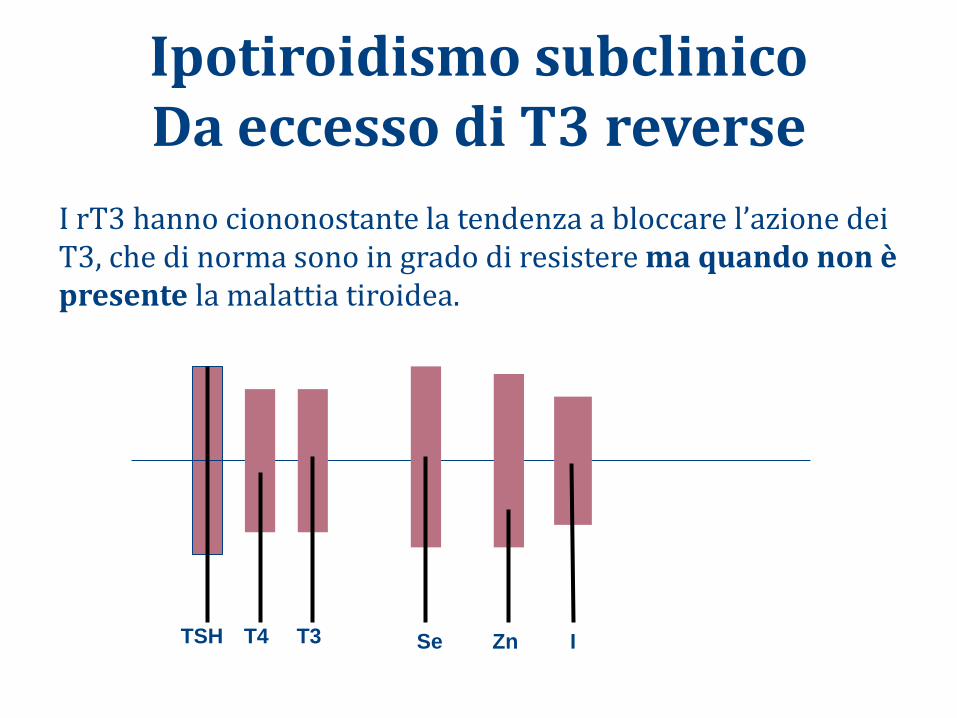
Ipotiroidismo subclinico Da eccesso di T3 reverse
I rT3 hanno ciononostante la tendenza a bloccare l’azione dei T3, che di norma sono in grado di resistere ma quando non è presente la malattia tiroidea.
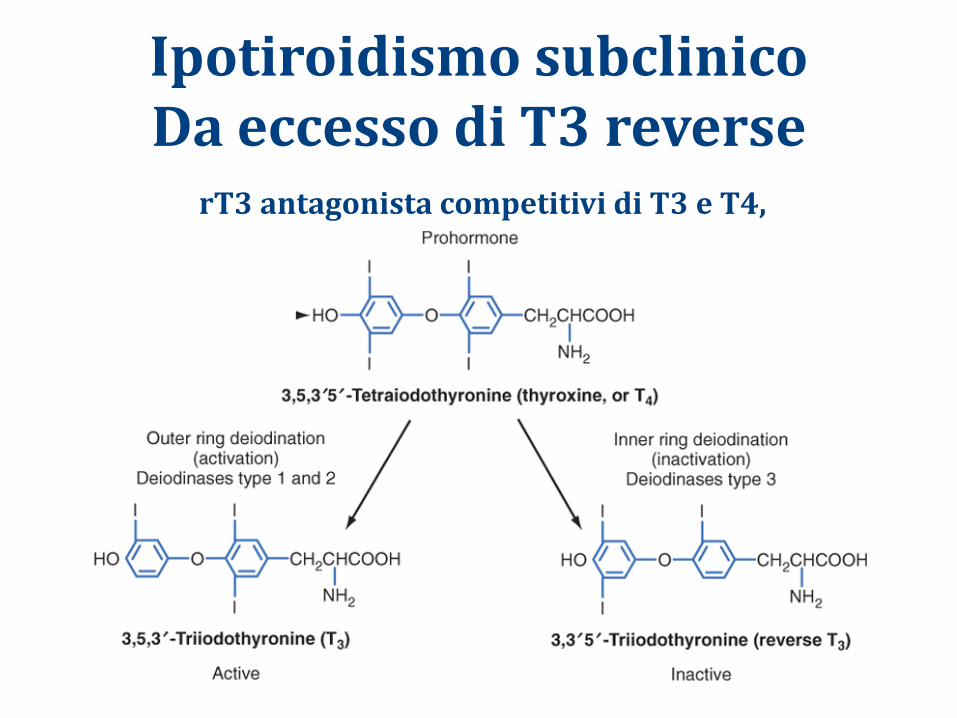
Ipotiroidismo subclinico Da eccesso di T3 reverse
rT3 antagonista competitivi di T3 e T4,
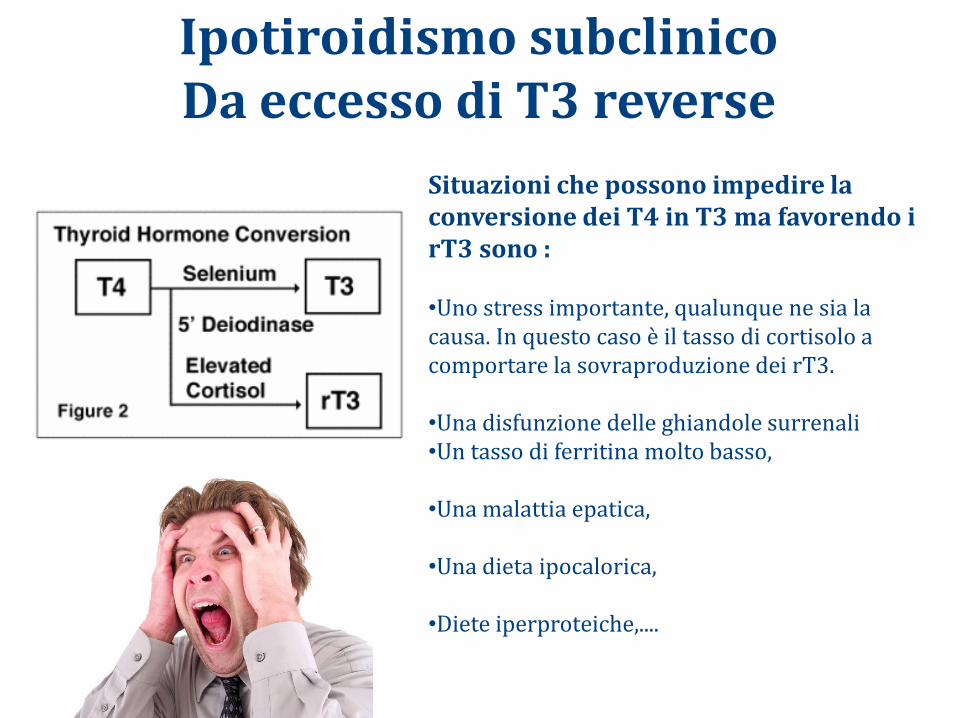
Ipotiroidismo subclinico Da eccesso di T3 reverse
Situazioni che possono impedire la conversione dei T4 in T3 ma favorendo i rT3 sono : •Uno stress importante, qualunque ne sia la causa. In questo caso è il tasso di cortisolo a comportare la sovraproduzione dei rT3. •Una disfunzione delle ghiandole surrenali •Un tasso di ferritina molto basso, •Una malattia epatica, •Una dieta ipocalorica, •Diete iperproteiche,....
• L-Tirosina • Iodio • Ferro • Selenio • Acidi grassi omega-3 • Intestino • Antiossidanti
Supporo nutrizionale e funzionale
Check up della donna
Ovulazione normale
Muco cervicale normale
Cavità e tube normali
Causa evidente o inspiegabile
Glutine e infertilità
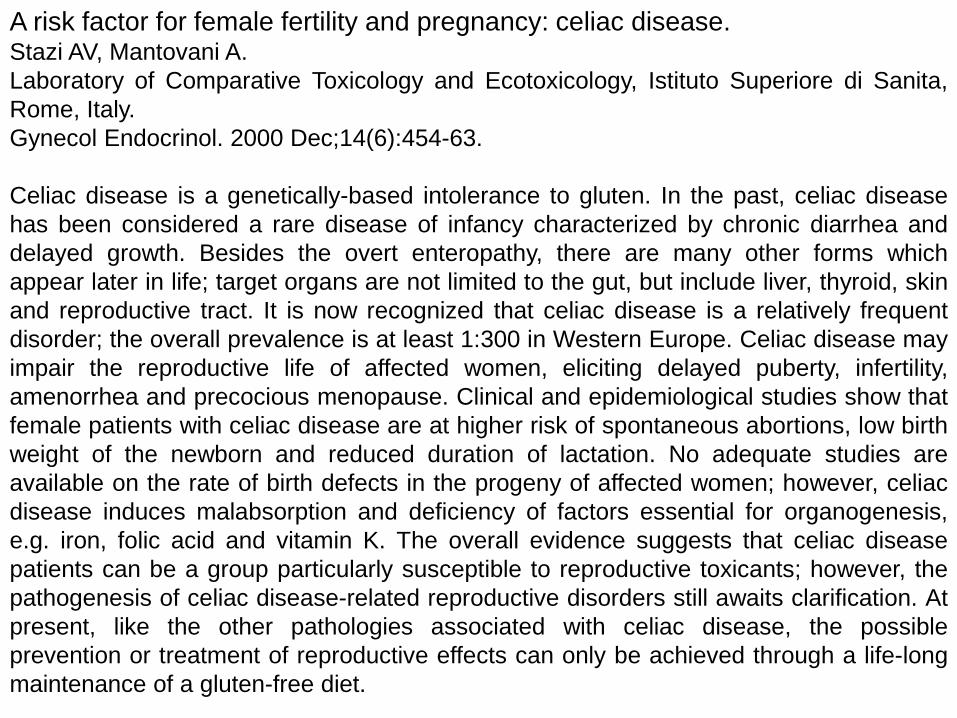
A risk factor for female fertility and pregnancy: celiac disease. Stazi AV, Mantovani A.
Laboratory of Comparative Toxicology and Ecotoxicology, Istituto Superiore di Sanita,
Rome, Italy.
Gynecol Endocrinol. 2000 Dec;14(6):454-63.
Celiac disease is a genetically-based intolerance to gluten. In the past, celiac disease
has been considered a rare disease of infancy characterized by chronic diarrhea and
delayed growth. Besides the overt enteropathy, there are many other forms which
appear later in life; target organs are not limited to the gut, but include liver, thyroid, skin
and reproductive tract. It is now recognized that celiac disease is a relatively frequent
disorder; the overall prevalence is at least 1:300 in Western Europe. Celiac disease may
impair the reproductive life of affected women, eliciting delayed puberty, infertility,
amenorrhea and precocious menopause. Clinical and epidemiological studies show that
female patients with celiac disease are at higher risk of spontaneous abortions, low birth
weight of the newborn and reduced duration of lactation. No adequate studies are
available on the rate of birth defects in the progeny of affected women; however, celiac
disease induces malabsorption and deficiency of factors essential for organogenesis,
e.g. iron, folic acid and vitamin K. The overall evidence suggests that celiac disease
patients can be a group particularly susceptible to reproductive toxicants; however, the
pathogenesis of celiac disease-related reproductive disorders still awaits clarification. At
present, like the other pathologies associated with celiac disease, the possible
prevention or treatment of reproductive effects can only be achieved through a life-long
maintenance of a gluten-free diet.
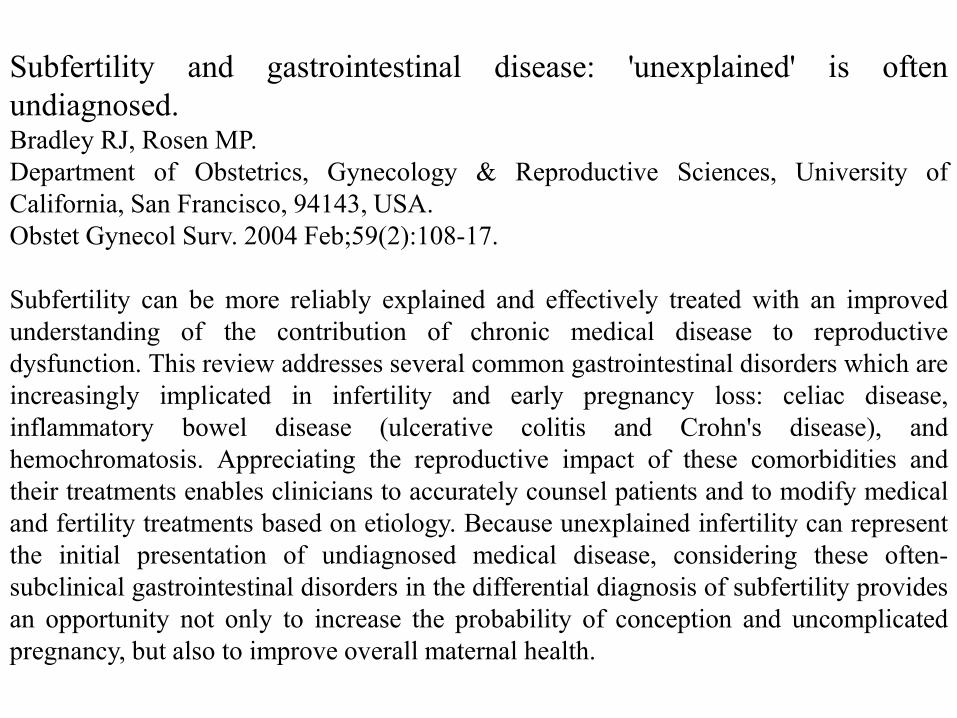
Subfertility and gastrointestinal disease: 'unexplained' is often
undiagnosed. Bradley RJ, Rosen MP.
Department of Obstetrics, Gynecology & Reproductive Sciences, University of
California, San Francisco, 94143, USA.
Obstet Gynecol Surv. 2004 Feb;59(2):108-17.
Subfertility can be more reliably explained and effectively treated with an improved
understanding of the contribution of chronic medical disease to reproductive
dysfunction. This review addresses several common gastrointestinal disorders which are
increasingly implicated in infertility and early pregnancy loss: celiac disease,
inflammatory bowel disease (ulcerative colitis and Crohn's disease), and
hemochromatosis. Appreciating the reproductive impact of these comorbidities and
their treatments enables clinicians to accurately counsel patients and to modify medical
and fertility treatments based on etiology. Because unexplained infertility can represent
the initial presentation of undiagnosed medical disease, considering these often-
subclinical gastrointestinal disorders in the differential diagnosis of subfertility provides
an opportunity not only to increase the probability of conception and uncomplicated
pregnancy, but also to improve overall maternal health.
Coeliac disease and reproductive disorders: a neglected association.
Rostami K, Steegers EA, Wong WY, Braat DD, Steegers-Theunissen RP.
Department of Internal Medicine, TwenteBorg Hospital, Almelo, The
Netherlands.
Eur J Obstet Gynecol Reprod Biol. 2001 Jun;96(2):146-9.
Coeliac disease is a chronic disease caused by a permanent intolerance to
ingested gluten resulting in immunologically mediated inflammatory
damage of the small-intestinal mucosa. The wide spectrum of clinical
symptoms is partly due to the malnourished state caused by the
malabsorption of macro- and micronutrients. Fertility problems, sexual
dysfunction and obstetrical complications are more frequently observed
in patients with coeliac disease. These reproductive disorders may be a
consequence of the endocrine derangements caused by selective nutrient
deficiencies. Nowadays, the early diagnosis and treatment of coeliac
disease is possible and not very costly. Therefore, coeliac disease must
be seriously considered in the preconceptional screening and treatment of
patients with reproductive disorders.
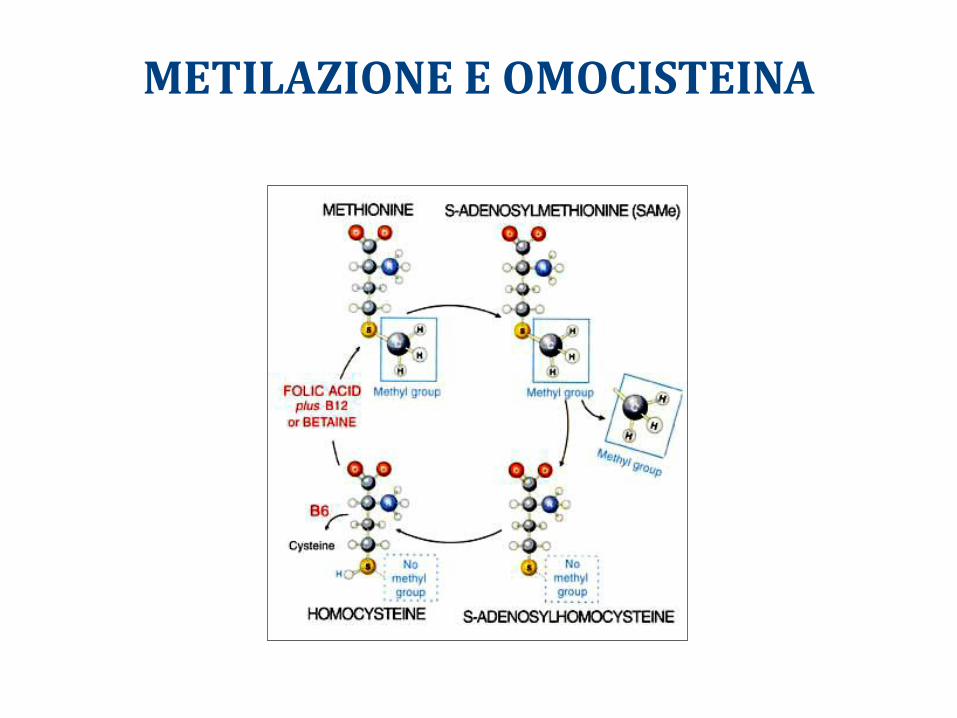
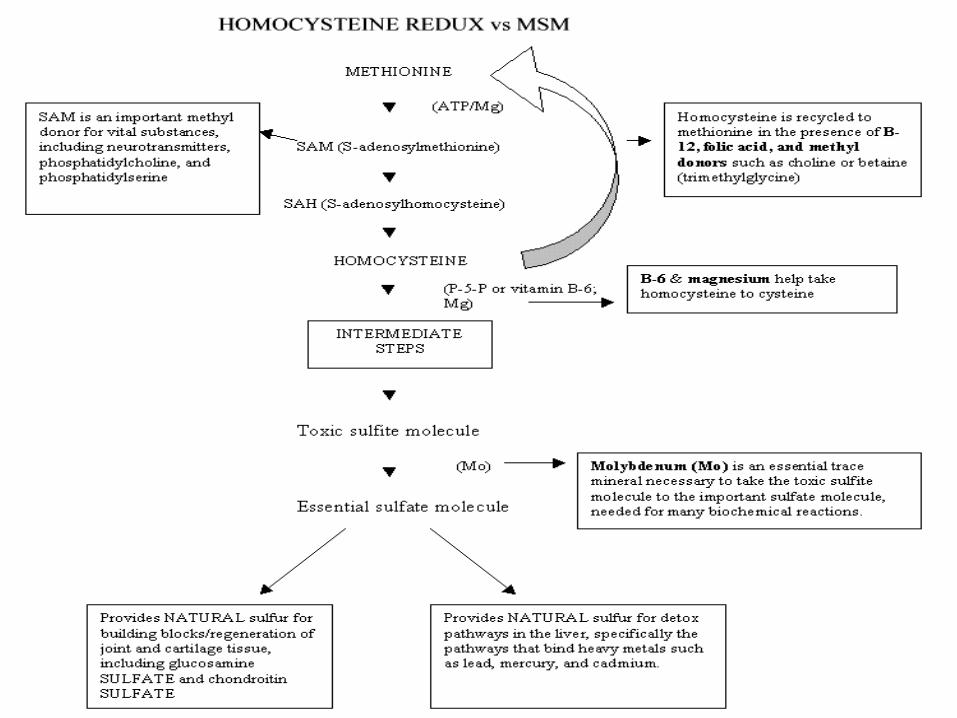
METILAZIONE E OMOCISTEINA
Plasma homocysteine levels correlated to interactions between folate status and
methylene tetrahydrofolate reductase gene mutation in women with unexplained
recurrent pregnancy loss. Kumar KS, Govindaiah V, Naushad SE, Devi RR, Jyothy A.
Institute of Genetics, Hyderabad, India. [email protected]
J Obstet Gynaecol. 2003 Jan;23(1):55-8.
Hyperhomocysteinaemia, a risk factor for recurrent pregnancy loss, is related either to a hereditary
defect within the methionine-homocysteine pathway or it might be acquired as a result of
deficiencies of vitamin B(12) and folate (B(9)). Because hyperhomocysteinaemia seems to be
determined by both genetic and environmental factors, the current study was undertaken to find out
the interactions between folate status and MTHFR mutation on the homocysteine concentration in
24 women experiencing unexplained three or more consecutive recurrent pregnancy losses. The
median fasting total plasma homocysteine concentration in the study group was 10.23 micro mol/l
compared to 8.95 micro mol/l; P = 0.096 in the controls. Elevated homocysteine levels > 18 micro
mol/l, which was considered to be a risk factor for recurrent early pregnancy loss, was found in four
women in the study group and none among the controls. Lower red cell folate levels (normal range
>/= 160 ng/ml) were observed in nine (37.5%) women among the study group, compared to five
(20.84%) women among controls. The mean +/- SD red cell folate levels in the study group was
found to be 154.37 +/- 37.07, while in the controls it was 159.0 +/- 28.97. In the present study six
women in the study group and two among controls were found to be carriers for the C677T MTHFR
mutation. None were homozygous for the mutant (TT) allele. The highest values of homocysteine
concentration were found in women experiencing recurrent pregnancy loss with both the CT
genotype and folate deficiency. Identification of hyperhomocysteinaemia in women with recurrent
pregnancy loss may help in therapeutic normalisation and might permit a normal birth.
The C677T polymorphism of the methylenetetrahydrofolate reductase gene and
idiopathic recurrent miscarriage. Unfried G, Griesmacher A, Weismuller W, Nagele F, Huber JC, Tempfer CB.
Department of Gynecologic Endocrinology and Reproductive Medicine, University of Vienna School
of Medicine, Vienna, Austria.
Obstet Gynecol. 2002 Apr;99(4):614-9.
OBJECTIVE:To investigate the association between the C677T polymorphism of the 5,10-
methylenetetrahydrofolate reductase gene (MTHFR), serum homocysteine levels, and idiopathic
recurrent miscarriage in a Middle-European white population.METHODS:In a case control study, we
investigated 133 women with a history of three or more consecutive pregnancy losses before 20
weeks' gestation and 74 healthy controls with at least two live births and no history of pregnancy
loss. A DNA extraction and polymerase chain reaction followed by restriction fragment length
polymorphism analysis were used to genotype women for the presence of the MTHFR C677T
polymorphism. Serum homocysteine levels were assessed by a fluorescence polarization
immunoassay.RESULTS:The MTHFR allele frequencies in women with idiopathic recurrent
miscarriage and controls were 34.6% and 21.6%, respectively, for the T allele (mutant) and 65.4%
and 78.4%, respectively, for the C allele (wild type) (P =.007, odds ratio 1.9, 95% confidence
interval 1.2, 3.1). The MTHFR genotype frequencies in women with idiopathic recurrent miscarriage
and controls were: 17.3% (T/T), 34.6% (C/T), 48.1% (C/C) and 5.4% (T/T), 32.4% (C/T), 62.2%
(C/C), respectively (P =.03, odds ratio 3.7, 95% confidence interval 1.2, 11.8 [T/T versus C/T and
C/C]). Serum concentrations of homocysteine were significantly higher in carriers of a MTHFR
mutant allele compared with women with no mutant allele (mean 7.4 +/- 2.4 micromol/L [T/T + C/T]
versus 6.5 +/- 2.6 micromol/L [C/C], P =.05).CONCLUSION:Carriage of the mutant allele of the
MTHFR C677T polymorphism is associated with elevated serum levels of homocysteine and
idiopathic recurrent miscarriage.
Hyperhomocysteinemia and recurrent early pregnancy loss: a meta-
analysis. Nelen WL, Blom HJ, Steegers EA, den Heijer M, Eskes TK.
Department of Obstetrics and Gynecology, Nijmegen, The Netherlands.
Fertil Steril. 2000 Dec;74(6):1196-9.
OBJECTIVE: To quantify the risk of recurrent early pregnancy loss in the presence of elevated
fasting or afterload homocysteine concentrations or homozygosity for the 677C-->T mutation in the
methylenetetrahydrofolate reductase (MTHFR) gene (T/T genotype). DESIGN: Case-control studies
published between January 1992 and November 1999 were identified with a MEDLINE-search.
These studies were combined with a recent case-control study performed by our own research
group. SETTING: Academic research environment. PATIENT(S): Studies published in the English
language, concerning two or more pregnancy losses before 16 weeks' menstrual age were
included. INTERVENTION(S): Meta-analysis of all of the studies included. MAIN OUTCOME
MEASURE(S): The number of subjects with and without hyperhomocysteinemia or with the T/T
genotype were derived, if necessary the study was supplemented by personal communication with
the original authors. RESULT(S): Pooled risk estimates of 2.7 (1.4 to 5.2) and 4.2 (2.0 to 8.8) were
calculated for fasting and afterload plasma homocysteine concentrations, respectively. For the
MTHFR T/T genotype a pooled risk estimate of 1.4 (1.0 to 2.0) was found. CONCLUSION(S):
These data support hyperhomocysteinemia as a risk factor for recurrent early pregnancy loss.
Further research should be focused on the pathophysiology of this relationship and on the clinical
efficacy of B vitamin supplementation.