-
1-3
4-10
11-17
18-24
25-34
35-39
40-42
ANA 43-44
45-46
47-52
() 53-62
() 63-67
() 68-78
() 79-82
() 83-85
-
() 86-87
() 88-90
() 91-94
() 95-98
()
(1) 99-100
(2) 101-103
(3) 104-106
(4) 107-109
(5) 110-112
(6) 113-115
(7) 116-117
118-129
130-137
138-141
142-146
147-150
151-154
-
155-169
C 170-173
174-179
180-183
184-186
187-189
190-196
197-202
203-204
205-207
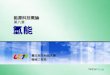
208-208
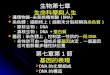
217-219
220-222
223-238
239-240
241-249
250-257
258-260
-
261-262
263-265
? 266-267
268-275
276-278
279-281
282-283
284-286
287-288
289-290
91 05 25
93 01 10
94 03 01
-
Editors
Contributors
(Chapter 11)
(Chapter 37,38,40)
(Chapter 6,20)
(Chapter 4,5)
(Chapter 14,16)
(Chapter 15)
(Chapter 17)
(Chapter 12)
(Chapter 32,43)
(Chapter 41,42)
(Chapter 39)
(Chapter 36,44,45)
-
1
20
4
(1)IFA assay: FIAX ANA fluorometer Fluorecent microscope
-
2
Inverted fluorecent microscope (2)ELISA: Reader Washer ELISA
fully automation Sample handling system (3)FEIA system: Auto CAP
system (4)DNA screening: PCR machine EP equipment Image system
Incubator-shaker UV cross-linker Sequence equipment
(5)Microcytotoxicity assay: Inverted microscope Seradot HLA
analyzer (6)Flow cytometry (7)Nephelometry Behring BN II Beckman
Image (8)Coagulation system ACL system (9)Polarized microscope
(10)Pulmonary function test machine (11)Capillary microscope (12)
Protein EP&IFE system Sebia hydrasys and hyrys system (13)West
blotting equipment
-
3
(14)Cell culture system Laminar flow CO2 incubator Autoclave
Oven(200C) (15)Ultrahighspeed centrifuge (16)Highspeed centrifuge
(17)Refrigerated centrifuge (18)Cytospin (19)Spectrophotometer
(20)PH meter (21)(ddH2O)
-
- 4 -
.
.
.
.
.
. C
.
.
.
.
,
-
- 5 -
C
:
:
:
ANA pattern recognition
HLA typing
Capillary microscope
-
- 6 -
1. Rheumatological medicine. Dieppe et al.
2. Textebook of rheumatology (Kelly, Harris, Ruddy, Sledge)
,,
7:30-8:00
19:00-21:30
14:00
18:00-19:30
8:00-12:30
9:00-10:00
*
16:00-17:30
14:30-16:00
,
,
9:00-10:00
16:00-17:30
14:30-16:30
-
- 7 -
()
Ex
cellent
Good
Fair
SLE
RA
5
: Excellent Good Fair Poor :
-
- 8 -
()
Ex
cellent
Good
Fair
DMARDs
Capillary
microscopy
SLE
RA
5
: Excellent Good Fair Poor :
-
- 9 -
Ex
cellent
Good
Fair
X
ANA
Topic:
Journal:
Accepted or
published.
: Excellent Good Fair Poor :
:
-
- 10 -
Ex
cellent
Good
Fair
CT/MRI
ANA
Topic:
Journal:
Accepted or
published.
: Excellent Good Fair Poor :
:
-
11
1. ,,, , team: 20G, 1086G, 1219C, 1034A, 961F 892J
2. , ; take over, ; take over, .
3. : 1) progression notes 2) 3): PS: scheduled MTP pulse
therapy, ES: Evaluation, B: Biopsy, RBx: Renal biopsy, LBx: Liver
biopsy, SBx: Skin biopsy, F: Fresh case; , ()
4. W62 bedside image
5. //
Lupus nephritis 24 hours urine protein WBC/Hb/Platelet
6. / sign on. 7. Cellcept, Ciclosporin,
Ribavirin/ Interferon 8. call 1. Admission note
2. Progression Note
-
12
Admission note Progression, accept ion note/progression note
cosign
3. Methylprednisolone (MTP) pulse therapyactive synovitis, skin
rash, positive SI tests positive findings, MTP pulse, C.C admitted
for MTP pulse
4. Special Chart
5. Progression Note SOAP 6. procedures: Arthrocentesis,
Intraarticular injection, Tendon
injection, Lumbar puncture, CVP insertion, Effusion
aspiration/tapping, Procedure Note Cell count, Sugar, Protein, ANA,
Gram stain, Acid Fast Stain, KOH, Indian inkinterpretation (ex.
Class I inflammatory synovial fluid)
7. Antibiotics, Anti-TB/Fungus agents, DMARDs: MTP, Endoxan,
Imuran, Dapsone, Ciclosporin, Cellcept; high dose Prednisolone
IndicationsProgression note TPR chart
8. diagnosis, ( antibiotics, HRCT of lung interstitial lung
disease, Renal biopsy lupus nephritis)
9. primary care case , assign primary care case, ,
10. primary care case complaint ( CPR), ,, , ,
procedure,
-
13
1. underlying disease activity , fever antibiotics,
immunosuppressants, , fever bedside , evaluation: CXR, Urine
routine/culture, Blood culture, Sputum Gram stain , , (ex.
Pneumonia, UTI, or Biliary tree infection, or Cellulitis) , TPR
chart
2. SLE sulfa drugs flare up, Norcardia, Salmonella, Pneumocystic
carinii Baktar/Bactrim sulfa drugs
3. iv form NSAID (ex Ketoprofen, Profenid) 4. prednisolone or
DMARDs: Salazopyrin, Plaquenil, Imuran,
Endoxan, MTX, Ciclosporin, Cellcept, D-penicillamine dose
5. H2 blocker, PPI: Lansoprazole, Lipid-lowering agents:
Simvastatin (Zocor)/ Benzalip, Albumin indications progression
notes.
6. , ,
7. Trial Cellcept, Ciclosporin , CR.
8. Renal biopsy Tapal, Persantin, Coumadin , .
1. , Don't wait for result only. CNS: /, GI: /, Bone & Soft
tissue: , Abd & Kidney Sono:() ,
2. Blood culture: Betadine tincture 3, () , , fever episodes 2,
15 30 vein blood culture 10ml blood, anaerobic bottle(), aerobic
bottle, 5ml Bacterial Endocarditis case 5 blood culture, 24
persisted bacteremia
3. Gram stain: infection , sputum, synovial
-
14
fluid, abscess, pleural effusion. progression note. Sputum Gram
stain
4. CRP, Ferritin, anti-PLT Ab, Heptoglobulin, anti-HCV Ab ()
.
5. , ( Dr), combine meeting.
orders 1. OPD immunology, 2. , CBC (
MCV) ( Liver function, renal function, Na/K/Ca/Cl, Fasting blood
sugar; proteinuria or hyperlipidemia case TG/Cholesterol)
3. Routine X-ray examination Chest PA & KUB Fresh SLE ()
CBC, Urine routine, Stool OB, Whole set renal/liver function
& electrolyte ESR, RPR, PT/Mixing APTT AIR Lab: ANA, DNA Ab,
ENA, LE factor, C3/C4 or CH50() Acute phase protein IgG/IgA/IgM,
RF-IgM, Lupus anticoagulant :ACA-IgG/ACA-IgM, ACA-IgA, AB2GPI,
APTS
Lupus nephritis
Biochemistry TG/Cholesterol For renal biopsy cases: CBC &
PT/APTT Check 24 hours urine protein/CCr/Urine IEP(AIR lab) Consult
Nephro doctor for renal biopsy renal biopsy: light microscopy,
Immonofloresent(IF), Electronic microscopy , biopsy. Biopsy kidney
pathology application form Gallium renal scan(): biopsy Biopsy
urine routine x1
Lupus cystitis lupus cystitis GU, Dr
-
15
Rheumatoid arthritis
CBC, Urine routine, Stool OB, Whole set renal/liver function
& electrolyte ESR, PT/Mixing APTT AIR Lab: ANA,
RF-IgM/RF-IgA(), acute phase protein, ENA:SSA/SSB, IgG/IgA/IgM
Uncorrectable Mixing APTT lupus anticoagulant(LA)
&:ACA-IgG/ACA-IgM, ACA-IgA, AB2GPI, APTS X-ray: hands/feet
& active joint; , active joints
Spondyloarthropathy (AS, Reiter syndrome, psoriatic
arthritis,
inflammatory bowel disease) CBC, Urine routine, Stool OB, Whole
set renal/liver function & electrolyte ESR, PT/Mixing APTT AIR
Lab: Acute phase protein, RF-IgM, HLA B27R , case X-ray: KUB, T-L
spine, SI joint C-Spine ROM limitation : C-spine flexion/extension
Bone scan
Hemolytic anemia
CBC(MCVRBC/Hb/Hct, Hct x100/RBC) Reticulocyte, PT/mixing APTT,
LDH, RPR Coombs tests:Direct/Indirect () AIR Lab: ANA,
Heptoglobulin, APS profile:LA (lupus anticoagulant)
&:ACA-IgG/ACA-IgM, ACA-IgA, AB2GPI, APTS
Autoimmune hepatitis Check complete liver function profiles: PT,
GOT/GPT/AlkP/Bil(T/D), rGT, Albumin/TP AIR Lab: IgG/IgA/IgM ASMA,
AMA( AMiA,) APA; AMA positive ama-m2
Lupus Abdominal vasculitis Standing CXR, KUB,
-
16
Abdominal CT small intestine , R/O abdominal vasculitis ( iv
contrast) sucussion splash/post-prandial vomiting: GI for
UGI-scopy, (mention duodenum 2nd portion) tenesmus/watery or bloody
diarrhea: CRS or GI for Sigmoidoscopy
CNS involvement Lumbar puncture: Cell count, Glucose ( blood
sugar), Protein Gram stain/Bacterial culture(aerobic &
anaerobic) Cryptococcal Ag/Indian ink/Fungus cuture AFS/TB culture,
AIR Lab:TB PCR CSF IgG index ( 3ml blood, CSF AIR Lab) CSF ANA MRI
of Brain ( contrast), HMPAO-SPECT
1. //,
2. , 3. , CR VS, .
4. , CR VS, "" CR or VS.
5. , ; , Ditto
6. Gouty arthritis Allopurinol & Benzbromarone, 24Hrs urine
Uric Acid underexcretion type .
7. Myofascial pain NSAID, ointment ( well documented)
8. NSAID cases benzoflex muscle relaxant, . 9. URI Danzen
SLE:
S/Ss: Malaise? Fever? Hair loss? Skin rash? Arthralgia? Lab:
CBC, U/R, DNA, C3/C4 or CH50 ( 3)
RA S/Ss: Active synovitis/Deformity, Morning stiffness?
-
17
Lab: WBC, Hb, Platelet, ESR/CRP, U/R, Cr, GPT, RF-IgM/RF-IgA
(,), 2-3.
X-ray of both hand/feet Active 6 Active synovitis DMARDs,
fellows SAE: AS, Reiter's, Psoriatic arthritis
S/Ss:Buttock pain/Lumbasacral pain/Cough pain/Sneezing
pain/Inguinal pain/Neck ROM Hip internal rotation
limitation/Sausage toes/fingers, active synovitis Lab: CBC, ESR,
CRP, Cr, U/R (For NSAID nephropathy) 3 1 X-ray of KUB/SI joint (),
T-L spine (C-spine) oligo-/poly-"active synovitis over ,
seronegative RA still should be suspected" 3 RF-IgM check X-ray
F/U, miss seronegative RA.
Gouty arthritis S/Ss: acute attack ? uric acid, Cr, U/R?
benzbromarone 24hrs urine uric acid ? synovial fluid finding prove
Gouty arthritis? revise diagnosiscrystal arthritis Lab: 3 check
uric acid, Cr, U/R
-
- 18 -
(-)
() (1)
-
- 19 -
(2)
(3)"" ""
""
(4)
Reiter
() (1)
-
- 20 -
(2)
(3)
(4) LymeB C Lyme DNA B19
Lyme (5)
(6) Crohn
(hypertrophic osteoarthropathy)
(7) () hydralazineprocanamide
"statin" ( NSAIDs Gold D-penicillamine)
-
- 21 -
()
Marfan
()
()
(Health Assessment Questionnaire, HAQ)(Arthritis Impact
Meseaurement Scale)
()
-
- 22 -
()
(1)
(2) ()
(rotator cuff)
(3)
(trigger Points)(referred Pain)
(4)
(5)
-
- 23 -
(6)
() (stiffness)
(polymyalgia rheumatica)
() (swelling)
() (weakness)
() (constitutional symptoms)
38.5C
() (Raynauds phenomenon)
-
- 24 -
CREST
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. Simons,
Travell, Myofascial pain and dysfunction the trigger point
manual, 2nd Ed. Williams & Wilkins 4. , ,
-
- 25 -
Doherty GALS 3-4GALS
() GALS
GALS (Gait, Arms, Leg, Spine)
(1) (2) (3)
GALS
-
- 26 -
GALS /
,
/
-
- 27 -
() (1)()
(2)
(3) 45 45 45
60 (4) 70-80 20-30 25-35
35-45
() (1)
(2)
-
- 28 -
(2) 90
90 45 160 60
(3) 90 60 55
90 120 45 75
(4)
() (1) 50 10-15
45
(2)
-
- 29 -
(3)
150 0 5
(4) 90
() (1)
123
(2)
70 80 30 20
()
(1)
Marfan
-
- 30 -
(2)
(Dupuytren's contracture)
(3)
(ulnar deviation)
Heberden
() : (1)
60% 40% (2)
(antalgic gait)
(3)gluteus medius Trendelenburg
-
- 31 -
5-10cm
(4)
(5) 90-120
(6) 90
30-40 40-60 30-40
(7)( 10-15 )( 30-50 )( 30 )
() :
(1)
"X " "O "(hamstring)
(2)
(3)
-
- 32 -
(4)()()()
(5)
(6)
() : (1)
(2) 20 45
30 20
() : (1) (hammer toes) (hallux valgus)
(2)
-
- 33 -
(3)(MTP) Morton
() (1)
(2) 10 cm 10 cm
() (1)
(2) (3)
(4)
-
- 34 -
(5)
()
(1)
(2)
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. Simons,
Travell, Myofascial pain and dysfunction the trigger point
manual, 2nd Ed. Williams & Wilkins 4. , ,
-
- 35 -
RF 1% RF 33.1% RF 0.3%30% RF 95.5%RF 9.7%
5% 14%23% 30%
(acute phase reactant)
-
- 36 -
C(CRP)(ESR)ESR (giant cell arteritis)(polgmyalgia rheumatica)ESR
50mm/ 10%ESR ESRRSR ESRHenoch-scholein
ESRESR(Spondyloarthropathy)
(ANA)ANCAHLA (lupus anticoagulant)
DNA
-
- 37 -
(Antinuclear Antibodies) Sm
DNA 95%
Ro (SSA) CH50 Ro
(Antineutrophil cytoplasmic antibodiesANCA) ANCA Wegener
ANCAANCA (c-ANCA) (p-ANCA)c-ANCA proteinase 3 (PR3)Wegener
70%-90% p-ANCA myeloperoxidasc (MPO)
p-ANCA MPO (inflammatory bowel disease) ANCA ANCA
-
- 38 -
(Rheumatoid factor) G Fc
75%-90%
B27 (HLA-B27) HAL-B27
95%80%50%70% HAL-B27 6.5% HLA-B27 HLA-B27
(complement) CH50 (Nephelometry)
C3C4 CH50 C1C2
ANA ANA Ro(SSA) CH50
-
- 39 -
RF
: 1. Doherty M, Hazleman BL, Hutton CW, Maddison PJ, et al.
Rheumatology
Examination and Injection Techniques. (Second edition) London),
W.B. Saunders, 1999
2. Cash JM. Evaluation of the Patient. A. History and Physical
Examination. Primer on the Rheumatic Diseases. 11 edition Arthritis
Foundation (Georgia), 89-94, 1997
3. Shmering RH, Liang MH. Evaluation of the Patient. B.
Laboratory Assessment. Primer on the Rheumatic Diseases. 11
edition. Arthritis Foundation (Georgia), 94-97,1997
-
- 40 -
C
IgG Y(Fab) IgG Y IgG (Fc)
IgG IgG
-
- 41 -
()
1. : 80% 20%
2. :
15 8%
()
1. 30% 80%
2. :
()
1. C:
C80%
-
- 42 -
2. :
()
()
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. , ,
-
43
ANA
-
44
-
- 45 -
BC BC
() Blood type compatible:
O, A, B, AB A A, AB B B, AB AB AB
() HBs (+) donor recipient HBs (+), or anti-HBs (+), or
anti-HBc(+)
[HBs (+) donor cannot be given to HBs (-), anti-HBs (-),
anti-HBc (-) recipient]
() Anti-HCV (+) donor anti-HCV (+) recipients
-
- 46 -
:
UNOS
() UNOS
Level
( 0.5) 0.5
HLA
0ABDR mismatch 0BDR mismatch 0AB mismatch 1BDR mismatch 2BDR
mismatch 3BDR mismatch More mismatch
10 7 6 3 2 1 0
>=80%
-
- 47 -
,
-
- 48 -
butterfly rash of SLE acne rosacea lupus pernio lupus vulgaris
seborrheic dermatitis
discoid rash bullous LE reverse Gottron sign digital and palmar
vasculitis
.Gottron sign, Shawl sign, mechanic hand
.sclerodactyly, digital pitting, telangiectasis, calcinosis
.nail pitting, salmon patch, onycholysis
.:rheumatoid nodules
. livedo reticularis atrophy blanche purpura, palpable purpura
erythema nodosum Raynauds phenomenon (two phase, three phase)
-
- 49 -
() (Trapezius) : (Sternocleidomastoid muscle) :
(Levator scapulae muscle) : ? (Splenius capitis and splenius
cervicis) : ( Posterior cervical muscles : multifundi,
semispinalis) :
( Suboccipital muscle ) : (Temporalis muscle) : : () (Scalene
Muscles):
(Supraspinatus Muscle):
(Infraspinatus Muscle):
(Teres Minor): (Latissmus Dorsi Muscle): (Teres Major):
-
- 50 -
(Rhomboideus Muscles): .(Deltoid Muscle):
(Pectoris Major & Minor): .(Sternalis):
(Serratus Anterior, Posterior): () (Biceps brachii):
(Hand extensors):
(Quadriceps femoris):
(Hamstring muscle):
(Gastrocnemius muscle): (Soleus muscle): () (Thoracolumbar
Paraspinal Muscles) (Quadratus Lumborum) (Iliopsoas Muscle)
(Gluteus Minimus) (Gluteus Medius) (Gluteus Maximus),
(Pyriformis muscle)
() ()
-
- 51 -
Goodpastures Wegerners
()
()
(Tubulointerstitial)
(ANCA)
( NSAIDs, Gold D-penicillamine)
()
()
-
- 52 -
()
()
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. Simons,
Travell, Myofascial pain and dysfunction the trigger point
manual,
2nd Ed. Williams & Wilkins 4. Daniel J. Wallace, Bevra
Hannahs Hahn, Edmund L. Lupus Erythematosus
Dubois, Dubois' Lupus Erythematosus, Lippincott Williams &
Wilkins Publishers
5. , ,
-
- 53 -
()
( SLE) 75/100,000SLE
SLE
SLE SLE
SLE
SLE(bullous) Ro (SSA)(subacute cutaneous lupus erythematosus,
SCLE) (discoid lupus)(hypertrophy)(verrucous DLE)(lupus
profundus)SLE 30% 10% SLE
SLE SLE 20%
-
- 54 -
(Raynauds phenomenon) 30% SLE
SLE
SLE SLE SLE
Jaccoud deformity ischemic necrosis of bone avascular necrosis
SLE 4%~10%SLE SLE
X X
SLE SLE
SLE (Cushingoid syndrome) 85% SLE 45%
-
- 55 -
: 1.
Zizic prednisolone 40mg prednisolone 30mgprednisolone 20mg 5%
SLE
2.
3.
5%~11%
SLE
15%(cytoid bodies) (macular degeneration) SLE SLE(central
retinal artery occlusion)(certral retinal vein thrombosis)(optic
neuritis)(proliferative retinopathy)
-
- 56 -
SLE
SLE14~56%5~17% 14~46% SLE
6~45% 21~49% 60~83%
10% SLE (mitral valve prolapse) SLE SLELibman-Sacks
SLE
SLE
42~60%16~40% X(lupus pneumonitis) (fibrosing alveolitis)
(alveolar hemorrhage)(pulmonary embolism)(pulmonary edema):
Gallium
-
- 57 -
3gm%SLE
SLE
2~6%
8~10% SLE (pseudopyloric obstruction);(rebound pain)(board like
rigidity) X
SLE
SLE
(malabsorption) X
SLE
10~30%30%~60%
(lupoid hepatitis), (autoimmune hepatitis)
-
- 58 -
B Cm
SLE
SLE
(lupus cystitis)(hydroureter)(Hydronephrosis) X
(sacroilitis)
SLE
SLE
38%~65% SLE SLE5~16% SLE
;
(creatinine)
C3 double strand DNA
5 10 86% 75%
-
- 59 -
85%
SLE
SLE
NSAID SLE
mononeuropathy multiplexacute psychosis
SLESLE
SLE SLE
SLE
-
- 60 -
SLE
2mg/dl
SLE C3 C3 C3SS-ALupus auticoagulant
Aspirin SSARo
SLE
SLE
SLE
16% Coombs
5%(ITP) SLERo (SSA) 5 SLE
-
- 61 -
1982 , ()()()()(Smithdouble strand DNA)
SLE DR2
SLE
SLE SLE
-
- 62 -
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed.,
Saunders 2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3.
Simons, Travell, Myofascial pain and dysfunction the trigger
point
manual, 2nd Ed. Williams & Wilkins 4. Daniel J. Wallace,
Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
5. , ,
-
- 63 -
()
:
: 1 2 3 4 5
:Paracetaminophen NSAID :NSAID :NSAID
-
- 64 -
:
: nifedipine :NSAIDs : : Danazol
() : : :Propranolol
"""" () (NSAIDs)
NSAIDs Salicylate NSAIDsNSAID NSAIDs NSAIDs(corticosteroid)
NSAID NSAIDs NSAIDs
(prostaglandin) NSAIDs NSAIDs NSAID NSAIDs
-
- 65 -
NSAIDs Ibuprofen
() (Corticosteroid)
5mg prednisolone prednisolone NSAIDprednisolone
methylprednisolone :
prednisolone prednisolone Methylprednisolone
-
- 66 -
() (Antimalarials)
() (Immunosuppressive drugs)
Chlorambucil cyclophosphamide Azathioprine
cyclophosphamide1.0~4.0mg/kg/day 0.5~1.0gm/m2 60 24 Chlorambucil
0.1~0.2mg/kgAzathioprine 1.0~4.0mg/kg
-
- 67 -
() (Plasma exchange)
40ml/kg5%
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. Daniel J.
Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
4. , ,
-
- 68 -
()
SLE
24 C3DAN
-
- 69 -
585%
BBTBDNADNA (in situ formation)
WHOWHO
1. ()
2. ()
-
- 70 -
3. ()()
(cresecents)(fibrinoid necrosis) (pyknosis)( karyorrhexis )
(wire loop)(hyaline thrombi) (hematoxylin bodies) (LE body)
LE
(membranoproliferative)
4. ()
IgGIgAIgM IgG C3C4C1q properdin C1q
-
- 71 -
(fibrin) (fibrinogen)
(tubuloreticular inclusions)
(tubulointerstitial)
CD8
(noninflammatory necrotizing vasculopathy)(thrombotic
microangiopathy)(necrotizing vasculitis)
(activity and chronicity index)
03+024(endocapillary proliferation)(fibrinoid necrosis)
-
- 72 -
(karyorrhexis) ( cellular crescent)(interstitial|inflammation)2
03+ 0 12(glomerulosclerosis)(fibrous crescents)(tubular
atrophy)(interstitial fibrosis) 124
WHO
: (1) WHOWHO
(2) WHO
: (1) WHOWHOWHO
(2) WHOWHOWHO
-
- 73 -
(1)
(2)
(3)
(4) (5)
(6) (7)
1.
2.
3.
GFR 4.
-
- 74 -
GFR
5.
GFR
1. ()
2. ()
3. ()
cyclophosphamide azathioprine prednisolone cyclophophamide NIH
methylprednisolone cyclophosphamide () cyclophosphamide
cyclophosphamide () prednisolone methylprednisolone (creatinine
)25% cyclophosphamide 25% cyclophosphamide 10%
-
- 75 -
cyclophosphamide cyclophosphamide 24
4. ()
ciclosporine
double strand DNA C3C4 DNA C3C4 24C
SLESLE 1/4
-
- 76 -
SLE
2mg/dl
prednisolone15mg
Azathioprineciclosporinecyclophosphamide
40012
14
-
- 77 -
1.
2.
3.
1. 461-466
2. Wallace DJ, Dubois: Dubois lupus erythematosus, 3rd ed.
Philadelphia: Lea and Febigrer, 1997
-
- 78 -
WHO ()
A. B.
WHO
I.() II. A. / B. /
III. A. B. C.
IV. A. B. C. D.
V. A. B.IIaIIb
VI.
-
- 79 -
()
23
HMPAO
HMPAO
SLE
NSAID SLE
mononeuropathy multiplexacute psychosis
(cognition dysfunction)
-
- 80 -
(
) NSAIDs
1. 2 6
2.
3. PET(positron emission tomography)
PETHMPAO SPECT (single-photon-emission computed tomography)
1.
-
- 81 -
2. SLE
3. SLE
CSF IgG index 4. HMPAO
5. MRI
6. PET
cyclophosphamide, azathioprine, cyclosporine , Aspirin,
(transverse myelopathy)(mononeuropathy multiplex) acute
inflammatory demyelinating polyneuropathyAIDP, chronic inflammatory
demyelinating polyneuropathyCIDP
cyclophosphamide
-
- 82 -
1. (hydroxychloroquine)
2. DHEA 3. 4.
5.
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 83 -
()
azathioprine
-
- 84 -
(migratory pain)
succussion splash
(pseudopyloric obstruction)
peritoneal sign
X
(Double contrast
Abdominal CT scan)
-
- 85 -
""
cyclophosphamide
(Endoxan)
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 86 -
()
76
DNA
hydralazine()procanamide()methyldopa()isoniazide()chloropromazine()D-penicillamine()
1. 2. 60( 86)
-
- 87 -
3. 4. 5.
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 88 -
()
1 : 9
1.
2.
LH, FSH
3.
-
- 89 -
4.
1.
2.
3.
(Plaquenil)
-
- 90 -
4. (Endoxan)
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 91 -
()
SSA 45%SSB 15%98% SSA SSB SSA SSB 6 8
20% 3%-5%
SSA SSBSSA SSB 40%
()
-
- 92 -
() :
()
() ()
() (AV block)
18 24
30 82% 30 18% SSA SSB
20% SSA SSB
SSASSB SSA 60KDa 52KDa SSA 48KDa
-
- 93 -
? SSA 52KDa SSB 48KDa
SSA/SSB
SS(Sjogren Syndrome) SSASSB SSA SSB
: 1. SSA 52KDa SSB 48KDa
2. 1820212223 24 24
:
1.
2. Dexamethasore 4mg
3. 4.
-
- 94 -
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 95 -
()
minocycline() (Drug-induced lupus) 1951 hydralazine
hydralazine () procanamide () methyldopa ()isoniazid
()chlorpromazine ()D-penicillamine () 90% 9%99% 1%
1.
-
- 96 -
hydralazineprocanamidemethyldopaD-penicillamine
2. isoniazid (INH)chlorpromazine (Thorazine)
sulfasalazineQuinidineCarbamazepine ()griseofulvin
()(minocycline)
3. (phenytointrimethadioneprimidoneethosuximide) (captopril ,
prazosin) (propylthiouracilmethimazole)
(practololacebutololatenolollabetalol) (mevacorlopidpravachol)
1. 2. 60 30
3.
hydrazine procanamide quinidine minocyclineminocycline
methyldopa
-
- 97 -
: IgG(H2A-H2B)-DNA
hydralazinequinidine minocycline
1.
2.
3. 4. IgG(H2A-H2B)-DNA
:
1. 2.
3.
:
-
- 98 -
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 99 -
() (1)
1. :
(1) (2) (3) (progesterone)(progesterone)
(1)
2.
3. ()
: 1960
-
- 100 -
(tartrazine)
(estrogen)(ethinyl estradiol) 35(progestogens)
(1) (2) (3) (4) (5) (6) (7) (8)
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 101 -
() (2)
1: 9
: 1.:
2.: (Endoxan) 24 20%-50% 30 80%
-
- 102 -
3.:
: 1. (mg%) 80%
2. 3.
4.
1. 2. :
heparin Aspirin
3. SSA/SSB Ro/La
Dexamethasone
-
- 103 -
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 104 -
() (3)
2~6
()
: 1. : 2. :
-
- 105 -
3. :()
4. :
15~30 1~2 5
(Dental floss)(Dental tape)(Rubber tips)(interproximal) 3
25%
!
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus,
Lippincott
-
- 106 -
Williams & Wilkins Publishers 2. , ,
-
- 107 -
() (4)
1992 Petri
21%31%(cephalosporin)57% 14% 2.6 1.8
1976 Gold man IgE1985 73% 37%SLE
? 1989 WHO ()
-
- 108 -
ciprofloxacin
40%
Amoxicillinampicillin
1.
2.
3.
-
- 109 -
4. 2 Amoxicilin 4-6
5.
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 110 -
() (5)
2714
X
10-15%
-
- 111 -
80% 1.
2. 3. 4. 5.
X
X
1.
2.
-
- 112 -
1. 2. 3. 4. 5. 6. 7.
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 113 -
() (6)
---(premature atherosclerosis)
5 30% 40%
15-30
1.
-
- 114 -
35 2.
(HDL-C) A1(APO-A1) 1
3.
10 prednisolone
4. 5.
6. 7. (homocystine) 8.
35
-
- 115 -
1. 2.
3. (hydroxychloroquine)
4.
5. B12B6
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 116 -
() (7)
-
- 117 -
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 118 -
(antiphospholipid syndrome)
12 HLA HLA
-
- 119 -
()
(1)
(prostacyclinPGI 2)
A2 (thromboxane A2) A2
III (antithrombin III) (thrombomodulin) (2)2GP1
2 1 (2GP1)
2 1 (3)
1 (placental anticoagulant 1)
1
()
(1)
-
- 120 -
30% 70%
(2)(thrombosis)
(3)
(Budd-Chiari )
(4)
(5)
-
- 121 -
(6) (catastrophic antibody syndrome)
()
(7)
(Libman-Sachs)
() 1988 Asherson 1989 Alarcon-Segovia 1998
1952 Moore SLE
FeinsteinRapaport
Harris
-
- 122 -
(cardiolipin) ELISA
1990 2 1 (2 GP1)2 GP12 GP1
(heparin) () (BFP-STS) VDRL
5% - 19%
() (lupus anticoagulant) 1972 Feinstein Rapaport
IgG IgM
(APTT) (KCT) (RVVT) KCT
2 GP1 C S () (antiphospholipid antibody) (anticardiolipin
antibody)
ELISA IgGIgAIgM
-
- 123 -
2 GP1X ELISA 2 GP1
1. 2.
3. 4.
5 Lediden C S III
(dysfibrinogenemia) Burger
-
- 124 -
1.
warfarin INR
2. 75heparin
warfarin 3.
dapsone dapsone 4.
-
- 125 -
1.Harris EN, Baguley E, Asherson RA, Hughes GRV. Clinical
and
serological features of the antiphospholipid syndrome (APS).Br J
Rheumatol, 1987,26:19
2.Bick RL. The antiphospholipid thrombosis( APL-T) syndromes
Characteristics and recommendations for classification and
treatment. Am J Clin Pathol, 1991,96:424
3.Asherson RA, Cervera R. Antiphospholipid antibodies and the
heart: Lessons and pitfalls for the cardiology, Circulation.
1991,84:920
4.Asherson RA ,Cervera R. Primary, 'Secondary' and other
variants of the antiphospholipid syndrome. Lupus, 1994,3:293
5.Hinton RC. Neurological Syndrome associated with
antiphospholipid antibodies. Semin thromb Hemost, 1994,20(1):46
6.Cervera R, Asherson RA, Lie JT. Clinicopathologic correlations
of the antiphospholipid syndrome. Semin Arthritis Rheum,
1995,24(5):262
7.Lockshin MD. Answers to the antiphospholipid antibody
syndrome. N Eng J Med. 1995,332:1025
8.Donato Alarcon-Segovia, Cabral A R. The
antiphospholipid/cofactor syndrome. J Rheumatol.
1996,23:1319-1321
9.Harris EN, Pierangeliss, Birch D. Anticardiolipin wet workshop
report: 5th International Symposium on Antiphospholipid Antibodies.
Am J Clin Pathol. 1994,101:616-624
10.Khamashta MA, Cuadrado MJ, Mujic F, et al. The management of
thrombosis in the antiphospholipid-antibody syndrome. N Engl J Med
1995,332:993-997
11.Khamashita MA : Hughs Syndrome Antiphospholipid Syndrome.
London : Springer-Verlag London Limited, 2000
-
- 126 -
. (1998Asherson) 1.
2. 3. 4.
1. IgG APL(/) 2. IgM APL(/) 3.
1. 1 1 2. APL 3. 5 SLE
-
- 127 -
. (1989Alarcon-Segovia)
(-) 1. 2. 3. 4. 5. 6. 7.
()(IgG IgM>5 SD)
(IgG IgM2-5 SD)
-
- 128 -
.SAPORO(1998)
1. 2. 3.
1.
2. 34
3.
(Anticardiolipin Ab) (aCL)
1.IgG/ IgM aCL
( ELISA2 -I)
1.
-
- 129 -
2.Activated partial thromboplastin timeKaolin clotting time,
diluted Russel Viper venom time
3.
4.
5.
-
- 130 -
(Rheumatoid Arthritis, RA)
(DMARDs)
(RA)
EBRetrovirus, parvovirus rubella
(molecular mimicry)
(superantigen) HLA-DR T
-
- 131 -
()
10
()
PIPMCP
Baker's 12
Swan-neck deformity, PIP hyperextensionDIP hyperflexion
Boutonniere deformity, PIP flexion DIP extensionZ deformity Radial
deviation ulnar deviation. phalanges palmar subluxationMallet
deformity, DIP flexion hallux valgus lateral deviation dorsal
subluxation
()
1. (Rheumatoid nodule)
extensor surface 20 30
2.
-
- 132 -
3.
4.
5.
Amyloidosis 6.
( 1987 ) 1. 2. 3. 4. 5. 6. 7. X
1990
-
- 133 -
():
88.9% 93.3% 1. 15 2. (
) 3.
4. 5. 6. X
()
1. : IgG IgG IgG
C
71%
2. :
-
- 134 -
1:160
3. : IgG 40%
4. HLA: HLA-DR4(040104050406) HLA-DR4 HLA-B27
5. :
6. 2003
C 2mg/dl HLA-DR4
-
- 135 -
()()()
()()
()
()
1.
COX2
2.
prednisolone 7.5mg
-
- 136 -
7.5mg
4. Hydroxychloroquine
(SulfasalazineMethotrexateMTXAvaraLeflunamide
ACyclosporin A
5.
Enbrel
(DMARDs) 1 3 2 3 4 40mm C 1.0 mg /dl
-
- 137 -
()
()
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. Simons,
Travell, Myofascial pain and dysfunction the trigger point
manual, 2nd Ed. Williams & Wilkins 4. , ,
-
- 138 -
(Progressive Systemic Scleroderma, PSS)
(Scleroderma)
30-50 3-4
;
()
(1):
-
- 139 -
(2):
(3):
(4):
()
(1):
(2)
(3)
-
- 140 -
(4)
1.:
-70 (Scl-70 antibody) (Nucleolar
antibody)(Centromere)
2. : (Capillary
microscopy)
( D-penicillamin,
Cyclosoporin )
():
PPI
-
- 141 -
(): (Acute fibrosing alveolitis)
(Interstitial lung disease)
1. Daniel J. Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
2. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4. , ,
-
- 142 -
, 2-3:1, 10-15 45-55
....
(anti-SRP)(antisynthetase), picornavirus, coxackievirus 131,
encephalomyocarditis virus-221A
()
IgGIgMC3C56-C9
Arahata Engel
B
-
- 143 -
perifascicular atrophy
,
(endomysial infiltration),
T B, CD8+T,
CD4+T B
()
1)
2)
3)
4)
5)
,
,
-
- 144 -
--Gottron
--(Heliotropes rash)(V-sign )(Shawal sign)(Mechanics
hand)(Periungal erythema)(dilated capillary loops)....
(subcutaneous calcification)
8%
(Amyotrtophic dermatomyositis)
(GOTCPKLDHAldolase) CPK 34
56
triad 1) increased insertional activity, fibrillations, and
sharpe positive waves; 2) spontaneous, bizarre, high-frequency
discharges
; 3) polyphasic motor-unit potentials
-
- 145 -
of low amplitude and short duration
Anti-Jo-1 20% aminoacyl-tRNA synthetaseanti-Jo-1 histidyl-tRNA
synthetase(anti-PL-7anti-PL12amti-EJantiOJ) Anti-Jo-1
anti-Jo-1ANAAnti-SRP (signal recogniton particle)
5 30%Anti-Mi-2 510%
Anti-PM-Scl Anti-Mi-2 (5 95%) Anti-PM-Scl (5 95%)
IgGIgM Ig
C SLE
prednisolone, 1-1.5mg/kg/day 1-1.5mg/kg/day()
azathioprine, methotrexate, cyclophosphamide,
cyclosporine,cellcecpt, chlorambucilHydroxychloroquine
3(methylprednisolone) 15mg/kg/mg
(750-1000mg/day)(IVIG(plasmapheresis)
-
- 146 -
-
- 147 -
(Raynauds Phenomenon)
?
15-40;
()
-
- 148 -
: () () ()
?
()
: 1. 2. 3.
4. 5. 6. 7. 8.
9.
10. 11. 12.
-
- 149 -
13. 14. 15. 16.
()
1. 2. 3. ok
4. 5.
6. 7.
8.
()
()
(calcium channel blocker)(nitrate)
-
- 150 -
()
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. , ,
-
- 151 -
(mixed connective tissue disease, MCTD)
(RNP)
8 15
()Raynaud phenomenon
scleroderma ()Swollen fingers/toes/hands/feet
/(sausage finger/toe)()
() SLE RA
()
-
- 152 -
10-20%
()
Scleroderma (DLCO )MCTD
() Scleroderma 65%
() 20% 10-30%
()
SLE ()
MCTD 25%U1-RNP
scleroderma SLE
()Skin and mucous membrane sclerderma SLE(typical malar rash or
discoid rash)(periungal erythema)
Achilles
-
- 153 -
() 75% 60% Coombs test
SLE
overlap syndrome
() CBC/DCESRCRPCPKAldolase
() ANAENA (SSA/SSB/RNP/SM) U1 RNP
() XEMG/NCVcapillary microscopy
steroid
(SLE scleroderma RA) ()
90.5 % 82.1%
( 35%)
-
- 154 -
1. , , , 2002; 50:376-380 2. Kelly, Harris, Ruddy, Sledege,
Textbook of Rheymatology, 5th Ed.,
Saunders 3. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 4.
Simons, Travell, Myofascial pain and dysfunction the trigger
point
manual, 2nd Ed. Williams & Wilkins 5. , ,
-
- 155 -
(Behets Disease)
1937 Behcet(Behcets disease)(Behcets
syndrome)(ocular-oral-genital syndrome)
""
80-370/10 13.5-20/10 14/10 0.12-0.33/10
1992 30.5/10 9.9/10 3
1982 310 89%
30 40
-
- 156 -
65%
()
HLA-B5 B51 HLA-B51 72%, 26% HLA-B51 57% 12% 53.3% HLA-B51 10.9%
HLA HLA B51 81% 13%HLA B51 HLA-B51
()
1. : EB
Cparvovirus B19
2. :
heat shock protein 3. :
-
- 157 -
1950
() :
1. : 60%
2. :
C9 CH50 C3 (A) T :
T
(B) : :1; 2
; 3 3. :
PGI2
-
- 158 -
()
()
()
()
-
- 159 -
()
24-482-10cm 1-2
() 70%24-48
1-3
()
60-80%
1. :
6
-
- 160 -
5
2. :
4
3. :
4. :
5. :
(parthergy reaction)
(A) :
-
- 161 -
(B) :
(C) :
48 ; 48 62.2% 4% 0 75% 10%HLA-B51
:1 48 ; 2; 3
()
1/3 2/3
-
- 162 -
()
(neuro-Behcets disease) 30% : 1; 2 1-3 ; 3; 4
; 5 ;
()
(vasculo-Behcets disease, angio-Behcets disease) 10-37%
()
-
- 163 -
()
C 2
VIII
ENA X
CT
1987 ()
-
- 164 -
1987 1.
(1) (2)
(3) (4)
2. (1) (2) (3) (4) (5)
3. (1) (2) 3 2 2
2 (3)
(4) 4.
(1) (2) CRP
(3) HLA-B51
-
- 165 -
1. 1 3
2.
3. ()
4. ()
5. 20 24-48
4 2 ()()
()
Tsank
()
HLA-B27 HLA-B51
() (Reiters syndrome)
-
- 166 -
;
() (sarcoidosis)
X
() (inflammatory bowel disease)
()
-
- 167 -
(80mg/)
() 3-4
()
1.
prednisolone 30-60mg 1 3 prednisolone 60-100mg/ 10-15mg/
Prednisolone 10-60mg/ Prednisolone
-
- 168 -
2.
3. (chlorambucil)
50-100mg/ 2-4mg/ 4
4. A (cyclosporine A):
(chlorambucil) A A 3-5mg/kg 2
5. (cyclophosphamide)
cyclophosphamide
A 1g/m2
6. FK506 A FK506
7. : levamisoleD-penicillamine
-
- 169 -
8. (colchicine)
0.5mg/ 2
9. (NSAID)
()
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. , ,
-
- 170 -
C
C~
C
61C
70%13131
(Cryoglobulin)
60 Wintrobe Bull
1947 Lemer Watoson
()
(Lympho-proliferative)
()
IgG IgM
()
IgG IgM
-
- 171 -
(essential mixed cryoglobulinemia)
C 36%
127 C 54%17%
34%
C 14.2
7.6
C
()(
)()()(
)
IgM IgM
C
C RNA
-
- 172 -
(1)
(2)
(3) C C
81
C
- Ribavirin
-
C
48
24 RNA
C
70-75 C RNA
-
C
C
C
C
-
- 173 -
1. Meltzer M, Franklin EC, Elias K, et al.
cryoglobulinemiaclinical and laboratory studycryoglobulins with
rheumatoid
factor activity. Am J med 1996;40837-42
2. Abel G, Zhang O-X, Angello V, Hepatitis C virus infection in
type mixed cryoglobulinemia.Arthtitis Rheum 1993;361341-9.
3. Angello V. HypothesisThe etiology of mixed cryoglobulinemia
associated with hepatitis C virus infection.Scand J Immunol
1995;42179-84.
4. Polzien F. SchottP. MihmS. Ramacoria. Hartmann H.
Inteferon-treatment of hepatitis C virus-associated mixed
cryoglobulinemia. J Hepatol.1997;2763-71.
-
- 174 -
(Ankylosing Spondylitis)
(Ankylosing Spondylitis)
510.5 ~ 1%
()
()
()
()
-
- 175 -
CRPESR(A)B27(HLA-B27)
()
()
1984Dr. van der Linden (Modified New York criteria1984)
1. 3 2. 3. 4. 23 41~3
() 1.NSAIDs
-
- 176 -
, COX2 Meloxicam MobicRofecoxibVioxxCelecoxibCelebrex
2.
(Salfasalazine)MTX (Methotrexate116234 5 ~ 10
()
(1)
(2)
()
-
- 177 -
(1)
(2)
(3)
(4)
(5)
() (1)
(2)
(3)
(4)
-
- 178 -
(5)
(6)
(7)
(8)
(9)
()
(10)
(11)
(12)
-
- 179 -
(13)
(14)Sulfasalazine
NSAIDs
(15)
(16)
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. , ,
-
- 180 -
(Chlamydial Arthritis)
1. :
-
- 181 -
8-15
281
2. :
() 3. :
4. :
5. :
6. :
-
- 182 -
7. :
() :
() :
IgM IgA
(1):
(2): DNADNA PCR
(3)(HLA): HLA-B27HLA-B27
-
- 183 -
1.
2. Quinolone
3. 4.
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. , ,
-
- 184 -
(Gonococcal Arthritis)
15 30 5 9
-
- 185 -
1.:
2.: 60-90% 5
3.:
90%
4.:
1. 4-5
2. 3.
:
80-90%50-75% 25% :
-
- 186 -
: 1.:
3 20
2.:
3.PCR:
PCR DNA
:
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. , ,
-
- 187 -
(Myofascial Pain Syndrome)
(Trapezius) :
(Sternocleidomastoid muscle) :
-
- 188 -
(Levator scapulae muscle) : ? (Splenius capitis and splenius
cervicis) : (Posterior cervical muscles : multifundi, semispinalis)
:
(Suboccipital muscle) : (Temporalis muscle) : :
(Scalene Muscles):
(Supraspinatus Muscle):
(Infraspinatus Muscle):
(Teres Minor): (Latissmus Dorsi Muscle): (Teres Major):
(Rhomboideus Muscles): . (Deltoid Muscle): (Pectoris Major &
Minor):
. (Sternalis):
(Serratus Anterior, Posterior):
-
- 189 -
(Biceps brachii):
(Hand extensors):
(Quadriceps femoris):
(Hamstring muscle):
(Gastrocnemius muscle): (Soleus muscle):
(Thoracolumbar Paraspinal Muscles): (Quadratus Lumborum):
(Iliopsoas Muscle): (Gluteus Minimus): (Gluteus Medius): (Gluteus
Maximus):,
(Pyriformis muscle)
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. , ,
-
- 190 -
Nonsteroid Anti-inflammatory Drugs; NSAIDS
()
Cox-1Cox-2Cox-1
Cox-2 Cox-2
Leukotriene
-
- 191 -
()
()
()
phenylbutazone Indomethacin
()
Indomethacin
-
- 192 -
IbuprofenTolmetin Sulindac
()
pyrazole
misprostol (Corticosteroids, )
-
-
- 193 -
1949 (Mayo Clinic) Hench 1950
Hench
( prednisolone 7.5mg)
()
prednisolone
1mg/kg 40mg prednisolone
()
20-40mg
prednisolone
prednisolone
()
2-20mg prednisolone
methotrexate
-
- 194 -
prednisolone 2 3
()
1.
2.
3.
4.
() :
1. H2 2.
3.
4. 5. 1()
6. 7. 8.
-
- 195 -
9.
DMARDs
(DMARDs, Disease Modifying Anti-rheumatic Drugs)DMARDs: 1.
(Sulfasalazine) 2. (Hydroxychloroquine) 3. (Methotrexate, MTX) 4.
(Arava, Leflunomide)
FDA
MTX MTX
5. (Enbrel) FDA
MTX
6. A (Ciclosporin A) A
T MTX DMARDs A
-
- 196 -
DMARDs
DMARD
DMARDs
1. Kelly, Harris, Ruddy, Sledege, Textbook of Rheymatology, 5th
Ed., Saunders
2. Klippel, Dieppe, Rheumatology, 2nd Ed. Mosby 3. Daniel J.
Wallace, Bevra Hannahs Hahn, Edmund L. Lupus
Erythematosus Dubois, Dubois' Lupus Erythematosus, Lippincott
Williams & Wilkins Publishers
4. , ,
-
- 197 -
1976-1986 (therapeutic plasma exchange) 1983-1992
1992 86 86 prednisolone cyclophosphamide 40 DNA 20% 17%
T cyclophosphamide T 1980 (60ml/kg albumin) cyclophosphamide
cyclophosphamide
-
- 198 -
14 8 56 14 4 1 17
(1). SLE (thrombotic thrombocytopenic prupura, TTP) (2). SLE
(3). SLE (4). ()
(1). (2). 1 1.5 (plasma volume) (3). 10
(antiphospholipid antibody) (lupus anticoagulant) 34% 44%
65%
"" (catastrophic antiphospholipid antibody syndrome) 60%
(DIC)(heparin)
-
- 199 -
(1). 14 34(2). 24 29
(thrombotic microangiopathy)
(1)(2)
47cc/kg
-
- 200 -
1992
(ANCA)
NIH
Churg-Strauss
prednisolone cyclophosphamide prednisolone cyclophosphamide
Wegeners
IgM
22.5
-
- 201 -
(1). (2). (3). 1
1. Lewis EJ, Hunsicker LG, Lan SP, Rohde RD, Lachin JM. Lupus
Nephritis Collaborative Study Group. A controlled trial of
plasmapheresis therapy in severe Lupus nephritis. N Engl J Med
1992;326:1373-1379.
2. Euler HH, Schroeder JO, Harten P, Zeuner RA, Gutschmidt HJ.
Treatment-free remission in severe systemic lupus erythematosus
following synchronization of plasmapheresis with subsequent pulse
cyclophosphamide. Arthritis Rheum 1994;34:1784-1794.
3. Euler HH, Schwab UM, Schroeder JO, Hasford J. The Lupus
Plasmapheresis Study Group: rationale and updated interim report.
Artif Organs 1996;20:356-359.
4. Fulcher D, Stewart G, Exner T, Trudinger B, Jeremy R.
Plasmaexchange and the anticardiolipin syndrome in pregnancy.
Lancet 1989;2:171.
5. Neuwelt CM, Daikh DI, Linfoot JA, Pfister DA, Young RG, Webb
RL, London SS, Asherson RA. Catastrophic antiphospholipid syndrome:
response to repeated plasmapheresis over three years. Arthritis
Rheum 1997;40:1534-1539.
6. Dwosh IL, Giles AR, Ford PM, Pater JL, Anastassiades TP and
the
-
- 202 -
Queens University Plasmapheresis Study Group. Plasmapheresis
therapy in rheumatoid arthritis: a controlled, double blind,
crossover trial. N Engl J Med 1983;308:1124-1129.
7. Brubaker DB, Winkelstein A. Plasma exchange in rheumatoid
vasculitis. Vox Sang 1981;41:295-301.
8. Madore F, Lazarus JM, Brady HR. Therapeutic plasma exchange
in renal disease. J Am Soc Nephrol 1996;7:367-386.
9. Miller FW, Leitman SF, Cronin ME, Hicks JE, Leff RL, Wesley
R, Fraser DD, Dalakas M, Plotz PH. Controlled trial of plasma
exchange and leukapheresis in polymyositis and dermatomyositis. N
Engl J Med 1992;326:1380-1384.
10. McCune M, Winkelmann RK, Osmundson PJ, Pineda AA. Plasma
exchange: a controlled study of the effect in patients with
Raynauds phenomenon and scleroderma. J Clin Apheresis
1983;1:206-214.
11. Endo H, Hosono T, Kondo H. Antineutrophil cytoplasmic
autoantibodies in 6 patients with renal failure and systemic
sclerosis. J Rheumatol 1994;21:864-870.
12. Guillevin L, Lhote F, Cohen P, Jarrousse B, Lortholary O,
Genereau T, Leon A, Bussel A. Corticosteroids plus pulse
cyclophosphamide and plasma exchanges versus corticosteroids plus
pulse cyclophosphamide alone in the treatment of polyarteritis
nodosa and Churg-Strauss syndrome patients with factors predicting
poor prognosis. A prospective, randomized trial in sixty-two
patients. Arthritis Rheum 1995;38:1638-1645.
13. OReilly MJG, Talpos G, Roberts VC. Controlled trial of
plasma exchange in treatment of Raynauds syndrome. Br Med J 1979;
1:1113-1115.
14. Frankel AH, Singer DRJ, Winearls CG, Evans DJ, Rees AJ,
Pusey CD. Type II essential mixed cryoglobulinemia: presentation,
treatment outcome in 13 patient. Q J Med 1992; 82: 101-124
-
- 203 -
1. methotrexate, ketoconazole
2.
3.
4.
-
- 204 -
5.
6.
7. 8. 9. spirolactone 10.
1.
2. 3. 4. 5. 6. 7.
8.
1. , ,
-
- 205 -
()(Alfalfa)
(L-canavanine)
-
- 206 -
T (suppressor-inducer T cell)
()(Echinaccea)
-
- 207 -
1. , ,
-
- 208 -
1. Monoarticular or pauciarticular symptoms 2. Polyarticular
joint symptoms 3. Diagnostic algorithm for polyarticular disorders
4. Inflammatory or non-inflammatory arthritis 5. Approach to
management in difficult fibromyalgia syndrome 6.
Spondyloarthropathy 7. Diagnostic algorithm for spinal disorders 8.
Cryoglobulinemia
-
- 209 -
Arthralgia limited to oneOr several joints
Complete History & Physical Examination
Significant Trauma or Focal Bone Pain
Effusion or Signs of Inflammation?
X-ray
FRACTURE, YUMOR or METABOLIC BONE
Joint Aspiratio
Probable Inflammatory
Process
Re-evaluate Bloody Bone Marrow
Elements Present >2000 WBCs? >75% PMNs?
COAGULOPATHY, PSEUDOGOUT,
TUMOR, TRAUMA, or CHARCOT JOINT
Check: PT/PTT Platelet Count Bleeding Time
INTRA- ARTICULAR FRACTURE
Cystals Identified
Positive Culture*
Sterile Inflammatory
Joint Fluid
MONOSODIUN URATE (gout)
CALCIUM PYTOPHOSPHATE
DIHYDRATE (pserfogout)
INFECTIOUS ARTHRITIS
*Synovial Fluid Culture as well as
cervical, urethal,pharyngeal, and/or
rectal evalusttions for Gonococcus and
Chlamydia when suspected
*
Check: CBC, ESR, RF Consider: LFTs, LHA-B27, ANA, Lyme
serologies, and Pelvis Radiographs
Point Tenderness or Trigger Points
BURSITIS, TENDINITIS, or FIBROMYALG1
OSTEOARTHRITIS, INTERNAL
DERANGEMENT, SOFT TISSUE
INJURY, or VIRAL (+)
(-)
(-)
(+)
(+)
(-) (+)
adnormal
normal
successful
unsuccessful
Supspect: RA, JRA, VIRAL, SLE, LYME, SARCOIDOSIS, OR
SPONDYLOART
-
- 210 -
?
?
Check: Blood Count Liver Function Tests Consider: Hepatitis B
and C Serology Parvovirus Serology
Check: CBC, ESR, RF, and/or
ANA; Creatinine, Urinalysis, Joint Aspiration (if effusion
present; see previous figure for analysis
Consider: Liver Function Tests Hepatitis B and C Serology
Radiographs Thyroid Stimulation Hormone Calcium Albumin Alkaline
Phosphatase
(-) (+)
(-)
(+) (-)
(+)
-
- 211 -
-
- 212 -
-
213
-
214
-
- 215 -
-
- 216 -
-
- 217 -
Clinical Pathway
( outcomes management )
-
- 218 -
( cost-effective )
( length of hospital stay )
4 4 103
12 12
-
- 219 -
_____________________________________
____/____/_____ ____/____/____ ___
1 2 3 4-5 B/R,U/R,S/R
BUN,Creat,GOT,GPT ESR,CRP Rheumatoid factor HLA-B27R X-ray :
C-spine
T-spine L-spine SI joint KUB Hip ______________
bone scan CT scan of spine
unstable spinal fracture fusion stable spinal fracture
bracing
NSAIDs Sulfasalazine MTX Plaquenil
spinal fracture, active discitis start methylprednisolone pulse
therapy
MTP pulse therapy
Vital signs,, Hot compression On TENS, 15,min,
qid
On bracing
30
,
,
MTP pulse
-
- 220 -
85
""
1. 2. () 3. ()
-
- 221 -
1. 1 2 3
2. 1
3. 2
4. 3
1. ()()()
2. ()()()()
3. ()()
-
- 222 -
()
4.
-
223
Systemic lupus erythematosus Rheumatoid arthritis Sjgrens
syndrome Systemic sclerosis Behets disease Ankylosing spondylitis
Reiters syndfome Relapsing Polychondritis
-
224
The 1982 revised criteria for classification of systemic lupus
erythematosus
Criterion Definition 1. Malar rash Fixed erythema, flat or
raised, over the malar eminences, tending to spare the nasolabial
folds
2. Discoid rash Erythematous raised patches with adherent
keratotic scaling and follicular plugging; atrophic scarring may
occur in older lesions
3. Photosensitivity Skin rash as a result of unusual reaction to
sunlight, by patient history or physician observation
4. Oral ulcers Oral or nasopharyngeal ulceration, usually
painless, observed by physician
5. Arthritis Nonerosive arthritis involving 2 or more peripheral
joints, characterized by tenderness, swelling, or effusion
6. Serositis
a) Pleuritis--convincing history of pleuritic pain or rubbing
heard by a physician or evidence of pleural effusion
OR b) Pericarditis--documented by ECG or rub or evidence of
pericardial effusion
7. Renal disorder
a) Persistent proteinuria greater than 0.5 grams per day or
grater than 3+ if quantitation not performed
OR b) Cellular casts--may be red cell, hemoglobin, granular,
tubular, or mixed
8. Neurologic disorder
a) Seizures--in the absence of offending drugs or known
metabolic derangements; e.g., uremia, ketoacidosis, or electrolyte
imbalance
OR b) Psychosis--in the absence of offending drugs or known
metabolic derangements, e.g., uremia, ketoacidosis, or electrolyte
imbalance
9. Hematologic disorder
a) Hemolytic anemia--with reticulocytosis OR
b) Leukopenia--less than 4,000/mm3 total on 2 or more occasions
OR
c) Lyphopenia--less than 1,500/mm3 on 2 or more occasions OR
d) Thrombocytopenia--less than 100,000/mm3 in the absence of
offending drugs
10. Immunologic disorder
a) Positive LE cell preparation OR
b) Anti-DNA: antibody to native DNA in abnormal titer OR
c) Anti-Sm: presence of antibody to Sm nuclear antigen OR
d) False positive serologic test for syphilis known to be
positive for at least 6 months and confirmed by Treponema pallidum
immobilization or fluorescent treponemal antibody absorption
test
11. Antinuclear antibody An abnormal titer of antinuclear
antibody by immunofluorescence or an equivalent assay at any point
in time and in the absence of drugs known to be associated with
"drug-induced lupus" syndrome
Updating the American College of Rheumatology Revised Criteria
for the Classification of Systemic
Lupus Erythematosus 1. Delete item 10(a) ("Positive LE cell
preparation"), and 2.Change item lO(d) to "Positive finding of
antiphospholipid antibodies based on
1) an abnormal serum level of IgG or IgM anticardiolipin
antibodies, 2) a positive test result for lupus anticoagulant using
a standard method, or 3) A false-positive serologic test for
syphilis known to be positive for at least 6 months and confirmed
by
Treponema pallidum immobilization or fluorescent treponemal
antibody absorption test.
-
225
1987 Criteria for the Classification of Acute Arthritis of
Rheumatoid Arthritis
Criterion Definition 1. Morning stiffness Morning stiffness in
and around the joints, lasting at least 1 hour before maximal
improvement
2. Arthritis of 3 or more joint areas
At least 3 joint areas simultaneously have had soft tissue
swelling or fluid (not bony overgrowth alone) observed by a
physician. The 14 possible areas are right or left PIP, MCP, wrist,
elbow, knee, ankle, and MTP joints
3. Arthritis of hand joints At least 1 area swollen (as defined
above) in a wrist, MCP, or PIP joint
4. Symmetric arthritis
Simultaneous involvement of the same joint areas (as defined in
2) on both sides fo the body (bilateral involvement of PIPs, MCPs,
or MTPs is acceptable without absolute symmetry)
5. Rheumatoid nodules Subcutaneous nodules, over bony
prominences, or extensor surfaces, or in juxtaarticular regions,
observed by a physician
6. Serum rheumatoid factor Demonstration of abnormal amounts of
serum rheumatoid factor by any method for which the result has been
positive in
-
226
Criteria for the Diagnosis of Sjogren's Syndrome Primary
Sjogren's Syndrome: all of the following
(1) keratoconjunctivitis sicca (see chapter on ophthalmology)
(2) xerostomia (see chapter on dentistry and oral medicine) (3) no
concurrent connective tissue disease
Secondary Sjogren's Syndrome (1) keratoconjunctivitis sicca
and/or xerostomia (2) connective tissue disorder
Rheumatoid arthritis Systemic Lupus Erythematosus Progressive
Systemic Sclerosis, Scleroderma Dermatomyositis, Polymyositis
Primary Biliary Cirrhosis Wegener's Granulomatosis Polyarteritis
Nodosa
Possible or Incipient Sjogren's Syndrome (1)
keratoconjunctivitis sicca or xerostomia (2) one of the following
conditions associated with an immune
dysfunction in the absence of a diagnosed connective tissue
disorder: pulmonary lymphocytic interstitial infiltrates
interstitial nephritis and/or renal tubular acidosis
hypergammaglobulinemia vasculitis with purpura polymyopathy chronic
noncirrhotic liver disease neuropathy
References: 1. Daniels TE. Chapter 6: Benign lymphoepithelial
lesion and Sjogren's syndrome. pages 83-106. IN:
Ellis GL, Auclair PL, Gnepp DR. Surgical Pathology of the
Salivary Glands.Volume 25 in Major Problems in Pathology. WB
Saunders Company. 1991. Table 6-1 page 97.
2. Manthorpe R, Oxholm P, et al. The Copenhagen criteria for
Sjogren's syndrome. Scand J Rheumatology. 1986; Supplement 61:
19-21.
3. Prause JU. Manthorpe R, et al. Definition and criteria for
Sjogren's syndrome used by the contributors to the First
International Seminar on Sjogren's Syndrome - 1986. Scand J
Rheumatology. 1986; Supplement 61: 17-18.
-
227
1980 Criteria for the Classification of Systemic Sclerosis
Glossary of clinical terms used in description or classification
of systemic sclerosis
1. Typical sclerodermatous skin changes: tightness, thickening,
and non-pitting induration, excluding the localized forms of
scleroderma (morphea or linear scleroderma)
a) Sclerodactyly: above-indicated changes limited to (fingers
and toes).
b) Proximal scleroderma: above-indicated changes proximal to the
metacarpophalangeal or metatarsophalangeal joints, affecting other
parts of the extremities, face, neck, or trunk (thorax or abdomen);
usually bilateral, symmetrical and almost always including
sclerodactyly
2. Other skin manifestations attributable to systemic sclerosis
or comparison disorders
a) Digital pitting scars or loss of substance from the finger
pad: depressed areas at tips of digits or loss of digital pad
tissue as a result of digital ischemia rather than trauma or
exogenous causes
b) Bilateral finger or hand edema: firm but pitting edema,
especially involving fingers (includes puffy sausage-like swelling
of fingers) or the dorsal aspect of the hands
c) Abnormal skin pigmentation: hyperpigmentation often
containing areas of punctate or patchy hypopigmentation or
depigmentation ("pepper and salt")
d) Raynaud's phenomenon: at least two-phase color change in
fingers and often toes consisting of pallor, cyanosis, and/or
reactive hyperemia in response to cold exposure or emotion, as
determined by patient's history or physician's observation
3. Visceral manifestations
a) Bibasilar pulmonary fibrosis: bilateral reticular pattern of
linear or lineonodular densities which are most pronounced in
basilar portions of the lungs on standard chest roentgenogram; may
assume appearance of diffuse mottling or "honeycomb lung," and
should not be attributable to primary lung disease
b) Lower (distal) esophageal dysphagia: substernal discomfort on
swallowing or sensation of food holdup in the retrosternal
location
c) Lower (distal) esophageal dysmotility: hypoperistalsis or
aperistalsis, as demonstrated by either cine esophagram or
fluoroscopy or by manometric study, often accompanied by evidence
of decrease in lower esophageal sphincter tone with reflux of
gastric contents into the esophagus
d) Colonic sacculations: wide-mouthed diverticula of colon
located along the antimesenteric border; found on barium enema
examination; these sacculations may also occur in ileum and
jejunum
-
228
-
229
New York Criteria for Ankylosing Spondylitis Overview: The New
York criteria for ankylosing spondylitis is a modification of
the
Rome criteria as proposed at the CIOMS Symposium in New York
during 1966. It combines both clinical criteria and radiographic
findings of the sacroiliac joint.
Clinical criteria (1) Limitation of motion of the lumbar spine
in all 3 planes (anterior flexion, lateral
flexion, extension). Skin markings to aid in the examination are
shown in the Figure on page 356 of Moll (1973).
(2) A history of pain or the presence of pain at the dorsolumbar
junction or in the lumbar spine.
(3) Limitation of chest expansion to 1 inch (2.5 cm) or less,
measured at the level of the fourth intercostal space.
Radiographic Changes in the Sacroiliac Joint(s) Grade normal 0
suspicious 1 1 minimal sacroiliitis 2 2 moderate sacroiliitis 3 3
ankylosis 4 4 Radiographic Change Clinical Criteria Present
Interpretation bilateral grade 3-4 sacroiliitis 1 or more definite
unilateral grade 3-4 sacroiliits criterion #1 definite bilateral
grade 2 sacroiliitis criterion #1 definite unilateral grade 3-4
sacroiliits criterion #2 or #3 definite bilateral grade 2
sacroiliitis criterion #2 or #3 definite bilateral grade 3-4
sacroiliitis 0 probable References:
1. Bennet PH, Wood PHN. Population studies of the rheumatic
diseases. Amsterdam, Excerpta Medica Foundation. 1968; 456-457. Eck
JC, Humphreys C. Diagnosis and treatment of common metabolic spinal
disorders in the geriatric population. Southern Medical Journal.
1998; 91: 1090-1097.
2. Goei The HS, Steven MM, et al. Evaluating of diagnostic
criteria for ankylosing spondylitis: A comparison of the Rome, New
York and modified New York criteria in patients with a positive
clinical history screening test for ankylosing spondylitis. Br J
Rheumatol. 1985; 24: 242-249. Moll JMH, Wright V. New York clinical
criteria for ankylosing spondylitis. Ann Rheum Dis. 1973; 32:
354-363.
3. Moll JMH. New criteria for the diagnosis of ankylosing
spondylitis. Scand J Rheumatology. 1987; Supplement 65: 12-24. van
der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic
criteria for ankylosing spondylitis. Arthritis Rheumatism. 1984;
27: 361-368.
-
230
Modified New York Criteria for Ankylosing Spondylitis Overview:
van der Linden et al proposed a modification to the original New
York criteria
for ankylosing spondylitis. This replaces the original New York
pain criterion with the pain criterion from the Rome criteria. The
authors are from the Erasmus University in Rotterdam.
Clinical criteria (1) low back pain and stiffness for more than
3 months which improves with exercise
but which is not relieved by rest. (2) Limitation of motion of
the lumbar spine in both the sagittal and frontal planes. (3)
Limitations of chest expansion relative to normal values corrected
for age and sex. Measurement of chest expansion needs to be
standardized to minimize variability.
measured in the 4th intercostal space van der Linden measured
the expansion twice, taking the larger of the 2. The result is
compared with tables broken down by age and sex (Moll and
Wright, 1972; Moll and Wright, 1973). Using 1 inch (2.5 cm) as
the measure was specific but insensitive.
Radiographic criteria:
(1) bilateral sacroiliitis >= 2 (2) unilateral sacroiliitis
>= 3
Definite anklyosing spondylitis (1) >= 1 clinical criterion
AND 1 radiologic criteria
Probable ankylosing spondylitis
(1) 3 clinical criteria AND no radiologic criteria (2) 1
radiologic criterion is present AND no clinical criteria
References: 1. Dougados M. Editorial: Diagnostic features of
ankylosing spondylitis. Br J Rheumatol. 1995; 34:
301-305. 2. Goei The HS, Steven MM, et al. Evaluating of
diagnostic criteria for ankylosing spondylitis: A
comparison of the Rome, New York and modified New York criteria
in patients with a positive clinical history screening test for
ankylosing spondylitis. Br J Rheumatol. 1985; 24: 242-249.
3. Moll JMH, Wright V. An objective clinical study of chest
expansion. Ann Rheum Dis. 1972; 31: 1-8. 4. Moll JMH, Wright V. The
pattern of chest and spinal mobility in ankylosing spondylitis: an
objective
clinical study of 106 patients. Rheumatol Rehab. 1973; 12:
115-134. 5. Moll JMH. New criteria for the diagnosis of ankylosing
spondylitis. Scand J Rheumatology. 1987;
Supplement 65: 12-24. 6. van der Linden S, Valkenburg HA, Cats
A. Evaluation of diagnostic criteria for ankylosing
spondylitis.
Arthritis Rheumatism. 1984; 27: 361-368.
-
231
American College of Rheumatology
1977 Criteria for the Classification of Acute Arthritis of
Primary Gout
1. More than one attack of acute arthritis
2. Maximum inflammation developed within 1 day
3. Monoarthritis attack
4. Redness observed over joints
5. First metatarsophalangeal joint painful or swollen
6. Unilateral first metatarsophalangeal joint attack
7. Unilateral tarsal joint attack
8. Tophus (proven or suspected)
9. Hyperuricemia
10. Asymmetric swelling within a joint on x ray*
11. Subcortical cysts without erosions on x ray
12. Monosodium urate monohydrate microcrystals in joint fluid
during attack
13. Joint fluid culture negative for organisms during attack
-
232
Criteria for the Diagnosis of Behcets Disease from the
International Study Group for Behcets Disease
Recurrent oral ulcerations, having all of the following
features:
minor aphthous ulcers, major aphthous ulcers, or herpetiform
lesions observed by physician or patient recur at least 3 times in
one 12 month period
AND Two or more of the following
recurrent genital ulcerations: aphthous ulceration or scarring
observed by physician or patient
eye lesions anterior uveitis posterior uveitis cells in vitreous
humor on slit lamp examination retinal vasculitis observed by
ophthalmologist
skin lesions: erythema nodosum observed by physician or patient
pseudofolliculitis papulopustular lesions acneiform nodules
observed by physician in postadolescent patients not on
corticosteroid treatment positive pathergy test
Pathergy (Behcetine) test: skin needle pricks or intradermal
injection of saline read by physician at 24-48 hours positive
reaction: indurated erythema or pustular formation Performance of
criteria sensitivity 91-95% specificity 96-98% References:
International Study Group for Behcets Disease. Criteria for
diagnosis of Behcets disease. Lancet. 1990; 335: 1078-1080.
-
233
ACR Clinical Classification Criteria for Osteoarthritis of the
Hand Overview:
The American College of Rheumatology (ACR) published criteria
for the diagnosis of osteoarthritis involving the hand based on
clinical findings.
10 selected joints evaluated for hard tissue enlargement and
deformity:
(1) second distal interphalangeal (DIP) joint, left hand (2)
third distal interphalangeal (DIP) joint, left hand (3) second
distal interphalangeal (DIP) joint, right hand (4) third distal
interphalangeal (DIP) joint, right hand (5) second proximal
interphalangeal (PIP) joint, left hand (6) third proximal
interphalangeal (PIP) joint, left hand (7) second proximal
interphalangeal (PIP) joint, right hand (8) third proximal
interphalangeal (PIP) joint, right hand (9) first carpometacarpal
(CMC) joint, left hand (10) first carpometacarpal (CMC) joint,
right hand
Traditional format: (1) hand pain, aching or stiffness, AND (2)
3 or 4 of the following:
(a) hard tissue enlargement in >= 2 of the 10 selected joints
(b) deformity of >= 1 of the 10 selected joints (c) hard tissue
enlargement of >= 2 DIP joints (d) swelling of 0 2 (< 3)
metacarpophalangeal (MCP) joints
Classification tree format: all of the following (1) hand pain,
aching or stiffness (2) hard tissue enlargement in >= 2 of the
10 selected joints (3) swelling of 0 2 (< 3) MCP joints (4) one
or both of the following
(a) hard tissue enlargement of >= 2 DIP joints (b) deformity
in >= 1 of the 10 selected joints
NOTE: In Table 6 (page 1607), the last item is "deformity of 2
or more of the 10 selected joints." However, in Figure 1 page 1606,
which is graphical representation of the table, >= 1 is used.
This matches the traditional format.
Performance characteristics:
traditional format has a sensitivity of 94% and specificity of
87% classification tree format has a sensitivity of 92% and
specificity of 98%
References: Altman R, Alarcon G, et al. The American College of
Rheumatology criteria for the classification and reporting of
osteoarthritis of the hand. Arthritis Rheumatism. 1990; 33:
1601-1610.
-
234
Criteria for Reiter's Syndrome Criteria of Calin et al for
Reiter's Syndrome
(1) seronegative (rheumatoid factor negative) asymmetric
arthropathy predominantlyaffecting the lower extremity. Usually
this is a polyarthropathy but may be a monoarthropathy.
(2) one or more of the following: urethritis, or cervicitis in
women dysentery inflammatory eye disease (conjunctivitis,
iridocyclitis, uveitis) mucocutaneous disease (balanitis in the
male, oral ulcerations, and/or keratodermia)
(3) none of the following primary ankylosing spondylitis
psoriatic arthropathy other rheumatic diseases
Other findings: (1) nail lesions (2) aortitis (3) tendonitis
Associations (1) Infection with Chlamydia trachomatis can be
found in over 70% of men with
untreated nondiarrheal Reiter's syndrome. (2) There is evidence
of exaggerated cell-mediated and humoral responses to
chlamydial antigens. (3) A similar syndrome may occur after
enteric infection with Salmonella, Shigella or
Campylobacter. (4) HLA-B27 is present in over 80% of affected
patients.
References: 1. Calin A, Fox R, et al. Prognosis and natural
history of Reiter's syndrome. Ann Rheumatic Dis. 1979;
38 (supplement): 29-31. 2. Stamm WE, Holmes KK. Chapter 140:
Chlamydial infections. pages 759-768 (page761 and 764).
IN: Isselbacher KJ, Braunwald E, et al. Harrison's Principles of
Internal Medicine, Thirteenth Edition. McGraw-Hill. 1994.
-
235
Criteria for the Diagnosis of Relapsing Polychondritis Initial
criteria: 3 or more of the following
(1) recurrent chondritis of both auricles (swelling, pain and
erythrema of the helix, antihelix, tragus and/or external auditory
canal, with sparing of the inferior lobule)
(2) nonerosive inflammatory arthritis (3) chondritis of the
nasal cartilage (4) ocular inflammation (5) chondritis of the
larynx, trachea, or both (6) damage to the cochlea, vestibule or
both, with hearing loss and tinnitus, or vertigo,
or both
Modified criteria (1) 1 or more of the above criteria, with
histologic confirmation (2) chondritis in 2 or more anatomic
locations, with a response to corticosteroids,
dapsone or both where: In the implementation, I counted the
following as separate anatomic locations for
the second modified criteria: one or both ears, nasal cartilage,
larynx and/or trachea, inner ear. Joint and eye involvement were
not included as written.
References: 1. Damiani JM, Levine HL. Relapsing polychrondritis
Rport of ten cases. Laryngoscope. 1979; 89:
929-946 (Table I, page 930). 2. Maddison PJ. Chapter 5.17.3:
Diseases of bone, cartilage, and synovium. pages 1617-1629
(pages
1626-1627). IN: Maddison PJ, Isenberg DA, et al (editors).
Oxford Textbook of Rheumatology, Second Edition. Oxford Medical
Publications. 1998.
3. McAdam LP, O'Hanlan MA, et al. Relapsing polychrondritis.
Prospective study of 23 patients and a review of the literature.
Medicine. 1976; 55: 193-215. Scully RE, Mark EJ, et al (editors).
Weekly clinicopathological exercises: Case 32-1999. N Engl J Med.
1999; 341: 1292-1299. (Table 2, page 1295)
-
236
Classification Tree for the Diagnosis of Takayasu Arteritis
Criteria Comment Age of disease onset 10mmhg
Difference of > 10 mm Hg in systolic blood pressure between
arms
Bruit over subclavian artery or aorta Bruit audible on
auscultation over one or Both subclavian arteries or abdominal
aorta
Arteriographic abnormalities
Narrowing, aneurysms or occlusion of the Entire aorta, its
primary branches, or large Arteries in the proximal upper or lower
Extremities, not due to arteriosclerosis, Fibromuscular dysplasia
or similar causes; Changes usually focal or segmental
-
237
Cirteria for Polymyalgia Rheumatica, 1982
Criteria for diagnosis all of the following: (1) Age of the
patient >= 50 years (2) Erythrocyte sedimentation rate > 40
mm/h (3) Bilateral aching and stiffness for >= 1 month involving
>= 2 of the 3
target body regions (4) Exclusion of all other diagnosis except
giant cell arteritis
Body regions: (1) Neck or torso (2) Shoulder or proximal regions
of the arms (3) Hips or proximal aspects of the thighs
-
238
-
239
A.
B.
C.
D.
(1)
(2)
(3)
E.
(1)
(2) ()
(3)
(4)
(5)
F.
COX-2
(60%)
-
240
(tenosynovitis)
(ceftriaxone ceftizoxime
) 24 36
ciprofloxacin500
amoxicillin/clavulanate500-850
(chlamydia)
B
parvo virus
()
(HIV)
(septic bursitis) olecranon prepatella
(housemaids kneewriters elbow)
( knee pads)
Borrelia burgdorferi
(erythema migrans)
-
241
(Gout)
1% 7 9 1;
3.3%
50~60 30~40 2.7
(Hyperuricemia)
(purine)
(uricase)
7mg/dl 6mg/dl 37
7mg/dl 6mg/dl
2-18% 80%
( 10-20%)(
80-90%)(
)(
)
()
9mg/dl
4.9%; 7 8.9 0.5%;
7mg/dl 0.1%
-
242
(cytokine)(Interleukin)-1-6-8
(Tumor necrosis factor, TNF)
;
2 (cycloxygenase-2)
()
():(1)
;(2) TNF-
;(3)
transforming growth factor (TGF)-;(4)
Peroxisome proliferators-activated reaptor (PPARr)
:
(1)
(2)
()
(3)
(4)
10
(strongly negatively birefringence)
X-
1977():
:: 12
X :1.
2.3.4.5.
-
243
6.7.8.9.10.
11.X -12.
;
(1) (2) (3)
(4)() (5)
()(Isolated hyperuricemia)
Weir (2003)( B)
10mg/dl
10mg/dl
, :
1. 2. 3. ( B) 4. () ()
(NSAID)
(Colchicin)
( B)
NSAIDs ()
NSAIDs( 2 -Cox-2 inhibitors)
NSAIDs( Indomethacin)( B)
Cox-2
/
( 1.0mg~1.5mg)
( B)
-
244
()
( 15~30 mg3-7
) Daxamethasone(5 mg1-2 )
Corticotropin ( C)
()
(
0.5~1.0mg)(
),
()
:
1. 10mg/dl
2.(3 /) 3.()
4.()
5.()
6.0mg/dl ;
5.0mg/dl
:
1. :Allopurinol Xanthine oxidase Xanthine
hypoxanthine()
( 100mg)
400mgAllopurinol
Allopurinol
Steven-Johnsons Allopurinol Steven-Johnsons
2. (Uricase):Rasburicase (Urate oxidase)
Allantoin ( 10~100 )
-
245
( B)
3. (Uricosuric drugs) probenecid(Benemid)Sulfinpyrazone
Benzbromarone(Nacaricin)(fenofibrate)
(Losartan) Allopurinol
probenecidSulfanpyrazone(50
/)(
)Benzbromarone
( C)
Allopurinol
Fenofibrate(Lipanthyl)
( C)
Losartan (Cozaar)
(Uric acid nephrolithiasis)
5~10%
10~20%
(2,6,8-trioxypurine)
(dissociation Constants)
:(1) (2)(pH)
pH 5.5 pH 6.5
()
: (1)(pH 5.5)(2)
(hyperuricuria) ( 24 600mg)(3)
-
246
() pH 24
X-
()
(1)( pH
6.0~6.5); Acetazolamide (2)
: Allopurinol(3)
1.5~2
-
247
1. 2.
3. 4.
5. / 6. II
1. /
2.
3. X
1.()
2.(
)
3.
4.
1.
2./
3.
4.
5.(BMI)
1.
2.
3.
4.
1.
-
248
1. 2. 3. 4. 5. ()
1.
( Cox-2 )
2.()
3.(1-2
)
4.
()
1.(3 /) 2.()
3.
4.
1.
2.
( 6)
3.(
)
2.
1.
2.
-
249
1. Terkeltaub RA. Clinical practice: gout. NEJM
2003;349:1647-55. 2. Rott KT, Agudelo CA. Contempo updates: gout.
JAMA 2003;289:2857-60. 3. Wortmann RL. Gout and hyperuricemia. Curr
Opin Rheumatol 2002;14:281-6. 4. Matsukawa A, Yoshimura T, Maeda T,
Takahashi T, Ohkawara S, Yoshinaga M.
Analysis of the cytokine network among tumor necrosis factor ,
interleukin-1, interleukin-8, and interleukin-1 receptor antagonist
in monosodium urate crystal-induced rabbit arthritis. Lab Invest
1998;78:559-69.
5. Schweyer S, Hemmerlein B, Radzun HJ, Fayyazi A. Continous
recruitment, co-expression of tumor necrosis factor and matrix
metalloproteinases, and apoptosis of macrophages in gouty tophi.
Virchows Arch 2000;437:534-9.
6. Yamamoto T, Moriwaki Y, Takahashi S, Tsutsumi Z, Ka T,
Fukuchi M, et al. A simple method of selecting gout patients for
treatment with uricosuric agents, using spot urine and blood
samples. J Rheumatol 2002;29:1937-41.
7. Segal JB, Albert D. Diagnosis of crystal-induced arthritis by
synovial fluid examination for crystals:lessons from an imperfect
test. Arthritis Care Res 1999;12:376-80.
8. Shekarriz B, Stoller ML. Uric acid nephrolisthiasis: current
consepts and controversies. J Urology 2002;168:1307-14.
9. Park YB, Park YS, Lee SC, Yoon SJ, Lee SK. Clinical analysis
of gouty patients with normouricemia at diagnosis. Ann Rheum Dis
2003;62:90-92.
10. Emmerson BT. Drug therapy: the management of gout. NEJM
1996;334:445-51. 11. Umpierrez A, Cuesta-Herranz J, De Las Heras M,
Liuch-Bernal M, Figueredo E,
Sastre J. Successful desensitization of a fixed drug eruption
caused by allopurinol. J Allergy Clin Immunol 1998;101:286-7.
12. Takahashi S, Moriwaki Y, Yamamoto T, Tsutsumi Z, Ka T,
Fukuchi M. Effects of combination treatment using
antu-hyperuricemic agents with fenofibrate and/or losartan on uric
acid metabolism. Ann Rheum Dis 2003;62:572-5.
13. Hepbum AL, Kaye SA, Feher MD. Long-term remission from gout
associated with fenofibrate therapy. Clin Rheumatol
2003;22:73-6.
14. Perez-Ruiz F, Alonso-Ruiz A, Calabozo M, Herrero-Beites A,
Garcia-Erauskin G, Ruiz-Lucea E. Efficacy of allopurinol and
benzbromarone for the control of hyperuricemia. A pathogenic
approach to the treatment of primary chronic gout. Ann Rheum Dis
1998;57:545-9.
15. Scott JT. Comparison of allopurinol/probenecid. Ann Rheum
Dis 1996;25:623-6. 16. Fam AG. Treating acute gouty arthritis with
selective COX-2 inhibitors. BMJ
2002;325:980-1.
-
250
(Vasculitis)
()
(1)-
(giant cell arthritis)(Takayasus disease); (2)
-(polyarteritis nodosa)
(Kawasakis disease); (3)-
(Wegeners granulomatosis)Churg-Strauss
(microscopic polyangiitis) (4)
-Henoch-Schonlein
(cryoglobulinemia)
(ethanol)
C-ANCA
P-ANCAC-ANCA Cytoplasmic ANCA
azurophilic granule proteinase 3(PR3) P-ANCA Perinuclear
ANCA
Myeloperoxidase(MPO) elastase, lactoferin,cathepsin G
P-ANCAANA
-
251
formalin
P-ANCA
C-ANCA ANCA
Churg-Strauss
Microscopic polyangiitis
Primary pauci-immune necrotizing and crescentic
glomerulonephritisRapidly
progressive glomerulonephritisRPGN C-ANCA
13652
C-ANCA 66
98 P-ANCA
Churg-Strauss
C
ELISAs
C-ANCAproteinase 3PR3p-ANCA
MyeloperoxidaseMPO
,
C-ANCAPR3
Sensitivity73Specificity
99ANCA
ANCA
(1)Induction therapyNIH
-
252
Cyclophosphamide 2mg/kg/day
Cyclophosphamide
Cyclophosphamide
(plasmapheresis)
751
IVIG0.4gm/kg/day
Cyclophosphamide
2Anti-thymocyteglobulin
T3anti-CD4anti-CDw52
4
(2)Cyclosphosphamide
Cyclo