Embed Size (px)
Citation preview

Chemioterapia raka jajnika
Radosław MądryKlinika Onkologii Uniwersytety
Medycznego im. K. Marcinkowskiego w Poznaniu

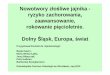
TIME LINE OF ADVANCES IN OVARIAN CANCER THERAPY
1960
1970
1980
1990
2000
CISPLATIN/ALKYLATORCOMBINATIONS
COMBINATION WITH SIGNAL REGULATORS
PACLITAXEL/CARBOPLATIN
ALKYLATORS
CISPLATIN
5 YR SURVIVAL ADVANCED (III/IV) DISEASE
40%35%15%15%0%
1960 1970 1980 1990 2000


I linia

GOG111
McGuire et al, N Engl J Med 334: 1-6, 1996
+5 Mon.
+14 Mon.
N = 386, FIGO III/IV, >1cmCisplatin/Cycloph. vs. Cisplatin/PaclitaxelCrossover to Paclitaxel 8% ‘early’ 34% overall
HR 0,7
HR 0,6

OV10
Piccart et al, J Natl Cancer Inst 92: 699-708, 2000
+4 Mon.
+10 Mon.
N = 680, FIGO IIB/IIC/III/IV6-9x Cisplatin/Cycloph. vs. 6-9x Cisplatin/PaclitaxelCrossover to Paclitaxel Higher (49%)
HR 0,74
HR 0,73

GOG132
Muggia et al, J Clin Oncol 18: 106-115, 2000
HR 1,06
HR 0,99
+2,3 Mon.
+3,9 Mon.
N = 614, FIGO IIB/IIC/III/IVCisplatin. vs. Cisplatin/Paclitaxel vs.Paclitaxel
High Cross-over
„the high rate of early crossover to paclitaxel that had occurred in this single-agent platinum armprior to progression (24%)”Piccard 2003

ICON3
ICON Group, Lancet 360: 505-515, 2002
N = 2027, FIGO I-IVCarboplatin/Paclitaxel vs. Carboplatinvs CAP 1/3 cross-over to Paclitaxelu po progresji
HR 0,93
HR 0,98

GOG 158
Ozols et al, J Clin Oncol 21: 3194-3200, 2003
N = 792, FIGO III, <1cmCispl./Paclit. vs. Carbopl./Paclit.
HR 0,88 ns
HR 0,84 ns
+1,3 Mon.
+8,7 Mon.

OVAR-3 AGO
Du Bois et al, J Natl Cancer Inst 95: 1320-2330, 2003
N = 798, FIGO IIB-IV, <1cmCispl./Paclit. vs. Carbopl./Paclit.
HR 1,05
HR 1,05



SCOTR0C
Vasey et al, J Natl Cancer Inst 96: 1682-1691, 2004
HR 0,97
HR 1,13
N = 1077, FIGO IC-IVCarboplatin/ Paclitaxel vs. Carboplatin/Docetaxel

Badania negatywne I rzutu
• paclitaxel / carboplatin with or without epirubicin - Kristensen
2004
• GOG 182 / ICON 5 Bookman 2005
• paclitaxel / carboplatin with or without topotecan Scarfone 2006
• paclitaxel / carboplatin with or without epirubicin Du Bois 2006
• paclitaxel / carboplatin / 4x topotecan vs. follow up Pfisterer 2006
• cisplatin plus topotecan followed by paclitaxel plus carboplatin versus standard carboplatin plus paclitaxel Hoskins 2008
• paclitaxel / carboplatin with or without gemcitabine Du Bois 2008

NSGO-EORTC-NCIC-GEICO
The addition of epirubicin to the standard carboplatin and paclitaxel treatment did not improve progression-free survival
Kristensen 2004 ASCO Annual Meeting First line treatment of ovarian/tubal/peritoneal cancer FIGO stage IIb-IV with paclitaxel/carboplatin with or without epirubicin (TEC vs TC). A Gynecologic Cancer Intergroup study of the NSGO, EORTC GCG, and NCIC CTG. Results on progression free survival.

MITO
Scarfone G, Scambia G, Raspagliesi F, et al. A multicenter, randomized, phase III study comparing paclitaxel/carboplatin versus topotecan/paclitaxel/carboplatin in patients with stage III (residual tumor > 1 cm after primary surgery) and IV ovarian cancer. Presented at the 42nd Annual Meeting of the American Society of Clinical Oncology; June 2–6, 2006; Atlanta, Ga. abstract 5003
Conclusions: The addition of topotecan to standard PC primary chemotherapy does not increase RR and TTP in stage III (residual tumor > 1 cm) or IV OC compared to PC alone. The TPC regimen was well tolerated with a minority of patients experiencing G3/4 hematological toxicity

AGO GINECO
Du Bois et al, J Clin Oncol 24: 1127-1135, 2006
N = 1282, FIGO IIB-IVCarboplatin/ Paclitaxel vs. Carboplatin/Paclitaxel/Epirubicin
HR 0,95
HR 0,93

AGO OVAR GINECO
N = 1308, FIGO IIB-IV 6x Carboplatin/Paclitaxel 4x Topotecan vs. Follow up
HR 0,97
HR 1,01
Pfisterer et al, J Natl Cancer Inst 98: 1036-1045, 2006

GOG 182 / ICON 5
ASCO 2006

GOG 182 / ICON 5
ASCO 2006

GOG 182 / ICON 5
ASCO 2006

GOG 182 / ICON 5
ASCO 2006

GOG 182 / ICON 5
ASCO 2006

NCIC-EORTC-GEICO OV16
Hoskins PJ. A phase III trial of cisplatin plus topotecan followed by paclitaxel plus carboplatin versus standard carboplatin plus paclitaxel as first-line chemotherapy in women with newly diagnosed advanced epithelial ovarian cancer. A Gynecologic Cancer Intergroup Study of the NCIC CTG, EORTC, GCG, and GEICO. ASCO 2008

AGO OVAR9
A phase III study of paclitaxel, carboplatin, and gemcitabine in previously untreated patients with epithelial ovarian cancer FIGO stage IC–IV (AGO-OVAR protocol OVAR-9) A. du Bois 2008

AGO-OVAR-9; du Bois A i wsp
Randomized phase-III GCIG study (AGO-OVAR-9,GINECO TCG, NSGO-OC-0102): gemcitabine-paclitaxel-carboplatin (TCG) vs. paclitaxel-carboplatin (TC) as firstline treatment of ovarian cancr (OC)
• VII’02 – IV’04• FIGO IC-IV• 1 724 pts
Więcej powikłań hematologicznych w ramieniu TCGBrak zysku z chth 3-lekowej




W trakcie badań

I linia - nowość
• Phase III trial of induction gemcitabine (G) or paclitaxel (T) plus carboplatin (C) followed by elective T consolidation in advanced ovarian cancer (OC): Interim analysis of induction chemotherapy Gordon 2008 ASCO
• Randomized phase III trial of conventional paclitaxel and carboplatin (c-TC) versus dose dense weekly paclitaxel and carboplatin (dd-TC) in women with advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer: Japanese Gynecologic Oncology
Isonishi ASCO 2008

Vergote I i wsp - Neoadjuvant chemotherapy
EORTC-GCG/NCIC-CTG randomised trial comparing primarydebulking surgery with neoadjuvant chemotherapy instage IIIC-IV ovarian, fallopian tube and peritoneal cancer
• IX’98 – XII’06• Potwierdzenie hist-pat raka jajnika LUB• Sugestia cytologiczna +
– guz w miednicy– zmiany przerzutowe ≥ 2 cm poza miednicą– CA125/CEA ≥ 25
• Follow up = 4,8 lat

Late-Breaker Presentation Vergote I i wsp - Neoadjuvant chemotherapy
FIGO IIIC-IV718 pts
Operacja pierwotna▼
6 x chth z platyną
3x chth▼
Operacja odroczona▼
3 x chth

Late-Breaker Presentation Vergote I i wsp - Neoadjuvant chemotherapy

Late-Breaker Presentation Vergote I i wsp - Neoadjuvant chemotherapy
Operacja pierwotna
Operacja odroczona
Śmiertelność ≤ 28 dni
2,7% 0,6%
Posocznica 8% 2%
Krwawienie 3/4° 7% 4%

Late-Breaker Presentation Vergote I i wsp - Neoadjuvant chemotherapy
Operacja pierwotna
Chth neoadj.
OS 29 msc 30 msc HR: 0,98;
CI: 0,85-1,14
PFS 11 msc 11 msc HR: 0,99;
CI: 0,87-1,13

Phase III trial of induction gemcitabine (G) or paclitaxel (T) plus carboplatin (C) followed by elective T
consolidation in advanced ovarian cancer (OC): Interim analysis of induction chemotherapy.
Gordon A, et al. ASCO 2008. Abstract 5536.
Anything other than CR(PR, SD, PD)
Anything other than CR(PR, SD, PD)
Clinical CR
Single-agent crossoverPaclitaxel 175 mg/m2 Day 1
Single-agent crossoverGemcitabine 1000 mg/m2 Days 1,
8
ElectiveT Consolidation Therapy
Paclitaxel 135 mg/m2 every 28 days for 12 cycles
Histologic diagnosis and prior resection of stage IC-IV epithelial ovarian, primary peritoneal,
or fallopian tube carcinoma
Induction GCGemcitabine 1000 mg/m2 Days 1,
8 + Carboplatin AUC 5 Day 1
x 6 cycles every 21 days
Induction TCPaclitaxel 175 mg/m2 Day 1+ Carboplatin AUC 6 Day 1
x 6 cycles q 21 days

Phase III trial of induction gemcitabine (G) or paclitaxel (T) plus carboplatin (C) followed by elective
T consolidation in advanced ovarian cancer (OC):
Interim analysis of induction chemotherapy Response Rates
Gordon A, et al. ASCO 2008. Abstract 5536.
Best response, n (%)Induction GC
(n = 66)Induction TC
(n = 58)P Value
CR* 30 (45.5) 26 (44.8)
PR 13 (19.7) 12 (20.7)
SD 5 (7.6) 8 (13.8)
PD 6 (9.1) 4 (6.9)
Data not available 12 (18.2) 8 (13.8)
ORR (CR + PR) 43 (65.2) 38 (65.5) .999
DCR (CR + PR + SD) 48 (72.7) 46 (79.3) .410
*CR required a normalized CA-125.

Gordon A, et al. ASCO 2008. Abstract 5536.
Toxicity, n (%)Induction GC
(n = 219)Induction TC
(n = 220)P Value
Hematologic
G3/4 thrombocytopenia88 (40.2)55 (25.1)
30 (13.6)10 (4.5)
.0001
G3/4 anemia 52 (23.7) 20 (9.1) .0001
Nonhematologic G2 neuropathy 24 (11.0) 43 (19.5) .0165
G2 alopecia 79 (36.1) 110 (50.0) .0038
Platelet transfusion 7 (3.2) 0 (0) .0073
Phase III trial of induction gemcitabine (G) or paclitaxel (T) plus carboplatin (C) followed by elective
T consolidation in advanced ovarian cancer (OC): Interim analysis of induction chemotherapy
Toxicity

NOVEL (New Ovarian ELaborate); Isonishi S i wsp
Randomized phase III trial of conventional paclitaxel andcarboplatin (c-TC) versus dose dense weekly paclitaxeland carboplatin (dd-TC) in women with advancedepithelial ovarian, fallopian tube, or primary peritonealcancer: Japanese Gynecologic OncologyASCO 2008: J Clin Oncol 2008; 26 (20 May suppl): A5506
• 637 pts
• Follow up - 29 msc

Randomized phase III trial of conventional paclitaxel and carboplatin (c-TC) versus dose dense weekly paclitaxel and
carboplatin (dd-TC) in women with advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer:
Japanese Gynecologic Oncology.Ovarian epithelial, primary peritoneal, or
fallopian tube cancer withFIGO stage II-IV
Conventional TC (c-TC)Paclitaxel 180 mg/m2 Day 1 +Carboplatin AUC 6.0 Day 1 every 21 days for 6-9 cycles
Dose-dense weekly TC (dd-TC)Paclitaxel 80 mg/m2 Days 1, 8, 15 +
Carboplatin AUC 6.0 Day 1every 21 days for 6-9 cycles
Dose-dense weekly TC (dd-TC)Paclitaxel 80 mg/m2 Days 1, 8, 15 +
Carboplatin AUC 6.0 Day 1every 21 days for 6-9 cycles
Stratified by residual disease ≤ 1 cm vs > 1 cm;
FIGO stage II vs III vs IV;histology: clear cell/mucinous vs serous/others
Isonishi S, et al. ASCO 2008. Abstract 5506.

P = .72 Evaluated by WHO criteria
Randomized phase III trial of conventional paclitaxel and carboplatin (c-TC) versus dose dense weekly paclitaxel and
carboplatin (dd-TC) in women with advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer:
Clinical Responses
MeasurablePatients, %
c-TC(n = 135)
dd-TC(n = 147)
Objective response 53 56
• CR 16 20
• PR 38 36
NC 31 29
PD 7 3
NE 9 12
Isonishi S, et al. ASCO 2008. Abstract 5506.

Treatment n Event Median PFS, mos P Value HR 95 %CI
c-TC 319 200 17.2
dd-TC 312 160 28.0 .0015 0.714 0.581-0.879
Isonishi S, et al. ASCO 2008. Abstract 5506.

NOVEL (New Ovarian ELaborate); Isonishi S i wsp
Analiza podgrup – nie uzyskano poprawy PFS przy
raku jasnokom. i śluzowym.
Większa toksyczność hematologiczna w dd-CT.
Neurotoksyczność podobna w obu grupach.
c-TC dd-CT
2-letnie OS (p=0,05)
77,7% 83,6%

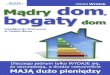
GOG 218: Bev in Primary Adjuvant Treatment and Consolidation Therapy
GOG Statistical Report, July 2008.
GOG 218
Patients with FIGO stage III epithelial ovarian or primary peritoneal cancer with any
gross (macroscopic or palpable) residual disease
or FIGO stage IV
Paclitaxel 175 mg/m2 over 3 hours x 6 cycles + Carboplatin AUC 6
x 6 cycles + Placebo every 3 weeks x 5 (cycles 2-6)
Paclitaxel 175 mg/m2 over 3 hours x 6 cycles + Carboplatin AUC 6
x 6 cycles + Bevacizumab 15 mg/kg every 3 weeks
x 5 (cycles 2-6)
Paclitaxel 175 mg/m2 over 3 hours x 6 cycles + Carboplatin AUC 6
x 6 cycles + Bevacizumab 15 mg/kg every 3 weeks
x 5 (cycles 2-6)
Placebo every 3 weeks x 16
Placebo every 3 weeks x 16
Bevacizumab 15 mg/kg every 3 weeks x 16

GOG 170D: Bevacizumab as Maintenance (Ongoing Phase III Trial)
Patients with stage III/IV ovarian
epithelial or primary peritoneal cancer
(N = 2000)
Arm 1: Paclitaxel over 3 hrs and Carboplatin over 30 mins on Day 1; Placebo* over 30-90 mins on Day 1 every 21 days for 6 courses; Placebo† over 30-90 mins
on Day 1 every 21 days for up to 22 courses
Arm 2: Paclitaxel and Carboplatin as in Arm 1 Day 1; Bevacizumab* over 30-90 mins on Day 1 every 21 days for 6 courses; Placebo† over 30-90 mins on
Day 1 every 21 days for up to 22 courses
Arm 2: Paclitaxel and Carboplatin as in Arm 1 Day 1; Bevacizumab* over 30-90 mins on Day 1 every
21 days for 6 courses; bevacizumab† over 30-90 mins on Day 1 every 21 days for up to 22 courses
*Beginning with course 2.†Beginning with course 7.
ClinicalTrials.gov. Available at: http://clinicaltrials.gov/ct2/results?term=NCT00262847.
• Primary endpoint: OS
• Secondary endpoints: PFS, severe toxicity and severe AEs, QoL, translational objectives by angiogenic markers and gene arrays

ICON-7
EOC, PP cancer
PaclitaxelCarboplatin
placebo
PaclitaxelCarboplatin
Bevacizumab
Bevacizumabx 12 cykli

IP


HISTORY OF IP CHEMO
• Weisberger 1955– Nitrogen mustard intraperitoneally for malignant
ascites
• Jones 1978– signicantly greater concentrations of certain
chemotherapeutic drugs in the peritoneal cavity than in the blood.
• SWOG/GOG– The first phase III trial– since 1980s, presented in 1996– In favor of IP arm

CLINICAL ASPECTS OF IP CHEMO
• Front-line chemotherapy
• Consolidation
• 2nd-line chemotherapy

PHASE III TRIALS OF IP vs IV CISPLATIN BASED CHEMOTHEPAY
(Hamilton, 2006)

PHASE III TRIALS OF IP vs IV CISPLATIN BASED CHEMOTHEPAY
Study Identifier /
Year published
Control Regimen Experimental Regimen Target population
No. of patients
SWOG/GOG-104
(Alberts et al. 1996)
Cisplatin 100 mg/m2 IV
Ctx 600 mg/m2 IVq 3 weeks x 6
Cisplatin 100 mg/m2 IP
Ctx 600 mg/m2 IVq 3 weeks x 6
Stage III
< 2 cm residual
546
Greece
(Polyzos et al. 1999)
Crbpt 350 mg/m2 IVCtx 600 mg/m2 IVq 3 weeks x 6
Crbpt 350 mg/m2 IVCtx 600 mg/m2 IVq 3 weeks x 6
Stage III
< or > 2 cm residual
90
GONO
(Gadducci et al. 2000)
Cisplatin 50 mg/m2 IVCtx 600 mg/m2 IVEpidox 60 mg/m2 IVq 4 weeks x 6
Cisplatin 50 mg/m2 IPCtx 600 mg/m2 IVEpidox 60 mg/m2 IVq 4 weeks x 6
Stage II-IV
< 2 cm residual
113+
GOG-114/SWOG
(Markman et al. 2001)
Cisplatin 75 mg/m2 IVTax 135 mg/m2 (24 hr) IV q 3 weeks x 6
Crbpt AUC 9 IV q 28 days x 2Cisplatin 100 mg/m2 IPTax 135 mg/m2 (24 hr) IV q 3 weeks x 6
Stage III
< 1 cm residual
462
Taiwan
(Yen et al. 2001)
Cisplatin 50 mg/m2 IVCtx 500 mg/m2 IVEpi/Adr 50 mg/m2 IVq 3 weeks x 6
Cisplatin 100 mg/m2 IVCtx 500 mg/m2 IVEpi/Adr 50 mg/m2 IVq 3 weeks x 6
Stage III
< 1 cm residual
118+
GOG-172
(Armstrong et al. 2006)
Cisplatin 75 mg/m2 IVTax 135 mg/m2 (24 hr) IVq 3 weeks x 6
Tax 135 mg/m2 (24 hr) IVCisplatin 100 mg/m2 IPTax 60 mg/m2 IV on day 8q 3 weeks x 6
Stage III
< 1 cm residual
415


MAIN RESULTS
• Eight randomized trials studied 1819 women receiving primary treatment for ovarian cancer.
• Women were less likely to die if they received an intraperitoneal (IP) component to the chemotherapy (hazard ratio (HR) =0.79; 95% confidence interval (CI): 0.70 to 0.90)and the disease free interval (HR =0.79; 95%CI: 0.69 to 0.90) was also significantly prolonged.
• There may be greater serious toxicity with regard to gastrointestinal effects, pain and fever but less ototoxicity with the intraperitoneal than the intravenous route.

HAZARD RATIO FOR TIME TO RECURRENCE (IP vs IV CH)

HAZARD RATIO FOR TIME TO DEATH (IP vs IV CH)

Alberts et al, N Engl J Med: 1950-1955, 1996
+8 Mon.
HR 0,76
n = 546 FIGO III, <2cm
Cisplatin 100 mg/m2i.v. vs. i.p.+Cyclophosphamid i.v.
GOG 104 (Alberts et al, 1996) CISPLATIN IV vs. IP

OS
GOG 104 (Alberts et al, 1996) CISPLATIN IV vs. IP

• As compared with IV cisplatin, IP cisplatin significantly improves survival and has significantly lower toxic effects in patients with stage III ovarian cancer and residual tumor mass of 2cm or less.
• The only same “dose-intensity” in both arms phase 3 RCT
GOG 104 (Alberts et al, 1996) CISPLATIN IV vs. IP

• GOG 111– Median survival from 24 months (P+C)
to 38 months ( P+T)
GOG 104 (Alberts et al, 1996) CISPLATIN IV vs. IP

GOG 114 (Markman et al, 2001) CISPLATIN/PACLITAXEL vs.
CARBO – PACLITAXEL / CISPLATIN IP
Markman et al, J Clin Oncol 19: 1001-1007, 2001
n = 462 FIGO III, <1cm
6x CP i.v. vs. 2x Carboplatin AUC9 –6x Paclitaxel i.v. /Cisplatin i.p.
HR 0,78
+6 Mon.
HR 0,81
+11 Mon.

GOG 114 (Markman et al, 2001) CISPLATIN/PACLITAXEL vs.
CARBO – PACLITAXEL / CISPLATIN IP
PFS
OS

GOG 114 (Markman et al, 2001) CISPLATIN/PACLITAXEL vs.
CARBO – PACLITAXEL / CISPLATIN IP
• The 2nd phase 3 RCT to show IP cisplatin is superior to IV cisplatin in small volume residual advanced ovarian cancer
• The 1st phase 3 trial in ovarian cancer to a median survival of >5 years
• Trial demonstrated that IP cisplatin favorably impacts survival, even through IV paclitaxel is a component of regimen

GOG 114 (Markman et al, 2001) CISPLATIN/PACLITAXEL vs.
CARBO – PACLITAXEL / CISPLATIN IP
• More complications in IP arm– Neutropenia, thrombocytopenia– G-I & metabolic toxicities
• Carbopltin x 2 cycles ( AUC 9)

GOG 172(Armstrong et al, 2006) CISPLATIN/PACLITAXEL IV vs. IP
Armstrong et al, N Engl J Med 354: 34-43
n = 415 FIGO III, < 1 cm
6x CP vs. 6x Paclitaxel i.v. d1+Cisplatin i.p. d2 + Paclitaxel i.p. d8
42% all 6 IP cycles
HR 0,77
HR 0,73
+5,5 Mon.
+15,9 Mon.

GOG 172(Armstrong et al, 2006) CISPLATIN/PACLITAXEL IV vs. IP

PFS
OS
GOG 172(Armstrong et al, 2006) CISPLATIN/PACLITAXEL IV vs. IP

GOG 172(Armstrong et al, 2006) CISPLATIN/PACLITAXEL IV vs. IP

GOG 172(Armstrong et al, 2006) CISPLATIN/PACLITAXEL IV vs. IP
• Significantly survival benefit in IP arm
• The 65.6 months median survival is the longest survival reported to date from a randomized trial in advanced ovarian cancer

GOG 172(Armstrong et al, 2006) CISPLATIN/PACLITAXEL IV vs. IP
• The IP regimen uses higher and more frequent dosing than the IV regimen
• Toxicities were greater on the IP arm
• Fewer patients on the IP arm were able to complete 6 cycles of therapy

GOG 172(Armstrong et al, 2006) CISPLATIN/PACLITAXEL IV vs. IP
• Although fewer than half the patients assigned to the IP group received six cycles of IP treatment, the group as a whole had a significant improvement in survival as compared with the intravenous group. It is possible that most of the benefit of IP therapy occurs early, during the initial cycles, or that the benefit of IP therapy may be greater if more patients can successfully complete six cycles of treatment.

IP vs IV IN ADVANCED OVARIAN CANCER
Progression-free survival
Investigators No. of Progression-free survival (mo)
year published pts Control arm Exp. Arm
Alberts et al, 1996 546 ND ND
Polyzos et al, 1999 90 19 18
Gadducci et al, 2000 113 25 42
Markman et al, 2001 462 22 281
Yen et al, 2001 118 ND ND
Armstrong et al, 2006 415 18 242
1 p = 0.01; 2 p = 0.05

IP vs IV IN ADVANCED OVARIAN CANCER
Overall survival
Investigators No. of Overall survival (mo)
year published pts Control arm Exp. Arm
Alberts et al, 1996 546 41 491
Polyzos et al, 1999 90 25 26
Gadducci et al, 2000 113 51 67
Markman et al, 2001 462 52 632
Yen et al, 2001 118 48 43
Armstrong et al, 2006 415 50 663
1 p = 0.02; 2 p = 0.05; 3 p = 0.03

IP CHEMOTHERPAY IN OPTIMAL STAGE III OVARIAN CANCER
WHY DID IT TAKE SO LONG?
• It was not a sexy drug
• The treatment was cumbersome
• There was always a reason why the results were interpreted differently– GOG 104: not better than using paclitaxel– GOG 114: because 8 cycles were used– GOG 172: it is toxic, but …

Conclusions on IPCT
• Combined use of IV and IP chemotherapy leads to a significant survival benefit in women with optimally debulked EOC (median + 12 mo).
• Based on the most recent trials, strong consideration should be given to a regimen with IP cisplatin (100 mg/m²) and a taxane (whether IV or IP).
• Toxicities, inconvenience and costs of IP therapy are justified by the improved survival.
Vermorken 2007

FIRST LINE

www.cancer.gov 2008
• the standard treatment approaches are subdivided into:– Treatment options for patients with optimally cytoreduced stage
III disease.– Treatment options for patients with suboptimally cytoreduced
stage III and stage IV disease.
• it is preferable to treat patients with several cycles of chemotherapy before interval debulking surgery.

Konsolidacja / leczenie podtrzymujące
“Still investigational”

Study Patients Randomization Results
Scarfone ’02
n=162
III-IV, SSL, pCR
Pt-Tax based
Epirubicin x 4
vs observation
OS NS
Pfisterer (2003)
n=1308
IIb-IV
Tax-Carbo
Topotecan x 4
vs observation
PFS NS
OS NS
De Placido (2004)
n=273
III-IV, SSL, pCR
< 2 cm, Pt-based
Topotecan x 4
vs observation
PFS NS
OS NS
Markman ’03
N=277
III-IV
Tax-Carbo, cCR
Paclitaxel
3 or 12 cycles
PFS 21 mo
vs 28 mo
P < 0.005
Consolidation/Maintenance TherapiesCytotoxic therapy

Markman et al, JCO 2003; 21: 2460-2465

Final Results of After-6 Protocol
• Methods: 200 pts in cCR (48%) or pCR (52%) after 6 cycles of platinum/paclitaxel were randomized to observation or 175 mg/m² paclitaxel x 6 q 3 weeks
• Results: – No difference in PFS or OS.– Irrespective of treatment arm median PFS was 34.4 mo with PCR
and 24.5 mo with cCR– 3-yr survival 87% (pCR) and 79% (cCR): p=0.04
Conte et al, ASCO abstract #5505 (2007)

II linia

Chore platyno - wrażliwe
Wznowa > 6 mieśięcy
Re -platynizacja
Chore platyno - oporne
Wznowa < 6 miesięcy
Leki nie oparte na platynie
Tradycyjny podział wznowy raka jajnika po leczeniu I rzutu

Chore platyno - oporne

*Approved by the US Food and Drug Administration.
• Clinical trial– GOG 126 (cytotoxic)
series– GOG 170 (biologic)
series– Trabectedin– Patupilone– Phenoxodiol– TLK286
Pegylated liposomal doxorubicin*
Topotecan*
Paclitaxel*
Docetaxel
Gemcitabine
Oral etoposide
Bevacizumab
Therapeutic Approaches for Relapsed Platinum-Resistant Disease

Topotecan vs PLD: Survival in Platinum Refractory/Resistant Subset
Gordon AN, et al. Gynecol Oncol. 2004;95:1-8.

Treatment n CR, % PR, % SD, % CB, % Median PFS, wks
Median OS, wks
Topotecan 124 0.8 5.6 42.7 49.1 13.6 41.3
PLD 130 0.8 11.5 27.7 40.0 9.1 35.6
P value .733 .455
Gordon AN, et al. J Clin Oncol. 2001;19:3312-3322.
Intent-to-treat analysis
Primary endpoint: PFS
Topotecan vs PLD: Survival in Platinum Refractory/Resistant Subset

years
survival rates n 1 2 3
Topotecan 124 43.2% 17.2% 9.5%
PLD 130 41.5% 21.1% 13.8%
Gordon AN, et al. Gynecologic Oncology 2004
Topotecan vs PLD: Survival in Platinum Refractory/Resistant Subset

GOG-126: Phase II Trial Series in Platinum Resistant/Refractory OC
Study N Regimen Principal Grade 3/4 Toxicity
ORR, %
GOG 126-N[1] 48Paclitaxel 80 mg/m2 weekly
Neuropathy (grade 3): 4%
Fatigue (grade 3): 8%20.9
GOG 126-J[2] 60 (58 eval)
Docetaxel 100 mg/m2
every 3 weeks
Neutropenia (grade 4): 75%
22.4
GOG 126-H[3] 41Oral etoposide
50 mg/m2* 21 of 28 days
Neutropenia (grade 3: 20%; grade 4: 25%)
26.8
Markman M, et al. Gynecol Oncol. 2006;101:436-440.Rose PG, et al. Gynecol Oncol. 2003;88:130-135.Rose PG et al. J Clin Oncol. 1998;16:405-410.
*30 mg/m2 for prior radiotherapy.

Gemcitabine 1000 mg/m2 IV on Days 1, 8
every 21 days
PLD 50 mg/m2 IV Day 1 every 28 days
Crossover*
Each treatment given for up to 2 cycles after CR attained
*Optional; allowed in case of progressive disease, undue toxicity, or cumulative PLD dose of 500 mg/m2.
Gemcitabine 1000 mg/m2 IV on Days 1, 8
every 21 days
PLD 50 mg/m2 IV Day 1 every 28 days
Patients with platinum-
resistant taxane-pretreated
ovarian cancer
(N = 195)
Mutch D, et al. SGO 2006. Abstract 28.
Gemcitabine vs PLD: Phase III Recurrent (Platinum Resistant)

Gemcitabine (median:15.6 weeks)
PLD (median: 13.3 weeks)
Log-rank P = .87
Mutch D, et al. SGO 2006. Abstract 28.
Gemcitabine vs PLD Phase III Recurrent (Platinum Resistant): PFS

Chore platyno - wrażliwe

Blackledge G, et al. Br J Cancer. 1989;59:650-653.Thigpen JT, personal communication.
Interval, % Platinum,Response
Other Agents, Response
0-6 mos 10 15
7-12 mos 29 20
13-18 mos 63 30
19-24 mos 94 30
Chemosensitive Disease: TFI

Retreatment With Cisplatin-Based Regimen
Markman, et al Gore, et al
Markman M, et al. J Clin Oncol. 1991;9:389-393. Gore ME, et al. Gynecol Oncol. 1990;36:207-211.
Effect of Platinum-Free Interval on Response Rate
Res
po
nse
Rat
e (%
)
< 12 13-24 > 24
27%
33%
59%
17%
27%
57%
n = 39
n = 20
n = 14
n = 29
n = 11
n = 39
0
10
20
30
40
50
60
Months
Res
po
nse
Rat
e (%
)
< 12 13-24 > 240
10
20
30
40
50
60
Months

Chemosensitive Disease: Major Trials
Trial Regimen
ICON 4/AGO-OVAR 2.2 Carboplatin ± paclitaxel
GCIG OVAR 2.5 Carboplatin ± gemcitabine
PLD/Topotecan PLD vs topotecan

ICON 4/AGO-OVAR 2.2
Paclitaxel + Platinum-based chemotherapy
(n = 392)
Platinum-based chemotherapy(n = 410)
Patients with platinum-sensitive
recurrent ovarian cancer
TFI ≥ 6 months
(N = 802)
Parmar MK, et al. Lancet. 2003;361:2099-2106.
• 2 parallel randomized, multicenter trials

Parmar MK, et al. Lancet. 2003;361:2099-2106.
Time Since Completion of Last Chemotherapy, %
Platinum(n = 410)
Paclitaxel/ Platinum (n = 392)
Total(N = 802)
≤12 mos 27 23 25
> 12 mos 73 77 75
ICON 4/AGO-OVAR 2.2: Patient Characteristics

Difference: 12% (-0.1 to 24.0); P = .06
Parmar MK, et al. Lancet. 2003;361:2099-2106.
Response, % Platinum(n = 128)
Paclitaxel/
Platinum (n = 119)
ORR (CR + PR) 54 66
ICON 4/AGO-OVAR 2.2: Response

• Hazard ratio: 0.76 (95% CI: 0.66-0.89; P = .0004)
• Absolute difference at 1 year: 10% (95% CI: 4-15)
• 50% (paclitaxel/platinum) vs 40%
Parmar MK, et al. Lancet. 2003;361:2099-2106.
ICON 4/AGO-OVAR 2.2: Progression-Free Survival
Patients at riskPaclitaxel + platinumConventional treatment
392410
179157
5245
2517
177

Patients at riskPaclitaxel + platinumConventional treatment
Parmar MK, et al. Lancet. 2003;361:2099-2106.
ICON 4/AGO-OVAR 2.2: Overall Survival
392410
306295
167150
9668
4333
1811
• Hazard ratio: 0.82 (95% CI: 0.69-0.97; P = .023)
• Absolute difference at 2 years: 7% (95% CI: 1-12)
• 57% (paclitaxel/platinum) vs 50%

ICON 4/AGO-OVAR 2.2: Previous Taxanes
OS
PFS
Paclitaxel/Platinum Platinum
No
Yes
0 0.5 1.0 1.5 2.0
No
Yes
P = .49
P = .62
Parmar MK, et al. Lancet. 2003;361:2099-2106.

• Randomized, phase III trial
Gemcitabine (1000 mg/m2) Days 1 and 8Carboplatin (AUC = 4) Day 1
every 21 days x 6 cycles(n = 178)
Carboplatin (AUC = 5) Day 1every 21 days x 6 cycles
(n = 178)
Patients with platinum-sensitive
recurrent ovarian cancer
≥ 6 months out from initial
platinum therapy
(N = 356)
Pfisterer J, et al. J Clin Oncol. 2006;24:4699-4707.
AGO-OVAR 2.5 (GCIG): Gemcitabine/ Carboplatin vs Carboplatin

Gemcitabine/Carboplatin (n = 178)
Carboplatin(n = 178)
Platinum-free interval, %
• 6-12 mos 39.9 39.9
• > 12 mos 59.6 60.1
First‑line therapy, %
• Platinum taxane 70.2 71.3
• Platinum nontaxane 28.7 27.5
• Platinum monotherapy 1.1 1.1
Pfisterer J, et al. J Clin Oncol. 2006;24:4699-4707.
AGO-OVAR 2.5 (GCIG): Platinum-free Interval and Previous Treatment

Parameter, % Gemcitabine/
Carboplatin (n = 178)
Carboplatin (n = 178)
Overall response (CR + PR)*
47.2 30.9
• CR 14.6 6.2
• PR 32.6 24.7
Stable disease 38.2 38.8
Progressive disease 7.9 16.3
Pfisterer J, et al. J Clin Oncol. 2006;24:4699-4707.
AGO-OVAR 2.5 (GCIG): Response Data
*P = .0016

Pfisterer J, et al. J Clin Oncol. 2006;24:4699-4707.
AGO-OVAR 2.5 (GCIG): Progression-free Survival
HR: 0.72 (95% CI: 0.58-0.90); P = .0031
Median: 8.6 mos (range: 7.9-9.7)
Median: 5.8 mos (range: 5.2-7.1)

Pfisterer J, et al. J Clin Oncol. 2006;24:4699-4707.
HR: 0.96 (95% CI: 0.75-1.23); P = .7349
Median: 18.0 mos (range: 16.2-20.2)
Median: 17.3 mos (range: 15.2-19.3)
AGO-OVAR 2.5 nie zaplanowane do oceny całkowitego przeżycia.
AGO-OVAR 2.5 (GCIG): Overall Survival*
Carboplatin

Therapy, % Gemcitabine/Carboplatin(n = 178)
Carboplatin(n = 178)
Any therapy postrecurrence or progression
83.7 78.7
Chemotherapy 75.8 72.5
• 1 regimen 16.3 13.5
• 2 regimens 12.4 15.7
• ≥ 3 regimens 9.6 10.7
• Unspecified no. regimens 37.6 32.6
Hormonal/immunologic/biologic therapy
19.7 18.0
Radiation 5.1 9.6
Other therapy—not specified 15.7 15.2
AGO-OVAR 2.5 (GCIG): Therapy After Recurrence/Progression

Patients with advanced ovarian cancer
(90% stage II/IV)
Recurrent or failed platinum-based therapy
Measurable disease
Median age: 60 years (range: 25-87)
(N = 474)
Topotecan 1.5 mg/m2/d IV for 5 consecutive days every 3 weeks
PLD 50 mg/m2 IV every 4 weeks
Stratification by platinum sensitivity and presence/absence of bulky disease
Gordon AN, et al. J Clin Oncol. 2001;19:3312-3322.
Pegylated Liposomal Doxorubicin vs Topotecan: Phase III Study Design

Patient Group, % PLD Topotecan P Value
Platinum sensitive(n = 220; PLD: 109; T: 111)
28 29 .964
Platinum refractory(n = 254; PLD: 130; T: 124)
12 7 .118
Gordon AN, et al. J Clin Oncol. 2001;19:3312-3322.
PLD vs Topotecan: Response Rates

Gordon AN, et al. Gynecol Oncol. 2004;95:1-8.
PLD vs Topotecan: Median Survival
Median Survival
Pegylated liposomal doxorubicin: 62.7 weeks
Topotecan: 59.7 weeks
HR: 1.23
(95% CI: 1.01-1.50;
P = .038)

Gordon AN, et al. Gynecol Oncol. 2004;95:1-8.
PLD vs Topotecan: Median Survival (Platinum-Sensitive Disease)
Median Survival
Pegylated liposomal doxorubicin: 107.9 weeks
Topotecan: 70.1 weeks
HR: 1.432 (95% CI: 1.066-1.923; P = .017)

Ferrero JM, et al. Ann Oncol. 2007;18:263-268.
• Patients with advanced ovarian cancer
– N = 105 (104 received treatment)
– TFI ≥ 6 months
• PLD 30 mg/m2 + carboplatin AUC 5 every 4 weeks
• Selected patient characteristics
– ECOG PS 1-2: 47%
– 2 prior regimens: 39%
– Measurable disease: 57%
GINECO Phase II Trial: Schema

*Median 6 cycles of therapy.
Ferrero JM, et al. Ann Oncol. 2007;18:263-268.
Outcome PLD/Carboplatin (n = 104)*
ORR (CR+ PR), % 63
• CR, % 38
PFS, mos 9.4
OS, mos 32
GINECO Phase II Trial: Results

Dostępna analiza pośrednia
• Pegylated liposomal doxorubicin (PLD)-carboplatin (C) (C-D) vs paclitaxel-carboplatin (C-P) in relapsing sensitive ovarian cancer (OC): A 500-patient interim safety analysis of the CALYPSO GCIG Intergroup phase III study.
Åvall-Lundqvist 2008 J Clin Oncol / ASCO
Conclusions: This planned interim safety analysis on the first 500 patients confirmed different toxicity profiles in the two arms, with less drug-related SAE and less early therapy termination in the C-D arm.

Chemosensitive Disease: Conclusions
• Platinum regimens superior to nonplatinum regimens tested to date
• Paclitaxel/carboplatin yields superior PFS and OS compared with carboplatin
• Gemcitabine/carboplatin produces superior response and PFS compared with carboplatin
• PLD/carboplatin produces excellent response, PFS, and OS

Chemosensitive Disease: Doublets
• Paclitaxel/carboplatin
• Gemcitabine/carboplatin
• PLD/carboplatin

• An Open-label Multicenter Randomized Phase 3 Study Comparing CAELYX® and YONDELIS™ with CAELYX alone in Relapsed Ovarian Cancer
ESMO 2008
II linia - nowość

Cluster of Ecteinascidia turbinata, a “sea squirt” or tunicate
from the Caribbean Sea
Yondelis: Tetrahydroisoquinoline
alkaloid, MW=762.
Yondelis™, trabectedin, ET-743
1996: PharmaMar starts clinical development of ET-7432001: Joint development of ET-743 by Johnson & Johnson Pharm R&D andPharmaMar

Yondelis™, trabectedin, ET-743
• Wiązanie do rowka mniejszego łańcucha DNA
• Najaktywniejsza w fazie G1• Działanie w czasie
transkrypcji• Interakcja z
mechanizmami naprawczymi DNA

An Open-label Multicenter Randomized Phase 3 Study Comparing CAELYX® and YONDELIS™ with CAELYX alone in Relapsed Ovarian Cancer
• Advanced Recurrent Epithelial Ovarian Cancer
– One prior regimen– Evaluable and measurable
disease– Platinum sensitive and resistant
Primary endpoint: OSOther endpoints: PFS, RR, Safety
Translational Research•Pharmacokinetics•Pharmacogenomics•Pharmacoeconomics•Quality of Life•Circulating tumor cells
RANDOMIZE
Caelyx® 50 mg/m2 q 4 wks
Caelyx® 30 mg/m2 plusYondelis® 1.1mg/m2Every 3 weeks
Accrual 7/11/2006: 374/650

33rd ESMO Congress Stockholm, 12-16 September 2008

OVA-301 Study Shows Significant Prolongation In
Progression Free Survival
• Positive final results of the Phase III randomized pivotal study of Yondelis® in ovarian cancer were presented during the Presidential Symposium at the ESMO congress in Stockholm.
• ESMO selects clinical studies that may result in a change in the current standard of care for presentation at the 2008 Presidential Symposium.

Progression-free survival (PFS)
• Median PFS was 7.3 months (trabectedin + PLD) vs 5.8 months in control arms (PLD)
• The hazard ratio (HR) was 0.79 (p=0.019) • 21% reduction in the risk of progression or
death during the observation period.
• Response rate 28% ( trabectedin and PLD) vs 19% in control arms (PLD)

Overall survival
• The interim survival data presented at ESMO are immature (55% censored) and the final analysis will be conducted after the occurrence of 520 events.
• Nonetheless, a positive trend with a 15% reduction in the risk of death favored patients treated with the Yondelis® and PLD combination.

Toxicity• Neutropenia was the most common toxicity (77%) in the
combination arm compared with 38% of patients in the Doxil®-only arm
• Similarly, reversible liver enzyme (transaminase) elevations were more common with the combination although without permanent liver damage or other clinical consequences.
• The addition of trabectedin enabled a lower dose of Doxil®, which may have contributed to the lower incidence of Doxil®-related toxicity observed with the combination.
• Specifically, hand and foot syndrome was seen in 54% of patients receiving alone compared with 24% of patients treated with trabectedin + Doxil.
• Similarily, stomatitis occurred in fewer patients receiving the trabectedin + Doxil® combination (20%) compared with those receiving Doxil® monotherapy (33%).

Podsumowanie
• I rzut:– Karboplatyna / Paclitaxel– Cisplatyna / Paclitexel IP
• II rzut:– Chore platyno – oporne: PLD, topotekan,
gemcitabine– Chore platyno – wrażliwe: Karboplatyna/ paclitaxel vel gemcitabine, PLD

Pytanie bez odpowiedzi
• - III rzut
• - sekwencyjność chemioterapii
• - miejsce VP-16
• - Leczenie celowane