Embed Size (px)
Citation preview

Cholangiozelluläres Karzinom – State of the art 2014
Prof. Dr. med. Arndt Vogel
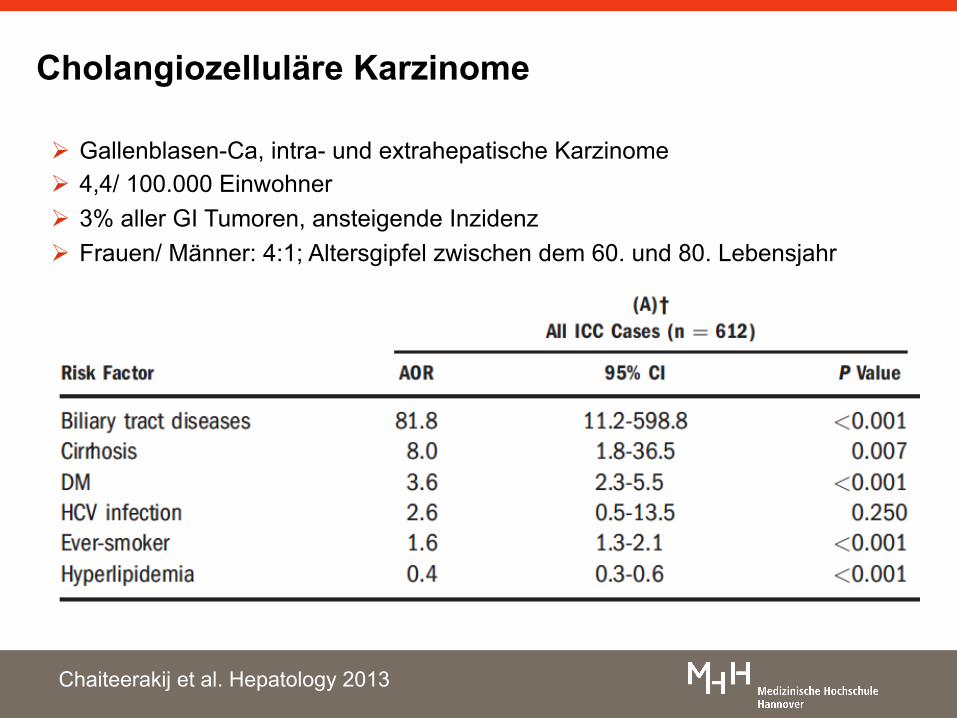
Cholangiozelluläre Karzinome
Ø Gallenblasen-Ca, intra- und extrahepatische Karzinome Ø 4,4/ 100.000 Einwohner Ø 3% aller GI Tumoren, ansteigende Inzidenz Ø Frauen/ Männer: 4:1; Altersgipfel zwischen dem 60. und 80. Lebensjahr
Chaiteerakij et al. Hepatology 2013
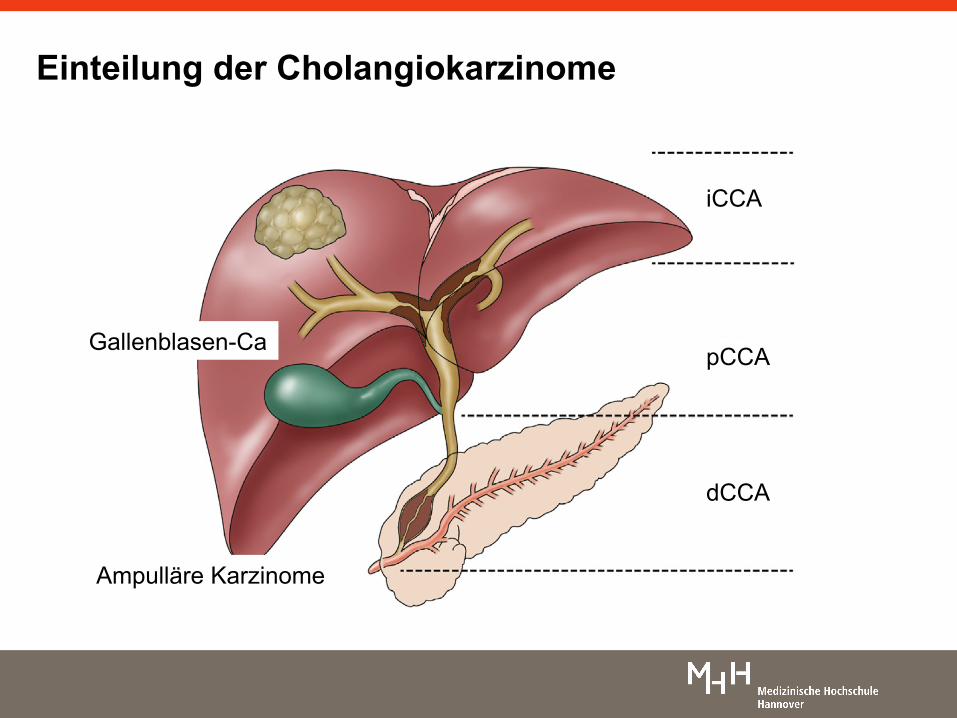
Einteilung der Cholangiokarzinome
iCCA
pCCA
dCCA
Gallenblasen-Ca
Ampulläre Karzinome
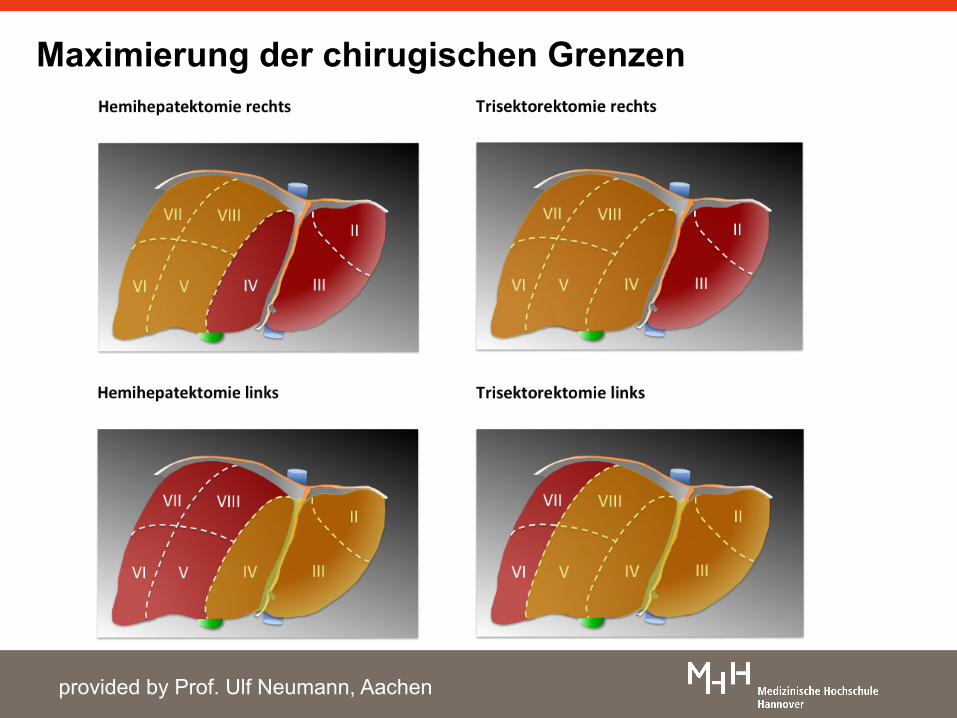
Maximierung der chirugischen Grenzen
provided by Prof. Ulf Neumann, Aachen
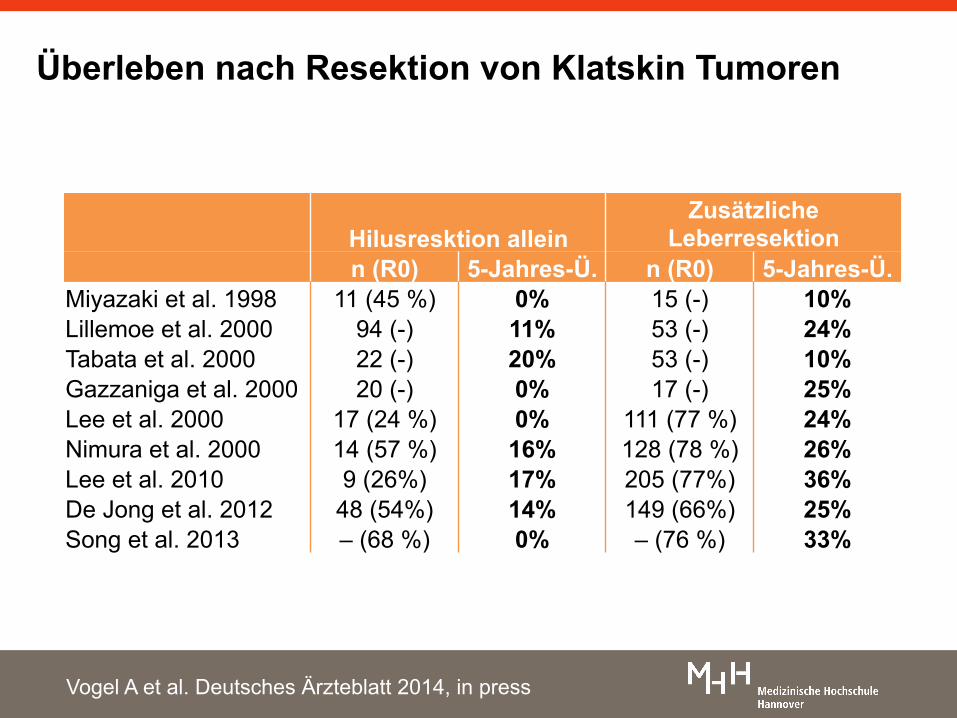
Überleben nach Resektion von Klatskin Tumoren
Hilusresktion allein Zusätzliche
Leberresektion n (R0) 5-Jahres-Ü. n (R0) 5-Jahres-Ü. Miyazaki et al. 1998 11 (45 %) 0% 15 (-) 10% Lillemoe et al. 2000 94 (-) 11% 53 (-) 24% Tabata et al. 2000 22 (-) 20% 53 (-) 10% Gazzaniga et al. 2000 20 (-) 0% 17 (-) 25% Lee et al. 2000 17 (24 %) 0% 111 (77 %) 24% Nimura et al. 2000 14 (57 %) 16% 128 (78 %) 26% Lee et al. 2010 9 (26%) 17% 205 (77%) 36% De Jong et al. 2012 48 (54%) 14% 149 (66%) 25% Song et al. 2013 – (68 %) 0% – (76 %) 33%
Vogel A et al. Deutsches Ärzteblatt 2014, in press
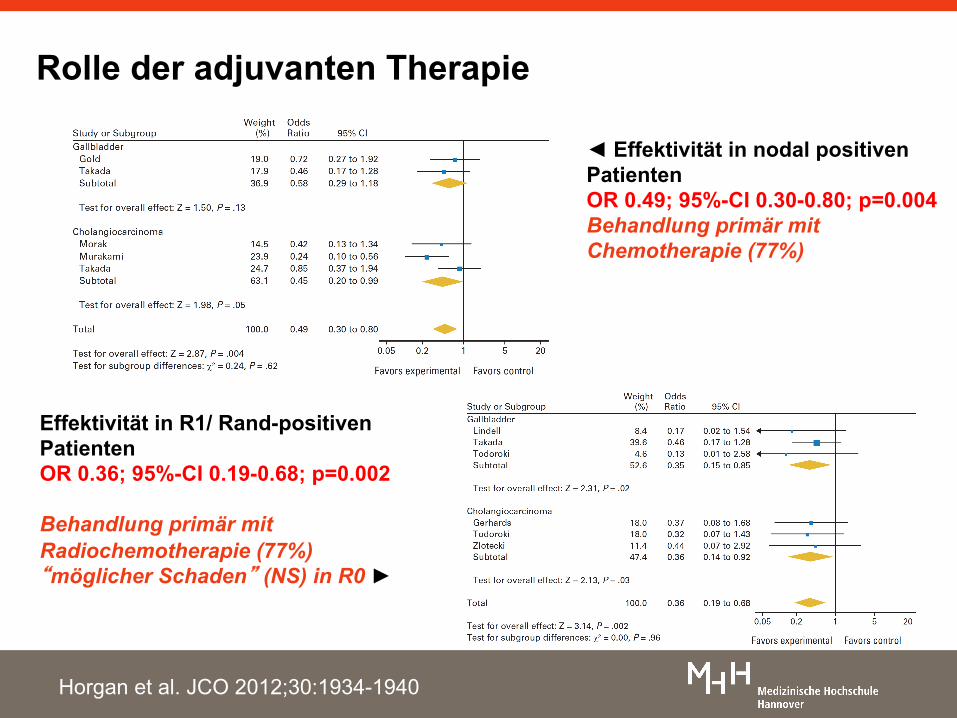
◄ Effektivität in nodal positiven Patienten OR 0.49; 95%-CI 0.30-0.80; p=0.004 Behandlung primär mit Chemotherapie (77%)
Effektivität in R1/ Rand-positiven Patienten OR 0.36; 95%-CI 0.19-0.68; p=0.002 Behandlung primär mit Radiochemotherapie (77%) “möglicher Schaden” (NS) in R0 ►
Horgan et al. JCO 2012;30:1934-1940
Rolle der adjuvanten Therapie
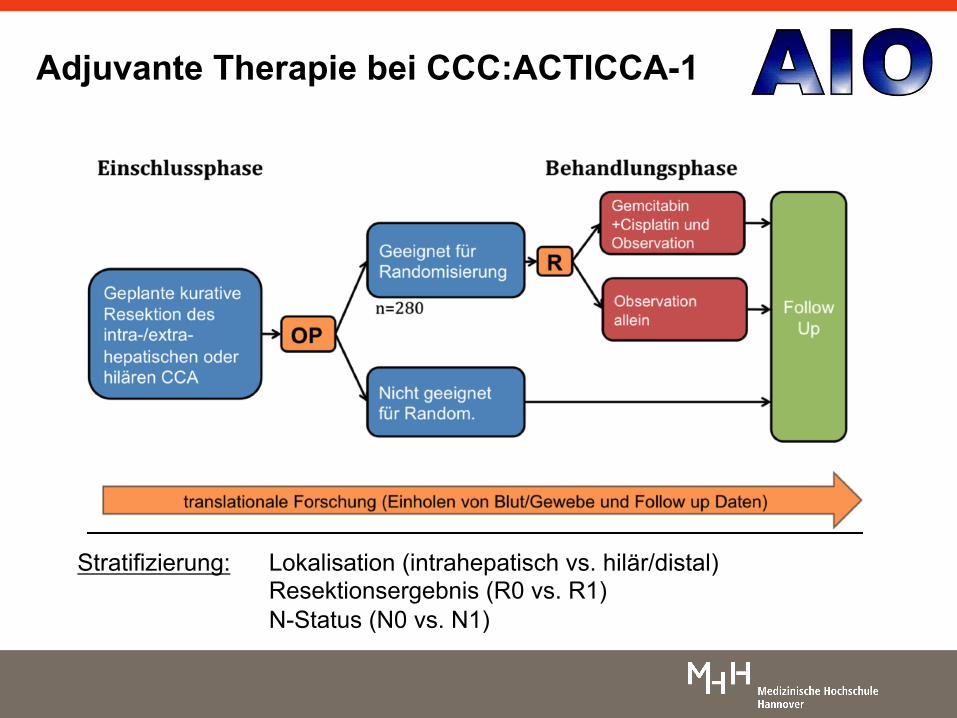
Stratifizierung: Lokalisation (intrahepatisch vs. hilär/distal) Resektionsergebnis (R0 vs. R1) N-Status (N0 vs. N1)
Adjuvante Therapie bei CCC:ACTICCA-1
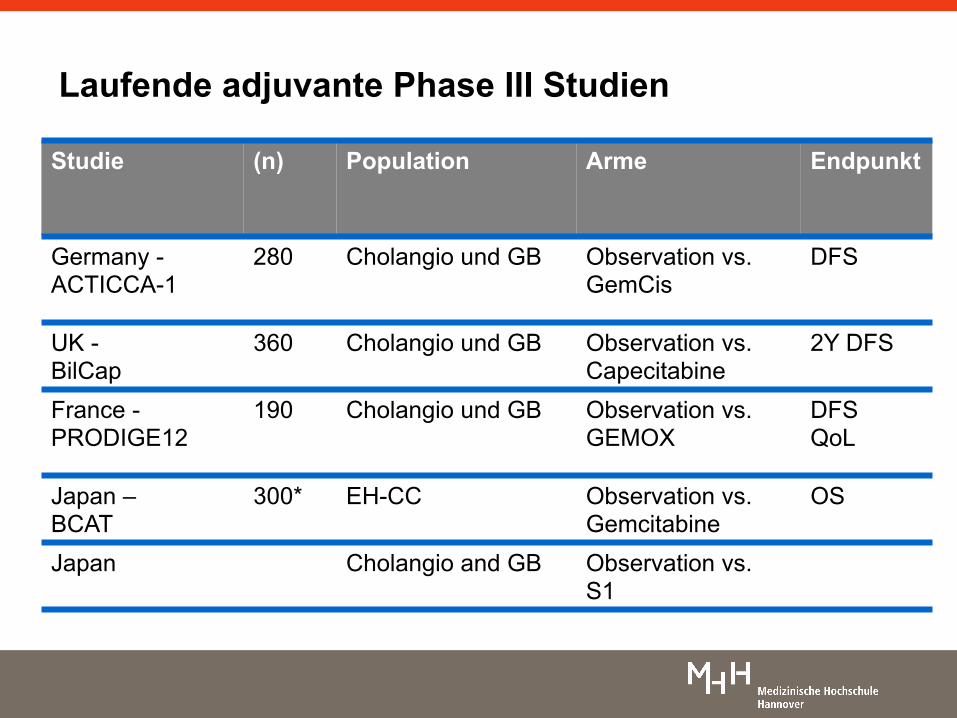
Studie (n) Population Arme Endpunkt
Germany -ACTICCA-1
280 Cholangio und GB Observation vs. GemCis
DFS
UK - BilCap
360 Cholangio und GB Observation vs. Capecitabine
2Y DFS
France - PRODIGE12
190 Cholangio und GB Observation vs. GEMOX
DFS QoL
Japan – BCAT
300* EH-CC Observation vs. Gemcitabine
OS
Japan Cholangio and GB Observation vs. S1
Laufende adjuvante Phase III Studien
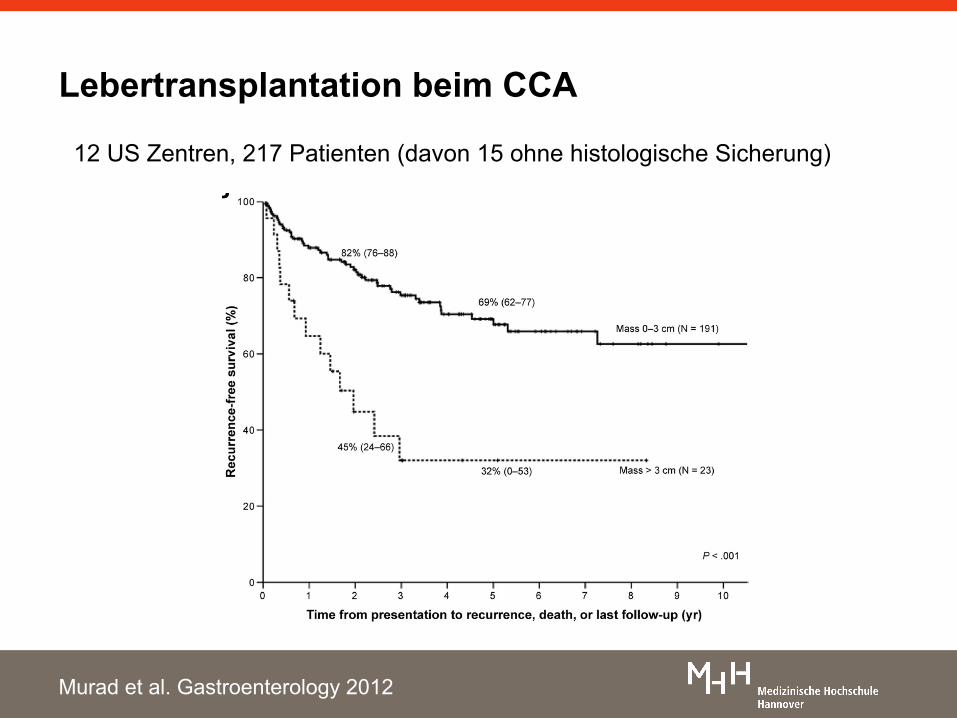
Lebertransplantation beim CCA
12 US Zentren, 217 Patienten (davon 15 ohne histologische Sicherung)
Murad et al. Gastroenterology 2012
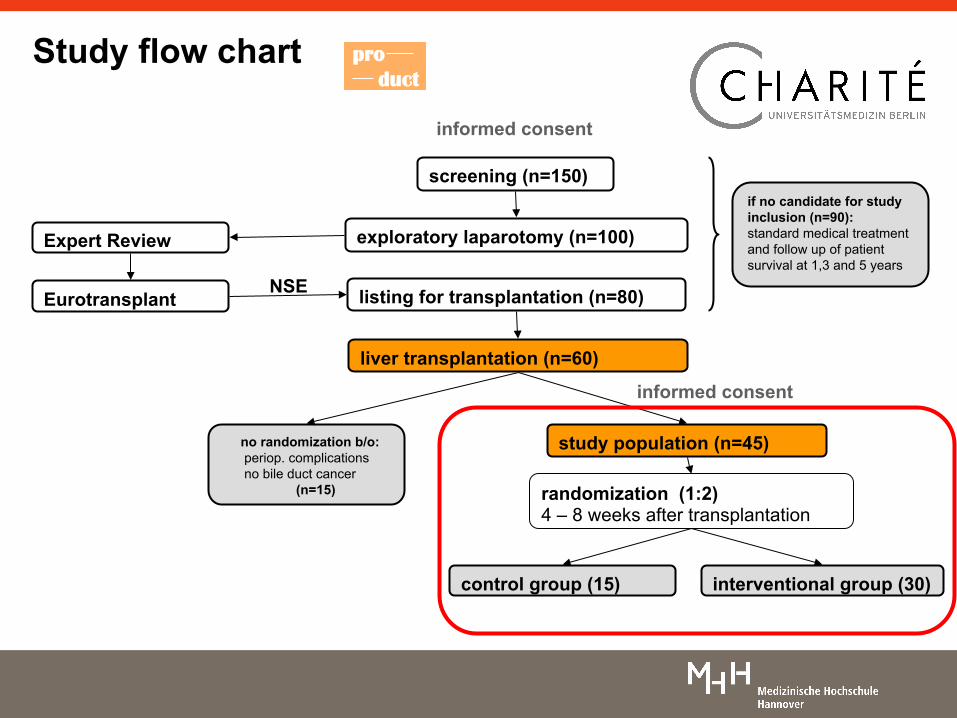
Study flow chart
control group (15) interventional group (30)
randomization (1:2) 4 – 8 weeks after transplantation
no randomization b/o: periop. complications no bile duct cancer (n=15)
listing for transplantation (n=80)
study population (n=45)
screening (n=150)
exploratory laparotomy (n=100)
liver transplantation (n=60)
if no candidate for study inclusion (n=90): standard medical treatment and follow up of patient survival at 1,3 and 5 years
informed consent
informed consent
Expert Review
Eurotransplant NSE
pro duct
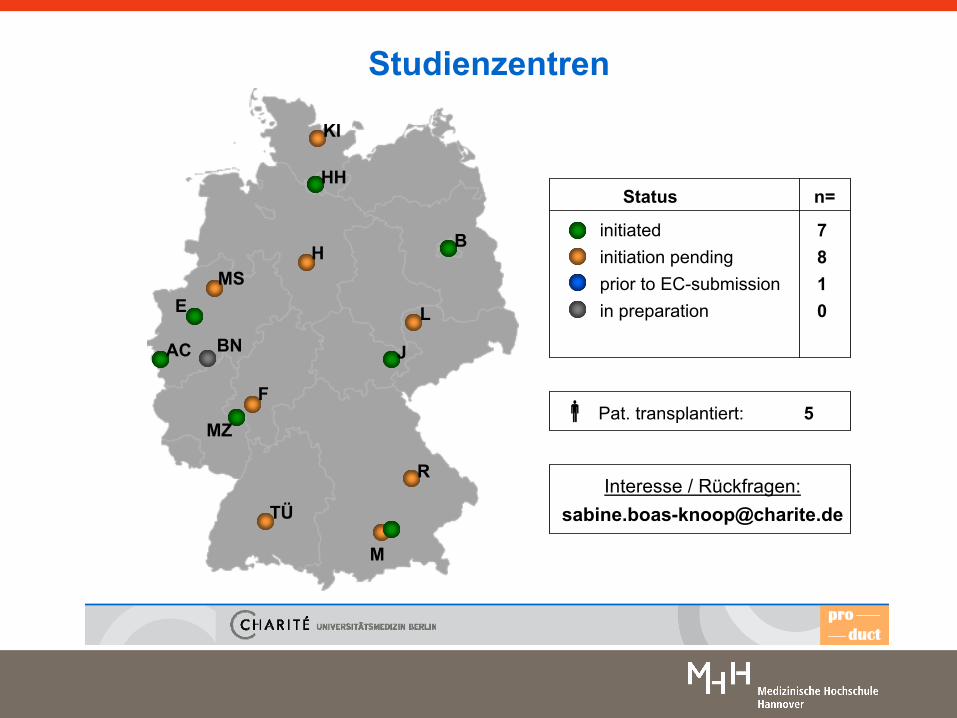
Studienzentren
product
initiatedinitiation pendingprior to EC-submissionin preparation
7810
Status n=
b Pat. transplantiert: 5
Interesse / Rückfragen:[email protected]
B
HH
AC
L
J
TÜ
MZ
F
E
KI
H
R
M
MS
BN
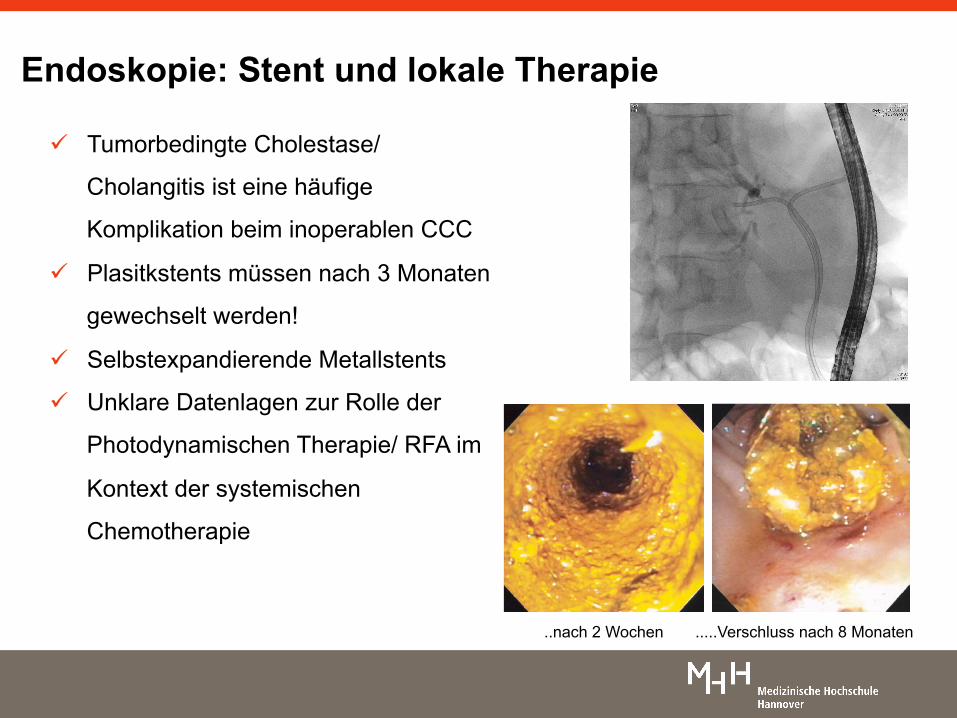
ü Tumorbedingte Cholestase/
Cholangitis ist eine häufige
Komplikation beim inoperablen CCC
ü Plasitkstents müssen nach 3 Monaten
gewechselt werden!
ü Selbstexpandierende Metallstents
ü Unklare Datenlagen zur Rolle der
Photodynamischen Therapie/ RFA im
Kontext der systemischen
Chemotherapie
Endoskopie: Stent und lokale Therapie
.....Verschluss nach 8 Monaten ..nach 2 Wochen
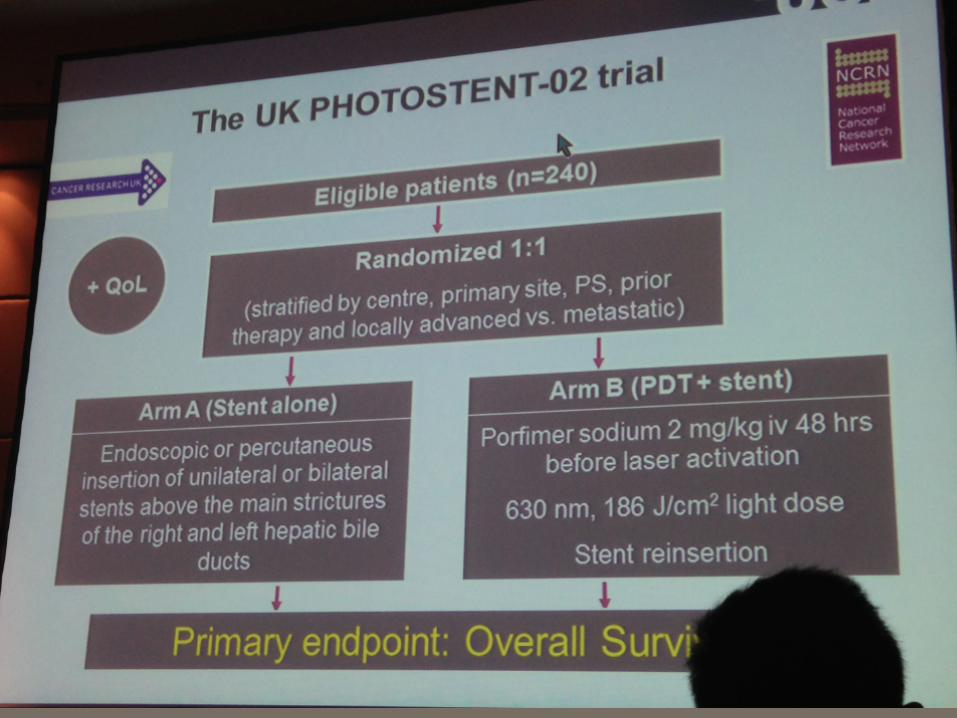
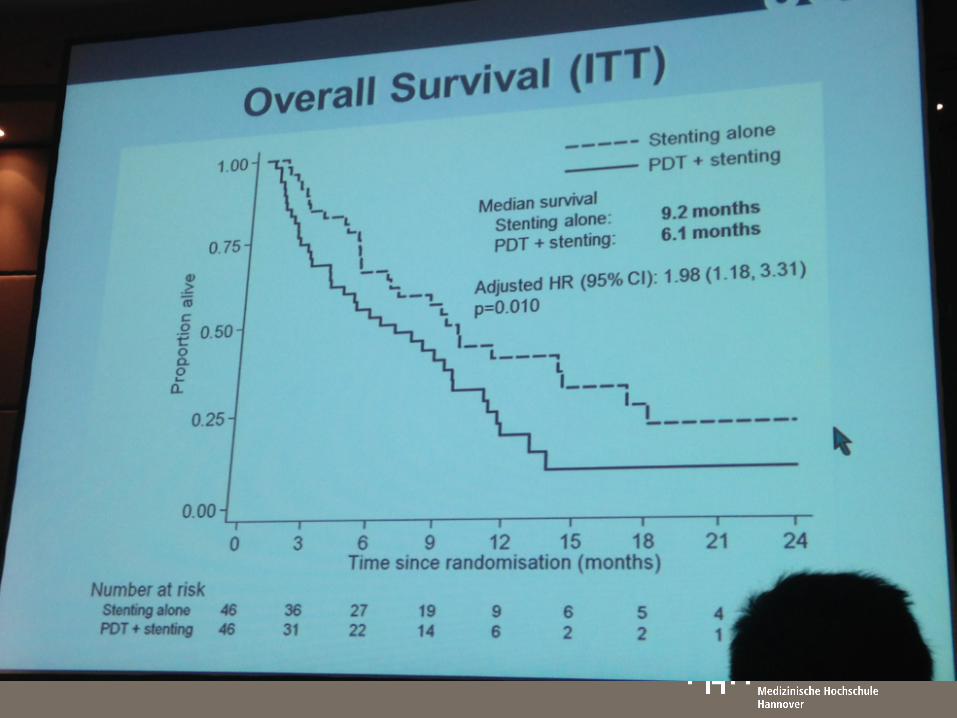
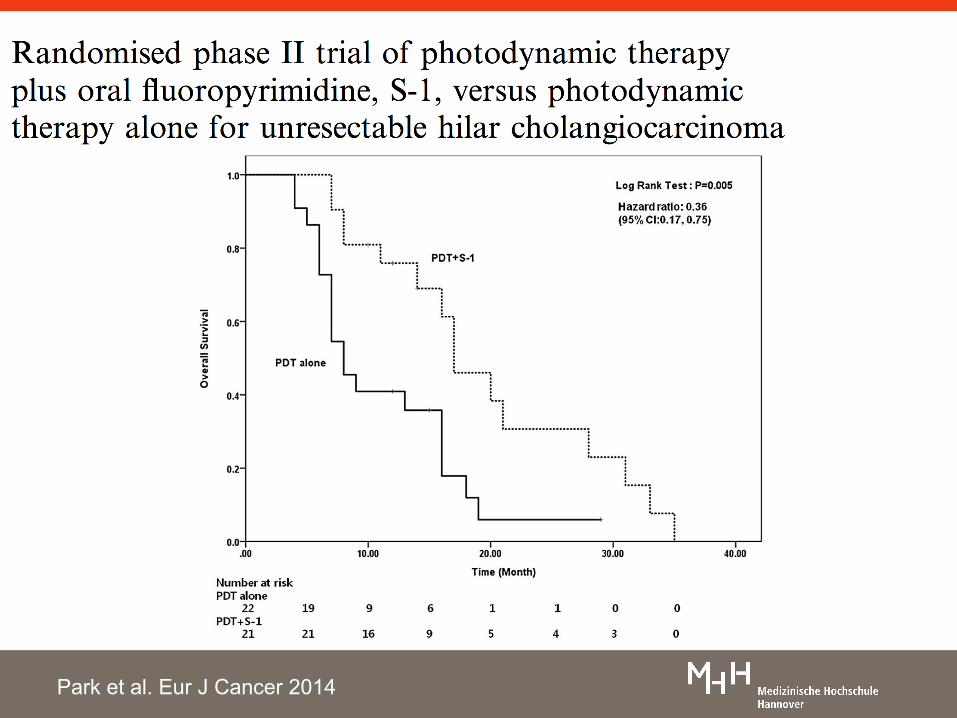
Park et al. Eur J Cancer 2014
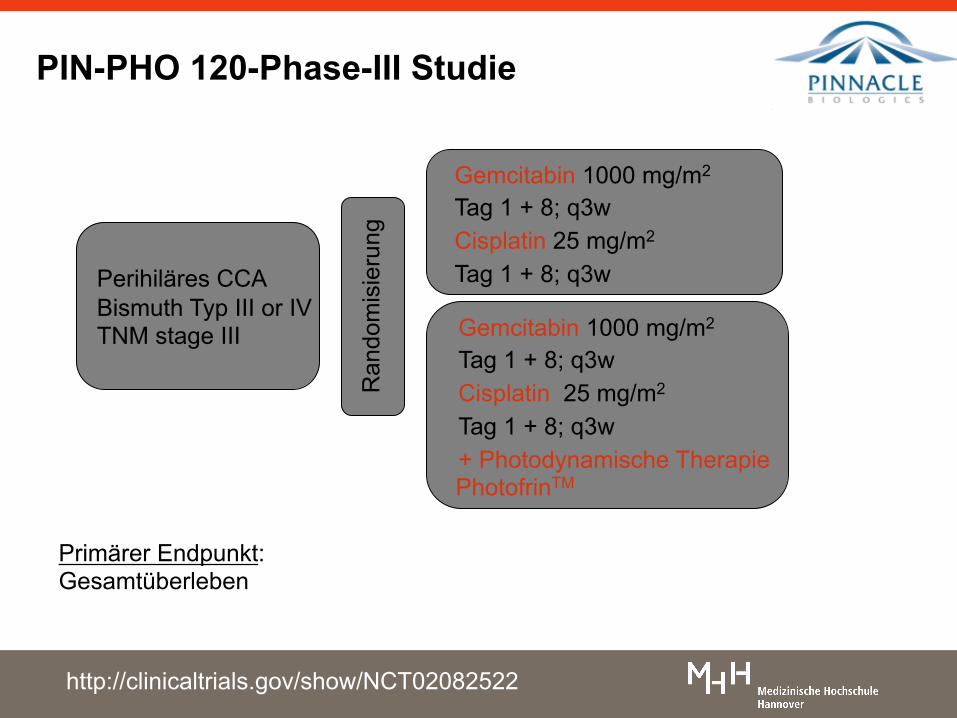
Primärer Endpunkt: Gesamtüberleben
PIN-PHO 120-Phase-III Studie
Ran
dom
isie
rung
Perihiläres CCA Bismuth Typ III or IV TNM stage III Gemcitabin 1000 mg/m2
Tag 1 + 8; q3w Cisplatin 25 mg/m2 Tag 1 + 8; q3w + Photodynamische Therapie PhotofrinTM
Gemcitabin 1000 mg/m2 Tag 1 + 8; q3w Cisplatin 25 mg/m2 Tag 1 + 8; q3w
http://clinicaltrials.gov/show/NCT02082522
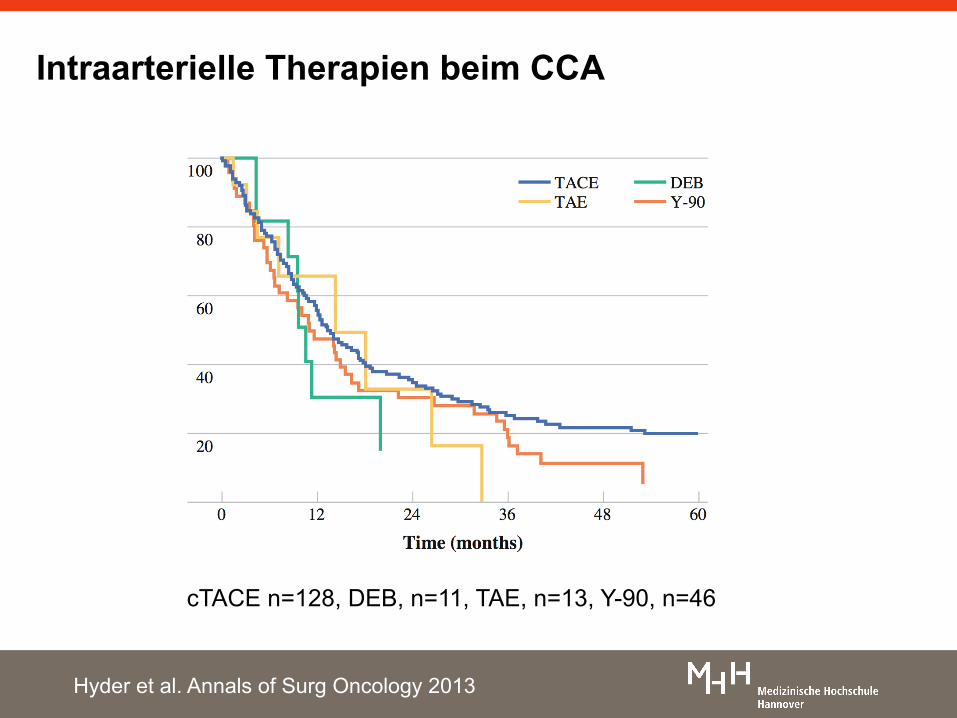
Intraarterielle Therapien beim CCA
cTACE n=128, DEB, n=11, TAE, n=13, Y-90, n=46
Hyder et al. Annals of Surg Oncology 2013
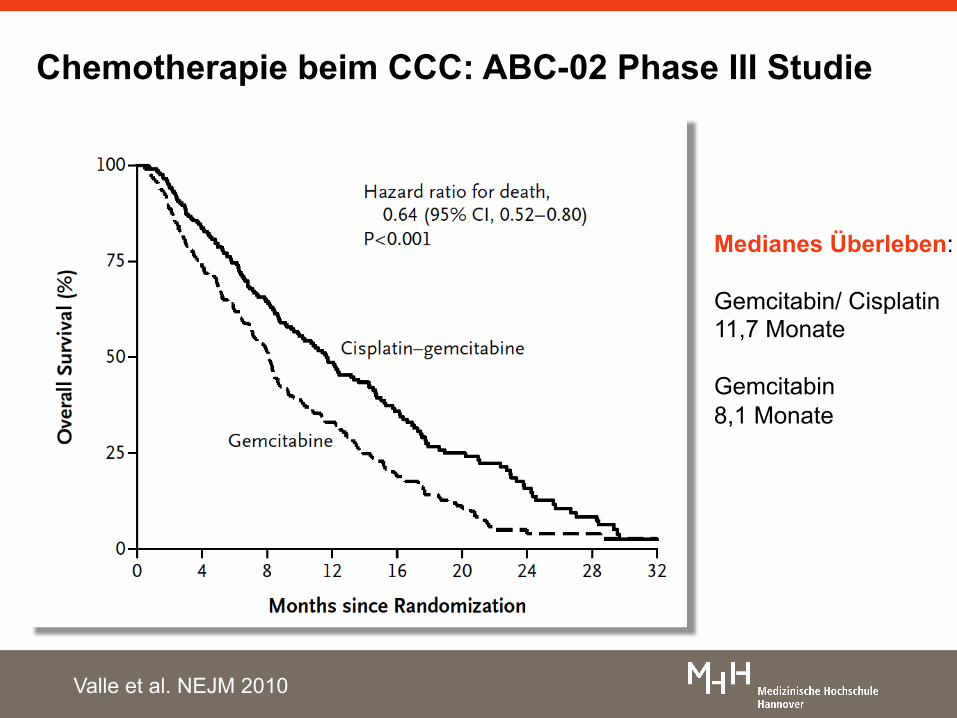
Chemotherapie beim CCC: ABC-02 Phase III Studie
Medianes Überleben: Gemcitabin/ Cisplatin 11,7 Monate Gemcitabin 8,1 Monate
Valle et al. NEJM 2010
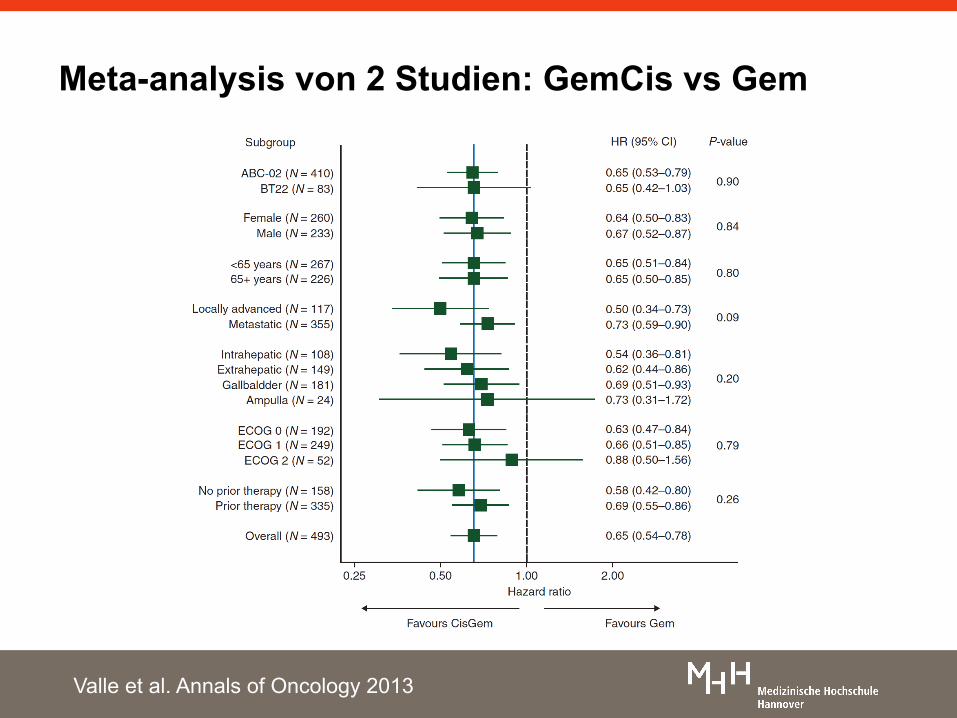
Meta-analysis von 2 Studien: GemCis vs Gem
Valle et al. Annals of Oncology 2013
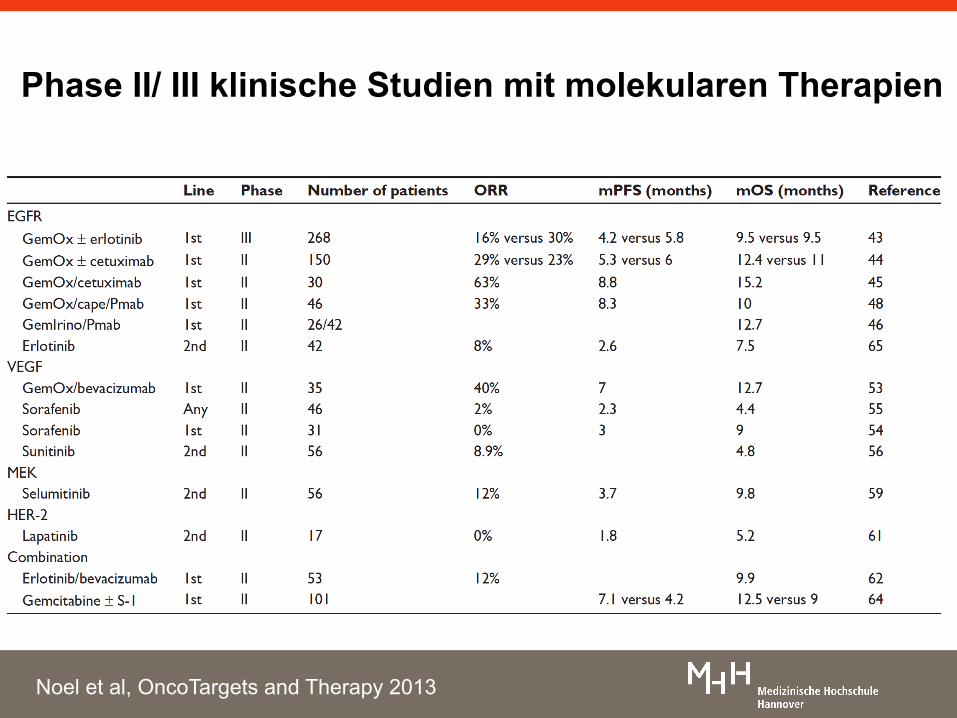
Phase II/ III klinische Studien mit molekularen Therapien
Noel et al, OncoTargets and Therapy 2013
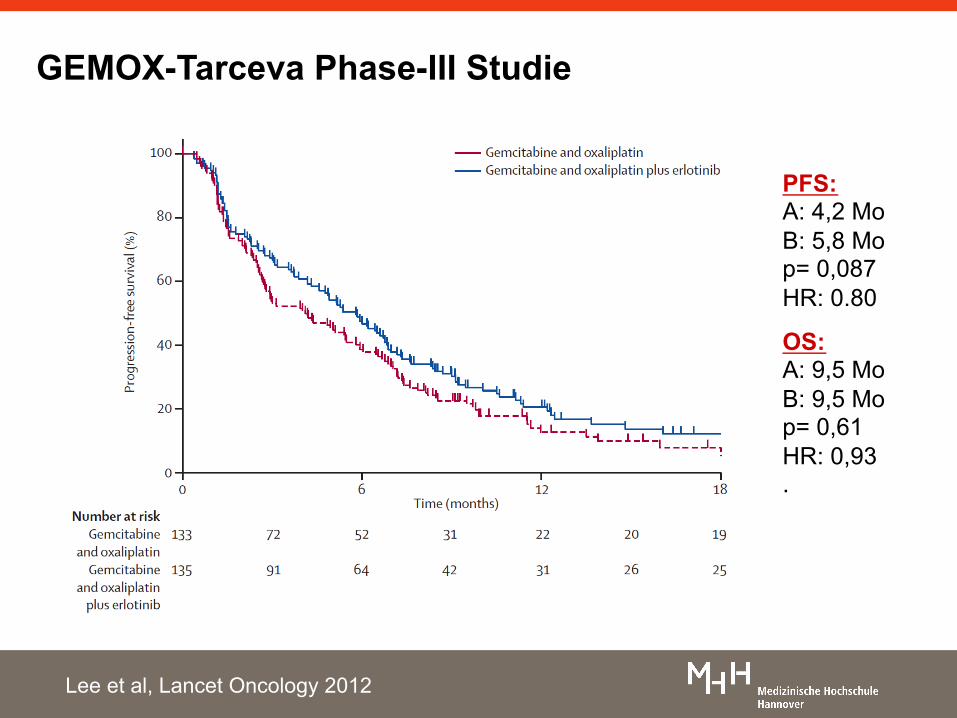
GEMOX-Tarceva Phase-III Studie
Lee et al, Lancet Oncology 2012
PFS: A: 4,2 Mo B: 5,8 Mo p= 0,087 HR: 0.80
OS: A: 9,5 Mo B: 9,5 Mo p= 0,61 HR: 0,93 .
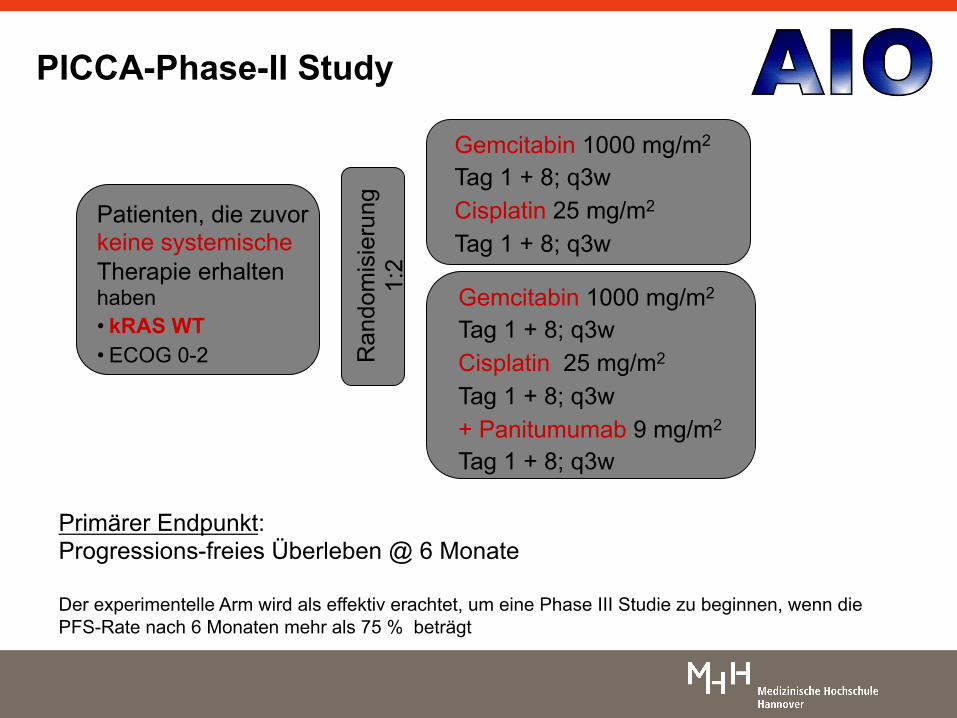
Primärer Endpunkt: Progressions-freies Überleben @ 6 Monate Der experimentelle Arm wird als effektiv erachtet, um eine Phase III Studie zu beginnen, wenn die PFS-Rate nach 6 Monaten mehr als 75 % beträgt
PICCA-Phase-II Study
Ran
dom
isie
rung
1:
2
Patienten, die zuvor keine systemische Therapie erhalten haben • kRAS WT • ECOG 0-2
Gemcitabin 1000 mg/m2 Tag 1 + 8; q3w Cisplatin 25 mg/m2 Tag 1 + 8; q3w + Panitumumab 9 mg/m2
Tag 1 + 8; q3w
Gemcitabin 1000 mg/m2 Tag 1 + 8; q3w Cisplatin 25 mg/m2 Tag 1 + 8; q3w
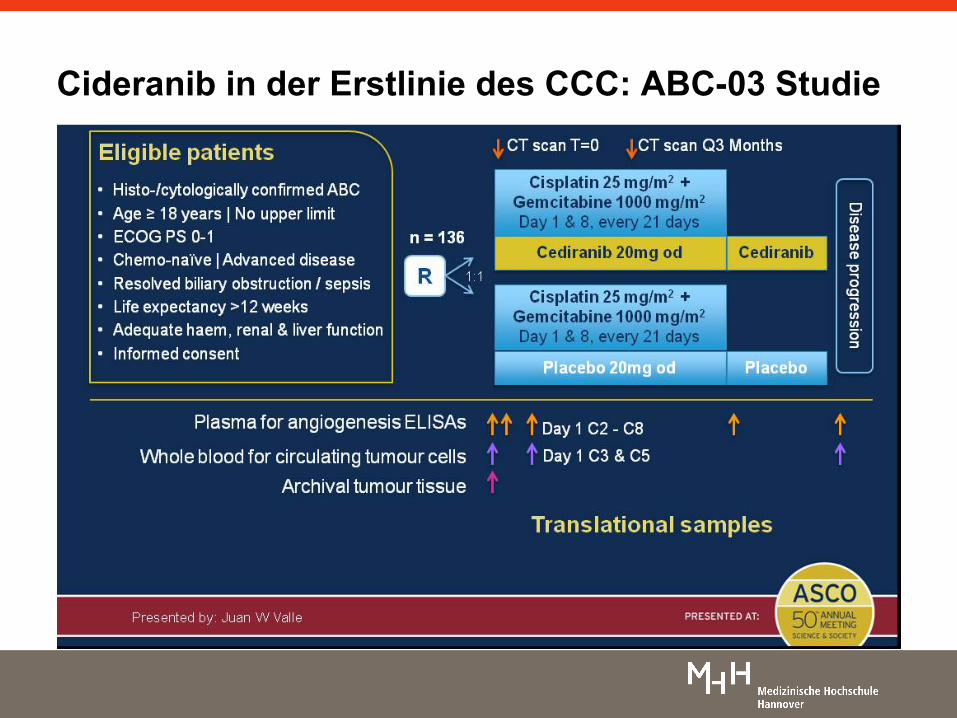
Cideranib in der Erstlinie des CCC: ABC-03 Studie
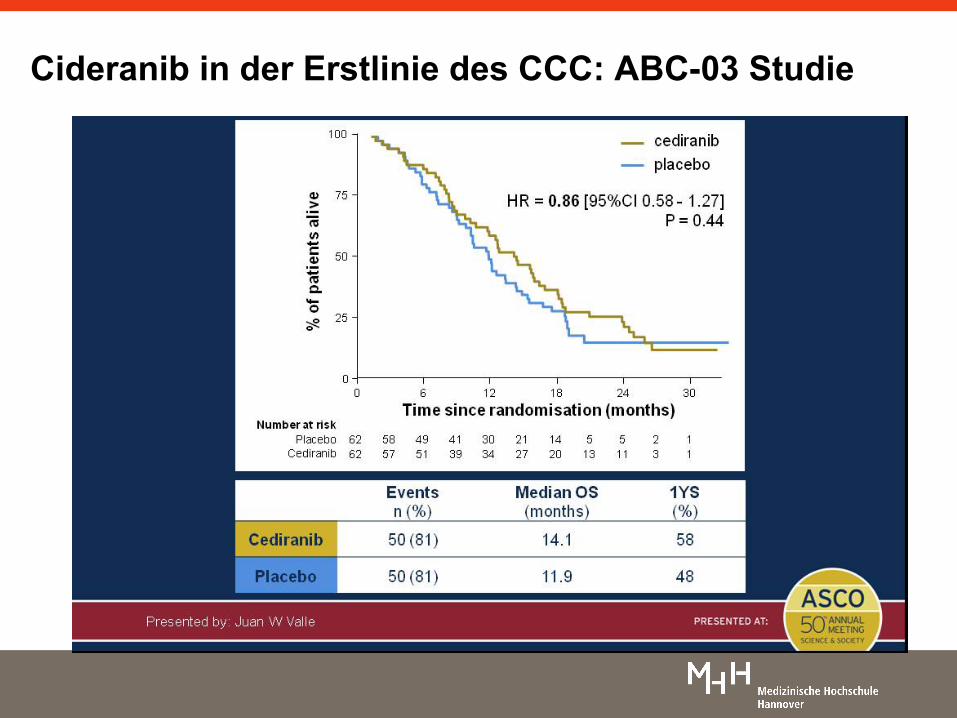
Cideranib in der Erstlinie des CCC: ABC-03 Studie
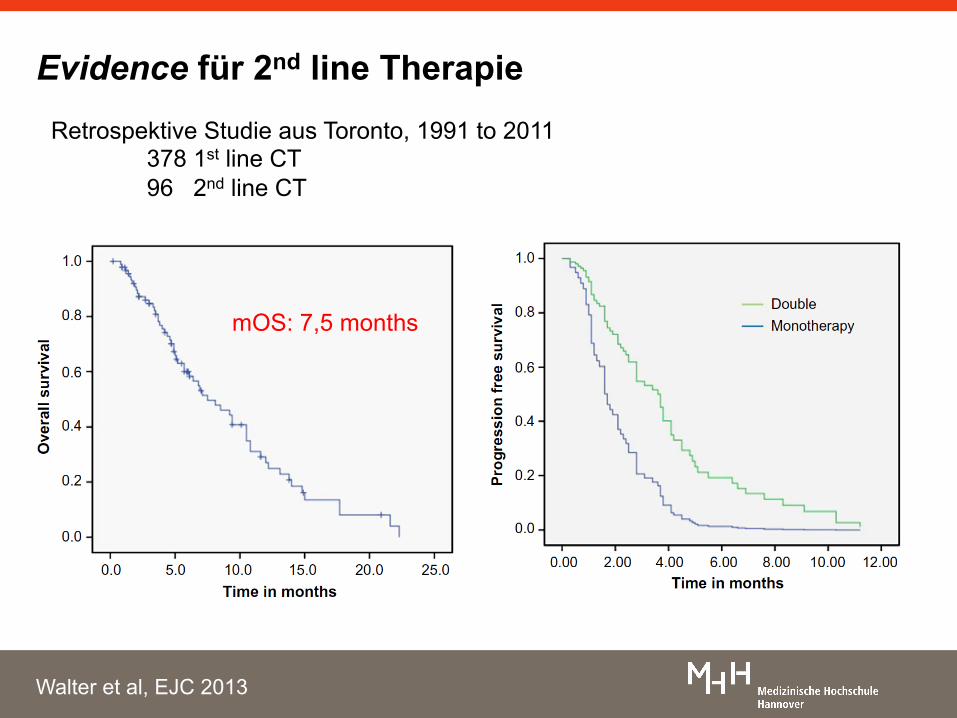
Evidence für 2nd line Therapie Retrospektive Studie aus Toronto, 1991 to 2011
378 1st line CT 96 2nd line CT
mOS: 7,5 months
Walter et al, EJC 2013
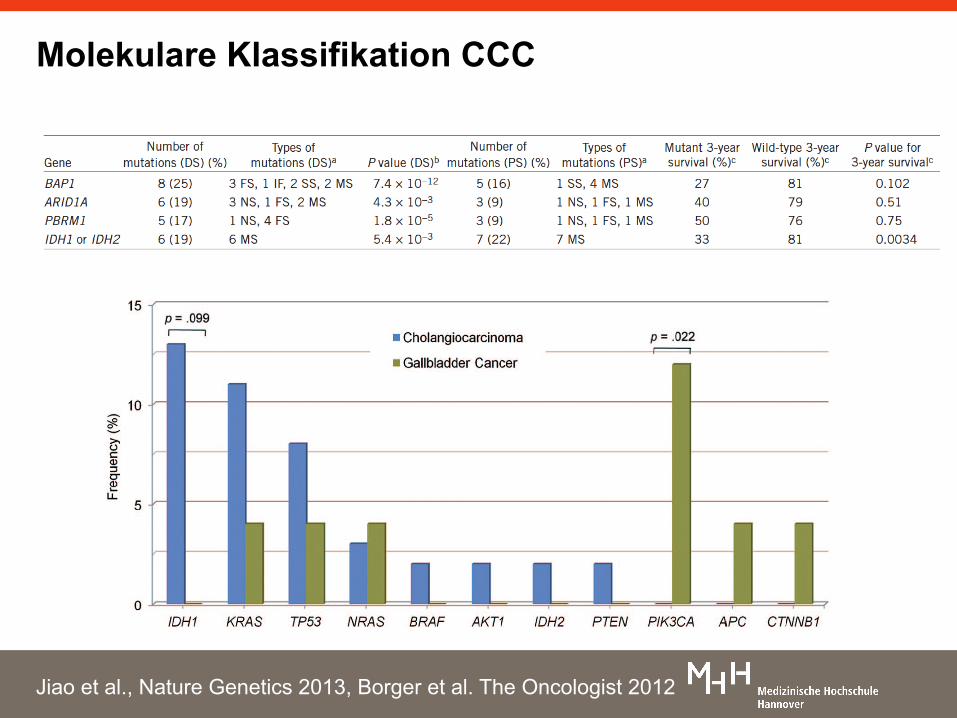
Molekulare Klassifikation CCC
Jiao et al., Nature Genetics 2013, Borger et al. The Oncologist 2012
mIDH1 Inhibitoren
Rohle et al. Science 2013
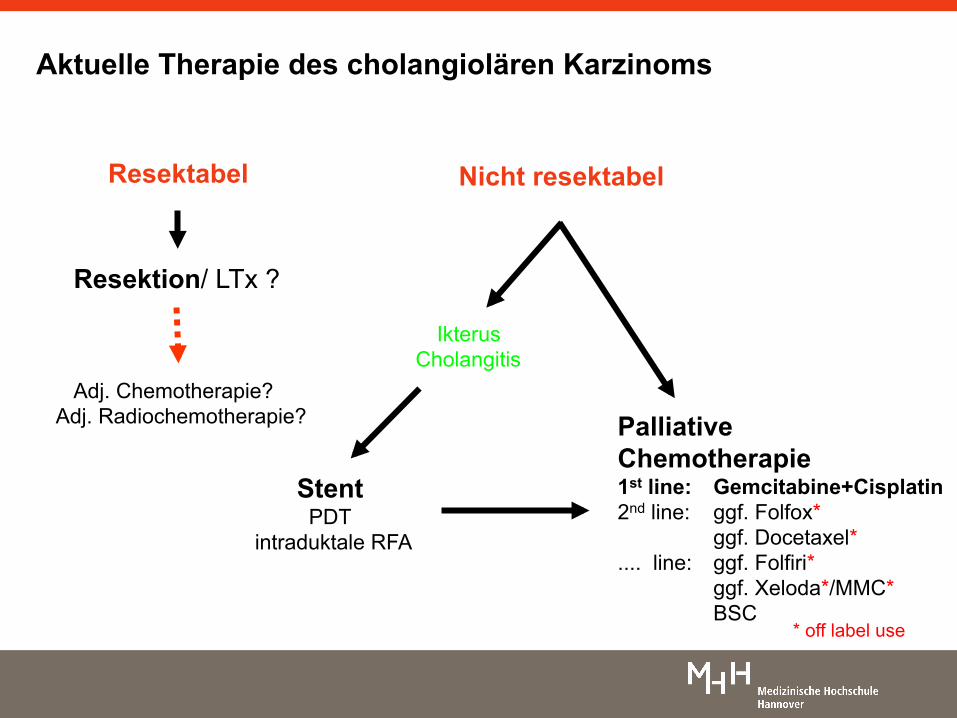
Resektabel
Resektion/ LTx ?
Stent PDT
intraduktale RFA
Nicht resektabel
Ikterus Cholangitis
Adj. Chemotherapie? Adj. Radiochemotherapie? Palliative
Chemotherapie 1st line: Gemcitabine+Cisplatin 2nd line: ggf. Folfox*
ggf. Docetaxel* .... line: ggf. Folfiri*
ggf. Xeloda*/MMC* BSC
* off label use
Aktuelle Therapie des cholangiolären Karzinoms





























