-
Christine Waszynski DNP, APRN, GNP-BC, FAANHartford Hospital
February 6, 2020
-
Hospital Inpatient
Consults & Programs
PPN SNFs/SNF programs
Home
Outpatient Geri Consults Primary Care
Geriatric oncology Co-management
APRN Home Visits/REACH
Hartford HealthCare Geriatric Continuum of Care
9 sites
8 sites
1 of 7hospitals
Serve 13 towns
-
Integration of AFHS into Hartford HealthCare
Core Values• Caring-individualized care;
dignity• Safety –promoting safe
mobilization• Excellence-evidence based
practice • Integrity-trust
4 M’s• What Matters• Medications• Mobility• Mentation
HHC Mission: To improve the health and healing of the people and
communities we serve
Goal: To provide an integrated, seamless, comprehensive care
system linking seniors and their families to the services required
and requested to maintain and restore health in alignment with
expressed patient goals/wishes.
-
Hartford HospitalHartford CT
-
Inpatient Geriatric Team Players
February 7, 2020Confidential and Proprietary Information 5
2 geriatricians1 geriatric nurse practitioner
2 masters prepared nurses with geriatric certification
GRN ChampsGRNs
GPCAsKeeping In Touch
Activity CartMeal Mates
MobilitySafety
VOLUNTEERS
-
Geriatric Education
Nursing StaffNurses• General Nursing Orientation• Nurse
Residency• Annual Competency• Geriatric Resource Nurse Program• GRN
Champ Program• Fellowships/rotationNursing Assistants• General
orientation• Annual Competency• Geriatric PCA
Other Staff Providers• New hire orientation• Grand rounds•
Geriatric consults• Geriatric rotationRehab• Inservices• Mobility
volunteer rotationsAll hospital staff• Annual competency
-
ADAPT- Making Delirium Awareness a Priority
•Began in 2012•Supported by hospital
administration•Inter-professional Team (representation across
departments and disciplines n=42)
•Plan for structure (delirium care pathway)Build supports in EHR
to guide documentation and gather dataEducation
(classroom/CESI/bedside)Adjunct Support (volunteer programs;
therapeutic activities)Quality / research/ feedback
-
ADAPT
Actions to enhance Delirium Assessment Prevention and
Treatment
Screening all patients (improve recognition)Preventative
measures for high risk patients (40% cases are
preventable)Quick response by health care team to a positive
delirium screen
(cause; safety; preservation of function) decreases severity and
duration of deliriumEvidence based interventions to improve
outcomes
-
Application of Universal Evidence-Based Best Practice
Strategies
•Information in Patient Handbook –patient and family to report
S/S of delirium promptly. Family encouraged to participate in
care
•Delirium assessment integrated into rounds and handoffs
•Early mobilization/noise reduction/ sleep enhancement
efforts
•Personalized care “Hartford HealthCare Cares About Me”
poster
-
Application of Universal Evidence-Based Best Practice
Strategies
•Creation of a sensory modulation room for patients and families
(Therapeutic HUB)
•Volunteer programs that focus efforts towards patient
experiencing or at high risk for delirium–Keeping in Touch
Volunteer Visiting Program; Meal Mates; Activity Cart; Safety
Volunteers; Mobility Volunteers
• Activated EHR alerts on medications that may cause
delirium
• Standardized provider order sets• Provide data driven feedback
to change practice
-
NO
• Document course and cause of Delirium if known
• Degree of resolution
• Discontinue unnecessary psychotropics
• Follow up for Delirium if not resolved
• Document on W10/After Visit Summary
7 Discharge
• CAM or CAM-ICU every 8 hours + prn• Comfort/calm/consistent•
Toileting• Feed/hydrate• Mobilize to maximum• Maintain normal
sleep/wake cycle• Touch/backrub• Assess response to medications•
Family & volunteer involvement• Alternative therapies (Reiki,
Pet, Art,
Music)• Document progress
5 Daily Care
• Physical exam• Med review• Determine potential
causes*• Differential diagnosis• Document acute
encephalopathy• Activate Delirium order set
in EPIC
• Diagnostics• Drugs for hyperactive
pts (RASS/mRASS ≥ +2)
• Haldol IV or Seroquel PO per delirium order set
• If contraindicated consult pharmacist
• Scheduled acetaminophen
3 Diagnosis / Do• Cognitive assessment
• F/U Diagnostics
• Review meds-adjust prn
5 Daily Visit• No harmful drugs*• Avoid abrupt
discontinuation* (Drugs, ETOH, nicotine)
• Avoid/limit Devices (catheters, lines, leads)
1 Deter
• Mobilize to maximum• Uninterrupted night-time rest
(noise, bundle care, eye shields, earplugs)
• Eyeglasses/hearing aids• Whiteboard up to date• Daily goals of
care• Calendar/clock/familiar items• Assist with food/fluids•
Comfort• “HHC Cares About Me” poster• Family as partners•
Volunteers for social interaction
1 Deter• CAM every 8 hours
and prn• Determine baseline
mental status• Notify provider
immediately of firstpositive CAM or CAM-ICU and activate “Acute
Confusion” CPG
2 Detection• Fall prevention• Discontinue/ Disguise devices•
Family teaching - brochure• Provide Distractors (music,
flashball, animal)• T-A-D-A (Tolerate, Anticipate,
Don’t Agitate)1
• Reassurance• Individualize plan of care in
EPIC• Nurse - Nurse handoff• Nurse - PCA handoff
3 Do
• Review CAM/CAM-ICU & RASS/mRASS Scores
• Daily cognitive assessment
• Determine baseline mental status
2 Detection
• Document successful strategies
• Discuss ongoing needs• Discharge with one time
use Distracters (doll, animal)
• Discuss follow-up with family
• Document individualized care needs on W10/After Visit
Summary
7 Discharge
CAM or CAM-ICU Positive
PROVIDE
R
PATIEN
T
NURSES
• Age > 65
• Dementia• Substance Dependency• Hx Delirium• ICU/SD• Impaired
vision/hearing
Risk Factors• ED screen
of pts age >65
• Attention screen
• SQID?
• Provider + Nursing • +/- Pharmacist
• Huddle• Make Plan
4 Discuss
• Provider + Nursing • +/- Family
• Progression Rounds
• Is Patient Improving?
6 Daily Dialogue Age > 65:• Geriatric medicine consult
Age < 65 or major psychiatric Dx:
• Psychiatric consult• Family meeting
*see back of brochure for more information 1 Flaherty, 2011
NO
-
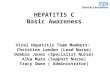
30 Day All Cause Readmission Rates Over Time
-
Outcome: Decreased Length of Stay In Patients with Delirium
ADAPT DATA
0
2
4
6
8
10
12
14
16
18
4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3
2012 2013 2014 2015 2016
Day
s
CAM NEG
CAM POS
February 7, 2020ADAPT Program - Hartford Hospital 13
-
Delirium Attributable DaysADAPT Data
February 7, 2020Confidential and Proprietary Information 14
0
5000
10000
15000
20000
25000
30000
35000
40000
45000
2013 2014 2015 2016 2017 2018
To
tol D
ays
Year
-
ROI Calculator Applied to ADAPT
-
2.26
2.50
2.06
2.33
2.56 2.53
1.932.06
2.40
2.10
2.33
2.06
2.602.50 2.50
2.97
2.66
2.90
2.302.40
2.60
2.27
1.90
2.102.00
1.90
0.260.36 0.40
0.23 0.17 0.20 0.10
0.30 0.300.23 0.26
0.36 0.40 0.30 0.260.40 0.40
0.300.43
0.530.37 0.37
0.230.40 0.36 0.30
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
Q3-
2013
Q4-
2013
Q1-
2014
Q2-
2014
Q3-
2014
Q4-
2014
Q1-
2015
Q2-
2015
Q3-
2015
Q4-
2015
Q1-
2016
Q2-
2016
Q3-
2016
Q4-
2016
Q1-
2017
Q2-
2017
Q3-
2017
Q4-
2017
Q1-
2018
Q2-
2018
Q3-
2018
Q4-
2018
Q1-
2019
Q2-
2019
Q3-
2019
Q4-
2019
Average Quarterly Falls
Average Monthly # of Falls Per 1000 pt Days
Average Monthly # of Falls with Injury Per 1000 pt Days
-
Assisted falls data
-
Safe Mobilization
February 7, 2020Confidential and Proprietary Information 18
• Mobility volunteers since 2011 (PT or other health profession
students) • 17,500 mobility episodes
• Implemented Gait belt and walker for all mobilization of high
fall risk patients
-
Bed Exercises- increase patient engagement in care
-
2/7/2020Place Title Here in Header and Footer 20
-
February 7, 2020Confidential and Proprietary Information 21
-
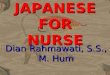
Personalized activities for patients with cognitive
impairment
• Observations were made on 74 agitated patients over a 6 month
period.
Chart1
Positive Response
No Change
Response One Hour After Compared to Prior
Response One Hour After Compared to Prior
47
27
Sheet1
Response One Hour After Compared to Prior
Positive Response47
No Change27
To resize chart data range, drag lower right corner of
range.
-
Family Video Messaging
February 7, 2020Confidential and Proprietary Information 23
• Non pharmacological intervention to:
Provide comfort and connection to agitated patients with altered
mental status
Engage families in care
Provide comfort to families
Offer a personalized intervention for staff
-
Example of Family Video Message
February 7, 2020Confidential and Proprietary Information 24
-
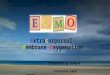
% of Participants Experiencing a Decrease in Agitation
February 7, 2020Confidential and Proprietary Information 25
0
10
20
30
40
50
60
70
80
90
100
Pre- During Pre- Post Pre- 30 min post
% R
edu
ctio
n in
AB
S S
core
Time Points
Family
Nature
Usual
-
The Therapeutic HUB
HealingUnderstandingBelief in patient as person
-
The Therapeutic HUB multi-sensory stimulation environment
February 7, 2020Confidential and Proprietary Information 27
-
February 7, 2020Confidential and Proprietary Information 28
Patients may feel safer and more “normalized” in a controlled,
multisensory environment compared
to a clinical, hospital room
-
Findings to date Jan 2018-2020Approximately 400 patients worked
with a
nurse in the HUBMost have altered mentation
(dementia/delirium/both)
• Agitated patients become more calm• Withdrawn patient become
more engaged• Improved eating• Improved mobilization• Improved
mood
Families express increased satisfaction Opportunities for
education
Staff implement bedside activitiesItems brought to bedside for
those who can
not visit the HUB
• Qualitative data: “Feels like home”“ I feel more normal”
Pilot study suggests the HUB improves cognition and normalizes
arousal levels.
-
Benefits of Therapeutic HUB
-
Voice over powerpoint with video: Therapeutic HUB
• https://vimeo.com/266874016/f693ff3a99
https://vimeo.com/266874016/f693ff3a99
-
Our 4 M Age Friendly Health System Focus
February 7, 2020Confidential and Proprietary Information 32
• Focused on 5 inpatient units 2 medical units 1 medical
oncology unit 1 transplant medical unit 1 cardiac ICU
-
What You Can Do
What MattersNurse PCA
Discuss goals of care in rounds XPatient friendly goals on white
board X XAsk pt what matters to them today X
XMutuality/individualization in EPIC XHHC Cares About Me poster in
room X XIdentify pts for Therapeutic HUB X XIdentify pts for
Keeping in Touch X XMobilityMobilize level 5 ambulatory patients to
maximum and document distance
X X
Give exercise sheet to patients and encourage them to do them X
XMentationScreen CAM and RASS every 8 hours XNotify nurse of any
changes in patient’s behavior XActivate Acute Confusion CPG for CAM
+ pts XMedication Identify new high risk meds and discuss with
provider/pharmacist XTeach pts not to take OTC “PM” meds X
-
Unit based data collection tool
February 7, 2020Confidential and Proprietary Information 34
-
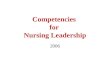
How are we doing addressing all 4 M’s with all older adults?
12% 14
%
14%
15%
12%
11%
18%
40% 4
3%
42% 4
5%
47%
42%
52%
38%
34% 37
%
33% 34
%
39%
25%
9% 8% 8% 8%
5%
8%
5%
0% 1%
0% 0% 1%
0% 0%
J ANUARY FEBRUARY MARCH APRIL MAY JUNE JULY
% OF NUMBER OF 4-M'S COMPLETED FOR ALL UNITS
4 Completed 3 Completed 2 Completed 1 Completed 0 Completed
-
How are we doing with each of the M’s with all older adults?
39%42% 40% 42% 41%
36%38%
85% 83%87% 87%
81%85%
88%
73% 74% 73% 74%77%
74%
83%
60%
67%63% 65%
66%
60%
73%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19
Percentage of 4-M's by Month all Units combined
What Matters Medication Mobility Mentation
-
56%45%
67%
0%
100% 100%
0%
20%
40%
60%
80%
100%
120%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
CollaboRATEB10I Percent of Perfect Scores
8.98.3
8.78.0
9 98.3 8.5
9.0 9.0 9 98.5
8.1
9.0
4.0
9 9
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
AVERAGE
SCORE
CollaboRATE B10I Average Scores
Question #1
Question #2
Question #3
-
Mentation
-
0%
20%
40%
60%
80%
100%
120%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
Mentation Protocol Completionfor Unit B10I
CAM every 8Hrs.
RASS every 8Hrs.
Baseline Done on Admit
Do CAM+RASS = Notes
CAM Pos. Intervention
-
0%50%
100%150%
Percentage of Patients with Delirium Screening at least 3x in a
24 hr period for Unit B10I
0%20%40%60%80%
100%120%
Percentage of Patients with RASS done every 8Hrs. for
Unit B10I
0%20%40%60%80%
100%120%
Percentage of Patients withBaseline Mental Status done
on Admit for Unit B10I
0%50%
100%150%
Percentage of Patients where CAM+RASS = Notes for Unit
B10I
-
0%
20%
40%
60%
80%
100%
120%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
Percentage of Patients with Positive CAM Intervention for
Unit
B10I
75%
79% 79%
76%
82%
70%
83%
64%66%68%70%72%74%76%78%80%82%84%
Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19
Percentage of Patients withDelirium screening at Least 2x/24
hour
PeriodB10I
-
Mobility
-
0%
20%
40%
60%
80%
100%
120%
Mobility Protocol Completion Unit B10I
Exercise Sheet in Room
Doc. Of Exercises in EPIC
Amb. >150/24hrs.
-
0%
20%
40%
60%
80%
100%
120%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
Percentage of Patients withExercise Sheet in Room
Unit B10I
0%
20%
40%
60%
80%
100%
120%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
Percentage of Patients withExercises Charted in EPIC
Unit B10I
0%
20%
40%
60%
80%
100%
120%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
Percentage of Level 5 Patients withAmbulation >150/Day
Unit B10I
-
0 0 0 0 0 0 0 00
0.2
0.4
0.6
0.8
1
Number of Patients withAssisted Falls Without a Gait
BeltB10I
10.0%13.2% 14.9% 12.7%
23.4%
4.2%
34.3%
0.0%
10.0%
20.0%
30.0%
40.0%
Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19
Percentage of Patients withDocumented Mobility
Screening( Progressive mobility Level)
B10I
-
What Matters
-
0%
20%
40%
60%
80%
100%
120%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
"What matters" Protocol Completionfor Unit B10I
HHC Cares Poster
Pt. Goals on W.B.
G.O.C. in EMR
Mutuality/EPIC
-
0%
20%
40%
60%
80%
100%
120%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
Percentage of Patients with HHC Cares About Me Poster in
Room for Unit B10I
0%10%20%30%40%50%60%70%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
Percentage of Patients with Advanced Directive/Goals of
Care in EMR for Unit B10I
0%
20%
40%
60%
80%
100%
120%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
Percentage of Patients withPatient Friendly Goals on White
Board for Unit B10I
0%
20%
40%
60%
80%
100%
120%
Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
Percentage of Patients with Mutuality/Individualization in
EPIC for Unit B10I
-
22.5%
31.6%
42.5%
31.6%
49.4%
38.0%
31.4%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19
Percentage of Patients withAdvanced Directive/Goals of Care
in
EMRN = All Pts. 65 and Over
B10I
-
1.3%
0.0%
1.1%
2.5% 2.6%
4.2%
2.9%
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
4.5%
Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19
Percentage of Patients withMutuality/Individualization in
EMR
N = All Pts. 65 & OverB10I
-
0 0 0 0 0 0 00
0.10.20.30.40.50.60.70.80.9
1
Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19
# of Patients withVisits to Theraputic Hub
B10I
00
0.10.20.30.40.50.60.70.80.9
1
Aug-19
# of Patients withK.I.T. Visits
B10I
-
12% 14%
14%
15%
12%
11%
18%
40% 43
%
42% 45
% 47%
42%
52%
38%
34% 37%
33%
34% 3
9%
25%
9% 8% 8% 8%
5%
8%
5%
0% 1%
0% 0% 1%
0% 0%
J ANUARY FEBRUARY MARCH APRIL MAY JUNE JULY
% OF NUMBER OF 4-M'S COMPLETED FOR ALL UNITS
4 Completed 3 Completed 2 Completed 1 Completed 0 Completed
1% 1%
6%
1%
4% 6% 6%
19%
25%
32%
24%
32%
23%
31%
50%
47%
40%
49%
48% 5
2%
46%
30%
25%
21% 2
5%
13%
20%
14%
0% 1%
1% 0%
3%
0%
3%
J ANUARY FEBRUARY MARCH APRIL MAY JUNE JULY
% OF NUMBER OF 4-M'S COMPLETED FOR UNIT B10I
4 Completed 3 Completed 2 Completed 1 Completed 0 Completed
-
39% 42% 40% 42% 41% 36% 38%
85% 83% 87% 87% 81% 85%88%
73% 74% 73% 74%77% 74%
83%
60%67%
63% 65% 66% 60%
73%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19
Percentage of 4-M's by Month all Units combined
What Matters Medication Mobility Mentation
24%
43% 44%33%
51%
38%31%
86%80% 84% 81%
71%
96%
80%
10% 13%15% 13%
23%
4%
34%
75% 79% 79% 76%82%
70%
83%
0%
20%
40%
60%
80%
100%
120%
Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19
Percentage of 4-M Completion for Unit B10I
What Matters Medication Mobility Mentation
-
Medications
-
0
10
20
30
40
50
60
70
80
90
May-19 Jun-19 Jul-19 Aug-19
Types of Prescriptions by MonthUnit B10I
Atypical Antipsychotics
Typical Antipsychotics
Benzodiazepines
Diphenhhdramine
Haldol
Muscle Relaxants
Sedative Hypnotics
Trycyclics
-
6 0
123
0 0 0 0 60
50100150
B10I Prescribed Medications
July 2019
AtypicalAntipsychotic
s
TypicalAntipsychotic
s
Benzodiazepines
Diphenhhdramine Haldol
MuscleRelaxants
SedativeHypnotics Trycyclics
CB2 132 18 1150 212 18 30 83 0CB3 157 7 670 123 12 22 105 33CB4
107 8 840 411 12 79 123 19CB5 281 23 1091 91 31 62 182 54B10I 6 0
123 0 0 0 0 6
0200400600800
100012001400
Axis Title
Prescribed MedicationsUnit Comparison
June 2018 - August 2019
CB2
CB3
CB4
CB5
B10I
-
The CESI mobile program
February 7, 2020Confidential and Proprietary Information 57
-
Post-Acute Care (PAC) experience
• 16-23% patients in sub-acute care enter with or develop
delirium• Poor progress toward standard goals
– D/E impairs participation– SNF generally lack skills and
strategy to rehabilitate and successfully
convalesce a delirious patient. No systematic studies to date. •
Sparse programming/expertise for cognitive rehabilitation•
Complicated by management ‘missteps’
– Medication choices that worsen confusion – Inappropriate goal
setting– Avoidable complications: UTI, dehydration, falls,
dysphagia,
behavioral incidents, readmissions.• Disposition dilemma
58
-
Overall Comparison
Baseline OrPre-educational intervention1
Educational Intervention1
Post-educational intervention1
Educational Intervention2
Pre-educational intervention2
Post-educational intervention2
3 to 6 monthsd1_pre d1_post d2_pre d2_post
KNOWLEDGE scores– compared across time points within
individuals
x ̅ =71.1 + 24.7 (0-100)Median=75.0
x ̅ =91.8 + 11.1 (50-100)Median=100.0
N=75Neg Ranks=4Positive Ranks=45Ties=26Z= -5.5p (2
tailed)=0.000
d1_pre vs d1_post
x ̅ =97.1 + 8.1 (75-100)Median=100.0
N=31Neg Ranks=0Positive Ranks=25Ties=6Z= -4.4p (2
tailed)=0.000
d1_pre vs d2_post
x ̅ =81.3 + 20.8 (25-100)Median=75.0
N=81Neg Ranks=3Positive Ranks=40Ties=38Z= -5.4p (2
tailed)=0.000
d2_pre vs d2_post
Wilcoxon Signed rank test was used to evaluate differences in
knowledge scores across time points. Results revealed that
Knowledge scores significantly improved post-educational
intervention 1. Median at time point 1 was 75 and at time point 2
was 100.
Results revealed that Knowledge scores significantly improved
post-educational intervention 2. Median at time point 3 was 75 and
at time point 4 was 100.
Results revealed that overall Knowledge scores significantly
improved post-2 educational interventions.Median at time point 1
was 75 and at time point 4 was 100.
-
Confidence questions
How confident are you:1. Screening for delirium
2.Assessing for acute onset/fluctuating course of mental status
different from baseline
3.Assessing for inattention
4.Assessing for altered level of consciousness
5.Assessing disorganized thinking
6.Notifying the provider of a positive CAM
-
Confidence scores– compared across time points within
individuals
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
1 2 3 4 5 6
Aver
age
Con
fiden
ce L
evel
Question
The Effects of Training on Average Confidence
-
Brownstone- Annual Wellness
Population health project:• Underserved older adults (2x the
rate of cognitive impairment than
surrounding community)• Operationalizes Annual wellness visit •
integrates 4Ms• Universal cognitive screening using mini-Cog and
CDR• Focused cognitive assessment using BrainCheck• Structured
assessment of Modifiable Factors• Wellness intervention• Fitness
Program, cognitive and physical
-
Brownstone Population seen
February 7, 2020Confidential and Proprietary Information 63
24 patients seen for focused cognitive assessment• - 17 non
English speaking, 5 english, 1 korean, 1 chinese• - Mean age 75
(57-99)• - 18 female, 6 male• - 13 referred because of Annual
Wellness Visit Screen fail; remainder referred because of
family concerns or observed compliance concerns (missed
appointments, medications, other)
Cognitive Diagnoses:• 14 MNCD, 7 mild, 5 moderate, 2 severe• 14
no previous NCD dx• 11 no previous focused medical work up for
treatable causes• 3 had core lab done in anticipation of the
consultative visit• 2 MCI• 2 Clinical Deprression• 6 NO
NeuroCognitive Disorder
-
February 7, 2020Confidential and Proprietary Information 64
-
Geriatric Oncology Program at HHC Cancer Institute
• Increased education for staffGRN and GPCA classes for in and
outpt staffAnnual geriatric oncology conference
• Geriatric assessment for newly diagnosed pts• Geriatric case
managementIntegrating the 4 Ms
-
Geriatric Oncology Program at HHC Cancer Institute
• Screen all older adults with a new cancer diagnosis using the
G8 to determine cognitive and function fitness
• Provide focused care by geriatric oncologist and geriatrician
Determine patient wishes and goalsAssess risksIntervene for
modifiable risksMake recommendations for treatment/care based upon
patient
fitness and individualized goals
-
November 2018: mG8
Pilot
-
November 2018: mG8
Pilot
-
Resource Coordinators
Transitional Care Nurses
Dementia Specialists
Geriatric Care Management
2/26/2019 69
Center For Healthy Aging Services
Hartford HealthCare
-
TCN Identified:• 92% Medication discrepancies• 82% High risk for
readmission/hospitalization• 16% Moderate risk for
readmission/hospitalization• 91% Fall risk• 35% of patients were
hospitalized within 12 months prior to seeing TCN• 43% of patients
live aloneLink to Community Services• 57% referred to certified
homecare services• 41% connected to provider• 23% linked to
caregiver services• 71% required referral to social work/resource
coordination• 24% connected to dementia specialists• 17% linked to
behavioral health services• 7.4% required referral to elderly
protective services
2/26/2019 70
Outcomes- Quality Data for TCNs
Hartford HealthCare
-
Caregiver education and support has delayed Skilled Nursing
Facility (SNF) placement by approx. 1.5 years
•N=198•Annual CT SNF =$144,000/year•18 Months CT SNF= $216,000•
Possible healthcare cost savings $42,768,000
Training for caregivers of people with dementia improves: •
Caregiver confidence • Ability to manage daily care challenges•
Supports caregivers in their role and relationship
*Mittleman, M.S., Haley, W.E., Clay, O.J., Roth, D.L. Neurology
2006;67:1592-1599 DOI: 10.1212/01.wnl.0000242727.81172.912/26/2019
71
Benefits of Dementia Education
Hartford HealthCare
-
Measurement ValueTotal patients referred to REACH 222Referred by
HHCMG provider 200Referred by non-HHCMG provider 18Active REACH
patients 170Index hospitalization rate 29.3%30 day readmission rate
5.9%Referrals from REACH to HHC 59.9%Referred to or utilizing home
health 83.8%Referred to or utilizing HHC at Home 41.4%Referred to
or utilizing hospice 32.9%Have an advance directive on file
24.8%Code status is DNR 32.9%ICP involved 63.5%Passed away 23.0%%
on Hospice among pt's who passed away 83.0%Passed away at home
60%Passed away in hospital 40%
HHCMG Geriatrics
REACH Data
-
Questions and Comments
February 7, 2020Confidential and Proprietary Information 73
Slide Number 1Slide Number 2Integration of AFHS into Hartford
HealthCareHartford Hospital�Hartford CTInpatient Geriatric Team
Players Geriatric EducationADAPT- Making Delirium Awareness a
PriorityADAPTApplication of Universal Evidence-Based Best Practice
StrategiesApplication of Universal Evidence-Based Best Practice
StrategiesSlide Number 1130 Day All Cause Readmission Rates Over
TimeOutcome: Decreased Length of Stay In Patients with Delirium �
ADAPT DATADelirium Attributable Days�ADAPT DataROI Calculator
Applied to ADAPTSlide Number 16Assisted falls dataSafe
MobilizationBed Exercises- increase patient engagement in careSlide
Number 20Slide Number 21Personalized activities for patients with
cognitive impairmentFamily Video MessagingExample of Family Video
Message% of Participants Experiencing a Decrease in Agitation�� The
Therapeutic HUBThe Therapeutic HUB multi-sensory stimulation
environment�Patients may feel safer and more “normalized” in a
controlled, multisensory environment compared �to a clinical,
hospital roomFindings to date Jan 2018-2020Benefits of Therapeutic
HUBVoice over powerpoint with video: Therapeutic HUBOur 4 M Age
Friendly Health System FocusWhat You Can DoUnit based data
collection toolHow are we doing addressing all 4 M’s with all older
adults?How are we doing with each of the M’s with all older
adults?Slide Number 37Slide Number 38Slide Number 39Slide Number
40Slide Number 41Slide Number 42Slide Number 43Slide Number 44Slide
Number 45Slide Number 46Slide Number 47Slide Number 48Slide Number
49Slide Number 50Slide Number 51Slide Number 52Slide Number 53Slide
Number 54Slide Number 55Slide Number 56The CESI mobile
programPost-Acute Care (PAC) experience�Slide Number 59Confidence
questionsConfidence scores– compared across time points within
individuals �Brownstone- Annual WellnessBrownstone Population
seenSlide Number 64Geriatric Oncology Program at HHC Cancer
Institute Geriatric Oncology Program at HHC Cancer InstituteSlide
Number 67Slide Number 68Center For Healthy Aging ServicesSlide
Number 70Benefits of Dementia Education REACH DataQuestions and
Comments