Embed Size (px)
Citation preview

209
대한안과학회지 2018년 제 59 권 제 3 호J Korean Ophthalmol Soc 2018;59(3):209-216ISSN 0378-6471 (Print)⋅ISSN 2092-9374 (Online)https://doi.org/10.3341/jkos.2018.59.3.209 Original Article
모락셀라 각막염의 임상양상과 치료 결과
Clinical Aspects and Treatment Outcomes of Moraxella keratitis
송용연1⋅방소라1⋅이태은1,2,3⋅강완석4⋅유인천1,2,3
Yong Yeon Song, MD1, Sora Bang, MD1, Tae Eun Lee, MD, PhD1,2,3, Wan Seok Kang, MD4, In Cheon You, MD, PhD1,2,3
전북대학교 의과대학 안과학교실1, 전북대학교 임상의학연구소2, 전북대학교병원 의생명연구원3, 전주푸른안과4
Department of Ophthalmology, Chonbuk National University Medical School1, Jeonju, KoreaResearch Institute of Clinical Medicine, Chonbuk National University2, Jeonju, KoreaBiomedical Research Institute, Chonbuk National University Hospital3, Jeonju, Korea
Pureun Eye Center4, Jeonju, Korea
Purpose: To analyze the clinical presentation, predisposing risk factors, and evaluate the treatment outcomes of Moraxellakeratitis.Methods: A retrospective analysis was conducted of 12 culture positive cases of Moraxella keratitis from hospital records be-tween March 2001 and November 2015 at a tertiary hospital to identify and analyze its risk factors, causative microbial organ-isms, clinical features, and therapeutic outcomes.Results: The mean patient age was 68 years (range, 46–86). The most common cause of keratitis was trauma (six eyes, 50.0%), and half of these patients had diabetes mellitus (three patients, 25.0%). Two patients (16.6%) were previously treated with pene-trating keratoplasty. The locations of keratitis involved the central (50.0%) and paracentral (50.0%) regions. Round-shaped cor-neal infiltration was found in seven eyes (58.3%), and irregular-shaped infiltration was found in five eyes (41.7%). Hypopyon was observed in five eyes (41.7%). All Moraxella isolates were susceptible to aminoglycosides and fluoroquinolones. The isolates from three patients were resistant to trimethoprim/sulfamethoxazole. The mean complete epithelial healing time was 32.4 days. The final visual acuity was 20/1,000 or less in seven eyes (58.3%). Three eyes developed corneal perforations and eventually underwent evisceration.Conclusions: In the Republic of Korea, Moraxella keratitis frequently occurs in eyes with trauma. The treatment response is very slow and has a poor visual outcome; thus, a long period of antibiotic therapy is necessary.J Korean Ophthalmol Soc 2018;59(3):209-216
Keywords: Moraxella keratitis, Predisposing factor, Trauma, Treatment outcome
■ Received: 2017. 9. 21. ■ Revised: 2017. 11. 12.■ Accepted: 2018. 2. 19.
■ Address reprint requests to In Cheon You, MD, PhDDepartment of Ophthalmology, Chonbuk National University Hospital, #20 Geonji-ro, Deokjin-gu, Jeonju 54907, KoreaTel: 82-63-250-2581, Fax: 82-63-250-1960E-mail: [email protected]
* Conflicts of Interest: The authors have no conflicts to disclose.
ⓒ2018 The Korean Ophthalmological SocietyThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
세균 각막염은 흔한 감염각막질환으로 심각한 시력손상 을 일으킬 수 있다. 각막감염의 중증도나 심각성은 감염 전
각막의 상태와 감염균의 병원성 정도에 따라 좌우된다. 그
러므로 각각의 개별 균주에 의해 발생하는 세균각막염의
다양한 임상양상 및 병태생리학적 측면을 이해하는 것은
중요하다. 모락셀라균은 세균각막염의 원인균으로 잘 알려
져 있지만 드물게 발견되는 균이다. 이전 연구에 따르면 미
국과 인도에서 세균배양으로 검출된 각막염 중 30%를 차
지한다고 하였다.1 일본에서 진행된 관찰연구에서는 세균,
진균, 아칸토아메바균이 포함된 범주의 각막염 검체에서

210
-대한안과학회지 2018년 제 59 권 제 3 호-
배양된 유기체 중에서 3.8%를 차지한다고 발표하였다.2 모
락셀라균은 그람 음성 구간균으로 호기성, 비운동성의 특
징을 가지며, 주로 상기도, 피부, 비뇨생식기 등에 서식하는
상재균이지만, 숙주 상태에 따라 병원성을 나타낸다.3-5
감염각막염은 선행 유발요인 없이 나타나는 경우는 드
물며, 이러한 성향은 모락셀라균과 같이 낮은 병원성을 띠
는 세균각막염에서 더 두드러진다.6,7 1980년 에는 모락
셀라 각막염과 만성 알코올 중독, 영양실조, 당뇨, 그리고
열악한 위생상태 등과의 연관성을 보고한 논문들이 발표
되었다.8-10 반면 1990년 이후에 발행된 논문들은 각막이
식, 단순헤르페스각막염, 콘택트렌즈 착용, 외상 등 안구
에 국한된 선행 위험인자와의 연관성을 주로 보고하였
다.3,4,11 동일한 세균각막염이라 할지라도 선행 인자는 지
리학적, 계절적 요소에 따라 다를 수 있으며, 이에 하여
국내에서 보고된 모락셀라 각막염의 임상양상을 보고한
논문은 현재까지 발표되지 않았다.
모락셀라균은 낮은 병원성을 가지고 있는 기회감염균
이긴 하나, 각막흉터, 천공, 그리고 안내염까지 심각한 시
력의 위협을 줄 수 있는 합병증을 일으킬 수 있는 균주이
다. 본 연구의 목적은 본원에서 검출된 모락셀라 각막염의
증례들을 통하여 국내의 모락셀라 각막염의 임상양상, 선
행 위험인자, 항생제에 한 감수성, 치료결과 및 예후 등
을 분석하여 기존의 해외 연구와 비교하고, 향후 치료에
도움이 되고자 한다.
대상과 방법
본 연구는 헬싱키 선언을 준수하며 진행되었다. 또한
본 연구는 본원 임상시험심사위원회의 승인을 얻고 진행
한 후향적 연구이다(IRB No. 2016-10-024-001). 후향적
차트 분석은 2001년 3월부터 2015년 11월까지 본원에서
세균각막염으로 치료받은 모든 환자를 상으로 이루어
졌다. 감염각막염은 기질의 침윤, 화농성 병변과 동반하여
각막상피의 결손을 보이는 것으로 정의하였다. 각막염 환
자들 중에서 각막 찰과를 통해 얻은 검체를 배양하여 모
락셀라균이 동정된 증례들만을 연구에 포함하였으며, 배
양 결과 진균 혹은 다른 바이러스 감염이 같이 검출된 경
우와 비감염성 각막질환은 제외하였다. 이 과정을 통하여
총 12증례가 연구에 등록되었다.
모락셀라 각막염에 하여 나이, 성별, 전신 질환, 안질
환, 선행 인자, 항생제 감수성, 치료, 상피 회복까지 걸린
시간, 경과관찰기간 등을 후향적 차트 연구를 통하여 조사
하였다. 과거력은 각막 외상력, 콘택트렌즈 착용 여부, 안
구표면질환 유무, 굴절 수술이나 각막이식과 같은 수술 기
왕력 등을 조사하였다. 각막 병변의 크기는 플루오세인 염
색으로 확인된 상피 결손에 하여, 결손의 가장 긴 직선
직경과 그에 수직인 가장 큰 직경의 수치를 곱하여 도출
된 직사각형의 면적으로 계산하였다. 각막병변은 위치에
따라 각막중심에서 3 mm 이내에 있는 경우를 중심부
(central), 각막윤부에서 3 mm 이내에 있는 경우를 주변부
(peripheral)로 나누고, 그 사이에 있는 경우는 중심주변부
(paracentral)로 정의하였다. 전방축농이 동반된 경우 그
높이를 각막하부 6시 방향에서 각막윤부로부터 전방축농
의 상단까지 길이를 밀리미터 단위로 측정하였다.
균 배양은 감염각막염이 의심되는 경우 시행하였다. 배
양검체는 0.5% Proparacaine hydrochloride (Alcaine®,
Alcon laboratory, Fort Worth, TX, USA)로 점안마취 후
개검기를 속눈썹이 닿지 않게 삽입한 후, 궤양의 기저부와
가장자리를 무균의 수술도로 긁어내어 검체를 채취한 후
염색검사(그람염색, 수산화칼륨 습식도말) 및 혈액한천배
지, 초콜릿배지, MacConkey 배지, Sabouraud’s 배지에 도
말하여 배양하였다. 배양 양성은 배지의 접종선을 따라 균
주가 자랄 때로 간주하였다. 항생제감수성 검사는 디스크
확산법을 이용하여, 접종배지에 놓인 각각의 항균제 디스
크 주위에 형성된 억제 의 직경을 측정하여 결정하였다.
이 측정은 임상검사표준협회에서 제공한 기준 프로토콜
에 준하여 해석하였다.
항생제 치료는 일반적으로 점안항생제를 첫 2시간 동안
30분마다 점안, 이후 48시간 동안 1시간마다 점안하였다.
항생제는 0.5% Moxifloxacin (Vigamox®, Alcon, Forth
worth, TX, USA) 단독, 강화된 Tobramycin 점안액과
Cefazolin 점안액 병용, Moxifloxacin 점안액과 Ceftazidime
점안액 병용, 그리고 Ceftazidime 점안액과 Vancomycin
점안액 병용 등의 방법을 사용하였다. 항생제 치료는 각막
염의 중등도, 환자의 순응도 및 임상 전문의의 선호도에
따라 다르게 선택되었다. 병변이 악화되는 경우 약물 치료
의 실패로 판단하였고, 이러한 경우 다양한 수술적 치료가
시행되었다.
결 과
모락셀라균에 감염된 12명의 환자 12안이 본 논문에서
연구되었다. 연령은 46세부터 86세로 다양하였고, 평균연
령은 68세였다. 성별은 남자 9명, 여자 3명이었다. 배양검
사 결과, 12안 모두 모락셀라 단일균이 검출되었고, 복합
균 감염은 없었다. 선행요인으로 10안(83.3%)에서 안구의
위험인자를 가지고 있었고, 그중 외상이 6안(50.0%), 이전
각막이식이 2안(16.6%)이었다(Table 1). 3명의 환자는 각

211
-송용연 외 : 국내 모락셀라 각막염의 후향적 연구-
A B
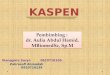
Figure 1. Representative slit-lamp photographs of Moraxella keratitis. (A) Anterior segment photograph shows small pacacentral type corneal ulceration (Case 2). His initial visual acuity was 20/500. He was well treated with topical moxifloxacin, and his final visual acuity was 20/25. (B) Anterior segment photograph shows large central type corneal ulceration with a 0.5 mm height of hypo-pyon (Case 4). His initial visual acuity was light perception. The lesion was well healed with topical ceftazidime and moxifloxacin, but the opacity remained and his final visual acuity was light perception.
Table 1. Predisposing factors associated with Moraxella kera-titis
Predisposing factorsNo. of
patients (%)Ocular factors 10 (83.3)
Ocular trauma Vegetative matters Soil/sand/stone Others
6 (50.0) 1 (8.3)
4 (33.3) 1 (8.3)
Previous ocular disease 3 (25.0) Herpetic keratitis 1 (8.3) Band keratopathy GlaucomaPrior ocular surgery Penetrating keratoplasty
Systemic factorsDiabetes mellitusHepatocellular carcinoma (anticancer therapy)Leprosy
1 (8.3) 1 (8.3) 2 (16.6) 2 (16.6)
5 (41.7)3 (25.0)
1 (8.3) 1 (8.3)
Values are presented as n (%).No. = number.
Table 2. Clinical presentations of Moraxella keratitis
No. of eyes (%)Location
Central ParacentralPeripheral
6 (50.0)6 (50.0)
0 (0.0)Shape
RoundIrregular
7 (58.3)5 (41.7)
Size≤ 6 mm2
> 6 mm2
HypopyonPositiveNegative
3 (25.0)9 (75.0)
5 (41.7)7 (58.3)
Values are presented as n (%).No. = number.
각 헤르페스 각막염, 띠각막병증, 녹내장 및 그로 인한 시
신경 위축의 과거력이 있었다. 5명(41.7%)은 전신질환을
가지고 있었고, 그중 3명(25.0%)은 당뇨를 앓고 있었다.
나머지 두 명은 각각 간세포암, 나병의 기왕력이 있었다.
5명(41.7%)은 안구 위험인자와 전신질환 둘 다 가지고 있
었다. 선행 위험인자가 없는 경우는 2명(16.6%)이었다.
각막병변의 위치는 중심부 6안(50%), 중심주변부 6안
(50.0%)이었다. 중심부에 위치한 경우 병변이 크고 최종
시력이 나쁜 경우가 많았다(Table 2). 3안(25.0%)은 병변
의 크기가 6 mm2보다 작거나 같았고, 나머지 9안(75.0%)
의 병변은 6 mm2보다 컸다. 병변의 크기가 10 mm2보다
큰 경우는 6안으로 이 중 한 명이 20/1,000의 최종시력을
보인 것을 제외하곤 모두 안전수동(hand movement, HM)
이하였다. 둥근 모양의 병변은 7안(58.3%)이었고, 불분명
한 경계를 가진 불규칙한 병변은 5안(41.7%)이었다. 전방
축농을 보인 경우는 5안(41.7%)이었으며 전방축농이 없
는 경우보다 최종시력이 나쁜 경우가 많았다(Table 2). 완
전한 상피 결손의 치유까지 걸린 시간은 12일에서 64일까
지의 분포를 보였다. 최종적으로 안구적출을 시행한 3안
을 제외한 9안의 평균 치유기간은 32.4일이었다. 본원 모
락셀라 각막염 환자의 표적인 세극등현미경 소견은 다
음과 같다(Fig. 1).
모락셀라 각막염 증례 각각에 한 치료 과정은 Table 3과
같고, Fluoroquinolone (Moxifloxacin) 단독 점안 치료는 1안,
강화된 Aminoglycoside (Tobramycin) 점안액과 Cefazolin 병용
치료는 3안이었다. 2안에 하여 Moxifloxacin과 Ceftazidime
점안액 병용치료를 시행하였고, 그 외 나머지 6안(50.0%)
에 하여 Ceftazidime과 Vancomycin 점안액 병용치료를
하였다. 모든 환자에서 전신 항생제 치료를 동시에 하였

212
-대한안과학회지 2018년 제 59 권 제 3 호-
Table 3. Management procedures for Moraxella keratitis
No. of eyes (%)Medical management (topical) Moxifloxacin alone 1 (8.3) Fortified tobramycin and cefazolin Moxifloxacin and ceftazidime
3 (25.0) 2 (16.6)
Ceftazidime and vancomycin 6 (50.0)Surgical management Penetrating keratoplasty 2 (16.6) Amniotic membrane transplantation 1 (8.3) Evisceration 3 (25.0)
Values are presented as n (%).No. = number.
고, 3명(25.0%)의 환자에서 병변이 악화되어 약물 치료의
실패로 판단 후 수술적 처치가 이루어졌다. 1안에서는 양
막이식술, 2안에서는 전층각막이식술이 이루어졌고, 이후
에도 소견이 악화되어 결국 안구내용제거술을 시행하였
다. 전층각막이식술을 하였던 Case 11의 경우 나병의 전
신병력이 있는 환자로, 이식된 각막에 병변이 있었고 항생
제 치료 후에도 호전을 보이지 않아 전층각막이식술을 시
행하였다. 이후에도 호전이 없어 각막이식술을 1차례 추
가 시행하였으나 재발하였고, 천공 임박한 소견을 보여 안
구적출술을 진행하였다. Case 12도 띠각막병증이 있는 눈
에서 발생한 궤양으로 1차례 각막이식술에도 안내염으로
발전하여 안구통이 지속되어 환자와 상의 후 안구적출술
을 시행하였다.
2안을 제외한 10안에서 항균제감수성 검사가 시행되었
다(Table 4). 모든 분리 균주에서 Amikacin, Gentamicin,
Ceftazidime, Meropenem, Ciprofloxacin, Levofloxacin에 감수
성을 보였다(Table 4). 3안의 분리 균주에서는 Trimethoprim/
sulfamethoxazole에 내성을 보였다.
12안 중에서 5안(41.7%)의 최 교정시력은 20/40 이상
이었다. 1안의 최종시력은 20/1,000이었고, 6안(50.0%)의
최종시력은 안전수동 및 그 이하였다.
Table 5는 본원에서 수집한 모락셀라 각막염 증례의 임
상양상, 치료와 결과를 정리하여 나열한 표이다. 그와 반
로 Table 6은 국외의 모락셀라 각막염 증례를 발표한 논문
을 분석하여 그 치료와 결과를 정리하여 나열한 표이다.
고 찰
모락셀라균은 상기도, 비뇨생식기, 사람의 피부 표면에
서 관찰되는 상재균이다.5 모락셀라 각막염은 모든 세균각
막염의 약 1-5%를 차치한다고 알려진 드문 질환이다.1,5,12
국내에서 진행된 몇몇 연구에서는 배양 증명된 각막궤양
의 0.2-0.6%를 차지한다고 알려져 있으며 이는 국외의 연
구보다 더 낮은 확률이다.13,14 본 연구는 이런 모락셀라 각
막염의 증례에 해서 다룬 국내의 첫 논문이다.
모락셀라 각막염은 알코올 중독, 당뇨, 면역저하자 등의
전신적 선행 위험인자를 가진 사람에게서 더 잘 발생할
수 있는 기회감염균이다.8,15,16 그러나 안구의 위험인자 또
한 모락셀라 각막염을 일으키는 데 중요한 인자로 인식되
고 있다. Cobo et al16은 모락셀라 각막염 환자 중 87.5%
에서 전신적 선행 위험인자가 없었으며, 만성적인 각막상
피 이상의 안구 위험인자가 가장 중요한 선행요인이라고
보고하였다. Inoue et al5에 따르면 배양된 30안의 모락셀
라 각막염 증례에서 안구 위험인자만을 가진 경우는
53.3%인 반면, 전신 위험인자와 안구 위험인자를 동시에
가지고 있는 경우는 23.3%로 보고하였다. 또한 전신 위험
인자에서는 주로 당뇨가 많았고, 안구 위험인자에서는 콘
택트렌즈 착용, 외상, 기타 안구표면질환이 부분이었음
을 보고하였다.5 본 연구에서는 10명(83.3%)의 환자에서
안구 위험인자를 가지고 있었고 그중 5명은 안구 위험인
자와 더불어 당뇨와 같은 전신질환을 가지고 있었다. 안구
위험인자는 외상이 6명(50.0%)으로 부분을 차지하였다.
하지만 오히려 외상으로 각막염이 발생한 환자들 6안 중
4안에서 20/25 이상의 좋은 시력 예후를 보였다. 또한 선
행 안구 위험인자와 전신인자를 동시에 가지고 있는 환자
5안 중 4안에서 20/1,000 이하의 좋지 않은 시력 예후를
보여 조를 이루었다. 본 연구에서 선행요인이 없던 2예
에 해서, Case 2의 경우 안외상의 기왕력과 전신인자가
없으나, 병력청취에서 직업상 먼지가 많은 야외활동을 주
로 한다고 하였고, 이로 인하여 이물이 눈 안에 들어가 감
염이 일어났을 가능성이 있다고 추측하고 있다. Case 3의
경우 특별한 안구 위험인자는 없으나, 환자가 뇌경색으로
인하여 마비 및 인지 기능 저하가 있어 거동을 못하고 침
상생활을 오래하였던 분으로, 전신상태의 악화로 인하여
발생하였을 가능성이 있다고 판단하였다. 그러나 본 연구
에서는 기존의 연구들과는 달리, 알코올 중독이나 영양실
조의 전신적 인자, 콘택트렌즈 착용의 선행요인을 가진 환
자는 없었다.
모락셀라 각막염의 임상적인 특징은 크게 두 가지 형태
의 각막궤양 양상을 보인다고 알려져 있다. 하나는 경도
의 전방 세포 반응을 동반한 무통성의 중심주변부 혹은
주변부 각막궤양이며, 다른 하나는 깊숙한 각막실질 침범
과 전방축농, 천공 위험을 동반한 각막 중심부의 궤양이
다.3,4,8,11 본 연구의 환자는 모두 중심부 혹은 중심주변부
각막궤양으로 위의 두 형태 모두 관찰할 수 있었다. 그리
고 중심주변부 각막염의 경우 전방축농을 보이는 경우는
없었고, 중심부 각막궤양 환자 6명 중 5명에서 전방축농

213
-송용연 외 : 국내 모락셀라 각막염의 후향적 연구-

214
-대한안과학회지 2018년 제 59 권 제 3 호-

215
-송용연 외 : 국내 모락셀라 각막염의 후향적 연구-
이 관찰되었다. 또한 궤양의 위치가 시력의 예후와 연관이
있었다. Garg et al4은 모락셀라 각막염을 궤양 위치에 따
라 중심부, 주변부로 나누었다. 그중에서 중심부 궤양 형
태가 병변의 정도가 더 심하며 천공이 잘 일어났다. 본 연
구에서 중심부에 발생한 궤양 6안 중 3안에서 안구적출을
시행하였고, 나머지 중 2안의 최종시력은 각각 광각없음,
20/1,000이었다. 반면에 중심주변부 병변의 각막염 6안 중
4안의 최종시력은 20/40 이상으로 조를 보였다. 이러한
결과들은 최종시력이 각막 침윤과 흉터의 위치에 의하여
영향을 받음을 시사하고 있다.
모락셀라 각막염은 다른 각막염에 비하여 비교적 각막
상피의 회복기간이 오래 걸린다고 알려져 있다. 이전의 논
문들에서, 이 기간은 3-102일에 걸쳐 다양하였다. Inoue et
al5은 평균 회복기간이 41.9일이었음을 보고하였고, Das et
al3은 35일로 보고하여 모락셀라 각막염이 치료에 늦게 반
응할 수 있음을 제시하였다. 본 연구의 경우, 완전한 각막
상피의 평균 회복기간은 32.4일로 기존의 논문들과 유사
한 결과를 보였다. 회복기간이 긴 정확한 원인은 알려진
바 없지만, 모락셀라균이 각막에 지속적인 염증반응을 일
으켜 치료에 오랜 기간이 필요한 것으로 생각된다.
Aminoglycoside 점안액은 녹농균과 모락셀라와 같은 그람
음성균에 흔히 사용되었던 치료이다.17 근래에 Fluoroquinolone
점안액은 항생제의 적용 범위가 넓은 덕분에 다양한 세균각막
염의 치료에 사용되고 있다.17-20 기존 연구들은 모락셀라 균주가
Aminoglycoside, Fluoroquinolone, Cephalosporin에 좋은 감수성을
보이며, 몇몇 연구는 Cefazolin에 내성을 보인다고 하였다. 본
연구 또한 Aminoglycoside, Fluoroquinolone, Cephalosporin 점안액
치료에 좋은 반응을 보였다. 놀라운 점은 본 연구에서 내성을 보
인 약제는 Trimethoprim/Sulfamethoxazole뿐으로 Ciprofloxacin과
Levofloxacin에 저항성을 보인 균주가 없었다. 그러므로 최근
새로운 세 의 Fluoroquinolone은 모락셀라 각막염의 단독치료
에 더 나은 선택이 될 수 있다고 생각된다.
추가적인 수술적 처치는 임상소견에 따라 종종 사용되
는 필요한 방법으로 Stern21의 모든 증례와 Marioneaux et
al8의 전체의 절반에 해당하는 환자들에게서 수술적 처치
가 필요하였다. 또한 Das et al3은 95명의 환자 중 8예에서
전층각막이식술을, 3예에서 안구내용제거술을 보고하였
다. 반면 Inoue et al5은 30안 중에서 각막염이 악화되어
수술적 처치가 필요하였던 증례는 한 건도 없었다고 보고
하였다. 본 연구에서는 25.0%에 해당하는 3명의 환자에서
최종적으로 안구내용제거술을 시행하였다. 3명 모두 초기
병변이 크고 전신상태가 불량하며 노출각막염이나 띠각
막병증과 같이 선행 안구표면질환이 있는 경우에 시행하
여 선행 위험인자가 있거나 병변이 큰 경우에는 초기부터
적극적인 약물치료 및 수술적 치료가 필요할 것으로 사료
된다.
모락셀라 감염은 다른 균들에 비해 상 적으로 병원성
은 낮으나 눈꺼풀염과 결막염, 각막염과 각막천공을 포함
하는 심한 실질침범의 궤양까지 다양한 임상 경과를 보이
는 균주이다.3 다른 각막염과는 다르게 전신 인자가 동반
된 경우 더 잘 나타날 수 있으며, 본 연구에서 전신인자와
안인자가 동반된 경우 더 안 좋은 시력 예후를 보임을 보
았을 때, 전신인자를 가진 환자에게 나타난 각막염에 해
주의 깊게 염두에 두어야 할 균주이다.
본원에서의 연구를 토 로 한 결론은 다음과 같다. 모
락셀라 각막염은 전신 선행인자 없이 발생할 수 있으며,
기회감염이 아닌, 외상이 가장 흔한 안구 위험인자였다.
항생제 감수성 검사상 내성을 보이지는 않았으나, 각막 상
피 회복에 오랜 시간이 걸리며, 시력 예후가 좋지 않았다.
조기 진단과 면밀한 경과 관찰이 중요하며, 특히 각막병변
이 중심부에 있을 시, 약물 치료와 함께 조기에 수술적 처
치도 모락셀라 각막염의 치료에 필요할 수 있음을 고려해
야 할 것이다.
REFERENCES
1) Srinivasan M, Mascarenhas J, Rajaraman R, et al. The steroids for corneal ulcers trial: study design and baseline characteristics. Arch Ophthalmol 2012;130:151-7.
2) National Surveillance of Infectious Keratitis in Japan. National Surveillance of Infectious Keratitis in Japan--current status of iso-lates, patient background, and treatment. Nippon Ganka Gakkai Zasshi 2006;110:961-72.
3) Das S, Constantinou M, Daniell M, Taylor HR. Moraxella keratitis: predisposing factors and clinical review of 95 cases. Br J Ophthalmol 2006;90:1236-8.
4) Garg P, Mathur U, Athmanathan S, Rao GN. Treatment outcome of Moraxella keratitis: our experience with 18 cases--a retrospective review. Cornea 1999;18:176-81.
5) Inoue H, Suzuki T, Inoue T, et al. Clinical characteristics and bac-teriological profile of Moraxella keratitis. Cornea 2015;34:1105-9.
6) Musch DC, Sugar A, Meyer RF. Demographic and predisposing factors in corneal ulceration. Arch Ophthalmol 1983;101:1545-8.
7) Benson WH, Lanier JD. Current diagnosis and treatment of corneal ulcers. Curr Opin Ophthalmol 1998;9:45-9.
8) Marioneaux SJ, Cohen EJ, Arentsen JJ, Laibson PR. Moraxella keratitis. Cornea 1991;10:21-4.
9) Baum J, Fedukowicz HB, Jordan A. A survey of Moraxella corneal ulcers in a derelict population. Am J Ophthalmol 1980;90:476-80.
10) Heidemann DG, Alfonso E, Forster RK, et al. Branhamella catar-rhalis keratitis. Am J Ophthalmol 1987;103:576-81.
11) Mian SI, Malta JB. Moraxella keratitis: risk factors, presentation, and management. Acta Ophthalmol 2011;89:e208-9.
12) Varaprasathan G, Miller K, Lietman T, et al. Trends in the etiology

216
= 국문초록 =
모락셀라 각막염의 임상양상과 치료결과
목적: 모락셀라 각막염의 임상 경과, 선행 위험인자, 치료 결과에 대하여 알아보고자 하였다.
대상과 방법: 2001년 3월부터 2015년 11월까지 3차병원인 본원 안과에서 시행한 배양검사에서 검출된 모락셀라 각막염 12안에 대하여
의무기록을 후향적으로 분석하였다. 연구는 각막궤양의 위험인자, 임상양상, 치료 결과 등을 분석하였다.
결과: 모락셀라 각막염 환자의 평균 나이는 68세였다. 가장 흔한 원인은 외상(6안, 50.0%)이었고, 그중 절반(3안, 25.0%)은 당뇨를
앓고 있었다. 두 명의 환자(16.6%)에서 이전에 각막이식술을 받은 기왕력이 있었다. 병변의 위치는 중심부(50.0%), 중심주변부(50.0%)
였고, 모양은 둥근 형태(58.3%)와 불규칙한 형태(41.7%)였다. 전방축농은 5안(41.7%)에서 관찰되었다. 모든 모락셀라 분리균은
aminoglycoside, fluoroquinolone 항생제에 감수성을 보였고, 3안은 trimethoprim/sulfamethoxazole에 내성을 보였다. 평균 상피 회
복 기간은 32.4일이었다. 최종시력은 7안(58.3%)에서 20/1,000 이하였다. 3안은 약물치료에도 불구하고, 각막천공으로 발전되어 안구
내용제거술을 시행받았다.
결론: 모락셀라 각막염은 안외상에 의해 종종 발생할 수 있으며, 치료 반응은 매우 느리고 시력적 예후는 대체로 좋지 않다. 이에
적절한 항생제 치료를 장기간으로 고려할 필요가 있다.
<대한안과학회지 2018;59(3):209-216>
-대한안과학회지 2018년 제 59 권 제 3 호-
of infectious corneal ulcers at the F. I. Proctor Foundation. Cornea 2004;23:360-4.
13) Cho EY, Lee SB. Gram-negative bacterial keratitis: a 15-year re-view of clinical aspects. J Korean Ophthalmol Soc 2015;56: 1479-88.
14) Hahn YH, Hahn TW, Tchah H, et al. Epidemiology of infectious Keratitis(II): a multi-center study. J Korean Ophthalmol Soc 2001;42:247-65.
15) Van Bijsterveld OP. Host-parasite relationship and taxonomic posi-tion of Moraxella and morphologically related organisms. Am J Ophthalmol 1973;76:545-54.
16) Cobo LM, Coster DJ, Peacock J. Moraxella keratitis in a non-alcoholic population. Br J Ophthalmol 1981;65:683-6.
17) Suzuki T, Ohashi Y. Combination effect of antibiotics against bac-teria isolated from keratitis using fractional inhibitory concen-
tration index. Cornea 2013;32:e156-60.18) Kowalski RP, Kowalski TA, Shanks RM, et al. In vitro comparison
of combination-and mono-therapy for the empiric and optimal cov-erage of bacterial keratitis based on incidence of infection. Cornea 2013;32:830-4.
19) Loh RS, Chan CM, Ti SE, et al. Emerging prevalence of micro-sporidial keratitis in Singapore: epidemiology, clinical features, and management. Ophthalmology 2009;116:2348-53.
20) Ly CN, Pham JN, Badenoch PR, et al. Bacteria commonly isolated from keratitis specimens retain antibiotic susceptibility to fluo-roquinolones and gentamicin plus cephalothin. Clin Exp Ophthalmol 2006;34:44-50.
21) Stern GA. Moraxella corneal ulcers: poor response to medical treatment. Ann Ophthalmol 1982;14:295-8.