Embed Size (px)
DESCRIPTION
tes
Citation preview

Dig Dis Sci (2007) 52:776–782DOI 10.1007/s10620-006-9541-2
ORIGINAL PAPER
Clinical Evaluation of Lens Culinaris Agglutinin-Reactiveα-Fetoprotein and Des-γ -Carboxy Prothrombin in HistologicallyProven Hepatocellular Carcinoma in the United StatesBrian I. Carr · Futoshi Kanke · Margaret Wise ·Shinji Satomura
Received: 27 March 2006 / Accepted: 25 July 2006 / Published online: 26 January 2007C© Springer Science+Business Media, Inc. 2006
Abstract There is no established clinical role for the lensculinaris agglutinin-reactive fraction of α-fetoprotein (AFP-L3%) and des-γ -carboxy prothrombin (DCP) in the man-agement of the U.S. hepatocellular carcinoma (HCC) patientpopulation. In order to clarify the clinical usefulness andcharacteristics of AFP-L3% and DCP, a prospective studywas performed on United States patients having histolog-ically proven hepatocellular carcinoma. Ninety-nine histo-logically proven HCC patients, who were diagnosed withunresectable cancer between July 1999 and March 2001 atthe Liver Cancer Center of the University of Pittsburgh Med-ical Center, were included for analysis. The sensitivity ofAFP-L3%, DCP, and AFP was 61.6%, 72.7%, and 67.7%,respectively. The highest sensitivity, 85.9%, was obtainedin the combination of three markers. Statistically significantdifferences were observed for portal vein invasion in AFP-L3% and AFP levels (P = 0.0059 and P = 0.0360, respec-tively). DCP was significantly associated with metastasis(P = 0.0368). There were significant associations betweenAFP-L3% and AFP results and patient survival (P = 0.0150and P = 0.0020, respectively). AFP-L3%, platelet count,andalbumin showed a significant difference with respect to out-
B. I. Carr (�)Liver Cancer Center, Starzl Transplantation Institute,University of Pittsburgh Medical Center,E1552 BST, 200 Lothrop Street, Pittsburgh,Pennsylvania 15213, USAe-mail: [email protected]
F. Kanke · S. SatomuraDiagnostics Division, Wako Pure Chemical Industries, Ltd.,Osaka, Japan
M. WiseDiagnostics Division, Wako Chemicals USA, Inc.,Richmond, Virginia, USA
comes on Cox’s proportional hazard model (P = 0.0059,P = 0.0073, and P = 0.0265, respectively). The combinationof AFP-L3%, DCP, and AFP was determined to be superiorfor detection of HCC compared with each marker alone orto other combinations. AFP-L3% was significantly relatedto portal vein invasion and patient outcomes and appears tobe a useful prognostic marker for HCC.
Keywords Lens culinaris agglutinin-reactive fraction ofα-fetoprotein . Des-γ -carboxy prothrombin (DCP) .
α-Fetoprotein . Hepatocellular carcinoma . Prognosis
Introduction
Hepatocellur carcinoma (HCC) is one of the most prevalentcancers in humans. It is the fifth most common neoplasm inthe world and the third most common cause of cancer-relateddeath [1]. In the United States, the incidence of HCC has in-creased approximately 80% over the past 20–30 years, and itis estimated that more than 18,000 new cases occur each year[2]. The most powerful risk factor for development of HCCis the existence of liver cirrhosis, regardless of its etiology[3]. Among cirrhotics, viral infection, such as hepatitis virusB (HBV) and hepatitis virus C (HCV), and high alcohol in-take are associated with the highest risk [4–7]. Recently, theAmerican Association for the Study of Liver Diseases pub-lished guidelines for HCC and stated that the early detectionof HCC is an essential issue since HCC patients can receiveeffective treatments such as hepatic resection, liver transplan-tation, and precutaneous ablation [8]. However, there are nowidely accepted approaches to regular surveillance in theUnited States. Therefore, most HCC patients are diagnosedat later or more advanced stages, usually when the tumoris nonresectable. As a consequence, the overall survival of
Springer

Dig Dis Sci (2007) 52:776–782 777
patients diagnosed with HCC remains poor. Recent ad-vances in imaging, such as a multidetector computed to-mography (CT) and magnetic resonance imaging (MRI),have improved the early radiologic diagnosis of HCC [9–14]. Currently, the only generally available serologic markerfor HCC surveillance, diagnosis, and monitoring is serumα-fetoprotein (AFP). The combination of ultrasonographyand AFP is commonly used for surveillance of HCC [15].However, it has been recognized that AFP has limited sensi-tivity and specificity for HCC, and ultrasonography is oper-ator skill–dependent and limited in its ability to differentiateHCC from nonneoplastic nodules [16, 17]. Many centers useCT and AFP. However, there is no evidence to support thatthis is good practice.
Recently, the lens culinaris agglutinin-reactive fractionof α-fetoprotein (AFP-L3) [18–28] and des-γ -carboxy pro-thrombin (DCP) [29–37] have become widely used for HCCdiagnosis and follow-up as serologic tumor markers in Japan.AFP-L3 is a variant of AFP, based on the sugar chain struc-ture. AFP-L3 has an additional α 1–6 fucose residue ap-pended to N-acetylglucosamine at the reducing end, andAFP-L3 production is observed mainly in malignant cells.DCP is an abnormal prothrombin protein that is generatedas a result of an acquired defect in the posttranslational car-boxylation of the prothrombin precursor in HCC cells. SinceAFP-L3% and DCP in serum behave independently, theyhave the potential to complement each other for the diag-nosis and monitoring of HCC [36, 38–41]. However, thereare no published data in the U.S. HCC population concern-ing their potential usefulness together. In order to clarifythe clinical usefulness and characteristics of AFP-L3% andDCP, a prospective study was performed with patients havinghistolologically proven HCC in the United States.
Materials and methods
Patients
Ninety-nine histologically proven HCC patients, who werediagnosed between July 1999 and March 2001 at the LiverCancer Center of the University of Pittsburgh MedicalCenter, Starzl Transplantation Institute, were included foranalysis. Clinical and laboratory information was prospec-tively gathered from the medical records. The diagnosis ofHCC was done by percutaneous core biopsy. All patientswere unresectable, and 98 patients received transarterialchemoembolization (TACE). None of the patients receivedliver transplantation. Blood was drawn within 4 weeks ofHCC diagnosis. The serum samples were frozen at − 70◦Cuntil measurement. Of 99 HCC patients, tumor number, por-tal vein invasion, vascularity, and metastasis informationwas available for 97. Ninety-two patients had tumor size
information available (two had diffuse tumor in the liver).This novel tumor marker study was approved by the Institu-tional Review Board of the University of Pittsburgh MedicalCenter, and informed consent was obtained from all patients.
Tumor marker measurement
Serum AFP-L3%, which is the ratio of AFP-L3 to total AFP,and DCP were measured on an automated analyzer, calledLiBASys (Liquid-Phase Binding Assay System), which ismanufactured by Wako Pure Chemical Industries, Ltd.,Osaka, Japan [42–44]. AFP was tested by an immunochemi-luminescent assay (ADVIA Centaur immunoassay system;Bayer Healthcare, Tarrytown, NY, USA). The cutoff valuefor AFP-L3% was set at 10% according to a previous study[20]. Cutoff values for DCP and AFP were 200 mAU/ml and25 ng/ml, respectively, which are used at our hospital.
Statistical analysis
The results are expressed as the mean ± SD or medianand range. In univariate analyses, statistical significance wasdetermined using the Kruskal-Wallis and chi-square test. Inmultivariate analyses, Cox’s proportional hazard model wasused with a continuous variable. The survival rate was cal-culated by Kaplan-Meier’s method, and the difference wasanalyzed by the generalized Wilcoxon test. All P values< 0.05 were considered statistically significant.
Results
Study population
Clinical characteristics of 99 patients are reported inTable 1. Seventy-eight patients were male (78.8%) and 21patients were female (21.1%). The median patient age was67.0 years (range, 19–93 years). The positive percentages ofHBV, HCV, and HCV + HBV were 5.1%, 29.3%, and 3.0%,respectively. Thirteen patients had no underlying liver dis-ease (13.1%), 6 patients had chronic hepatitis (CH) (6.1%),77 patients had liver cirrhosis (LC), and 3 patients had otherdiseases (3.0%). Tumor characteristics of 99 patients arelisted in Table 2 in terms of number, size, portal vein inva-sion, vascularity, and metastasis. Platelet count, prothrom-bin time, bilirubin, albumin, alkaline phosphatase, and γ -glutamyl transpeptidase, in addition to AFP-L3%, DCP, andAFP, were evaluated as a liver function serum marker. Thedistribution of these markers is summarized in Table 3.
Sensitivity of AFP-L3%, DCP, and AFP
Sensitivity of AFP-L3%, DCP, and AFP was 61.6%, 72.7%,and 67.7%, for each independent marker, respectively
Springer

778 Dig Dis Sci (2007) 52:776–782
Table 1 Demographics of the study population
Demographics n (%)
Age< 60 36 (36.4)≥ 60 63 (63.6)
SexMale 78 (78.8)Female 21 (21.2)
EthnicWhite 97 (98.0)Black 2 (2.0)
Underlying liver diseaseChronic hepatitis 6 (6.1)Liver cirrhosis 77 (77.8)Other 3 (3.0)No disease 13 (13.1)
Hepatitis virusHBV 5 (5.1)
(Table 4). When the combinations of these markers wereanalyzed, AFP-L3% + AFP had a sensitivity of 73.7%,AFP-L3% + DCP had a sensitivity of 84.8%, DCP + AFPhad a sensitivity of 84.8%, and AFP-L3% + DCP + AFPhad a sensitivity of 85.9%.
Table 2 Tumor characteristics of study population
Characteritics n (%)
Number1 19 (19.2)2 21 (21.2)3 10 (10.1)≥ 4 47 (47.5)No data 2 (2.0)
Tumor size (cm; Maximum)≤ 2 5 (5.1)2.1–5.0 38 (38.4)≥ 5.1 49 (49.5)No data 7 (7.1)
Portal vein invasion+ 25 (25.3)− 72 (72.7)No data 2 (2.0)
VascularityHypo. 19 (19.2)Hetero. 44 (44.4)Hyper. 34 (34.3)No data 2 (2.0)
Metastasis+ 43 (43.4)− 54 (54.5)No data 2 (2.0)
Table 3 Serum markers of the study population
Serum markers n Median Range
AFP-L3% (%) 99 20.0 0.5–99.5DCP (mAU/ml) 99 1008 9.9–295115AFP (ng/ml) 99 121 1.9–2005000Platelet count ( × 104µl) 99 15.5 3.9–100.9Prothrobmin time (sec) 99 12.7 10.6–18.4Billrubin (mg/dl) 99 0.9 0.1–9.2Albumin (g/dl) 99 3.5 2.3–4.6Alkaline phosphatase (units/L) 99 147 68–854Gamma glutamyl transpeptidase(units/L)
99 182 25–908
Tumor characteristics with respect to AFP-L3%,DCP, and AFP
Table 5 reports the relationship between tumor character-istics and AFP-L3%, DCP, and AFP. None of the threemarkers presented any significant relationship with respectto tumor size and vascularity. However, there was significantrelationship between tumor number and AFP (p = 0.0440).Statistically significant differences were observed for portalvein invasion in AFP-L3% positive and AFP positive re-sults (P = 0.0059 and P = 0.0360 respectively). Only DCPlevels were significantly associated with metastasis of HCC(P = 0.0368).
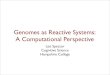
Survival rate with respect to AFP-L3%, DCP, and AFP
Figure 1 provides survival data for the positive and negativegroups of AFP-L3%, DCP, and AFP. Overall survival ratesat 6 and 12 months were 60.5% and 51.0%, respectively. Thesurvival rates of AFP-L3% positive cases at 6 and 12 monthswere 51.0% and 45.1%, and those for AFP-L3% negativecases at 6 and 12 months were 74.8% and 61.0%. A sig-nificant difference between AFP-L3% positive and negativecases in the survival rate was observed by the generalizedWilcoxon test (P = 0.0150). With respect to AFP, the sur-vival rate of patients with positive AFP levels was signifi-cantly lower than those of patients with negative AFP levels
Table 4 Sensitivities of AFP-L3%, DCsPand AFP
Tumor markers Sensitivity(%)
AFP-L3% 61.6DCP 72.7AFP 67.7AFP-L3% + DCP 84.8AFP-L3% + AFP 73.7DCP + AFP 84.8AFP-L3% + DCP + AFP 85.9
Springer

Dig Dis Sci (2007) 52:776–782 779
Tabl
e5
Tum
orch
arac
teri
stic
sw
ithre
spec
tto
AFP
-L3%
,DC
Pan
dA
FP
AFP
-L3%
DC
PA
FPT
umor
char
acte
rist
ics
Posi
tive
Neg
ativ
ep
valu
ePo
sitiv
eN
egat
ive
pva
lue
Posi
tive
Neg
ativ
ep
valu
e
Num
ber
1/2/
3/≥
412
/10/
8/29
7/11
/2/1
80.
7570
16/1
1/8/
363/
10/2
/11
0.73
3110
/11/
9/35
9/10
/1/1
20.
0440
Size
(cm
)≤
2.0/
2.1
to5.
0/≥
5.1
2/21
/31
3/17
/18
0.29
094/
23/3
91/
15/1
00.
1193
3/22
/35
2/16
/14
0.19
97
Port
alve
inin
vasi
on38
/21
34/4
0.00
5949
/22
23/3
0.05
2444
/21
28/4
0.03
60V
ascu
lari
tyH
ypo.
/Het
ero.
/Hyp
er.
10/2
8/21
9/16
/13
0.62
3311
/37/
238/
7/11
0.87
4112
/31/
227/
13/1
20.
9504
Met
asta
sis
−/+
31/2
823
/15
0.43
9735
/36
19/7
0.03
6833
/32
21/1
10.
1661
(P = 0.0020). Six- and 12-month survival rates of AFP pos-itive cases were 48.3% and 38.9%. The survival rates forAFP negative cases at 6 and 12 months were 85.3% and74.9%, respectively. DCP alone was not associated with thecumulative survival rate (P = 0.9581).
Patient outcome with respect to serum markers
The relationship between patient outcome and serum mark-ers including AFP-L3 %, DCP, AFP, platelet count, pro-thrombin time, bilirubin, albumin, alkaline phosphatase, andγ -glutamyl transpeptidase was analyzed by Cox’s propor-tional hazard model (Table 6). AFP-L3%, platelet count, andalbumin showed significance with respect to patient outcome(P = 0.0059, P = 0.0073, and P = 0.0265, respectively).
Discussion
HCC is one of those cancers that have been difficult to treatadequately, since most patients with HCC have either under-lying cirrhosis or advanced cancer or both. The severity of theunderlying cirrhosis has a profound effect on all treatmentdecisions and limits all treatment modalities. Although theAmerican Association for the Study of Liver Diseases pub-lished guidelines for HCC last year [8], it has not been longsince the publication. Therefore, there are still no commonscreening and surveillance programs in the United States,and most patients with HCC rarely present with symptomsuntil there is advanced-stage cancer or end-stage liver dis-ease, when curative treatment is not possible. These facts areclosely related to the current status of poor survival of HCCpatients [45]. AFP and ultrasonography have most com-monly been used for HCC surveillance [15]. However, thesensitivity and specificity of AFP are dependent on the cutoffvalue, and ultrasonography is operator skill-dependent [16,17]. Obviously, sophisticated strategies and new tools arenecessary, and a new serologic tumor marker would be use-ful for changing the present situation. Although AFP-L3%and DCP are widely recognized as useful tumor markers forHCC in Japan, no comparative data on AFP-L3% and DCPin the U.S. HCC population have been published. Therefore,an assessment of these markers in a U.S. HCC population isnecessary to determine the clinical usefulness of AFP-L3%and DCP.
In this study, AFP-L3%, DCP, and AFP showed > 60%sensitivity. Moreover, the combinations of AFP-L3% +DCP, DCP + AFP, or AFP-L3% + DCP + AFP had> 80% sensitivity. According to previous publications, AFP-L3% and DCP, each as independent markers, showed a higherspecificity than AFP alone [19, 20, 22, 32, 33, 37]. The com-bination of AFP-L3% and DCP might be the best panel todetect HCC.
Springer

780 Dig Dis Sci (2007) 52:776–782
0%
20%
40%
60%
80%
100%
0 5 10 15 20 25
Months
Su
rviv
al r
ate
: %
AFP-L3% Positive
AFP-L3% Negative
p=0.0150
A
p=0.9581
B
0%
20%
40%
60%
80%
100%
0 5 10 15 20 25
Months
Sur
viva
l rat
e: %
DCP Positive
DCP Negative
0%
20%
40%
60%
80%
100%
0 5 10 15 20 25
Months
Sur
viva
l rat
e: %
AFP Positive
AFP Negative
p=0.0020C
Fig. 1 Survival rate ofAFP-L3% (A), DCP (B), andAFP (C). Solid line, patientswith positive results for eachmarker; dashed line, patientswith negative results for eachmarker
An appropriate treatment at the right time is importantto improve the mortality and survival of HCC patients. Inthis regard, many Japanese study groups have reported thatAFP-L3% had a tendency to show positivity in the worstprognosis cases of HCC [26, 28]. In the current study,AFP-L3% was significantly associated with portal vein in-vasion and presented a strong statistical relationship to pa-tient outcome. AFP-L3% could thus be a useful tool fordetermination of proper treatments and prognostic evalu-ation, since portal vein invasion is related to recurrence
and survival after treatment. On the other hand, althoughDCP showed significance in metastasis, there was no as-sociation between DCP results and patient survival. Theseresults are different from previous reports [46, 47]. Sinceprevious results came only from Japanese HCC patients,these discrepancies might possibly be caused by ethnic dif-ferences or differences in HCC populations. In order toclarify the usefulness of AFP-L3% and DCP as a prognos-tic marker, a prospective study is needed in the U.S. HCCpopulation.
Springer

Dig Dis Sci (2007) 52:776–782 781
Table 6 Cox’s proportional hazard model of patient outcome withrespect to serum markers
Serum marker β SE (β) p value
AFP-L3% 0.0147 0.0054 0.0059DCP 1.801 × 10−6 3.504 × 10−6 0.6072AFP 5.091 × 10−7 5.838 × 10−7 0.3832Platelet count 3.074 × 10−6 1.1464 × 10−6 0.0073Prothrombin time 0.1925 0.1362 0.1576Bilirubin 0.2251 0.1281 0.0790Albumin − 0.6902 0.3110 0.0265Alkaline
phosphatase− 0.0022 0.0016 0.1737
Gamma glutamyltranspeptidase
0.0010 0.0009 0.3164
In conclusion, the combination of AFP-L3%, DCP, andAFP was demonstrated to be superior in the detection of HCCcompared with each marker alone. Since AFP-L3% wassignificantly related to portal vain invasion and patient out-come, AFP-L3% has the potential to be a prognostic markerfor HCC.
Acknowledgment This work was supported in part by NIH Grant CA82723 (to B.I.C.).
References
1. Parkin DM, Bray F, Ferlay J, Pisani P (2001) Estimating the worldcancer burden globocan 2000. Int J Cancer 94:153–156
2. El-Serag HB (2004) Hepatocellular carcinoma: recent trends in theUnited States. Gastroenterology 127:S27–S34
3. Zaman SN, Melia WM, Johnson RD, Portmann BC, Johnson PJ,Williams R (1985) Risk factors in development of hepatocellularcarcinoma in cirrhosis: prospective study of 613 patients. Lancet1:1357–1360
4. Poynard T, Aubert A, Lazizi Y, et al (1991) Independent risk fac-tors for hepatocellular carcinoma in French drinkers. Hepatology13:896–901
5. Colombo M, Franchis Rd, Ninno ED, et al. (1991) Hepatocellularcarcinoma in Italian patients with cirrhosis. N Engl J Med 325:675–680
6. Tsukuma H, Hiyama T, Tanaka S, et al. (1993) The factors for hep-atocellular carcinoma among patients with chronic liver disease. NEngl J Med 328:1797–1801
7. Chevret S, Trinchet JC, Mathieu D, Rached AA, Beaugrand M,Chastang C (1999) A new prognostic classification for predict-ing survival in patients with hepatocellular carcinoma. J Hepatol31:133–141
8. Bruix J SMPGC, American Association for the Study of LiverDiseases (2005) Management of hepatocellular carcinoma. Hepa-tology 42:1208–1236
9. Shinagawa T, Ohto M, Kimura K, et al. (1984) Diagnosis and clin-ical features of small hepatocellular carcinoma eith emphasis onthe utility of real-time ultrasonography. Gastroenterology 86:495–502
10. Ikeda K, Saitoh S, Koida I, et al. (1993) Diagnosis and follow-up ofsmall hepatocellular carcinoma with selective intraarterial digitalsubtraction angiography. Hepatology 17:1003–1007
11. Oka H, Tamori A, Kuroki T, Kobayashi K, Yamamoto S (1994)Prospective study of α-fetoprotein in cirrhotic patients monitoredfor development of hepatocellular carcinoma. Hepatology 19:61–66
12. Takayasu K, Moriyama N, Muramatsu Y, et al. (1990) The diagno-sis of small hepatocellular carcinoma: efficacy of various imagingprocedures in 100 patients. AJR 155:49–54
13. Takayasu K, Furukawa H, Wakao F, et al. (1995) CT diagnosisof early hepatocellular carcinoma: sensitivity, findings, and CT-pathologic correlation. AJR 164:885–890
14. Ebara M, Ohto M, Watanabe Y, et al. (1986) Diagnosis of smallhepatocellular carcinoma: Correlation of MR imaging and tumorhistologic studies. Radiology 159:371–377
15. Daniele B, Bencivenga A, Megna AS, Tinessa V (2004) α-Fetoprotein and ultrasonography screening for hepatocellular car-cinoma. Gastroenterology 127:S108–S12
16. Bruix J, Sherman M, Llovet JM, et al. (2001) Clinical managementof hepatocellular carcinoma. Conclusion of the Barcelona-2000EASL conference. European Association for the Study of the Liver.J Hepatol 35:421–430
17. Sheu JC, Sung JL, Chen DS, et al. (1985) Early detection of hepa-tocellular carcinoma by real-time ultrasonography. A prospectivestudy. Cancer 56:660–666
18. Taketa K, Sekiya C, Namiki M, et al. (1990) Lectin-reactive profilesof alpha-fetoprotein characterizing hepatocellular carcinoma andrelated conditions. Gastroenterology 99:508–518
19. Taketa K, Endo Y, Sekiya C, et al. (1993) A collaborative study forthe evaluation of lectin-reactive a-fetoproteins in early detection ofhepatocellular carcinoma. Cancer Res 53:19–23
20. Oka H, Saito A, Ito K, et al. (2001) Multicenter prospective anal-ysis of newly diagnosed hepatocellular carcinoma with respect tothe percentage of lens culinaris agglutinin-reactive a-fetoprotein. JGastroenterol Hepatol 16:1378–1383
21. Sato Y, Nakata K, Kato Y, et al. (1993) Early recognition of hepa-tocellular carcinoma based on altered profiles of alpha-fetoprotein.N Engl J Med 328:1802–1806
22. Shiraki K, Takase K, Tameda Y, Hamada M, Kosaka Y, NakanoT (1995) A clinical study of lectin-reactive alpha-fetoprotein asan early indicator of hepatocellular carcinoma in the follow-up ofcirrhotic patients. Hepatology 22:802–807
23. Yamashita F, Tanaka M, Satomura S, Tanikawa K (1995) Monitor-ing of lectin-reactive a-fetoprotein in patients with hepatocellularcarcinoma treated using transcatheter arterial embolization. Eur JGastroenterol Hepatol 7:627–633
24. Yamashita F, Tanaka M, Satomura S, Tanikawa K (1996) Prognos-tic significance of lens culinaris agglutinin A-reactive a-fetoproteinin small hepatocellular carcinomas. Gastroenterology 111:996–1001
25. Hayashi K, Kumada T, Nakano S, et al. (1999) Usefulnessof measurement of lens culinaris agglutinin-reactive fractionof α-fetoprotein as a marker of prognosis and recurrence ofsmall hepatocellular carcinoma. Am J Gastroenterol 94:3028–3033
26. Kumada T, Nakano S, Takeda I, et al. (1999) Clinical utility oflens culinaris aggulutinin-reactive alpha-fetoprotein in small hep-atocellular carcinoma: special reference to imaging diagnosis. JHepatol 30:125–130
27. Tanaka M, Saito A, Ito K, et al. (2000) Lens culinaris agglutinin-reactive alpha-fetoprotein (AFP-L3) is the most significant prog-nostic factor for hepatocellular carcinoma after therapy. Hepatol-ogy 34:233A
28. Tada T, Kumada T, Toyoda H, et al. (2005) Relationship betweenlens culinaris agglutinin-reactive α-fetoprotein and pathologic fea-tures of hepatocellular carcinoma. Liver Int 25:1–6
29. Ono M, Ohta H, Ohhira M, Sekiya C, Namiki M (1990) Measure-ment of immunoreactive prothrombin precursor and vitamin-K
Springer

782 Dig Dis Sci (2007) 52:776–782
dependent gamma-carboxylation in human hepatocellular carci-noma tissues: decreased carboxylation of prothrombin precursoras a cause of des-gamma-carboxyprothrombin synthesis. TumorBiol 11:319–326
30. Liebman HA (1989) Isolation and characterization of a hepatoma-associated abnormal (des-gamma carboxy) prothrombin. CancerRes 49:6493–6497
31. Aoyagi Y, Oguro M, Yanagi M, et al. (1996) Clinical significance ofsimultaneous determination of alpha-fetoprotein and des-gammacarboxyprothrombin in monitoring recurrence in patients with hep-atocellular carcinoma. Cancer 77:1781–1786
32. Mita Y, Aoyagi Y, Yanagi M, Suda T, Suzuki Y, Asakura H (1998)The usefulness of determining des-gamma carboxyprothrombin bysensitive enzyme immunoassay in the early diagnosis of patientswith hepatocellular carcinoma. Cancer 82:1643–1648
33. Nomura F, Ishijima M, Kuwa K, Tanaka N, Nakai T, Ohnishi K(1999) Serum des-gamma carboxyprothrombin levels determinedby a new generation of sensitive immunoassay in patients withsmall-sized hepatocellular carcinoma. Am J Gastroenterol 94:650–654
34. Izuno K, Fujiyama S, Yamasaki K, Sato M, Sato T (1995) Earlydetection of hepatocellular carcinoma associated with cirrhosis bycombined assay of des-gamma carboxy prothrombin and alpha-fetoprotein: a prospective study. Hepatogastroenterology 42:387–393
35. Ikoma J, Kaito M, Ishihara T, et al. (2002) Early diagnosis of hepa-tocellular carcinoma using a sensitive assay for serum des-gammacarboxy prothrombin: a prospective study. Hepatogastroenterology49:235–238
36. Shimauchi Y, Tanaka M, Kuromatsu R, et al. (2000) A simulta-neous monitoring of lens culinaris aggulutinin A-reactive alpha-fetoprotein and des-gamma carboxyprothrombin as an early di-agnosis of hepatocellular carcinoma in the follow-up of cirrhoticpatients. Oncol Rep 7:249–256
37. Ishii M, Gama H, Chida N, et al. (2000) Simultaneous measure-ments of serum alpha-fetoprotein and protein induced by vitaminK absence for detecting hepatocellular carcinoma. Am J Gastroen-terol 95:1036–1040
38. Fujiyama S, Tanaka M, Maeda S, Ashihara H, Hirata R, Tomita K(2002) Tumor markers in early diagnosis, follow-up and manage-
ment of patients with hepatocellular carcinoma. Oncology 62:57–63
39. Okuda H, Nakanishi T, Takatsu K, et al. (2002) Clinicopathologicfeatures of patients with hepatocellular carcinoma seropositive fora-fetoprotein-L3 and seronegative for des-g-carboxy prothrombinin comparison with those seropositive for des-g-carboxy prothrom-bin alone. J Gastroenterol Hepatol 17:772–778
40. Okuda H, Saito A, Haruyama K, et al. (2004) Unique clini-caopathological features of patients with primary malignant hep-atic tumors who are seropositive for lectin-reactive α-fetoproteinalone: report of five cases. J Gastroenterol Hepatol 19:113–119
41. Okuda H, Saito A, Shiratori K, Yamamoto M, Takasaki K, NakanoM (2005) Clinicopathologic feature of patients with primary ma-lignant hepatic tumors seropositive for a-fetoprotein-L3 alone incomparison with other patients seropositive for a-fetoprotein-L3.J Gastroenterol Hepatol 20:759–764
42. Katoh H, Nakamura K, Tanaka T, Satomura S, Matsuura S (1998)Automatic and simultaneous analysis of Lens culinaris agglutinin-reactive alpha-fetoprotein ratio and total alpha-fetoprotein concen-tration. Anal Chem 70:2110–2114
43. Yamagata Y, Katoh H, Nakamura K, Tanaka T, Satomura S, Mat-suura S (1998) Determination of alpha-fetoprotein concentrationbased on liquid-phase binding assay using anion exchange chro-matography and sulfated peptide introduced antibody. J ImmunolMethods 212:161–168
44. Yamagata Y, Shimizu K, Nakamura K, et al. (2003) Simultaneousdetermination of percentage of Lens culinaris agglutinin-reactivealpha-fetoprotein and alpha-fetoprotein concentration using theLiBASys clinical auto-analyzer. Clin Chim Acta 327:59–67
45. El-Serag HB, Mason AC, Key C (2001) Trends in survival ofpatients with hepatocellular carcinoma between 1977 and 1996 inthe United States. Hepatology 33:62–65
46. Hamamura K, Shiratori Y, Shiina S, et al. (2000) Unique clini-cal characteristics of patients with hepatocellular carcinoma whopresent with plasma des-gamma-carboxy prothrombin and lowserum alpha-fetoprotein. Cancer 88:1557–1564
47. Koike Y, Shiratori Y, Sato S, et al. (2001) Des-gamma-carboxyprothrombin as a useful predisposing factor for the development ofportal venous invasion in patients with hepatocellular carcinoma:a prospective analysis of 227 patients. Cancer 91:561–569
Springer