Embed Size (px)
Citation preview

Vol. 4, 235-240, January 1998 Clinical Cancer Research 235
Clinical Features of Ovarian Cancer in Japanese Women with
Germ-Line Mutations of BRCA1’
Hiroshi Aida, Koichi Takakuwa, Hiroshi Nagata,Ikunosuke Tsuneki, Masashi Takano, Shoji Tsuji,
Takeshi Takahashi, Takahiko Sonoda,
Masayuki Hatae, Katsuyuki Takahashi,Kazuo Hasegawa, Hideki Mizunuma,Nagayasu Toyoda, Hiroyuki Kamata,Ywchi Toni, Noriyasu Saito, Kohei Tanaka,Michiaki Yakushiji, Tsutomu Araki, and
Kenichi Tanaka2Departments of Obstetrics and Gynecology [H. A., Koi. T., H. N.,
I. T., M. T., Ke. T.] and Neurology [S. T.], Niigata University Schoolof Medicine, Niigata 95 1 ; Niigata Cancer Center, Niigata 95 1 [T. T.];Department of Gynecology, National Cancer Center, Tokyo 104[T. S.]; Kagoshima City Hospital, Kagoshima 892 [M. H.]; SendaiNational Hospital, Miyagi 983 [Ka. T.]; Hyogo Medical Center forAdults, Hyogo 673 [K. H.]; Department of Obstetrics andGynecology, Gunma University School of Medicine, Gunma 371
[H. M.]; Department of Obstetrics and Gynecology, Mie University
School of Medicine, Mie 514 [N. T.]; Tochigi Cancer Center, Tochigi320 [H. K.]; Seirei-Hamamatsu Hospital, Shizuoka 430 [Y. T.];
Shonai Hospital, Yamagata 997 [N. S.]; Akita Red Cross Hospital,
Akita 010 [Koh. T.]; Department of Obstetrics and Gynecology,Kurume University School of Medicine, Fukuoka 830 [M. Y.]; andDepartment of Obstetrics and Gynecology, Nihon Medical College,Tokyo I 13 [T. A.], Japan
ABSTRACTWe analyzed the clinical features of 25 ovarian cancer
patients who were associated with germ-line mutations ofBRCAJ from four site-specific ovarian cancer families andseven breast-ovarian cancer families in Japan. The average
age at diagnosis was 51.1 years (range, 38-77 years). Histo-logical examination revealed 24 serous cyst adenocarcino-mas in 25 patients. In 23 patients with clear clinical records,3 patients had stage I disease, 17 had stage Ill disease, and3 had stage LV disease. Thirteen patients with stage IIIdisease who were treated with cisplatin.contaimng chemo-therapy following tumor reduction surgery showed morefavorable outcomes in both the survival rate and disease-free intervals, compared with age- and treatment course-
Received 7/16/97; revised 10/23/97; accepted 10/23/97.The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to
indicate this fact.‘ This work was supported in part by a Grant-in-Aid from the Ministry
of Health and Welfare for the Second-Term Comprehensive 10-YearStrategy for Cancer Control.2 To whom requests for reprints should be addressed, Department ofObstetrics and Gynecology, Niigata University School of Medicine,1-757, Asahimachi-dori, Niigata City 951, Japan. Phone: 25-223-6161,
ext. 2620; Fax: 25-225-5550; E-mail [email protected].
matched controls (5-year survival rate, 0.786 versus 0.303;
median disease-free interval, 91.43 versus 40.92 months; P <
0.05 for both, by logarithmic rank test). Our statistical
model for the inheritance of susceptibility to ovarian cancer
was derived from the analysis of 26 patients and 19 healthy
carriers of 12 families. The expected lifetime risk of ovarian
cancer is about 80% for women with mutations of BRCAJ.
These results suggest that the clinical outcome of ovarian
cancer with germ-line mutations of BRCAJ appears to he
more favorable than that with sporadic cases and that the
disease penetrance among pedigrees with germ-line muta-
tions of the BRCAJ gene is substantially high.
INTRODUCTIONAfter the BRCAI gene, which is thought to be related to
susceptibility to hereditary breast and ovarian cancer and, in
part, to sporadic cases, was identified, detailed studies of
BRCAJ mutations were performed on affected individuals from
over 100 breast and breast-ovarian cancer families ( I , 2). Re-
cently, we reported six different mutations found in 3 of 13
(23. 1 %) site-specific ovarian cancer families and 4 of 6 (66.7%)
breast-ovarian cancer families (3). In Japan, germ-line muta-
tions were detected in only 2 of 20 breast cancer families and 4
of 103 breast cancer patients (4, 5). The median age at diagnosis
of breast cancer patients is different from that in Western
countries (6). These results suggested that genetic and epige-
netic alterations in familial breast and breast-ovarian cancer in
Japan may differ from those in Western countries. Every year,
approximately 1 80,000 new cases of breast cancer and 26,000
new cases of ovarian cancer are diagnosed in the United States
(7). However, in Japan, only 20,000 new cases of breast cancer
and 6,000 cases of ovarian cancer were diagnosed last year (8).
In addition, it has been reported that lifetime risk of these two
malignancies for women in the United States is 3 or 4 times
higher than that in Japan.
Hence, it is worthwhile to answer the question of whether
these genetic and epidemiobogical differences may influence the
clinical features of familial ovarian cancers with mutations of
BRCA 1 because many types of cancer are sensitive to environ-
mental changes, such as dietary factors, prevalence of hysterec-
tomy or unilateral oophorectomy, lower parity, and dietary
intake of milk or fat. With regard to previous reports of the
clinical characteristics of ovarian cancer patients or breast can-
cer patients carrying germ-line mutations ofBRCAI, the issue of
prognostic features is controversial, even now (9-1 1). Here, we
tried to identify these aspects for the inheritance of susceptibility
to ovarian cancer in a Japanese population and analyzed the
clinical features and pathological characteristics of 25 ovarian
cancer patients with documented germ-line mutations of
BRCAJ.
on July 1, 2018. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

236 Ovarian Cancer Patients with BRCA 1 Mutations
3 The abbreviation used is: CDDP, cisplatin.
PATIENTS AND METHODS
Ovarian Cancer Patients. Of 45 patients in 13 site-
specific ovarian cancer families and 21 patients in 10 breast
ovarian cancer families, we identified 26 patients with mutations
of BRCAJ. The criteria for a site-specific ovarian cancer family
are as follows: two or more members with well-documented
epithebial ovarian cancer in the first-degree relatives, and no
breast cancer cases in the third-degree relatives. When the
family had at beast one breast cancer case in the third-degree
relatives, it was classified as a breast-ovarian cancer family.
Several patients were seen at other hospitals. We examined the
clinical data from hospital records and pathological reports or
asked physicians to answer the questionnaires or record data
from patients. All experiments were performed under informed
consent.
Survival and Disease-free Intervals. The survival rates
and disease-free intervals of the patients with the BRCAI mu-
tation with stage III disease were compared with those of
controls with stage III ovarian cancer who were treated at
Niigata University Hospital. Each patient was matched to a
control subject for clinical tumor stage, histological subtypes,
and treatment protocol; in both groups, all patients were treated
with at least two courses of CDDP3-containing chemotherapy
following tumor reduction surgery. In addition, the survival rate
of patients with BRCA 1 mutation at S years after the time of
diagnosis was compared with that obtained from the data from
mubticenter studies on the prognosis of ovarian cancer in Japan
(12).
Evaluation of Responsiveness to Chemotherapy. Re-sponse to CDDP-containing chemotherapy was evaluated ac-
cording to the criteria of the Japanese Society for Cancer Ther-
apy, as follows: complete remission, absence of any detectable
tumor mass for >4 weeks; partial remission, a decrease of
>50% in the product of the two perpendicular diameters of the
measurable lesions, without an increase in size of other detected
areas of disease or appearance of new lesions for >4 weeks; no
change, <50% reduction or <25% increase in the products of
the perpendicular diameters of any measurable lesion; and pro-
gressive disease, an increase of >25% in the products of per-
pendicular diameters of any measurable lesion or the appearance
of a new lesion.
Mutational Analysis. The mutational analysis method
we used has been described in detail elsewhere (3). In brief,
after obtaining informed consent, we collected whole blood or
tissue samples from both affected and unaffected members of
the pedigree. DNAs were extracted from these samples by a
phenol-chloroform method (13). Single-strand conformation
polymorphism following direct sequencing was performed in
the entire coding regions of BRCAI. When the germ-line mu-
tation was identified in DNA from the affected member, we
examined all available members in the pedigree.
Statistical Analysis. Survival data and disease free-inter-
vabs were calculated by the Kaplan-Meier method and compared
by the logarithmic rank test (14, 15).
Disease Penetrance. Disease penetrance was calculated
by the Kaplan-Meier method, based on age at diagnosis for
patients with ovarian cancer and present age of healthy women
and breast cancer patients (14).
RESULTS
Clinical Analysis. By screening the whole coding region
of BRCAJ of 45 patients, we found 1 1 independent mutations in
26 patients from 12 families: 9 patients in four-site specific
ovarian cancer families and 17 patients in eight breast-ovarian
cancer families. Among the 1 1 independent mutations, 1 mis-
sense mutation (T-to-A substitution at nucleotide 300) that was
observed presumably leads to boss of a zinc-binding motif. This
mutation was not found in healthy women in this family or in a
substantial number of healthy volunteers who had no family
history of ovarian and/or breast cancer, indicating that this
abnormality could be diagnosed as a pathogenic mutation but
not as a polymorphism. All others were nonsense mutations or
small deletions that were predicted to result in the protein
truncation. The characteristics of 25 patients with the germ-line
BRCAJ mutation and the 1 18 control patients treated in Niigata
University Hospital from 1983 to 1996 are shown in Table 1.
One patient was not shown in Table 1 because there were not
enough data on her clinical characteristics. There were no sig-
nificant differences in average age at diagnosis between BRCAJ
cases and sporadic cases (5 1 . 1 versus 52.0), and 24 of 25
patients with germ-line mutation had a serous type of adeno-
carcinoma.
Survival Analysis. Survival data were available for 13
patients with stage III disease, and all of them completed at least
two courses of CDDP-containing chemotherapy following tu-
mor reduction surgery. Table 2 shows the courses of CDDP-
containing chemotherapy and patient responses to them. Twelve
patients were excluded from this survival analysis. The clinical
information for three patients was not available, and three pa-
tients were not treated with chemotherapy or were treated with
chemotherapy other than CDDP. Each of the three patients were
at stage IV or stage I. The average follow-up period for all 13
patients was 54.8 months from the time of diagnosis. As of May
1997, three patients had died of ovarian cancer, and two patients
had died of other diseases, with no evidence of ovarian cancer
at the time of death. Five patients were alive, with no evidence
of disease. As a control, we examined the clinical data of 29
sporadic cases with ovarian cancer at stage III who were treated
in Niigata University Hospital from 1983 to 1996 (16). The
actual survivors from 1 3 familial ovarian cancers with germ-line
mutations ofBRCAJ and 29 sporadic cases are shown in Fig. lA
(Kapban-Meier method). The estimated 5-year overall survival
rates in the BRCAJ group and the control group were 0.786 and
0.303, respectively. Median survival was 1 15.48 months for
patients with the mutation, compared to 52.75 months for the
control group. The favorable prognosis in the 5-year survival
rate and median survival was similarly observed in 12 BRCAJ
patients, when histological subtype was limited to serous cyst
adenocarcinoma (0.786 versus 0.193 and 1 15.48 versus 36.69
months, respectively; Fig. 1B). The differences between the
5-year overall survival rate and median survivals of patients in
the two groups were statistically significant (logarithmic rank
on July 1, 2018. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Clinical Cancer Research 237
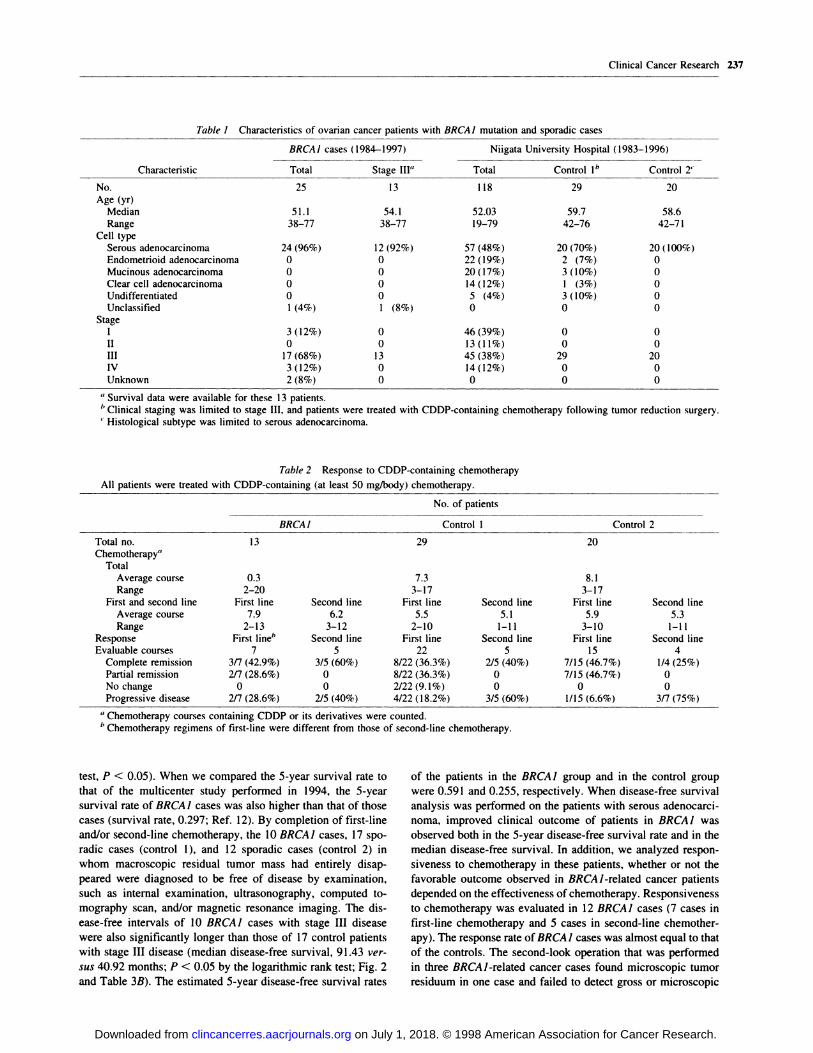
Table I Char acteristics of ovarian cancer patients with BRCAJ mutation and sporadic cases
Characteristic
BRCAI cases (1984-1997) Niigata University Hospital (1983-1996)
Total Stage III” Total Control I” Control 2’
No. 25 13 118 29 20
Age (yr)
Median 51.1 54.1 52.03 59.7 58.6Range 38-77 38-77 19-79 42-76 42-71
Cell typeSerous adenocarcinoma 24 (96%) 12 (92%) 57 (48%) 20 (70%) 20(100%)Endometrioid adenocarcinoma 0 0 22 (19%) 2 (7%) 0Mucinous adenocarcinoma 0 0 20 (17%) 3 (10%) 0
Clear cell adenocarcinoma 0 0 14 (12%) 1 (3%) 0Undifferentiated 0 0 5 (4%) 3 (10%) 0
Unclassified 1 (4%) 1 (8%) 0 0 0
StageI 3(12%) 0 46(39%) 0 0II 0 0 13(11%) 0 0
III 17(68%) 13 45(38%) 29 20
IV 3(12%) 0 14(12%) 0 0Unknown 2(8%) 0 0 0 0
‘4 Survival data were available for these 13 patients.
1. Clinical staging was limited to stage II!, and patients were treated with CDDP-containing chemotherapy following tumor reduction surgery.C Histological subtype was limited to serous adenocarcinoma.
Table 2 Response to CDDP-containing chemotherapy
All patients were treated with CDDP-containing (at least 50 mg/body) chemotherapy.
No. of patients
BRCAI Control 1 Contr ol 2
Total no. 13 29 20
Chemotherapy”Total
Average course 0.3 7.3 8.1Range 2-20 3-17 3-17
First and second line First line Second line First line Second line First line Second line
Averagecourse 7.9 6.2 5.5 5.! 5.9 5.3Range 2-13 3-12 2-10 1-11 3-10 1-11
Response First line” Second line First line Second line First line Second lineEvaluable courses 7 5 22 5 15 4
Complete remission 3/7 (42.9%) 3/5 (60%) 8/22 (36.3%) 2/5 (40%) 7/15 (46.7%) 1/4 (25%)
Partial remission 2/7 (28.6%) 0 8/22 (36.3%) 0 7/15 (46.7%) 0
Nochange 0 0 2/22(9.1%) 0 0 0Progressive disease 2/7 (28.6%) 2/5 (40%) 4/22 (18.2%) 3/5 (60%) 1/15 (6.6%) 3/7 (75%)
a Chemotherapy courses containing CDDP or its derivatives were counted.b Chemotherapy regimens of first-line were different from those of second-line chemotherapy.
test, P < 0.05). When we compared the 5-year survival rate to
that of the mubticenter study performed in 1994, the 5-year
survival rate of BRCAJ cases was also higher than that of those
cases (survival rate, 0.297; Ref. 12). By completion of first-line
and/or second-line chemotherapy, the 10 BRCAJ cases, 17 spo-
radic cases (control 1), and 12 sporadic cases (control 2) in
whom macroscopic residual tumor mass had entirely disap-
peared were diagnosed to be free of disease by examination,
such as internal examination, ultrasonography, computed to-
mography scan, and/or magnetic resonance imaging. The dis-
ease-free intervals of 10 BRCAI cases with stage III disease
were also significantly longer than those of 17 control patients
with stage III disease (median disease-free survival, 91 .43 ver-
sus 40.92 months; P < 0.05 by the logarithmic rank test; Fig. 2
and Table 3B). The estimated 5-year disease-free survival rates
of the patients in the BRCAJ group and in the control group
were 0.591 and 0.255, respectively. When disease-free survival
analysis was performed on the patients with serous adenocarci-
noma, improved clinical outcome of patients in BRCA I was
observed both in the 5-year disease-free survival rate and in the
median disease-free survival. In addition, we analyzed respon-
siveness to chemotherapy in these patients, whether or not the
favorable outcome observed in BRCA 1-related cancer patients
depended on the effectiveness of chemotherapy. Responsiveness
to chemotherapy was evaluated in 12 BRCAJ cases (7 cases in
first-line chemotherapy and 5 cases in second-line chemother-
apy). The response rate of BRCA 1 cases was almost equal to that
of the controls. The second-look operation that was performed
in three BRCAJ-related cancer cases found microscopic tumor
residuum in one case and failed to detect gross or microscopic
on July 1, 2018. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
1.
4’
V
4’V0,
VV14
V
VVV
V
V
4’
0a0
a0 1 2 3 4
BRCA1 (n10)
A1
.� 0.8
I 0.6V
� 0.4
U 0.2
0
B
0.8a.� 0.6
a
a
.� 0.44’V
a
� 0.2U
control 1 (n-17)
BRCA1 casVs (n-12)
5 2 3 4 5
Years aftVr diagnosis Dis.ss.-fr.. int.rval. (y.r.)
0 1
control 2 (n12)
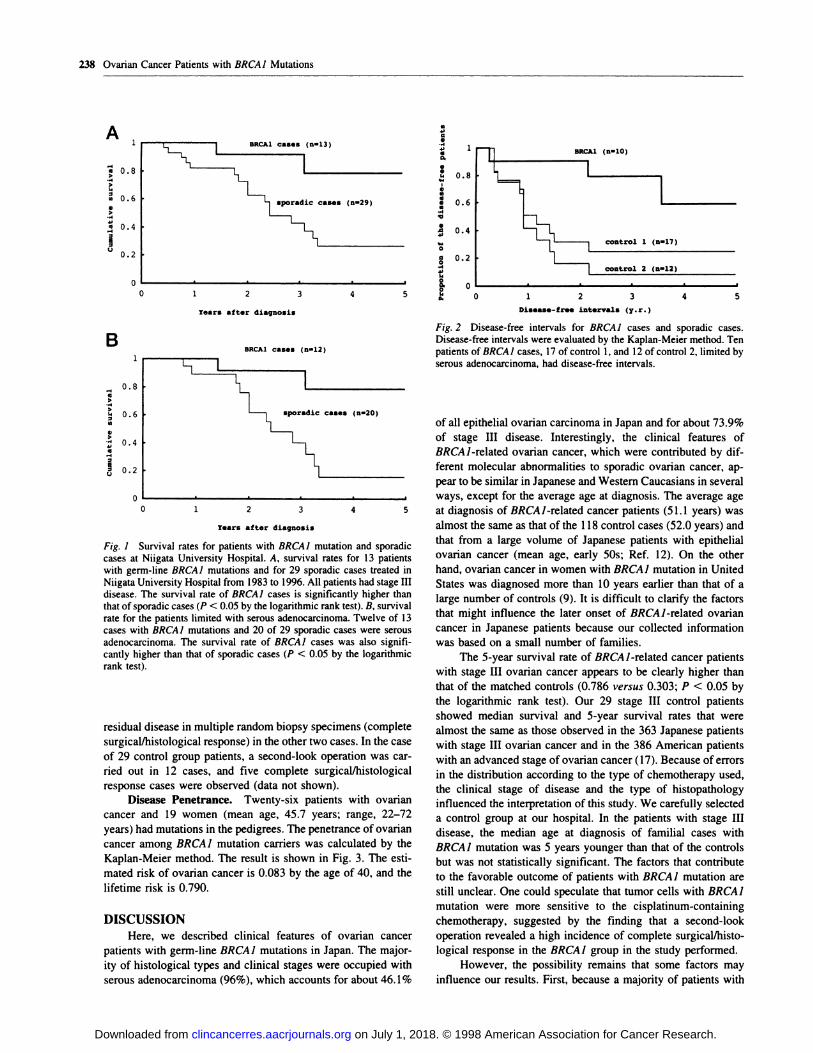
Fig. 2 Disease-free intervals for BRCA1 cases and sporadic cases.Disease-free intervals were evaluated by the Kaplan-Meier method. Tenpatients of BRCAJ cases, 17 of control 1, and 12 of control 2, limited byserous adenocarcinoma, had disease-free intervals.
2 3 4 5
Years after diagnocis
238 Ovarian Cancer Patients with BRCAJ Mutations
Fig. I Survival rates for patients with BRCAJ mutation and sporadiccases at Niigata University Hospital. A, survival rates for 13 patientswith germ-line BRCA 1 mutations and for 29 sporadic cases treated in
Niigata University Hospital from 1983 to 1996. All patients had stage IIIdisease. The survival rate of BRCAJ cases is significantly higher thanthat of sporadic cases (P < 0.05 by the logarithmic rank test). B, survival
rate for the patients limited with serous adenocarcinoma. Twelve of 13cases with BRCAJ mutations and 20 of 29 sporadic cases were serous
adenocarcinoma. The survival rate of BRCAJ cases was also signifi-
cantly higher than that of sporadic cases (P < 0.05 by the logarithmicrank test).
residual disease in multiple random biopsy specimens (complete
surgical/histological response) in the other two cases. In the case
of 29 control group patients, a second-look operation was car-
ned out in 12 cases, and five complete surgical/histological
response cases were observed (data not shown).
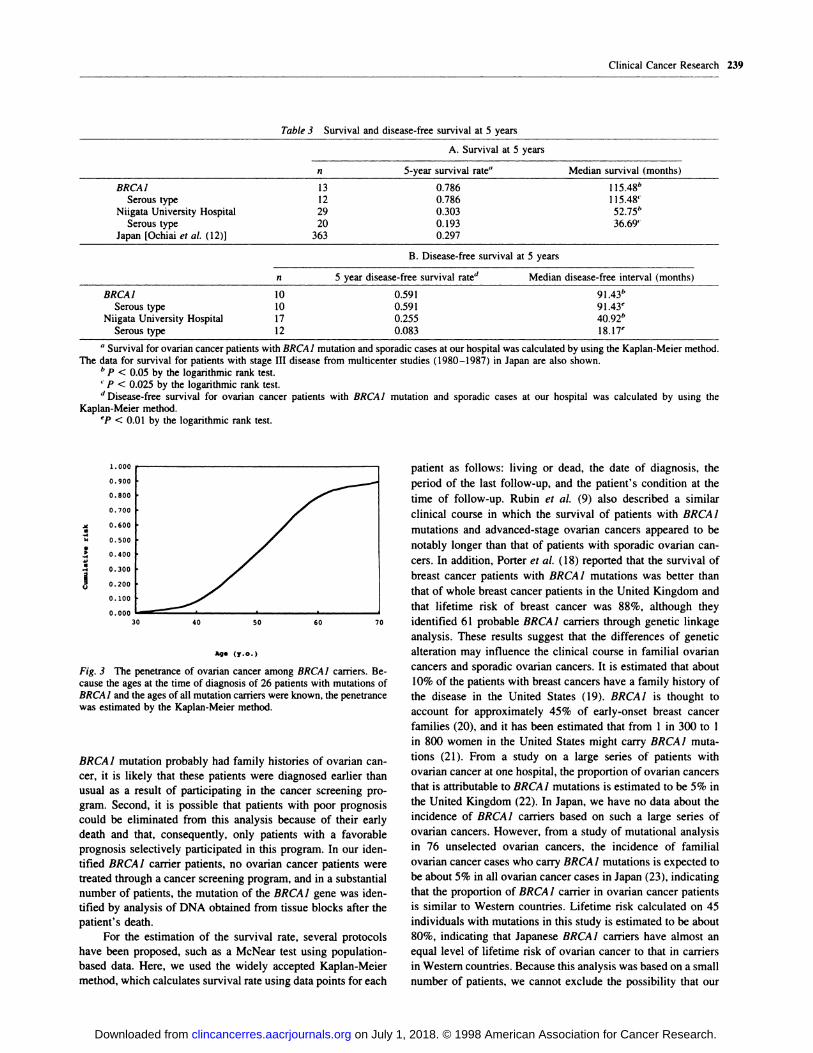
Disease Penetrance. Twenty-six patients with ovarian
cancer and 19 women (mean age, 45.7 years; range, 22-72
years) had mutations in the pedigrees. The penetrance of ovarian
cancer among BRCA 1 mutation carriers was calculated by the
Kaplan-Meier method. The result is shown in Fig. 3. The esti-
mated risk of ovarian cancer is 0.083 by the age of 40, and the
lifetime risk is 0.790.
DISCUSSION
Here, we described clinical features of ovarian cancer
patients with germ-line BRCAJ mutations in Japan. The major-
ity of histological types and clinical stages were occupied with
serous adenocarcinoma (96%), which accounts for about 46.1%
of all epithelial ovarian carcinoma in Japan and for about 73.9%
of stage III disease. Interestingly, the clinical features of
BRCAJ-related ovarian cancer, which were contributed by dif-
ferent molecular abnormalities to sporadic ovarian cancer, ap-
pear to be similar in Japanese and Western Caucasians in several
ways, except for the average age at diagnosis. The average age
at diagnosis of BRCAJ-related cancer patients (51.1 years) was
almost the same as that of the 1 18 control cases (52.0 years) and
that from a large volume of Japanese patients with epithelial
ovarian cancer (mean age, early SOs; Ref. 12). On the other
hand, ovarian cancer in women with BRCAJ mutation in United
States was diagnosed more than 10 years earlier than that of a
large number of controls (9). It is difficult to clarify the factors
that might influence the later onset of BRCAJ-related ovarian
cancer in Japanese patients because our collected information
was based on a small number of families.
The 5-year survival rate of BRCAJ-related cancer patients
with stage III ovarian cancer appears to be clearly higher than
that of the matched controls (0.786 versus 0.303; P < 0.05 by
the logarithmic rank test). Our 29 stage III control patients
showed median survival and 5-year survival rates that were
almost the same as those observed in the 363 Japanese patients
with stage HI ovarian cancer and in the 386 American patients
with an advanced stage of ovarian cancer (17). Because of errors
in the distribution according to the type of chemotherapy used,
the clinical stage of disease and the type of histopathology
influenced the interpretation of this study. We carefully selected
a control group at our hospital. In the patients with stage III
disease, the median age at diagnosis of familial cases with
BRCAJ mutation was 5 years younger than that of the controls
but was not statistically significant. The factors that contribute
to the favorable outcome of patients with BRCAJ mutation are
still unclear. One could speculate that tumor cells with BRCAJ
mutation were more sensitive to the cisplatinum-containing
chemotherapy, suggested by the finding that a second-look
operation revealed a high incidence of complete surgical/histo-
logical response in the BRCAI group in the study performed.
However, the possibility remains that some factors may
influence our results. First, because a majority of patients with
on July 1, 2018. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
30 40 50 60
Clinical Cancer Research 239
Tab le 3 5 urvival and disease-free survival at 5 years
A. Survival at 5 years
n 5-year survival rate” Median survival (months)
BRCAJ 13 0.786 115.48”
Seroustype 12 0.786 115.48’
Niigata University Hospital 29 0.303 52.75”
Serous type 20 0.193 36.69’Japan [Ochiai et al. (12)] 363 0.297
B. Disease-free survival at 5 years
n 5 year disease-free survival rate” Median disease-free interval (months)
BRCAI 10 0.591 91.43”Serous type 10 0.591 9l.43e
Niigata University Hospital 17 0.255 40.92”
Serous type 12 0.083 18.17e
“ Survival for ovarian cancer patients with BRCAJ mutation and sporadic cases at our hospital was calculated by using the Kaplan-Meier method.The data for survival for patients with stage III disease from multicenter studies (1980-1987) in Japan are also shown.
b p < 0.05 by the logarithmic rank test.Cp < 0.025 by the logarithmic rank test.d Disease-free survival for ovarian cancer patients with BRCA1 mutation and sporadic cases at our hospital was calculated by using the
Kaplan-Meier method.ep < 0.01 by the logarithmic rank test.
4’V
70
Age (y.o.)
Fig. 3 The penetrance of ovarian cancer among BRCAI carriers. Be-cause the ages at the time of diagnosis of 26 patients with mutations ofBRCAI and the ages of all mutation carriers were known, the penetrancewas estimated by the Kaplan-Meier method.
BRCAJ mutation probably had family histories of ovarian can-
cer, it is likely that these patients were diagnosed earlier than
usual as a result of participating in the cancer screening pro-
gram. Second, it is possible that patients with poor prognosis
could be eliminated from this analysis because of their early
death and that, consequently, only patients with a favorable
prognosis selectively participated in this program. In our iden-
tified BRCAI carrier patients, no ovarian cancer patients were
treated through a cancer screening program, and in a substantial
number of patients, the mutation of the BRCAJ gene was iden-
tified by analysis of DNA obtained from tissue blocks after the
patient’s death.
For the estimation of the survival rate, several protocols
have been proposed, such as a McNear test using population-
based data. Here, we used the widely accepted Kaplan-Meier
method, which calculates survival rate using data points for each
patient as follows: living or dead, the date of diagnosis, the
period of the last follow-up, and the patient’s condition at the
time of follow-up. Rubin et a!. (9) also described a similar
clinical course in which the survival of patients with BRCA 1
mutations and advanced-stage ovarian cancers appeared to be
notably longer than that of patients with sporadic ovarian can-
cers. In addition, Porter et al. (18) reported that the survival of
breast cancer patients with BRCAJ mutations was better than
that of whole breast cancer patients in the United Kingdom and
that lifetime risk of breast cancer was 88%, although they
identified 61 probable BRCAI carriers through genetic linkage
analysis. These results suggest that the differences of genetic
alteration may influence the clinical course in familial ovarian
cancers and sporadic ovarian cancers. It is estimated that about
10% of the patients with breast cancers have a family history of
the disease in the United States ( 19). BRCAI is thought to
account for approximately 45% of early-onset breast cancer
families (20), and it has been estimated that from 1 in 300 to I
in 800 women in the United States might carry BRCA1 muta-
tions (21). From a study on a large series of patients with
ovarian cancer at one hospital, the proportion of ovarian cancers
that is attributable to BRCAI mutations is estimated to be 5% in
the United Kingdom (22). In Japan, we have no data about the
incidence of BRCAI carriers based on such a large series of
ovarian cancers. However, from a study of mutational analysis
in 76 unselected ovarian cancers, the incidence of familial
ovarian cancer cases who carry BRCAJ mutations is expected to
be about 5% in all ovarian cancer cases in Japan (23), indicating
that the proportion of BRCA 1 carrier in ovarian cancer patients
is similar to Western countries. Lifetime risk calculated on 45
individuals with mutations in this study is estimated to be about
80%, indicating that Japanese BRCAJ carriers have almost an
equal level of lifetime risk of ovarian cancer to that in carriers
in Western countries. Because this analysis was based on a small
number of patients, we cannot exclude the possibility that our
on July 1, 2018. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

240 Ovarian Cancer Patients with BRC’AI Mutations
8. Tominaga, H., Aoki, K., Hanai, A., and Kurihara, N. The StatisticalYearbook for Cancer. p. 159. Tokyo. Japan: Shinohara Press, 1993.
lifetime risk calculation might be unsubstantial, and it appears to
be premature to elucidate the conclusion. However, a very rare
case has been reported about the clinical features of patients
with the mutation of BRCA I gene in Asian countries; hence the
findings in the present study would lead to worthwhile and
valuable information in the future. Nevertheless, because the
number of patients suffering from ovarian cancer is dramatically
increasing and because ovarian cancer is the most lethal gyne-
cological malignancy in Japan, the prospect of a project that
analyzes a hereditary ovarian cancer family, including counsel-
ing, or which clarifies the genetic abnormalities other than
mutations of the BRC’Al or BRC’A2 gene offers an attractive
model for further investigation.
ACKNOWLEDGMENTS
We are grateful to the patients and their families for participating in
this study and to Dr. 1. Jinbo (Tokyo Rosai Hospital) for providing
clinical information and blood and tumor samples of patients.
REFERENCES
I. Miki, Y., Swensen, J., Shattuck-Eidens, D., Futreal, P. A., Harshman,K.. Tavtigan. S.. Liu. Q.. Cochran, C.. Bennett, L. M., Ding, W., Bell,R., Rosenthal, J., Hussey, C.. Tran, 1., McClure, M., Frye, C., Hattier,1., Phelps, R., Haugen-Strano. A., Katcher, H., Yakumo, K., Gholami,z., Shaffer. D.. Stone. S., Bayer, S., Wray, C., Bodgen, R., Dayananth,
P.. Ward, J., Tonin, P., Narod, S., Bristow, P. K., Norris, F. H.,Helvering. L., Morrison, P., Rosteck, P., Lai, M., Barrett, J. C., Lewis,
C., Neuhausen, S., Cannon-Albright, L., Goldgar. D., Wiseman, R.,Kamb, A., and Skolnick, M. H. A strong candidate for the breast andovarian cancer susceptibility gene BRcAI. Science (Washington DC),
266: 66-71, 1994.
2. Szabo, C. I., and King, M-C. Inherited breast and ovarian cancer.Hum. Mol. Genet., 4: 1811-1817, 1995.
3. Takano, M. Aida, H., Tsuneki, I., Takakuwa, K., Hasegawa, I.,Tanaka, H., Saito, M., Tsuji, S., Sonoda, 1., Hatae, M., Chen, J-T.,
Takahashi, K.. Hasegawa, K., Toyoda, N., Saito, N., Yakushiji, M.,
Araki, T., and Tanaka, K. Mutational analysis ofBRCAI gene in ovariancancer and breast-ovarian cancer families in japan. Jpn. J. Cancer Res.,88: 407-413, 1997.
4. Inoue, R., Fukutomi, T., Ushijima, 1., Matsumoto, Y., Sugimura, T.,and Nagao. M. Germ-line mutation of BRCAI in Japanese breast cancer
families. Cancer Res., 55: 3521-3524, 1995.
5. Katagiri, 1.. Emi, N., Ito, I., Kobayashi, K.. Yoshimoto, M., Iwase,T., Kasumi, F., Miki, Y.. Skolnick, M. H., and Nakamura, Y. Mutationsin the BRCA I gene in Japanese breast cancer patients. Hum. Mutat., 7:334-339, 1996.
6. Parkin, M. D., Muir, S. C., Whelan, S. L., Gao, Y. T., Ferlay, J.. andPowell, J. Cancer Incidence of Five Continents. IARC Sci. Publ. No.120, pp. 301-501. Lyon, France: IARC. 1992.
7. Berry, D. A. Parmigiani, G.. Sanchez, J., Schildkraut, J., and Winer,E. Probability of carrying a mutation of breast-ovarian cancer geneBRCAI based on family history. J. Natl. Cancer Inst. (Bethesda), 89:
227-238, 1997.
9. Rubin, S. C., Benjamin, I., Behbakht, K., Takahashi, H., Morgan,M. A., LiVolsi, V. A., Berchuck, A., Muto, M. G., Garber, J. E., Weber,B. L., Lynch, H. T., and Boyd, J. Clinical and pathological features ofovarian cancer in women with germ-line mutations of BRCAJ. N. Engl.J. Med., 335: 1413-1416, 1996.
10. Buller, R. E., Anderson, B., Connor, J. P., and Robinson, R. Fa-milial ovarian cancer. Gynecol. Oncol., 51: 160-166, 1993.
1 1. Marcus, J. N., Watson, P., Page, D. L., Narod, S. A., Lenoir, G. M.,Tonin, P., Linder-Stephenson, L., Salerno, 0., Conway, T. A., andLynch, H. T. Hereditary breast cancer: pathobiobogy, prognosis, BRCAJand BRCA2 gene linkage. Cancer (Phila.), 77: 697-709, 1996.
12. Ochiai, K., Sasaki, H., Terashima, Y., and Fukushima, M. Prognos-tic factor analysis and treatment results of ovarian cancer in Japan. Int.
J. Technol. Assessment Health Care, 10: 406-425, 1994.
13. Sambrook, J., Fritsch, E. F., and Maniatis, T. Isolation of high-
molecular-weight DNA from mammalian cells. In: Molecular Cloning:A Laboratory Manual, pp. 9. 14-9.23. Cold Spring Harbor, NY: ColdSpring Harbor Laboratory, 1989.
14. Kaplan. E.. and Meier, P. Nonparametric estimation from incom-plete observations. J. Am. Stat. Assoc., 53: 457-481, 1958.
15. Mantel, N. Evaluation of survival data and two new rank orderstatistics arising in its consideration. Cancer Chemother. Rep., 50:
163-170, 1966.
16. Kodama, S., and Tanaka, K. Today’s stats (ovary). Ann. CancerRes. Ther., 5: 75, 1996.
17. McGuire, W. P., Hoskins, W. J., Brady, M. F., Kucera, P. R.,Partridge, E. E., Look, K. Y., Clarke-Pearson, D. L., and Davidson, M.Cyclophosphamide and cisplatin compared with paclitaxel and cisplatinin patients with stage and stage ovarian cancer. N Engl. J. Med., 334:
1-6, 1996.
18. Porter, D. E., Cohen, B. B., Wallace, M. R., Smyth, E., Chetty, U.,Dixon, J. M., Steel, C. M., and Carter, D. C. Breast cancer incidence,penetrance and survival in probable carriers of BRCA1 gene mutation in
families linked to BRCAI on chromosome l7q12-2l. Br. J. Surg., 81:
1512-1515, 1994.
19. Ottman, R., Pike, M. C., King, M. C., Casagrande, J. T., andHenderson, B. Familial breast cancer in a population-based series.Am. J. Epidemiol., 123: 15-21, 1986.
20. Easton, D. F., Bishop, D. T., Ford, D., Crockford, G. 0., and theBreast Cancer Consortium. Genetic linkage analysis in familial breastand ovarian cancer: results from 214 families. Am. J. Hum. Genet., 52:
678-701, 1993.
21. Struewing, J. P., Abebiovich, D., Peretz, T., Avishai, N., Kaback,
M. M., Collins, F. S., and Brody, L. C. The carrier frequency of the
BRCAJ l85delAG mutation is approximately 1% in Ashkenazi Jewishindividuals. Nat. Genet., 11: 198-200, 1995.
22. Stratton, J. F., Gayther, S. A., Russell, P., Dearden, J., Gore, M.,Blake, P., Easton, D., and Ponder, B. A. J. Contribution of BRCAJmutations to ovarian cancer. N. Engl. J. Med., 336: 1125-1130,
1997.
23. Matsushima, M., Kobayashi, K., Emi, M., Saito, J., Suzumori, K.,and Nakamura, Y. Mutation analysis of the BRCAJ gene in 76 Japaneseovarian cancer patients: four germ-line mutations, but no evidence ofsomatic mutation. Hum. Mol. Genet., 4: 1953-1956, 1995.
on July 1, 2018. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
1998;4:235-240. Clin Cancer Res H Aida, K Takakuwa, H Nagata, et al. germ-line mutations of BRCA1.Clinical features of ovarian cancer in Japanese women with
Updated version
http://clincancerres.aacrjournals.org/content/4/1/235
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/4/1/235To request permission to re-use all or part of this article, use this link
on July 1, 2018. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from





























