Embed Size (px)
Citation preview
CLINICAL STUDIES
ANALYSIS OF COMPLICATIONS OF RADIOFREQUENCY
PALLIDOTOMY
Zhang Hua, M.D.Department of Neurosurgery,Tangdu Hospital, The FourthMilitary Medical University, Xi’an,People’s Republic of China
Gao Guodong, M.D.,Ph.D.Department of Neurosurgery,Tangdu Hospital, The FourthMilitary Medical University, Xi’an,People’s Republic of China
Liang Qinchuan, M.D.Department of Neurosurgery,Tangdu Hospital, The FourthMilitary Medical University, Xi’an,People’s Republic of China
Zhao Yaqun, M.D.Department of Neurosurgery,Tangdu Hospital, The FourthMilitary Medical University, Xi’an,People’s Republic of China
Wang Qinfen, M.D.Department of Neurosurgery,Tangdu Hospital, The FourthMilitary Medical University, Xi’an,People’s Republic of China
Wang Xuelian, M.D.Department of Neurosurgery,Tangdu Hospital, The FourthMilitary Medical University, Xi’an,People’s Republic of China
Reprint requests:Zhang Hua, M.D., Department ofNeurosurgery, Tangdu Hospital,The Fourth Military MedicalUniversity, Xi’an, ShaanxiProvince, People’s Republic ofChina, 710038.Email: [email protected]
Received, October 25, 2001.
Accepted, August 12, 2002.
OBJECTIVE: To systematically report the complications of pallidotomy and to tenta-tively determine the incidences of complications of pallidotomy, possible influencingfactors, and the acceptability of symptomatic hemorrhage rates for microelectrode-guided pallidotomy.METHODS: Clinical events were analyzed for 1116 patients with Parkinson’s diseasewho underwent microelectrode-guided pallidotomies at our center. Complicationsincluded visual field deficits, weakness, fatigue, hypersomnia, drooling, dysphagia,speech disorders, hiccups, hemorrhage, seizures, apraxia, coma, infection, mentalconfusion, and impaired memory. Complication rates for bilateral pallidotomy anddouble-lesion groups were compared with those for unilateral pallidotomy and single-lesion groups, respectively.RESULTS: Among the total of 1116 patients, the incidences of visual field deficits,weakness, fatigue, hypersomnia, drooling, dysphagia, and speech disorders were 0.4,4.2, 19.9, 12.4, 7.0, 3.7, and 11.9%, respectively. Symptomatic hemorrhage wasobserved for 17 patients, apraxia for 3 patients, coma for 2 patients, mental confusionfor 24 patients, and impaired memory for 18 of the 1116 patients. The incidences offatigue, speech disorders, drooling, dysphagia, and hypersomnia were 18.1, 10.3, 5.2,2.4, and 11.6%, respectively, in the unilateral pallidotomy group and 34.9, 25.5, 22.6,14.2, and 17.0%, respectively, in the staged pallidotomy group. Of the three patientswho underwent simultaneous bilateral pallidotomies (all �50 yr of age), all developedsevere fatigue and two exhibited drooling and dysphagia. The incidences of weakness,fatigue, speech disorders, drooling, dysphagia, and hypersomnia were 8.7, 30.4, 18.8,7.2, 2.9, and 20.3%, respectively, in the double-lesion group and 3.2, 17.2, 9.7, 5.0,2.3, and 11.5%, respectively, in the single-lesion group.CONCLUSION: Staged bilateral pallidotomy should be carefully evaluated beforedecision-making, whereas simultaneous bilateral pallidotomy is undesirable. Our studysuggests that the size of the final lesion should be limited, to minimize the risks ofcomplications. The incidence of symptomatic hemorrhage in microelectrode-guided pal-lidotomy is low and acceptable, because of the benefits of microelectrode-guidedpallidotomy.
KEY WORDS: Complication, Pallidotomy, Parkinson’s disease, Stereotaxy
Neurosurgery 52:89-101, 2003 DOI: 10.1227/01.NEU.0000038933.95427.AE www.neurosurgery-online.com
In functional neurosurgery to treat Parkin-son’s disease (PD) and other movementdisorders, the initial attempts were di-
rected at different levels of the nervous system(9, 15, 30, 32, 35, 36, 44). Pallidotomy, whichwas first reported by Guiot and Brion (14) andNarabayashi and Okuma (31) in 1953, hasbeen used as a surgical treatment for PD fornearly 50 years. The most effective target inthe pallidum, as now widely accepted, is in
the posteroventral part of the nucleus (24, 25,41). Pallidotomy is now used in almost everyfunctional neurosurgery center in the world.Successful experiences with pallidotomieshave been reported by many teams in func-tional neurosurgery centers throughout theworld (8, 19, 22, 25, 26, 28, 29, 41, 43). Com-plications of pallidotomies have also been re-ported, however (2, 7, 11, 17, 19, 22, 23, 25, 28,29, 38, 41). Most of the reported complications
NEUROSURGERY VOLUME 52 | NUMBER 1 | JANUARY 2003 | 89

involved a limited number of patients and varied amongreports. Alkhani and Lozano (1) described pallidotomy com-plications for 1510 patients identified in the National Libraryof Medicine online PubMed database. However, there hasbeen no systematic report of a larger number of patientstreated at a single institution, to provide an overview of pal-lidotomy complications.
The purposes of this article are to systematically reportpallidotomy complications observed among a large number ofpatients treated at our center and to tentatively answer thefollowing questions. 1) Is the incidence of complications withbilateral pallidotomy acceptable? 2) Is the incidence of com-plications affected by different lesioning procedures? 3) Is theincidence of symptomatic hemorrhage with microelectrode-guided pallidotomy acceptable?
PATIENTS AND METHODS
Patient Population
Between 1997 and 2001, 1116 patients with PD underwentpallidotomies at our institution; 713 were male and 403 werefemale (mean age, 57.4 yr). All patients were diagnosed ashaving idiopathic PD. Most responded to levodopa. In addi-tion to the main symptoms of PD, such as tremor, rigidity, andbradykinesia/akinesia, some of the patients also experienceddrug-induced dyskinesia, freezing episodes, and pain. Boththe inclusion and exclusion criteria were the same as thoseused by most other medical centers (5, 19, 26, 43). Of the 1116patients, 1007 underwent unilateral pallidotomies, 106 under-went staged bilateral pallidotomies, and 3 underwent simul-taneous bilateral pallidotomies. The characteristics of the pa-tients are summarized in Table 1.
Stereotactic Procedure
Most patients discontinued the use of antiparkinsonianmedication at least 12 hours before pallidotomy; some patientscontinued to use their medication if they could not bear the“off-state.” Either meperidine or midazolam was adminis-tered for head frame fixation. No sedation was used duringthe procedure, to allow the necessary cooperation of the pa-tients. During surgery, the average blood pressure was con-trolled at less than 95 mm Hg, to minimize the risk ofhemorrhage.
A Cosman-Roberts-Wells stereotactic head frame (Radion-ics, Burlington, MA) was placed as parallel to the intercom-missural plane as possible, with local anesthesia. Patients un-derwent computed tomographic (CT) scanning (TomascanAV; Phillips Medical Systems, Eindhoven, The Netherlands),and the data were transported to a workstation (Phillips Med-ical Systems) for reconstruction of three-dimensional images.After identification of the anterior and posterior commissureson a reconstructed sagittal image at the workstation, a tenta-tive target was located at a point 2 to 3 mm anterior to themidpoint of the anterior commissure-posterior commissureline, 4 to 6 mm below the intercommissural line, and 18 to 22
mm lateral to the midline of the third ventricle, because ofvariations in anatomic structures.
After the establishment of appropriate coordinates, the pa-tient was taken to the operating room and kept in a supineposition on the operating table. Local anesthesia was admin-istered at the entry point on the scalp, just anterior to thecoronal suture and 3 cm from the midline. After the scalpincision, a wide burr hole was drilled and a guide tube wasdirected into the cortex, with careful observation.
Microelectrode Localization
Microelectrode recording was performed with platinum/iridium-coated microelectrodes with a tip diameter of 2 to 4�m (impedance, 0.2–0.8 M� at 1000 Hz). The microelectrodewas inserted into the guide tube and advanced to the targetwith a water hydraulic or electric microdrive, in the micronrange or coarse range. The methods for microelectrode record-ing were similar to those noted in previous reports (28, 43).The recording was started 15 mm above the original target. Ahead stage consisting of a preamplifier and the hydraulic orelectric drive was mounted on the arc adapter. Signals fromthe preamplifier were amplified, filtered, and displayed on anoscilloscope window. The recording continued from the glo-bus pallidus (GP) externa, the external segment of the GPinterna (GPi), the internal segment of the GPi, and the ansalenticulars. During the recording, we first recorded cell activ-ity from the GP along the original trajectory. Because cell
TABLE 1. Characteristics of the patients whounderwent pallidotomiesa
Characteristic Value
Sex (no. of patients)Male 713Female 403
Age (yr)Mean � SD 57.4 � 9.3Range 34–78
Disease duration (yr)Mean � SD 7.7 � 4.2Range 3–32
Type of pallidotomy (no. of patients)Unilateral 1007
R-pallidotomy 492L-pallidotomy 515
Staged bilateral 106Interval between operations (mo)
Mean � SD 11.6 � 6.9Range 0.5–32
Simultaneous bilateral 3
a SD, standard deviation; R-pallidotomy, right-sided pallidotomy;L-pallidotomy, left-sided pallidotomy.
HUA ET AL.
90 | VOLUME 52 | NUMBER 1 | JANUARY 2003 www.neurosurgery-online.com

discharges disappeared as the microelectrode was advancedbeyond the GPi, the border point of the GPi on the firsttrajectory was identified. After completion of the microrecord-ing of the first trajectory, the microelectrode was adjusted 2 to3 mm anterior or posterior to the primary trajectory in thesame plane, and the border points of the GPi were identified.All GP border points along the trajectories were marked. Afterconnection of all points in a sagittal plane, the posterior borderof the posteroventral GP was delineated. By moving the mi-croelectrode medially or laterally in the same plane in thesame way, the medial border of the posteroventral GP couldalso be identified. During identification of the posterior andmedial borders of the GPi, the ventral border of the GPi wasidentified. The number of microelectrode passes ranged fromthree to nine. Generally, four or five microelectrode passeswere performed for each patient.
Data from the microelectrode mapping were analyzed afterthe completion of all recordings. A border in a sagittal planeindicated that the optimal target was approximately 2 to 3 mmanterior to it. In a coronal plane, the optimal target was ap-proximately 2 to 3 mm lateral to the medial border. The initiallesion target was finally located 3 mm lateral to the medialborder, 2 to 3 mm anterior to the posterior border, and close tothe most ventral border of the pallidum along the trajectory.
Radiofrequency Thermolesioning
A lesioning electrode with an exposed tip of either 1.1 � 2mm or 1.8 � 2 mm (Radionics) was advanced to the finaltarget. Macrostimulation thresholds for the presence of motorand visual responses were no less than 1.3 and 1.0 V, respec-tively, with a stimulating pulse of 100 Hz and a 1.0-millisecond pulse duration. With an electrode of 1.1 � 2 mm,the lesioning was started with a radiofrequency generator(RFG-3CF; Radionics) at 75°C for 70 seconds. After the initiallesioning, the electrode was withdrawn in 1.5-mm incrementsand the lesioning process was repeated at three depths, at80°C, 85°C, and 85°C for 70 seconds. With an electrode of 1.8� 2 mm, after the initial lesioning at 70°C for 70 seconds, theelectrode was withdrawn in 1.5-mm increments and the le-sioning process was repeated at three depths, at 75°C, 82°C,and 82°C for 70 seconds.
Sixty-nine patients received double lesions in unilateral pal-lidotomies. All of them underwent pallidotomies with a le-sioning electrode of 1.1 � 2 mm. After lesioning of the firsttrajectory with the method described above, lesioning of asecond trajectory, parallel and 2 mm anterior to the first, wasperformed. For the second lesion, the electrode was with-drawn in 1.5-mm increments from 1 mm above the lowest GPiborder and the lesioning process was performed at threedepths, at 75°C, 80°C, and 80°C for 70 seconds.
Complication Description
Generally, patients were discharged 8 days after surgery. Inaddition to regular physical examinations during the hospitalstays, questionnaire and telephone contacts after discharge
were used for the evaluation of complications. Patients withcomplications in this series were monitored for at least 3months. During the hospital stays, physicians performed neu-rological examinations of the patients once each day. All pa-tients with complications underwent CT scanning. The com-plications included visual field deficits, weakness, fatigue,hypersomnia, drooling, dysphagia, speech disorders (hy-pophonia and dysarthria), hiccups, symptomatic hemorrhage,seizures, apraxia, coma, infection, mental confusion, and im-paired memory. Weakness, i.e., loss of movement or strengthcaused by internal capsule injury, included acute weakness(immediately after surgery) and delayed weakness. Becausenot all patients underwent CT scanning or magnetic resonanceimaging, we cannot establish exactly how many patients de-veloped hemorrhage. All patients with complications under-went CT scanning, however, and we can thus determine ex-actly how many patients developed symptomatichemorrhage. After surgery, patients with hypersomnia exhib-ited increases in sleep (often 2–3 h/d) and were drowsy in thedaytime.
Statistical Analyses
SPSS 10.0 software (SPSS, Inc., Chicago, IL) was used forstatistical analyses. A �2 analysis was used to compare theincidences of complications for the staged bilateral group andthe unilateral group and to compare the incidences of compli-cations in the survey reported by Alkhani and Lozano (1) andour series. A �2 analysis was also used for other comparisonsof incidences.
RESULTS
Improvement
Most patients tolerated the operation well. Its benefits to thepatients were similar to those reported by other authors (3, 8,24, 26, 33, 38, 43). Details will be reported in a separate article.
Complications
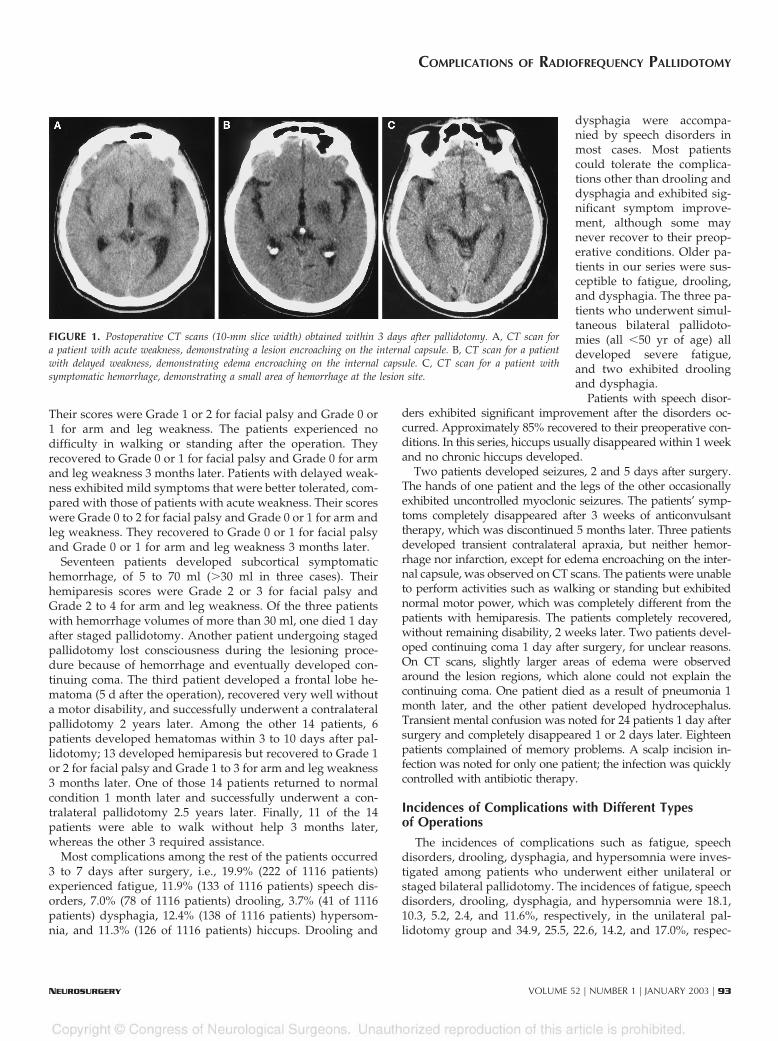
Of the total of 1116 patients, 364 patients experienced com-plications. Some patients developed a single complication,whereas others developed multiple complications. The com-plications are detailed in Table 2. Of our series of 1116 patients,4 patients (0.4%) experienced unrecoverable visual field defi-cits. Another seven patients (0.6%) complained of deteriora-tion of vision without objective visual field deficits. Forty-seven patients (4.2%) developed weakness, of whom 13experienced acute weakness and 34 experienced delayedweakness. No confirmed hemorrhage was observed on post-operative scans for the patients with weakness. The items offacial palsy and motor arm and leg weakness in the NationalInstitutes of Health Stroke Scale (12) were used to evaluate theseverity of weakness. Five of the 13 patients with acute weak-ness, for whom lesions encroaching on the internal capsule(Fig. 1) were observed on postoperative scans, developed se-vere acute weakness. The scores for those five patients were
COMPLICATIONS OF RADIOFREQUENCY PALLIDOTOMY
NEUROSURGERY VOLUME 52 | NUMBER 1 | JANUARY 2003 | 91
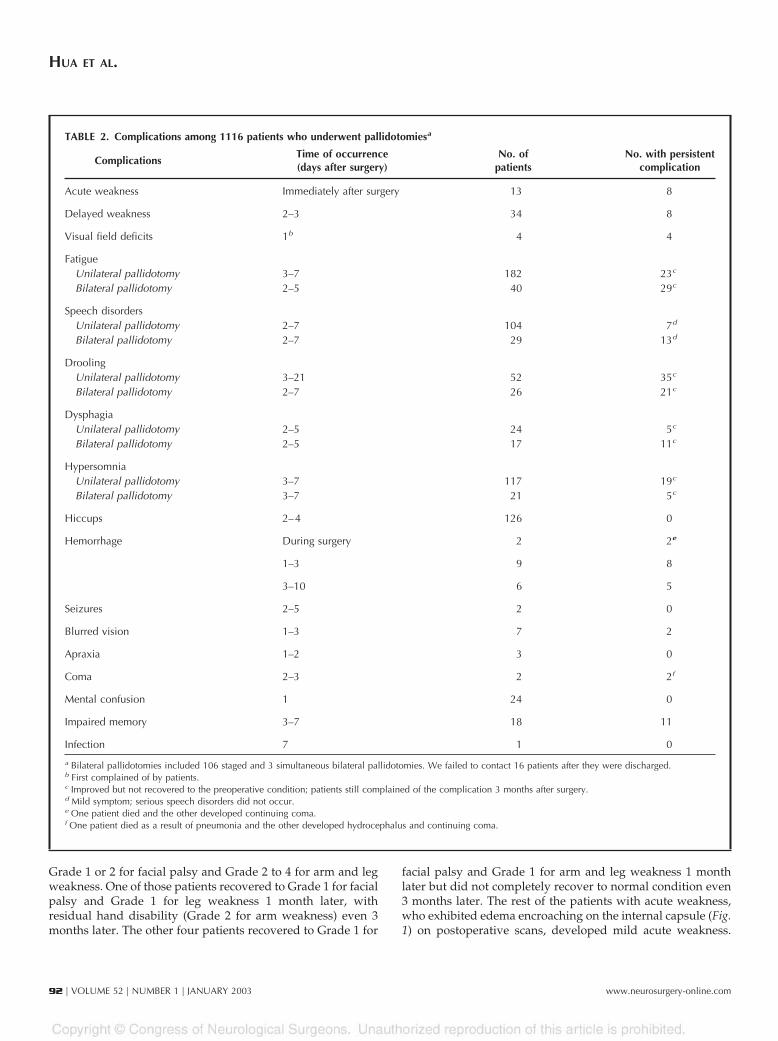
Grade 1 or 2 for facial palsy and Grade 2 to 4 for arm and legweakness. One of those patients recovered to Grade 1 for facialpalsy and Grade 1 for leg weakness 1 month later, withresidual hand disability (Grade 2 for arm weakness) even 3months later. The other four patients recovered to Grade 1 for
facial palsy and Grade 1 for arm and leg weakness 1 monthlater but did not completely recover to normal condition even3 months later. The rest of the patients with acute weakness,who exhibited edema encroaching on the internal capsule (Fig.1) on postoperative scans, developed mild acute weakness.
TABLE 2. Complications among 1116 patients who underwent pallidotomiesa
ComplicationsTime of occurrence(days after surgery)
No. ofpatients
No. with persistentcomplication
Acute weakness Immediately after surgery 13 8
Delayed weakness 2–3 34 8
Visual field deficits 1b 4 4
FatigueUnilateral pallidotomy 3–7 182 23c
Bilateral pallidotomy 2–5 40 29c
Speech disordersUnilateral pallidotomy 2–7 104 7d
Bilateral pallidotomy 2–7 29 13d
DroolingUnilateral pallidotomy 3–21 52 35c
Bilateral pallidotomy 2–7 26 21c
DysphagiaUnilateral pallidotomy 2–5 24 5c
Bilateral pallidotomy 2–5 17 11c
HypersomniaUnilateral pallidotomy 3–7 117 19c
Bilateral pallidotomy 3–7 21 5c
Hiccups 2–4 126 0
Hemorrhage During surgery 2 2e
1–3 9 8
3–10 6 5
Seizures 2–5 2 0
Blurred vision 1–3 7 2
Apraxia 1–2 3 0
Coma 2–3 2 2f
Mental confusion 1 24 0
Impaired memory 3–7 18 11
Infection 7 1 0
a Bilateral pallidotomies included 106 staged and 3 simultaneous bilateral pallidotomies. We failed to contact 16 patients after they were discharged.b First complained of by patients.c Improved but not recovered to the preoperative condition; patients still complained of the complication 3 months after surgery.d Mild symptom; serious speech disorders did not occur.e One patient died and the other developed continuing coma.f One patient died as a result of pneumonia and the other developed hydrocephalus and continuing coma.
HUA ET AL.
92 | VOLUME 52 | NUMBER 1 | JANUARY 2003 www.neurosurgery-online.com
Their scores were Grade 1 or 2 for facial palsy and Grade 0 or1 for arm and leg weakness. The patients experienced nodifficulty in walking or standing after the operation. Theyrecovered to Grade 0 or 1 for facial palsy and Grade 0 for armand leg weakness 3 months later. Patients with delayed weak-ness exhibited mild symptoms that were better tolerated, com-pared with those of patients with acute weakness. Their scoreswere Grade 0 to 2 for facial palsy and Grade 0 or 1 for arm andleg weakness. They recovered to Grade 0 or 1 for facial palsyand Grade 0 or 1 for arm and leg weakness 3 months later.
Seventeen patients developed subcortical symptomatichemorrhage, of 5 to 70 ml (�30 ml in three cases). Theirhemiparesis scores were Grade 2 or 3 for facial palsy andGrade 2 to 4 for arm and leg weakness. Of the three patientswith hemorrhage volumes of more than 30 ml, one died 1 dayafter staged pallidotomy. Another patient undergoing stagedpallidotomy lost consciousness during the lesioning proce-dure because of hemorrhage and eventually developed con-tinuing coma. The third patient developed a frontal lobe he-matoma (5 d after the operation), recovered very well withouta motor disability, and successfully underwent a contralateralpallidotomy 2 years later. Among the other 14 patients, 6patients developed hematomas within 3 to 10 days after pal-lidotomy; 13 developed hemiparesis but recovered to Grade 1or 2 for facial palsy and Grade 1 to 3 for arm and leg weakness3 months later. One of those 14 patients returned to normalcondition 1 month later and successfully underwent a con-tralateral pallidotomy 2.5 years later. Finally, 11 of the 14patients were able to walk without help 3 months later,whereas the other 3 required assistance.
Most complications among the rest of the patients occurred3 to 7 days after surgery, i.e., 19.9% (222 of 1116 patients)experienced fatigue, 11.9% (133 of 1116 patients) speech dis-orders, 7.0% (78 of 1116 patients) drooling, 3.7% (41 of 1116patients) dysphagia, 12.4% (138 of 1116 patients) hypersom-nia, and 11.3% (126 of 1116 patients) hiccups. Drooling and
dysphagia were accompa-nied by speech disorders inmost cases. Most patientscould tolerate the complica-tions other than drooling anddysphagia and exhibited sig-nificant symptom improve-ment, although some maynever recover to their preop-erative conditions. Older pa-tients in our series were sus-ceptible to fatigue, drooling,and dysphagia. The three pa-tients who underwent simul-taneous bilateral pallidoto-mies (all �50 yr of age) alldeveloped severe fatigue,and two exhibited droolingand dysphagia.
Patients with speech disor-ders exhibited significant improvement after the disorders oc-curred. Approximately 85% recovered to their preoperative con-ditions. In this series, hiccups usually disappeared within 1 weekand no chronic hiccups developed.
Two patients developed seizures, 2 and 5 days after surgery.The hands of one patient and the legs of the other occasionallyexhibited uncontrolled myoclonic seizures. The patients’ symp-toms completely disappeared after 3 weeks of anticonvulsanttherapy, which was discontinued 5 months later. Three patientsdeveloped transient contralateral apraxia, but neither hemor-rhage nor infarction, except for edema encroaching on the inter-nal capsule, was observed on CT scans. The patients were unableto perform activities such as walking or standing but exhibitednormal motor power, which was completely different from thepatients with hemiparesis. The patients completely recovered,without remaining disability, 2 weeks later. Two patients devel-oped continuing coma 1 day after surgery, for unclear reasons.On CT scans, slightly larger areas of edema were observedaround the lesion regions, which alone could not explain thecontinuing coma. One patient died as a result of pneumonia 1month later, and the other patient developed hydrocephalus.Transient mental confusion was noted for 24 patients 1 day aftersurgery and completely disappeared 1 or 2 days later. Eighteenpatients complained of memory problems. A scalp incision in-fection was noted for only one patient; the infection was quicklycontrolled with antibiotic therapy.
Incidences of Complications with Different Typesof Operations
The incidences of complications such as fatigue, speechdisorders, drooling, dysphagia, and hypersomnia were inves-tigated among patients who underwent either unilateral orstaged bilateral pallidotomy. The incidences of fatigue, speechdisorders, drooling, dysphagia, and hypersomnia were 18.1,10.3, 5.2, 2.4, and 11.6%, respectively, in the unilateral pal-lidotomy group and 34.9, 25.5, 22.6, 14.2, and 17.0%, respec-
FIGURE 1. Postoperative CT scans (10-mm slice width) obtained within 3 days after pallidotomy. A, CT scan fora patient with acute weakness, demonstrating a lesion encroaching on the internal capsule. B, CT scan for a patientwith delayed weakness, demonstrating edema encroaching on the internal capsule. C, CT scan for a patient withsymptomatic hemorrhage, demonstrating a small area of hemorrhage at the lesion site.
COMPLICATIONS OF RADIOFREQUENCY PALLIDOTOMY
NEUROSURGERY VOLUME 52 | NUMBER 1 | JANUARY 2003 | 93
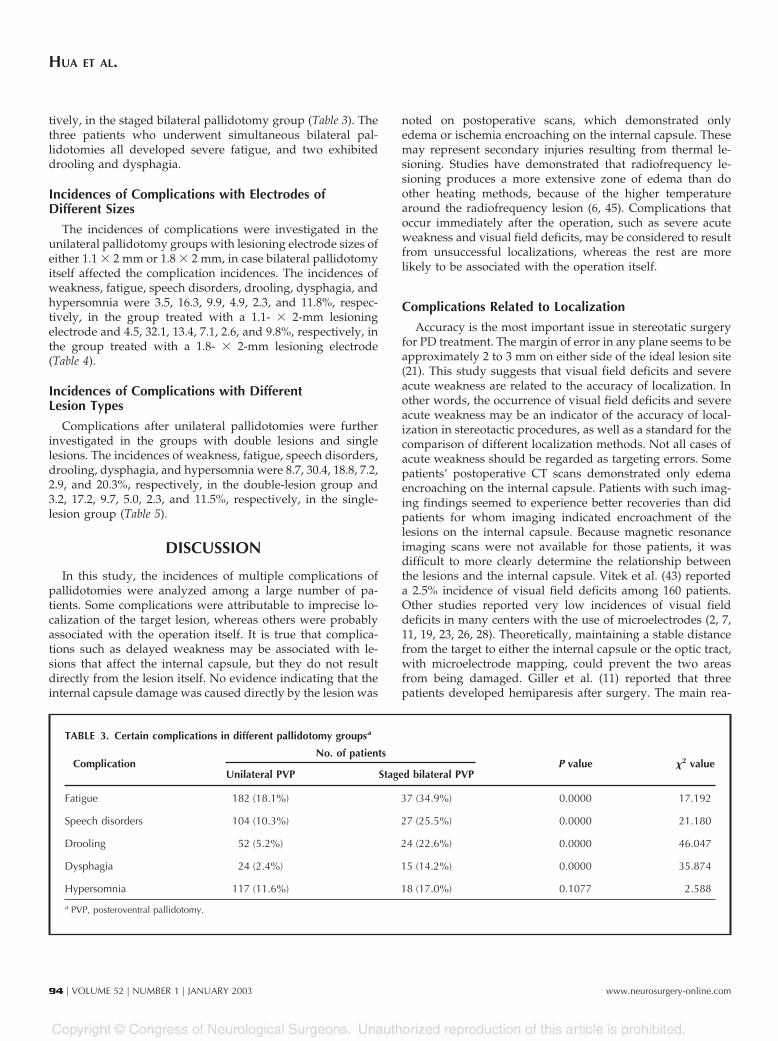
tively, in the staged bilateral pallidotomy group (Table 3). Thethree patients who underwent simultaneous bilateral pal-lidotomies all developed severe fatigue, and two exhibiteddrooling and dysphagia.
Incidences of Complications with Electrodes ofDifferent Sizes
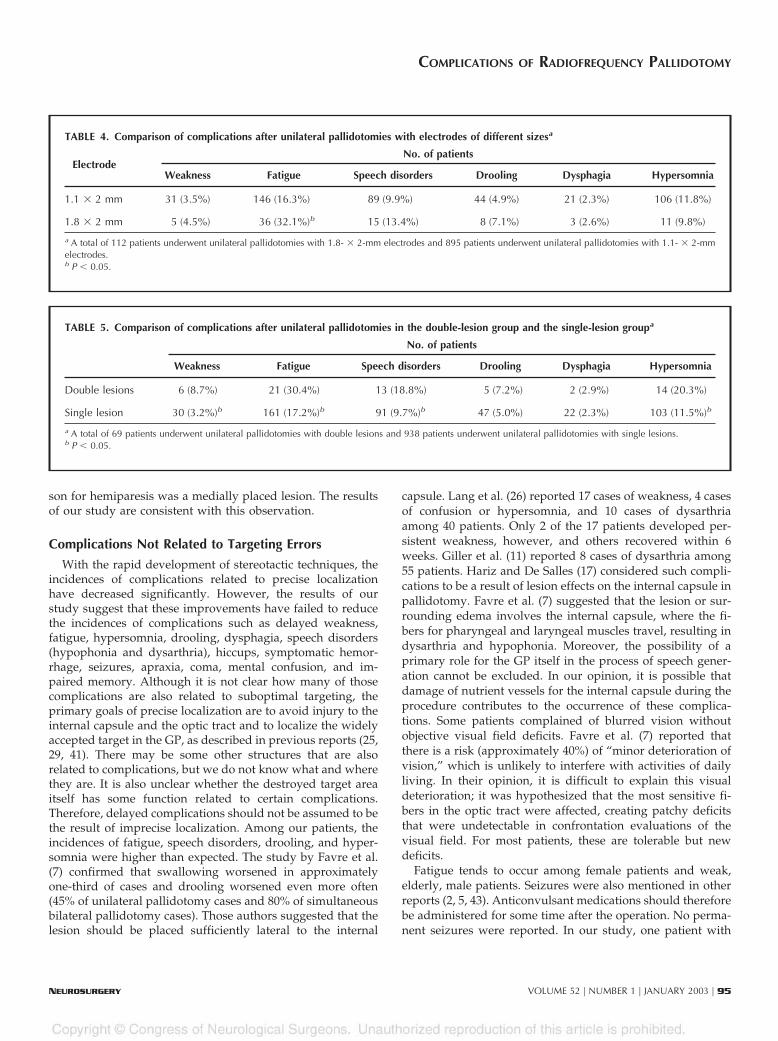
The incidences of complications were investigated in theunilateral pallidotomy groups with lesioning electrode sizes ofeither 1.1 � 2 mm or 1.8 � 2 mm, in case bilateral pallidotomyitself affected the complication incidences. The incidences ofweakness, fatigue, speech disorders, drooling, dysphagia, andhypersomnia were 3.5, 16.3, 9.9, 4.9, 2.3, and 11.8%, respec-tively, in the group treated with a 1.1- � 2-mm lesioningelectrode and 4.5, 32.1, 13.4, 7.1, 2.6, and 9.8%, respectively, inthe group treated with a 1.8- � 2-mm lesioning electrode(Table 4).
Incidences of Complications with DifferentLesion Types
Complications after unilateral pallidotomies were furtherinvestigated in the groups with double lesions and singlelesions. The incidences of weakness, fatigue, speech disorders,drooling, dysphagia, and hypersomnia were 8.7, 30.4, 18.8, 7.2,2.9, and 20.3%, respectively, in the double-lesion group and3.2, 17.2, 9.7, 5.0, 2.3, and 11.5%, respectively, in the single-lesion group (Table 5).
DISCUSSION
In this study, the incidences of multiple complications ofpallidotomies were analyzed among a large number of pa-tients. Some complications were attributable to imprecise lo-calization of the target lesion, whereas others were probablyassociated with the operation itself. It is true that complica-tions such as delayed weakness may be associated with le-sions that affect the internal capsule, but they do not resultdirectly from the lesion itself. No evidence indicating that theinternal capsule damage was caused directly by the lesion was
noted on postoperative scans, which demonstrated onlyedema or ischemia encroaching on the internal capsule. Thesemay represent secondary injuries resulting from thermal le-sioning. Studies have demonstrated that radiofrequency le-sioning produces a more extensive zone of edema than doother heating methods, because of the higher temperaturearound the radiofrequency lesion (6, 45). Complications thatoccur immediately after the operation, such as severe acuteweakness and visual field deficits, may be considered to resultfrom unsuccessful localizations, whereas the rest are morelikely to be associated with the operation itself.
Complications Related to Localization
Accuracy is the most important issue in stereotatic surgeryfor PD treatment. The margin of error in any plane seems to beapproximately 2 to 3 mm on either side of the ideal lesion site(21). This study suggests that visual field deficits and severeacute weakness are related to the accuracy of localization. Inother words, the occurrence of visual field deficits and severeacute weakness may be an indicator of the accuracy of local-ization in stereotactic procedures, as well as a standard for thecomparison of different localization methods. Not all cases ofacute weakness should be regarded as targeting errors. Somepatients’ postoperative CT scans demonstrated only edemaencroaching on the internal capsule. Patients with such imag-ing findings seemed to experience better recoveries than didpatients for whom imaging indicated encroachment of thelesions on the internal capsule. Because magnetic resonanceimaging scans were not available for those patients, it wasdifficult to more clearly determine the relationship betweenthe lesions and the internal capsule. Vitek et al. (43) reporteda 2.5% incidence of visual field deficits among 160 patients.Other studies reported very low incidences of visual fielddeficits in many centers with the use of microelectrodes (2, 7,11, 19, 23, 26, 28). Theoretically, maintaining a stable distancefrom the target to either the internal capsule or the optic tract,with microelectrode mapping, could prevent the two areasfrom being damaged. Giller et al. (11) reported that threepatients developed hemiparesis after surgery. The main rea-
TABLE 3. Certain complications in different pallidotomy groupsa
ComplicationNo. of patients
P value �2 valueUnilateral PVP Staged bilateral PVP
Fatigue 182 (18.1%) 37 (34.9%) 0.0000 17.192
Speech disorders 104 (10.3%) 27 (25.5%) 0.0000 21.180
Drooling 52 (5.2%) 24 (22.6%) 0.0000 46.047
Dysphagia 24 (2.4%) 15 (14.2%) 0.0000 35.874
Hypersomnia 117 (11.6%) 18 (17.0%) 0.1077 2.588
a PVP, posteroventral pallidotomy.
HUA ET AL.
94 | VOLUME 52 | NUMBER 1 | JANUARY 2003 www.neurosurgery-online.com
son for hemiparesis was a medially placed lesion. The resultsof our study are consistent with this observation.
Complications Not Related to Targeting Errors
With the rapid development of stereotactic techniques, theincidences of complications related to precise localizationhave decreased significantly. However, the results of ourstudy suggest that these improvements have failed to reducethe incidences of complications such as delayed weakness,fatigue, hypersomnia, drooling, dysphagia, speech disorders(hypophonia and dysarthria), hiccups, symptomatic hemor-rhage, seizures, apraxia, coma, mental confusion, and im-paired memory. Although it is not clear how many of thosecomplications are also related to suboptimal targeting, theprimary goals of precise localization are to avoid injury to theinternal capsule and the optic tract and to localize the widelyaccepted target in the GP, as described in previous reports (25,29, 41). There may be some other structures that are alsorelated to complications, but we do not know what and wherethey are. It is also unclear whether the destroyed target areaitself has some function related to certain complications.Therefore, delayed complications should not be assumed to bethe result of imprecise localization. Among our patients, theincidences of fatigue, speech disorders, drooling, and hyper-somnia were higher than expected. The study by Favre et al.(7) confirmed that swallowing worsened in approximatelyone-third of cases and drooling worsened even more often(45% of unilateral pallidotomy cases and 80% of simultaneousbilateral pallidotomy cases). Those authors suggested that thelesion should be placed sufficiently lateral to the internal
capsule. Lang et al. (26) reported 17 cases of weakness, 4 casesof confusion or hypersomnia, and 10 cases of dysarthriaamong 40 patients. Only 2 of the 17 patients developed per-sistent weakness, however, and others recovered within 6weeks. Giller et al. (11) reported 8 cases of dysarthria among55 patients. Hariz and De Salles (17) considered such compli-cations to be a result of lesion effects on the internal capsule inpallidotomy. Favre et al. (7) suggested that the lesion or sur-rounding edema involves the internal capsule, where the fi-bers for pharyngeal and laryngeal muscles travel, resulting indysarthria and hypophonia. Moreover, the possibility of aprimary role for the GP itself in the process of speech gener-ation cannot be excluded. In our opinion, it is possible thatdamage of nutrient vessels for the internal capsule during theprocedure contributes to the occurrence of these complica-tions. Some patients complained of blurred vision withoutobjective visual field deficits. Favre et al. (7) reported thatthere is a risk (approximately 40%) of “minor deterioration ofvision,” which is unlikely to interfere with activities of dailyliving. In their opinion, it is difficult to explain this visualdeterioration; it was hypothesized that the most sensitive fi-bers in the optic tract were affected, creating patchy deficitsthat were undetectable in confrontation evaluations of thevisual field. For most patients, these are tolerable but newdeficits.
Fatigue tends to occur among female patients and weak,elderly, male patients. Seizures were also mentioned in otherreports (2, 5, 43). Anticonvulsant medications should thereforebe administered for some time after the operation. No perma-nent seizures were reported. In our study, one patient with
TABLE 4. Comparison of complications after unilateral pallidotomies with electrodes of different sizesa
ElectrodeNo. of patients
Weakness Fatigue Speech disorders Drooling Dysphagia Hypersomnia
1.1 � 2 mm 31 (3.5%) 146 (16.3%) 89 (9.9%) 44 (4.9%) 21 (2.3%) 106 (11.8%)
1.8 � 2 mm 5 (4.5%) 36 (32.1%)b 15 (13.4%) 8 (7.1%) 3 (2.6%) 11 (9.8%)
a A total of 112 patients underwent unilateral pallidotomies with 1.8- � 2-mm electrodes and 895 patients underwent unilateral pallidotomies with 1.1- � 2-mmelectrodes.b P � 0.05.
TABLE 5. Comparison of complications after unilateral pallidotomies in the double-lesion group and the single-lesion groupa
No. of patients
Weakness Fatigue Speech disorders Drooling Dysphagia Hypersomnia
Double lesions 6 (8.7%) 21 (30.4%) 13 (18.8%) 5 (7.2%) 2 (2.9%) 14 (20.3%)
Single lesion 30 (3.2%)b 161 (17.2%)b 91 (9.7%)b 47 (5.0%) 22 (2.3%) 103 (11.5%)b
a A total of 69 patients underwent unilateral pallidotomies with double lesions and 938 patients underwent unilateral pallidotomies with single lesions.b P � 0.05.
COMPLICATIONS OF RADIOFREQUENCY PALLIDOTOMY
NEUROSURGERY VOLUME 52 | NUMBER 1 | JANUARY 2003 | 95

delayed weakness developed a delayed internal capsule in-farction, as confirmed with CT scans 7 days after the opera-tion. Because CT or magnetic resonance imaging scans werenot routinely obtained after surgery, some delayed internalcapsule infarctions might not have been identified. Accordingto Lim et al. (27), more cases of delayed internal capsuleinfarctions might occur weeks or months after pallidotomy.
Complications after Bilateral Pallidotomies
Certain complications occur more frequently with bilateralpallidotomies than with unilateral pallidotomies (7, 20). Ourstudy demonstrated that patients who underwent bilateralpallidotomies were at higher risk of drooling and dysphagiaand were more symptomatic than those who underwent uni-lateral pallidotomies. Speech disorders tended to occur afterbilateral pallidotomies. Giller et al. (11) reported that 8 of 55patients experienced speech or oral function disturbances and7 of those patients had undergone bilateral procedures. There-fore, whether patients should undergo bilateral pallidotomiesshould be carefully and fully assessed. With staged bilateralpallidotomies, the increased risks of complications can bereduced to acceptable levels for carefully selected candidates.Patients more than 60 years of age, those in poor health, andthose with mild speech disorders should undergo completeassessments before decision-making. Bilateral pallidotomy isnot recommended for patients with drooling and dysphagia,regardless of whether the conditions are severe or not. Forsuch patients, pallidal stimulation would be an attractive al-ternative (13, 34, 39). Simultaneous bilateral pallidotomy is notfavorable because of the high incidence of complications (Table6). Scott et al. (37) reported on eight patients who underwentsimultaneous bilateral pallidotomies, of whom two experi-enced confusion, one hypophonia, three dysarthria, two drool-ing, and four reduced verbal fluency. Ghika et al. (10) con-cluded that the incidence of complications is too high for theprocedure to be performed, although simultaneous bilateralpallidotomy can better improve the symptoms of PD. In ourstudy, three young patients who underwent simultaneousbilateral pallidotomies developed severe fatigue, dysarthria,dysphagia, and drooling, despite remarkably good relief of PD
symptoms. We also think that simultaneous bilateral pal-lidotomy should not be performed because of its high risks.With the advent of deep brain stimulation, it is possible toreduce the incidences of complications associated with eitherbilateral or unilateral operations (4, 39, 40). In view of theincidences of complications, deep brain stimulation might be agood alternative to ablative procedures.
Electrodes of Different Sizes and DifferentLesioning Procedures
There was no significant difference between the groupstreated with electrodes of 1.1 � 2 mm or 1.8 � 2 mm. Only theincidence of fatigue in the 1.8- � 2-mm electrode-treatedgroup was significantly higher than that in the 1.1- � 2-mmelectrode-treated group. For the group treated with a 1.8- �2-mm electrode, the initial target was set 3 mm anterior to theposterior border of the GPi, and the lesioning temperature waslower than that used with the 1.1- � 2-mm electrode.
There were significant differences in the incidences of certaincomplications between the double-lesion group and the single-lesion group. The incidences of weakness, fatigue, speech disor-ders, and hypersomnia were much higher in the double-lesiongroup than in the single-lesion group. Postoperative CT scansdemonstrated that patients in the double-lesion group had muchlarger lesions than did those in the single-lesion group. Ourstudy indicates that the final lesion should not be too large, tominimize the incidence of complications.
Symptomatic Hemorrhage after Microelectrode-guided Pallidotomies
There are two main disadvantages of microelectrode record-ing during pallidotomy (18, 22), namely prolongation of theprocedure and increased risk of hemorrhage. The precise infor-mation obtained with microelectrode recording could reducedamage to the optic tract and the internal capsule, despite thelong time required. However, the increased risk of hemorrhageshould be considered when microelectrode recording is used forpallidotomy. Shannon et al. (38), taking into consideration 3 cases
TABLE 6. Complications among patients with Parkinson’s disease who underwent simultaneous bilateral pallidotomies
Series (ref. no.)No. of
patientsComplications
(no. of patients)
Iacono et al., 1995 (19) 49 Symptomatic hemorrhage (2), infection (1)
Scott et al., 1998 (37) 8 Confusion (1), hypophonia (1), dysarthria (3), drooling (2), reduced verbalfluency (4)
Giller et al., 1998 (11) 3 Speech impairment (3)
Ghika et al., 1999 (10) 4 Bulbar syndrome (1), depression (2), abulia (1), compulsions (1), apraxia ofeyelid opening (1)
Favre et al., 2000 (7) 17 Swelling or drooling (6), speech deterioration (9)
HUA ET AL.
96 | VOLUME 52 | NUMBER 1 | JANUARY 2003 www.neurosurgery-online.com
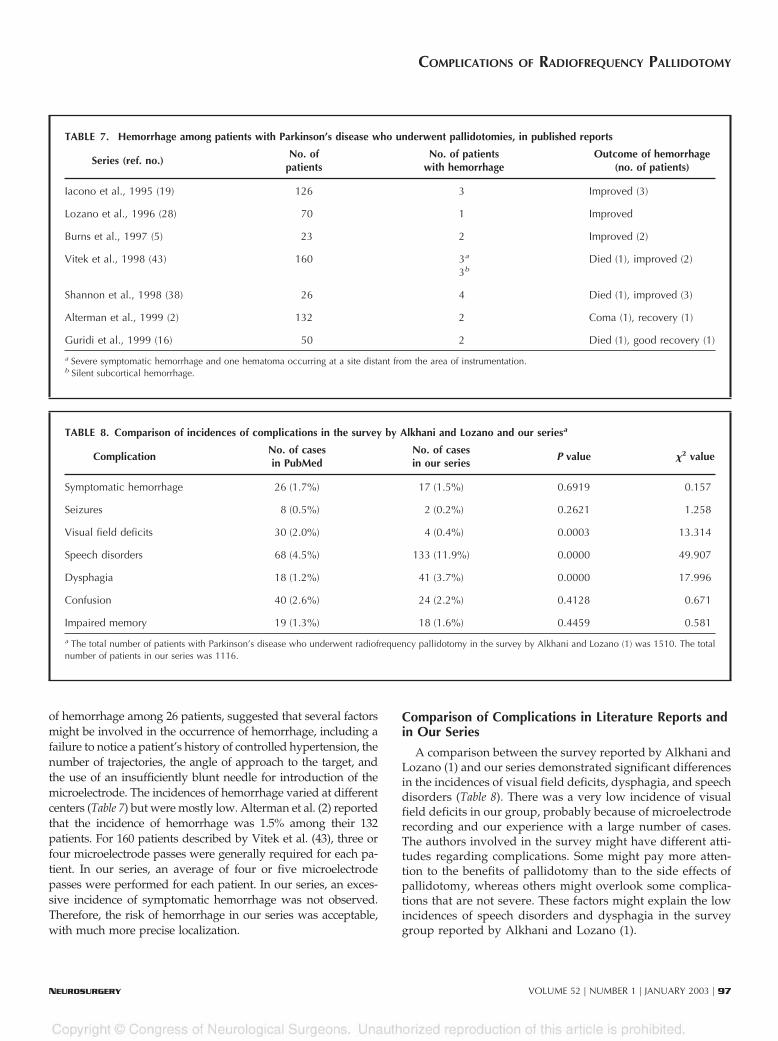
of hemorrhage among 26 patients, suggested that several factorsmight be involved in the occurrence of hemorrhage, including afailure to notice a patient’s history of controlled hypertension, thenumber of trajectories, the angle of approach to the target, andthe use of an insufficiently blunt needle for introduction of themicroelectrode. The incidences of hemorrhage varied at differentcenters (Table 7) but were mostly low. Alterman et al. (2) reportedthat the incidence of hemorrhage was 1.5% among their 132patients. For 160 patients described by Vitek et al. (43), three orfour microelectrode passes were generally required for each pa-tient. In our series, an average of four or five microelectrodepasses were performed for each patient. In our series, an exces-sive incidence of symptomatic hemorrhage was not observed.Therefore, the risk of hemorrhage in our series was acceptable,with much more precise localization.
Comparison of Complications in Literature Reports andin Our Series
A comparison between the survey reported by Alkhani andLozano (1) and our series demonstrated significant differencesin the incidences of visual field deficits, dysphagia, and speechdisorders (Table 8). There was a very low incidence of visualfield deficits in our group, probably because of microelectroderecording and our experience with a large number of cases.The authors involved in the survey might have different atti-tudes regarding complications. Some might pay more atten-tion to the benefits of pallidotomy than to the side effects ofpallidotomy, whereas others might overlook some complica-tions that are not severe. These factors might explain the lowincidences of speech disorders and dysphagia in the surveygroup reported by Alkhani and Lozano (1).
TABLE 7. Hemorrhage among patients with Parkinson’s disease who underwent pallidotomies, in published reports
Series (ref. no.)No. of
patientsNo. of patients
with hemorrhageOutcome of hemorrhage
(no. of patients)
Iacono et al., 1995 (19) 126 3 Improved (3)
Lozano et al., 1996 (28) 70 1 Improved
Burns et al., 1997 (5) 23 2 Improved (2)
Vitek et al., 1998 (43) 160 3a
3bDied (1), improved (2)
Shannon et al., 1998 (38) 26 4 Died (1), improved (3)
Alterman et al., 1999 (2) 132 2 Coma (1), recovery (1)
Guridi et al., 1999 (16) 50 2 Died (1), good recovery (1)
a Severe symptomatic hemorrhage and one hematoma occurring at a site distant from the area of instrumentation.b Silent subcortical hemorrhage.
TABLE 8. Comparison of incidences of complications in the survey by Alkhani and Lozano and our seriesa
ComplicationNo. of casesin PubMed
No. of casesin our series
P value �2 value
Symptomatic hemorrhage 26 (1.7%) 17 (1.5%) 0.6919 0.157
Seizures 8 (0.5%) 2 (0.2%) 0.2621 1.258
Visual field deficits 30 (2.0%) 4 (0.4%) 0.0003 13.314
Speech disorders 68 (4.5%) 133 (11.9%) 0.0000 49.907
Dysphagia 18 (1.2%) 41 (3.7%) 0.0000 17.996
Confusion 40 (2.6%) 24 (2.2%) 0.4128 0.671
Impaired memory 19 (1.3%) 18 (1.6%) 0.4459 0.581
a The total number of patients with Parkinson’s disease who underwent radiofrequency pallidotomy in the survey by Alkhani and Lozano (1) was 1510. The totalnumber of patients in our series was 1116.
COMPLICATIONS OF RADIOFREQUENCY PALLIDOTOMY
NEUROSURGERY VOLUME 52 | NUMBER 1 | JANUARY 2003 | 97

CONCLUSION
The incidences of fatigue, speech disorders, drooling, dys-phagia, and hypersomnia were relatively higher than ex-pected, especially in the bilateral pallidotomy group. There-fore, staged bilateral pallidotomy should be carefullyevaluated before decision-making; simultaneous bilateral pal-lidotomy is undesirable. This study indicates that patientswith poor health and those who develop mild speech disor-ders, drooling, and dysphagia after the first operation shouldnot undergo contralateral pallidotomy. Our study suggeststhat the size of the final lesion should be limited, to minimizethe risk of complications. The incidence of symptomatic hem-orrhage in this series is in accordance with literature data andis acceptable, compared with the benefits of surgery.
REFERENCES
1. Alkhani A, Lozano AM: Pallidotomy for Parkinson disease: A review ofcontemporary literature. J Neurosurg 94:43–49, 2001.
2. Alterman RL, Sterio D, Beric A, Kelly PJ: Microelectrode recording duringposteroventral pallidotomy: Impact on target selection and complications.Neurosurgery 44:315–323, 1999.
3. Baron MS, Vitek JL, Bakay RAE, Green J, Kaneoke Y, Hashimoto T, TurnerRS, Woodard JL, Cole SA, McDonald WM, DeLong MR: Treatment ofadvanced Parkinson’s disease by posterior GPi pallidotomy. Ann Neurol40:355–366, 1996.
4. Burchiel KJ: Thalamotomy for movement disorders. Neurosurg Clin N Am6:55–71, 1995.
5. Burns JM, Wilkinson S, Kieltyka J, Overman J, Lundsgaarde T, Tollefson T,Koller WC, Pahwa R, Troster AI, Lyons KE, Batnitzky S, Wetzel L, GordonMA: Analysis of pallidotomy lesion positions using three-dimensional re-construction of pallidal lesions, the basal ganglia, and the optic tract.Neurosurgery 41:1303–1318, 1997.
6. Cosman ER, Nashold BS, Ovelman-Levitt J: Theoretical aspects of radiofre-quency lesions in the dorsal root entry zone. Neurosurgery 15:945–950, 1984.
7. Favre J, Burchiel KJ, Taha JM, Hammerstad J: Outcome of unilateral andbilateral pallidotomy for Parkinson’s disease: Patient assessment. Neuro-surgery 46:344–355, 2000.
8. Fazzini E, Dogali M, Sterio D, Eidelberg D, Beric A: Stereotactic pallidotomyfor Parkinson’s disease. Neurology 48:1273–1277, 1997.
9. Foerster OH: Resection of the posterior spinal nerve roots in the treatmentof gastric crisis and spastic paralysis. Proc R Soc Lond B Biol Sci 3:226–254,1911.
10. Ghika J, Ghika-Schmid F, Fankhauser H, Assal G, Vingerhoets F, AlbaneseA, Bogousslavsky J, Favre J: Bilateral contemporaneous posteroventral pal-lidotomy for the treatment of Parkinson’s disease: Neuropsychological andneurological side effects—Report of four cases and review of the literature.J Neurosurg 91:313–321, 1999.
11. Giller CA, Dewey RB, Ginsburg MI, Mendelsohn DB, Berk AM: Stereotaticpallidotomy and thalamotomy using individual variations of anatomic land-marks for localization. Neurosurgery 42:56–65, 1998.
12. Goldstein LB, Bertels C, Davis JN: Interrater reliability of the NIH StrokeScale. Arch Neurol 46:660–662, 1989.
13. Gross C, Rougier A, Guehl D, Boraud T, Julien J, Bioulac B: High-frequencystimulation of the globus pallidus internalis in Parkinson’s disease: A studyof seven cases. J Neurosurg 87:491–498, 1997.
14. Guiot G, Brion S: Traitment des mouvements anormaux par la coagulationpallidale: Technique et resultats. Rev Neurol (Paris) 89:578–580, 1953.
15. Guiot G, Pecker J: Tractotomie mesencephalique anterieure pour tremble-ment parkinsonien. Rev Neurol (Paris) 81:387–389, 1949.
16. Guridi J, Gorospe A, Ramos E, Linazasoro G, Rodriguez MC, Obeso JA:Stereotactic targeting of the globus pallidus internus in Parkinson’s disease:Imaging versus electrophysiological mapping. Neurosurgery 45:278–289,1999.
17. Hariz MI, De Salles AA: The side-effects and complications ofposteroventral pallidotomy. Acta Neurochir Suppl (Wien) 68:42–48, 1997.
18. Hariz MI, Fodstad H: Do microelectrode techniques increase accuracy ordecrease risks in pallidotomy and deep brain stimulation? A critical reviewof the literature. Stereotact Funct Neurosurg 72:157–169, 1999.
19. Iacono RP, Shima F, Lonser RR, Kuniyoshi S, Maeda G, Yamada S: Theresults, indications, and physiology of posteroventral pallidotomy for pa-tients with Parkinson’s disease. Neurosurgery 36:1118–1127, 1995.
20. Intemann PM, Masterman D, Subramanian I, De Salles A, Behnke E,Frysinger R, Bronstein JM: Staged bilateral pallidotomy for treatment ofParkinson disease. J Neurosurg 94:437–444, 2001.
21. Kelly PJ: Pallidotomy in Parkinson’s disease. Neurosurgery 36:1154–1157,1995 (comment).
22. Kishore A, Turnbull IM, Snow BJ, de la Fuente-Fernandez R, Schulzer M,Mak E, Yardley S, Calne DB: Efficacy, stability and predictors of outcome ofpallidotomy for Parkinson’s disease: Six-month follow-up with additional1-year observations. Brain 120:729–737, 1997.
23. Kopyov O, Jacques D, Duma C, Buckwalter G, Kopyov A, Lieberman A,Copcutt B: Microelectrode-guided posteroventral medial radiofrequencypallidotomy for Parkinson’s disease. J Neurosurg 87:52–59, 1997.
24. Laitinen LV: Pallidotomy for Parkinson’s disease. Neurosurg Clin N Am6:105–112, 1995.
25. Laitinen LV, Bergenheim AT, Hariz MI: Leksell’s posteroventral pallidotomy inthe treatment of Parkinson’s disease. J Neurosurg 76:53–61, 1992.
26. Lang AE, Lozano AM, Montgomery E, Duff J, Tasker RR, Hutchinson W:Posteroventral medial pallidotomy in advanced Parkinson’s disease. N EnglJ Med 337:1036–1042, 1997.
27. Lim JY, De Salles AAF, Bronstein J, Masterman DL, Saver JL: Delayedinternal capsule infarctions following radiofrequency pallidotomy.J Neurosurg 87:955–960, 1997.
28. Lozano AM, Hutchison W, Kiss Z, Tasker R, Davis K, Dostrovsky J: Methods formicroelectrode-guided posteroventral pallidotomy. J Neurosurg 84:194–202, 1996.
29. Lozano AM, Lang AE, Galvez-Jimenez N, Miyasaki J, Duff J, HutchinsonWD, Dostrovsky JO: Effect of GPi pallidotomy on motor function inParkinson’s disease. Lancet 346:1383–1387, 1995.
30. Meyers R: The human frontocorticopontine tract: Functional inconsequenceof its surgical interruption. Neurology 1:341–356, 1951.
31. Narabayashi H, Okuma T: Procaine oil blocking of the globus pallidus fortreatment of rigidity and tremor of Parkinsonism: Preliminary report. ProcJpn Acad 29:134, 1953.
32. Oliver LC: Surgery in Parkinson’s disease: Division of the lateral pyramidaltract for tremor—Report on forty-eight operations. Lancet 1:910–913, 1949.
33. Ondo WG, Jankovic J, Lai EC, Sankhla C, Khan M, Ben-Arie L, Schwartz K,Grossman RG, Krauss JK: Assessment of motor function after stereotacticpallidotomy. Neurology 50:266–270, 1998.
34. Pahwa R, Wilkinson S, Smith D, Lyons K, Miyawaki E, Koller WC: High-frequency stimulation of the globus pallidus for the treatment of Parkinson’sdisease. Neurology 49:249–253, 1997.
35. Putnam TJ: Treatment of athetosis and dystonia by section of the extrapy-ramidal motor tracts. Arch Neurol Psychiatry 29:504–521, 1933.
36. Putnam TJ: Results of treatment of athetosis by section of extrapyramidaltracts in the spinal cord. Arch Neurol Psychiatry 39:258–275, 1938.
37. Scott R, Gregory R, Hines N, Carroll C, Hyman N, Papanasstasiou V,Leather C, Rowe J, Silburn P, Aziz T: Neuropsychological, neurological andfunctional outcome following pallidotomy for Parkinson’s disease: A con-secutive series of eight simultaneous bilateral and twelve unilateral proce-dures. Brain 121:659–675, 1998.
38. Shannon KM, Penn RD, Kroin JS, Adler CH, Janko KA, York M, Cox SJ:Stereotactic pallidotomy for the treatment of Parkinson’s disease. Neurol-ogy 50:434–438, 1998.
39. Siegfried J, Lippitz B: Bilateral chronic electrostimulation ofventroposterolateral pallidum: A new therapeutic approach for alleviatingall parkinsonian symptoms. Neurosurgery 35:1126–1130, 1994.
40. Starr PA, Vitek JL, Bakay RAE: Ablative surgery and deep brain stimulationfor Parkinson’s disease. Neurosurgery 43:989–1015, 1998.
41. Svennilison E, Torvik A, Lowe R, Leksell L: Treatment of parkinsonism bystereotactic thermolesion in pallidal region. Acta Psychiatr Scand 35:358–377, 1960.
HUA ET AL.
98 | VOLUME 52 | NUMBER 1 | JANUARY 2003 www.neurosurgery-online.com

42. Deleted in proof.43. Vitek JL, Bakay RAE, Hashimoto T, Kaneoke Y, Mewes K, Zhang JY, Rye D,
Starr P, Baron M, Turner R, DeLong MR: Microelectrode-guided pal-lidotomy: Technical approach and its application in medically intractableParkinson’s disease. J Neurosurg 88:1027–1043, 1998.
44. Walker A-E: Cerebral pedunculotomy for the relief of involuntary move-ments: Part 2–Parkinsonian tremor. J Nerv Ment Dis 116:766–775, 1952.
45. Zervas NT, Kuwayama A: Pathological characteristics of experimental ther-mal lesions: Comparison of induction heating and radiofrequency electro-coagulation. J Neurosurg 37:418–422, 1972.
AcknowledgmentsWe thank Prof. Wan Yehan of the Anhuei Provincial Hospital for initially
encouraging us to investigate the side effects of pallidotomy. We also thankWang Qiong for assistance with the preparation of this manuscript and ShangLei for statistical analyses. We do not have any personal or institutional interestin any drugs, materials, or devices described here, and we did not receive anyfinancial support in conjunction with the generation of this submission.
COMMENTS
In this study, Hua et al. have examined the complications ofpallidotomy in the largest single-center series yet reported. The
authors exhaustively list many possible adverse side effects ofsurgery that are seldom described in detail in the literature butare familiar to surgeons who evaluate their patients carefully inthe postoperative period. The authors’ patients’ reported inci-dences of fatigue, speech disorders, drooling, and hypersomniaseem relatively high; however, this is most likely due to morecareful observation than to a true increase in incidence. Theirtheory regarding “damage of nutrient vessels for the internalcapsule” being responsible for these complications is interestingbut unsubstantiated. It is entirely possible that many of these sideeffects are unavoidable complications of lesioning, regardless oftargeting accuracy. As the authors acknowledge, the use of deepbrain stimulation (DBS) can avoid many of the risks of lesioning.This technology is rapidly replacing lesioning as the treatment ofchoice because of its safety, reversibility, and adjustability.
The authors contend that microelectrode recording in-creases the risk of hemorrhage. Although individual reportsvary widely, Alkhani and Lozano’s (1) review of the literatureprovides a valuable comparison and is cited by the authors. Inthis review, pallidotomies performed with microrecordingcarried a 2.7% hemorrhage risk in contrast to 0.5% in pal-lidotomies performed with macrostimulation alone. Thepresent study’s 1.5% risk is thus well below the aggregate riskof hemorrhage in microelectrode-guided pallidotomy. It hasbeen suggested that experience with the operation, rather thanthe specific technique used, dictates the complication rate. Thelarge experience of Hua et al., coupled with their relativelylow rate of hemorrhage, lends support to this concept.
Despite the extremely low (0.2%) incidence of seizures in thisseries, the authors recommend prophylactic postoperative anti-convulsant therapy. The risks of even short-term anticonvulsanttherapy, including the inevitable falls as a result of ataxia in anelderly population prone to postural instability, seem to out-weigh any minor benefit conferred to this small number ofpatients.
Of particular interest is the number of delayed hemorrhages(6 of the total of 14 symptomatic hemorrhages) as well as thedelayed weakness from edema (34 cases) reported in thisstudy. These symptoms appeared 3 to 10 days after surgerywas performed. Delayed complications may be more preva-lent than previously suspected, suggesting that increased vig-ilance, including longer hospital stays, may be warranted.
The authors contribute important insights by making care-ful observations and describing their very large experience.This information will be useful to neurosurgeons who stillperform lesioning procedures in patients with movement dis-orders. It also provides a valuable benchmark against whichfuture studies of DBS can be judged.
Jaimie M. HendersonAli R. RezaiCleveland, Ohio
1. Alkhani A, Lozano AM: Pallidotomy for Parkinson disease: A review ofcontemporary literature. J Neurosurg 94:43–49, 2001.
This article presents complications of microelectrode-guided radiofrequency pallidotomy in a very large single-
center series. The incidence of complications in any series isrelated to the methods used to detect complications. The in-cidence of visual field cut, for instance, is extremely low in thisseries (4 patients, or 0.4%). It is not completely clear whetherscoring of this complication depended on patients’ reporting itor on formal visual field examinations. Patients may be un-aware of a visual field cut, especially in the early postoperativeperiod. Conducting neurological examinations with visualfield testing by confrontation increases the detection rate. Per-forming formal Goldman perimetry examinations increasesthe detection rate even more (1).
One of the most useful aspects of this article is the compar-ison of complications of unilateral versus bilateral pal-lidotomy. As the results in smaller series have also indicated,bilateral pallidotomy has a much higher incidence of compli-cations, especially those related to corticobulbar tract function.
The authors recommend limiting the size of lesions, given theirfinding that lesions created with multiple lesioning trajectoriesresulted in a higher incidence of complications than lesions madewith single tracts. This recommendation should be interpretedcautiously. No outcome data are reported in this article. Al-though it is logical that smaller lesions may be associated withfewer complications, it is also possible for small lesions that leavea significant portion of the motor territory intact to be associatedwith reduced therapeutic benefit.
Philip A. StarrSan Francisco, California
1. Biousse V, Newman NJ, Carroll C, Mewes K, Vitek JL, Bakay RA, Baron MS,DeLong MR: Visual fields in patients with posterior GPi pallidotomy. Neu-rology 50:258–265, 1998.
COMPLICATIONS OF RADIOFREQUENCY PALLIDOTOMY
NEUROSURGERY VOLUME 52 | NUMBER 1 | JANUARY 2003 | 99

Hua et al. present their enormous single-institution expe-rience (n � 1116 patients) with the use of posteroventral
pallidotomy (PVP) for the treatment of patients with Parkin-son’s disease, and they offer a critique of the complications ofunilateral, staged bilateral, and bilateral procedures. Targetingwas based on computed tomographic imaging andmicroelectrode-recording confirmation. The authors’ reportedcomplication rate was comparable to that published in a recentsurvey of numerous institutions, although Hua et al. encoun-tered a much higher rate of speech difficulties (11.9 versus4.5%) and dysphagia (3.7 versus 1.2%). Perhaps they haveassessed their results more completely than previous investi-gators. It is not surprising that doubling the number of lesionsat each site was associated with a higher complication rate(Table 5) or that a small number of simultaneous bilateralprocedures produced speech difficulties and pseudobulbarpalsies. This trend is nicely demonstrated in Table 3, wherestaged bilateral pallidotomy is appropriately scrutinized. Thecomplications of bilateral thalamotomies are more thoroughlydocumented in the literature, and this study reflects similarconsequences with bilateral pallidal lesioning.
Kim J. BurchielPortland, Oregon
Hua et al. report the largest series published to date ofpatients who underwent stereotactic PVP, and they pro-
vide a careful and honest report of the complications in thisgroup of patients. The series is large enough that risk percent-ages for the various complications can be assigned, which isimportant information for preoperative patient counseling.Not surprising is that more side effects are noted with thecreation of larger lesions. They also caution against simulta-neous bilateral pallidotomy but also point out that stagedbilateral pallidotomy essentially doubles the risk of postoper-ative side effects (fatigue, speech disorders, drooling, dyspha-gia, and hypersomnia).
Pallidotomy was a good operation to perform for the treat-ment of unilateral symptoms—primarily rigidity and drug-induced dyskinesia. Most neurosurgeons shied away frombilateral procedures. Happily, the advent of DBS proceduresprovided a lower-risk option for dealing with symptoms thatappear contralateral to the treated side. DBS procedures areexpensive and more time-consuming, however, and not allcountries may be able to afford the costly instrumentation. Ithink that pallidotomy should not be forgotten as a means ofproviding to desperate patients relief that may palliate theirsymptoms for a few years before progression of the diseasecatches up with them.
Patrick J. KellyNew York, New York
This article describes the complications experienced by 1116patients at a single medical center in China after the use of
microelectrode-guided PVP. In the authors’ extraordinary ex-perience, their patients’ complication rate is remarkably low.This group of neurosurgeons with an exceptionally large ex-
perience is clearly a highly talented group. Their 4-year expe-rience comprised 1222 operations in 106 patients who hadstaged bilateral pallidotomy and in 3 who underwent simul-taneous bilateral pallidotomy.
As with all retrospective studies, there is difficulty in vali-dating the database regarding the accuracy of the data gath-ering and the quality of the ascertainment of complications.The statistical analysis leaves much to be desired because ofthe lack of randomization, the small number of bilateral si-multaneous PVP procedures performed, and some inappro-priate comparisons. These authors have obviously gone wellbeyond the learning curve, and their data are of considerableinterest. Their attempt to define the complications by impre-cise localization of the target and complications related to theprocedure itself is a useful exercise.
One area of controversy that this article touches on is the useof microelectrodes and intracranial hemorrhage. Clearly withan intracranial hemorrhage rate of 1.5% in 1116 patients, therisk of hemorrhage in expert hands is very low. A high per-centage of these hemorrhages tended to result in persistentcomplications, as others have reported (3). The visual fielddefect rate was an extraordinary 0.4%. Another point of con-troversy is the unilateral versus bilateral pallidotomy. In com-paring unilateral with bilateral pallidotomy, clearly there is adoubling or more of the described complications. Althoughthese patients were not randomized, the inferences are quiteclear. The size of the lesion created in single- and double-lesion procedures also seemed to make a difference after theunilateral pallidotomy by increasing complications across theboard. For data analysis with multiple comparisons, however,P � 0.05 may not be appropriate. Missing from all of theseevaluations is reporting of the clinical outcome to help deter-mine the risk-to-benefit ratio. Does the creation of large lesionresult in better outcome, and is it therefore worth a somewhathigher complication rate? Compared with the compilation ofcomplications reported by Alkhani and Lozano (1), Hua etal.’s patients apparently had significantly fewer visual fieldsdeficits, speech disorders, and dysphasia but showed no sta-tistically significant difference in the symptomatic hemor-rhage rate. Again, these data are not truly comparable. TheAlkhani and Lozano article is a conglomeration of small, non-homogeneous articles that predominately represent the learn-ing curve of many groups (3). It is unfortunate that no cogni-tive or neuropsychological tests were performed.
Although this study does not establish the utility and safetyof microelectrode recording or the role of bilateral PVP, theresults are certainly most interesting. The authors do notadvocate performing simultaneous bilateral PVP, owing to itshigher complication risks, but they studied only three pa-tients. The difference in the size of the two patient groups andthe lack of randomization make this assertion an opinion.Their cautions concerning the evaluation of a patient beforeperforming PVP in the second side are worth considering.They recognize that minimizing the size of the lesion is im-portant, which all neurosurgeons think is essential. The largerthe lesion is, the greater the likelihood that there will be
HUA ET AL.
100 | VOLUME 52 | NUMBER 1 | JANUARY 2003 www.neurosurgery-online.com

collateral damage; but if too small a lesion is created, effectiveor prolonged improvement may not be produced. Certainly, ifone is going to perform bilateral staged or simultaneous bilat-eral PVP, smaller lesions are recommended. I agree with theauthors’ opinion that the incidence of symptomatic hemor-rhage in microelectrode-guided pallidotomy is low and thatits use is efficacious in defining the target and avoiding com-plications. This is opinion, because there are no scientific datathat suggest that this is conclusive. Unfortunately, there willprobably never be a randomized trial conducted by an expertgroup comparing microelectrode-guided pallidotomy withPVP with and without microelectrode recording. The adjust-ability of DBS, which helps to avoid complications of speech,swallowing, and so forth, yields itself so well to contemporary
practice in the United States that very few PVP procedureswill be performed in the future (2).
Roy A.E. BakayChicago, Illinois
1. Alkhani A, Lozano AM: Pallidotomy for Parkinson disease: A review ofcontemporary literature. J Neurosurg 94:43–49, 2001.
2. The Deep-Brain Stimulation for Parkinson’s Disease Study Group: Deep-brain stimulation of the subthalamic nucleus or the pars interna of the globuspallidus in Parkinson’s disease. N Engl J Med 345:956–963, 2001.
3. Sierens DK, Bakay RAE: Pallidotomy for Parkinson’s disease, in Tarsy D,Vitek JL, Lozano AM (eds): Surgical Treatment for Parkinson’s Disease and OtherMovement Disorders. Totowa, Humana Press, 2003, pp 115–128.
Julian T. Hoff, M.D., joined the faculty at theUniversity of Michigan in 1981 as Head
of the Section of Neurosurgery.Since that time, he has estab-lished a strong clinical, teach-ing, and research unit, whichbecame a separate departmentof the medical school in July2001. He presently is RichardC. Schneider Professor in theDepartment of Neurosurgeryand has served as the Neuro-surgery Residency ProgramDirector since 1981. The Neu-rosurgery Department nowhas a nationally recognizedresearch laboratory with 6 extramurallyfunded investigators, 10 clinical faculty,
and 12 residents in a 6-year training pro-gram.
Dr. Hoff is currently chair ofthe Neurosurgery Researchand Education Foundation ofthe AANS. He has been presi-dent of three national neuro-surgery societies, chair of theAmerican Board of Neurologi-cal Surgeons, and a member ofthe Residency Review Com-mittee for Neurosurgery. Dr.Hoff was elected to the Insti-tute of Medicine, NationalAcademy of Sciences, in 1999.He was awarded the Cushing
Medal of the AANS and the Grass Prize of theSociety of Neurological Surgeons in 2001.
JULIAN T. HOFF
HONORED GUEST
53rd Annual Meeting of theCongress of Neurological Surgeons
Denver, ColoradoOctober 18–23, 2003
COMPLICATIONS OF RADIOFREQUENCY PALLIDOTOMY
NEUROSURGERY VOLUME 52 | NUMBER 1 | JANUARY 2003 | 101