Embed Size (px)
DESCRIPTION
Combined HCC-CC with stem cell component.,
Citation preview
Am J Clin Pathol 2013;140:329-340 329329 DOI: 10.1309/AJCP66AVBANVNTQJ 329
© American Society for Clinical Pathology
AJCP / Original Article
Clinicopathologic Significance of Combined Hepatocellular-Cholangiocarcinoma With Stem Cell Subtype Components With Reference to the Expression of Putative Stem Cell Markers
Hiroko Ikeda, MD,1 Kenichi Harada, MD,2 Yasunori Sato, MD,2 Motoko Sasaki, MD,2 Norihide Yoneda, MD,3 Seiko Kitamura, MD,1 Yoshiko Sudo, MD,4 Akishi Ooi, MD,5 and Yasuni Nakanuma, MD1,2
From the 1Section of Diagnostic Pathology, Kanazawa University Hospital, Kanazawa, Japan; 2Department of Human Pathology, Kanazawa University Graduate School of Medicine, Kanazawa, Japan; 3Department of Radiology, Kanazawa University Hospital, Kanazawa, Japan; 4Department of Pathology, Fukui Saiseikai Hospital, Fukui, Japan; and 5Department of Molecular Cellular Pathology, Kanazawa University Graduate School of Medicine, Kanazawa, Japan.
Key Words: Combined hepatocellular-cholangiocarcinoma; DLK1; Hepatoblast; NCAM/CD56; Stem cells
DOI: 10.1309/AJCP66AVBANVNTQJ
ABSTRACT
Objectives: To examine the clinicopathologic features of combined hepatocellular-cholangiocarcinoma (HC-CC), which the World Health Organization (WHO) proposed classifying into 2 types, and the expression of delta-like 1 homolog (DLK1), as well as putative stem cell markers, such as NCAM/CD56 and CD133.
Methods: In this study we examined the expression of stem cell markers using immunohistochemistry.
Results: Thirty-six cases of combined HC-CC were subclassified into 24 cases, with more than 5% stem cell features (group B) and 12 cases with less than 5% stem cell areas (group A). The postoperative overall survival rate was worse for group B than for group A. DLK1 was frequently expressed in group B cases compared with group A, hepatocellular carcinoma, and intrahepatic cholangiocarcinoma cases.
Conclusions: The 2010 WHO classification seems important for elucidating the pathogenesis of stem cell–related liver cancers.
Combined hepatocellular-cholangiocarcinoma (HC-CC) of the liver is a primary liver tumor containing hepatocellular carcinoma (HCC) and cholangiocarcinoma (CC) elements that are intimately admixed. In the 2010 World Health Orga-nization (WHO) classification, combined HC-CC is divided into 2 histologic forms: the classic type and subtypes with stem cell features.1 The former is the traditional, commonly used definition of combined HC-CC, in which areas of typi-cal HCC and CC are mixed within the tumor. The category including subtypes with stem cell features is new and further subdivided into typical, intermediate-cell, and cholangiocel-lular subtypes.
Several markers and approaches have been used to detect and characterize hepatic stem/progenitor cells.2-5 For exam-ple, the simultaneous immunohistochemical expression of an HCC marker (HepPar1 or a-fetoprotein [AFP]) and a biliary marker (cytokeratin [CK] 19 or carcinoembryonic antigen) has been recommended for the identification of hepatic stem/progenitor cells in nonneoplastic and neoplastic livers, and the expression of nuclear cell adhesion molecule (NCAM/CD56) and epithelial cell adhesion molecule (EpCAM) has been reported in small and oval-shaped stem cell–like cells.1-5
Delta-like 1 homolog (DLK1) has been reported to be a biomarker of hepatic stem/progenitor cells in murine liver, because DLK1 is expressed in fetal liver, but it is restricted to a subpopulation of oval/hepatic progenitor cells in adult liver. Moreover, purified DLK1-positive cells can differentiate into both hepatocyte and biliary epithelial lineages and repopulate the normal liver in vivo after transplantation.6-8 The expres-sion of DLK1 has been reported in human fetal liver but not in normal adult liver or diseased livers with viral hepatitis and cir-rhosis.9,10 However, upregulation of DLK1 expression recently
Ikeda_2012100561.indd 329 8/1/13 11:14 AM

330 Am J Clin Pathol 2013;140:329-340330 DOI: 10.1309/AJCP66AVBANVNTQJ
© American Society for Clinical Pathology
Ikeda et al / Liver Cancer With Stem Cell Features and DLK1
has been reported in hepatoblastomas and some HCCs.10-14 Xu et al14 suggested that DLK1-positive HCC cells might have similar characteristics to cancer stem/progenitor cells, because DLK1-positive HCC cells showed increased chemoresistance, colony formation, spheroid formation, and in vivo tumorige-nicity compared with DLK1-negative cells. To our knowledge, the expression of DLK1 has not been investigated in combined HC-CC, and the significance of DLK1 upregulation in liver cancers needs to be elucidated.
While subtypes with stem cell features in addition to classic combined HC-CC have been proposed for evaluat-ing combined HC-CC in the 2010 WHO classification, their clinicopathologic characteristics, pathogenesis, and prognosis remain unclear. Furthermore, the expression of so-called hepatic stem/progenitor cell markers in combined HC-CC has not been reported with respect to the 2010 WHO classification.
In this study, we evaluated the clinicopathologic char-acteristics of combined HC-CC with or without stem cell features using a series of primary liver cancer specimens and attempted to clarify the expression of putative hepatic stem cell markers, especially DLK1.
Materials and Methods
Selection of Cases and Tissue Preparation
We reevaluated primary liver cancers (4,379 cases) regis-tered in the pathology files of Kanazawa University Hospital and affiliated hospitals (2001-2011). A total of 36 cases were diagnosed as combined HC-CC. As a control, 101 cases of HCC and 23 cases of intrahepatic cholangiocarcinoma (ICC) were chosen from the pathology files. Six human fetal livers at the gestational ages of 7 to 10 weeks were also collected from the files. All HCCs, ICCs, and combined HC-CCs were surgically resected cases, and fetal livers were collected from aborted fetuses. The nonneoplastic parts of these primary liver cancers were available, and 10 cases of liver cirrhosis (5 hepatitis C virus–related cases and 5 hepatitis B virus–related cases) and 5 specimens of normal liver from these cases were used as nonneoplastic adult liver for immunohistochemistry. The liver specimens were fixed in formalin and embedded in paraffin, and more than 20 thin sections (4 mm thick) were prepared from each paraffin block. Several sections were subjected to H&E staining, Azan-Mallory staining, and Gomori reticulin staining for routine histologic observation. The remaining sections were used for immunohistochemical staining. This research project was approved by the Kanazawa University Ethics Committee.
We diagnosed HCC, ICC, and combined HC-CC according to the 2010 WHO classification of gastrointes-tinal tumors.1 The HCC components of combined HC-CC consist of tumor cells that resemble hepatocytes and are
immunohistochemically positive for HepPar1. The CC com-ponents are tubular or papillary or cord-like adenocarcinomas that are positive for CK7 and CK19. Combined HC-CC was classified into 2 types in this study: group A and group B. Group A is the classic form in the 2010 WHO classification and is composed of typical HCC and CC components, with less than 5% of the area occupied by subtypes with stem cell features, and group B is combined HC-CC with more than 5% stem cell–like areas. The components of combined HC-CC with stem cell features are divided into 3 forms: typi-cal, intermediate, and cholangiocellular. The typical subtype shows stem cell–like cells around the HCC nests facing the fibrous septa, and these stem cell–like cells are small with a high nucleus to cytoplasm ratio and occasionally positive for CK19. The intermediate-cell subtype contains carcinoma cells with features intermediate between those of hepatocytes and cholangiocytes, which show cytoplasmic immunostaining of HepPar1 and CK19 simultaneously. The cholangiocellular subtype has neoplastic components resembling reactive bile ductules or the canals of Hering, which are arranged in a cord-like and anastomosing pattern, the so-called antler-like pattern embedded in fibrous stroma, and usually are positive for CK7 and/or CK19. Occasionally, these stem cell features were focally admixed, and we classified the predominant subtype when the tumors consisted of 2 or 3 components. In group B, there was always unequivocal HCC in addition to these subtypes, with stem cell features within the tumor. It did not matter whether there were typical CC components.
ImmunohistochemistryImmunostaining was carried out with an autostainer (HX
System BenchMark; Ventana Medical Systems, Tucson, AZ) according to the manufacturer’s instructions. Primary anti-bodies, clones, sources, and dilutions are listed in ❚Table 1❚. Appropriate positive and negative controls were included for each immunostaining.
❚Table 1❚Antibodies Used for Immunohistochemical Staining in an Autostainer
Antibody Clone Source Dilution
AFP Polyclonal DAKO (Glostrup, Denmark) 1:200CD133 AC133 Miltenyi Biotec (Auburn, CA) 1:100CK7 OV-TL 12/30 DAKO 1:75CK19 RCK108 DAKO 1:75DLK1 Polyclonal Abcam (Tokyo, Japan) 1:500EpCAM HEA125 DAKO 1:100Glypican 3 GC33 Chugai Pharmaceutical 1:500 (Tokyo, Japan)HepPar1 OCH1E5 DAKO 1:50NCAM/CD56 1B6 Novocastra (Newcastle 1:75 upon Tyne, England)
AFP, a-fetoprotein; CK, cytokeratin; DLK1, delta-like 1 homolog; EpCAM, epithelial cell adhesion molecule; NCAM, neural cell adhesion molecule.
Ikeda_2012100561.indd 330 8/1/13 11:14 AM
Am J Clin Pathol 2013;140:329-340 331331 DOI: 10.1309/AJCP66AVBANVNTQJ 331
© American Society for Clinical Pathology
AJCP / Original Article
Double immunostaining for HepPar1/CK19 (rabbit poly-clonal; Abcam, Tokyo, Japan) was carried out according to the manual supplied. Briefly, deparaffinized sections were microwaved in citrate buffer and then incubated with each pri-mary antibody overnight. After incubation with Alexa Fluor 594 goat anti–rabbit immunoglobulin G (IgG) and Alexa Fluor 488 goat anti–mouse IgG (Life Technologies, Carlsbad, CA), nuclei were stained by 4′,6-diamino-2-phenylindole dihydrochloride and examined under a confocal laser micro-scope (LSM5 7; Carl Zeiss, Oberkochen, Germany).
ScoringThe immunostaining was semiquantitatively scored as
follows: score 0, no positive cells; score 1+, less than 5% of tumor cells positive; score 3+, more than 50% positive, and score 2+, between scores 1+ and 3+. The positive ratio was the percentage of immunohistochemical positive cells among morphologic stem cell–like cells, not in all tumor cells, in the stem cell type of combined HC-CC.
Statistical AnalysisThe statistical analysis was performed using the Mann-
Whitney test, the Spearman rank correlation coefficient by rank test, and the Kaplan-Meier method. The differences between the survival curves were tested using the log rank test. P < .05 was considered significant.
Results
Clinicopathologic Findings of HC-CC in Comparison With HCC and ICC
The 36 cases of combined HC-CC were classified into 12 cases in group A and 24 cases in group B. The latter were subclassified into 6 cases of the typical subtype, 12 cases of the
intermediate-cell subtype, and 6 cases of the cholangiocellular subtype. The main clinicopathologic features of combined HC-CC (groups A and B), HCC, and ICC are summarized in ❚Table 2❚. The mean age of patients was significantly younger for HC-CC in group B than for HCC (P = .005) and ICC (P = .017). There was no significant difference in mean age between the 3 subtypes of group B (P = .07). There was no sta-tistical difference in sex between the groups. As for the back-ground liver, the ratio of normal liver was higher for ICC than for HCC, HC-CC (group A), and HC-CC (group B), and the frequency of cirrhosis was lowest in the ICC group. There was no significant difference between the 3 subtypes of group B.
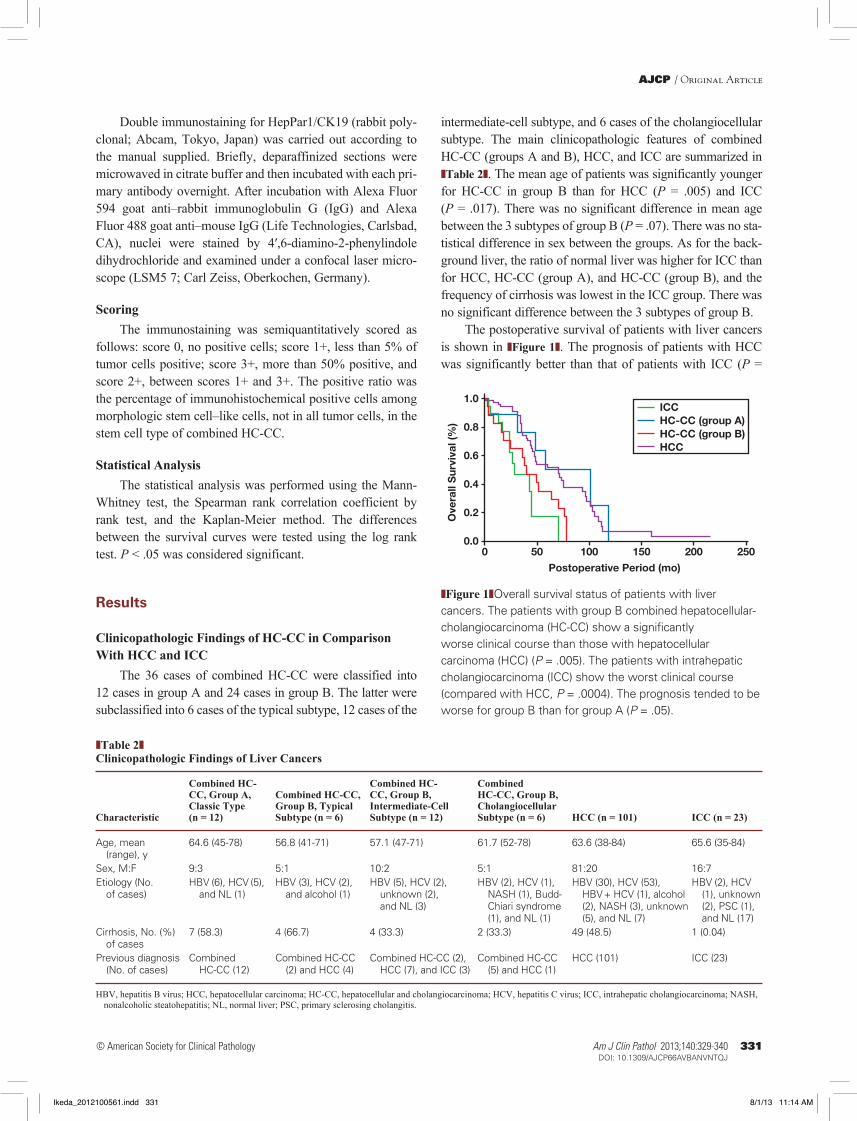
The postoperative survival of patients with liver cancers is shown in ❚Figure 1❚. The prognosis of patients with HCC was significantly better than that of patients with ICC (P =
❚Table 2❚Clinicopathologic Findings of Liver Cancers
Combined HC- Combined HC- Combined CC, Group A, Combined HC-CC, CC, Group B, HC-CC, Group B, Classic Type Group B, Typical Intermediate-Cell Cholangiocellular Characteristic (n = 12) Subtype (n = 6) Subtype (n = 12) Subtype (n = 6) HCC (n = 101) ICC (n = 23)
Age, mean 64.6 (45-78) 56.8 (41-71) 57.1 (47-71) 61.7 (52-78) 63.6 (38-84) 65.6 (35-84) (range), y Sex, M:F 9:3 5:1 10:2 5:1 81:20 16:7Etiology (No. HBV (6), HCV (5), HBV (3), HCV (2), HBV (5), HCV (2), HBV (2), HCV (1), HBV (30), HCV (53), HBV (2), HCV of cases) and NL (1) and alcohol (1) unknown (2), NASH (1), Budd- HBV + HCV (1), alcohol (1), unknown and NL (3) Chiari syndrome (2), NASH (3), unknown (2), PSC (1), (1), and NL (1) (5), and NL (7) and NL (17)Cirrhosis, No. (%) 7 (58.3) 4 (66.7) 4 (33.3) 2 (33.3) 49 (48.5) 1 (0.04) of cases Previous diagnosis Combined Combined HC-CC Combined HC-CC (2), Combined HC-CC HCC (101) ICC (23) (No. of cases) HC-CC (12) (2) and HCC (4) HCC (7), and ICC (3) (5) and HCC (1)
HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HC-CC, hepatocellular and cholangiocarcinoma; HCV, hepatitis C virus; ICC, intrahepatic cholangiocarcinoma; NASH, nonalcoholic steatohepatitis; NL, normal liver; PSC, primary sclerosing cholangitis.
0.0
0.2
0.4
ICCHC-CC (group A)HC-CC (group B)HCC
0 50 100
Postoperative Period (mo)
Ove
rall
Sur
viva
l (%
)
150 200 250
0.6
0.8
1.0
❚Figure 1❚Overall survival status of patients with liver cancers. The patients with group B combined hepatocellular-cholangiocarcinoma (HC-CC) show a significantly worse clinical course than those with hepatocellular carcinoma (HCC) (P = .005). The patients with intrahepatic cholangiocarcinoma (ICC) show the worst clinical course (compared with HCC, P = .0004). The prognosis tended to be worse for group B than for group A (P = .05).
Ikeda_2012100561.indd 331 8/1/13 11:14 AM
332 Am J Clin Pathol 2013;140:329-340332 DOI: 10.1309/AJCP66AVBANVNTQJ
© American Society for Clinical Pathology
Ikeda et al / Liver Cancer With Stem Cell Features and DLK1
.0004), whereas there were no significant differences between combined HC-CC (groups A and B) and HCC or ICC. There was no statistical difference between HCC and HC-CC in group A, but the prognosis was significantly worse for HCC in group B (P = .005). There tended to be a poor survival rate for group B compared with group A (P = .05).
Immunohistochemistry
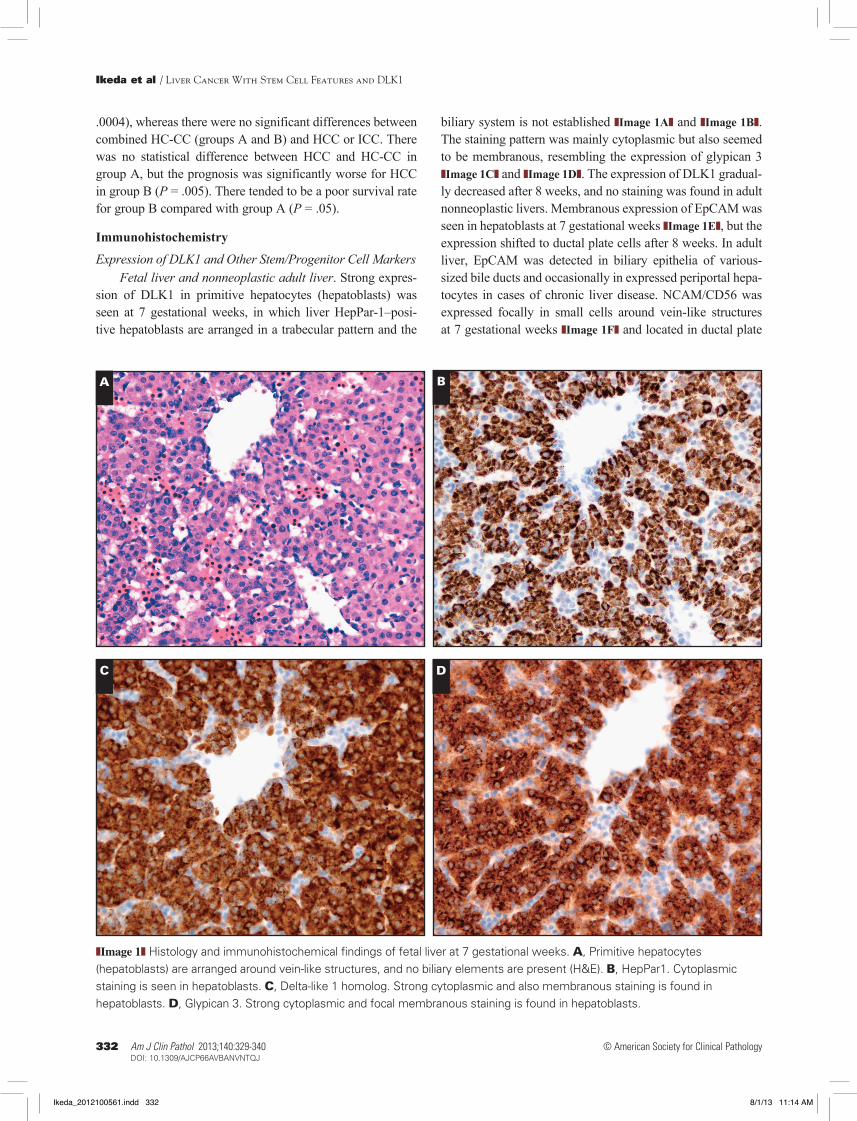
Expression of DLK1 and Other Stem/Progenitor Cell MarkersFetal liver and nonneoplastic adult liver. Strong expres-
sion of DLK1 in primitive hepatocytes (hepatoblasts) was seen at 7 gestational weeks, in which liver HepPar-1–posi-tive hepatoblasts are arranged in a trabecular pattern and the
biliary system is not established ❚Image 1A❚ and ❚Image 1B❚. The staining pattern was mainly cytoplasmic but also seemed to be membranous, resembling the expression of glypican 3 ❚Image 1C❚ and ❚Image 1D❚. The expression of DLK1 gradual-ly decreased after 8 weeks, and no staining was found in adult nonneoplastic livers. Membranous expression of EpCAM was seen in hepatoblasts at 7 gestational weeks ❚Image 1E❚, but the expression shifted to ductal plate cells after 8 weeks. In adult liver, EpCAM was detected in biliary epithelia of various-sized bile ducts and occasionally in expressed periportal hepa-tocytes in cases of chronic liver disease. NCAM/CD56 was expressed focally in small cells around vein-like structures at 7 gestational weeks ❚Image 1F❚ and located in ductal plate
A B
C D
❚Image 1❚ Histology and immunohistochemical findings of fetal liver at 7 gestational weeks. A, Primitive hepatocytes (hepatoblasts) are arranged around vein-like structures, and no biliary elements are present (H&E). B, HepPar1. Cytoplasmic staining is seen in hepatoblasts. C, Delta-like 1 homolog. Strong cytoplasmic and also membranous staining is found in hepatoblasts. D, Glypican 3. Strong cytoplasmic and focal membranous staining is found in hepatoblasts.
Ikeda_2012100561.indd 332 8/1/13 11:14 AM

Am J Clin Pathol 2013;140:329-340 333333 DOI: 10.1309/AJCP66AVBANVNTQJ 333
© American Society for Clinical Pathology
AJCP / Original Article
cells after 8 weeks. No staining of CD133 was found in fetal liver. Basolateral membranous staining of NCAM/CD56 and luminal staining of CD133 were frequently observed in reac-tive ductules in cases of liver cirrhosis.
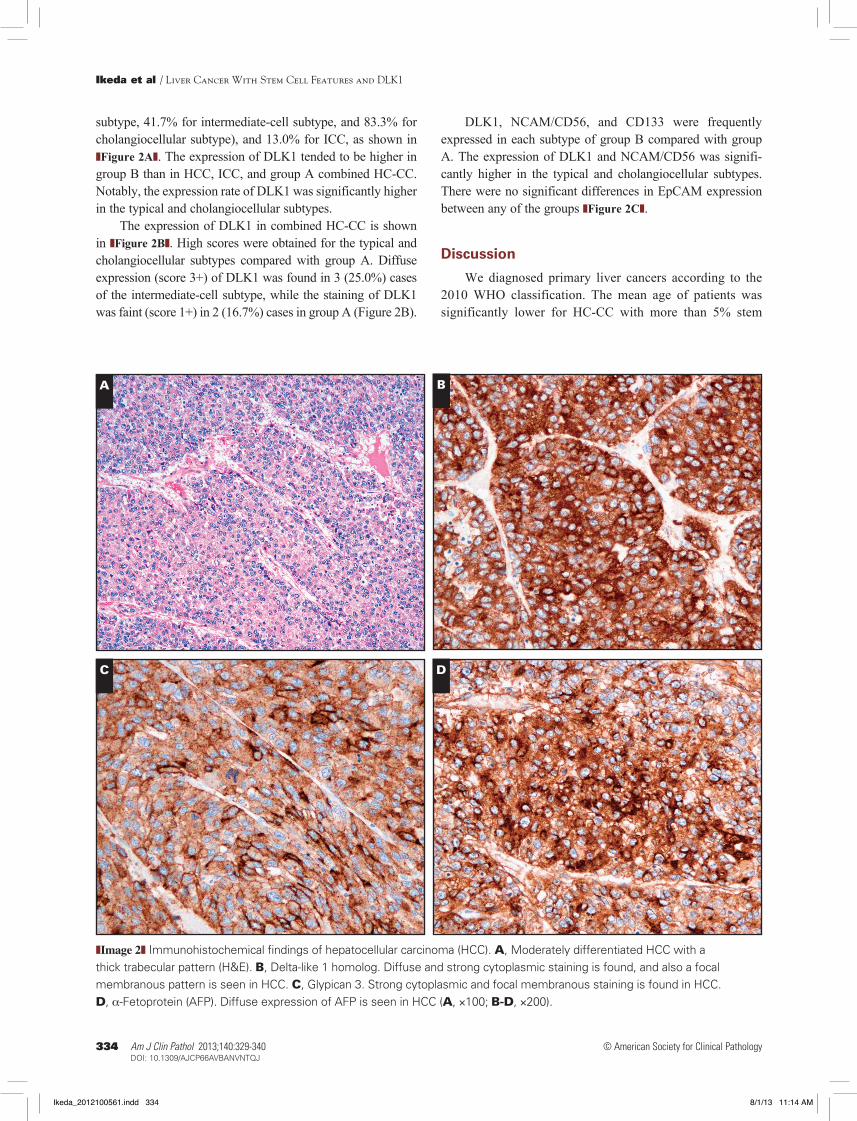
HCC and ICC. DLK1 was expressed in 11 (10.9%) of 101 cases of HCC, all of which contained moderately or poorly differentiated components. The staining of DLK1 in HCC cells was cytoplasmic but usually concomitant with membranous staining with an occasional canalicular pattern. Diffuse and strong staining of DLK1 (score 3+) was found in only 5 cases of DLK1-positive HCC. The expression of glypican 3 was detected in all cases of DLK1-positive HCC, and AFP expression was also frequently seen. The distribu-tion of DLK1-positive cells in HCC cases was similar to that of glypican 3 and AFP, and the expression of DLK1 showed a significant correlation with that of glypican 3 or AFP ❚Image 2❚. The cytoplasmic expression of DLK1 in ICC was seen in 3 cases (13.0%) with papillary components, but few DLK1-positive cells were detected (score 1+/2+). EpCAM was expressed in 21.0% of HCC cases. NCAM and CD133 were not detected in HCC. NCAM, EpCAM, and CD133 were expressed in most CC cases (96.0%).
Group A combined HC-CC. All HCC and CC compo-nents in group A were moderately or poorly differentiated HCCs or adenocarcinomas. A score of 1+ for the expression of DLK1 was seen in just 2 cases, one of which showed focal positive findings with a canalicular pattern in the HCC region and the other HC-CC showing focal cytoplasmic staining in the adenocarcinoma area.
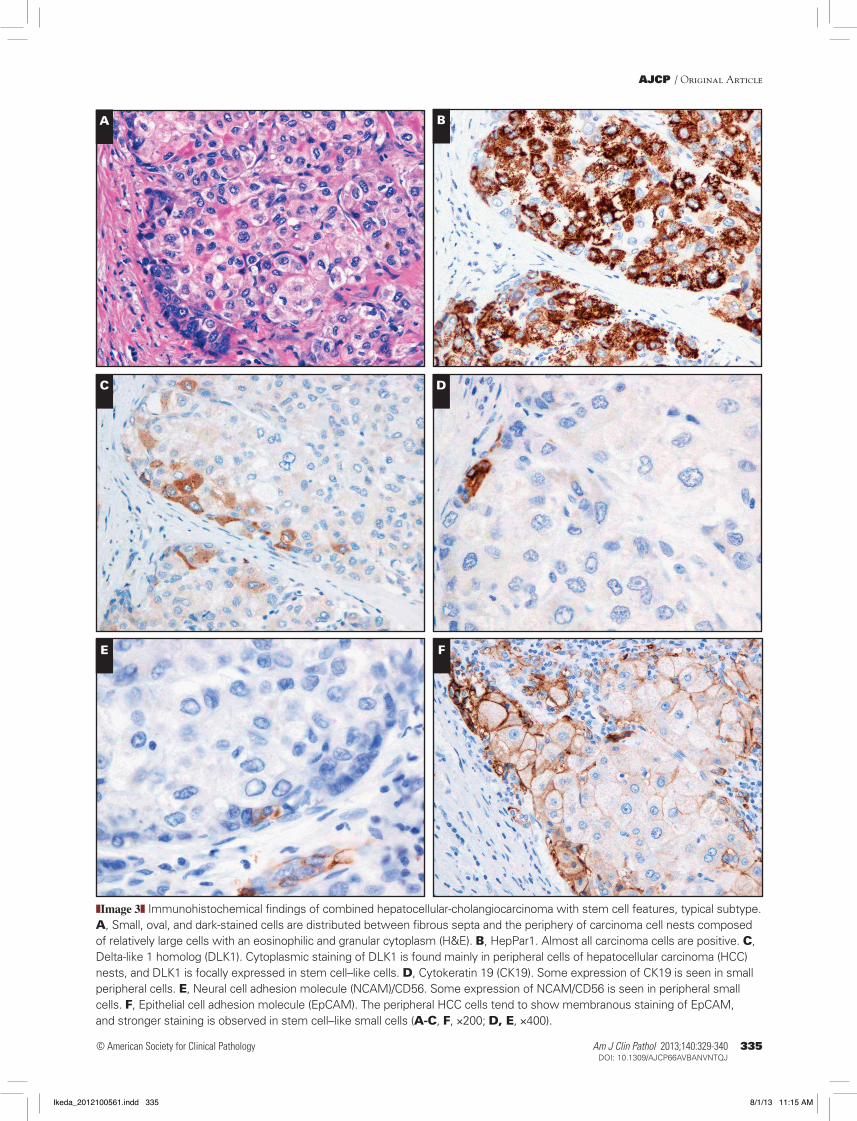
Typical subtype components of group B. Stem/progenitor cell–like small and oval cells were located at the periphery of differentiated HC nests in all 6 cases; in 1 case there were also
CC components. Cytoplasmic expression of DLK1 in stem-like cells was found in 4 (66.7%) cases and focal expression in the HCC area in 3 (50%) cases. The expression of CK19, NCAM/CD56, and EpCAM in stem-like cells was rare or focal and almost never occurred in the same cell. The frequency and location of DLK1 expression did not correlate to these stem cell–related molecules either ❚Image 3❚.
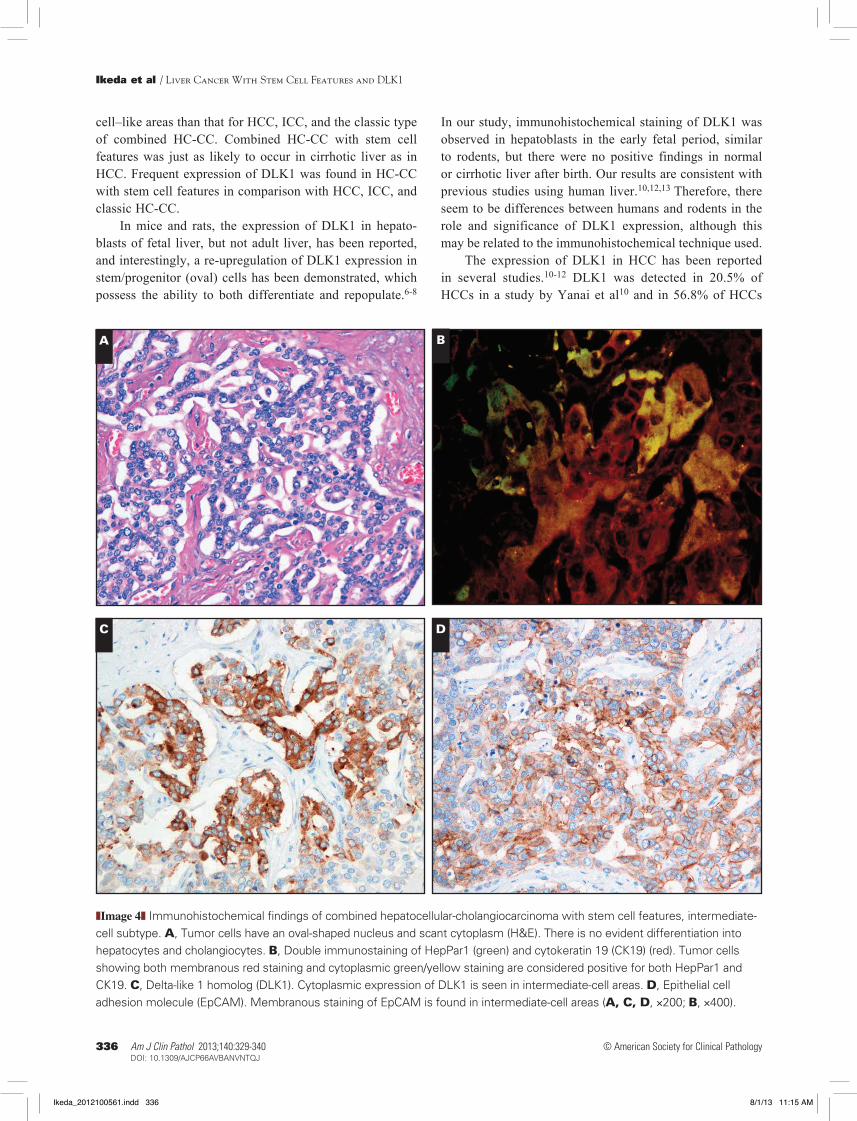
Intermediate-cell subtype component of group B. All samples contained morphologic and phenotypical intermediate tumor cells showing simultaneous expression of HepPar1 and CK19 ❚Image 4A❚ and ❚Image 4B❚. The expression of DLK1 was found in 5 (41.7%) cases, and diffuse staining (score 3+) was seen in 3 (25.0%) cases. The frequency of each marker in intermediate cells was 75.0% (9 cases) for EpCAM, 50.0% (6 cases) for NCAM/CD56, and 41.7% (5 cases) for CD133. The positive correlation of immunohistochemical scores between DLK1 and EpCAM was demonstrated by statistical analysis (P = .03) ❚Image 4C❚ and ❚Image 4D❚.
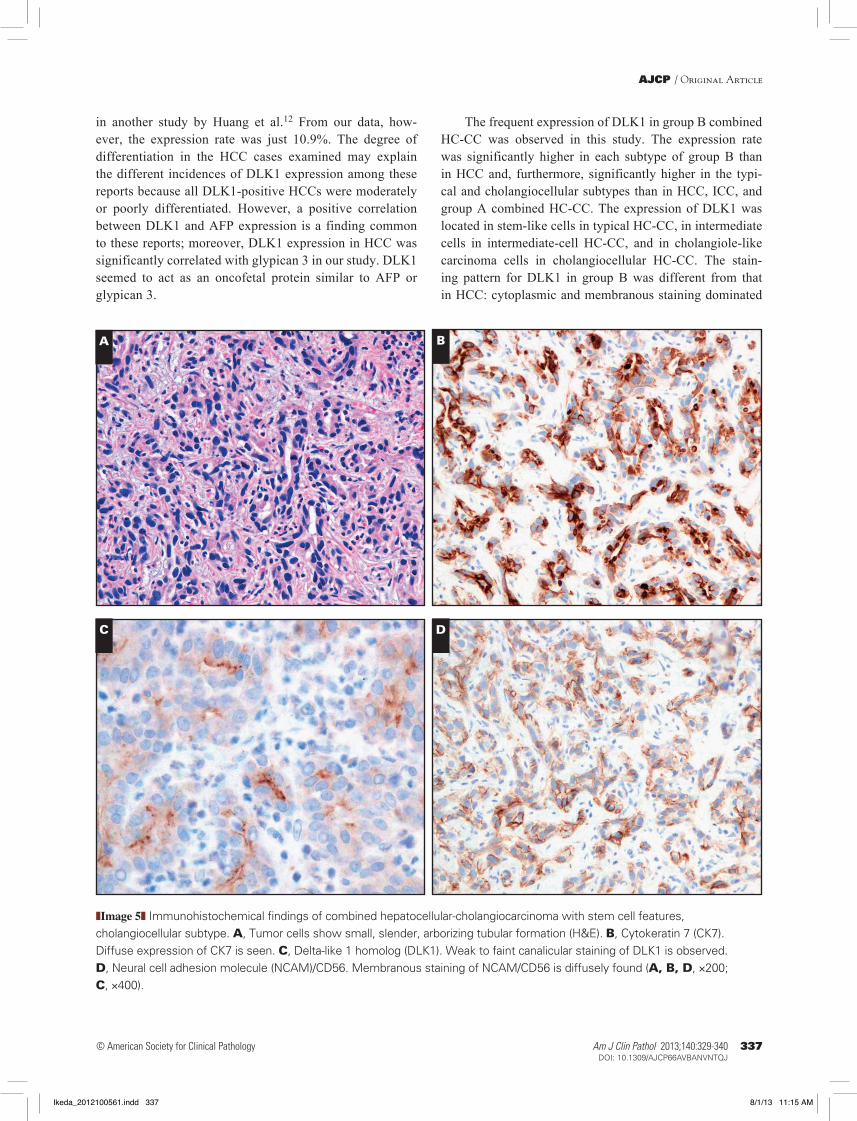
Cholangiocellular subtype of group B. The tumors showed focal cholangiocellular features, with CK7-positive small, slender, and arborizing tubules ❚Image 5A❚ and ❚Image 5B❚. NCAM/CD56 was detected in all cholangiocellular types to various degrees ❚Image 5D❚. The expression of DLK1 was seen in 5 (83.3%) cases, showing a cytoplasmic or canalicular staining pattern ❚Image 5C❚. No correlation of immunohisto-chemical scores between DLK1 and other stem cell–related markers was demonstrated by statistical analysis.
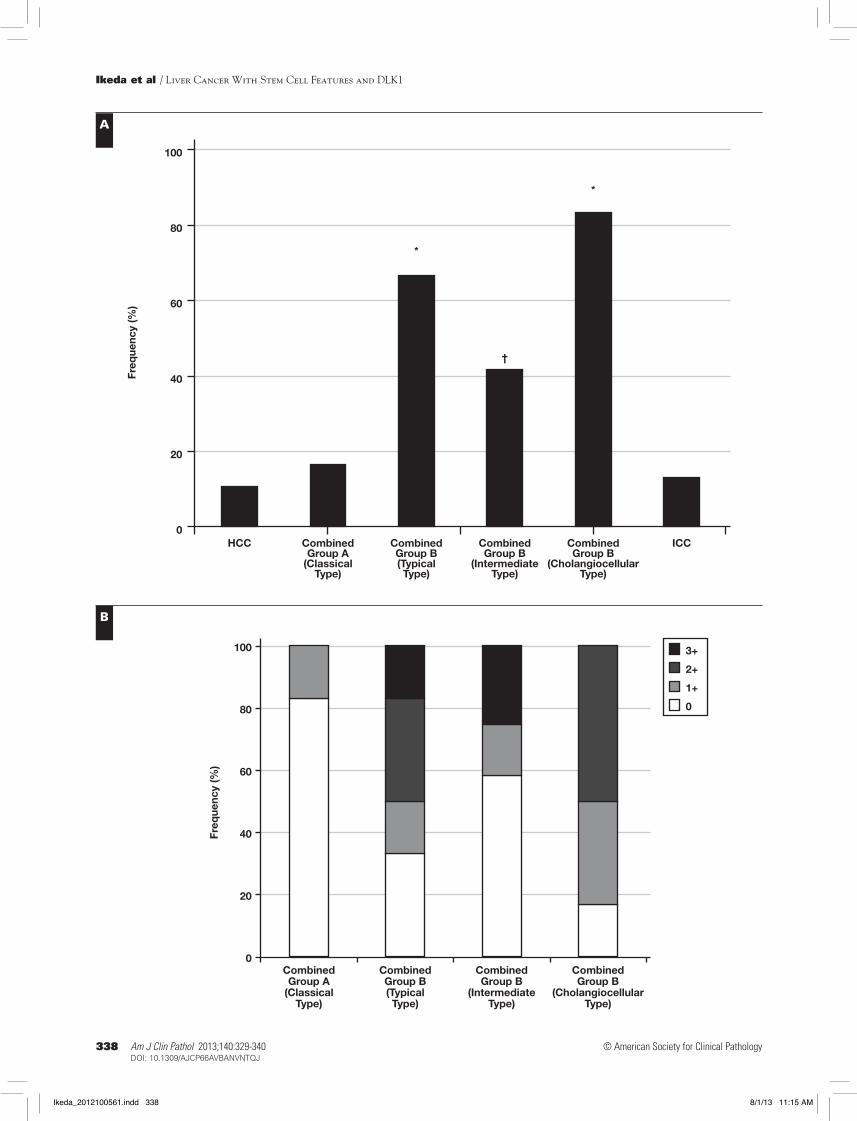
Comparison of DLK1 Expression in Liver CancersThe frequency of DLK1-positive cases (score 1+, 2+,
and 3+) was 10.9% for HCC, 16.7% for combined HC-CC in group A, 58.3% for HC-CC in group B (66.7% for typical
E F
E, Epithelial cell adhesion molecule. Membranous expression is seen in hepatoblasts. F, Neural cell adhesion molecule (NCAM)/CD56. NCAM/CD56 seems to be expressed in small cells around vein-like structures (A-F, ×200).
Ikeda_2012100561.indd 333 8/1/13 11:14 AM
334 Am J Clin Pathol 2013;140:329-340334 DOI: 10.1309/AJCP66AVBANVNTQJ
© American Society for Clinical Pathology
Ikeda et al / Liver Cancer With Stem Cell Features and DLK1
subtype, 41.7% for intermediate-cell subtype, and 83.3% for cholangiocellular subtype), and 13.0% for ICC, as shown in ❚Figure 2A❚. The expression of DLK1 tended to be higher in group B than in HCC, ICC, and group A combined HC-CC. Notably, the expression rate of DLK1 was significantly higher in the typical and cholangiocellular subtypes.
The expression of DLK1 in combined HC-CC is shown in ❚Figure 2B❚. High scores were obtained for the typical and cholangiocellular subtypes compared with group A. Diffuse expression (score 3+) of DLK1 was found in 3 (25.0%) cases of the intermediate-cell subtype, while the staining of DLK1 was faint (score 1+) in 2 (16.7%) cases in group A (Figure 2B).
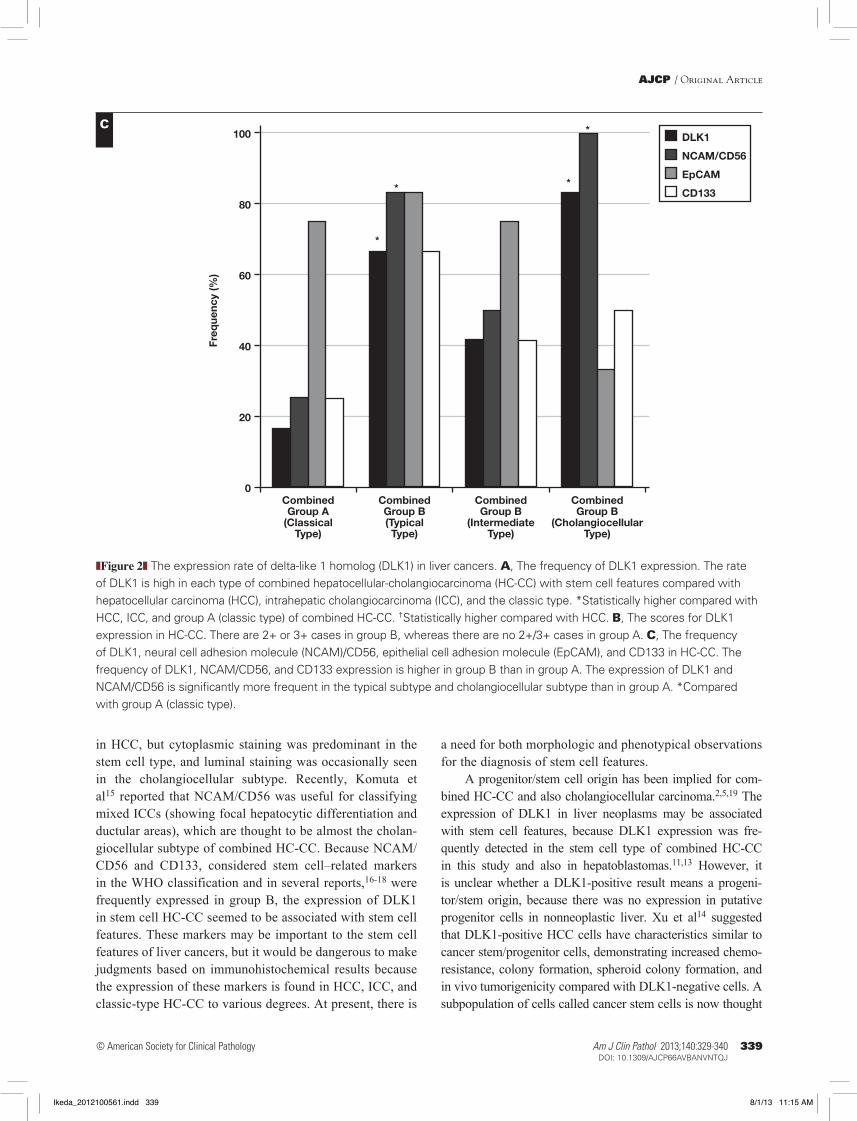
DLK1, NCAM/CD56, and CD133 were frequently expressed in each subtype of group B compared with group A. The expression of DLK1 and NCAM/CD56 was signifi-cantly higher in the typical and cholangiocellular subtypes. There were no significant differences in EpCAM expression between any of the groups ❚Figure 2C❚.
Discussion
We diagnosed primary liver cancers according to the 2010 WHO classification. The mean age of patients was significantly lower for HC-CC with more than 5% stem
A B
C D
❚Image 2❚ Immunohistochemical findings of hepatocellular carcinoma (HCC). A, Moderately differentiated HCC with a thick trabecular pattern (H&E). B, Delta-like 1 homolog. Diffuse and strong cytoplasmic staining is found, and also a focal membranous pattern is seen in HCC. C, Glypican 3. Strong cytoplasmic and focal membranous staining is found in HCC. D, a-Fetoprotein (AFP). Diffuse expression of AFP is seen in HCC (A, ×100; B-D, ×200).
Ikeda_2012100561.indd 334 8/1/13 11:14 AM
Am J Clin Pathol 2013;140:329-340 335335 DOI: 10.1309/AJCP66AVBANVNTQJ 335
© American Society for Clinical Pathology
AJCP / Original Article
A B
C D
E F
❚Image 3❚ Immunohistochemical findings of combined hepatocellular-cholangiocarcinoma with stem cell features, typical subtype. A, Small, oval, and dark-stained cells are distributed between fibrous septa and the periphery of carcinoma cell nests composed of relatively large cells with an eosinophilic and granular cytoplasm (H&E). B, HepPar1. Almost all carcinoma cells are positive. C, Delta-like 1 homolog (DLK1). Cytoplasmic staining of DLK1 is found mainly in peripheral cells of hepatocellular carcinoma (HCC) nests, and DLK1 is focally expressed in stem cell–like cells. D, Cytokeratin 19 (CK19). Some expression of CK19 is seen in small peripheral cells. E, Neural cell adhesion molecule (NCAM)/CD56. Some expression of NCAM/CD56 is seen in peripheral small cells. F, Epithelial cell adhesion molecule (EpCAM). The peripheral HCC cells tend to show membranous staining of EpCAM, and stronger staining is observed in stem cell–like small cells (A-C, F, ×200; D, E, ×400).
Ikeda_2012100561.indd 335 8/1/13 11:15 AM
336 Am J Clin Pathol 2013;140:329-340336 DOI: 10.1309/AJCP66AVBANVNTQJ
© American Society for Clinical Pathology
Ikeda et al / Liver Cancer With Stem Cell Features and DLK1
In our study, immunohistochemical staining of DLK1 was observed in hepatoblasts in the early fetal period, similar to rodents, but there were no positive findings in normal or cirrhotic liver after birth. Our results are consistent with previous studies using human liver.10,12,13 Therefore, there seem to be differences between humans and rodents in the role and significance of DLK1 expression, although this may be related to the immunohistochemical technique used.
The expression of DLK1 in HCC has been reported in several studies.10-12 DLK1 was detected in 20.5% of HCCs in a study by Yanai et al10 and in 56.8% of HCCs
cell–like areas than that for HCC, ICC, and the classic type of combined HC-CC. Combined HC-CC with stem cell features was just as likely to occur in cirrhotic liver as in HCC. Frequent expression of DLK1 was found in HC-CC with stem cell features in comparison with HCC, ICC, and classic HC-CC.
In mice and rats, the expression of DLK1 in hepato-blasts of fetal liver, but not adult liver, has been reported, and interestingly, a re-upregulation of DLK1 expression in stem/progenitor (oval) cells has been demonstrated, which possess the ability to both differentiate and repopulate.6-8
A B
C D
❚Image 4❚ Immunohistochemical findings of combined hepatocellular-cholangiocarcinoma with stem cell features, intermediate-cell subtype. A, Tumor cells have an oval-shaped nucleus and scant cytoplasm (H&E). There is no evident differentiation into hepatocytes and cholangiocytes. B, Double immunostaining of HepPar1 (green) and cytokeratin 19 (CK19) (red). Tumor cells showing both membranous red staining and cytoplasmic green/yellow staining are considered positive for both HepPar1 and CK19. C, Delta-like 1 homolog (DLK1). Cytoplasmic expression of DLK1 is seen in intermediate-cell areas. D, Epithelial cell adhesion molecule (EpCAM). Membranous staining of EpCAM is found in intermediate-cell areas (A, C, D, ×200; B, ×400).
Ikeda_2012100561.indd 336 8/1/13 11:15 AM
Am J Clin Pathol 2013;140:329-340 337337 DOI: 10.1309/AJCP66AVBANVNTQJ 337
© American Society for Clinical Pathology
AJCP / Original Article
The frequent expression of DLK1 in group B combined HC-CC was observed in this study. The expression rate was significantly higher in each subtype of group B than in HCC and, furthermore, significantly higher in the typi-cal and cholangiocellular subtypes than in HCC, ICC, and group A combined HC-CC. The expression of DLK1 was located in stem-like cells in typical HC-CC, in intermediate cells in intermediate-cell HC-CC, and in cholangiole-like carcinoma cells in cholangiocellular HC-CC. The stain-ing pattern for DLK1 in group B was different from that in HCC: cytoplasmic and membranous staining dominated
in another study by Huang et al.12 From our data, how-ever, the expression rate was just 10.9%. The degree of differentiation in the HCC cases examined may explain the different incidences of DLK1 expression among these reports because all DLK1-positive HCCs were moderately or poorly differentiated. However, a positive correlation between DLK1 and AFP expression is a finding common to these reports; moreover, DLK1 expression in HCC was significantly correlated with glypican 3 in our study. DLK1 seemed to act as an oncofetal protein similar to AFP or glypican 3.
A B
C D
❚Image 5❚ Immunohistochemical findings of combined hepatocellular-cholangiocarcinoma with stem cell features, cholangiocellular subtype. A, Tumor cells show small, slender, arborizing tubular formation (H&E). B, Cytokeratin 7 (CK7). Diffuse expression of CK7 is seen. C, Delta-like 1 homolog (DLK1). Weak to faint canalicular staining of DLK1 is observed. D, Neural cell adhesion molecule (NCAM)/CD56. Membranous staining of NCAM/CD56 is diffusely found (A, B, D, ×200; C, ×400).
Ikeda_2012100561.indd 337 8/1/13 11:15 AM
338 Am J Clin Pathol 2013;140:329-340338 DOI: 10.1309/AJCP66AVBANVNTQJ
© American Society for Clinical Pathology
Ikeda et al / Liver Cancer With Stem Cell Features and DLK1
0
20
40
HCC CombinedGroup A
(ClassicalType)
CombinedGroup B(TypicalType)
*
CombinedGroup B
(IntermediateType)
CombinedGroup B
(CholangiocellularType)
†
*
ICC
Freq
uenc
y (%
) 60
80
100
0
20
40
3+
2+
1+
0
CombinedGroup A
(ClassicalType)
CombinedGroup B(TypicalType)
CombinedGroup B
(IntermediateType)
CombinedGroup B
(CholangiocellularType)
Freq
uenc
y (%
) 60
80
100
A
B
Ikeda_2012100561.indd 338 8/1/13 11:15 AM
Am J Clin Pathol 2013;140:329-340 339339 DOI: 10.1309/AJCP66AVBANVNTQJ 339
© American Society for Clinical Pathology
AJCP / Original Article
a need for both morphologic and phenotypical observations for the diagnosis of stem cell features.
A progenitor/stem cell origin has been implied for com-bined HC-CC and also cholangiocellular carcinoma.2,5,19 The expression of DLK1 in liver neoplasms may be associated with stem cell features, because DLK1 expression was fre-quently detected in the stem cell type of combined HC-CC in this study and also in hepatoblastomas.11,13 However, it is unclear whether a DLK1-positive result means a progeni-tor/stem origin, because there was no expression in putative progenitor cells in nonneoplastic liver. Xu et al14 suggested that DLK1-positive HCC cells have characteristics similar to cancer stem/progenitor cells, demonstrating increased chemo-resistance, colony formation, spheroid colony formation, and in vivo tumorigenicity compared with DLK1-negative cells. A subpopulation of cells called cancer stem cells is now thought
in HCC, but cytoplasmic staining was predominant in the stem cell type, and luminal staining was occasionally seen in the cholangiocellular subtype. Recently, Komuta et al15 reported that NCAM/CD56 was useful for classifying mixed ICCs (showing focal hepatocytic differentiation and ductular areas), which are thought to be almost the cholan-giocellular subtype of combined HC-CC. Because NCAM/CD56 and CD133, considered stem cell–related markers in the WHO classification and in several reports,16-18 were frequently expressed in group B, the expression of DLK1 in stem cell HC-CC seemed to be associated with stem cell features. These markers may be important to the stem cell features of liver cancers, but it would be dangerous to make judgments based on immunohistochemical results because the expression of these markers is found in HCC, ICC, and classic-type HC-CC to various degrees. At present, there is
❚Figure 2❚ The expression rate of delta-like 1 homolog (DLK1) in liver cancers. A, The frequency of DLK1 expression. The rate of DLK1 is high in each type of combined hepatocellular-cholangiocarcinoma (HC-CC) with stem cell features compared with hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma (ICC), and the classic type. *Statistically higher compared with HCC, ICC, and group A (classic type) of combined HC-CC. †Statistically higher compared with HCC. B, The scores for DLK1 expression in HC-CC. There are 2+ or 3+ cases in group B, whereas there are no 2+/3+ cases in group A. C, The frequency of DLK1, neural cell adhesion molecule (NCAM)/CD56, epithelial cell adhesion molecule (EpCAM), and CD133 in HC-CC. The frequency of DLK1, NCAM/CD56, and CD133 expression is higher in group B than in group A. The expression of DLK1 and NCAM/CD56 is significantly more frequent in the typical subtype and cholangiocellular subtype than in group A. *Compared with group A (classic type).
0
20
40
*
* *
*DLK1
NCAM/CD56
EpCAM
CD133
CombinedGroup A
(ClassicalType)
CombinedGroup B(TypicalType)
CombinedGroup B
(IntermediateType)
CombinedGroup B
(CholangiocellularType)
Freq
uenc
y (%
) 60
80
100C
Ikeda_2012100561.indd 339 8/1/13 11:15 AM

340 Am J Clin Pathol 2013;140:329-340340 DOI: 10.1309/AJCP66AVBANVNTQJ
© American Society for Clinical Pathology
Ikeda et al / Liver Cancer With Stem Cell Features and DLK1
5. Woo HG, Lee JH, Yoon JH, et al. Identification of a cholangiocarcinoma-like gene expression trait in hepatocellular carcinoma. Cancer Res. 2010;70:3034-3041.
6. Tanimizu N, Nishikawa M, Saito H, et al. Isolation of hepatoblasts based on the expression of Dlk/Pref-1. J Cell Sci. 2003;116:1775-1786.
7. Jensen CH, Jauho EI, Santoni-Rugiu E, et al. Transit-amplifying ductular (oval) cells and their hepatocytic progeny are characterized by a novel and distinctive expression of delta-like protein/preadipocyte factor 1/fetal antigen 1. Am J Pathol. 2004;164:1347-1359.
8. Oertel M, Menthena A, Chen YQ, et al. Purification of fetal liver stem/progenitor cells containing all the repopulation potential for normal adult rat liver. Gastroenterology. 2008;134:823-832.
9. Floridon C, Jensen CH, Thorsen P, et al. Does fetal antigen 1 (FA1) identify cells with regenerative, endocrine and neuroendocrine potentials? a study of FA1 in embryonic, fetal, and placental tissue and in maternal circulation. Differentiation. 2000;66:49-59.
10. Yanai H, Nakamura K, Hijioka S, et al. Dlk-1, a cell surface antigen on foetal hepatic stem/progenitor cells, is expressed in hepatocellular, colon, pancreas and breast carcinomas at a high frequency. J Biochem. 2010;148:85-92.
11. Luo JH, Ren B, Keryanov S, et al. Transcriptomic and genomic analysis of human hepatocellular carcinomas and hepatoblastomas. Hepatology. 2006;44:1012-1024.
12. Huang J, Zhang X, Zhang M, et al. Up-regulation of DLK1 as an imprinted gene could contribute to human hepatocellular carcinoma. Carcinogenesis. 2007;28:1094-1103.
13. Dezso K, Halász J, Bisgaard HC, et al. Delta-like protein (DLK) is a novel immunohistochemical marker for human hepatoblastomas. Virchows Arch. 2008;452:443-448.
14. Xu X, Liu RF, Zhang X, et al. DLK1 as a potential target against cancer stem/progenitor cells of hepatocellular carcinoma. Mol Cancer Ther. 2012;11:629-638.
15. Komuta M, Govaere O, Vandecaveye V, et al. Histological diversity in cholangiocellular carcinoma reflects the different cholangiocyte phenotypes. Hepatology. 2012;55:1876-1888.
16. Fujii T, Zen Y, Harada K, et al. Participation of liver cancer stem/progenitor cells in tumorigenesis of scirrhous hepatocellular carcinoma—human and cell culture study. Hum Pathol. 2008;39:1185-1196.
17. Kozaka K, Sasaki M, Fujii T, et al. A subgroup of intrahepatic cholangiocarcinoma with an infiltrating replacement growth pattern and a resemblance to reactive proliferating bile ductules: ‘bile ductular carcinoma’. Histopathology. 2007; 51:390-400.
18. Yoshikawa S, Zen Y, Fujii T, et al. Characterization of CD133+ parenchymal cells in the liver: histology and culture. World J Gastroenterol. 2009;15:4896-4906.
19. Komuta M, Spee B, Vander Borght S, et al. Clinicopathological study on cholangiolocellular carcinoma suggesting hepatic progenitor cell origin. Hepatology. 2008;47:1544-1556.
20. Reya T, Morrison SJ, Clarke MF, et al. Stem cells, cancer, and cancer stem cells. Nature. 2001;414:105-111.
21. Al-Hajj M, Clarke MF. Self-renewal and solid tumor stem cells. Oncogene. 2004;23:7274-7282.
to be responsible for tumor initiation, growth, metastasis, and recurrence.20,21 It seems possible that the expression of DLK1 in liver cancers, mainly in group B combined HC-CC, is related to the existence of cancer stem cells, but more studies are needed.
We were able to classify primary liver cancers according to the 2010 WHO classification. New subtypes of combined HC-CC with stem cell features—namely, typical, intermedi-ate-cell, and cholangiocellular subtypes—were identified in more than 5% of the tumors in 24 of 36 cases in this study. The frequent expression of DLK1 and NCAM/CD56 was seen in stem-like cells in the typical subtype and also chol-angiocellular components. However, in the intermediate-cell subtype, the expression rate for DLK1 was higher than in HCC, but DLK1, NCAM/CD56, and CD133 tended to be expressed less frequently than in other stem cell subtypes. The intermediate-cell subtype may reflect transdifferentiation rather than a stem cell origin.
The distribution of DLK1 expression was not the same in NCAM/CD56 and/or CD133-positive cells. DLK1 seems to be a candidate for a stem cell marker, although the significance of its expression is not yet clear. DLK1 could be a potential therapeutic target against cancer stem/progenitor cells,12,14 and the analysis of DLK1-positive cells in liver cancers, mainly in the stem cell type of combined HC-CC, is urgently needed.
In conclusion, the expression of DLK1 in combined HC-CC seems to be associated with stem cell features, and DLK1 is likely to be a candidate stem cell marker in liver can-cer. There are differences in etiology, morphology, and stem cell phenotype for HC-CC with stem cell features. Therefore, the classification of combined HC-CC in the fourth edition of the WHO system seems to be significant and important to elucidation of the pathogenesis of stem cell–related cancers.
Address reprint requests to Dr Ikeda: Section of Diagnostic Pathology, Kanazawa University Hospital, Kanazawa 920-8641, Japan; e-mail: [email protected].
References 1. Theise ND, Park YN, Nakanuma Y. Combined
hepatocellular-cholangiocarcinoma. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, eds. WHO Classification of Tumours of the Digestive System. 4th ed. Lyon, France: IARC; 2010:225-227.
2. Theise ND, Yao JL, Harada K, et al. Hepatic “stem cell” malignancies in adults: four cases. Histopathology. 2003;43:263-271.
3. Chiba T, Zheng YW, Kita K, et al. Enhanced self-renewal capability in hepatic stem/progenitor cells drives cancer initiation. Gastroenterology. 2007;13:937-950.
4. Zhang F, Chen XP, Zhang W, et al. Combined hepatocellular cholangiocarcinoma originating from hepatic progenitor cells: immunohistochemical and double-fluorescence immunostaining evidence. Histopathology. 2008;52:224-232.
Ikeda_2012100561.indd 340 8/1/13 11:15 AM