Embed Size (px)
Citation preview
Complicaciones cardiovasculares por consumo de cocaína. Dolor torácico
inducido por cocaína. Arritmias cardíacas.
Robert S. Hoffman, MD

Cocaine-Related Chest Pain Cocaine-Related Chest Pain
History / Epidemiology Clinical Presentation Mechanism Differential Diagnosis Evaluation Treatment Disposition
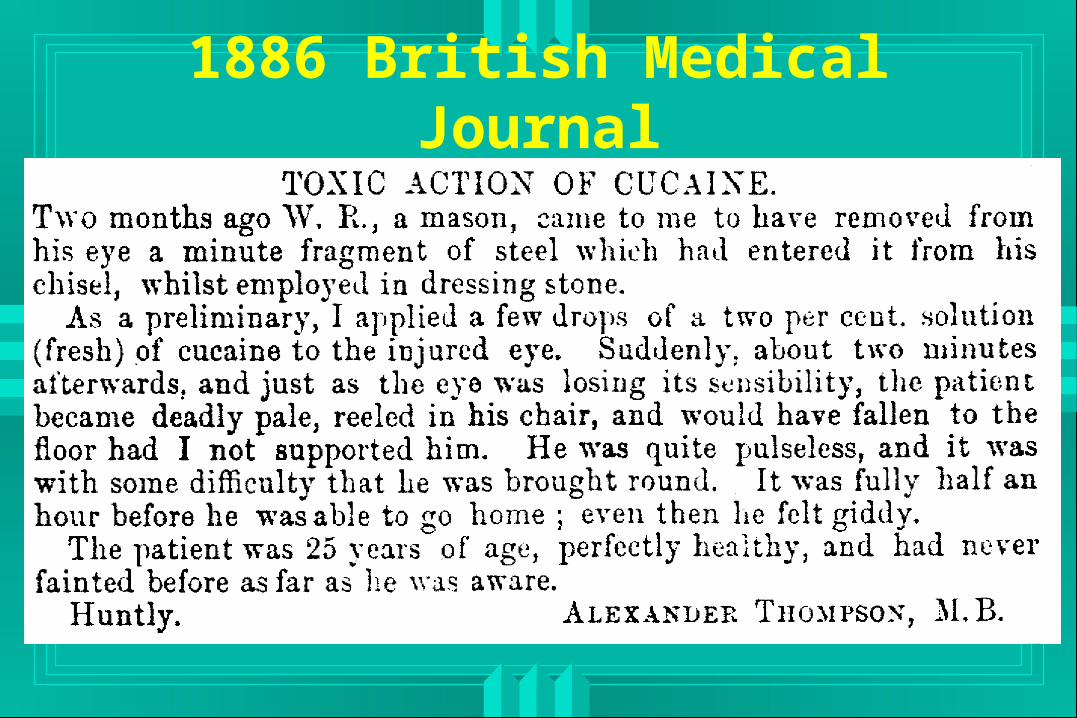
1886 British Medical Journal
Cocaine Chest PainCocaine Chest Pain
175,000 cocaine-related ED visits each year
Chest pain is the most common complaint• 40% of the patients• 57% admitted to the hospital• Average LOS = 3 days• Cost exceeds $83 million in hospital expenses
alone• Most rule out for MI• Most continue to use cocaine after discharge
Cocaine-Chest PainCocaine-Chest Pain
Most common chief complaints can be easily associated with CV disease• Chest pain 39.5%• Short of breath 21.9%• Palpitations 20.6%• Diaphoresis 6.4%
– Brody SL: Am J Med 1990;88:325 (n=233)

Cocaine-Myocardial InfarctionCocaine-Myocardial Infarction
First case of cocaine related MI was in 1982• Coleman DL: West J Med 1982;136:444
91 MI’s reviewed from existing reports81 males, average age 32.8, all routes of use
Time to onset: Mean 30 min, Max 24 hours
Tobacco in 87%, other risk factors rare
ASHD 31%, thrombosis without ASHD 24%
• Hollander and Hoffman: J Emerg Med 1992;10:169
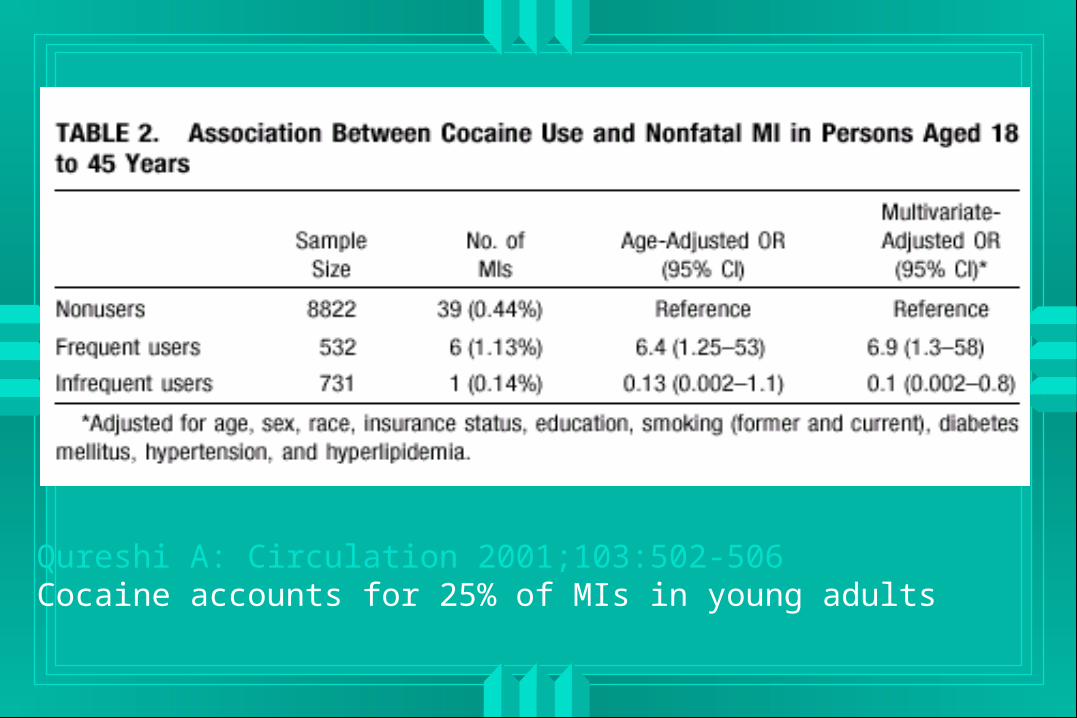
Qureshi A: Circulation 2001;103:502-506Cocaine accounts for 25% of MIs in young adults

FarmacologíaVía Absorción máxima Duración
(minutos) (horas)
Intravenoso 0,5-2,0 0,25-0,5
Intranasal 30 1-2
Gastrointestinal 60-90 >3
Fumada 0,5-1 0,25-0,5
Mecanismo de acción
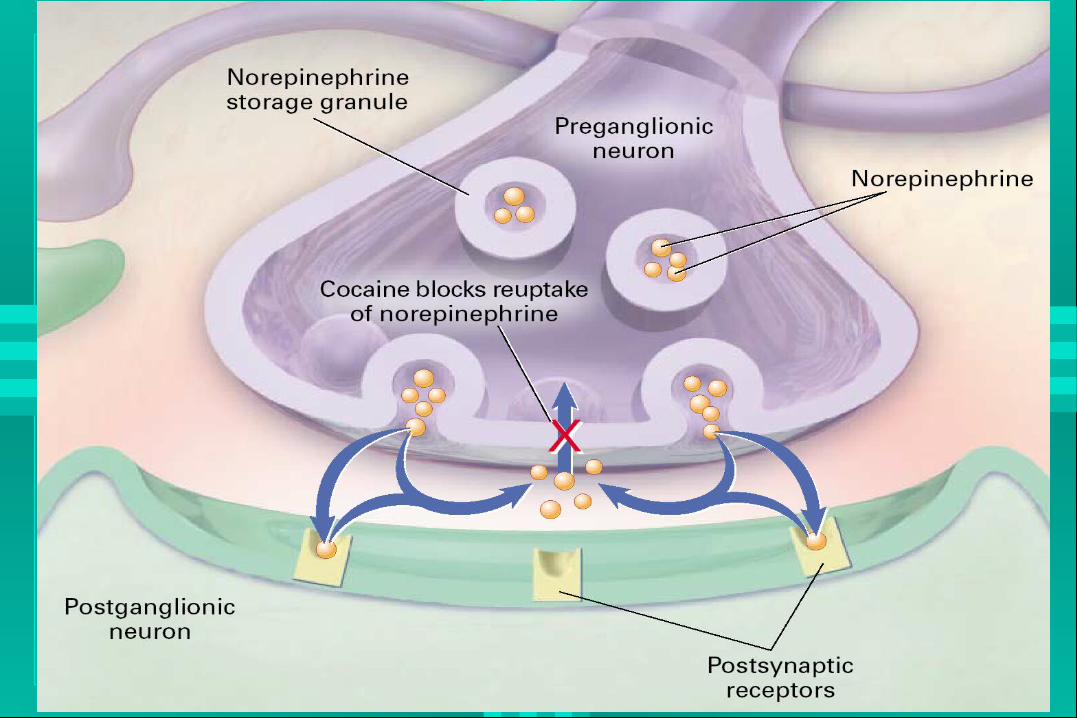
Bloqueo de la recaptación• Dopamina• Noradrenalina• Serotonina
Aminoácidos excitadores agonistas Efecto antiarritmico Tipo I Otros
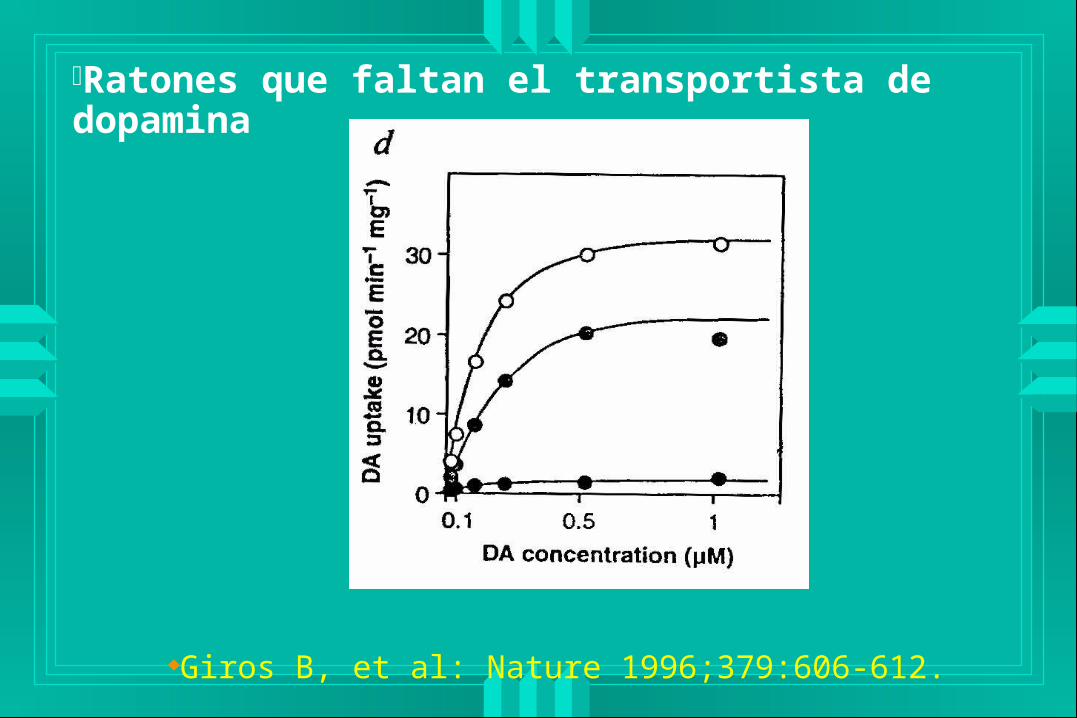
Ratones que faltan el transportista de dopamina
Giros B, et al: Nature 1996;379:606-612.
Homocigotos• Agitación psicomótora
• Pobre ganacia de peso
• Mueren jovenes
Heterocigoto• Comportamiento intermedio
– Giros B, et al: Nature 1996;379:606-612.
Agitación Psicomótora y Dopamina
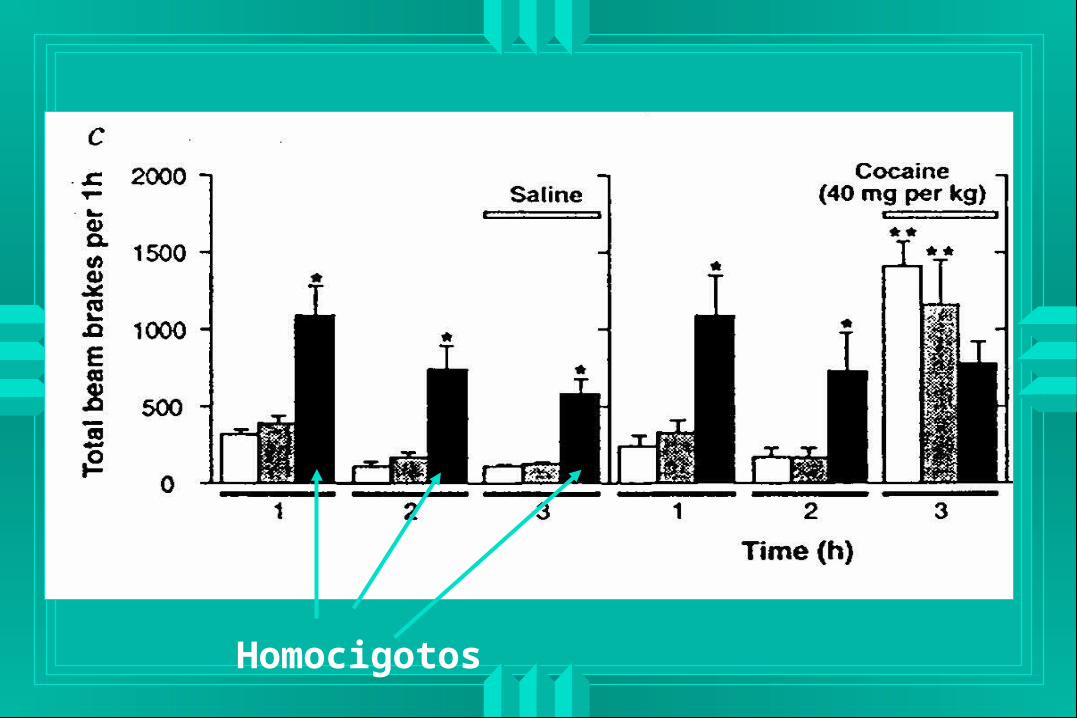
Homocigotos
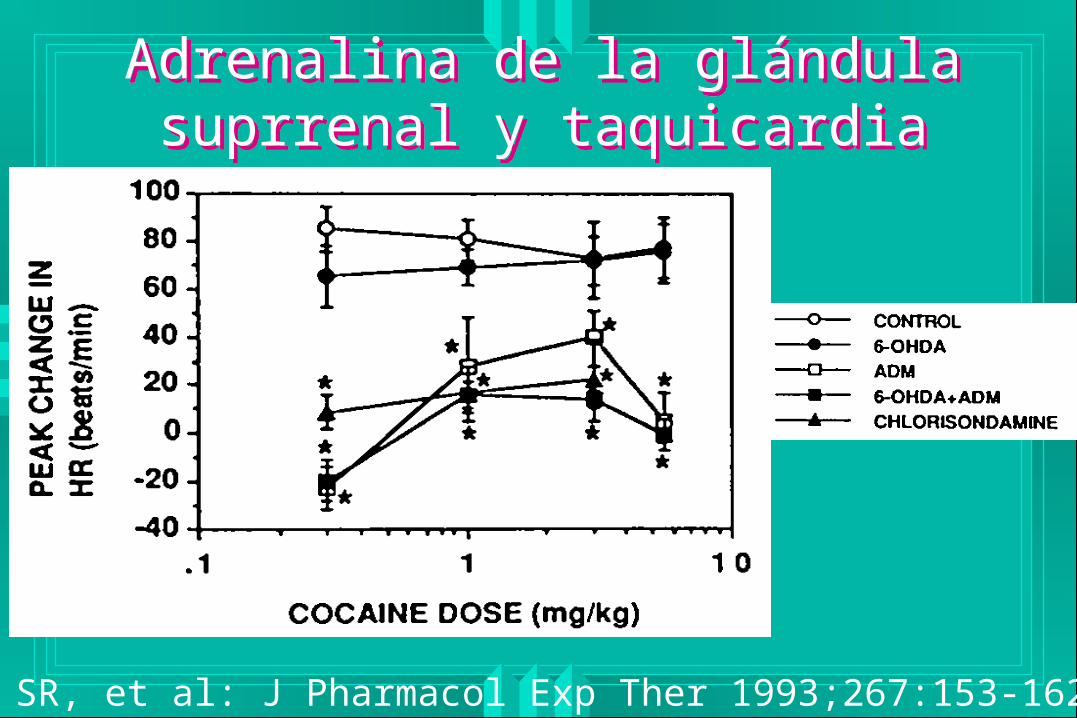
Adrenalina de la glándula suprrenal y taquicardia
Adrenalina de la glándula suprrenal y taquicardia
Tella SR, et al: J Pharmacol Exp Ther 1993;267:153-162
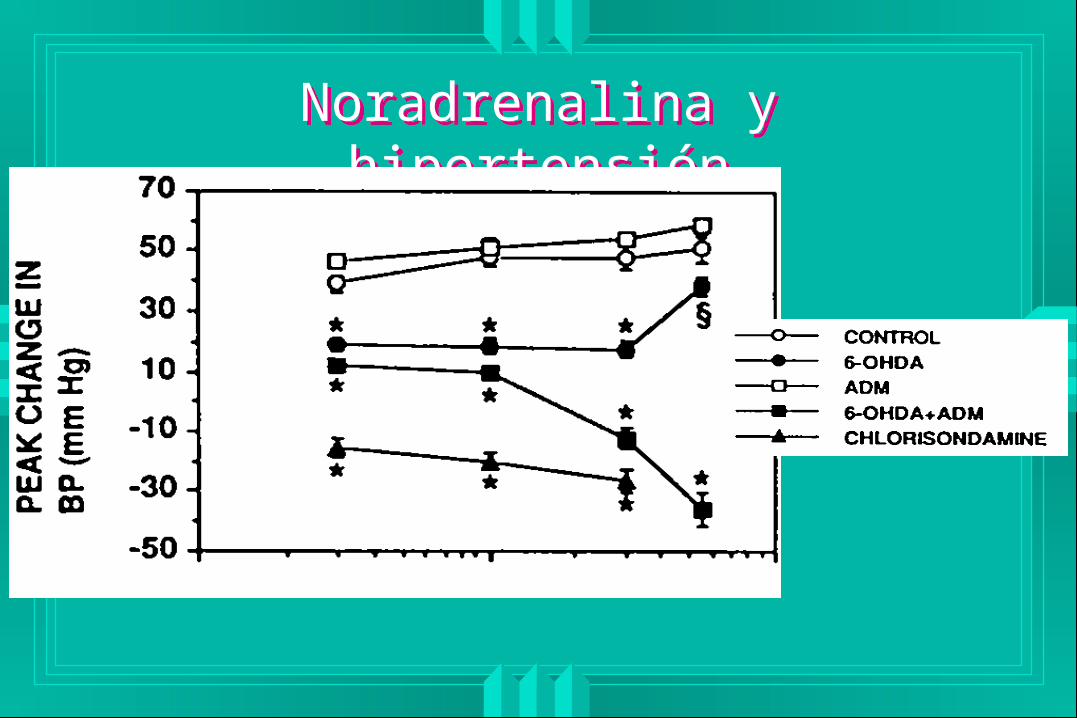
Noradrenalina y hipertensiónNoradrenalina y hipertensión
PathophysiologyPathophysiology
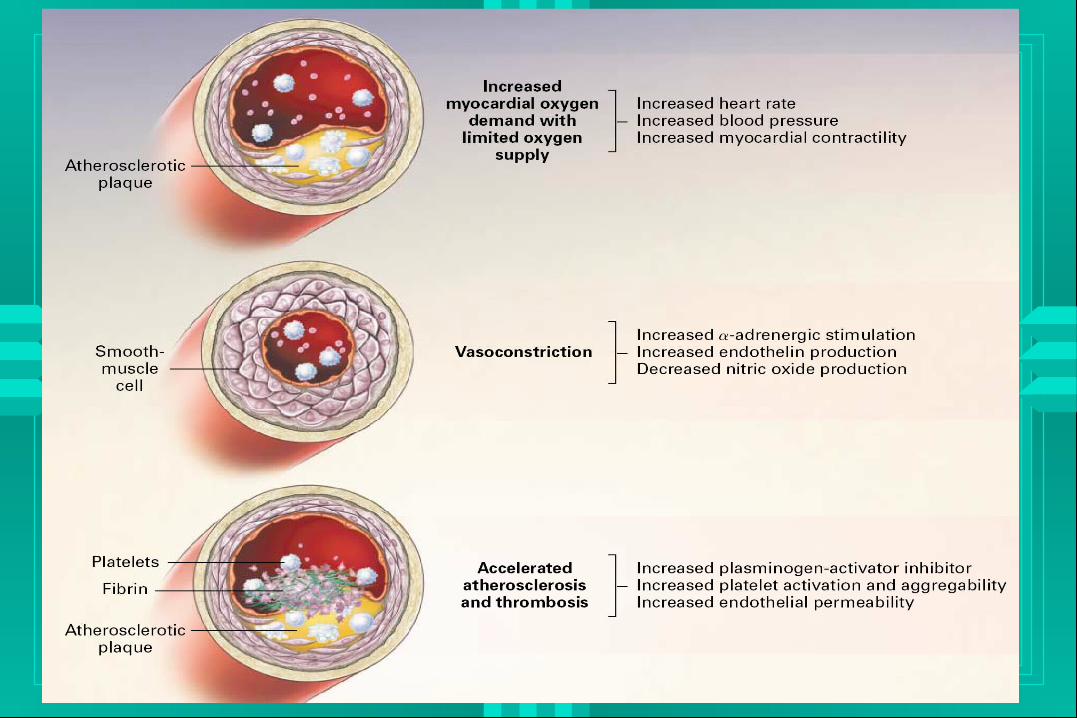
Increased Oxygen DemandIncreased Oxygen Demand
Increased catecholamines in patients with cocaine related cardiac symptoms• Karch: Ann Emerg Med 1987;16:481
Norepinephrine (345-622 g/L)• normal (0-90 g/L)
Epinephrine (135-202 g/L)• normal (0-55 g/L)
Hypertension and tachycardia result
Cocaine-induced VasospasmCocaine-induced Vasospasm Human volunteer study of patients given
intranasal cocaine during cardiac cath• Coronary sinus blood flow decreases
• Left coronary artery diameter decreases
• Coronary vascular resistance increases
• Effects reversed by phentolamine
• Effects exacerbated by propranolol– Lange RA: NEJM 1989;321:1557
– Lange RA: Ann Intern Med, 1990;112:897
Accelerated AtherogenesisAccelerated Atherogenesis
Animal data• Normal rabbits never develop ASHD• Rabbits fed a high cholesterol diet never
develop ASHD• Rabbits fed a high cholesterol diet plus cocaine
develop atherosclerotic heart disease– Langner RO: FASEB 1989;3:297
Accelerated AtherogenesisAccelerated Atherogenesis
High incidence of ASHD (for age) in patients with cocaine related MI who undergo catheterization
– Hollander and Hoffman: J Emerg Med 1992;10:169
62-77% of patients with cocaine related myocardial infarctions will have some abnormality of their coronary arteries
– Minor RL: Ann Intern Med 1991;115:797– Kontos MC: J Emerg Med 2003;24:9-13
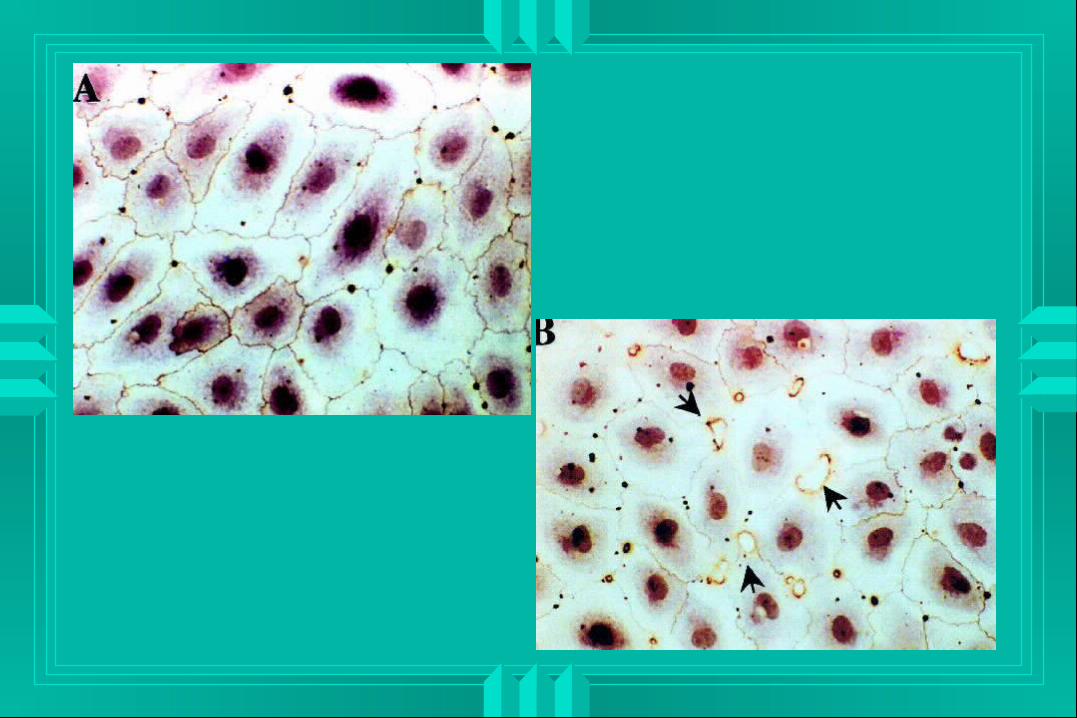
Enhanced CoagulationEnhanced Coagulation
Endothelial effects• Denuded endothelium
– Surface exposed to trigger coagulation
• Loss of EDRF (nitric oxide)– Impaired relaxation
– Impaired inhibition of platelet aggregation
• Reduced prostacycline – Impaired relaxation
Enhanced CoagulationEnhanced Coagulation
Platelet effects• Increased responsiveness to thromboxane and
prostacycline– Increased aggregation
• Increased aggregation releases serotonin• Serotonin constricts dysfunctional endothelium
– Tonga G: Haemostasis 1985;15:100
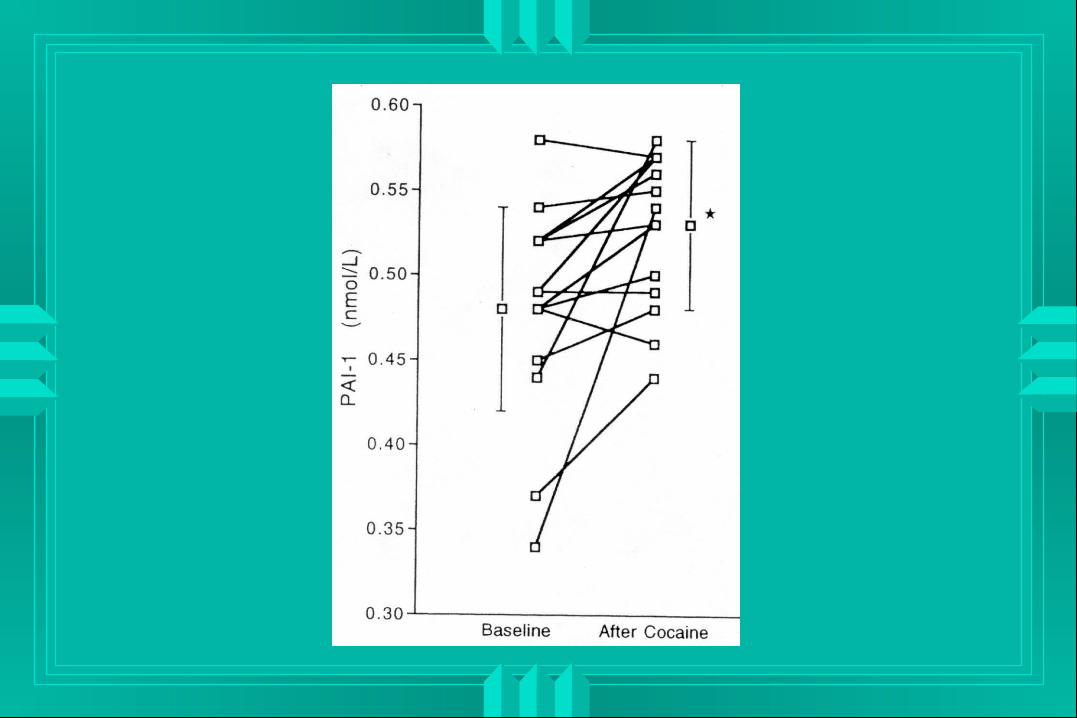
Enhanced CoagulationEnhanced Coagulation
Human study of plasma constituents after receiving intranasal cocaine• Moliterno DJ: Am J Med 1994;96:492
No effect seen on fibrinogen, plasminogen, lipoprotein, or plasminogen activator
Cocaine use resulted in an increase in tissue plasminogen activator inhibitor activity IMPAIRED THROMBOLYSIS
Effects of Cigarette SmokingEffects of Cigarette Smoking
Smoking exacerbates myocardial oxygen demand and vasoconstrictive effects of cocaine• Moliterno: NEJM 1994;330:454
In 51 cocaine chest pain patients the time to onset of pain was related to the interval between tobacco and cocaine use• Hollander JE: VHT 1994;36:349
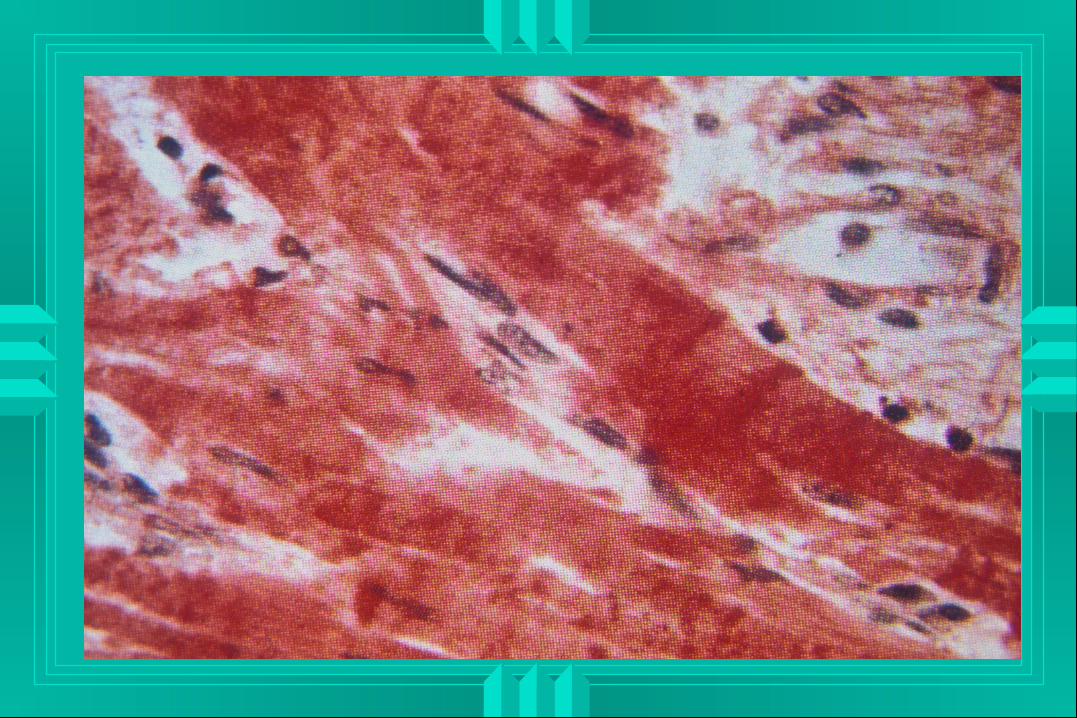
HistologyHistology
Classic myocardial infarction
Contraction band necrosis
Inflammatory infiltrate
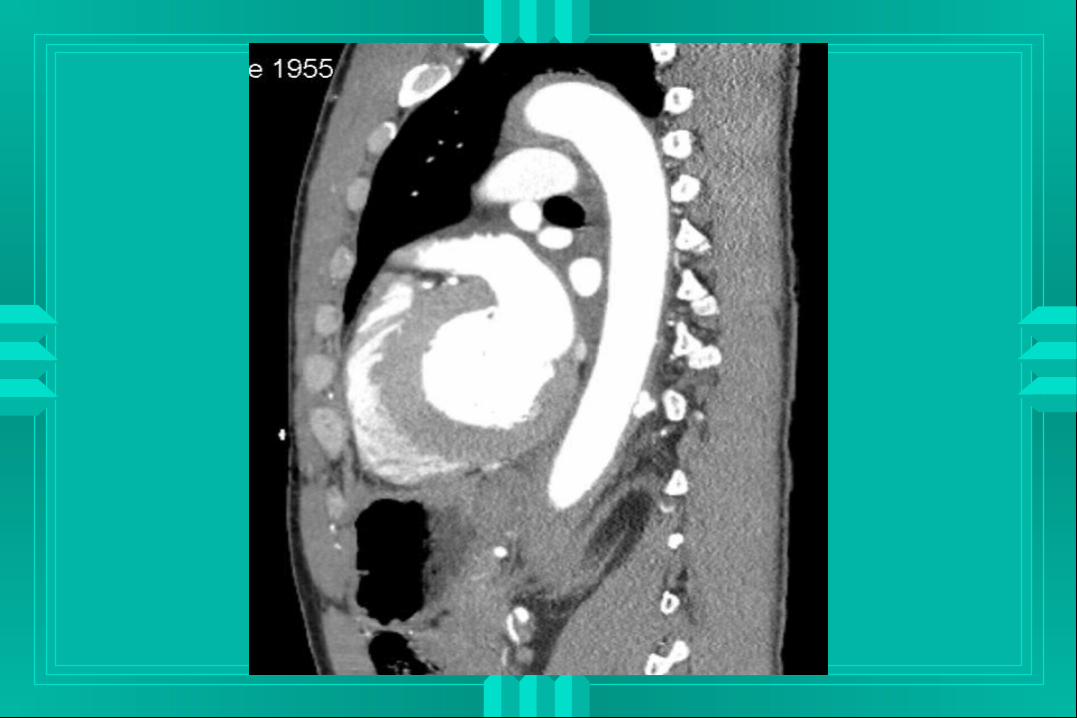
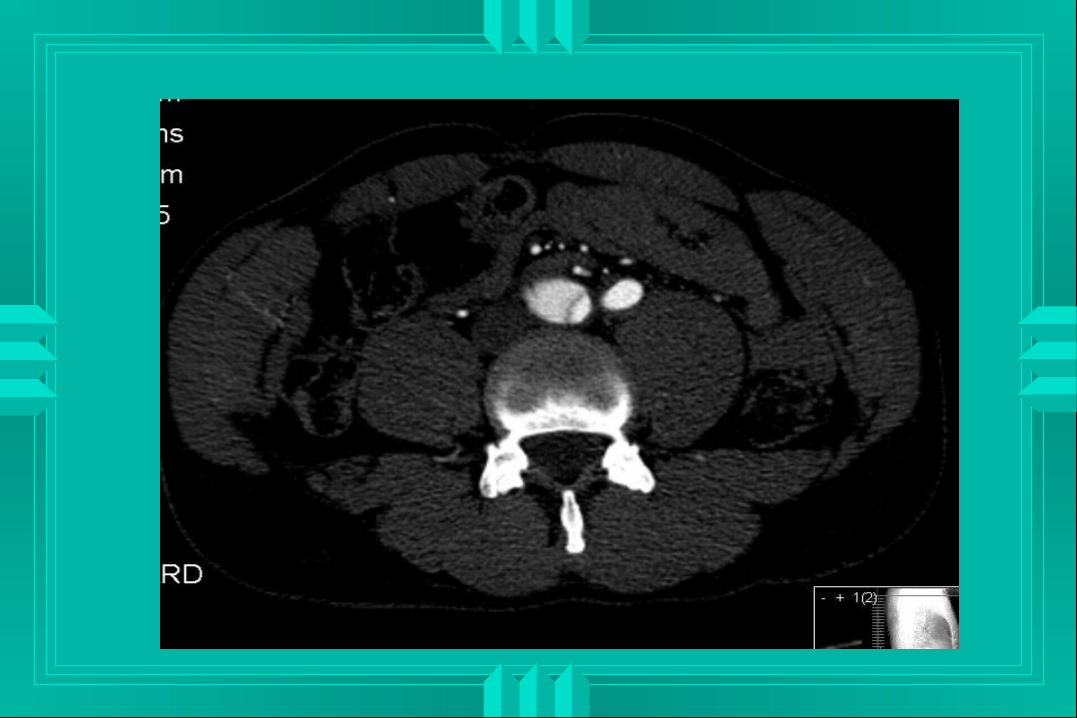
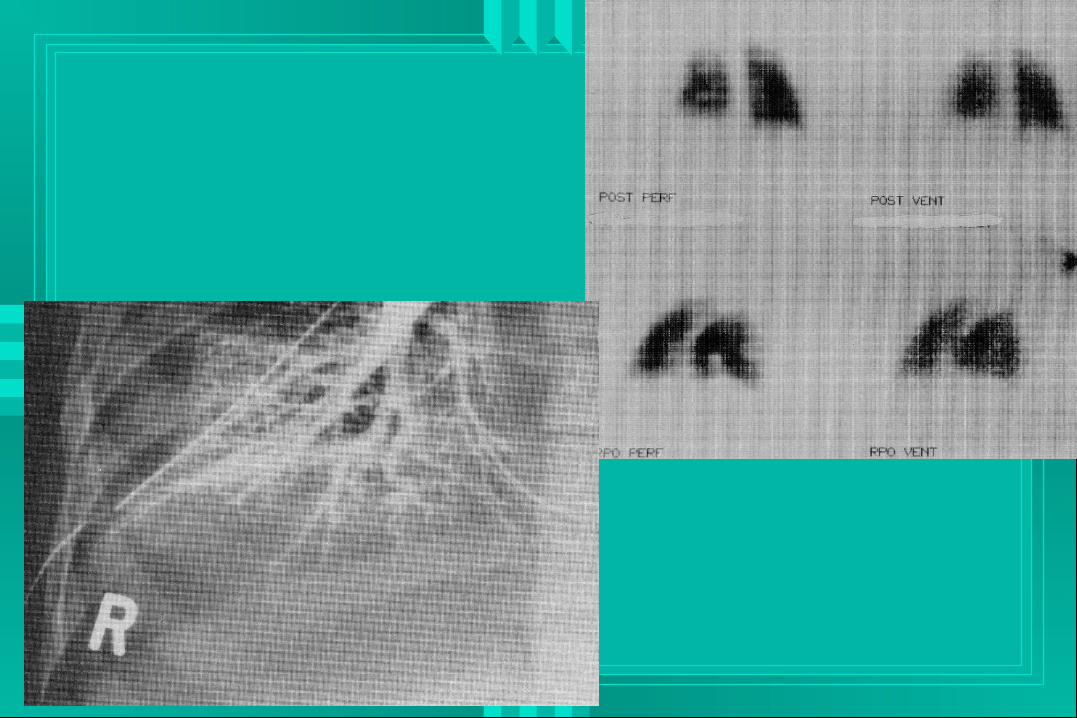
Differential DiagnosisDifferential Diagnosis
Ischemia or infarction Dysrhythmia Dissection Pneumothorax, mediastinum, pericardium Pulmonary infarction or alveolar injury Musculoskeletal Esophageal


EvaluationEvaluation
History• Cocaine use• Tobacco use, other cardiac risk factors• Pain
– Onset
– Duration
– Quality
• Associated factors
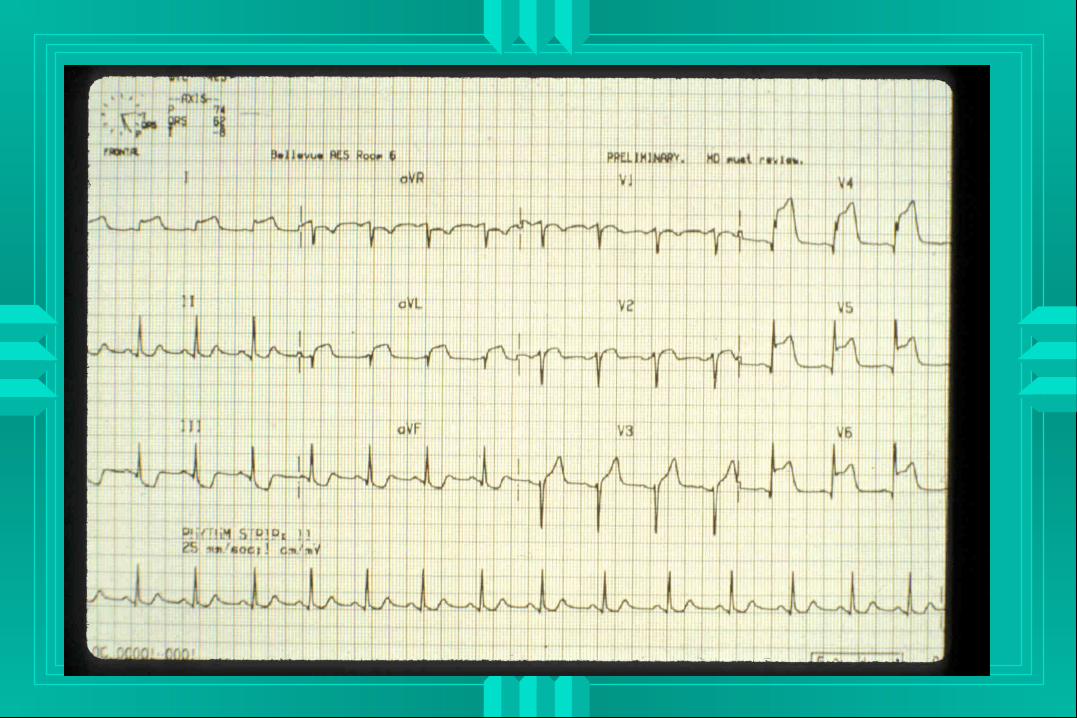
Screening Value of the ECGScreening Value of the ECG
Some patients with normal or nondiagnostic ECG’s will develop myocardial infarction
Many patients with very abnormal ECG’s will never develop an MI
There is a high incidence of “abnormal” ECG’s in this population. This usually represents early repolarization• Hollander JE: J Emerg Med 1994;12:144
COCHPACOCHPA
Prospective study of patients who presented to the ED with cocaine-related chest pain• Hollander and Hoffman: Acad Emerg Med
1994;1:330 Six emergency departments Consecutive enrollment protocol 46 month study 246 patients enrolled
COCHPA ResultsCOCHPA Results
14 MI’s (5.7%, 95% CI 2.7%-8.7%) Median age 33 71.5% male Median onset to chest pain 60 minutes 12 arrhythmias, 4 CHF, 2 deaths 92.9% tobacco use Other cardiac risk factors were low
COCHPA ResultsCOCHPA Results
ECG utility• Sens 35.7% Spec 89.9% • PPV 17.9% NPV 95.8%
History, physical examination or laboratory factors useful for predicting MI• NONE
COCHPA One Year Follow-upCOCHPA One Year Follow-up Prospective study of COCHPA patients
• Hollander and Hoffman: Acad Emerg Med 1995;2:179
203 patients followed for a mean of 408 days• 6 deaths (none from MI): 98% 1 year survival• 2 nonfatal MI’s• Continued cocaine use common (60%)• Recurrent chest pain was more common in
continued users (75% vs 31%)
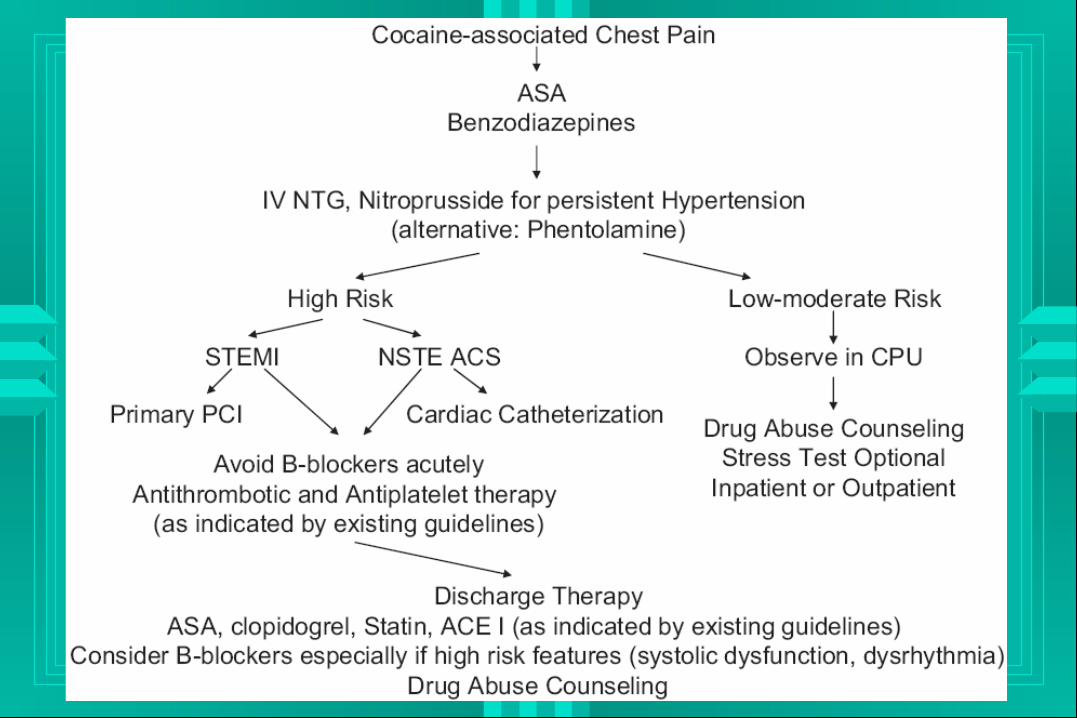
TreatmentTreatment Oxygen Sedation Aspirin, Heparin Nitrates NO Beta adrenergic antagonists Phentolamine Thrombolysis Lidocaine
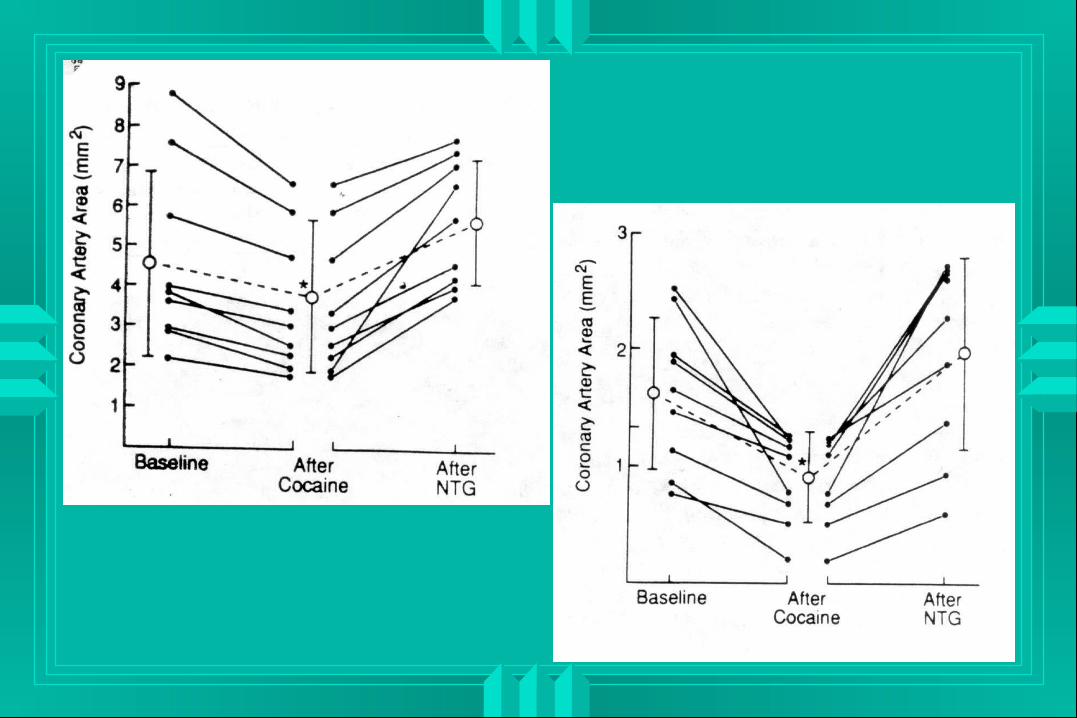
NitratesNitrates
12 patients were given cocaine during routine cardiac catheterization• Brogan WC: J Am Coll Cardiol 1991;18:581-6
Normal arteries constricted 22% Diseased arteries constricted 45% (p<0.02) All vessels responded to sublingual
nitroglycerin
Nitrates - COCHPANitrates - COCHPA
83 patients given nitrates by various routes• J Toxicol Clin Toxicol 1994;32:243
37 (45%): relief or reduction of chest pain 4 (5%): other benefits (CHF) 1 adverse effect:
• hypotension in a patient with a documented right ventricular infarction
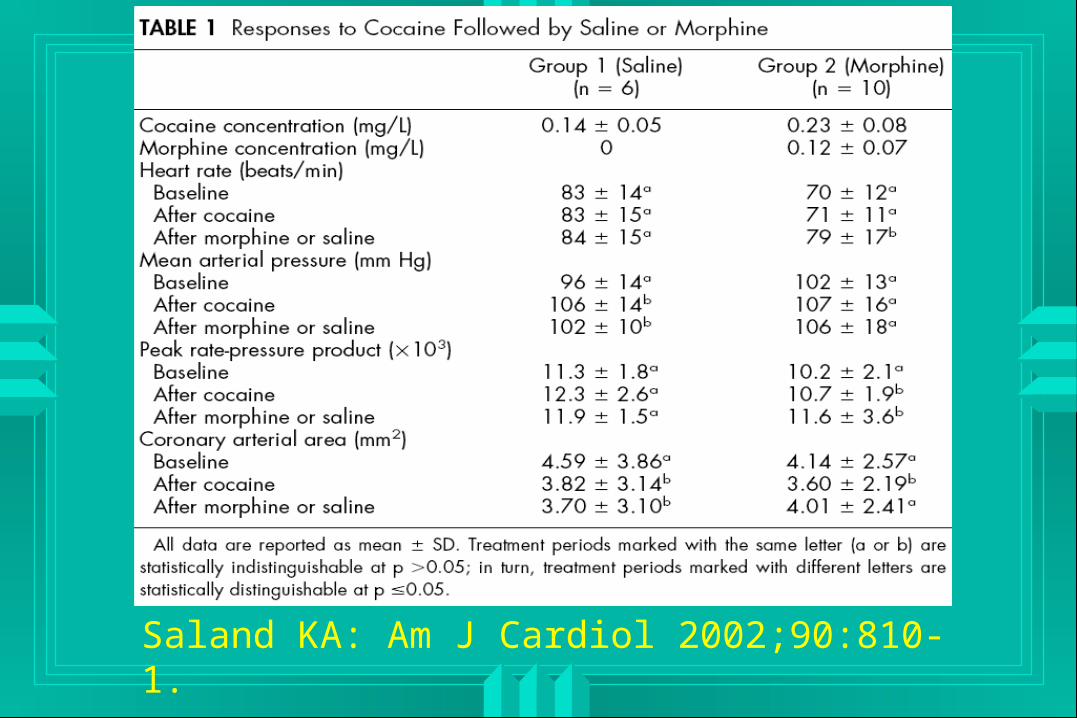
Saland KA: Am J Cardiol 2002;90:810-1.
PhentolaminePhentolamine
38 year old male with 2 hours of chest pain after using cocaine• Hollander and Hoffman: NEJM 1992;327:361
Agitated, 140/90, 120 ST elevations in V2-V4 No response to oxygen, nitrates, aspirin or
diazepam Symptoms and ECG resolved with
phentolamine
Phentolamine Phentolamine
Chan GM, Sharma R, Price D, Hoffman RS, Nelson LS. Phentolamine therapy for cocaine-association acute coronary syndrome. J Med Toxicol. 2006 Sep;2(3):108-11.
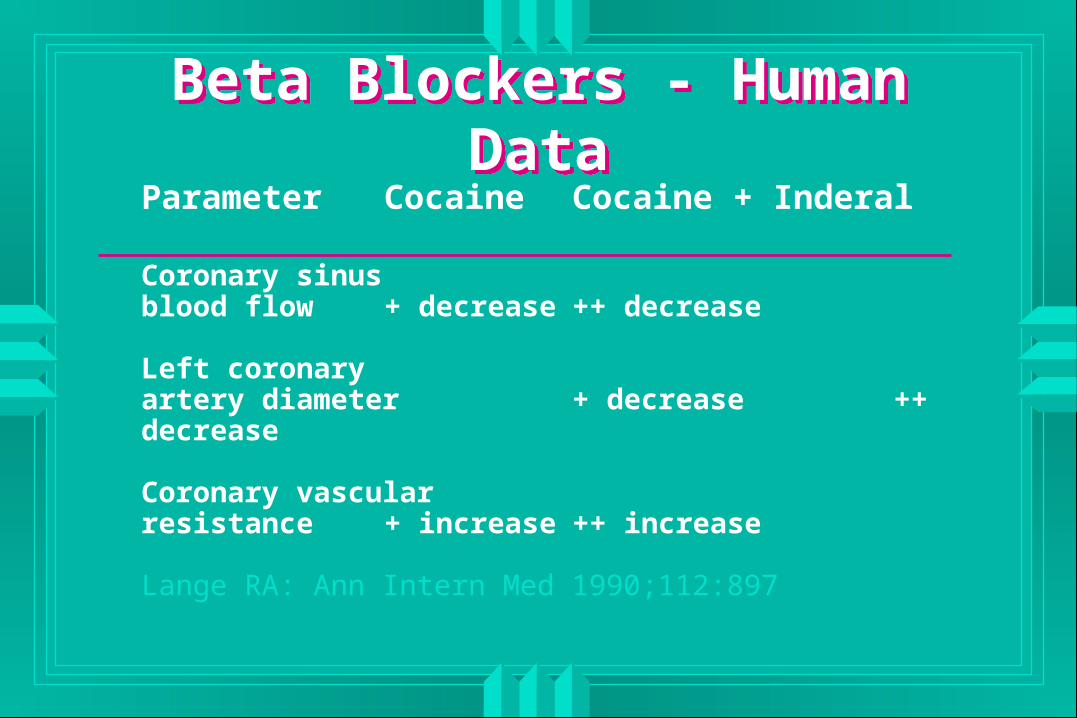
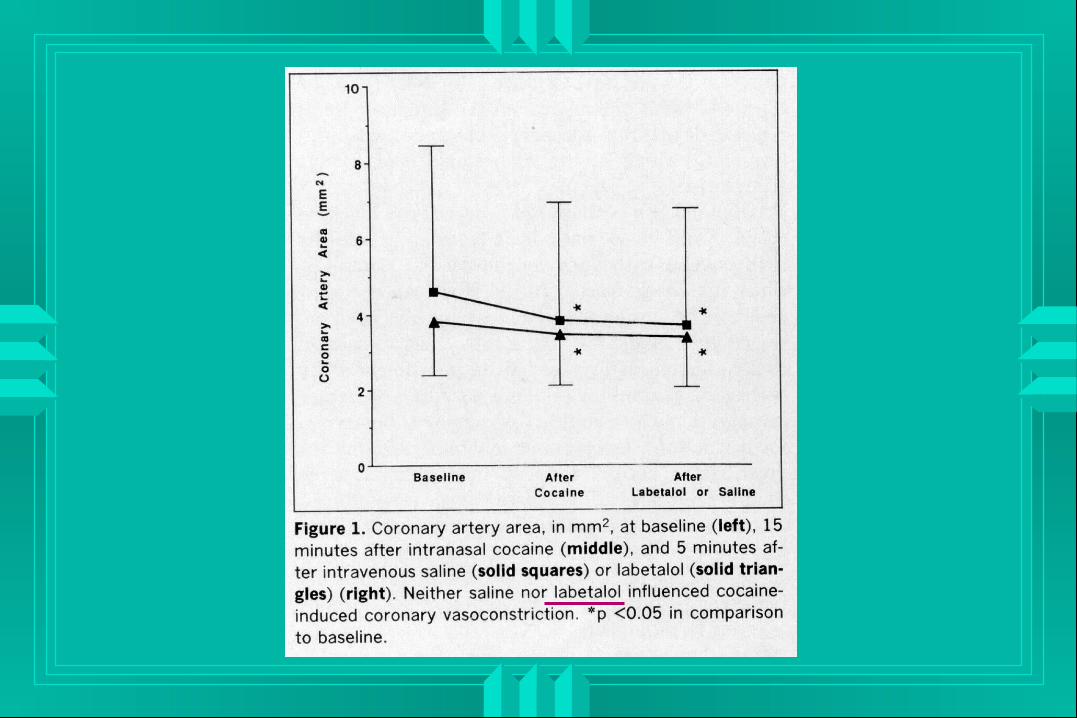
Beta Blockers - Human DataBeta Blockers - Human DataParameter Cocaine Cocaine + Inderal
Coronary sinusblood flow + decrease ++ decrease
Left coronaryartery diameter + decrease ++ decrease
Coronary vascularresistance + increase ++ increase
Lange RA: Ann Intern Med 1990;112:897
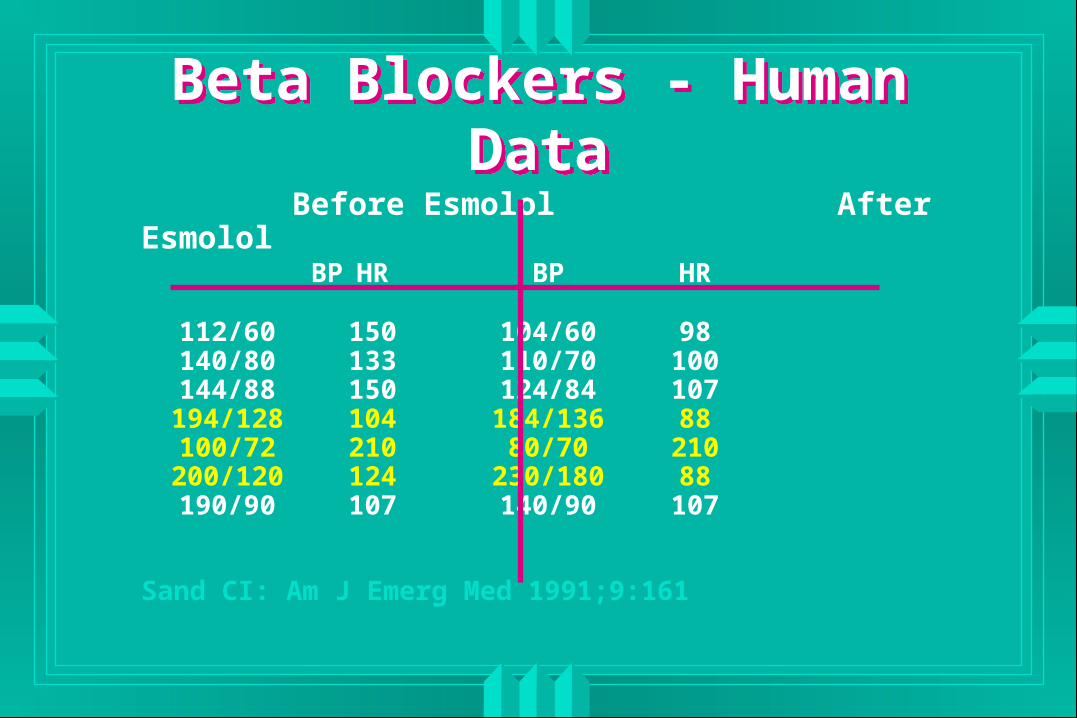
Before Esmolol After Esmolol BP HR BP HR
112/60 150 104/60 98140/80 133 110/70 100144/88 150 124/84 107194/128 104 184/136 88100/72 210 80/70 210200/120 124 230/180 88190/90 107 140/90 107
Sand CI: Am J Emerg Med 1991;9:161
Beta Blockers - Human DataBeta Blockers - Human Data
J Med Toxicol 2007;3:169-172
Thrombolysis - COCHPAThrombolysis - COCHPA
Retrospective study of 136 cocaine-related myocardial infarctions• Hollander and Hoffman: Chest 1995;107:1237
Thrombolysis given in 25 cases No significant adverse effects Insufficient data to judge efficacy Recommended use with cautions
ResultsResults
342 patients evaluated• 42 direct admissions• 302 in final study group
No patient died of a cardiovascular event • 95% CI 0-0.99%
4 of the 256 with good follow up had nonfatal myocardial infarction • 95% CI 0.1-3.1%. • All 4 continued to use cocaine.
ImplicationsImplications
Cocaine chest pain does not equal admission
Low risk patients can be safely discharged after a period of evaluation
Most important intervention is to offer cocaine detoxification / counseling
Dysrhythmic EffectsDysrhythmic Effects
Sodium Channel Blockade Sodium Channel Blockade
Wide complex arrhythmia• Terminal 40 msec rightward axis deviation• Right bundle branch block morphology
Heart rate• Tachycardia: catecholaminergic effects• Bradycardia: initially or following massive
overdose Brugada pattern

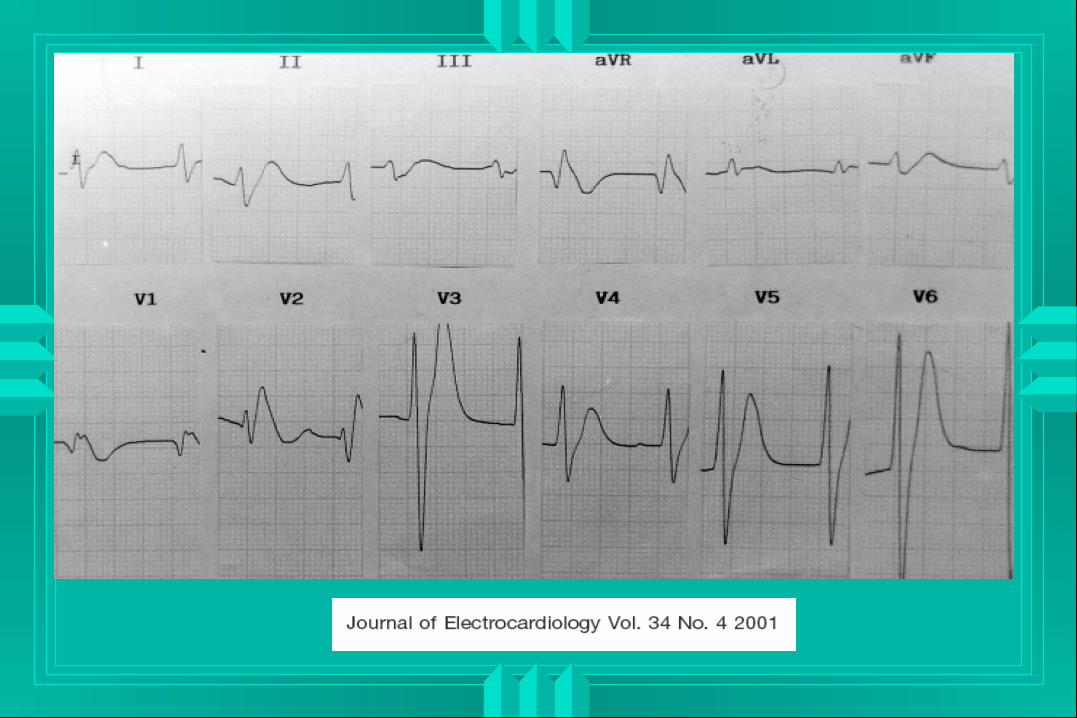
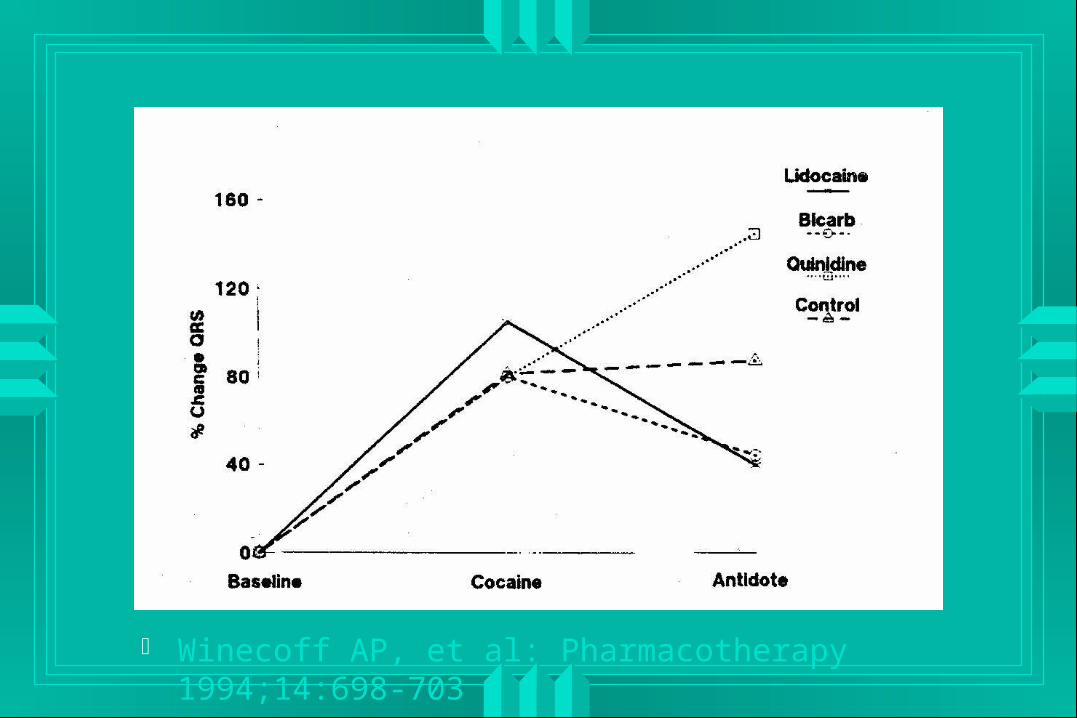
Winecoff AP, et al: Pharmacotherapy 1994;14:698-703
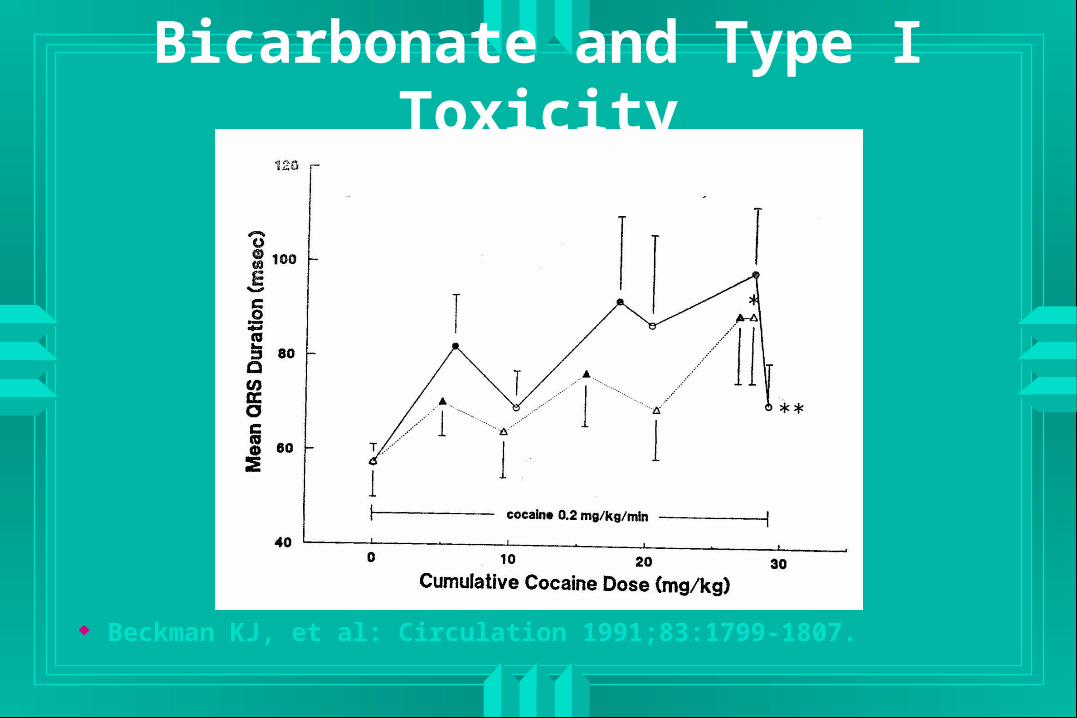
Bicarbonate and Type I Toxicity
Beckman KJ, et al: Circulation 1991;83:1799-1807.
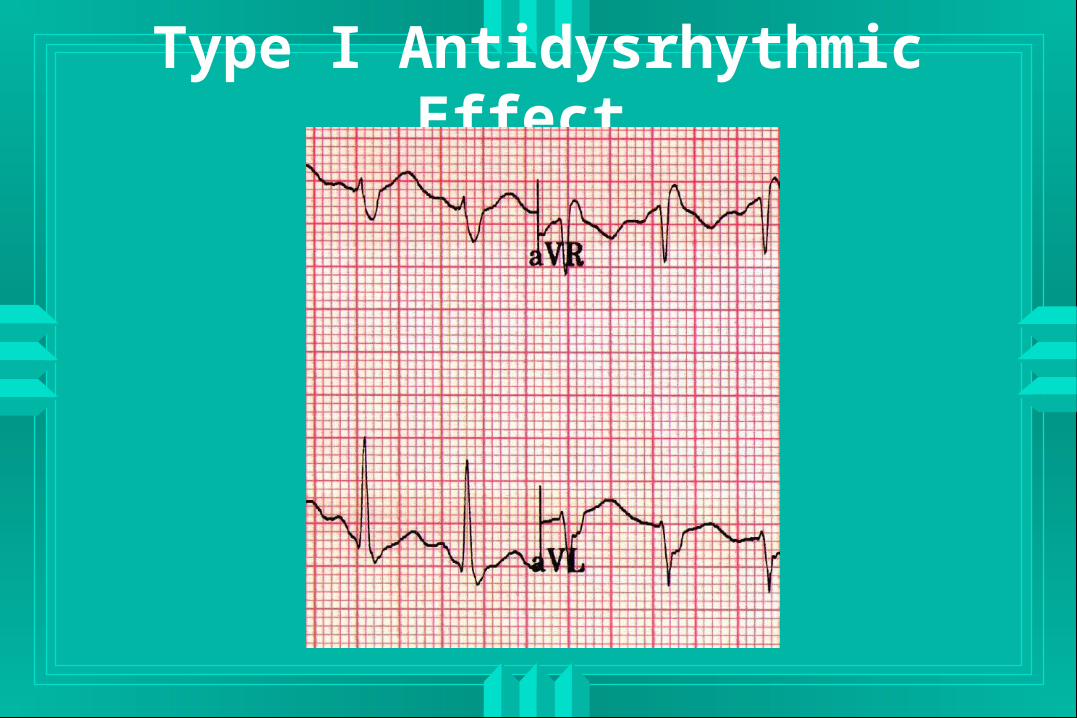
Type I Antidysrhythmic Effect
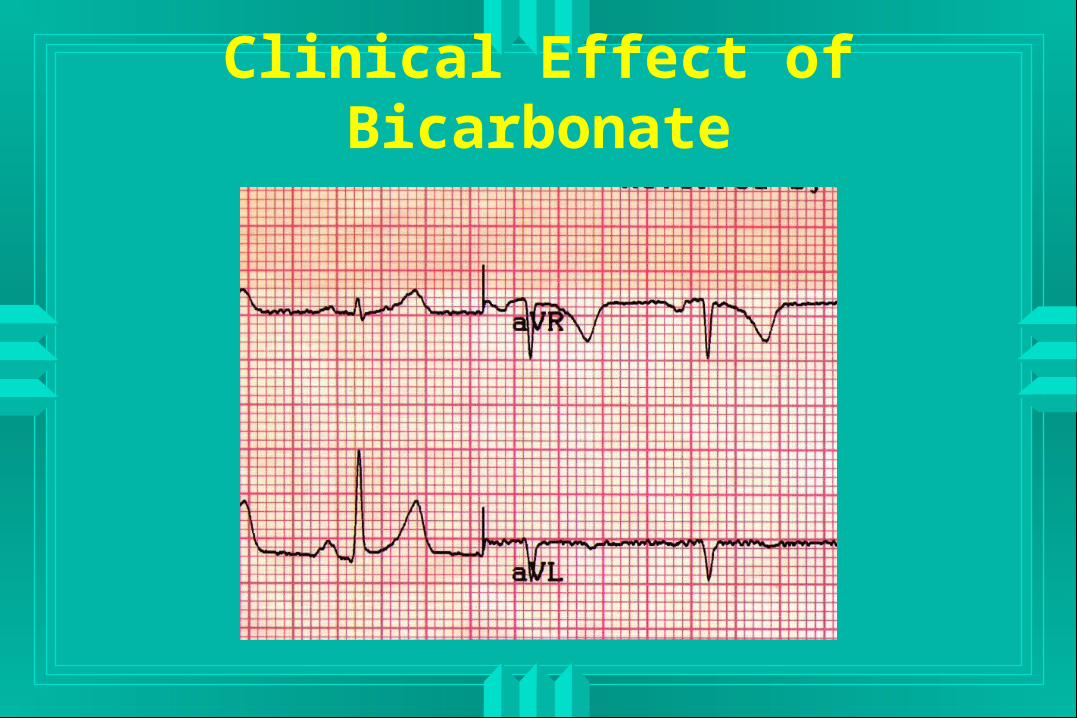
Clinical Effect of Bicarbonate
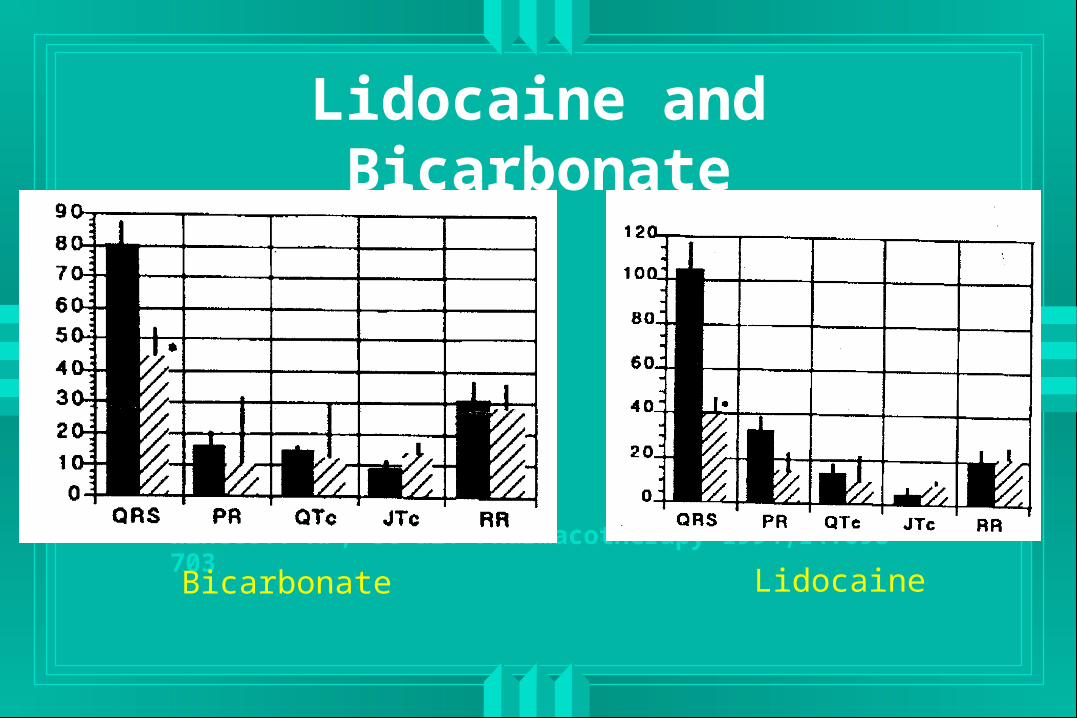
Lidocaine and Bicarbonate
Winecoff AP, et al: Pharmacotherapy 1994;14:698-703Bicarbonate Lidocaine
Retrospective study of 155 cocaine-related myocardial infarctions• Shih RD: Vet Hum Toxicol 1994;36:349
29 patients treated with lidocaine• 31% for prophylaxis• 31% for PVC’s• 38% for V-tach or V-fib
No arrhythmogenesis or seizures
Lidocaine - COCHPALidocaine - COCHPA
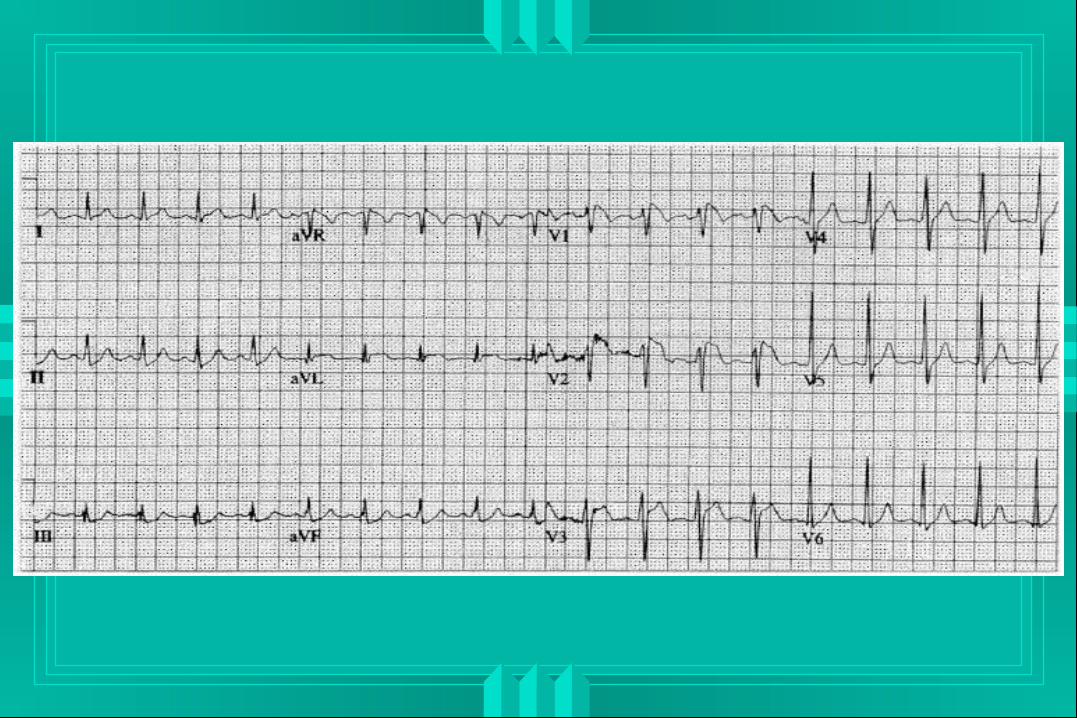
Potassium Channel BlockadePotassium Channel Blockade
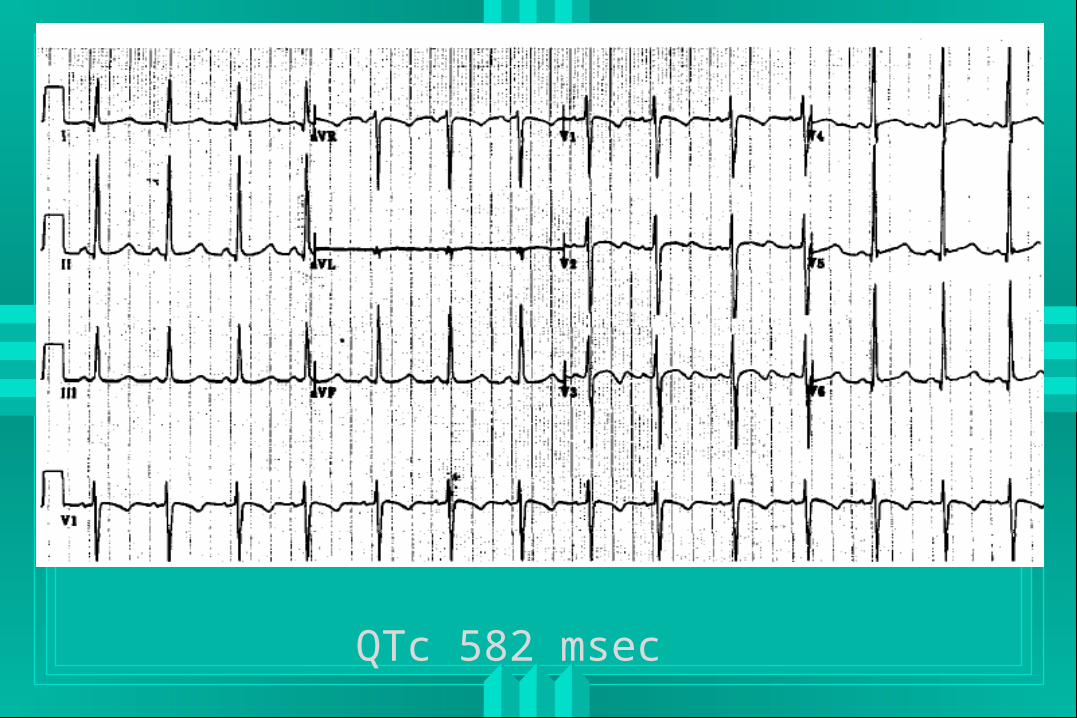
QTc 582 msec
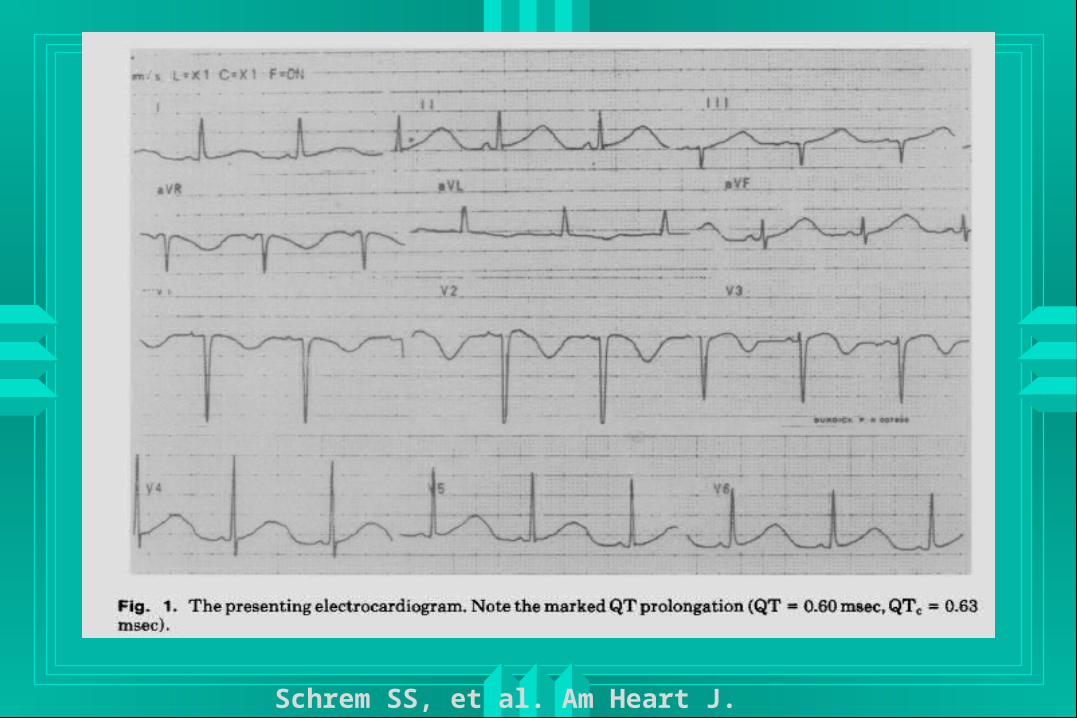
Schrem SS, et al. Am Heart J. 1990;120:980-4.
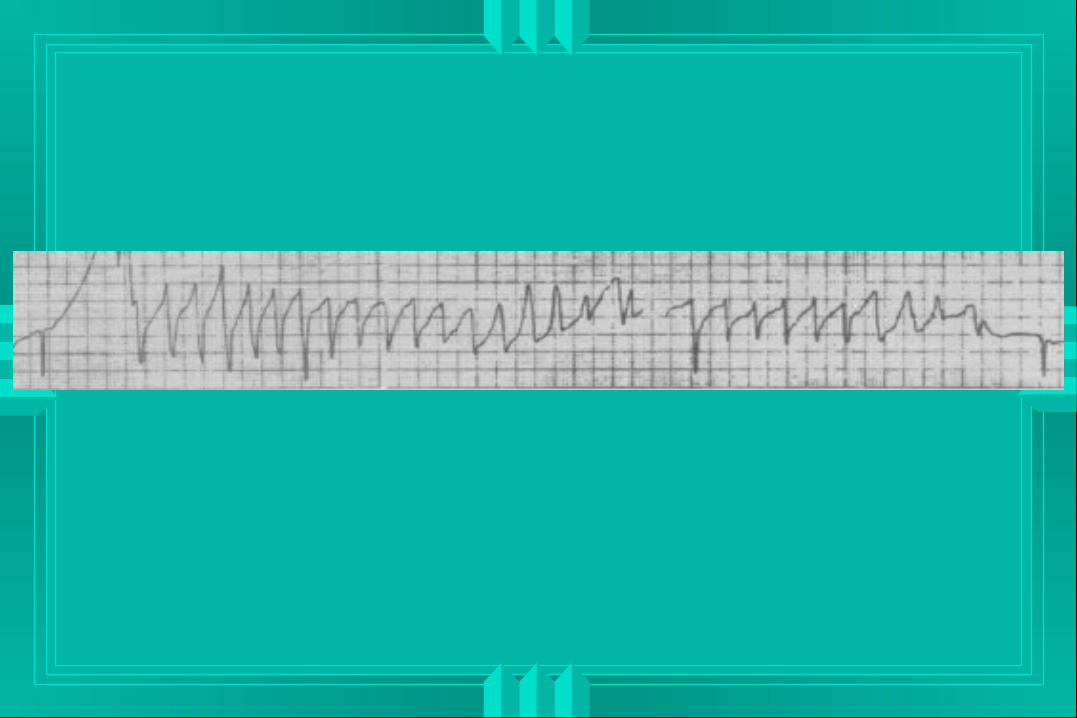
J Addict Dis. 2005;24(1):53-60.
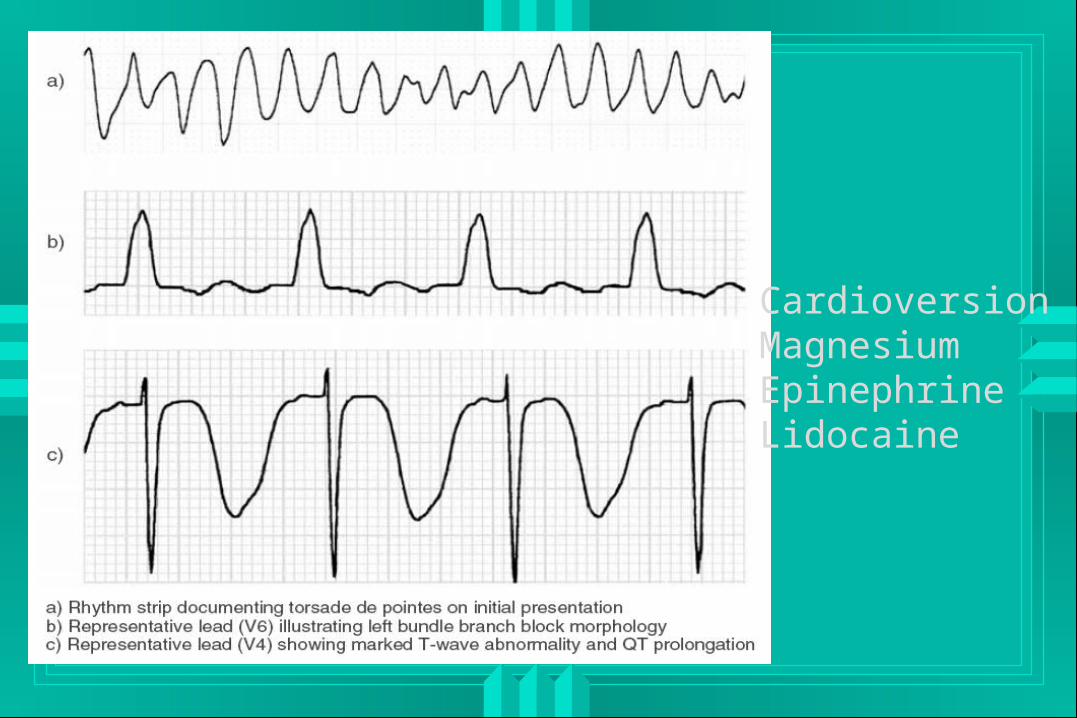
CardioversionMagnesiumEpinephrineLidocaine
QT Prolongation and TdPQT Prolongation and TdP
Cardioversion if unstable Magnesium Overdrive pacemaker Subsequent options unclear
Chest Pain SummaryChest Pain Summary
ACLS / AHA• Minus beta blockers
Absence of complication• Short period of observation• Clinical stability• Stable ECG + Negative marker(s)
Referral for detoxification








![Aborto inducido[2]](https://img.pdfslide.tips/doc/110x75/558982a1d8b42a514a8b4631/aborto-inducido2.jpg)