Embed Size (px)
Citation preview

Congenital Diaphragmatic Hernia
SC 林恆旭SC 楊景堯

Patient Profile
Name: 陳 XX 之子 Age: 1 day Gender: male Admission date: 94/04/27 Chief Complaint:
Antenatal diagnosed congenital diaphragmatic hernia

Birth History G2P1, GA: 37 wks, C/S, PROM(-), DOIC (-),
Perinatal insult(-) Growth: BBW: 2860 gm (25~50 percentile)
BBL: 49 cm ( 50~75 percentile)
BHG: 33.3 cm ( 50~75 percentile)
Maternal Hx:
Denied drug or radiation exposure during pregnancy
Denied any systemic dz; HBsAg(-); HBeAg(-); VDRL(-)

Brief History
GA 23~24 wk: Perinatal ultrasound revealed L’t congenital diaphragmatic hernia in 成大 hospital.
Referred to Dr. 施景中’ s OPD. No polyhydramnia
Amniocentesis no chromosome anomaly Prenatal steroid was given once.

Brief History
Elective C/S at 11:38 AM on 94/04/27. After birth: weak initial crying; HR:60~100 bpm; decreased
muscle tone; cyanosis Immediate ETT with positive pressure
ventilation HR>100bpm; muscle tone improved; skin color turned red
Apgar score: 4(1”)8(5”) OG insertion with drainage

Brief History PE: Scaphoid abdomen ; Decreased L’t breathing sound ;
Hypoactive bowel sound Lab: Micorbubble test: 11/mm2 ; moderate
Hb Hct MCV Plt PT PTT INR
13.8 40 105 320 14.5 51.4 1.3
ABG (on ventilator)
PH Pco2 Po2 HCO3 BE
7.332 41.8 105.6 22.2 -2.9

CxR

Ventilation

Echo
Brain echo:
R/o IVH, Gr.II, Left
Cavum septum pellucidum
Cardiac echo:
Mild TR
PFO

Pre-op evaluation PE: T/P/R: 37/115/40 BP: 65/45 mmHg Scaphoid abdomen ; Decreased L’t breathing sound ;
Hypoactive bowel sound Lab: Hb Hct MCV Plt PT PTT INR 13.8 40 105 320 14.5 51.4 1.3
ABG (on ventilator)
PH Pco2 Po2 HCO3 BE 7.332 41.8 105.6 22.2 -2.9

Pre-op evaluation
EKG: Probable RV hypertrophy Image:
CxR; Echo: as mentioned above Diagnosis:
Congenital diaphragmatic hernia with no other congenital anomaly

Anesthesia record
Ketamine 3 mg ( pre-medication) Esmeron 2 mg O2, air with isoflurane

Anesthesia record

IV:70mlpRBC:30 ml

Op on 04/28
A defect at left diaphragm, about 1*3cm was noted.
Bowel, stomach and spleen at thocacic cavity were pulled back into abdominal cavity.
Large bowel volvulus at ascending colon was noted. (360 degree, clockwise) After reduction of the volvulus, the color turned pink.
Prophylactive appendectomy was done.


CxR pre-op post-op

Post-op condition
Extubation on 05/02. Respiratory pattern was stable after
extubation. Transferred to 7A on 05/04

Discussion

Reference1. Lonnqvist PA. Major abdominal surgery of the neonate:
anesthetic considerations. Best Practice & Research. Clinical Anaesthesiology. 2004 ;18(2):321-42.
2. Liu LM. Neonatal surgical emergencies. Anesthesiology Clinical North America 2001; 19(2): 265-86.
3. Downard CD. Wilson JM. Current therapy of infants with congenital diaphragmatic hernia. Seminars in Neonatology. 2003; 8(3):215-21.

My Outline
1. Introduction of CDH
2. Current management of CDH
3. Anesthetic considerations in CDH

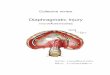
Introduction of CDH

Introduction of CDH
Incidence: about 1/2500 Etiology:
– Failure of the pleural and peritoneal canal to close at about GA 8 wk
– Herniation of the abdominal viscera into the thoracic cavity and pulmonary hypoplasia from compression by the viscera on the developing lungs
Cause: Unknown

Introduction of CDH Diaphragmatic defect: 3
types– Posterolateral
Bochdalek hernia: 80%, 左側五倍於右側 , size 最大
– Anterior Morgagni hernia: 2%
– Esophageal hiatus hernia: 18%

Introduction of CDH
Simple pathophysiology after herniation:– Compressionpulmonary hypoplasia – Dysfunction of the surfactant system– Increased muscularization of the intra-
acinar pulmonary arteriespulmonary hypertension
– In very severe cases, left ventricular hypoplasia is observed.

Introduction of CDH
Another idea:
failure of normal lung development?
(Iritani I. Anat Embryol 169:133–139, 1984)

Current Management of CDH
Prenatal diagnosis Prenatal treatment Perinatal treatment Operative treatment

Prenatal Diagnosis
Prenatal ultrasound: 59% detection rate, at average GA 24.2 wk
Predictors of outcome by prenatal ultrasound: Polyhydramnios, Intrathoracic stomach or liver, Abd circumference, lung-to-head ratio(LHR), lung/transverse thorax ratio
New predictors: PA diameter and LV mass (by fetal echocardiography), MRI lung volumetry
1/3 P’t have associated malformations: CV, GU, GI, CNS, chromosome anomalies

Prenatal Diagnosis
Other concern: At least once fetal echocardiogram Amniocentesis:
when chromosome anomalies is suspected

Prenatal Treatment
Antenatal steroid admistration?Van Tuyl M, Hosgor M, Tibboel D. Pediatr Res 2001;50:441–4.
Fetal surgery for CDH: fetoscopic placement of tracheal-occlusion devices

Perinatal Treatment
首先 :– Timing of delivery: close to term– Is C/S really necessary?
Betremieux P,et al. Prenat Diagn 2002;22:988–94
– Delivery of infants with CDH in an ECMO center Major concern:
– Pulmonary hypoplasia: Keep adequate ventilation– Pulmonary hypertension: honeymoon period

Perinatal Treatment
Fetal stabilization: Naso- or Oro-gastric tube: placed as soon as
possibledecompression ICU monitor: cross-match, CBC, electrolyte,
blood gas, CXR, head ultrasound(for IVHECMO), echocardiogram(for previously undetected cardiac anomalies, pulmonary hypertension)

Perinatal Treatment
Ventilation:– Permissive hypercapnea: gentle
ventilation– Avoidance of hyperventilation and
barotrauma– HFOV: controversy
Surfactant administration: controversyDownard CD. Wilson JM. Seminars in Neonatology. 2003; 8:215-21.

Perinatal Treatment
Indication of HFOV:– 使用傳統呼吸器無效者 – 肺部間質性肺氣腫
(Pulmonary interstitial emphysema)
– 氣胸 – 減少體外循環的機會 – 重度早產兒呼吸窘迫症 – 二氧化碳 (CO2) 移除 – 降低肺部壓力傷害 – 減少慢性肺部疾病

Perinatal Treatment
Inhaled NO: – Selective pulmonary vasodilator– 100hr honeymoon period of pulmonary
hypertension? PPHN?Charlton AJ,et al. Anaesthesia 1991; 46: 820–823
– iNO vs 100% O2: no differenceThe Neonatal Inhaled Nitric Oxide Study Group (NINOS). Pediatrics 1997;99:838–45
– Monitor PVR by heart echo initially!.
– Phosphodiesterase inhibitors: sildenafil, dypiridamole

Perinatal Treatment
Unable to stabilize P’t on reasonable ventilatory settings– pH >7.25 with peak inspiratory pressure
<30 cm H2O
– pre-ductal oxygen saturation >90% with FiO2<60%
iNO, HFOV, or ECMO

Operation
Honeymoon period:
delayed surgical intervention Synthetic patch, rotational muscle flaps Re-herniation

Key Points of Treatment
Adequate initial ventilation Keep attention to pulmonary
hypertension and RV function

Anesthetic Considerations in CDH
Pre-Oxygenation Induction Airway management Monitoring requirements Maintenance Regional blockade Pulmonary vasospasm Other modalities

Pre-Oxygenation
建議至少 oxygenation 60s Avoid high inflation pressure:
– Stomach in the chest– Lower Esophageal Sphincter
incompetence Induction 後 , 即便給純氧兩分鐘 , 約過
80~90s apnea 後 neonate 就會desaturation (SpO2<90%)
(Patel R, et al. Canadian Journal of Anaesthesia 1994; 41: 771–774.)

Induction
Larger dose for induction than adult– Thiopental (5~10mg/Kg):
hemodynamically stabe– Propofol (3~3.5mg/Kg): another choice– Ketamine (1~2mg/Kg): for
hemodynamically unstable patients– Atropine (0.02mg/Kg): prevent bradycardia
Rapid sequence induction if available N2O should be avoided!!

Airway Management
Succinylcholine:
Larger dose(3mg/kg), due to larger ECF volume
Non-depolarizing muscle relaxants: dose 不變 , onset 較成人快 , duration 較成人久

Monitoring Requirements
SpO2 in right hand and one of the feet:
Extrapulmonary R-L shunting Multi-lumen central venous line

Maintenance
Moderate-high doses of opioidhigher degree of hemodynamic stability
Fentanyl (15~25μg/kg)Liu LM. Anesthesiology Clinical North America 2001;19:265-86
Fentanyl (25~100μg/kg)Lonnqvist PA. Best Practice & Research.
Clinical Anaesthesiology. 2004 ;18:321-42

Regional Blockade
Caudal epidural block Ipsilateral T6~7 thoracic paravertebral
block Reduce dosage of opioid and muscle
relaxants

Anesthetic Considerations in CDHPulmonary Vasospasm
BP drop!!!– Interference with venous return?– Volume bolus and inotropic support: corrected?– Extrapulmonary R-L shunt: increasing gap of SpO2
between R’t hand and feet Management:
– Additional bolus of opioid, increase ventilation and FiO2
– Inhaled NO– After OP, the ventilation setting should be
elevated.

Other Modalites
Inhaled NO:
P’t should receive IVG ECMO:
full heparinization, watch for intra- or post-OP bleeding

Anesthetic Considerations in CDH
Preservation of spontaneous respiration or rapid sequence induction.
N2O should be avoided!
High dose of opoid Regional block is preferred Watch for episode of pulmonary
vasospasm IVG when NO is inhaled

Thank you for your attention