Embed Size (px)
Citation preview

Congresso Nazionale del
Cenacolo italiano diaudiovestibologia
Chieti 24 e 25 giugno 2016
Presidente del Congresso: Prof. Adelchi CROCEResponsabile Scientifico: Prof. Giampiero NeriDipartimento di Neuroscienze e ImagingUniversità degli Studi “G. d’Annunzio” - Chieti-Pescara
VERTIGINE EMICRANICA
Diagnosi e trattamento
Mario Faralli
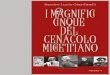
recurrent vestibular symptoms history of migraine temporal association between vestibular and migraine symptoms esclusion of other causes
Consensus document of the Barany Society and the International Headache society
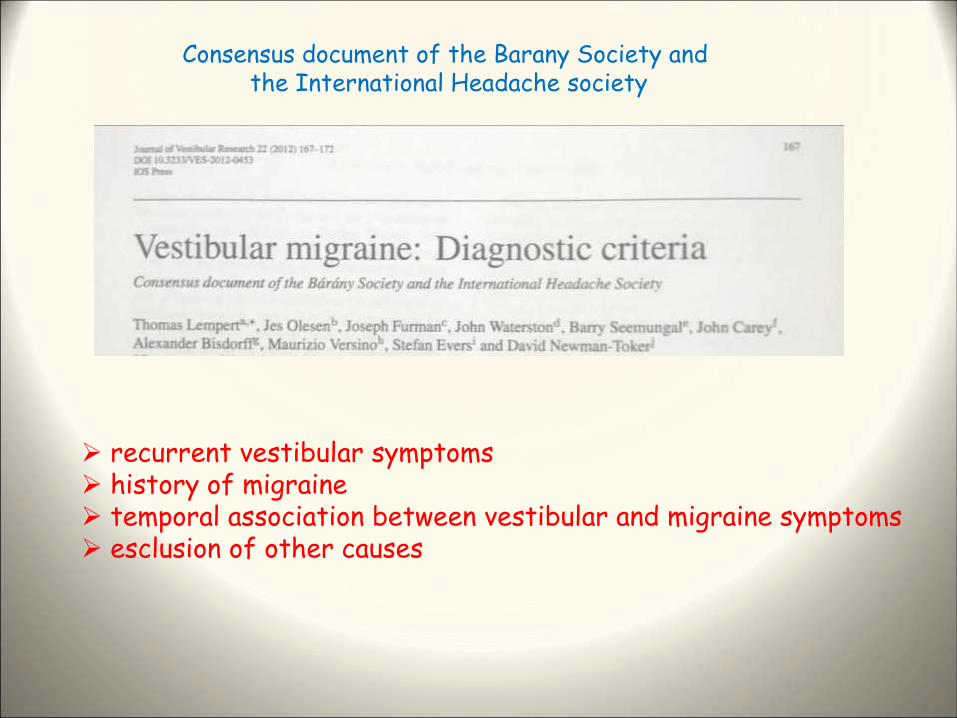
Vestibular symptoms
Spontaneous vertigo including
-Internal vertigo- external vertigo
positional vertigo
Visually-induced vertigo
head motion-induced vertigo
head motion-induced dizziness
Notes
Vestibular symptoms
rated moderate or severe
Duration of episode
highly variable
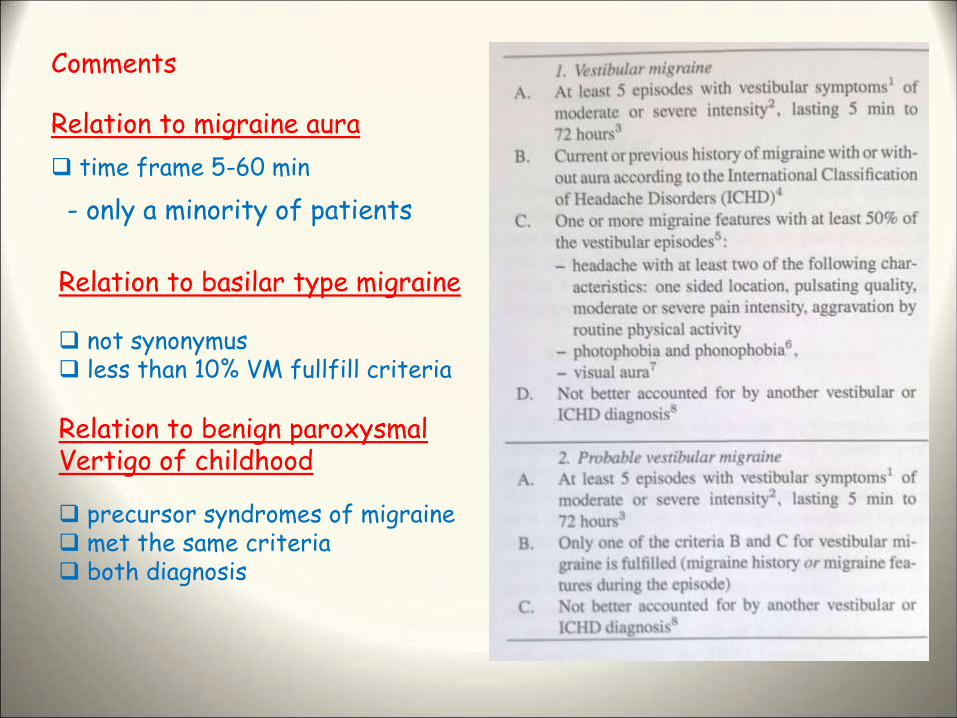
Relation to migraine aura
time frame 5-60 min
- only a minority of patients
Comments
Relation to basilar type migraine
not synonymus less than 10% VM fullfill criteria
precursor syndromes of migraine met the same criteria both diagnosis
Relation to benign paroxysmalVertigo of childhood
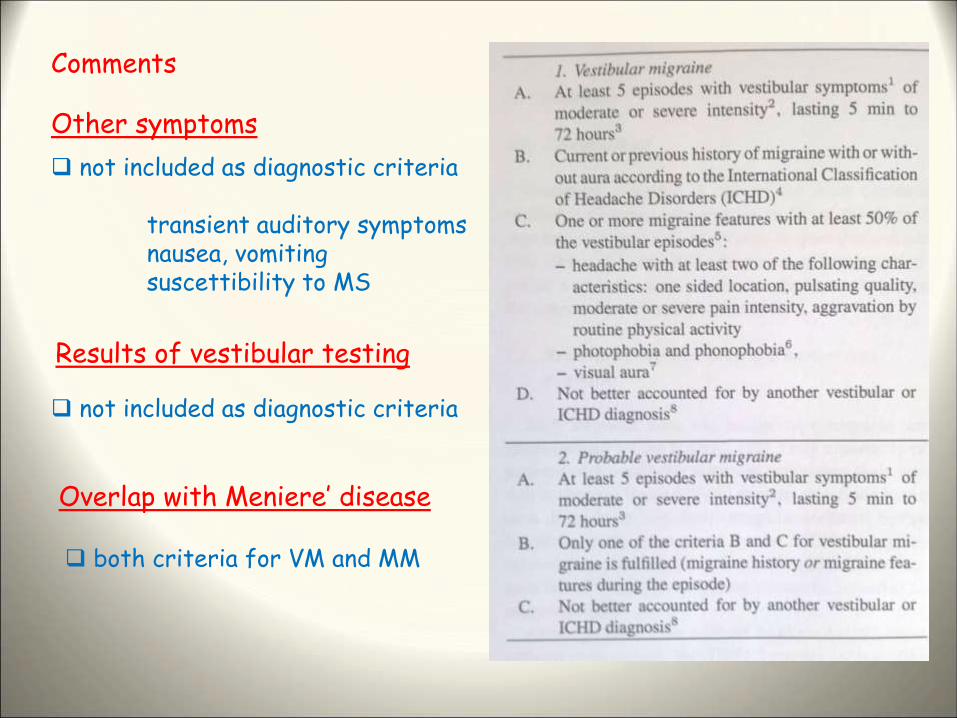
Other symptoms
not included as diagnostic criteria
transient auditory symptomsnausea, vomitingsuscettibility to MS
Comments
Results of vestibular testing
not included as diagnostic criteria
Overlap with Meniere’ disease
both criteria for VM and MM
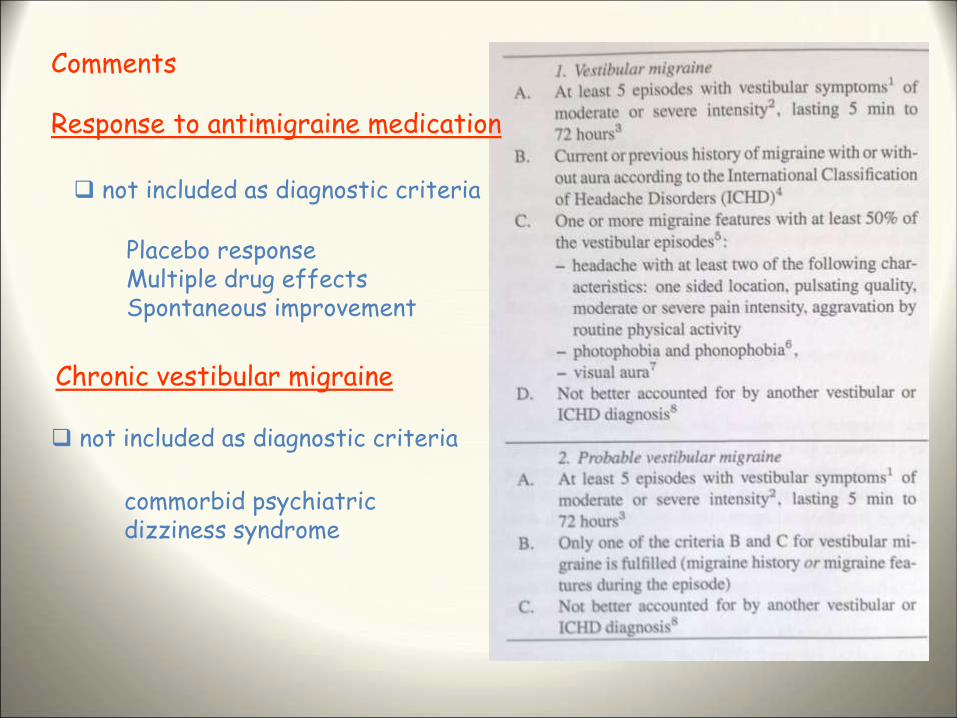
Response to antimigraine medication
commorbid psychiatricdizziness syndrome
Comments
Chronic vestibular migraine
not included as diagnostic criteria
not included as diagnostic criteria
Placebo responseMultiple drug effectsSpontaneous improvement
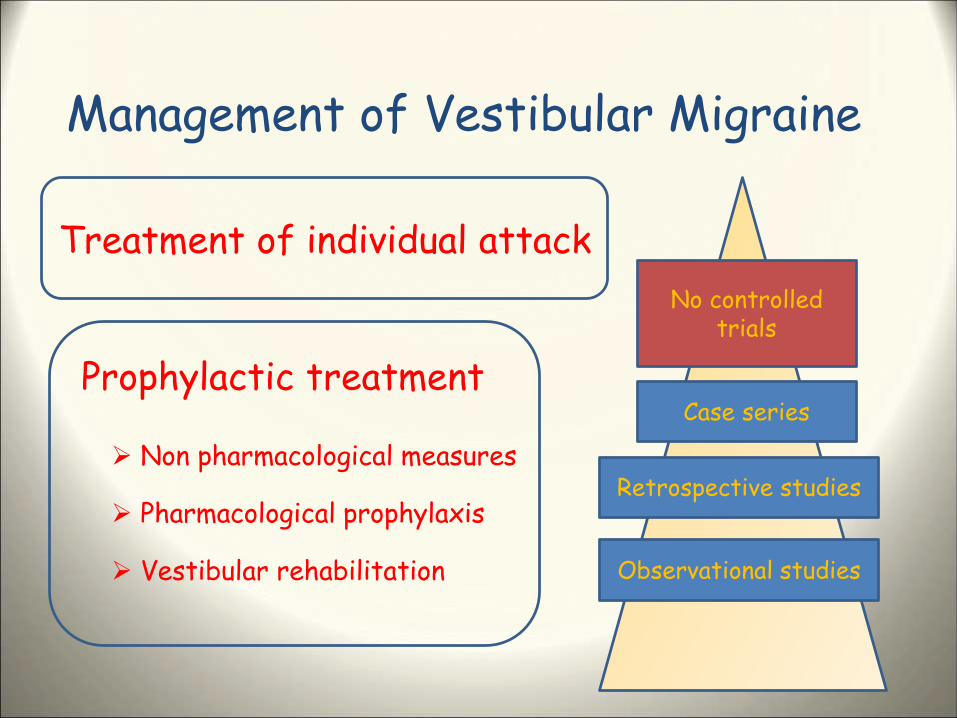
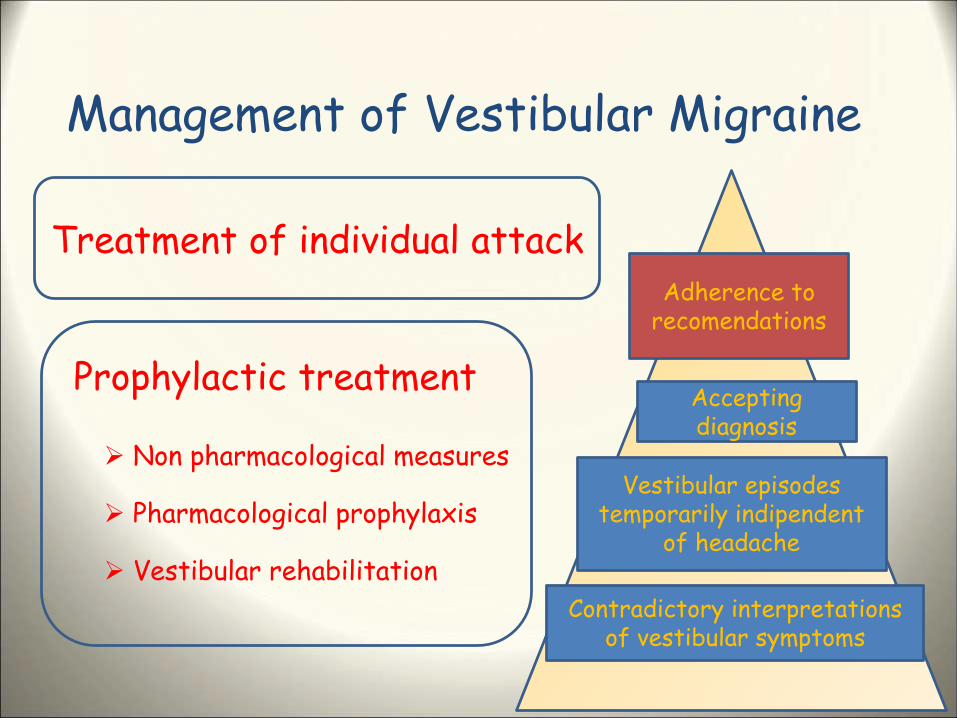
Management of Vestibular Migraine
Treatment of individual attack
Prophylactic treatment
Non pharmacological measures
Pharmacological prophylaxis
Vestibular rehabilitation
No controlledtrials
Case series
Retrospective studies
Observational studies
Management of Vestibular Migraine
Treatment of individual attack
Prophylactic treatment
Non pharmacological measures
Pharmacological prophylaxis
Vestibular rehabilitation
Adherence torecomendations
Acceptingdiagnosis
Vestibular episodestemporarily indipendent
of headache
Contradictory interpretationsof vestibular symptoms
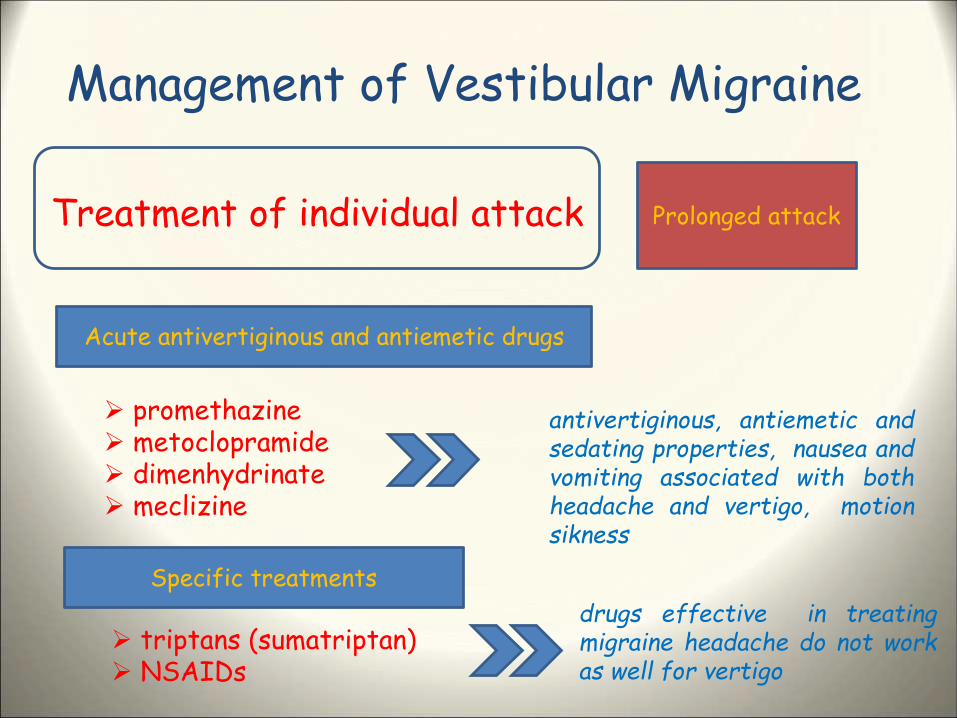
Management of Vestibular Migraine
Treatment of individual attack
promethazine metoclopramide dimenhydrinate meclizine
Prolonged attack
Acute antivertiginous and antiemetic drugs
Specific treatments
antivertiginous, antiemetic andsedating properties, nausea andvomiting associated with bothheadache and vertigo, motionsikness
triptans (sumatriptan) NSAIDs
drugs effective in treatingmigraine headache do not workas well for vertigo
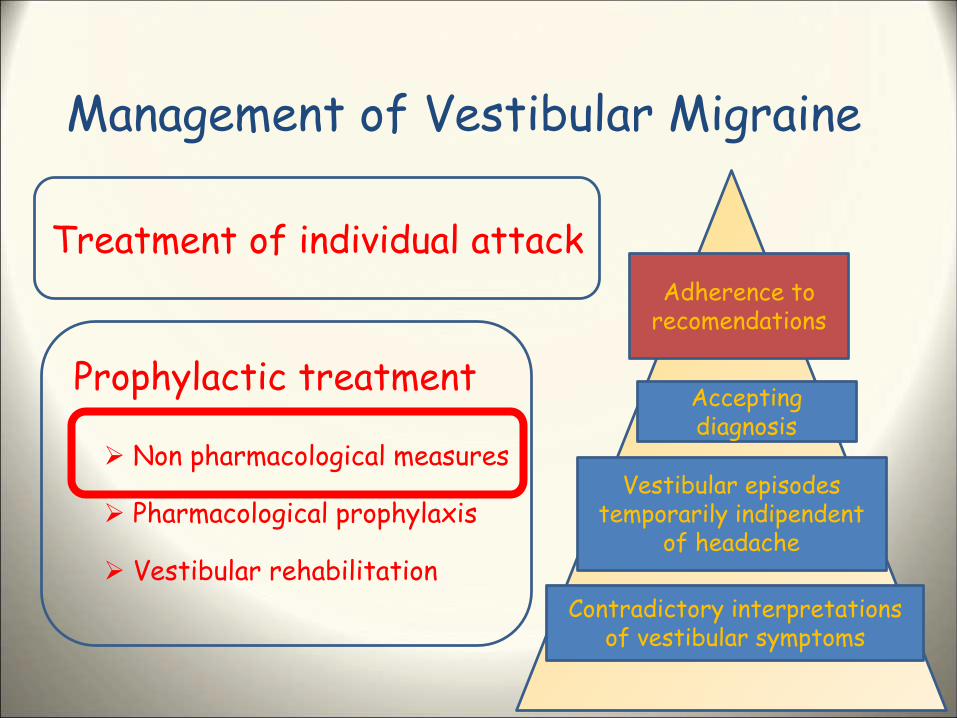
Management of Vestibular Migraine
Treatment of individual attack
Prophylactic treatment
Non pharmacological measures
Pharmacological prophylaxis
Vestibular rehabilitation
Adherence torecomendations
Acceptingdiagnosis
Vestibular episodestemporarily indipendent
of headache
Contradictory interpretationsof vestibular symptoms
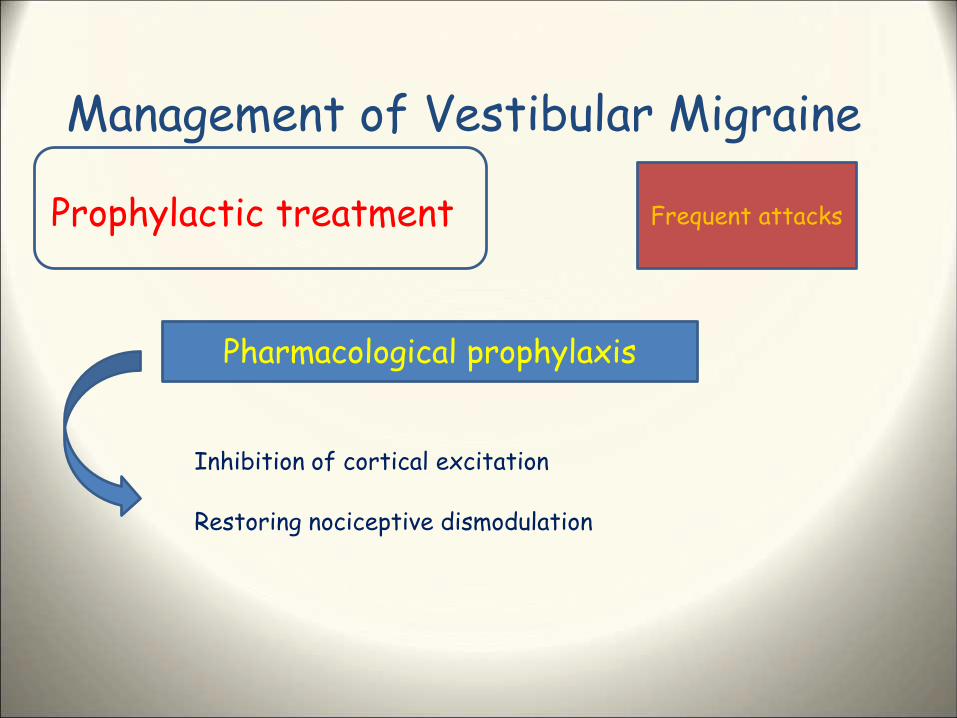
Management of Vestibular Migraine
Prophylactic treatment
Pharmacological prophylaxis
Frequent attacks
Inhibition of cortical excitation
Restoring nociceptive dismodulation
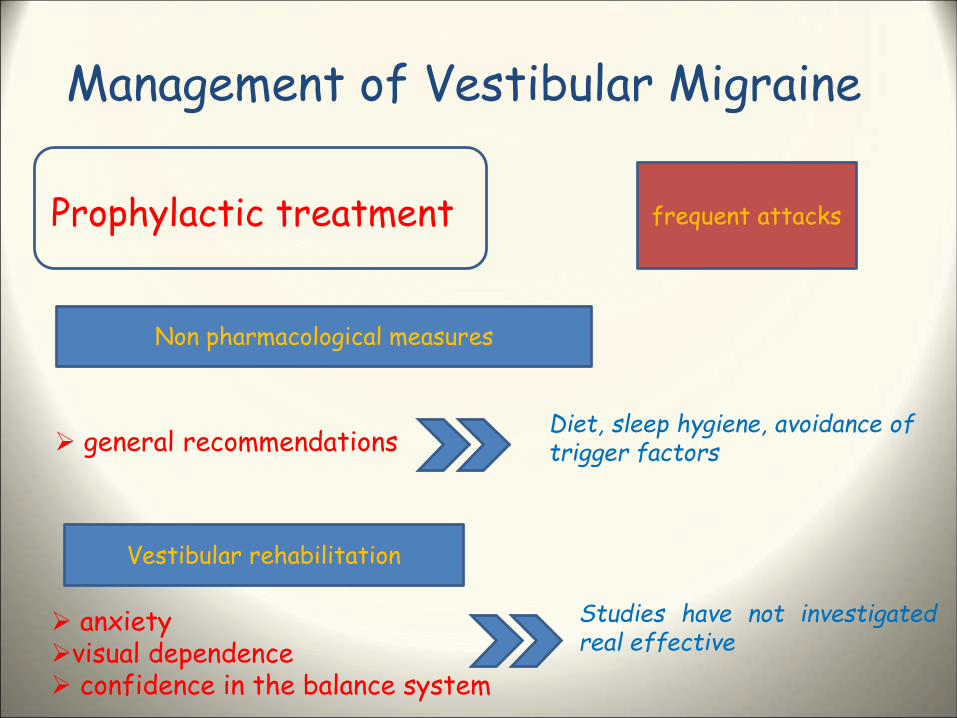
Management of Vestibular Migraine
Prophylactic treatment
general recommendations
frequent attacks
Non pharmacological measures
Vestibular rehabilitation
Diet, sleep hygiene, avoidance oftrigger factors
anxietyvisual dependence confidence in the balance system
Studies have not investigatedreal effective
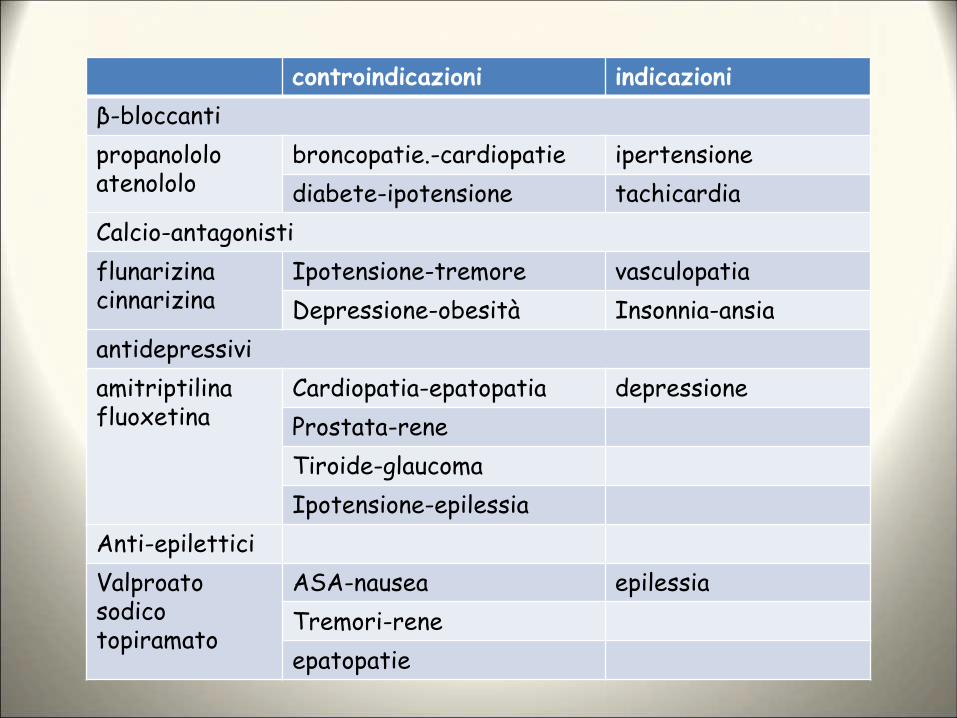
controindicazioni indicazioni
β-bloccanti
propanololoatenololo
broncopatie.-cardiopatie ipertensione
diabete-ipotensione tachicardia
Calcio-antagonisti
flunarizinacinnarizina
Ipotensione-tremore vasculopatia
Depressione-obesità Insonnia-ansia
antidepressivi
amitriptilinafluoxetina
Cardiopatia-epatopatia depressione
Prostata-rene
Tiroide-glaucoma
Ipotensione-epilessia
Anti-epilettici
Valproato sodicotopiramato
ASA-nausea epilessia
Tremori-rene
epatopatie
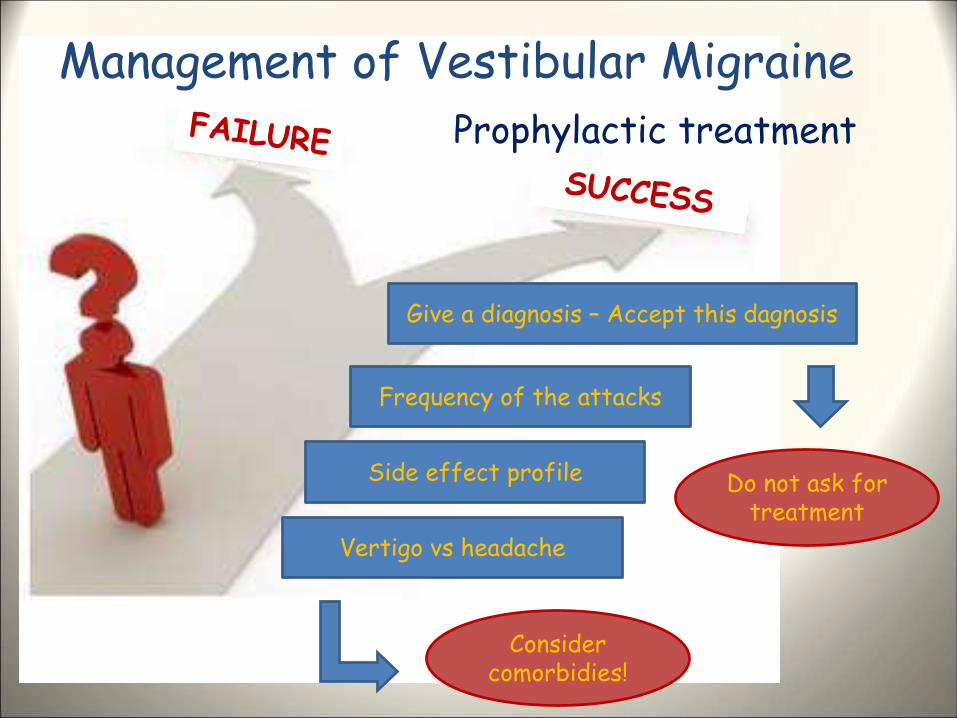
Give a diagnosis – Accept this dagnosis
Frequency of the attacks
Side effect profile
Considercomorbidies!
Management of Vestibular Migraine
Do not ask fortreatment
Prophylactic treatment
Vertigo vs headache
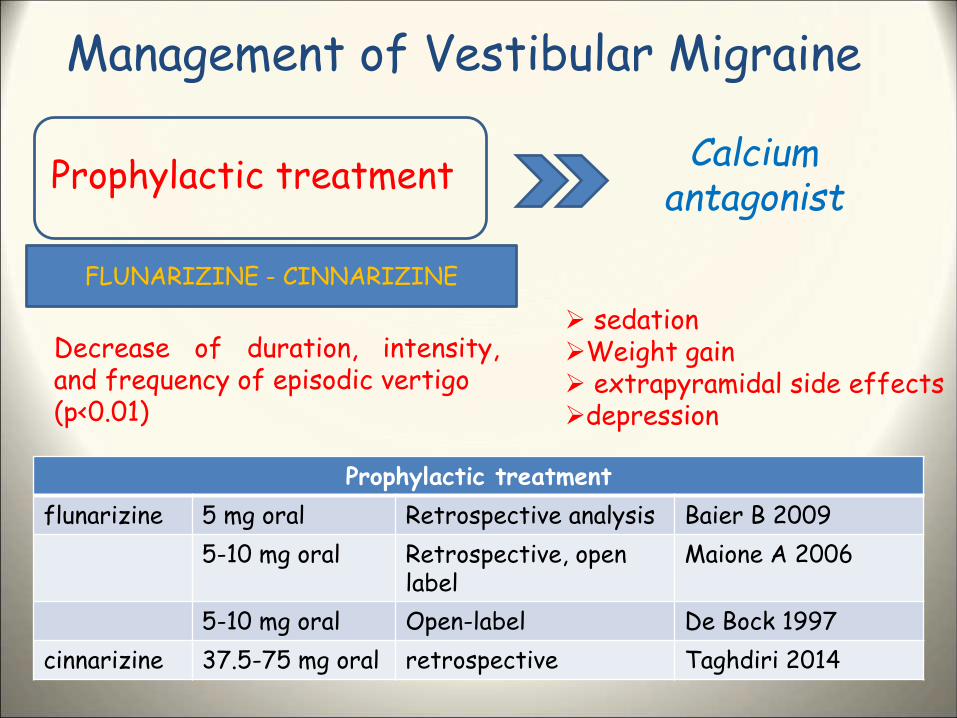
Management of Vestibular Migraine
Prophylactic treatment
FLUNARIZINE - CINNARIZINE
sedationWeight gain extrapyramidal side effectsdepression
Calcium antagonist
Prophylactic treatment
flunarizine 5 mg oral Retrospective analysis Baier B 2009
5-10 mg oral Retrospective, open label
Maione A 2006
5-10 mg oral Open-label De Bock 1997
cinnarizine 37.5-75 mg oral retrospective Taghdiri 2014
Decrease of duration, intensity,and frequency of episodic vertigo(p<0.01)
Management of Vestibular Migraine
Prophylactic treatmentCalcium
antagonist
randomized control trial 48 patients with Definitive MV 12 weeks duration 24 patients received 10 mg flunarizine daily + betahistine 16 mg 24 patients betahistine 16 mg daily flunarizine (10 mg) is effective on vestibular symptoms
Management of Vestibular Migraine
Prophylactic treatmentCalcium
antagonist
retrospective open lable 24 patients with VM and 16 patients with BM Assessement of V and H attacks after 1, 2 and three months mean frequency of V and H per months were significantly reduced after three months of cinnarizine therapy
Management of Vestibular Migraine
Prophylactic treatmentCalcium
antagonist
prospective study 22 patients with definite VM association of cinnarizine (20 mg) and dimenhydrinate (40mg) one tablet twice a day-1 month repeated three times (1 month interval) control group lifestyle measures main outcome: vertigo and headache episodes before and after treatment decrease of vertigo (5.3 to 2.1) and headache (4.3 to 1.7) decrease of vertigo (3.5 to 2.2) and headache (2.6 to 2)
Management of Vestibular Migraine
Prophylactic treatment
PROPRANOLOL- METOPROLOL
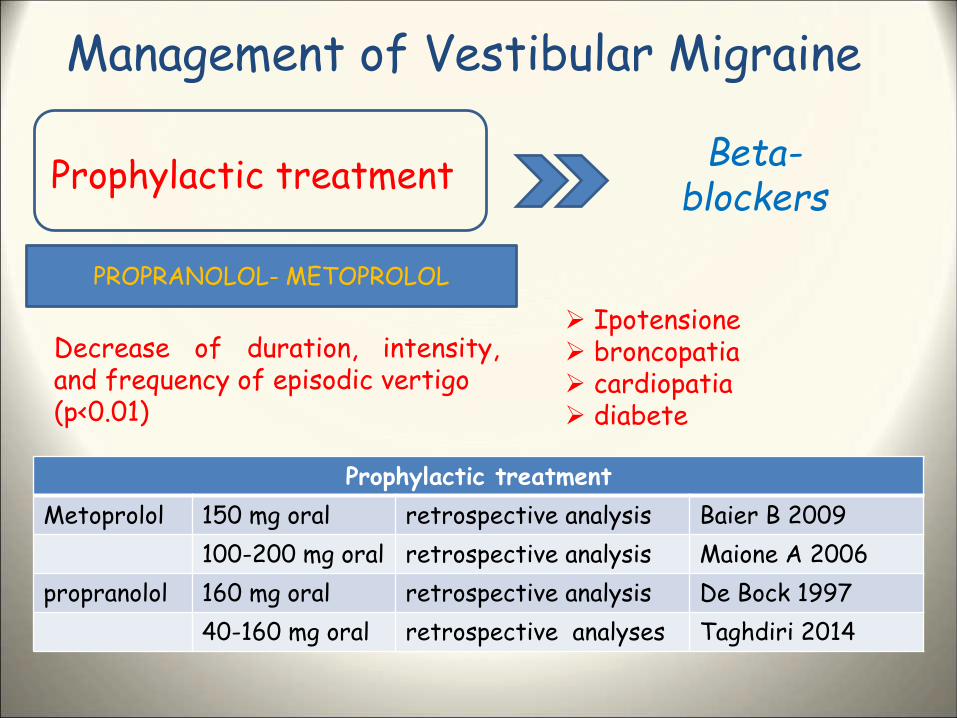
Ipotensione broncopatia cardiopatia diabete
Beta-blockers
Prophylactic treatment
Metoprolol 150 mg oral retrospective analysis Baier B 2009
100-200 mg oral retrospective analysis Maione A 2006
propranolol 160 mg oral retrospective analysis De Bock 1997
40-160 mg oral retrospective analyses Taghdiri 2014
Decrease of duration, intensity,and frequency of episodic vertigo(p<0.01)
Management of Vestibular Migraine
Prophylactic treatmentBeta-
blockers
prospective, randomized, controlled clinical trial 64 patients with definite VM group P (40-160mg daily); group V (37,5-150mg daily) outcomes: DHI, VSS, n° attacks, BAI and BDI (before-after 4 months DHI (P<.001), VSS (P<.001), n° attacks (p<.001) BAI significantly decreased in both groups BDI significantly decreased only in group V
Management of Vestibular Migraine
Prophylactic treatment
retrospective study 100 patients (median age 47, range 21-72 years) with D and P VM 74 patients with medical prophylaxis, 26 patients only lifestyle reccom. outcomes: duration, intensity and frequency of episodic vertigo outcomes: associated features all patients (MP) showed ↓ of duration, intensity and frequency of vertigo all patients (MP) showed ↓ of all associated features patients without MP showed only decrease of intensity of vertigo episode patients without MP showed only decrease of few associated features
Management of Vestibular Migraine
Prophylactic treatment
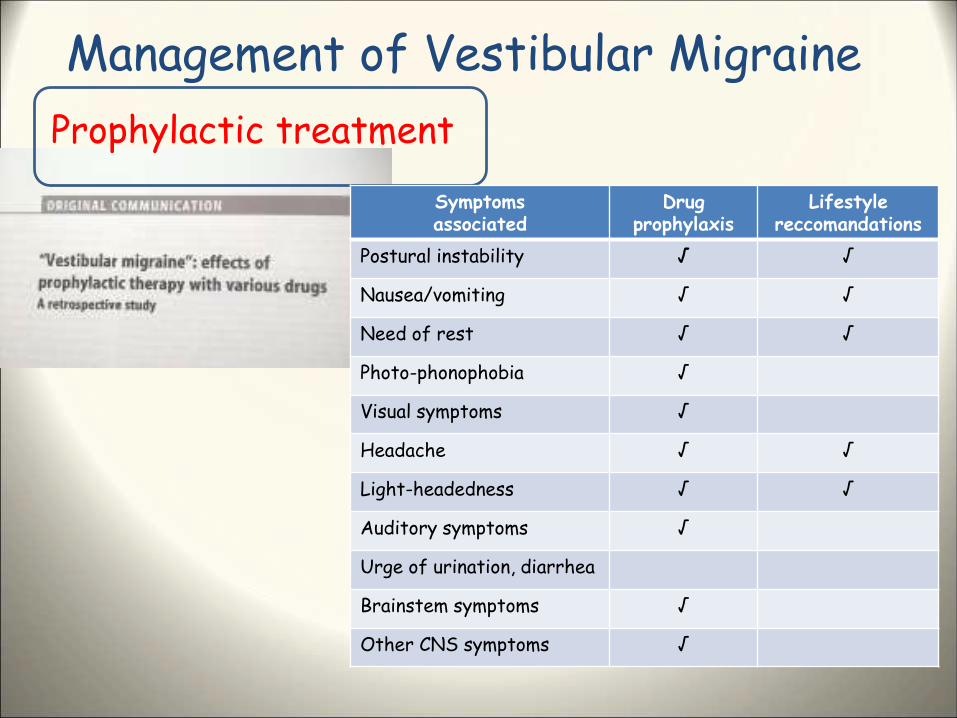
Symptomsassociated
Drugprophylaxis
Lifestylereccomandations
Postural instability √ √
Nausea/vomiting √ √
Need of rest √ √
Photo-phonophobia √
Visual symptoms √
Headache √ √
Light-headedness √ √
Auditory symptoms √
Urge of urination, diarrhea
Brainstem symptoms √
Other CNS symptoms √
Management of Vestibular Migraine
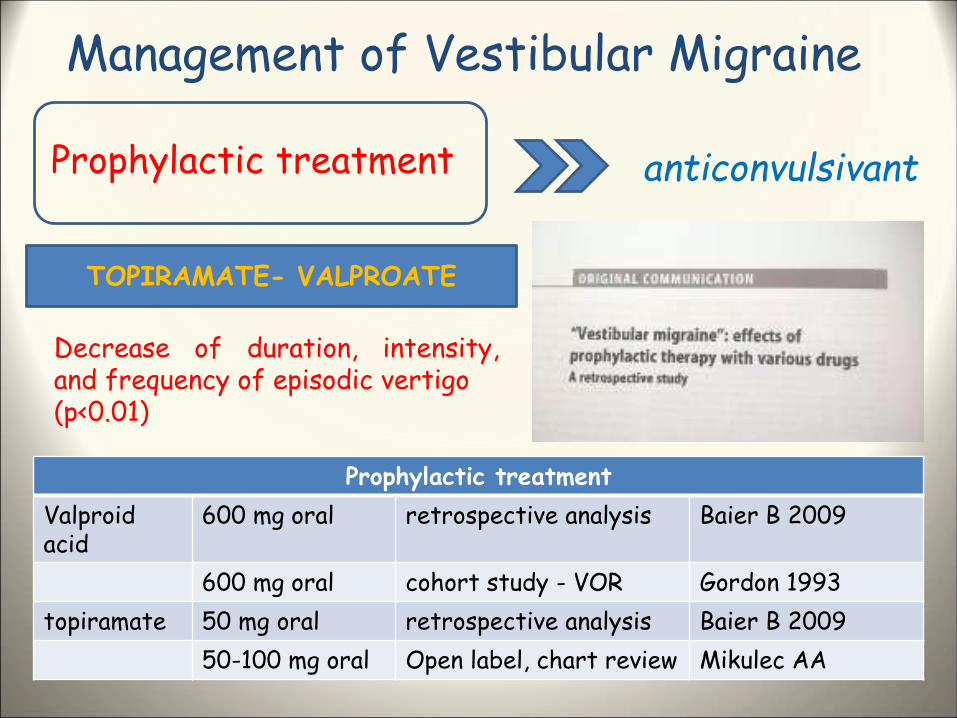
Prophylactic treatment anticonvulsivant
TOPIRAMATE- VALPROATE
Decrease of duration, intensity,and frequency of episodic vertigo(p<0.01)
Prophylactic treatment
Valproidacid
600 mg oral retrospective analysis Baier B 2009
600 mg oral cohort study - VOR Gordon 1993
topiramate 50 mg oral retrospective analysis Baier B 2009
50-100 mg oral Open label, chart review Mikulec AA
Management of Vestibular Migraine
Prophylactic treatment anticonvulsivant
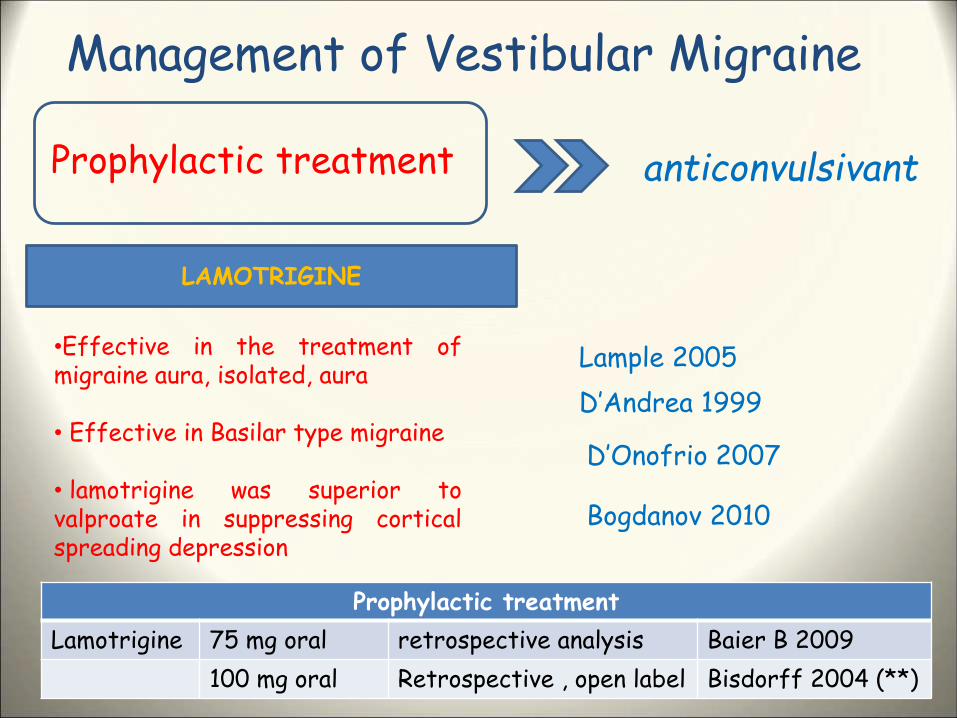
LAMOTRIGINE
•Effective in the treatment ofmigraine aura, isolated, aura
• Effective in Basilar type migraine
• lamotrigine was superior tovalproate in suppressing corticalspreading depression
Prophylactic treatment
Lamotrigine 75 mg oral retrospective analysis Baier B 2009
100 mg oral Retrospective , open label Bisdorff 2004 (**)
Lample 2005
Bogdanov 2010
D’Andrea 1999
D’Onofrio 2007
Management of Vestibular Migraine
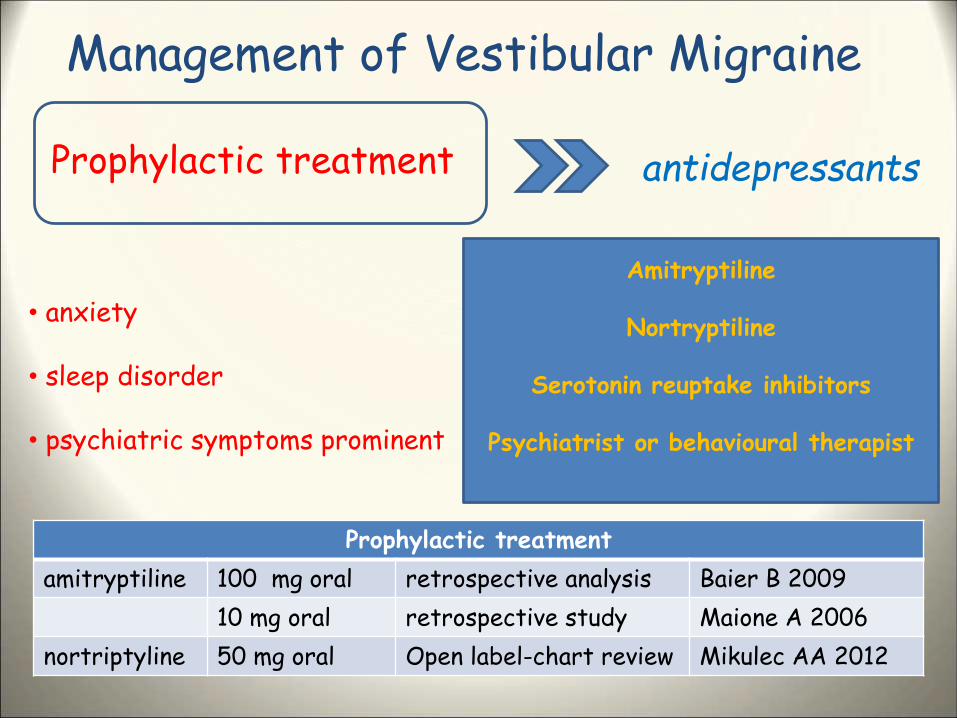
Prophylactic treatment antidepressants
• anxiety
• sleep disorder
• psychiatric symptoms prominent
Amitryptiline
Nortryptiline
Serotonin reuptake inhibitors
Psychiatrist or behavioural therapist
Prophylactic treatment
amitryptiline 100 mg oral retrospective analysis Baier B 2009
10 mg oral retrospective study Maione A 2006
nortriptyline 50 mg oral Open label-chart review Mikulec AA 2012
Management of Vestibular Migraine
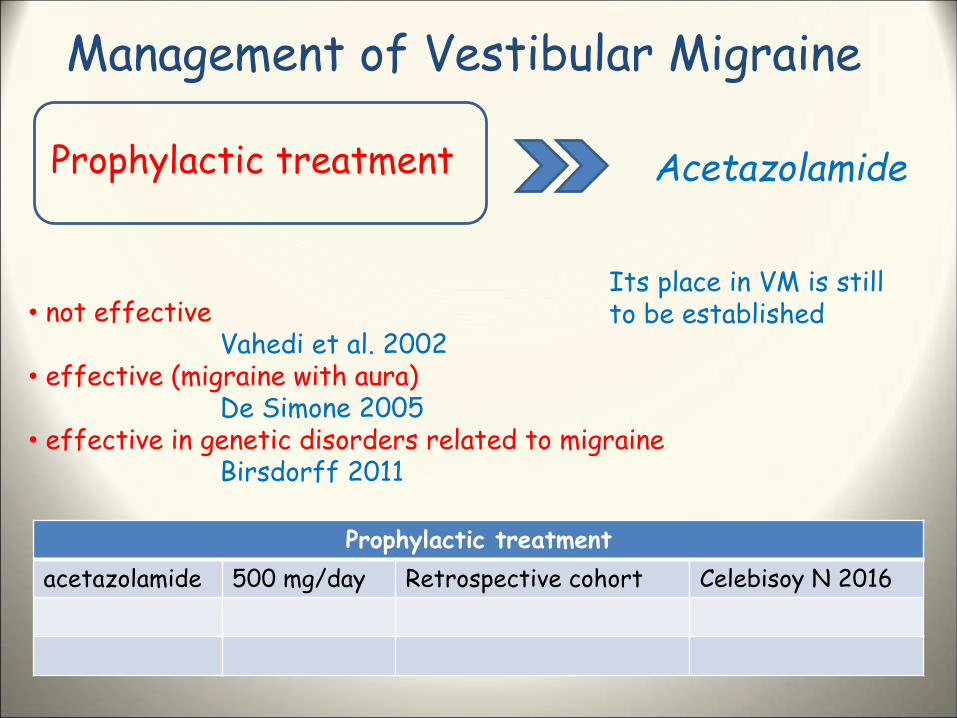
Prophylactic treatment Acetazolamide
• not effectiveVahedi et al. 2002
• effective (migraine with aura)De Simone 2005
• effective in genetic disorders related to migraineBirsdorff 2011
Prophylactic treatment
acetazolamide 500 mg/day Retrospective cohort Celebisoy N 2016
Its place in VM is stillto be established
Management of Vestibular Migraine
Prophylactic treatment Acetazolamide
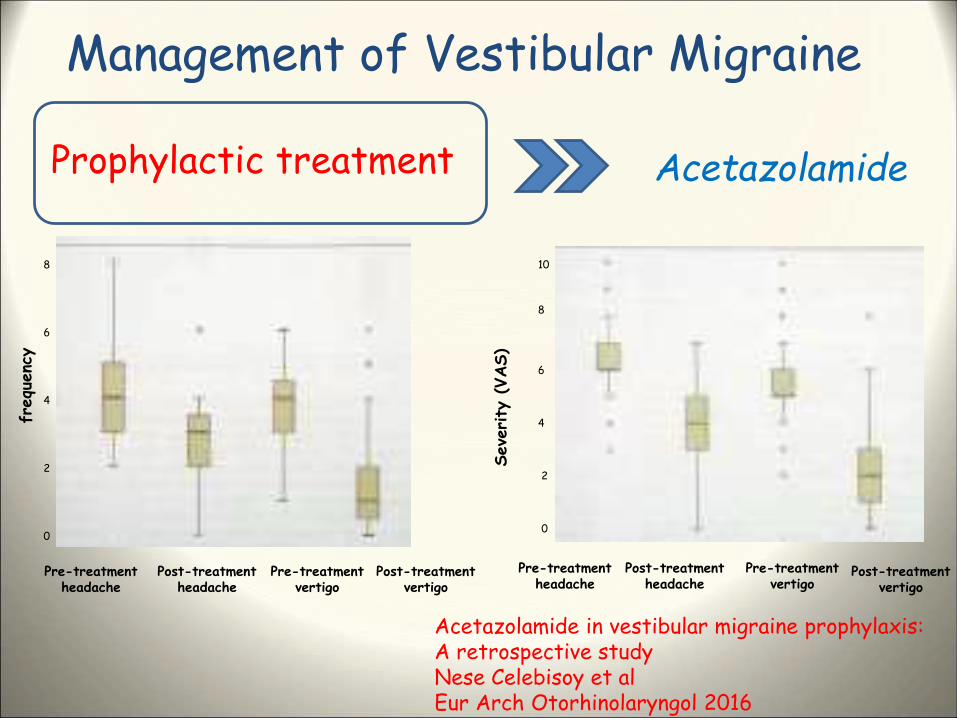
Acetazolamide in vestibular migraine prophylaxis:A retrospective studyNese Celebisoy et alEur Arch Otorhinolaryngol 2016
retrospective study 39 patients 500 mg/day acetazolamide outcomes: intensity (vas) and frequency (n°) of vertigo attacks evaluation after three months treatment
Management of Vestibular Migraine
Prophylactic treatment Acetazolamide
Pre-treatmentheadache
Pre-treatmentvertigo
Post-treatmentvertigo
Post-treatmentheadache
0
2
4
6
8
frequ
enc
y
Seve
rity
(VAS)
Pre-treatmentheadache
Post-treatmentheadache
Pre-treatmentvertigo
Post-treatmentvertigo
0
2
4
6
8
10
Acetazolamide in vestibular migraine prophylaxis:A retrospective studyNese Celebisoy et alEur Arch Otorhinolaryngol 2016
Management of Vestibular Migraine
Prophylactic treatment Meniere’s disease or migraine associated vertigo?
A trial with prophylactic drug treatment for migraine might be suggestedIn patients with clear symptoms of migraine and recurrent cocleovestibulardisorders
Management of Vestibular Migraine
Prophylactic treatment Meniere’s disease and Migraine
data support a proactive role for cinnarizine in preventing vertigo spells,especially in MD patients with migraine.
decrease in vertigo spells from 9.4 to 3.8 (MD with migraine) decrease in vertigo spells from 6.8 to 5.9 (MD without migraine)
Management of Vestibular Migraine
Vestibular rehabilitation Physiotherapy
retrospective case series 14 patients with (MRV) physical therapy exercise program (mean visits:4.9; mean duration: 4 months outcome measures (DHI, DGI, ABC) before and after treatment
Improvement in physical performance measures and self-percievedabilities
Management of Vestibular Migraine
Vestibular rehabilitation Physiotherapy
anxiety visual dependence chronic dizziness
Furman et al. 2005
Management of Vestibular Migraine
treatment recommendations for VM are similar to those for migraine with or without aurea
Some reccomandations are based on the authors experience
Anamnestic factors are rilevant for diagnosis
Anamnestic factors and functional aspects in the selection of patientswith migrainous vertigoFaralli et al.Eur Arch Othorhinolaryngol (2010) 267; 1157-1162






![[Una vertigine ma non solo una vertigine!!!!!] Dr. ssa Lidia Catarzi Dr. Gianni Taccetti Ictus tra territorio ed ospedale](https://img.pdfslide.tips/doc/110x75/5542eb59497959361e8c4bfc/una-vertigine-ma-non-solo-una-vertigine-dr-ssa-lidia-catarzi-dr-gianni-taccetti-ictus-tra-territorio-ed-ospedale.jpg)