Embed Size (px)
Citation preview

CASE REPORT
Cowden's Disease Diagnosed through Mucocutaneous Lesionsand Gastrointestinal Polyposis with Recurrent Hematochezia,
Unrevealed by Initial DiagnosisMasako Kato, Akira Mizuki, Tatsuhiko Hayashi, Takamu Kunihiro, Hiroshi Nagata, Nobuhiro Tsukada,
Hideki Orikasa* and Shojiroh Morinaga*
Abstract
A 51-year-old man was admitted to our hospital becauseof hematochezia and painful keratotic plaques involvingboth hands. He had gastrointestinal polyposis, and a his-tory of liver hemangiomas and thyroid tumor. Numerouspapules on the face and papillomatosis on the oral mucosawere present. A diagnosis was madeas a typical case ofCowden's disease according to the criteria proposed bySalem and Steck (J AmAcad Dermatol 8: 686, 1983). Thepatient was not correctly diagnosed initially in spite of typi-cal manifestations of Cowden's disease, mainly due to hisconcomitant manifestations which occurred chronologi-cally.
(Internal Medicine 39: 559-563, 2000)
Key words: multiple hamartoma syndrome, thyroid tumor,liver hemangioma
Introduction
Cowden's disease inherited in an autosomal dominant modeis associated with high susceptibility to diverse tumors, benignor malignant ( 1). It is also called multiple hamartoma syndrome;the disease is characterized by multiple hamartomas and neo-plasms of ectodermal, endodermal, and mesodermal origin af-fecting many different organ systems, including multiple mu-cocutaneous hamartomas, fibrocystic disease and cancer of thebreast, nontoxic goiter, thyroid cancer, and hamartomatouspolyps of the stomach, small intestine, and colon (1, 2). It isimportant to recognize Cowden'sdisease, which leads to earlydetection of malignant tumors. This report describes a casewhich had not been diagnosed as Cowden's disease for a longtime because each disorder was thought to be independent de-spite typical manifestations.
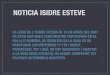
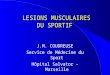
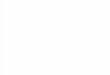
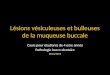
Case ReportA 51-year-old man was admitted to our hospital because ofrepeated visible hematochezia and painful keratotic plaquesinvolving both hands. At the age of 40, he developed multiplepapules on his face and extremities, but did not seek medicalattention. When he was 43, polypectomy was performed sev-eral times for recurrent bleedings from rectal polyps. Eight yearsearlier, excision of thyroid tumor (details unknown) and sub-sequent tracheotomy for bilateral recurrent nerve paralysis wereperformed in another hospital. He had a history of appendec-tomy and cholecystectomy as well. He was a homeless personand his memorywas vague so we could not get any informa-tion regarding his family history.On physical examination, a number of skin-coloured plaqueswere found on his face (Fig. 1) and around the ears. Numeroussmall plaques on the lips and a number of pinpoint papules onthe oral mucosaand tongue could be seen. Healso had kera-totic plaques, 1-5 mmin diameter, on his extremities (Fig. 2).There was a surgical varicosity in his left groin.Laboratory tests, including peripheral blood count, bloodchemistry and thyroid function were almost within normal lim-its despite recurrent hematochezia (Table 1 ). There were giantplatelets in the peripheral blood count, but bleeding time andcoagulation time were within normal limits. An increased num-ber of megakaryocytes were present in the bone marrow. Therewere no symptomsor signs of disseminated intravascular co-agulation or thrombotic thrombocytopenia purpura. Upper gas-trointestinal endoscopy and colonoscopy revealed multiplepolyposis from all around the oral mucosa to the duodenumand from the rectum (Fig. 3B) to the descending colon. Mostprominent were whitish flat elevations over the total area ofthe esophagus (Fig. 3A). Histopathological examination ofpolyps showed glycogenic acanthosis in the esophagus (Fig.4A), and hyperplasia seen in the stomach and colon (Fig. 4B).But none of them were found to be malignant. Abdominalul-trasonography revealed multiple hemangiomas in the liver. The
From the Department of Internal Medicine and *the Department of Pathology, Tokyo Saiseikai Central Hospital, TokyoReceived for publication July 5, 1999; Accepted for publication February 7, 2000Reprint requests should be addressed to Dr. Nobuhiro Tsukada, the Department of Internal Medicine, Tokyo Saiseikai Central Hospital, 1-4- 17, Mita, Minato-
ku, Tokyo 108-0073
Internal Medicine Vol. 39, No. 7 (July 2000) 559

Kato et al
Figure 1. A number of skin-coloured plaques on the fore-head.
Figure 2. Keratotic plaques on the hand.
Table 1. Laboratory DataH e m a to lo g y B l o o d c h e m i s t r y
R e d b l o o d c e l l 3 8 4 x l O 4 / u l S o d iu m 1 4 1 m E q / /H e m o g l o b i n 1 2 . 4 g / d l P ot a s s iu m 3 . 4 m E q //H e m a t o c r i t 3 6 . 5 % C h lo rid e 1 0 5 m E q / /P l a t e l e t 1 3 9 . O x 1 0 3 / u l G lu c o se 7 9 m g / d lW h i t e b l o o d c e l l 4 , 1 0 0 / u l C R P 0 . 3 m g /d l
S e g m e n t 7 1 . 0 % B l oo d ur e a ni t r og e n 32 m g / d lB a n d 3 .C C re a tin in e 0 . 6 m g /d l
L y m p h o c y t e 1 3 . 0 % To ta l p ro te in 6. 9 g/d lM o n o c y t e 1 0 . 0 % A sp a r t at e am i n ot r a n sf e r as e 3 5 IU / ZE o s in o p h il A l an i n e am i n o t ra n s f e ra s e 3 4 I U/ /B a so p h i1 1 .0 % L a c t a te d e h y d r o g e n a s e 52 3 I U / /
M e tam y e lo c y te A l k al i n e ph o s p h a ta s e 1 87 IU //
R e t i c u l o c y t e ¥ l % cP r o t h r o m b i n t i m e 1 0 . 9 s e c o n d s B l o o d h o r m o n eA c t iv a t e d p a r ti a l th r o m bo p l a st i n ti m e 3 4. 4 se c o n d s T S H 8. 3 u U /u l
F re e -T 3 2 .47 pg /ji l
F re e -T 4 1 .0 3 n g/ nl
TSH: thyroid stimulating hormone, T3: triiodothyronine, T4: thyroxine.
bronchoscope inserted through a hole of tracheotomy showedmultiple polyps on the trachea.Thus, a diagnosis of Cowden's disease was established onthe basis of gastrointestinal polyposis and characteristic mu-cocutaneous lesions.
Discussion
In the initial case report, Cowden's disease was character-ized by the presence of mucocutaneous hamartomas (2). Thediagnostic criteria, proposed by Salem and Steck, were basedon the dermatological point of view (3). The hallmark of thedisease is the presence of multiple facial trichilemmomas, which
arise from the follicular epithelium and typically occur aroundthe eyes, nose, and mouth. Mucocutaneouslesions were ob-served in almost all cases (4). Although not mentioned in theearly reports, hamartomatous polyps of the gastrointestinal tracthave been described (1). Since the first report by Lloyd andDennis in 1963 (2), over 150 case reports have been publishedin English (5). Although the gastrointestinal tract has been ex-amined in only a fourth of reported cases, approximately 35%of affected patients exhibit gastrointestinal polyps, includingthe esophagus (3). In Japan, to our best knowledge, 93 cases,in total, of Cowden's disease, including our case were pub-lished (6-28). The incidence of gastrointestinal polyp by le-sions is esophagus 65.6%, stomach 75%, duodenum 36.5%,
560 Internal Medicine Vol. 39, No. 7 (July 2000)

Cowden's Disease Unrevealed by Initial Diagnosis
A
B
Figure 3. Endoscopic view showing multiple polyposis onthe esophagus (A) and rectum (B).
A
B
Figure 4. Histopathological examination of the polyps showedglycogenic acanthosis in the esophagus (A) and prominentstroma, compatible with juvenile polyps in the rectum (B) (HEstain, A: x75, B: xl50).
and colon 65.6%, respectively. A number of different types ofhamartomas occur, including lipomas, juvenile polyps, inflam-matory polyps, ganglioneuromas, and lymphoid hyperplasia(29). Pathologically, hyperplastic polyp is most common.Esophageal lesions composedof glycogenic acanthosis, arecharacteristic of Cowden's disease (5). They are helpful in dis-tinguishing Cowden's disease from other polypous diseases.
There are descriptions that breast cancer, nontoxic goiter, thy-roid cancer, and a variety of soft tissue and visceral tumors,including hemangiomas, lipomas, lymphangiomas, neurofibro-mas, uterine leiomas, and meningiomas, were complicated (30).A potential risk of malignancy seems to be great in associa-tion with this disease. In fact, adenocarcinoma of the colonoccasionally supervenes. Of the 93 cases in Japan, 12 werebreast cancer (12.9%), 9 were colon cancer (9.6%),4 were thy-roid cancer (4.3%), and 17 were other carcinomas (18%). Thus,42 out of 93 cases (45%) among which 8 were double or triplecancers were found to be complicated with malignancy. Be-sides gastrointestinal lesions, hemangioma was observed in 17cases (18%), among which 5 were seen in the liver. Concomi-tant symptomswerealso seen such as cataracta, varices andfibromas showing various outcomes. Our patient had a historyof removal of thyroid tumor, liver hemangiomas, and develop-ment of characteristic mucocutaneouslesions. In addition,
Internal Medicine Vol. 39, No. 7 (July 2000) 561

Kato et al
multiple tracheal polyps were present. A literature searchyielded no reports of tracheal polyp in Cowden's disease.Mucocutaneouslesions maybe present on the face or ex-tremities when the patients are born (3 1). Mostly, however,this condition was noticed whenthe patients are in their twen-ties (the average age was 26.9 in Japanese literature includingour case). Generally mucocutaneouslesions went unnoticedwhen the patients were young. In a report of a patient with acomplication of stomach carcinoma, it was described that mu-cocutaneous lesions had once decreased after gastrectomy, butdeveloped again as liver metastasis occurred. That suggestedthat the mucocutaneouslesion represented paraneoplastic der-matosis (31).
Ten out of 93 cases were first diagnosed asymptomatic gas-trointestinal polyposis during health examinations performedwhen the patients were in their thirties. But 9, including ourcase, suffered from hematochezia, due to gastrointestinal ero-sion or hemorrhagic polyp. It was difficult to determine theorder of the appearance concerning this disease, but there wasa tendency that first gastrointestinal polyposis and then muco-cutaneous lesions were diagnosed rather than the opposite se-quence in literature reference. There was only one case reportconcerning a teenager, a 16-year-old man in Japan. He hadmucocutaneous lesions on his face but no symptomson hisextremities or oral mucosa. He also had polyps which werelocated in the stomach, duodenum, sigmoid colon, and rectum(6). All cases that we had checked in Japanese literature in-cluded mucocutaneous lesions. It seems that gastrointestinallesions like polyps appear at the early stage similar to mucocu-taneous lesions. Out of the 93 cases, 52 had abnormalities ofthe thyroid gland which were mostly adenomatous goiter andwere diagnosed in their thirties (mean age was 27.5).A chronological sequence of symptomsof our case was asfollows: at the age of 18 years, appendicitis and cholecystec-tomy; 20 years, varices; 40 years, mucocutaneous lesions; 43years, hematochezia, polyposis and thyroid tumor. He was ahomeless person who could not rememberin detail. The factthat cholecystectomy was performed whenhe was 1 8, suggestedhe had already had some symptom of Cowden's disease. Outof 93 cases in Japan, 7 patients had gallbladder polyp orcholelithiasis.
There was no description in the literature on the relation-ship between giant platelets and Cowden's disease, thus fur-ther investigation is necessary. Manycases likely are undiag-nosed because skin papules and gastrointestinal polyps, the mostcommonmanifestations, are often unnoticed. If gastrointesti-nal polyposis with mucocutaneous lesions is encountered, apossible diagnosis of Cowden's disease should never be over-looked, because of its high risk of malignancy.The underlying biological mechanism in this disease is yetunknown. Familial occurrence has been observed and it isthought to be a multisystem disease complex inherited in anautosomal dominant manner ( 1 ). Recently, it was reported thatthe mutational abrogation of the tumor suppressor gene, namely,phosphatase and tensin homolog deleted on chromosometen/mutated in multiple advanced cancers (PTEN/MMAC1 ) plays
a causal role in the genesis of gastrointestinal polyps inCowden's disease (32). Wefound these mutations of the PTENgene on 10 q in the present case and the details will be reportedalong with another case. Finally, we would like to repeat theimportance of identifying Cowden's disease as it leads to peri-odic medical examination of all affected persons for malig-nancies.
References
1) Weinstock JV, Kawanishi H. Gastrointestinal polyposis with orocutaneoushamartomas (Cowden's disease). Gastroenterology 74: 890-895, 1978.
2) Lloyd KM, Dennis M. Cowden's disease. A possible new symptom com-plex with multiple system involvement. Ann Intern Med58: 136-142,
1963.
3) Salem OS, Steck WD. Cowden's disease (multiple hamartoma and neo-plasia syndrome). A case report and review of the English literature. JAm Acad Dermatol 8: 686-696, 1983.
4) Case records of the Massachusetts General Hospital. Weekly clinicopatho-logical exercises. Case 24-1987. A 56-year-old man with a substernalgoiter, multiple cutaneous and mucosal lesions, and a positive stool testfor occult blood. N Engl J Med 316: 1531-1540, 1987.
5) Kay PS, Soetikno RM, Mindelzun R, Young HS. Diffuse esophageal gly-cogenic acanthosis: an endoscopic marker of Cowden's disease. AmJGastroenterol 92: 1038-1040, 1997.
6) Sumioka M, Watanabe C, Yamada H, et al. Two cases of Cowden's dis-ease. Nippon Shokakibyo Gakkai Zasshi 91: 2219-2224, 1994 (in Japa-
nese).
7) Nakamura Y, Kinoshita M, Yabune H, Yukawa S. A case report ofCowden's disease with squamous cell carcinoma in papillomatous tonsil.Nippon Shokakibyo Gakkai Zasshi 95: 436-440, 1998 (in Japanese).
8) Kitazoe K, Hosijima Y, Aoki H, et al. A case of Cowden's disease associ-ated with rectal carcinoid. Nippon Shokakibyo Gakkai Zasshi 95: 1244-1248, 1998 (in Japanese).
9) Itakura S, Miyoshi E, Aoki S, et al. An autopsy case ofCowden's diseasewith variegated lesions. Rinsho Shokaki Naika 12 (9): 1373-1378, 1997(in Japanese).
10) Yano S, Atsuta T, Watanabe F, et al. Acase ofCowden's disease accom-panied by hamartoma of the liver and rectal cancer. Nippon ShokakigekaGakkai Zasshi 30: 779-783, 1997 (in Japanese, Abstract in English).
ll) Nemoto K, Oda H, Kanemura M, Yokoyama M, Onishi Y, Oohara K.Cowden's disease associated with intrapelvic arterio-venous malforma-tion and right renal tumor. Rinsho Hinyokika 51: 586-588, 1997 (in Japa-nese, Abstract in English).
12) Inagaki T, Ebisuno S. A case of Cowden's disease accompanied by pros-tatic cancer. Iryo 50: 228-232, 1996 (in Japanese, Abstract in English).
13) Kobayashi M, Kurachi K, Inoue C, Seo Y, Doi K. Acae ofCowden'sdisease associated with colon cancer and gastrointestinal polyposis. Hifu(Skin Research) 38: 243-248, 1996 (in Japanese, Abstract in English).
14) Kaneko M, Saiki M, Yokobayashi T, Sode Y, Usui T, Saida T. A case ofCowden's disease accompanied by verruciform xanthoma. Rinsho Hifu49: 840-842, 1995 (in Japanese).
15) Nakazaki T, Kimino K, Tobinaga K, Taketomi K, Nakasone T, KishikawaM. A case of Cowden's disease accompanied with bilateral breast can-cers, colon cancer and gastrointestinal polyposis. Nippon Rinsho GekaiGakkai Zasshi 56: 1972-1976, 1995 (in Japanese).
16) Takahashi M, Umeki K, Harada K, Sugiyama S. A case of Cowden'sdisease. Rinsho Hifu 49: 736-738, 1995 (in Japanese).
17) Suzuki M, Kato H, Yaoita H, Yoshida Y, Kasano T, Kimura K. Acase ofCowden's disease. Rinsho Hifu 49: 60-63, 1995 (in Japanese).
18) Inoue T, Hibi T, Hayashi A, et al. A case ofCowden's disease withouttypical skin eruptions. Gastroenterol Endosc 37 (1): 65-71, 1995 (in Japa-nese, Abstract in English).
19) Fujita K, Yoshida K, Kitamura C, et al. A case ofCowden's disease asso-ciated with inflammatory fibroid polyp. Gastroenterol Endosc 37 (4) : 800-
562 Internal Medicine Vol. 39, No. 7 (July 2000)

Cowden's Disease Unrevealed by Initial Diagnosis804, 1995 (in Japanese, Abstract in English).
20) Kirizuka K, Nishizaki H, Tani M, Nishigami T, Harada H. A case ofCowden's disease. Kobe Shiritsu Shimin Byoin Kiyo 33: 97-101, 1995(in Japanese, Abstract in English).
21) Yamamoto Y, Higaki Y, Kawashima M. Cowden's disease. HifubyouShinryo 16: 1029-1032, 1994 (in Japanese).
22) Iwabe C, Shindo H, Hayashi N, Kazama Y, Komatsu T, Nagasako K. Acase of Cowden'sdisease with pelvic arteriovenous malformations.Gastroenterol Endosc 36: 1237-1242, 1994 (in Japanese, Abstract in
English).
23) Takao Y, Hirata I, Murano S, et al. A case ofCowden's disease accompa-nied with colon cancer and gastrointestinal polyposis. GastroenterolEndosc 36: 1433-1438, 1994 (in Japanese, Abstract in English).
24) Endoh K, Yokoyama Y, Itoh M, Takeuchi T. Cowden's disease associatedwith lung cancer. I to Cho (Stomach and Intestine) 29: 1417-1421, 1994(in Japanese, Abstract in English).
25) Segawa M, Hirono T, Fujita H, et al. A typical case of Cowden's disease.Nippon Rinsho Gekai Gakkai Zasshi 55: 2405-2409, 1994 (in Japanese,Abstract in English).
26) Nishiyama N, Yano T, Yamamoto S, et al. A case of multiple hamartomasyndrome (Cowden's disease). Nishinihon Hifu 56: 450-457, 1994 (inJapanese, Abstract in English).
27) Yokota M, Matsuba S, Tsuji T. A case of Cowden's disease. Rinsho Hifu46: 471-473, 1992 (in Japanese).
28) Seta T, Kyoi M, Yoshimitsu K, Miwa U, Ooya T. A case of Cowden'sdisease accompanied with primary hyperparathyroidism. Horumon toRinsho 35: 164-166, 1987 (in Japanese).
29) Haggitt RC, Reid BJ. Hereditary gastrointestinal polyposis syndromes.Am J Surg Pathol 10: 871-887, 1986.
30) Burt RW, Jacoby RF. Polyposis syndromes, in: Textbook of Gastroenter-ology. 3rd ed. Yamada T, Alpers DH, Laine L, Owyang C, Powell DW,Eds. Lippincott Williams & Wilkins, Philadelphia, New York, Baltimore,
1999: 1995-2022.
31) Kosaka M, Ishiguro N, Higaki Y, Kawashima M, Hidano A, Oochi T. Acase of Cowden's disease. Rinsho Hifu 44: 197-201, 1990 (in Japanese).
32) Chi SG, Kim HJ, Park BJ, et al. Mutational abrogation of the PTEN/MMAC1gene in gastrointestinal polyps in patients with Cowden dis-ease. Gastroenterology 115: 1084-1089, 1998.
Internal Medicine Vol. 39, No. 7 (July 2000) 563