Embed Size (px)
Citation preview

CRPC雄激素通路治疗进展
何志嵩

The Effect of Castration, of Estrogen, and of Androgen Injection on Serun Phosphatase in Metastatic Carcinoma of the Prostate
Huggins C, Hodges CV. Cancer Res. 1941;1:293-297.60
40
20
040 50 60 70
Uni
ts p
er 1
00 m
L Se
rum
Time (Days)
Stilbestrol, 1 mg daily
Acid Phosphatase
Alkaline Phosphatase
前列腺癌雄激素去除治疗(ADT)的历史

转移性前列腺癌雄ADT效果:SWOG9346
轻度转移 广泛转移
N Engl J Med. 2013 Apr 4;368(14):1314-25.

前列腺癌的疾病进程
Mayo Clin Proc. 2015 Dec;90(12):1719-33.
CRPC是前列腺癌患者的主要致死因素

CRPC的定义
2016 EAU1
• 血清睾酮达去势水平*• 且以下条件满足一项即可:
− 生化进展:相隔一周, 连续3次PSA上升, 较最低值升高50%以上,且 PSA >2 ng/ml− 影像学进展:骨扫描发现≥ 2个骨病灶或RECIST(实体瘤疗效评价)评估软组织病灶增大
注:仅仅症状的进展不足以诊断CRPC
2015 AUA2
• 血清睾酮达去势水平*• PSA 升高幅度超过最低值 25%,升高值大于2ng/mL, ≥3周进行二次确认
1.EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Eur Urol. 2016 Aug 31. pii S0302-2838(16)30469-9.2. Castration-Resistant Prostate Cancer: AUA Guideline Amendment 2015. J Urol. 2016 May;195(5)1444-52.3. 2014年中国前列腺癌诊断治疗指南.
* 睾酮水平 <50ng/dL 或 <1.7nmol/L
2014 CUA3
• 血清睾酮达去势水平*• 相隔一周, 连续3次PSA上升, 较最低值升高50%以上

下丘脑
垂体
肾上腺
睾丸 雄激素(雄烯二酮、睾酮)
备选配体雄激素应答细胞
突变体
微管
联合因子
雄激素应答基因
转录激活(如,TMPRSS2 : ERG、PSA)
雄激素信号轴
Attard G et al. Clin Cancer Res 2011;17:1649-1657
去势治疗(ADT)

早期CRPC的治疗
双侧肾上腺切除及垂体照射 抗雄治疗
氟他胺Flutamide

早期的抗雄治疗未提供生存获益
PCTC meta-analysis .Lancet 2000, 355; 9214:1491-1498
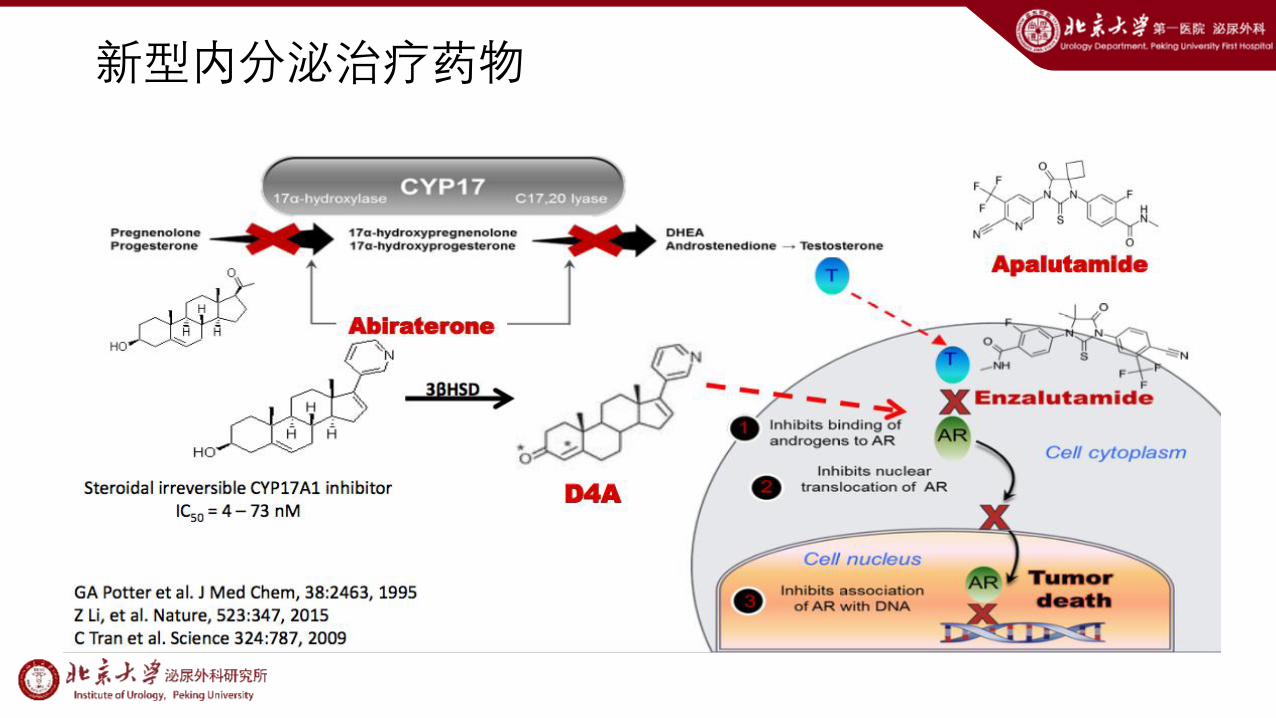
新型内分泌治疗药物

Dharia et al. Biol Report 2004; 71:83-88
睾丸、肾上腺以及产生雄激素的前列腺肿瘤组织均可表达
CYP17,CPY-17是雄激素产生的关键酶之一
阿比特龙作用机制

• 恩杂鲁胺可以抑制–雄激素与雄激素受体结合–抑制雄激素及其受体向细胞核移位–抑制雄激素与雄激素受体识别并结合DNA序列
• 没有AR激动效应
恩杂鲁胺作用机制

阿帕鲁胺作用机制
directly binds to the LBD of AR with high affinity, inhibiting its nuclear import and DNA binding capacity. 1) greater antitumor activity at a lower dose
and exposure than MDV3100; 2) steady-state levels of ARN-509 are 2- to 4-
fold lower than MDV3100 at equivalent doses, whereas intratumoral levels are equivalent, indicative of a higher tumor/plasma ratio for ARN-509;
3) brain levels of ARN-509 are 4-fold lower than MDV3100, suggesting a reduced risk of seizure activity.
Cancer Res. 2012 Mar 15;72(6):1494-503.

FOR INTERNAL PURPOSES ONLY
新型抗雄药物的优势:Enzalutamide vs Bicalutamide
• Shore ND et al. Lancet Oncol. 2016;17:153-63.

转移性CRPC生存获益的治疗
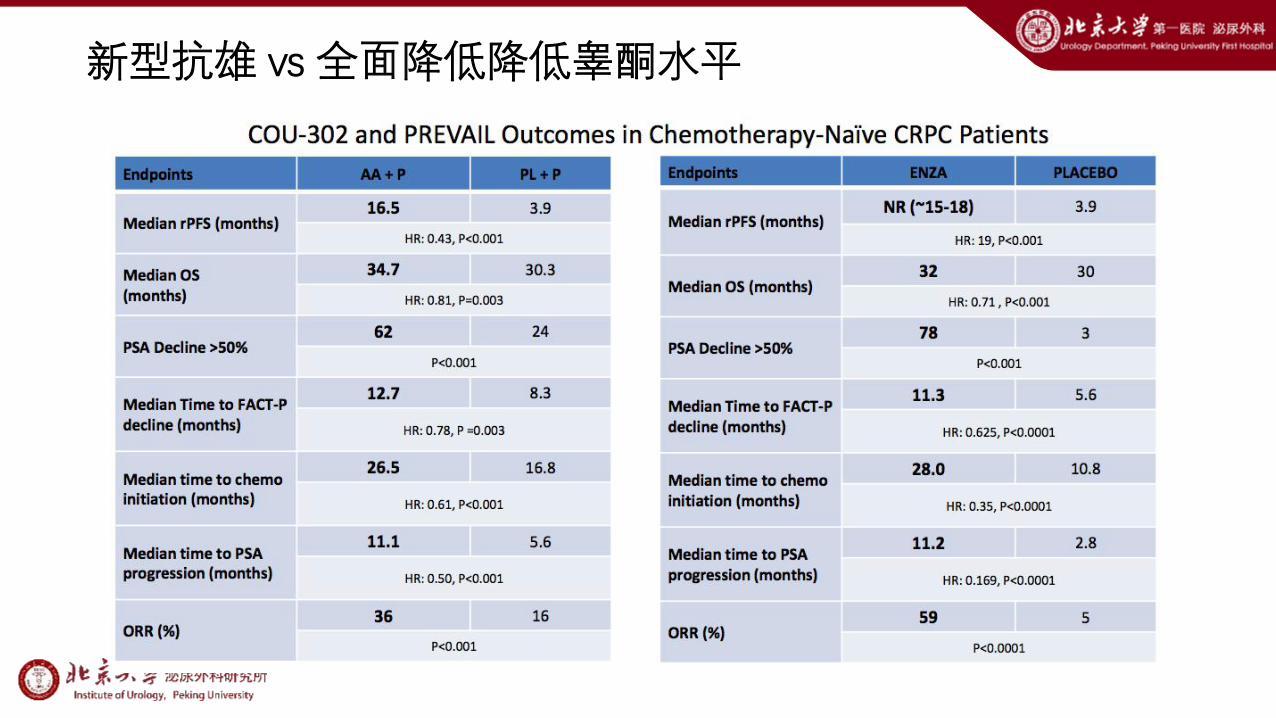
新型抗雄 vs 全面降低降低睾酮水平

抗雄与降低睾酮水平序贯
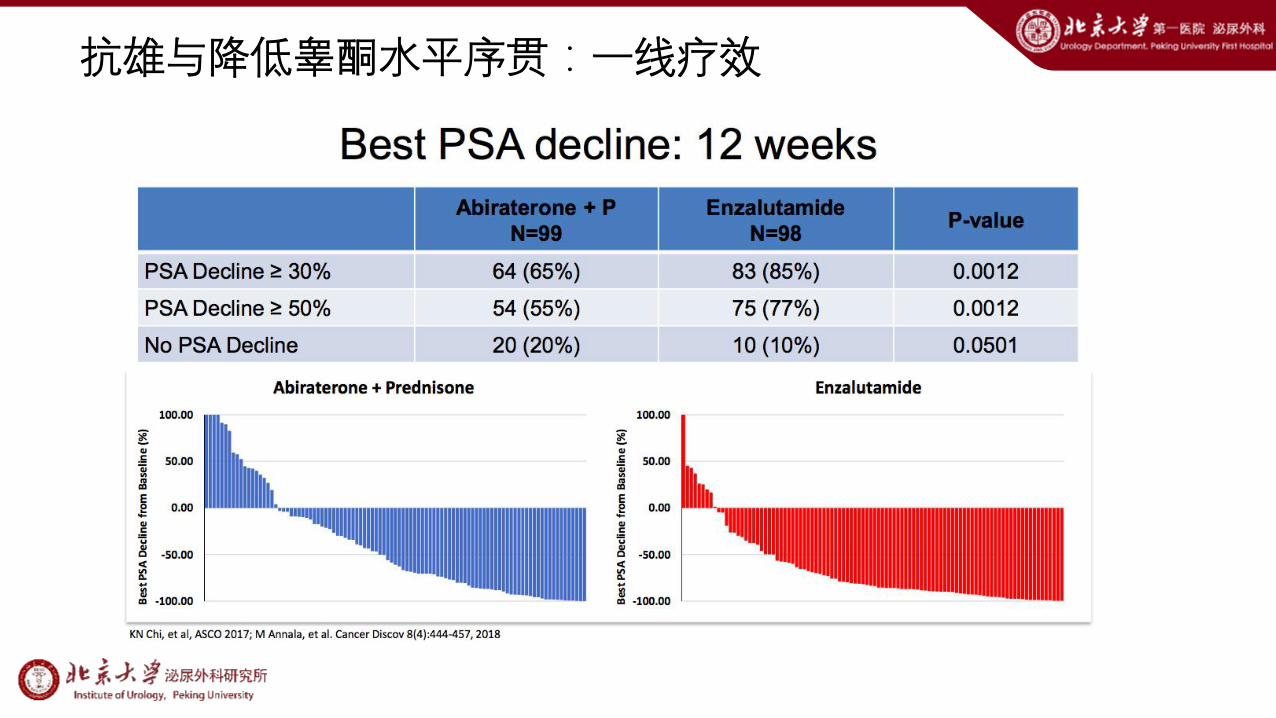
抗雄与降低睾酮水平序贯:一线疗效

抗雄与降低睾酮水平序贯:一线疗效
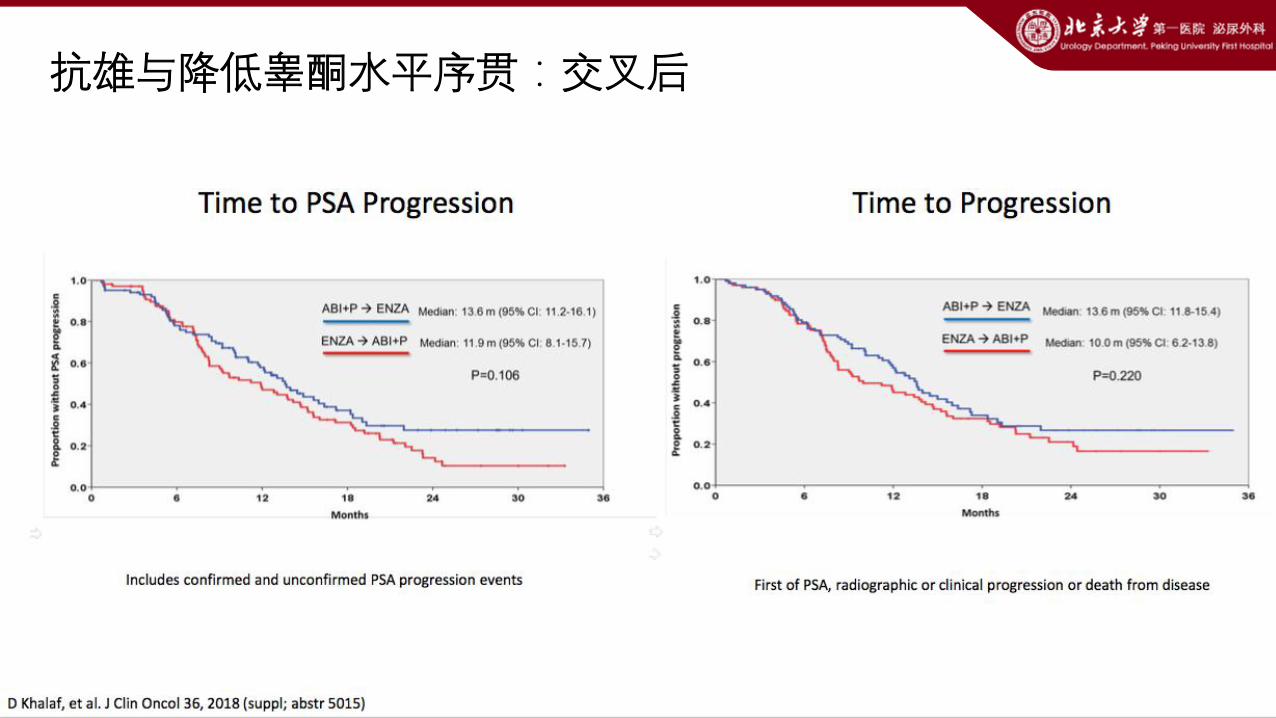
抗雄与降低睾酮水平序贯:交叉后

抗雄与降低睾酮水平序贯:总生存

抗雄与降低睾酮水平序贯:安全性

J Clin Oncol 24:190-205.

• PROSPER:III期随机、对照、双盲研究(NCT02003924)
• 目的:评估恩杂鲁胺(160mg)治疗M0 CRPC的疗效
• 入组:M0 CRPC and PSA-DT≤10 mo and PSA≥2ng/ml (N=1401,2:1分为ENZA+ADT/PBO+ADT)
• 主要终点:MFS
• 次要终点:OS
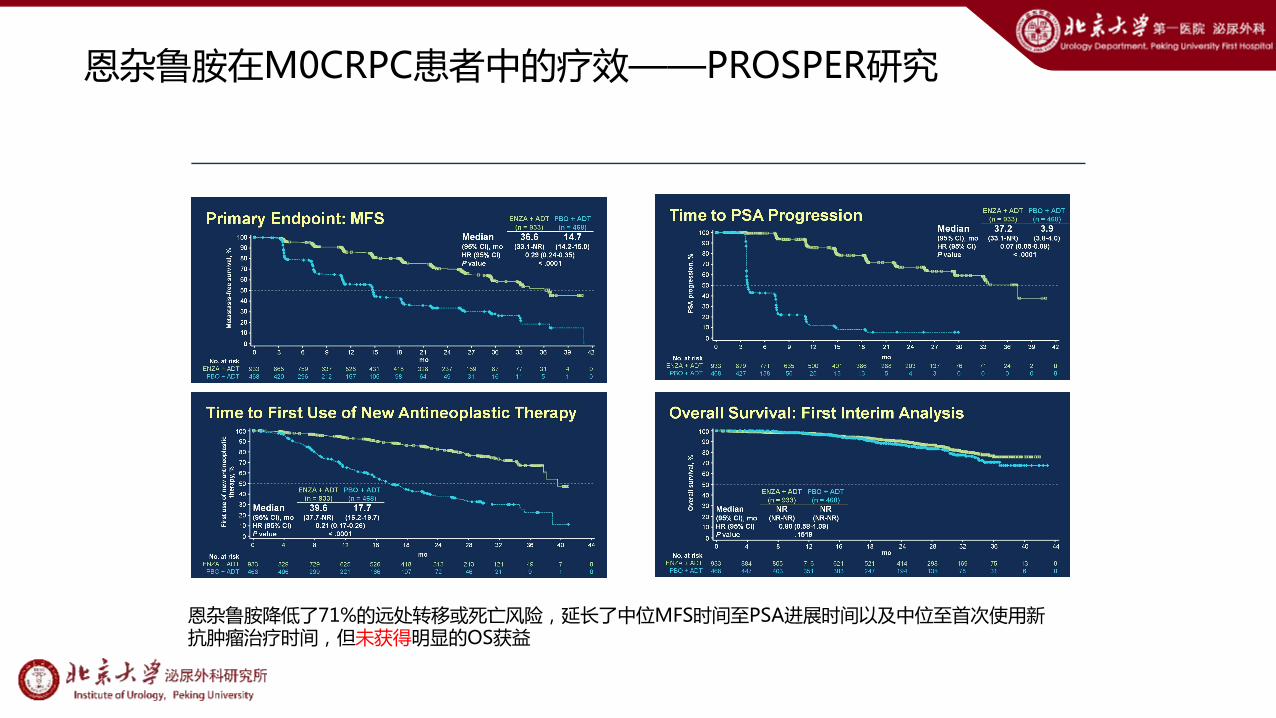
恩杂鲁胺在M0CRPC患者中的疗效——PROSPER研究
恩杂鲁胺在M0CRPC患者中的疗效——PROSPER研究
恩杂鲁胺降低了71%的远处转移或死亡风险,延长了中位MFS时间至PSA进展时间以及中位至首次使用新抗肿瘤治疗时间,但未获得明显的OS获益

安全性报告

• 在M0 CRPC、PSA快速倍增(中位3.7个月)的患者中,恩杂鲁胺降低了71%的进展为M1 CRPC的相对风险--中位PFS恩杂鲁胺组36.6个月vs安慰剂组14.7个月(HR, 0.29; P<0.0001)
• 治疗耐受性良好;总体上副作用与之前的CRPC临床试验结果基本一致
• 恩杂鲁胺同样显著延长了次要终点(至PSA进展时间、至首次使用新抗肿瘤治疗时间)
• 中位OS在首次中期分析时两组均未达到,恩杂鲁胺组并未获得OS获益
恩杂鲁胺在M0CRPC患者中的疗效——PROSPER研究
EAU 2018,abstruct 604

SPARTAN, a Phase 3 Double-Blind, Randomized Study of Apalutamide vs Placebo in Patients With Nonmetastatic Castration-Resistant Prostate Cancer


Slide 5
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

CRPC新型内分泌治疗:治疗前提可获更好疗效?
nmCRPCEnzalutamide
PFS 36.6m vs 14.7mOS 3y约 80% vs 70%
ApalutamidePFS 40.5m vs 16.2m
OS 3y 约80%
AbirateronePFS 16.5m vs 8.2mOS 35.3m vs 30.1m
3y 约 40+%
EnzalutamidePFS NR m vs 14.8mOS 32.4m vs 30.2m
3y 约 40+%
mCRPC
?

CRPC 新型内分泌治疗:应用更加广泛
mCRPC 化疗后 未化疗
Abiraterone COU-AA-301(2011) COU-AA-302(2012)
Enzalutamide AFFIRM(2012) PREVAIL(2013)
CRPC(未化疗) M1 M0 M0
Enzalutamide TERRAIN / STRIVE(Vs. Bicalutamide)
STRIVE(Vs. Bicalutamide)
PROSPER(2018)
Apalutamide SPARTAN(2018)

所有的CRPC都适合应用新型内分泌治疗?

总结
• CRPC患者需维持雄激素剥夺治疗(ADT)
• 新型内分泌治疗药物显著提高mCRPC患者的生存
• 对于高危无转移CRPC患者推荐应用Apalutamide和恩杂鲁胺

感谢聆听!





























