Embed Size (px)
Citation preview
16. Spiral-CT WorkshopHannover, 11.-13. Sep 2009
Joachim LotzInstitut für Radiologie
Triple Rule Out
CT Angiographie
Montag, 14. September 2009
Medizinische Hochschule Hannover
CT - AngiographieProzedere
1. Festlegung der Scanlänge2. Festlegung der Scanparameter in
Abhängigkeit von Scanlänge und Dauer3. Wahl der Kontrastmittelparameter4. Bildauswertung interaktiv5. Befundpräsentation
Montag, 14. September 2009
Medizinische Hochschule Hannover
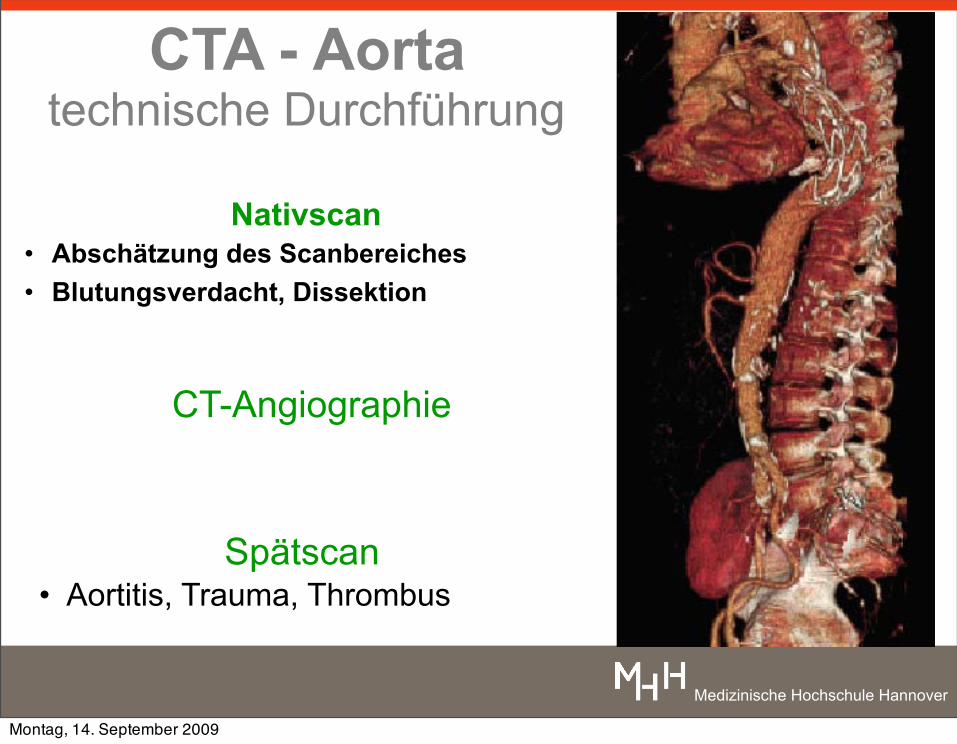
CTA - Aortatechnische Durchführung
Nativscan• Abschätzung des Scanbereiches• Blutungsverdacht, Dissektion
CT-Angiographie
Spätscan• Aortitis, Trauma, Thrombus
Montag, 14. September 2009
Medizinische Hochschule Hannover
CTA ScanprotokolleScanbereich bestimmt die Kollimation
Montag, 14. September 2009
Medizinische Hochschule Hannover
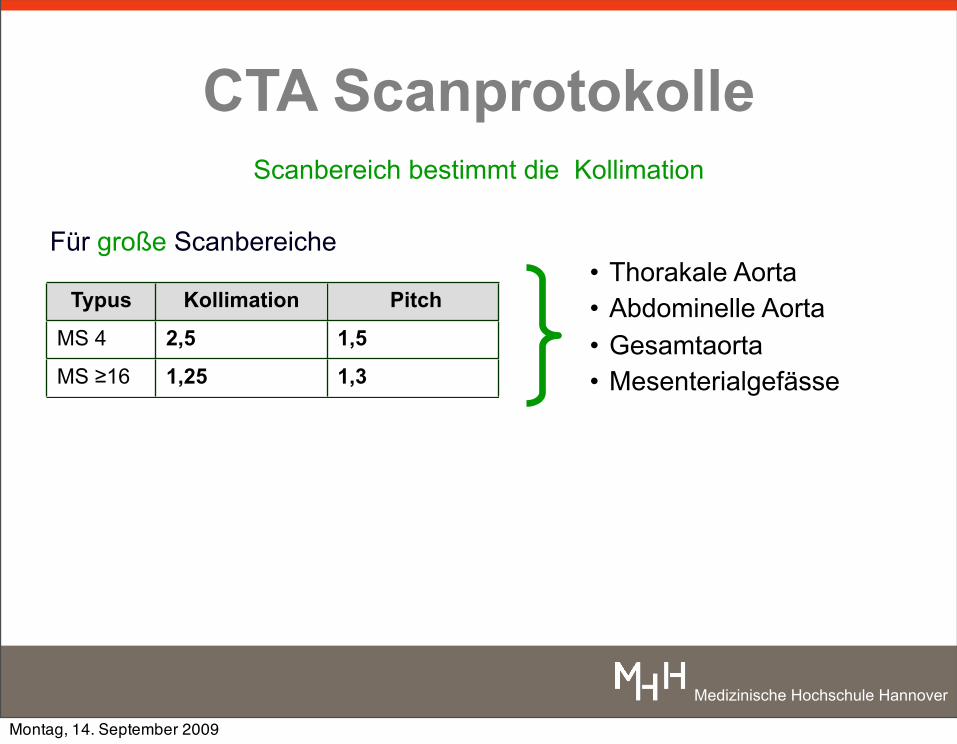
CTA Scanprotokolle
Für große Scanbereiche
Typus Kollimation Pitch
MS 4 2,5 1,5
MS ≥16 1,25 1,3
Scanbereich bestimmt die Kollimation
• Thorakale Aorta• Abdominelle Aorta• Gesamtaorta• Mesenterialgefässe
Montag, 14. September 2009
Medizinische Hochschule Hannover
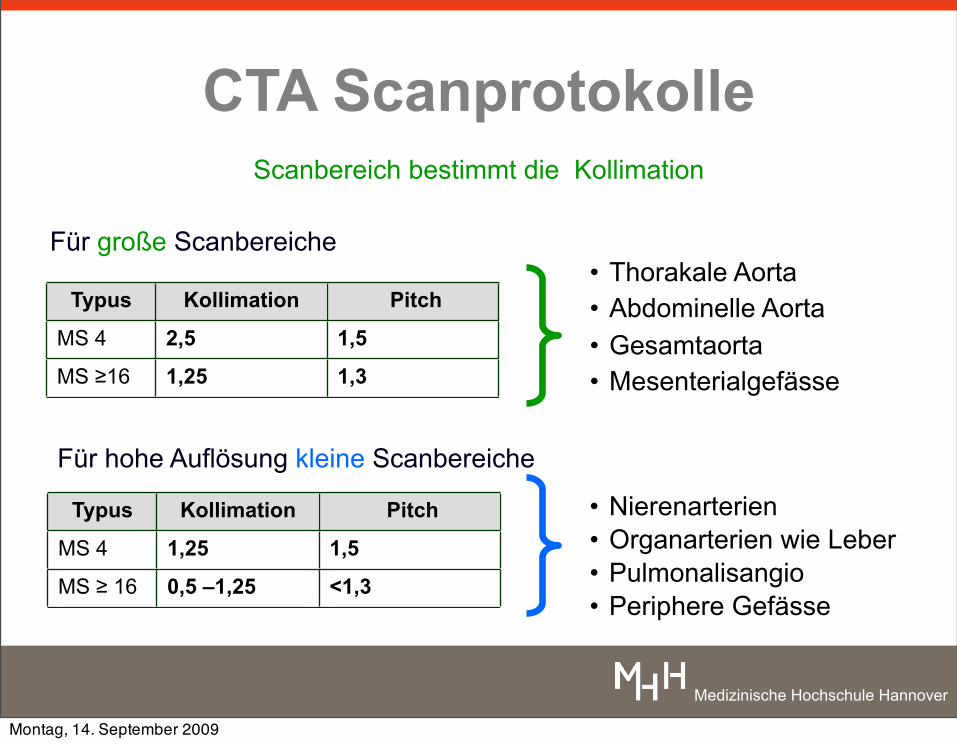
CTA Scanprotokolle
Für große Scanbereiche
Für hohe Auflösung kleine Scanbereiche
Typus Kollimation Pitch
MS 4 2,5 1,5
MS ≥16 1,25 1,3
Scanbereich bestimmt die Kollimation
Typus Kollimation Pitch
MS 4 1,25 1,5
MS ≥ 16 0,5 –1,25 <1,3
• Nierenarterien• Organarterien wie Leber• Pulmonalisangio• Periphere Gefässe
• Thorakale Aorta• Abdominelle Aorta• Gesamtaorta• Mesenterialgefässe
Montag, 14. September 2009
Medizinische Hochschule Hannover
CTA AortaIndikation:
sämtliche Aortenerkrankungen
Montag, 14. September 2009
Medizinische Hochschule Hannover
CTA AortaIndikation:
sämtliche Aortenerkrankungen
keine Indikationspinale Versorgung bei Aortenaneurysmen
Montag, 14. September 2009
Medizinische Hochschule Hannover
CTA AortaIndikation:
sämtliche Aortenerkrankungen
keine Indikationspinale Versorgung bei Aortenaneurysmen
Dissektion / Aneurysma: ersetzt DSA akute Notfälle: Methode der Wahlprä-/ postinterventionell: Methode der Wahl
Montag, 14. September 2009
Medizinische Hochschule Hannover
CTA AortaIndikation:
sämtliche Aortenerkrankungen
keine Indikationspinale Versorgung bei Aortenaneurysmen
Dissektion / Aneurysma: ersetzt DSA akute Notfälle: Methode der Wahlprä-/ postinterventionell: Methode der Wahl
Scanprotokoll: mono / biphasisch (nativ + arteriell)Für Aortitis: Spätphase nach 60s
Montag, 14. September 2009
Medizinische Hochschule Hannover
Montag, 14. September 2009

Medizinische Hochschule Hannover
Montag, 14. September 2009
Medizinische Hochschule Hannover
CTA Pulmonalembolie: derzeitiger Stand
Indikation: akute oder chronische Lungenembolie
Montag, 14. September 2009
Medizinische Hochschule Hannover
CTA Pulmonalembolie: derzeitiger Stand
Indikation: akute oder chronische Lungenembolie
keine Indikationgeringer Embolie-Verdacht
Montag, 14. September 2009
Medizinische Hochschule Hannover
CTA Pulmonalembolie: derzeitiger Stand
Indikation: akute oder chronische Lungenembolie
keine Indikationgeringer Embolie-Verdacht
Sensitivität: >90% Spezifität: > 90% negativer Vorhersagewert: > 95%
wenn in Übereinstimmung mit Klinik (Wells-Scala)kann Szintigraphie ersetzen
Montag, 14. September 2009
Medizinische Hochschule Hannover
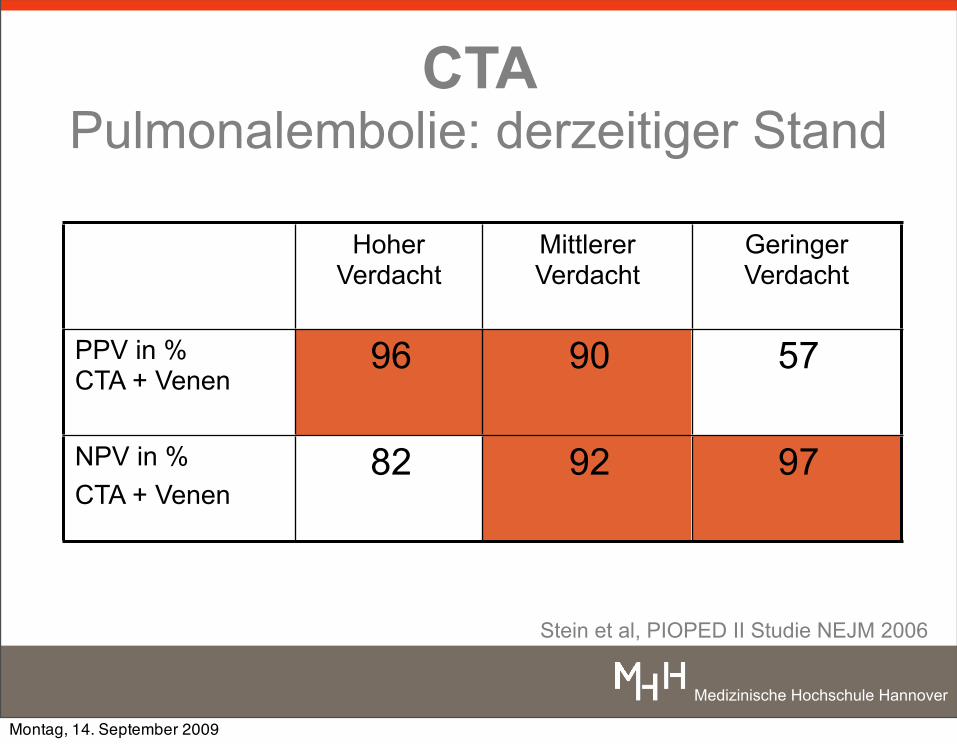
CTA Pulmonalembolie: derzeitiger Stand
Stein et al, PIOPED II Studie NEJM 2006
HoherVerdacht
Mittlerer Verdacht
Geringer Verdacht
PPV in % CTA + Venen
96 90 57
NPV in %CTA + Venen
82 92 97
Montag, 14. September 2009
Medizinische Hochschule Hannover
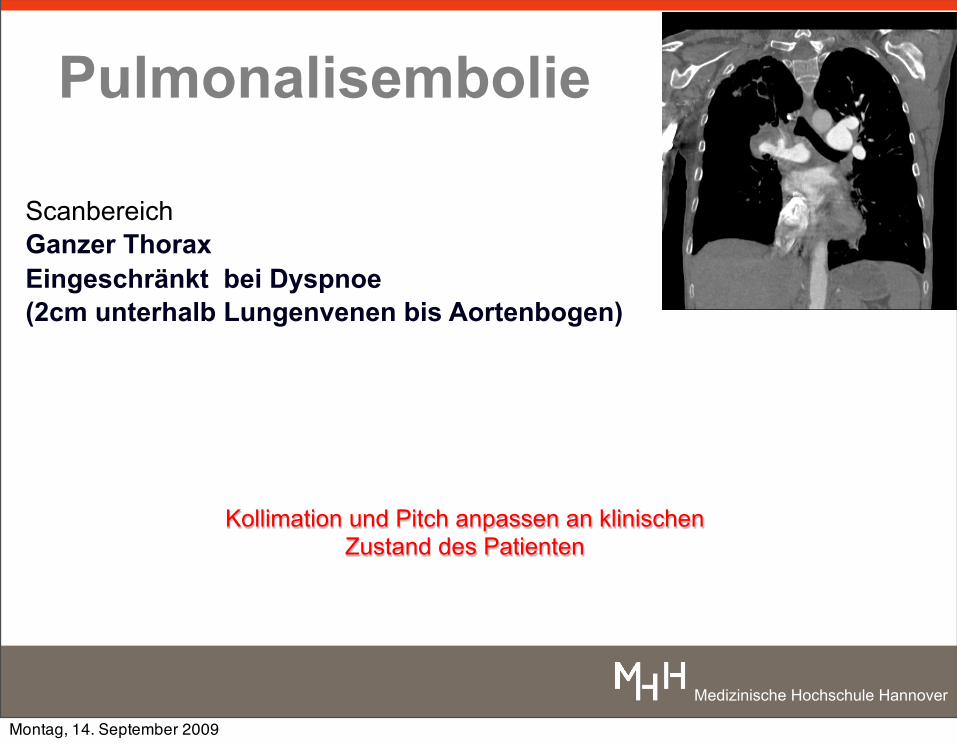
Pulmonalisembolie
ScanbereichGanzer Thorax Eingeschränkt bei Dyspnoe(2cm unterhalb Lungenvenen bis Aortenbogen)
Kollimation und Pitch anpassen an klinischen Zustand des Patienten
Montag, 14. September 2009
Medizinische Hochschule Hannover
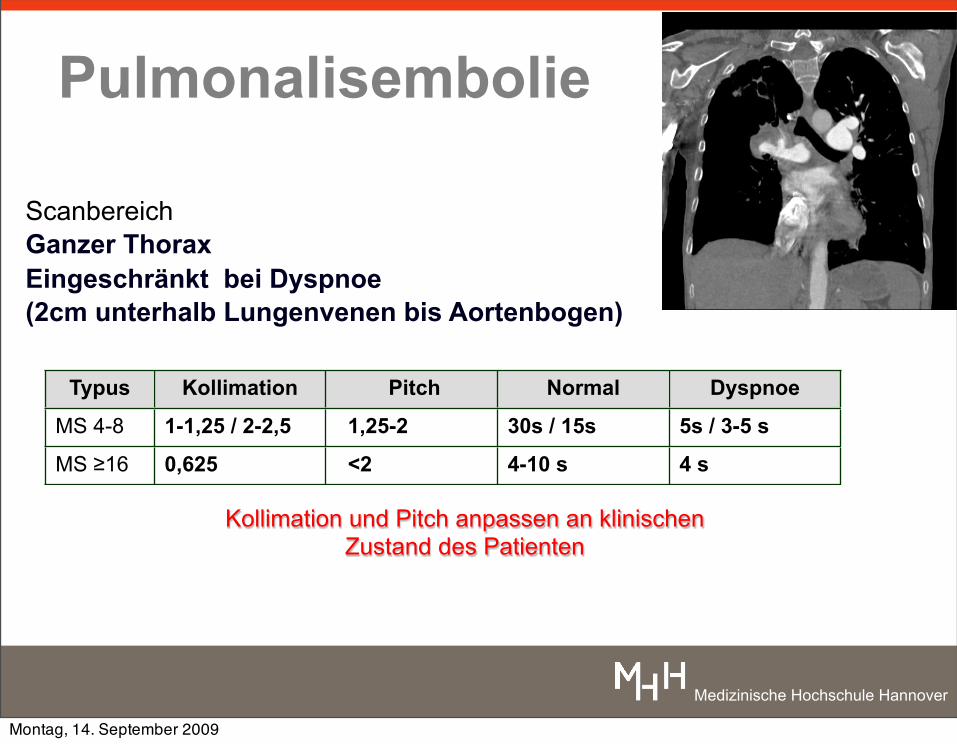
Pulmonalisembolie
ScanbereichGanzer Thorax Eingeschränkt bei Dyspnoe(2cm unterhalb Lungenvenen bis Aortenbogen)
Typus Kollimation Pitch Normal Dyspnoe
MS 4-8 1-1,25 / 2-2,5 1,25-2 30s / 15s 5s / 3-5 s
MS ≥16 0,625 <2 4-10 s 4 s
Kollimation und Pitch anpassen an klinischen Zustand des Patienten
Montag, 14. September 2009
Medizinische Hochschule Hannover
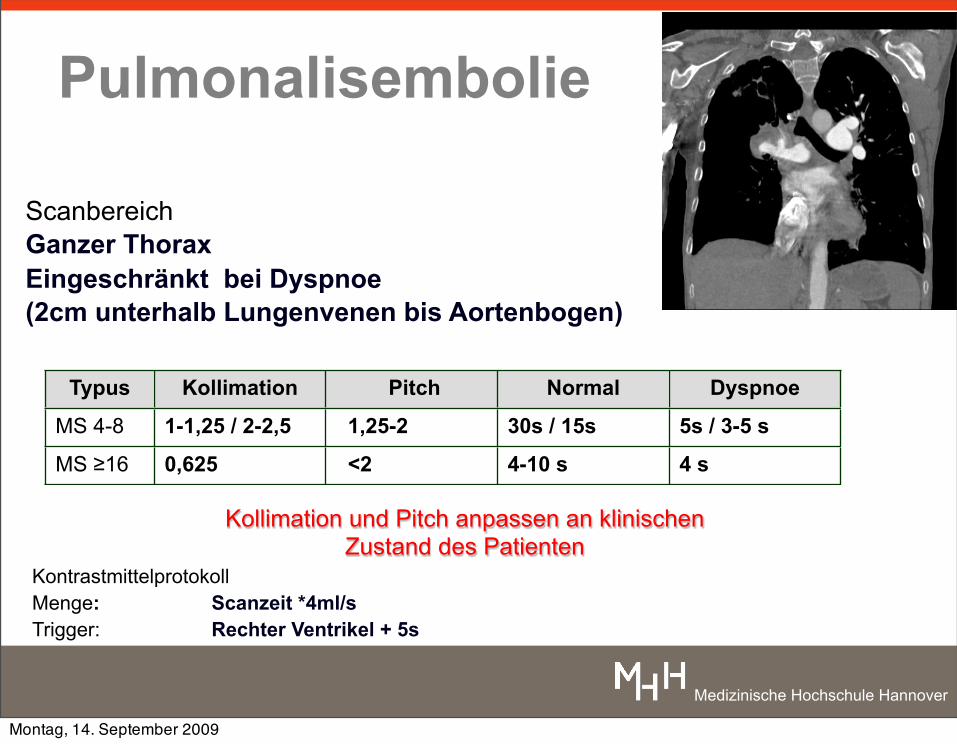
Pulmonalisembolie
KontrastmittelprotokollMenge: Scanzeit *4ml/s Trigger: Rechter Ventrikel + 5s
ScanbereichGanzer Thorax Eingeschränkt bei Dyspnoe(2cm unterhalb Lungenvenen bis Aortenbogen)
Typus Kollimation Pitch Normal Dyspnoe
MS 4-8 1-1,25 / 2-2,5 1,25-2 30s / 15s 5s / 3-5 s
MS ≥16 0,625 <2 4-10 s 4 s
Kollimation und Pitch anpassen an klinischen Zustand des Patienten
Montag, 14. September 2009
Medizinische Hochschule Hannover
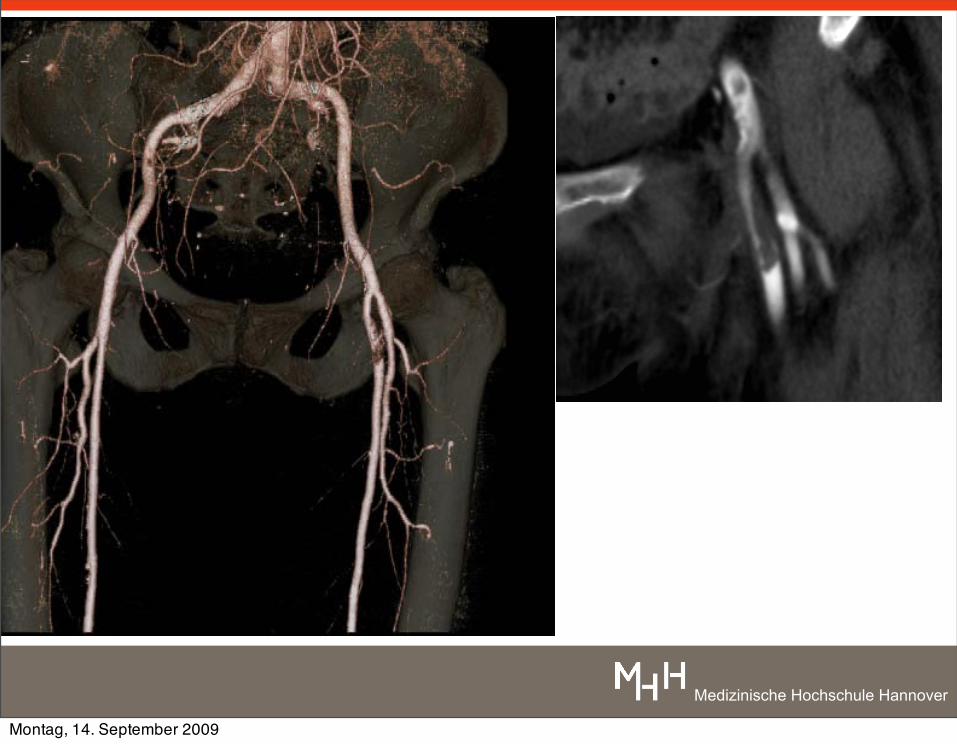
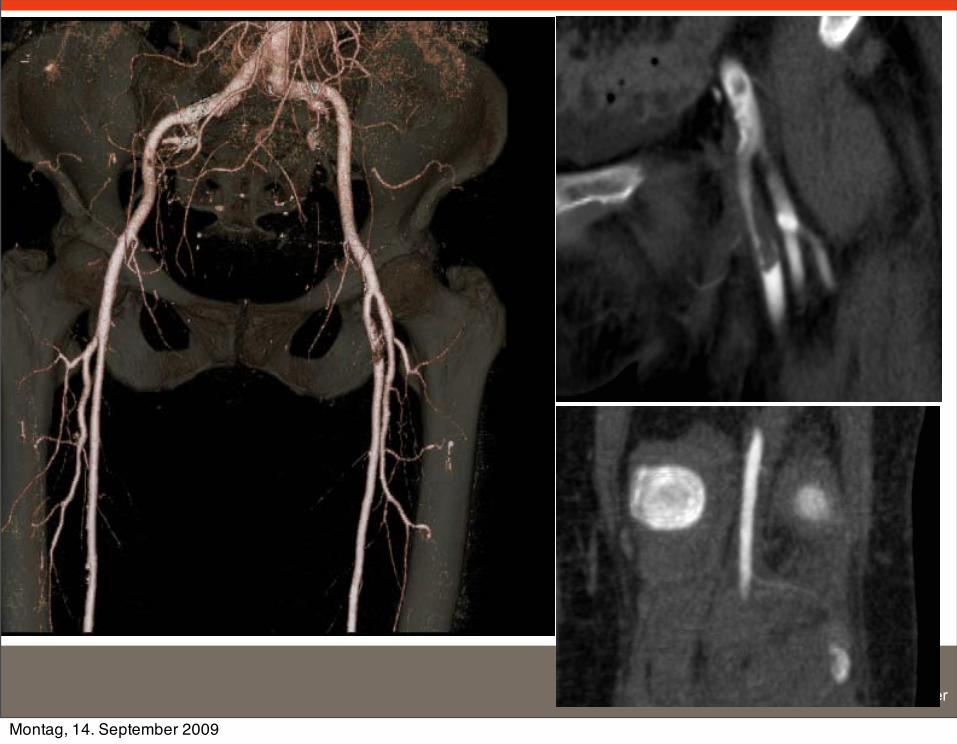
CTABecken-Bein: TraumaDetektion von Gefäßverletzungen nach Trauma
Verwertbarkeit: 98%Sensitivität: ca. 95-100%Spezifität ca. 99-100%
Nachweis und Lokalisation von Gefäßverletzungen
Klassifkiation: Nicht gelistet.
Inaba et al J. Trauma 2006 60(3)Soto et al Radiology 2001
Montag, 14. September 2009
Medizinische Hochschule Hannover
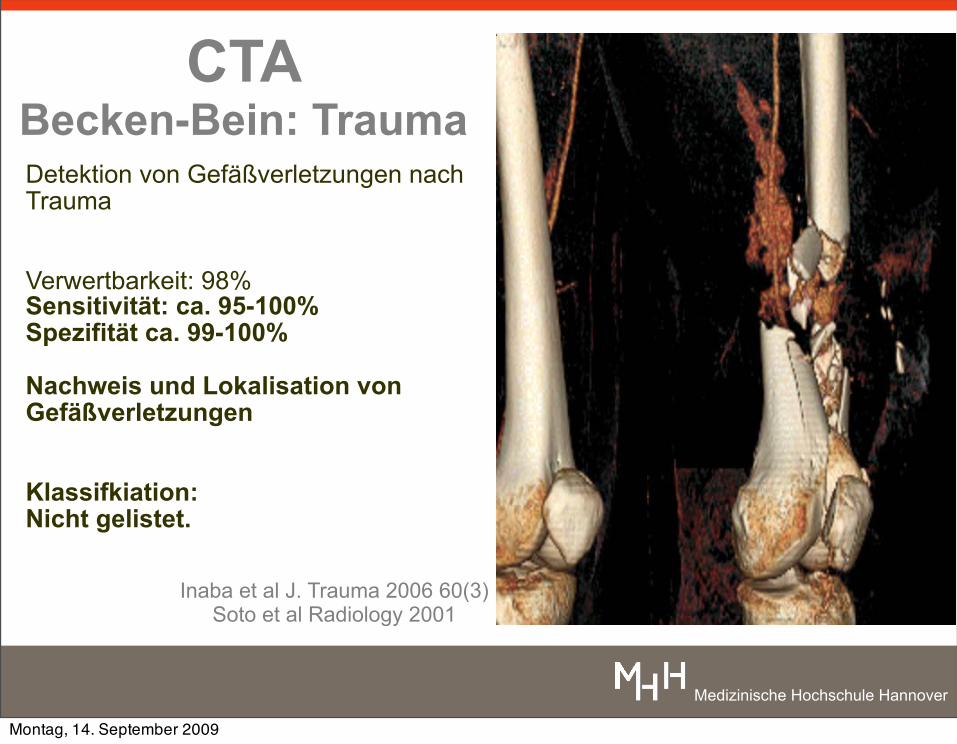
CTABecken-Bein: TraumaDetektion von Gefäßverletzungen nach Trauma
Verwertbarkeit: 98%Sensitivität: ca. 95-100%Spezifität ca. 99-100%
Nachweis und Lokalisation von Gefäßverletzungen
Klassifkiation: Nicht gelistet.
Inaba et al J. Trauma 2006 60(3)Soto et al Radiology 2001
Montag, 14. September 2009
Medizinische Hochschule Hannover
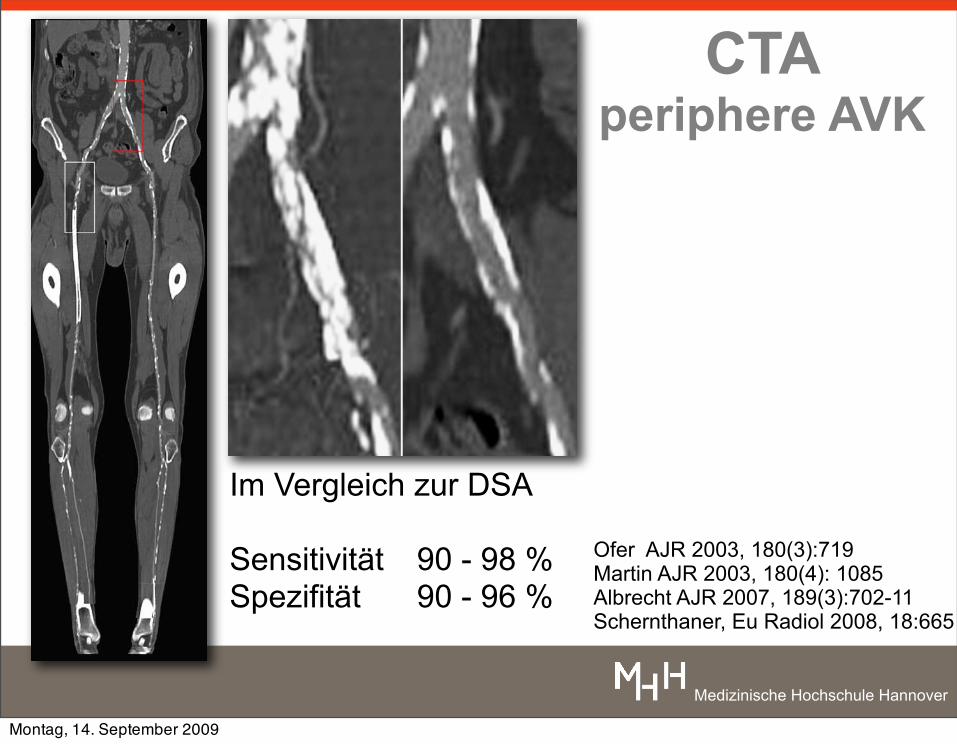
CTAperiphere AVK
Im Vergleich zur DSA
Sensitivität 90 - 98 %Spezifität 90 - 96 %
Ofer AJR 2003, 180(3):719Martin AJR 2003, 180(4): 1085Albrecht AJR 2007, 189(3):702-11Schernthaner, Eu Radiol 2008, 18:665
Montag, 14. September 2009
Medizinische Hochschule Hannover
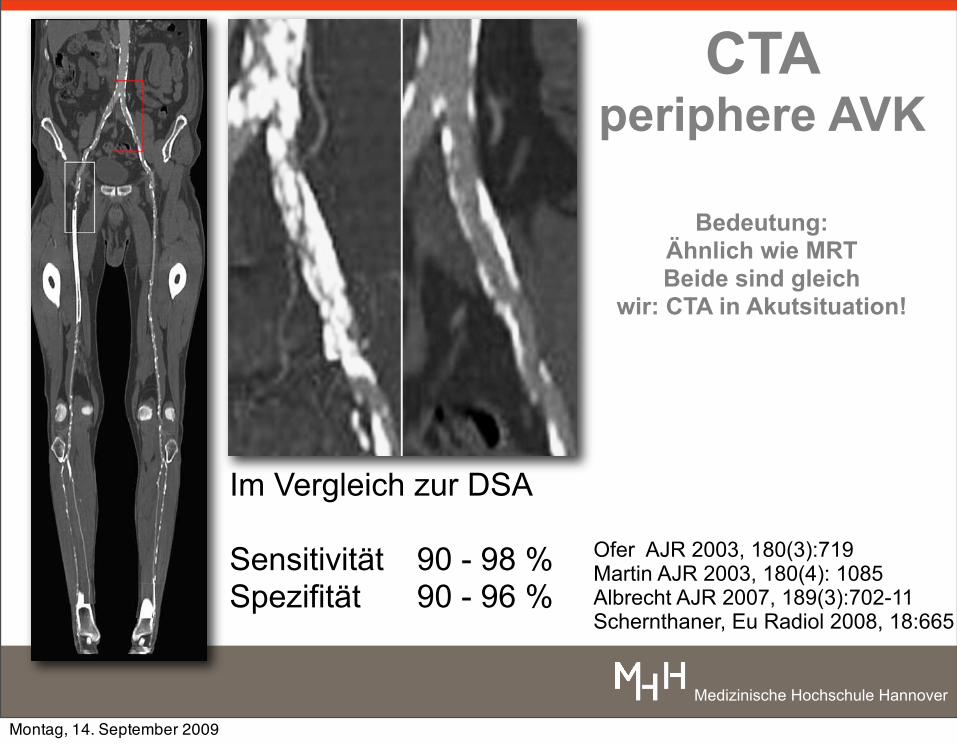
CTAperiphere AVK
Bedeutung: Ähnlich wie MRTBeide sind gleich
wir: CTA in Akutsituation!
Im Vergleich zur DSA
Sensitivität 90 - 98 %Spezifität 90 - 96 %
Ofer AJR 2003, 180(3):719Martin AJR 2003, 180(4): 1085Albrecht AJR 2007, 189(3):702-11Schernthaner, Eu Radiol 2008, 18:665
Montag, 14. September 2009
Medizinische Hochschule Hannover
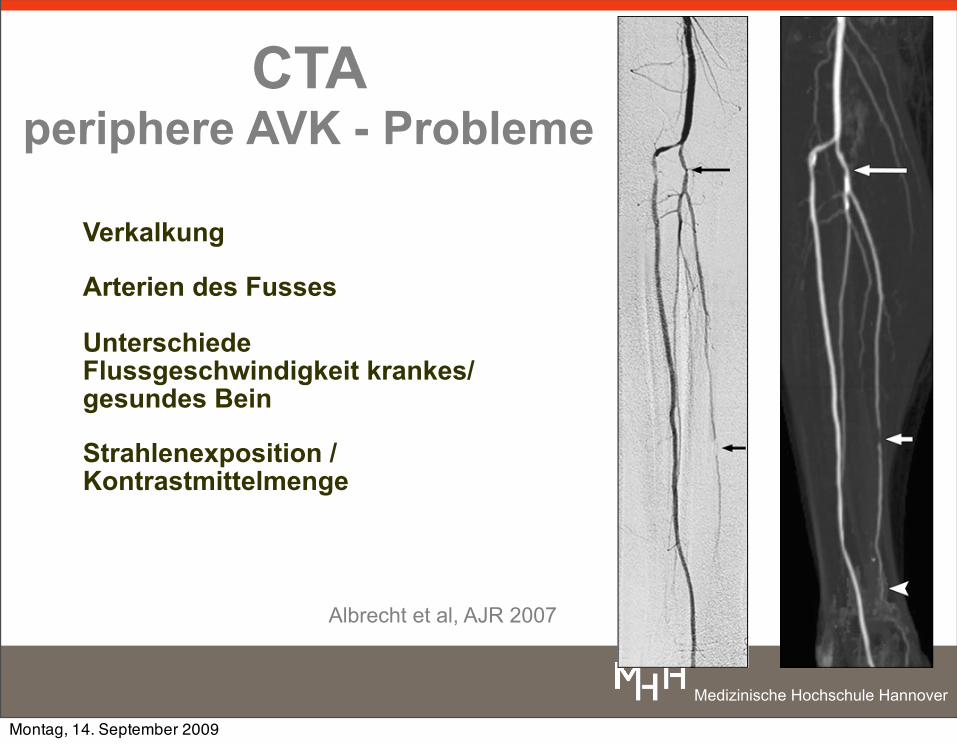
CTAperiphere AVK - Probleme
Verkalkung
Arterien des Fusses
Unterschiede Flussgeschwindigkeit krankes/ gesundes Bein
Strahlenexposition / Kontrastmittelmenge
Albrecht et al, AJR 2007
Albrecht et al.
708 AJR:189, September 2007
09_07_2333_Albrecht.fm — 7/30/07
resolution. This may have been exacerbatedby the effective slice thickness of 2 mm usedin this study; thinner slices should reduce par-tial volume effects and may improve collat-eral visualization. Regardless of the visual-ization of collateral circulation, visualizationof refilling native arteries distal to occlusionswas better on CTA than on DSA in our study(Figs. 3 and 4), which is consistent with pre-vious reports [6, 12, 13].
In terms of patient management decisions,our results revealed equivalence of CTA and
DSA in 49 of the 50 patients. This finding fur-ther supports the use of CTA as a noninvasivealternative to DSA for diagnostic imaging ofthe peripheral vasculature.
The mean time for image analysis waslonger for the two CTA observers than for theDSA observers. Although the additional timenecessary for postprocessing and evaluationof CTA images is offset by savings in tableand examination time, the large amount ofdata generated on CTA is an established prob-lem of the technique.
Until the introduction of MDCT scannerswith four detector rows, imaging of the pe-ripheral vascular tree was limited to not morethan 40 cm of craniocaudal coverage after asingle IV injection of iodine-based contrastmedium [3–5, 21–23]. However, the rela-tively slow speed of acquisition and poor z-axis resolution of single-detector CT scannersprecluded full coverage of the peripheral vas-cular tree from the renal arteries to the toes.The advent of 4-MDCT technology improvedthe utility of CTA for evaluation of peripheral
A B A B
Fig. 2—Digital subtraction angiography (DSA) and CT angiography (CTA) performed 5 days after stent placement in right distal superficial femoral artery in 59-year-old man with recurring claudication.A, DSA image (posteroanterior projection) of thigh shows 5-cm occlusion of stented segment (arrow) with grade 1 collaterals (arrowheads).B, Corresponding CTA image (maximum-intensity-projection reconstruction) also shows occlusion (arrow) proximal to stent (asterisk) and similar number of collateral vessels (arrowheads) judged as grade 1 by both observers.
Fig. 3—Digital subtraction angiography (DSA) and CT angiography (CTA) of below-knee arteries of right leg in 54-year-old man with chronic claudication and two proximal high-grade stenoses (not shown).A, DSA image (posteroanterior projection) shows grade 2 stenosis of tibiofibular trunk (long arrow) and grade 3 stenosis of posterior tibial artery (short arrow). Most distal part of posterior tibial artery is not visualized.B, Corresponding CTA image underestimates stenosis of tibiofibular trunk (long arrow) as grade 1 (both observers) but correctly shows grade 3 stenosis (as judged by both observers) of posterior tibial artery (short arrow). Posterior tibial artery (arrowhead) is visualized down to ankle and thus is shown more completely on CTA than on DSA.
Montag, 14. September 2009
Medizinische Hochschule Hannover
Montag, 14. September 2009
Medizinische Hochschule Hannover
Montag, 14. September 2009
Medizinische Hochschule Hannover
Montag, 14. September 2009

Medizinische Hochschule Hannover
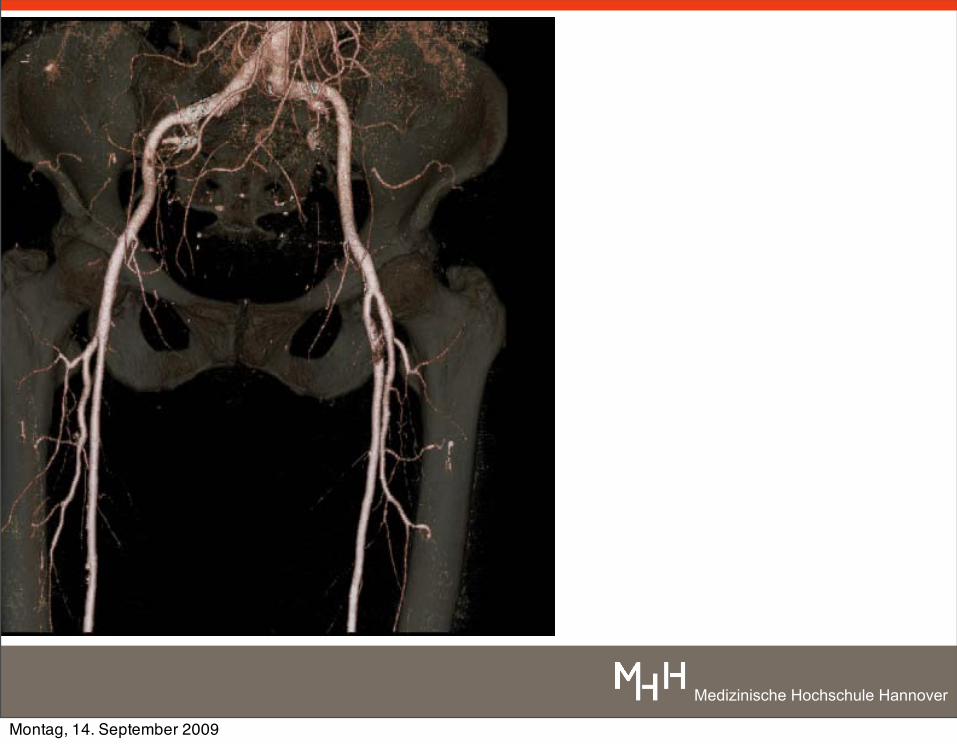
periphere Gefäße Becken-Bein
Montag, 14. September 2009
Medizinische Hochschule Hannover
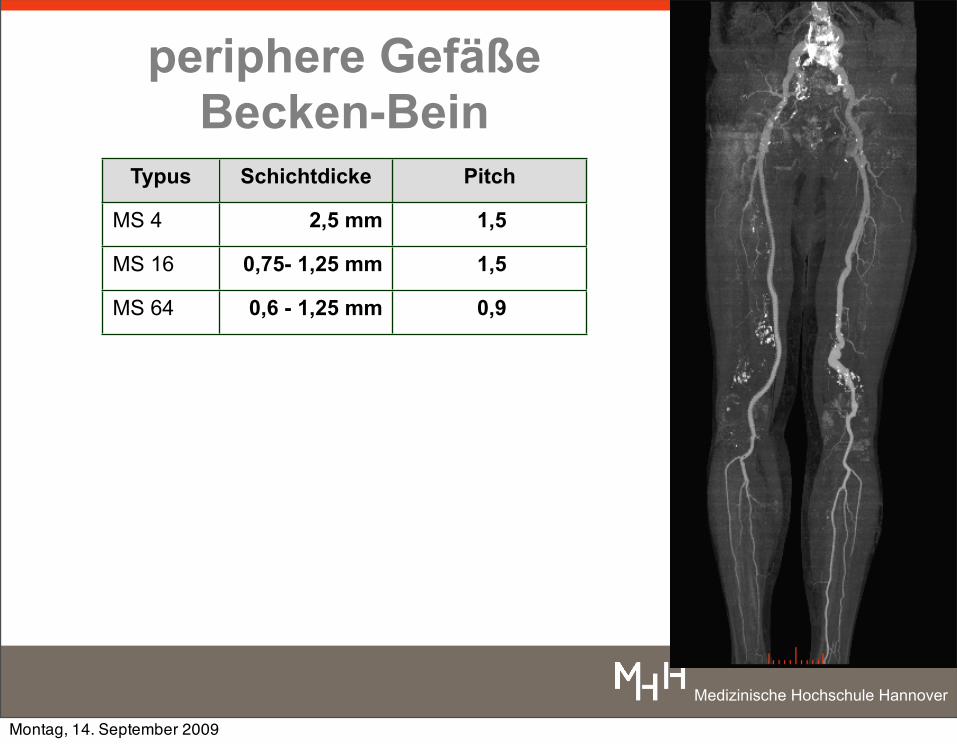
periphere Gefäße Becken-Bein
Typus Schichtdicke Pitch
MS 4 2,5 mm 1,5
MS 16 0,75- 1,25 mm 1,5
MS 64 0,6 - 1,25 mm 0,9
Montag, 14. September 2009
Medizinische Hochschule Hannover
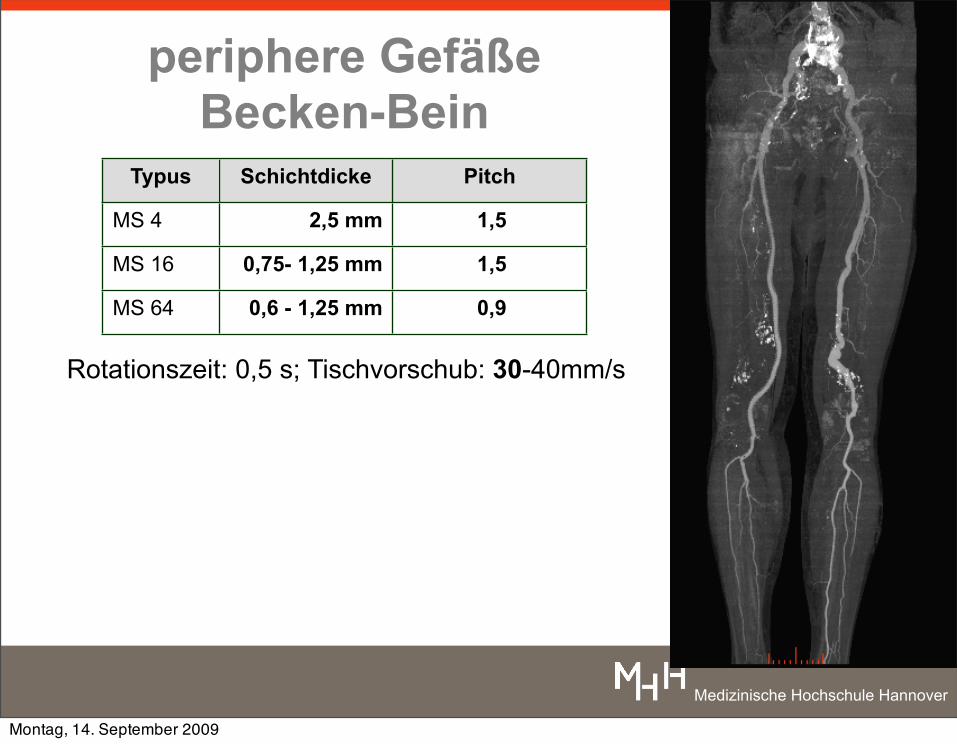
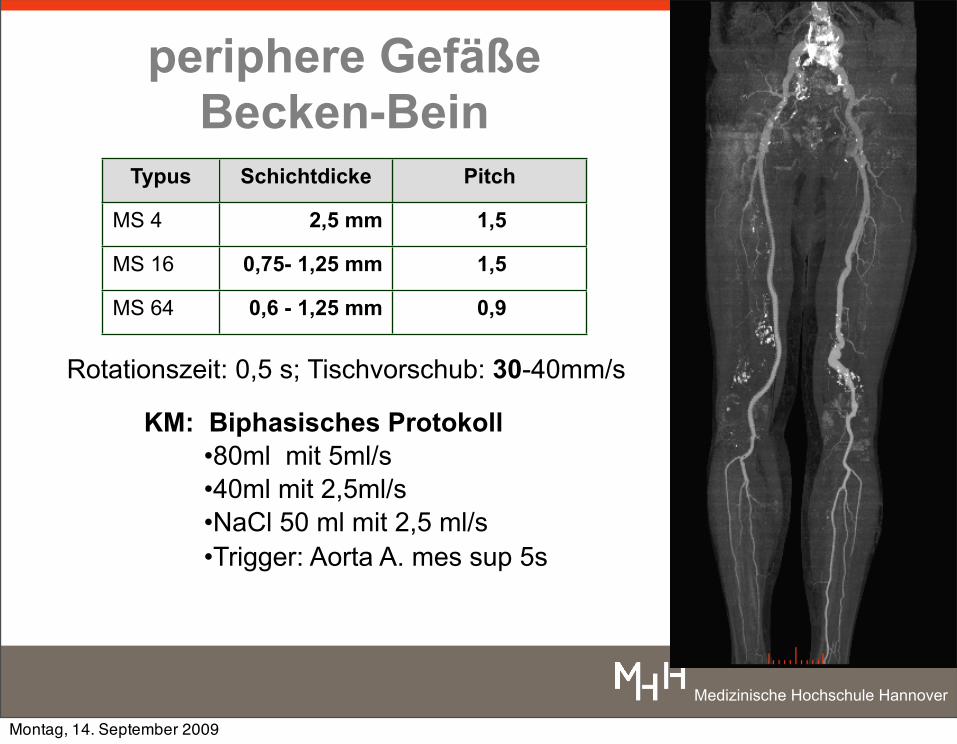
periphere Gefäße Becken-Bein
Typus Schichtdicke Pitch
MS 4 2,5 mm 1,5
MS 16 0,75- 1,25 mm 1,5
MS 64 0,6 - 1,25 mm 0,9
Rotationszeit: 0,5 s; Tischvorschub: 30-40mm/s
Montag, 14. September 2009
Medizinische Hochschule Hannover
periphere Gefäße Becken-Bein
Typus Schichtdicke Pitch
MS 4 2,5 mm 1,5
MS 16 0,75- 1,25 mm 1,5
MS 64 0,6 - 1,25 mm 0,9
KM: Biphasisches Protokoll•80ml mit 5ml/s•40ml mit 2,5ml/s•NaCl 50 ml mit 2,5 ml/s •Trigger: Aorta A. mes sup 5s
Rotationszeit: 0,5 s; Tischvorschub: 30-40mm/s
Montag, 14. September 2009
Medizinische Hochschule Hannover
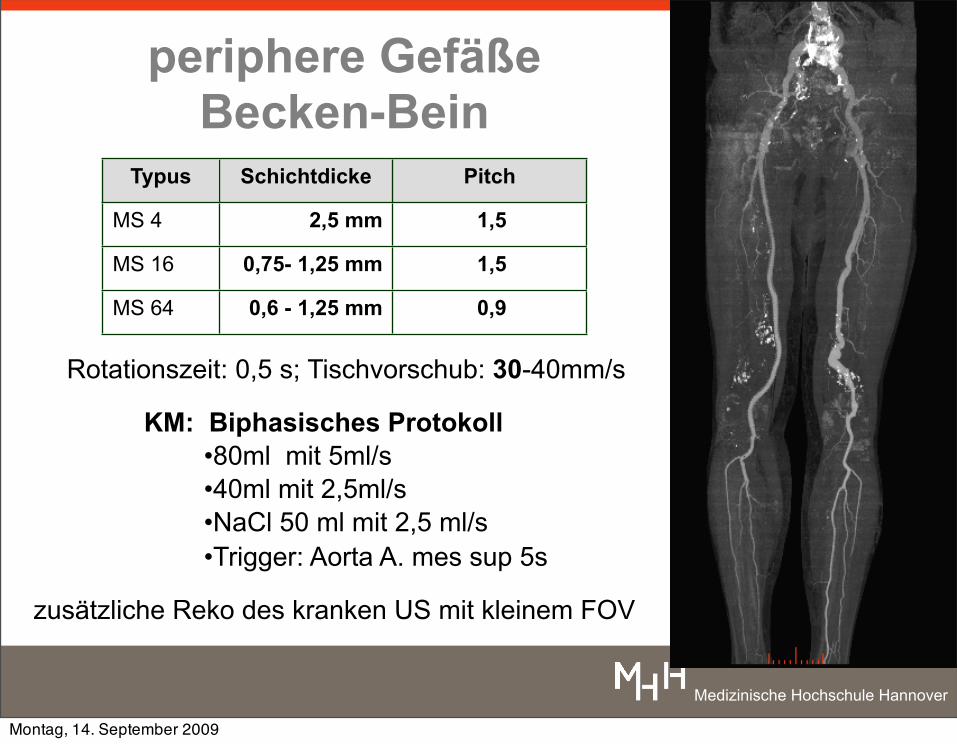
periphere Gefäße Becken-Bein
Typus Schichtdicke Pitch
MS 4 2,5 mm 1,5
MS 16 0,75- 1,25 mm 1,5
MS 64 0,6 - 1,25 mm 0,9
zusätzliche Reko des kranken US mit kleinem FOV
KM: Biphasisches Protokoll•80ml mit 5ml/s•40ml mit 2,5ml/s•NaCl 50 ml mit 2,5 ml/s •Trigger: Aorta A. mes sup 5s
Rotationszeit: 0,5 s; Tischvorschub: 30-40mm/s
Montag, 14. September 2009
Medizinische Hochschule Hannover
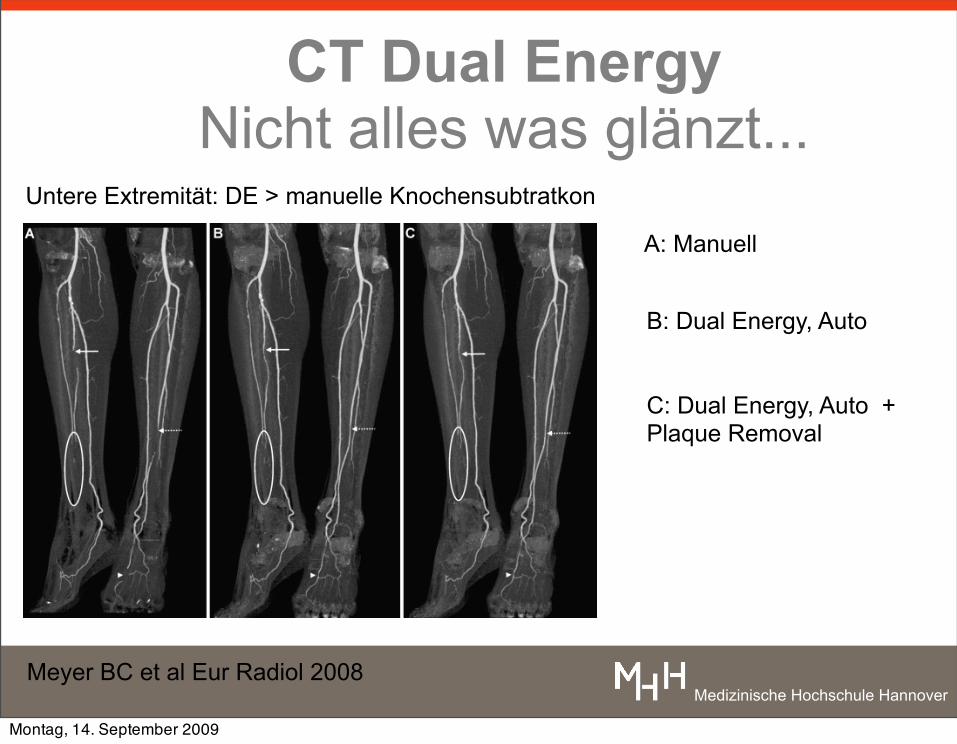
CT Dual Energy Nicht alles was glänzt...
Meyer BC et al Eur Radiol 2008
Untere Extremität: DE > manuelle Knochensubtratkon
A: Manuell
B: Dual Energy, Auto
C: Dual Energy, Auto + Plaque Removal
Montag, 14. September 2009
Medizinische Hochschule Hannover
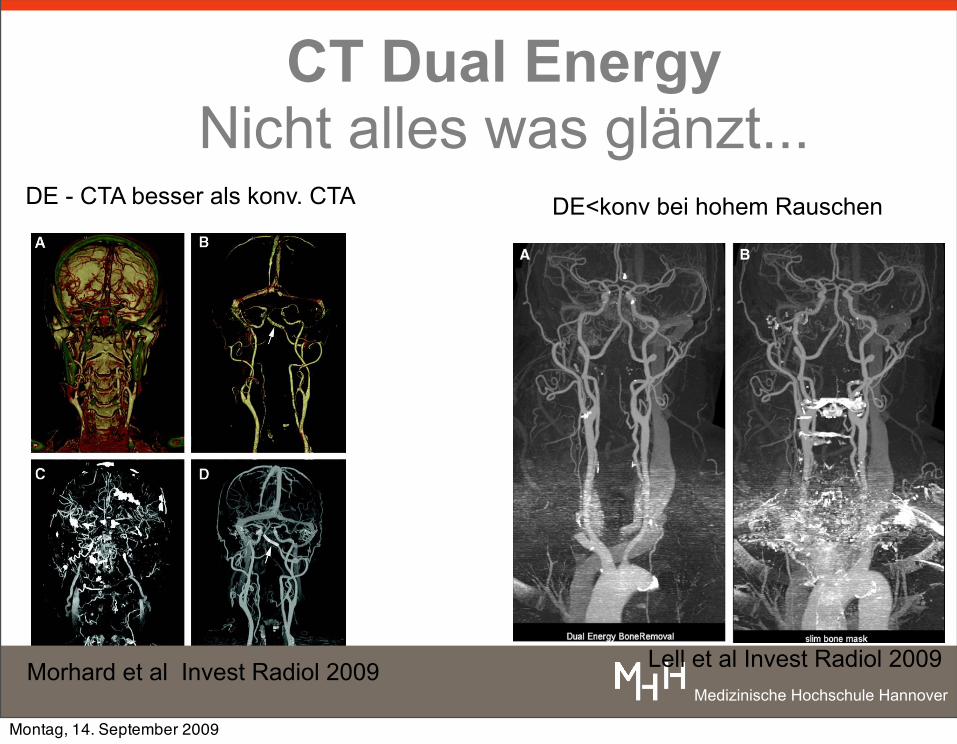
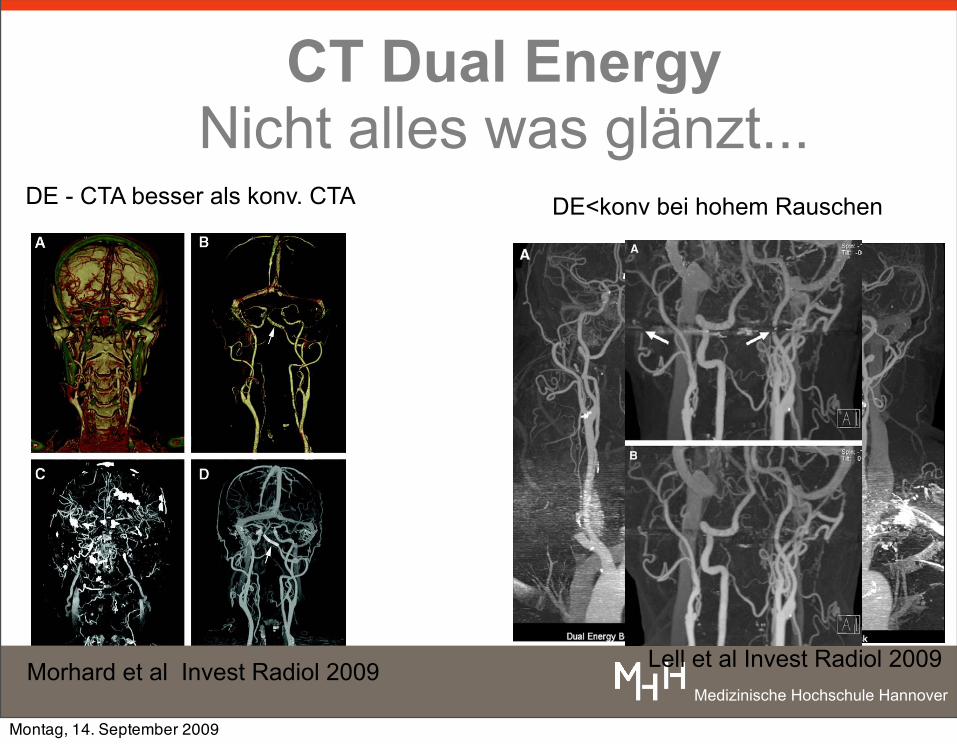
CT Dual Energy Nicht alles was glänzt...
Morhard et al Invest Radiol 2009
DE - CTA besser als konv. CTA DE<konv bei hohem Rauschen
Lell et al Invest Radiol 2009
Montag, 14. September 2009
Medizinische Hochschule Hannover
CT Dual Energy Nicht alles was glänzt...
Morhard et al Invest Radiol 2009
DE - CTA besser als konv. CTA DE<konv bei hohem Rauschen
Lell et al Invest Radiol 2009
Montag, 14. September 2009
Medizinische Hochschule Hannover
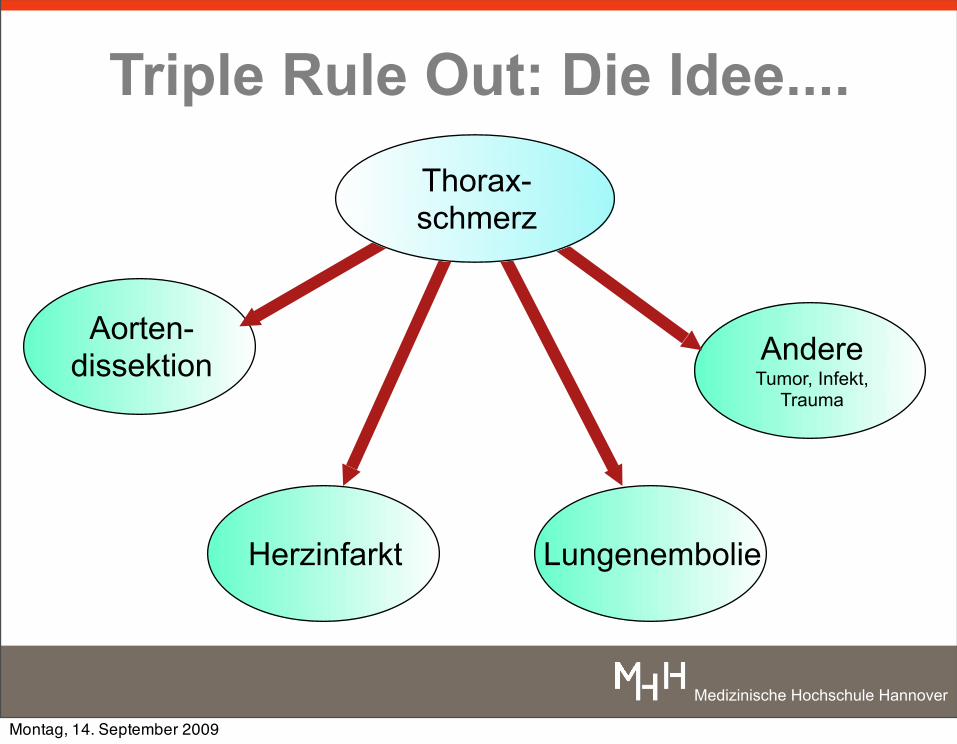
Triple Rule Out: Die Idee....
Herzinfarkt
Aorten-dissektion
Lungenembolie
AndereTumor, Infekt,
Trauma
Thorax-schmerz
Montag, 14. September 2009
Medizinische Hochschule Hannover
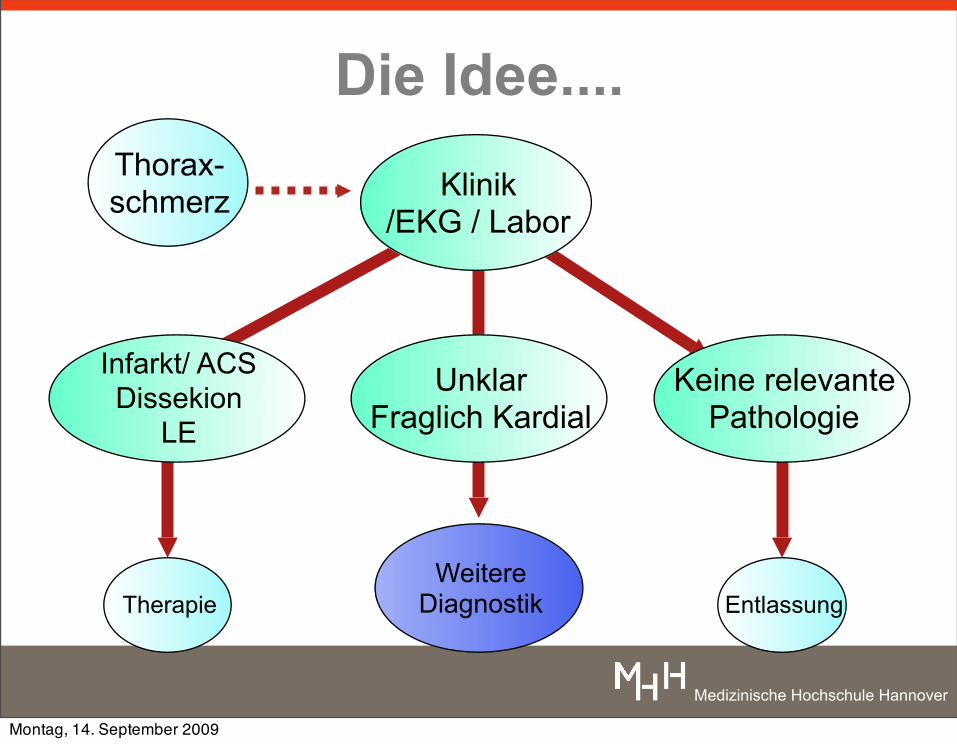
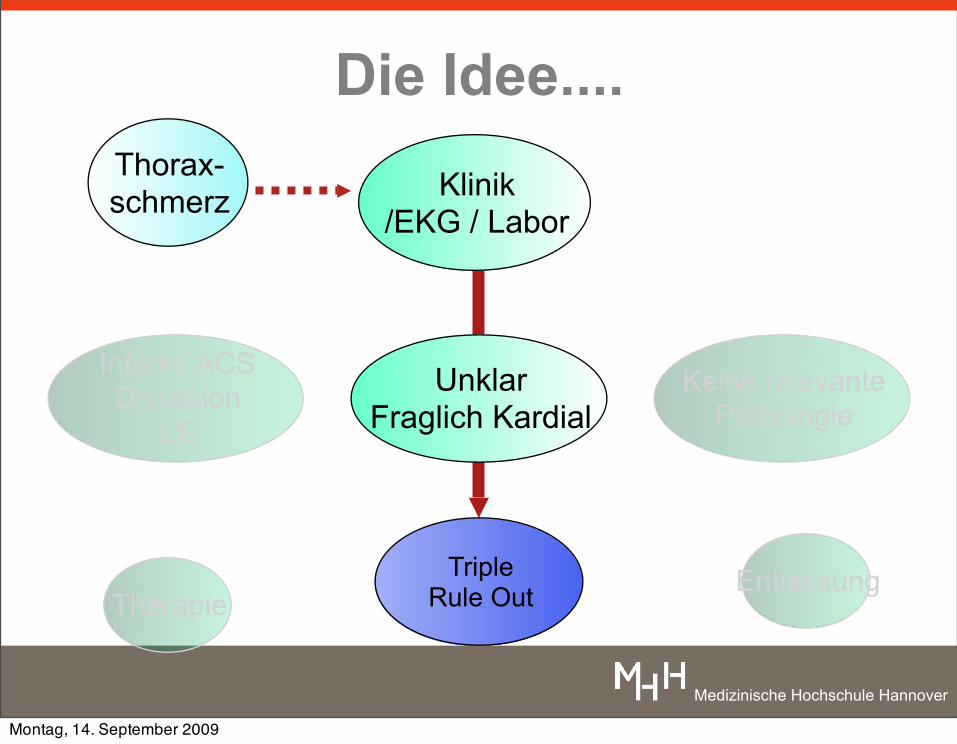
Die Idee....Thorax-schmerz Klinik
/EKG / Labor
UnklarFraglich Kardial
Infarkt/ ACSDissekion
LE
Keine relevantePathologie
Therapie EntlassungWeitere
Diagnostik
Montag, 14. September 2009
Medizinische Hochschule Hannover
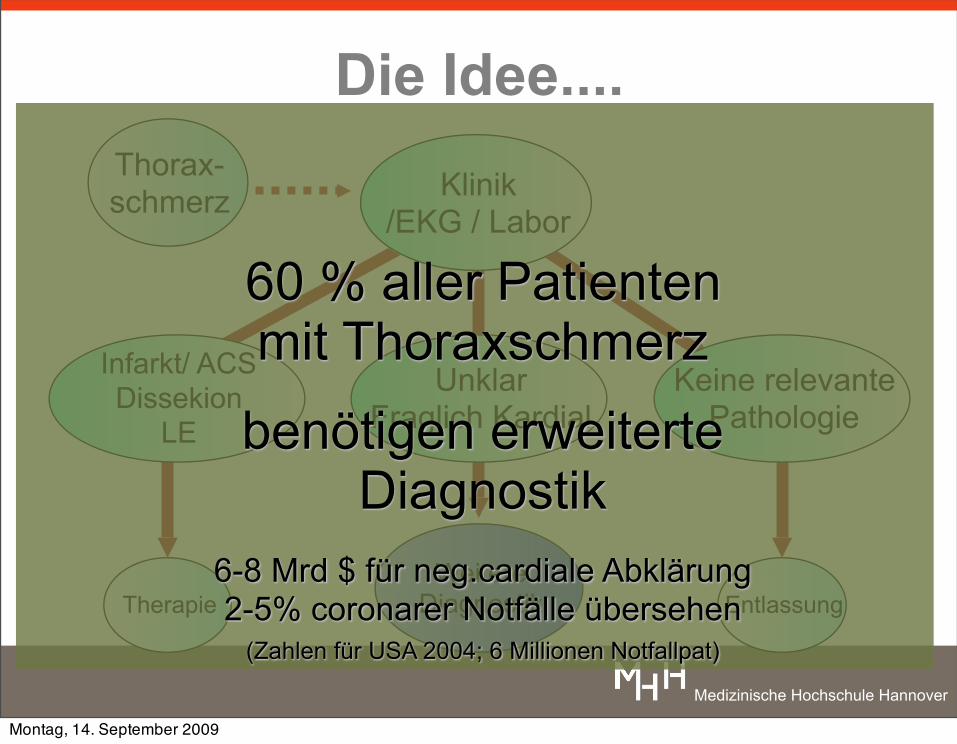
Die Idee....Thorax-schmerz Klinik
/EKG / Labor
UnklarFraglich Kardial
Infarkt/ ACSDissekion
LE
Keine relevantePathologie
Therapie EntlassungWeitere
Diagnostik
60 % aller Patientenmit Thoraxschmerz
benötigen erweiterte Diagnostik
6-8 Mrd $ für neg.cardiale Abklärung2-5% coronarer Notfälle übersehen
(Zahlen für USA 2004; 6 Millionen Notfallpat)
Montag, 14. September 2009
Medizinische Hochschule Hannover
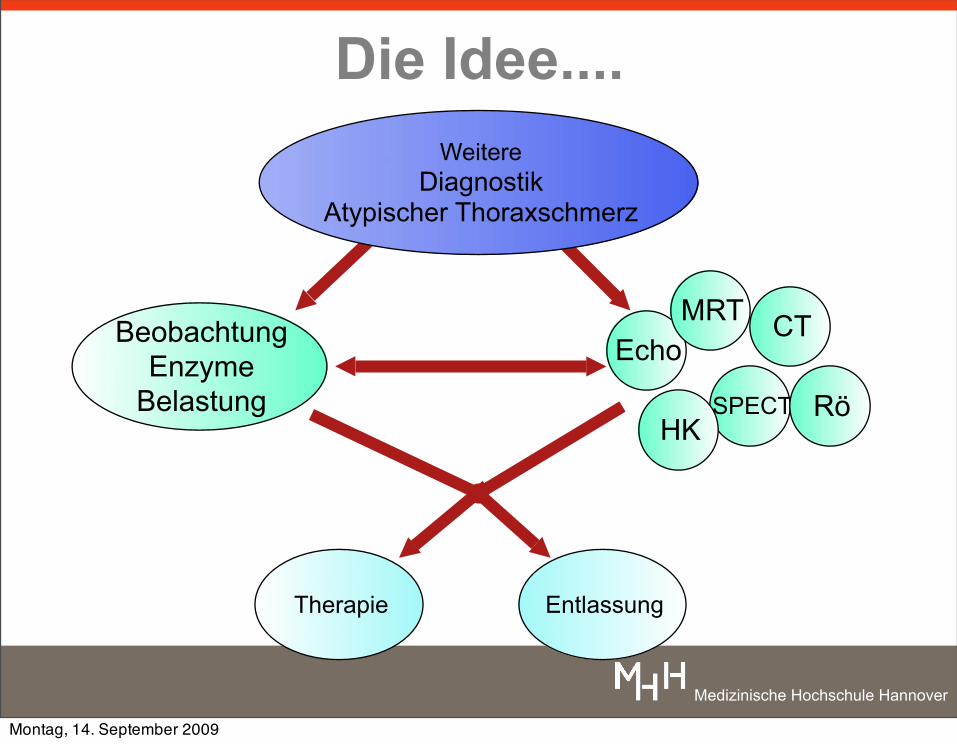
Die Idee....
BeobachtungEnzyme
Belastung
Therapie
EchoCTMRT
SPECT RöHK
WeitereDiagnostik
Atypischer Thoraxschmerz
Entlassung
Montag, 14. September 2009
Medizinische Hochschule Hannover
Die Idee....Thorax-schmerz
Infarkt/ ACSDissekion
LE
Keine relevantePathologie
TherapieEntlassung
Klinik/EKG / Labor
UnklarFraglich Kardial
Triple Rule Out
Montag, 14. September 2009
Medizinische Hochschule Hannover
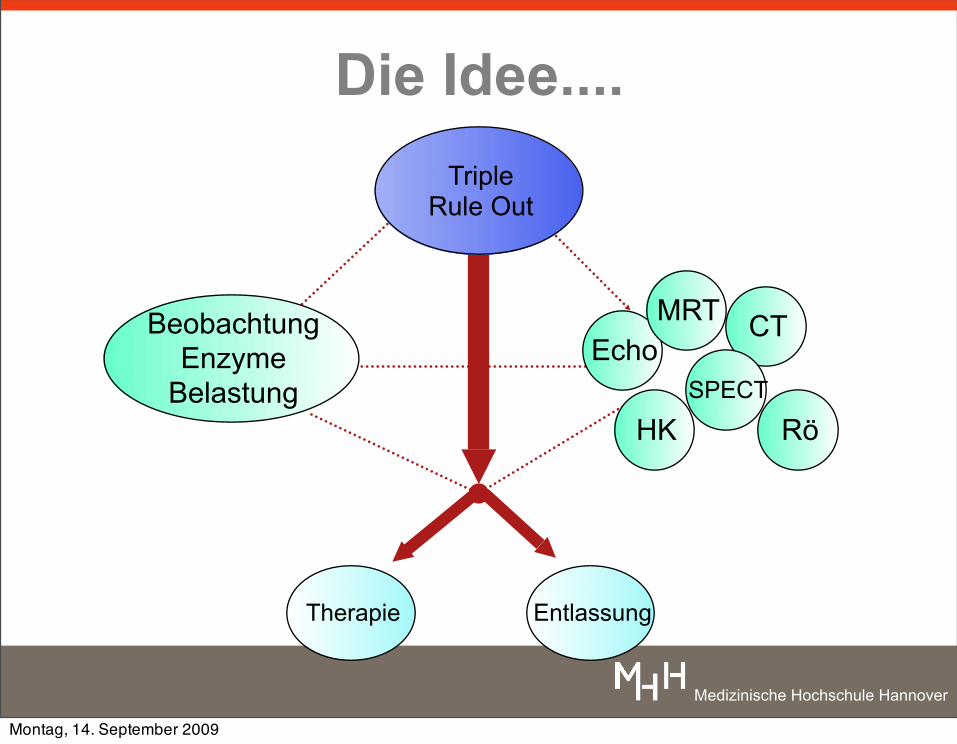
Die Idee....
BeobachtungEnzyme
Belastung
Therapie Entlassung
EchoCTMRT
SPECT
RöHK
Triple Rule Out
Montag, 14. September 2009
Medizinische Hochschule Hannover
Triple Rule OutDie Idee
kürzere Zeit von Diagnose zur Primärtherapie Bessere Prognose? Höhere Kosteneffizienz?
Atypischer Thoraxschmerz MSCT Lungenembolie / Coronarsyndrom / Dissektion / Andere
• Eine Untersuchung• Scandauer:15s, 1x Kontrastmittel• Rasche Diagnosesicherung • rasche Therapieentscheidung
Montag, 14. September 2009
Medizinische Hochschule Hannover
Triple Rule OutVoraussetzung
MSCT >= 32EKG-Fähigkeit
Nähe zur NotaufnahmeVerfügbarkeit des Scanpersonals
Rasche Nachverarbeitung /BefundvermittlungWhite, Baltimore: ca 60min
Charles S. White, J Thorac Imaging Volume 22, Number 1, February 2007
Takakuwa (Philadelphia), Radiology 2008
Montag, 14. September 2009
Medizinische Hochschule Hannover
Triple Rule OutDurchführung
EKG, ß-Blocker, Nitro!Scout
KM Timing (Biphasisches Protokoll)1 Spirale Aortenbogen Lebervenen
Rekonstruktion75% RR: FOV 300 - 400 mm: Dissektion und LE
75% RR: FOV 180-200 mm: KoronarienKernel: medium (B26f-B30f)
Analyse1. Aortendissektion 2. Pulmonalisembolie 3. Koronarien
Halpern, Radiology 2009, Frauenfelder Eur Radiol 2009
Montag, 14. September 2009
Medizinische Hochschule Hannover
Triple Rule OutProblembereiche
Strahlenbelastung: >18 mSv (Takakuwa, Radiology 2008, n=197 Patienten)
~8 mSv mit Dosismodulation (Takakuwa, AJR 2009)
<5 mSv mit neuesten Geräten? (Frauenfelder Eur Radiol 2009)
EKG- Triggerung: Prospektive? Retrospektive?Betablocker? Nitro? Arrhythmien?Cave cardiale Dekompensation
Kontrast-TimingBi-phasische Protokolle?
Dyspnoe?
Montag, 14. September 2009
Medizinische Hochschule Hannover
Triple Rule OutZusammenfassung
Triple Rule Out: Wird kommen
Montag, 14. September 2009
Medizinische Hochschule Hannover
Triple Rule OutZusammenfassung
Triple Rule Out: Wird kommen
Wichtigstes Nahziel : Reduktion Strahlendosis: <8mSv (derzeit: 7-17 mSv)
Montag, 14. September 2009
Medizinische Hochschule Hannover
Triple Rule OutZusammenfassung
Triple Rule Out: Wird kommen
Indikation in naher ZukunftTriple rule Out wenn CTA primär für LE /Aortendissektion indiziert ist - EKG getriggertes CT für verbesserte parakardiale Diagnostik
Wichtigstes Nahziel : Reduktion Strahlendosis: <8mSv (derzeit: 7-17 mSv)
Montag, 14. September 2009
Medizinische Hochschule Hannover
Triple Rule OutZusammenfassung
Triple Rule Out: Wird kommen
Primärer Einsatz beim atypischen Thoraxschmerz : • Bei neg. Troponin, EKG normal• ca. 10-15% coronare Ursachen• ca. 10-15% nicht coronare Ursachen
Indikation in naher ZukunftTriple rule Out wenn CTA primär für LE /Aortendissektion indiziert ist - EKG getriggertes CT für verbesserte parakardiale Diagnostik
Wichtigstes Nahziel : Reduktion Strahlendosis: <8mSv (derzeit: 7-17 mSv)
Montag, 14. September 2009





























