Embed Size (px)
Citation preview
4/8/2021
1
Participating in the Webinar
All attendees will be muted and will remain in Listen Only Mode.
Type your questions here so that the moderator can see them. Not all questions will be answered but we will get to as many as possible.
1
2
American College of Gastroenterology
4/8/2021
2
How to Receive CME and MOC Points
LIVE VIRTUAL GRAND ROUNDS WEBINAR
ACG will send a link to a CME & MOC evaluation to all attendees on the live webinar.
ABIM Board Certified physicians need to complete their MOC activities by December 31, 2021 in order for the MOC points to count toward any MOC requirements that are due by the end of the year. No MOC credit may be awarded after March 1, 2022 for this activity.
MOC QUESTION
If you plan to claim MOC Points for this activity, you will be asked to: Please list specific changes you will make in your
practice as a result of the information you received from this activity.
Include specific strategies or changes that you plan to implement.THESE ANSWERS WILL BE REVIEWED.
3
4
American College of Gastroenterology
4/8/2021
3
ACG Virtual Grand RoundsJoin us for upcoming Virtual Grand Rounds!
Visit gi.org/ACGVGR to Register
Week 16, 2021Opioid Induced Esophageal Dysfunction: What to Know and How to Manage ItMarcelo F. Vela, MD, MSCR, FACGApril 22, 2021 at Noon Eastern
Week 15, 2021Exocrine Pancreatic InsufficiencyJodie A. Barkin, MDApril 15, 2021 at Noon Eastern
Disclosures:
Speaker: Christine Y. Hachem, MD, FACGDIGEST grant awardee from Cystic fibrosis foundation
Moderator: James M. Abraham, MDDr. Abraham, faculty for this educational event, has no relevant financial relationship(s) with ineligible companies to disclose.
5
6
American College of Gastroenterology
4/8/2021
4
Cystic Fibrosis‐Navigating Gastrointestinal ComplicationsChristine Y. Hachem, MD, FACG
Objectives
• Recognize GI dysfunction in Cystic Fibrosis
• Identify risk factors for GI complications in Cystic Fibrosis
• Discuss management of GI issues in Cystic Fibrosis
7
8
American College of Gastroenterology
4/8/2021
5
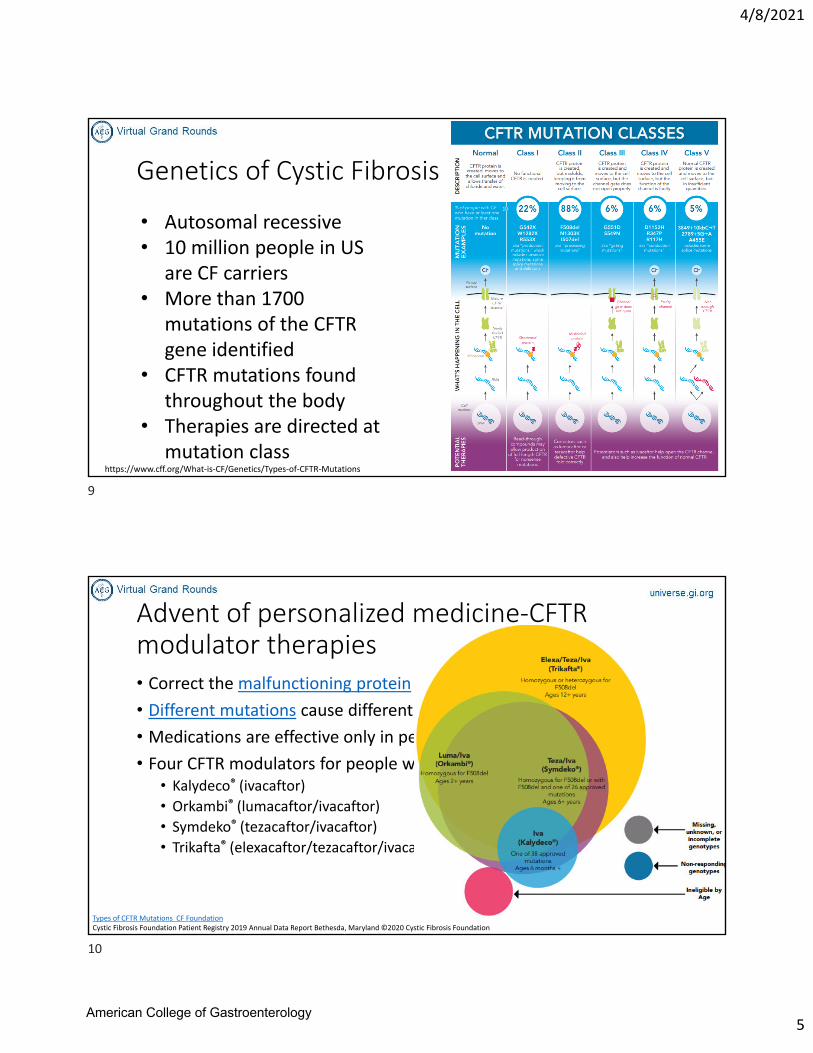
Genetics of Cystic Fibrosis
https://www.cff.org/What‐is‐CF/Genetics/Types‐of‐CFTR‐Mutations
• Autosomal recessive• 10 million people in US
are CF carriers• More than 1700
mutations of the CFTR gene identified
• CFTR mutations found throughout the body
• Therapies are directed at mutation class
Advent of personalized medicine‐CFTR modulator therapies• Correct the malfunctioning protein made by the CFTR gene
• Different mutations cause different defects in the protein
• Medications are effective only in people with specific mutations
• Four CFTR modulators for people with certain CFTR mutations: • Kalydeco® (ivacaftor)
• Orkambi® (lumacaftor/ivacaftor)
• Symdeko® (tezacaftor/ivacaftor)
• Trikafta® (elexacaftor/tezacaftor/ivacaftor)
Types of CFTR Mutations CF FoundationCystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
9
10
American College of Gastroenterology
4/8/2021
6
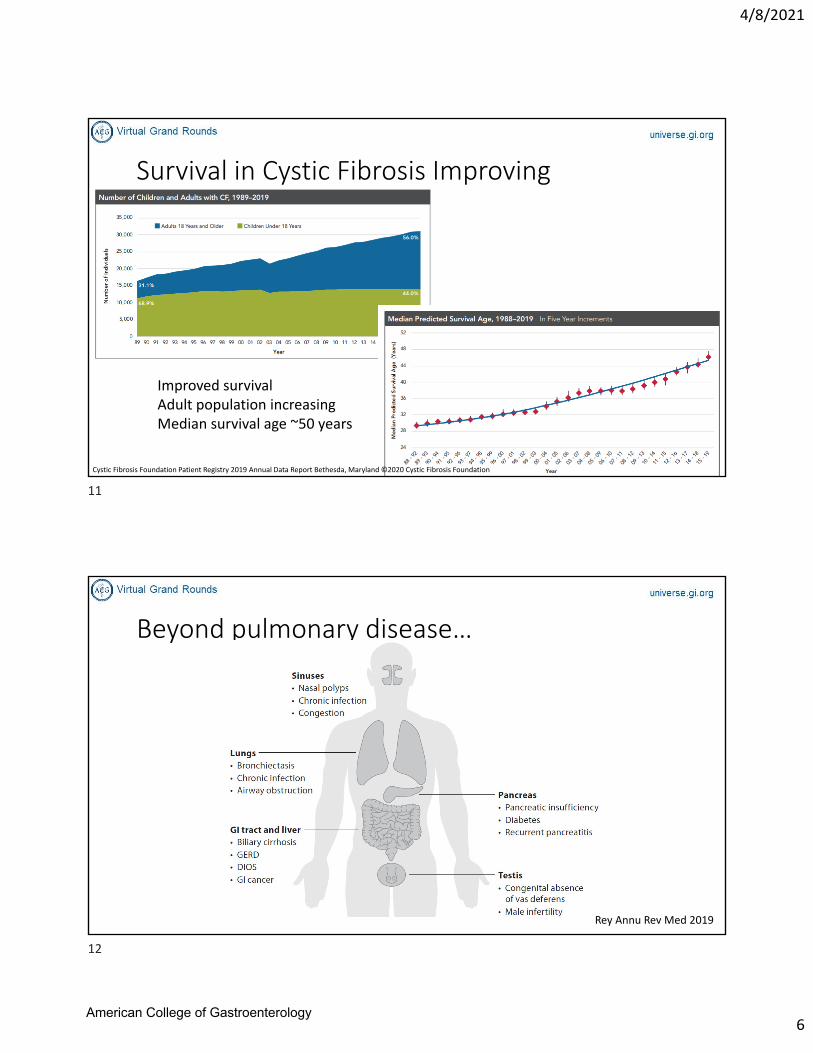
Survival in Cystic Fibrosis Improving
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
Improved survivalAdult population increasingMedian survival age ~50 years
Beyond pulmonary disease…
Rey Annu Rev Med 2019
11
12
American College of Gastroenterology
4/8/2021
7
FINDING THE INTESTINAL
FEV1
EQUIVALENT:THE GALAXY
STUDY
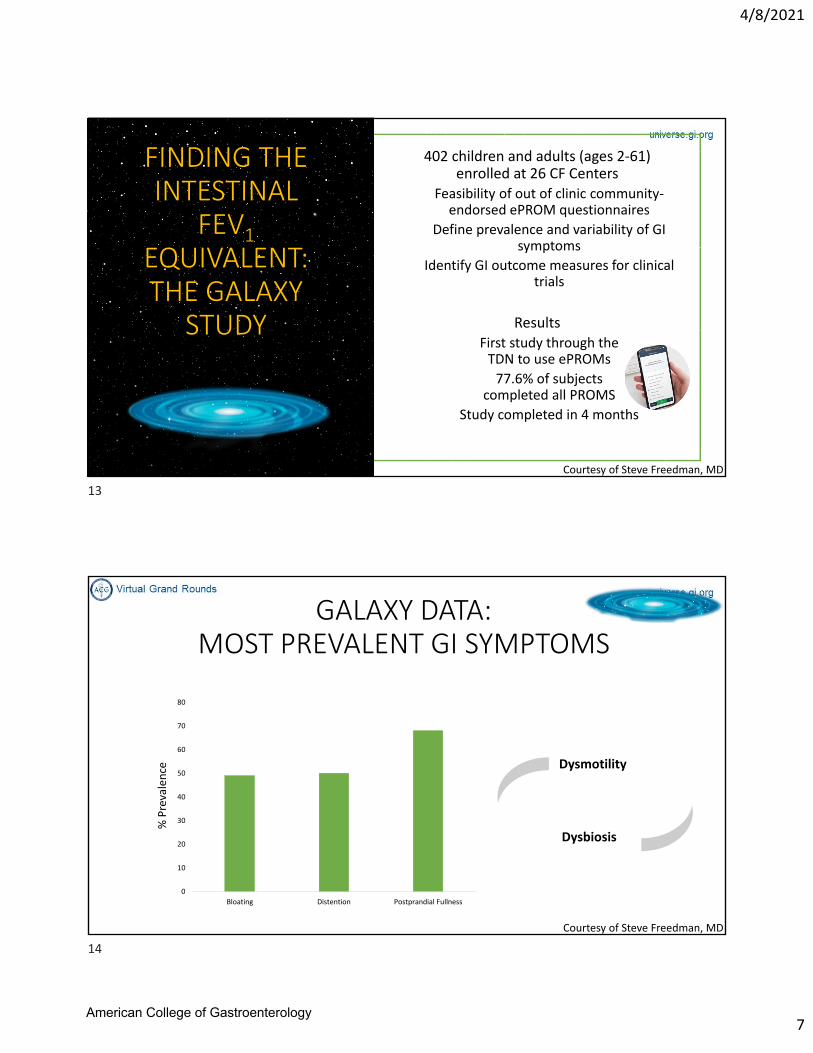
402 children and adults (ages 2‐61) enrolled at 26 CF Centers
Feasibility of out of clinic community‐endorsed ePROM questionnaires
Define prevalence and variability of GI symptoms
Identify GI outcome measures for clinical trials
ResultsFirst study through the TDN to use ePROMs
77.6% of subjects completed all PROMS
Study completed in 4 months
Courtesy of Steve Freedman, MD
GALAXY DATA: MOST PREVALENT GI SYMPTOMS
49 50
68
0
10
20
30
40
50
60
70
80
Bloating Distention Postprandial Fullness
% Prevalence Dysmotility
Dysbiosis
Courtesy of Steve Freedman, MD
13
14
American College of Gastroenterology
4/8/2021
8
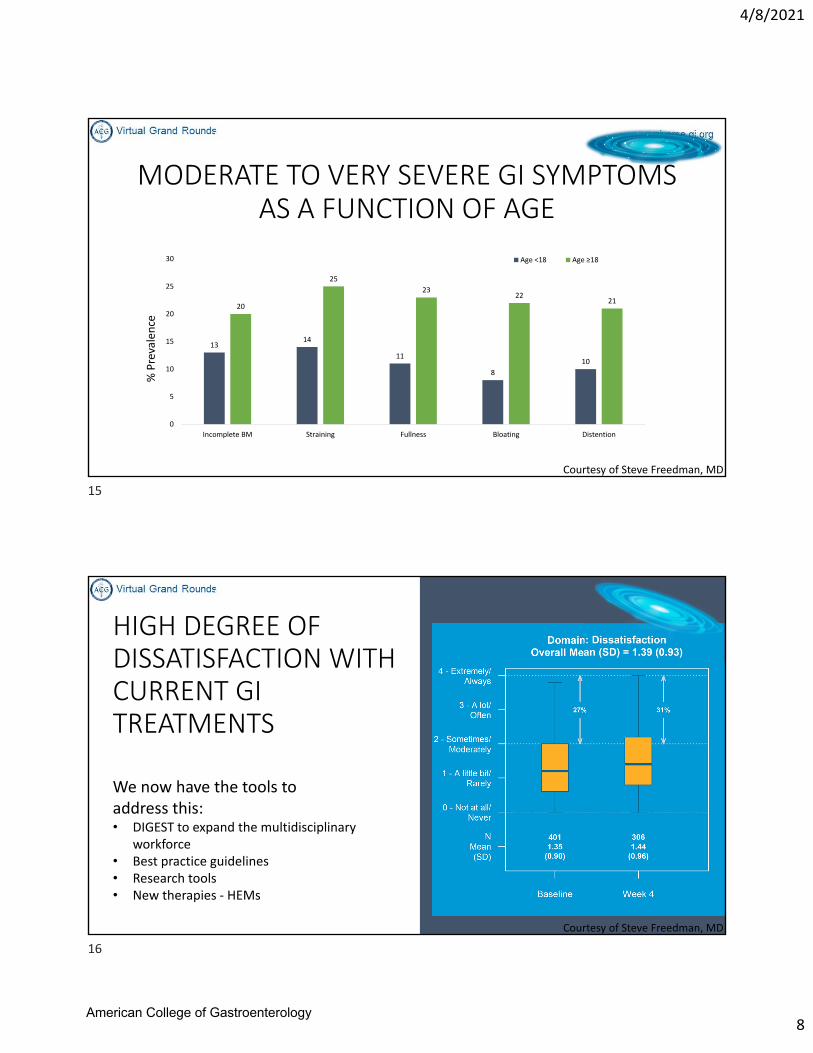
MODERATE TO VERY SEVERE GI SYMPTOMS AS A FUNCTION OF AGE
1314
11
8
10
20
25
2322
21
0
5
10
15
20
25
30
Incomplete BM Straining Fullness Bloating Distention
Age <18 Age ≥18
% Prevalence
Courtesy of Steve Freedman, MD
HIGH DEGREE OF DISSATISFACTION WITH CURRENT GI TREATMENTS
We now have the tools to address this:• DIGEST to expand the multidisciplinary
workforce• Best practice guidelines• Research tools• New therapies ‐ HEMs
Courtesy of Steve Freedman, MD
15
16
American College of Gastroenterology
4/8/2021
9
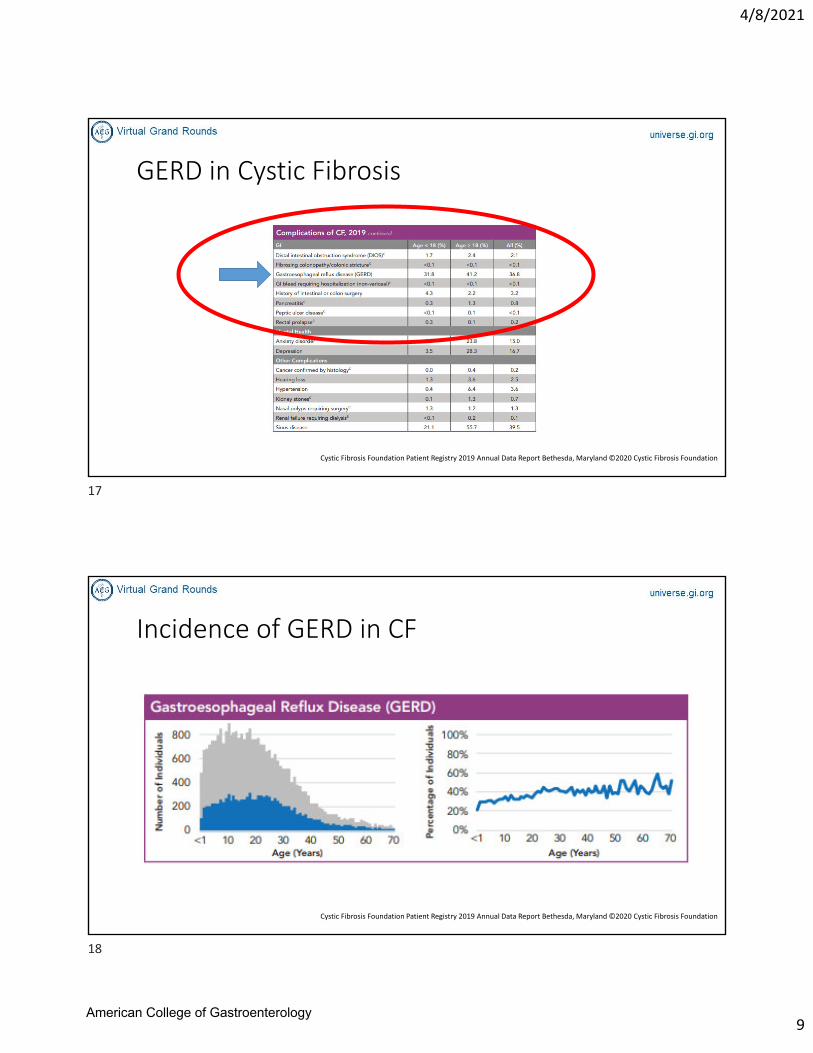
GERD in Cystic Fibrosis
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
Incidence of GERD in CF
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
17
18
American College of Gastroenterology
4/8/2021
10
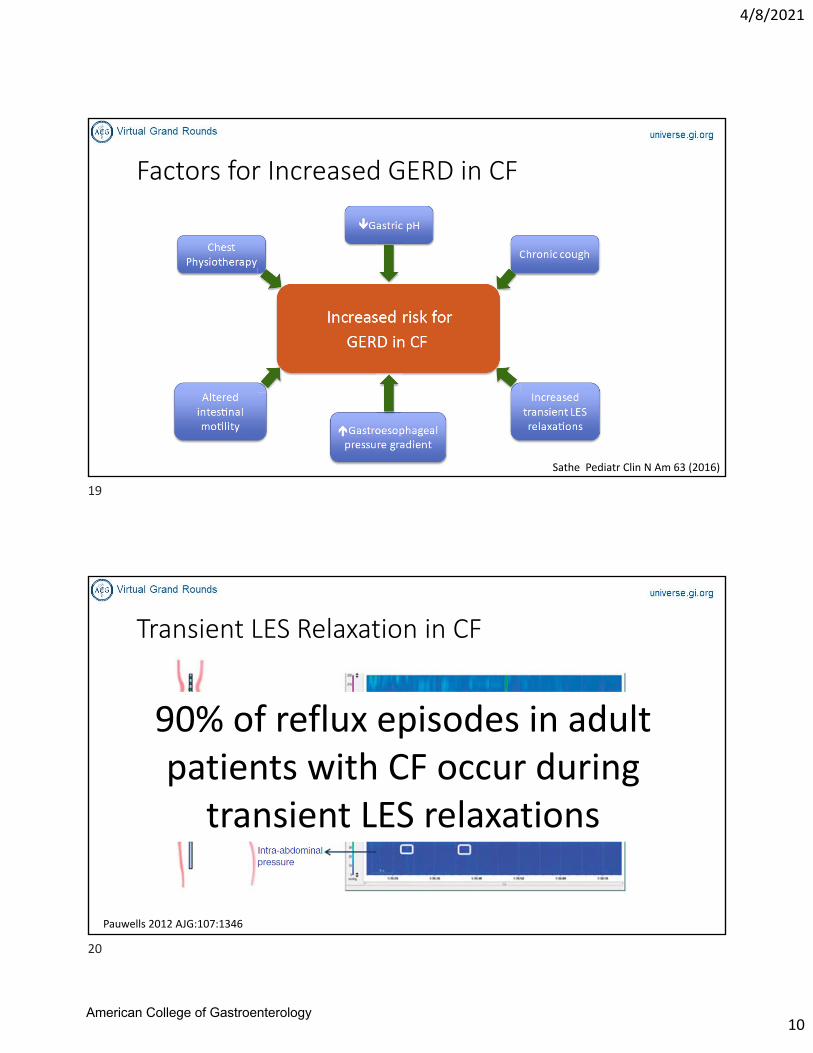
Factors for Increased GERD in CF
Sathe Pediatr Clin N Am 63 (2016)
Transient LES Relaxation in CF
90% of reflux episodes in adult patients with CF occur during transient LES relaxations
Pauwells 2012 AJG:107:1346
19
20
American College of Gastroenterology
4/8/2021
11
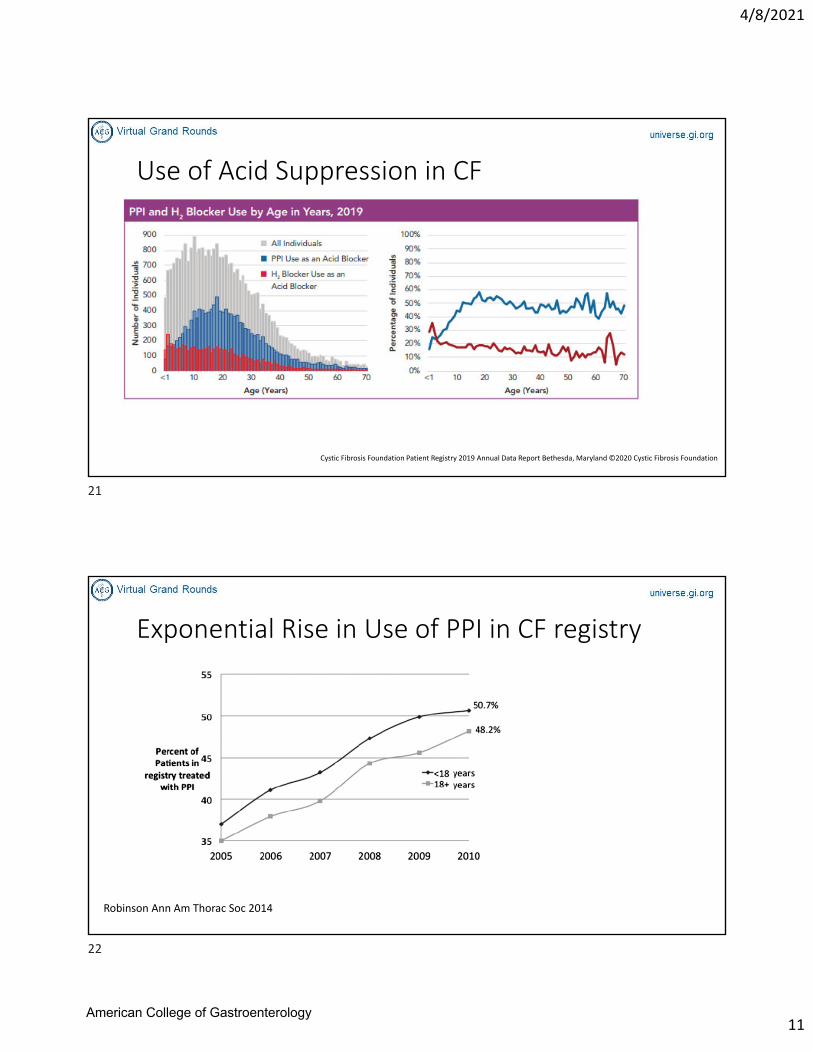
Use of Acid Suppression in CF
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
Exponential Rise in Use of PPI in CF registry
Robinson Ann Am Thorac Soc 2014
21
22
American College of Gastroenterology
4/8/2021
12
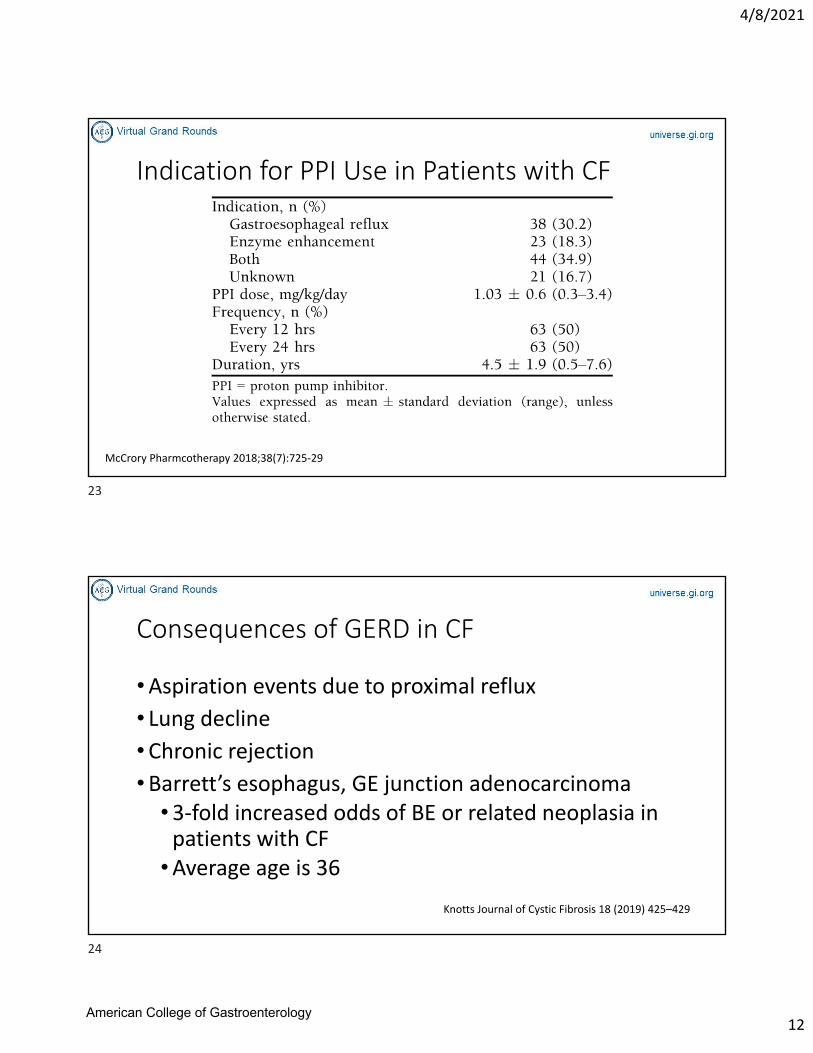
Indication for PPI Use in Patients with CF
McCrory Pharmcotherapy 2018;38(7):725‐29
Consequences of GERD in CF
•Aspiration events due to proximal reflux
• Lung decline•Chronic rejection•Barrett’s esophagus, GE junction adenocarcinoma
•3‐fold increased odds of BE or related neoplasia in patients with CF
•Average age is 36
Knotts Journal of Cystic Fibrosis 18 (2019) 425–429
23
24
American College of Gastroenterology
4/8/2021
13
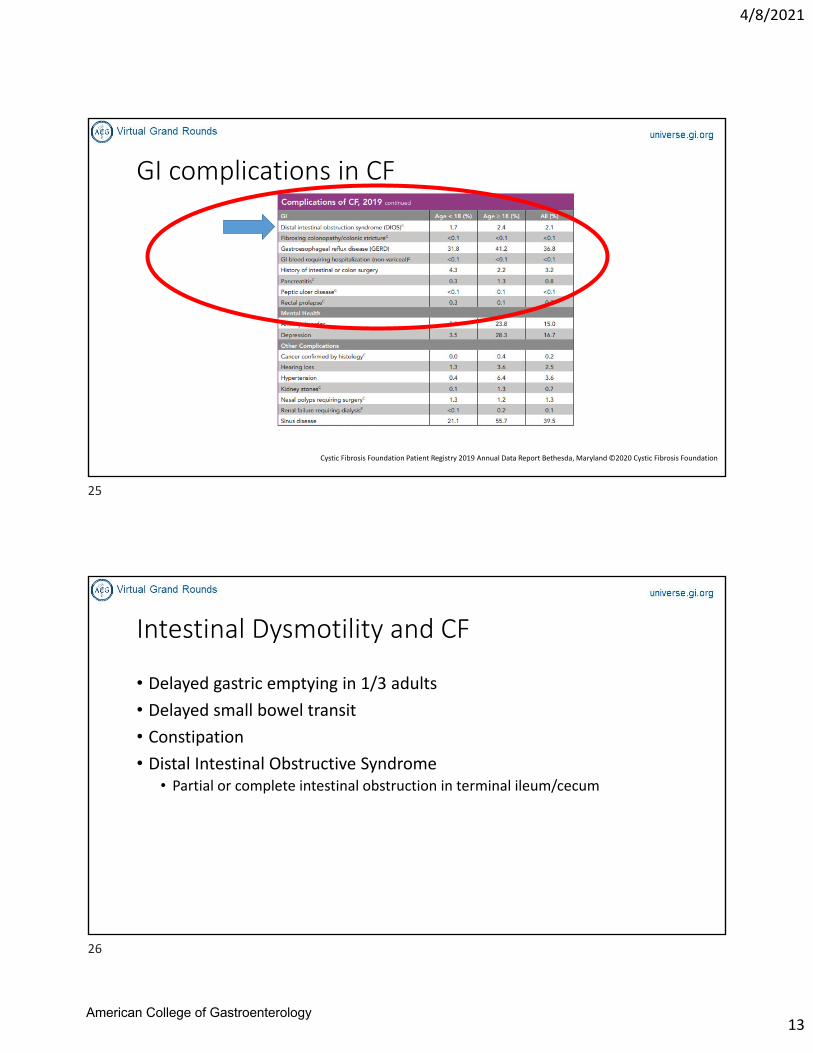
GI complications in CF
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
Intestinal Dysmotility and CF
• Delayed gastric emptying in 1/3 adults
• Delayed small bowel transit
• Constipation
• Distal Intestinal Obstructive Syndrome• Partial or complete intestinal obstruction in terminal ileum/cecum
25
26
American College of Gastroenterology
4/8/2021
14
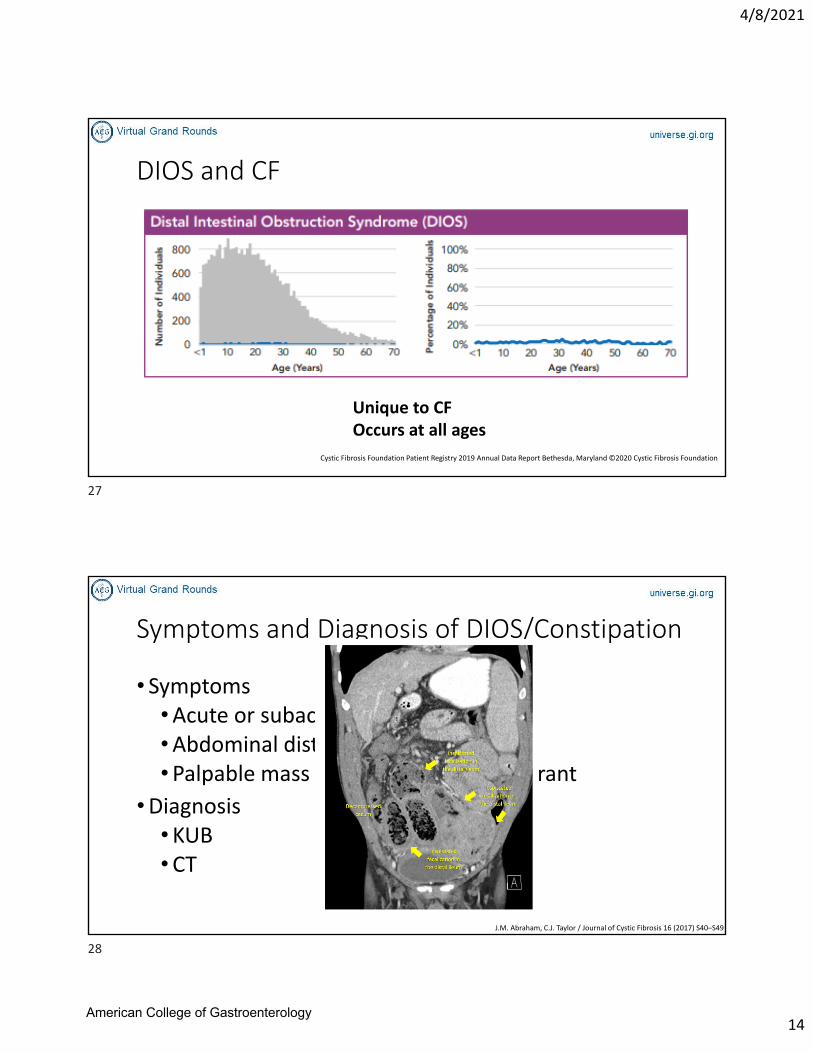
DIOS and CF
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
Unique to CFOccurs at all ages
Symptoms and Diagnosis of DIOS/Constipation
• Symptoms•Acute or subacute abdominal pain•Abdominal distention•Palpable mass in the right lower quadrant
•Diagnosis•KUB•CT
J.M. Abraham, C.J. Taylor / Journal of Cystic Fibrosis 16 (2017) S40–S49
27
28
American College of Gastroenterology
4/8/2021
15
Pathophysiology of DIOS
• Intestinal dysmotility
• Intestinal inflammation
• Fat malabsorption (activation of ileal break)
• Defective ion and water secretion into the gut lumen
Abraham J Cyst Fibrosis 2017
Risk Factors for DIOS/Constipation in CF
• Adults
• Dehydration
• Genotype
• Pancreatic insufficiency – 90%
• History of meconium ileus‐ 50%
• Lung transplant history‐10‐20% in post operative period
• Prior DIOS
29
30
American College of Gastroenterology
4/8/2021
16
Management of Constipation/DIOS
•Constipation; a spectrum to “DIOS”• Keep at risk patients on Polyethylene glycol (PEG)
• Teach to recognize early symptoms, start oral polyethylene glycol at high dose at home
• Slow NG PEG +/‐ lytes (“Golytely”). “colonoscopy clean out”
• Minimize pain meds
• Hyperosmolar contrast enema/Gastrograffin enemas
• Mucomyst
• Anecdotal experience with other bowel agents (lubiprostone, linaclotide, etc)
• Adherence to PERT
• Surgical consultation
Surgery
Endoscopy/Imaging Therapies
Aggressive Medical therapy
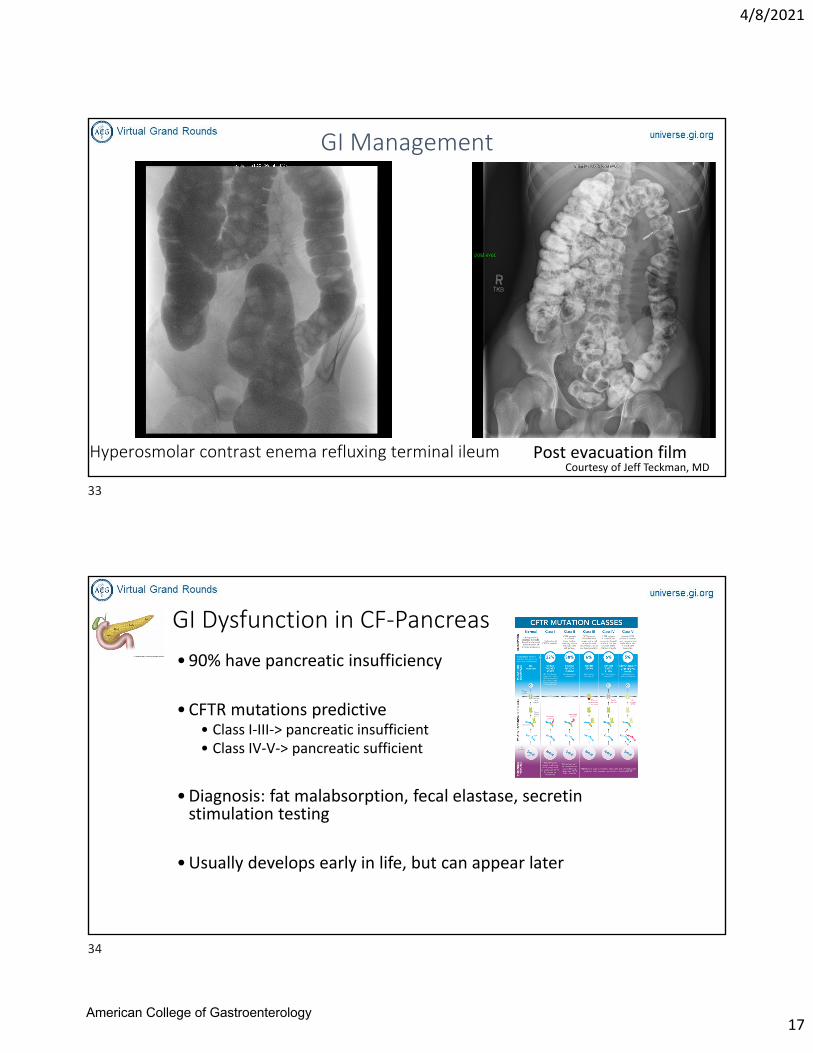
GI Management
A child with constipation and abdominal pain
Courtesy of Jeff Teckman, MD
31
32
American College of Gastroenterology
4/8/2021
17
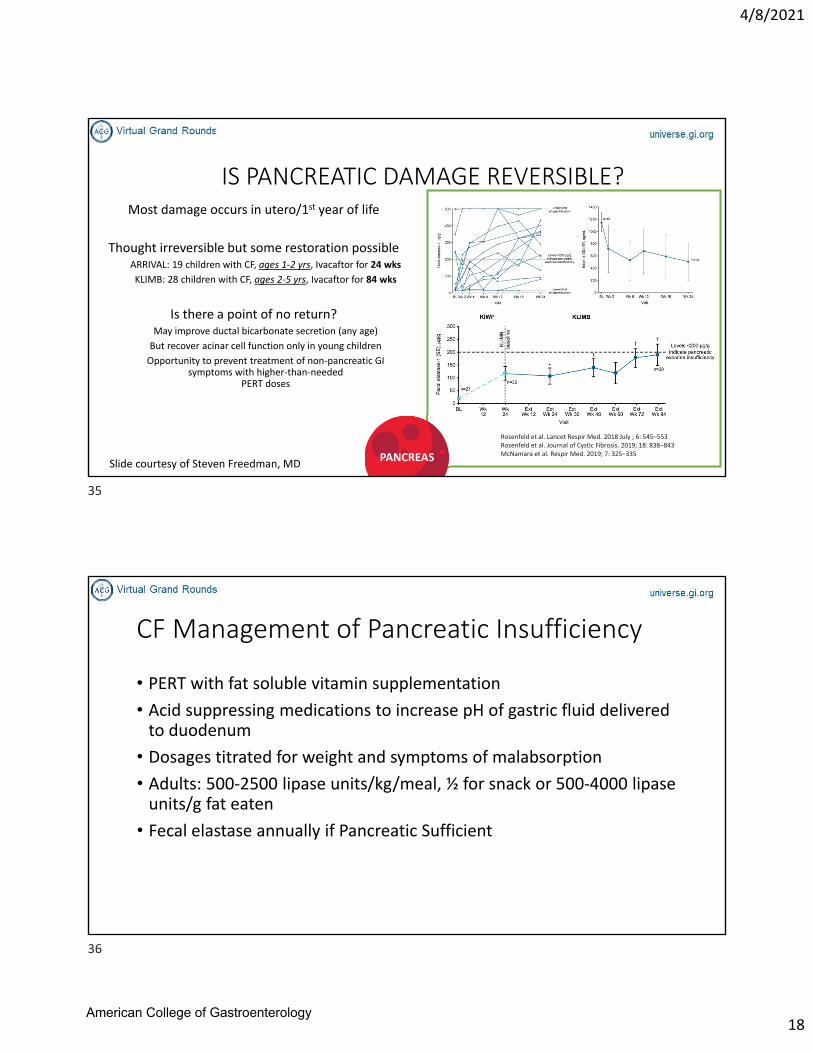
GI Management
Hyperosmolar contrast enema refluxing terminal ileumCourtesy of Jeff Teckman, MD
Post evacuation film
GI Dysfunction in CF‐Pancreas
•90% have pancreatic insufficiency
•CFTR mutations predictive • Class I‐III‐> pancreatic insufficient • Class IV‐V‐> pancreatic sufficient
•Diagnosis: fat malabsorption, fecal elastase, secretin stimulation testing
•Usually develops early in life, but can appear later
33
34
American College of Gastroenterology
4/8/2021
18
IS PANCREATIC DAMAGE REVERSIBLE?Most damage occurs in utero/1st year of life
Thought irreversible but some restoration possibleARRIVAL: 19 children with CF, ages 1‐2 yrs, Ivacaftor for 24 wks
KLIMB: 28 children with CF, ages 2‐5 yrs, Ivacaftor for 84 wks
Is there a point of no return?May improve ductal bicarbonate secretion (any age)
But recover acinar cell function only in young children
Opportunity to prevent treatment of non‐pancreatic GI symptoms with higher‐than‐needed
PERT doses
Rosenfeld et al. Lancet Respir Med. 2018 July ; 6: 545–553Rosenfeld et al. Journal of Cystic Fibrosis. 2019; 18: 838–843McNamara et al. Respir Med. 2019; 7: 325–335PANCREAS
Slide courtesy of Steven Freedman, MD
CF Management of Pancreatic Insufficiency
• PERT with fat soluble vitamin supplementation
• Acid suppressing medications to increase pH of gastric fluid delivered to duodenum
• Dosages titrated for weight and symptoms of malabsorption
• Adults: 500‐2500 lipase units/kg/meal, ½ for snack or 500‐4000 lipase units/g fat eaten
• Fecal elastase annually if Pancreatic Sufficient
35
36
American College of Gastroenterology
4/8/2021
19
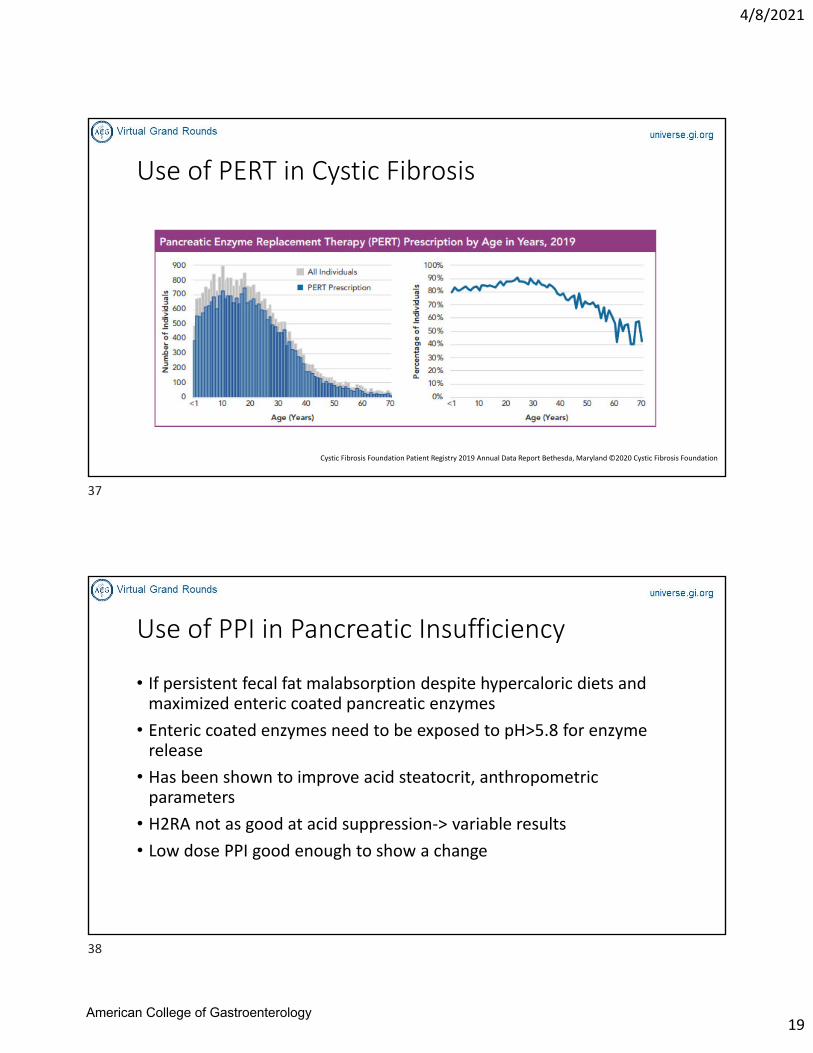
Use of PERT in Cystic Fibrosis
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
Use of PPI in Pancreatic Insufficiency
• If persistent fecal fat malabsorption despite hypercaloric diets and maximized enteric coated pancreatic enzymes
• Enteric coated enzymes need to be exposed to pH>5.8 for enzyme release
• Has been shown to improve acid steatocrit, anthropometric parameters
• H2RA not as good at acid suppression‐> variable results
• Low dose PPI good enough to show a change
37
38
American College of Gastroenterology
4/8/2021
20
Pancreatitis in Cystic Fibrosis
• Milder class mutations Class IV and V
• Pancreatic sufficient
• Good correlation between genotype and PI/PS but not pancreatitis
• Risk factors for pancreatitis: pulmonary exacerbations, viral infections, post surgical
• Can be initial presentation
• Recurrent in 2‐13%
• Can lead to CF related diabetes
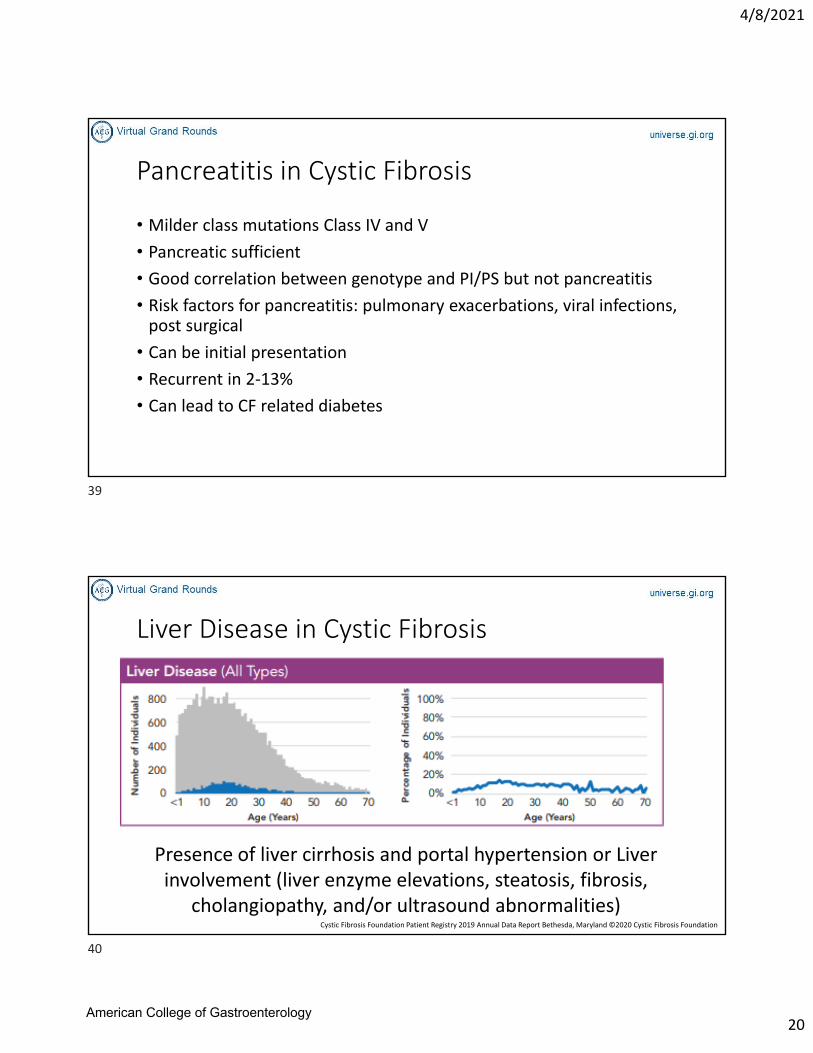
Liver Disease in Cystic Fibrosis
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
Presence of liver cirrhosis and portal hypertension or Liver involvement (liver enzyme elevations, steatosis, fibrosis,
cholangiopathy, and/or ultrasound abnormalities)
39
40
American College of Gastroenterology
4/8/2021
21
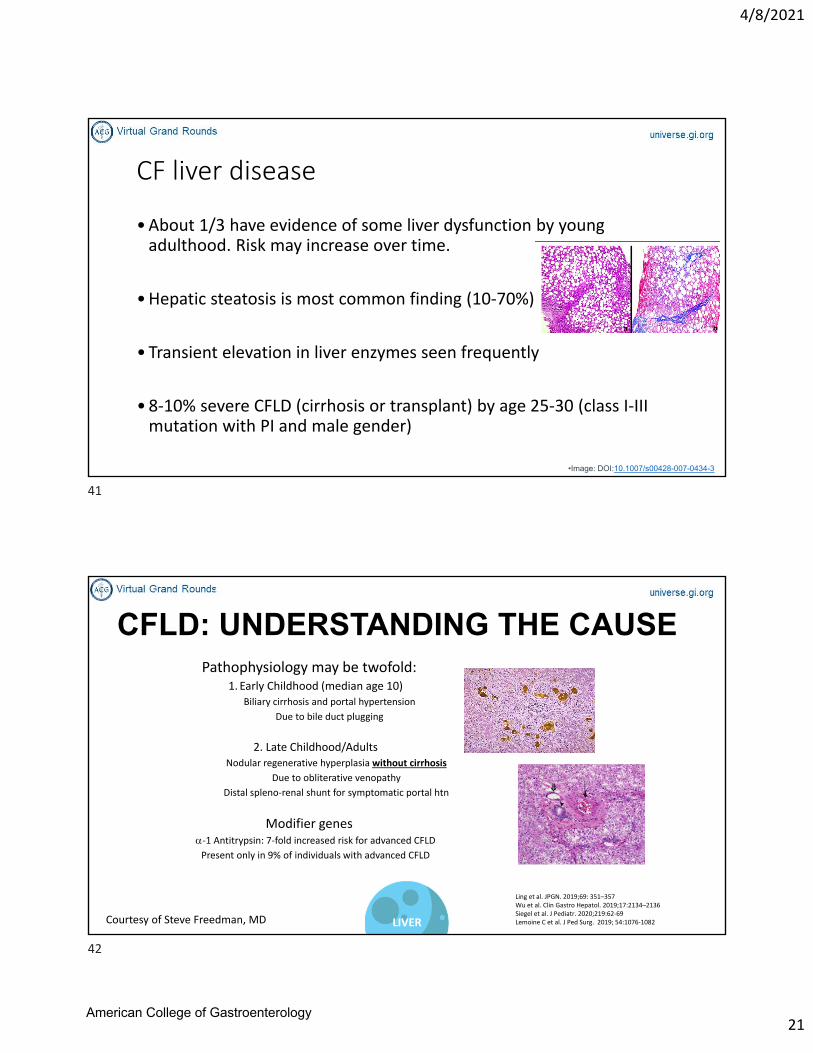
CF liver disease
•About 1/3 have evidence of some liver dysfunction by young adulthood. Risk may increase over time.
•Hepatic steatosis is most common finding (10‐70%)
• Transient elevation in liver enzymes seen frequently
• 8‐10% severe CFLD (cirrhosis or transplant) by age 25‐30 (class I‐III mutation with PI and male gender)
•Image: DOI:10.1007/s00428-007-0434-3
Pathophysiology may be twofold: 1. Early Childhood (median age 10)
Biliary cirrhosis and portal hypertension
Due to bile duct plugging
2. Late Childhood/AdultsNodular regenerative hyperplasia without cirrhosis
Due to obliterative venopathy
Distal spleno‐renal shunt for symptomatic portal htn
Modifier genes‐1 Antitrypsin: 7‐fold increased risk for advanced CFLDPresent only in 9% of individuals with advanced CFLD
Sokol et al. JPGN. 1999; 28 Suppl 1:S1‐S13Ling et al. JPGN. 2019;69: 351–357Wu et al. Clin Gastro Hepatol. 2019;17:2134–2136Siegel et al. J Pediatr. 2020;219:62‐69Lemoine C et al. J Ped Surg. 2019; 54:1076‐1082
CFLD: UNDERSTANDING THE CAUSE
LIVERCourtesy of Steve Freedman, MD
41
42
American College of Gastroenterology
4/8/2021
22
CF Severe Liver Disease Risk Factors
•Male sex•Δ F508 homozygote•Worse lung function•Worse nutritional status•History of meconium ileus
CFLD: DEFINING BIOMARKERS
PUSH trialDefining biomarkers predictive of progression to CFLD
Liver US patterns (heterogeneous or nodular) correlated with biomarkers of liver disease severity
4‐year planned interim analysisHeterogeneous liver ultrasound pattern using research criteria
9.1‐fold increased incidence of nodular pattern, surrogate for advanced CFLD
Reflects clinically relevant, progressive liver disease
Opens the possibility of preventive interventions
Sokol et al. JPGN. 1999; 28 Suppl 1:S1‐S13Ling et al. JPGN. 2019;69: 351–357Wu et al. Clin Gastro Hepatol. 2019;17:2134–2136Siegel et al. J Pediatr. 2020;219:62‐69
LIVER
Courtesy of Steve Freedman, MD
43
44
American College of Gastroenterology
4/8/2021
23
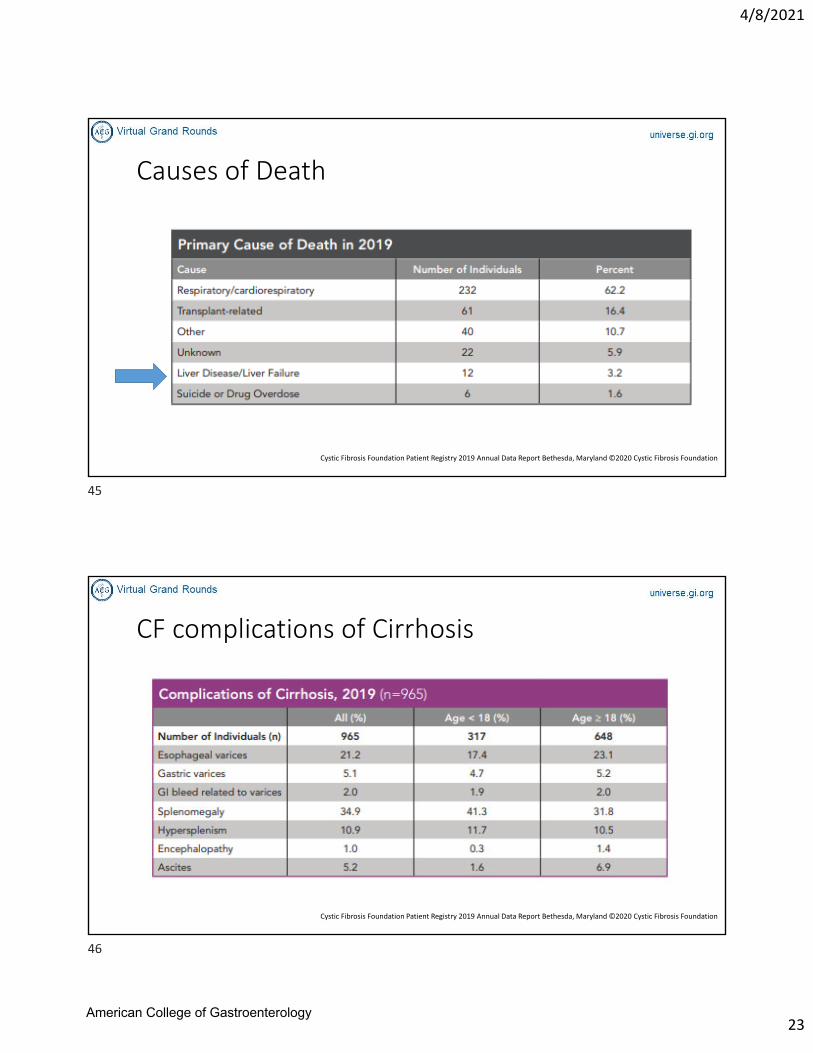
Causes of Death
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
CF complications of Cirrhosis
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis Foundation
45
46
American College of Gastroenterology
4/8/2021
24
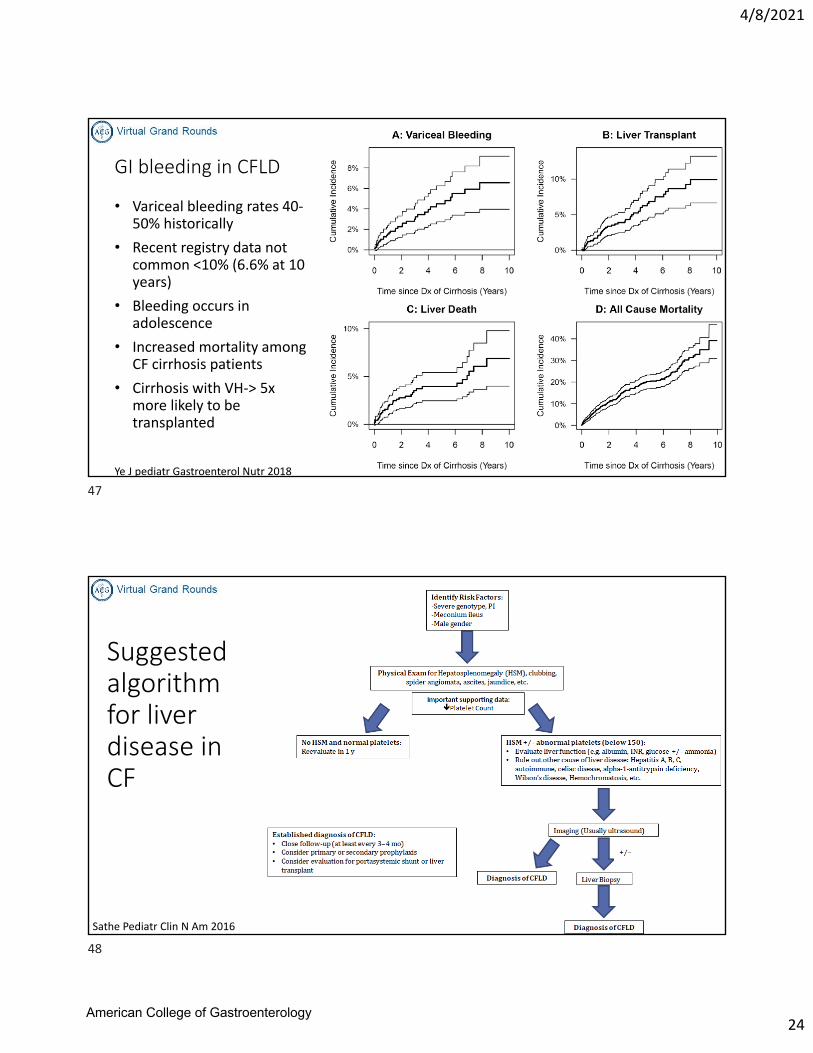
GI bleeding in CFLD
• Variceal bleeding rates 40‐50% historically
• Recent registry data not common <10% (6.6% at 10 years)
• Bleeding occurs in adolescence
• Increased mortality among CF cirrhosis patients
• Cirrhosis with VH‐> 5x more likely to be transplanted
Ye J pediatr Gastroenterol Nutr 2018
Suggested algorithm for liver disease in CF
Sathe Pediatr Clin N Am 2016
47
48
American College of Gastroenterology
4/8/2021
25
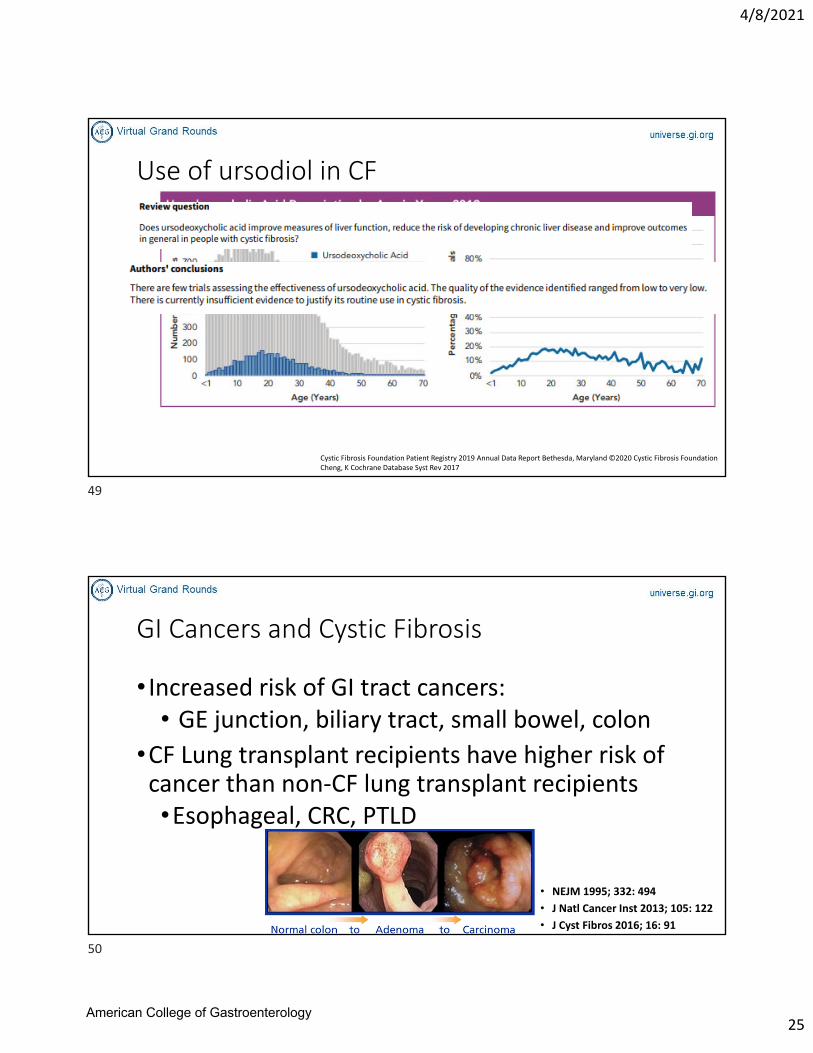
Use of ursodiol in CF
Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report Bethesda, Maryland ©2020 Cystic Fibrosis FoundationCheng, K Cochrane Database Syst Rev 2017
GI Cancers and Cystic Fibrosis
• Increased risk of GI tract cancers:• GE junction, biliary tract, small bowel, colon
•CF Lung transplant recipients have higher risk of cancer than non‐CF lung transplant recipients•Esophageal, CRC, PTLD
• NEJM 1995; 332: 494
• J Natl Cancer Inst 2013; 105: 122
• J Cyst Fibros 2016; 16: 91
49
50
American College of Gastroenterology
4/8/2021
26
Colon Cancer Risk in Cystic Fibrosisrosis
• CFTR: tumor suppressor gene in GI tract of mice• Loss of CFTR results in GI tumor formation• Dysregulation of immune response, intestinal stem cells and growth signaling regulators
• Stagnant mucous‐> bacterial overgrowth‐> dysregulation in gene expression and epithelial homeostasis, inflammation
• Nearly all CRC in CF patients diagnosed before age 50• Screening colonoscopy at age 50 not appropriate in CF patients
• Majority of CRC appear to be right sided• Science 2009; 323: 1747
• Oncogene 2016; 35: 4179
Risk Factors for Cystic Fibrosis related CRC
•Male sex
• Severe functional CF genotype• F508del homozygosity
•Age >30 years • Lung transplantation
51
52
American College of Gastroenterology
4/8/2021
27
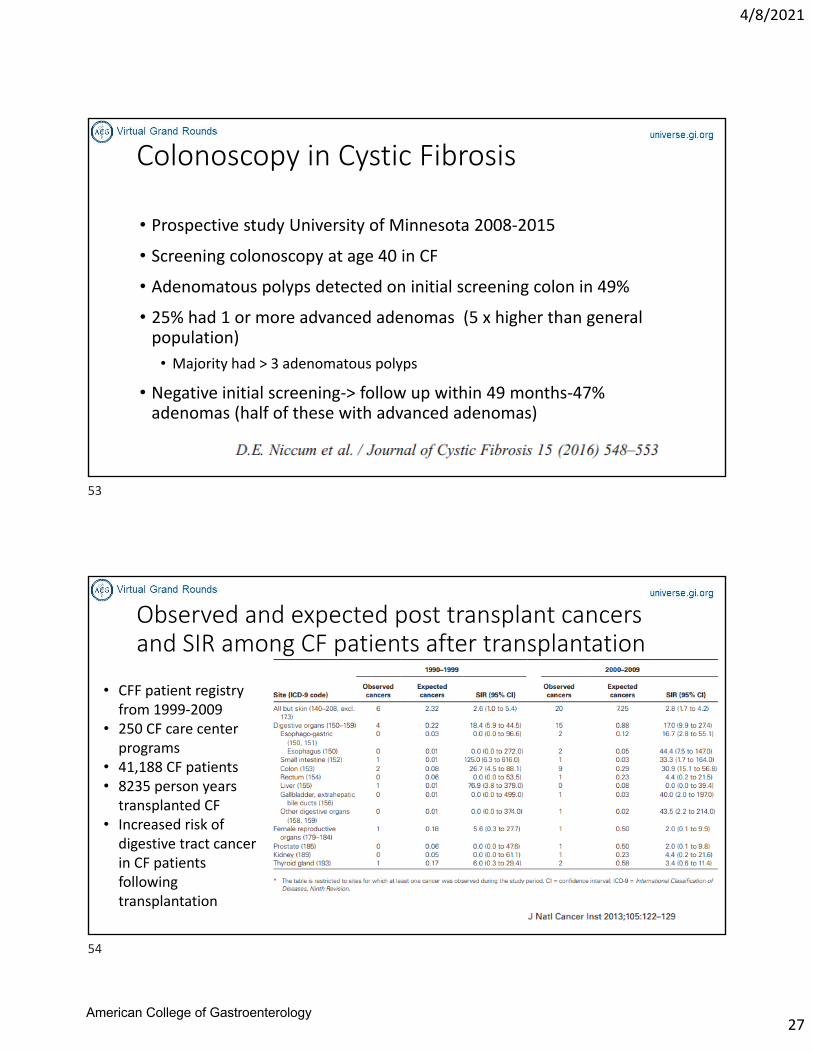
Colonoscopy in Cystic Fibrosis
• Prospective study University of Minnesota 2008‐2015
• Screening colonoscopy at age 40 in CF
• Adenomatous polyps detected on initial screening colon in 49%
• 25% had 1 or more advanced adenomas (5 x higher than general population)
• Majority had > 3 adenomatous polyps
• Negative initial screening‐> follow up within 49 months‐47% adenomas (half of these with advanced adenomas)
Observed and expected post transplant cancers and SIR among CF patients after transplantation
• CFF patient registry from 1999‐2009
• 250 CF care center programs
• 41,188 CF patients• 8235 person years transplanted CF
• Increased risk of digestive tract cancer in CF patients following transplantation
53
54
American College of Gastroenterology
4/8/2021
28
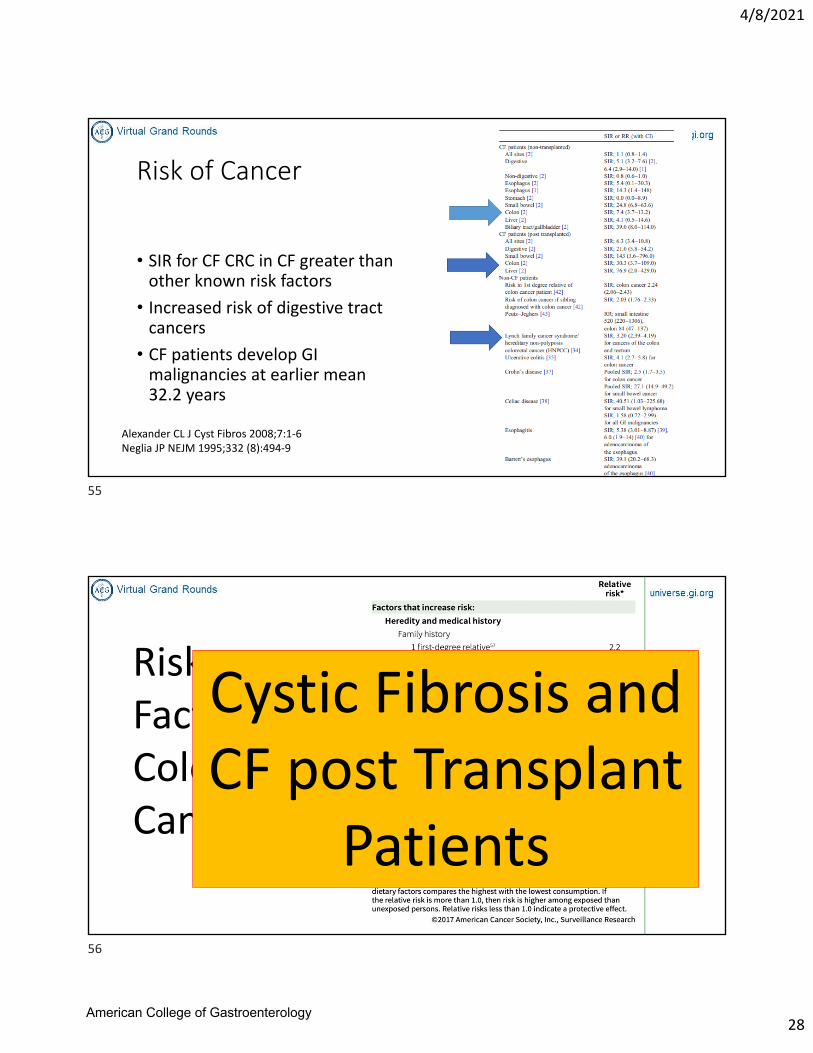
Risk of Cancer
• SIR for CF CRC in CF greater than other known risk factors
• Increased risk of digestive tract cancers
• CF patients develop GI malignancies at earlier mean 32.2 years
Alexander CL J Cyst Fibros 2008;7:1‐6Neglia JP NEJM 1995;332 (8):494‐9
What causes colorectal cancer?
• We do not know the exact cause
• Some changes in the genetic material (DNA) in our cells
• Related to lifestyle
• Many risk factors
Risk Factors for Colon Cancer
Cystic Fibrosis and CF post Transplant
Patients
55
56
American College of Gastroenterology
4/8/2021
29
CF Consensus Recommendation Statement1. Shared decision between patient and provider
2. Jointly managed by CF health care professionals and an endoscopist
3. Colonoscopy only *****
4. Insufficient evidence for the use of CT colonography, FIT/FOBT, or flex‐sig in CRC for CF
1. * Stool based FIT testing may be cost effective and attractive option but FIT characteristics in CF population are lacking
57
58
American College of Gastroenterology
4/8/2021
30
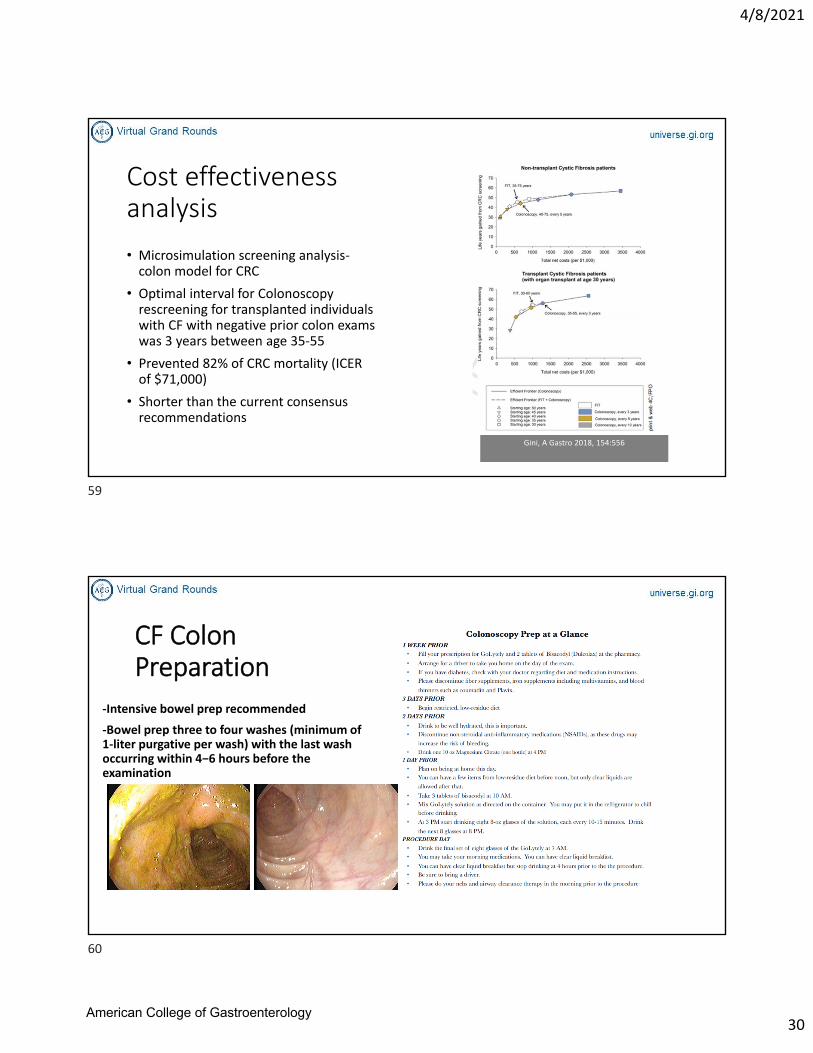
Cost effectiveness analysis
• Microsimulation screening analysis‐colon model for CRC
• Optimal interval for Colonoscopy rescreening for transplanted individuals with CF with negative prior colon exams was 3 years between age 35‐55
• Prevented 82% of CRC mortality (ICER of $71,000)
• Shorter than the current consensus recommendations
Gini, A Gastro 2018, 154:556
CF Colon Preparation
‐Intensive bowel prep recommended
‐Bowel prep three to four washes (minimum of 1‐liter purgative per wash) with the last wash occurring within 4−6 hours before the examination
59
60
American College of Gastroenterology
4/8/2021
31
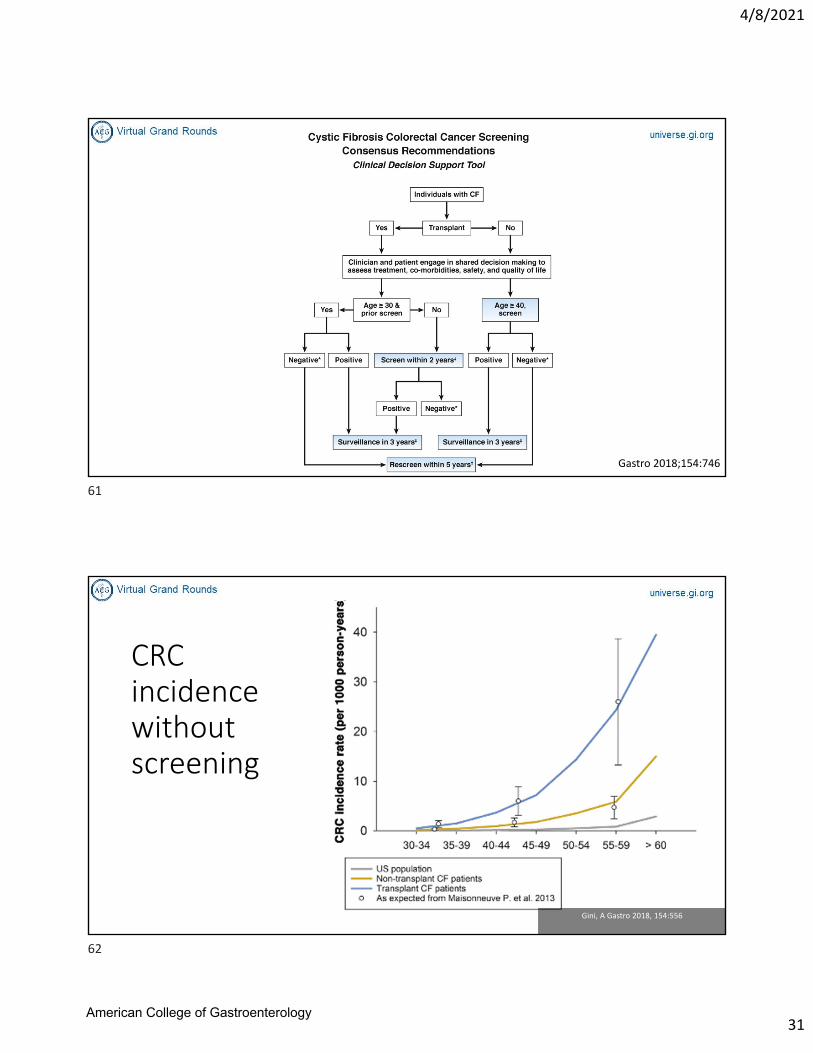
Gastro 2018;154:746
CRC incidence without screening
Gini, A Gastro 2018, 154:556
61
62
American College of Gastroenterology
4/8/2021
32
Take home points• CF is a multisystem disease that involves the GI tract
• CFTR mutations play a role in GI presentations
• Risk of CRC with CF may be greater than that in Lynch syndrome
• All patients with CF should be screened for CRC with colonoscopy and need extended preps
• Stool based testing may be an option in future
• Multiple opportunities for research in CF GI related diseases
Research and Clinical Grants through Cystic Fibrosis Foundation• Developing Innovative Gastroenterology Specialty Training (DIGEST) Program
• The Cystic Fibrosis Foundation recognizes the growing demand for physicians who are trained to address the unique gastroenterological needs of people with cystic fibrosis and the need for a greater focus on gastrointestinal (GI) issues in the clinical research enterprise.
cff.org
63
64
American College of Gastroenterology
4/8/2021
33
Questions?
Speaker: Christine Y. Hachem, MD, FACG
Moderator: James M. Abraham, MD
65
66
American College of Gastroenterology











![Doxycycline improves clinical outcomes during cystic ... · Introduction Cystic fibrosis (CF) is the most common inherited genetic disorder in Caucasians worldwide [1]. It is due](https://img.pdfslide.tips/doc/110x75/5edf2429ad6a402d666a7de0/doxycycline-improves-clinical-outcomes-during-cystic-introduction-cystic-fibrosis.jpg)