Embed Size (px)
Citation preview

Dental pulp (牙髓)何坤炎副教授:高醫醫學大學何坤炎副教授:高醫醫學大學 口腔醫學院牙醫學系口腔醫學院牙醫學系 07-312110107-3121101 轉 轉 7004 , 70297004 , 7029 [email protected]@kmu.edu.tw

學習目標:pulp的解剖結構pulp的的組織結構pulp的功能pulp的退行性變化
學習資源:學習資源:1.1. Ten Cate’s Oral histology. sixth edition, pp 397-416Ten Cate’s Oral histology. sixth edition, pp 397-4162. Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, pp105-122

Anatomy of the pulpIt consists of soft connective tissue, vascular,lymphatic, and nervous tissue
* Human has 20 primary and 32 permanent in each respective dentitionTotal volume for permanent teeth is about 0.38 ml
Avery JK. Essentials of oral histology and embryology
A clinical approach. 1992, p106, Fig.9.1

Pulp * Coronal portion--- pulp chamber occupies the crown of the tooth and resembles the shape the outer surface of crown dentin
* Radicular portion--- root canal --- Apical foramen --- Accessory canal (Incidence: 33 % permanent teeth)
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p107, Fig.9.2
Coronal pulp --- pulp chamber * Pulp horn, pulp extend into cusp, No of
these horns depends on cuspal number * With age, coronal pulp decreases in size owing to continued dentine formation, progresses faster on the floor than other wall
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p107, Fig.9.2

Radicular pulp• Root canal extend from cervical to apex of the root, tapered and conical* Continuous with the periapical tissue through apical foramen
* Become smaller with age owing to continued dentinogenesis, smaller also due to apical cementum deposition
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p107, Fig.9.3

Apical foramen is the pulp opening to periodontium
1. Opening varies in size from 0.3 to 0.6 mm, slightly
larger in maxillary than in mandibular teeth
2. Generally is centrically located in the newly formed
root apex but become more eccentrically located wit
h age, and functional influence

Apical foramen3. Sometimes apical opening is found on the lateral
side of the apex
4.Tooth tipped apex deviate
in the opposite direction
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p108, Fig.9.4

DevelopmentIn earliest stage: the future papilla cause the ora
l epithelium to invaginate and form enamel organs
Dental papilla further control the forming enamel organs to be an incisor or molar
* Pulp is initially called dental papilla, after dentin
forms: pulp
* 8th week of embryonic life Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p110, Fig.9.7

Histology of the pulp1. Large nerve trunk &blood vessel in the central
2. Peripherally: odontogenic region cell-free zone (Weil’s) cell-rich zone
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p109, Fig.9.5

Histology of the pulpCell-free zone (Weil’s): area of mobilization and
replacement of odontoblasts
Cell-rich zone: composed principally of fibroblasts
and undifferentiated mesenchymal cells
* During early dentinogenesis,
many young collagen fibers
in this zone
From KMU
OD
CFZ
CRZ

Odontoblast5-7 m in diameter, 25-40 m in length
Near pulp-predentin junction, cytoplasma is devoid of organelles, at this clear zone cell constricts to 3-4 m, where the cell process enters the predentinal tubule
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p109, Fig.9.5

Odontoblast process into
mineralized dentin, contains
filaments and microtubes
through its length to DEJ
Recent information indicate
it extends through DEJ into
enamel as spindles
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p111, Fig.9.8

The form and arrangement of the cell
bodies of odontoblasts are not uniform
throughout the pulpHighly columnar in crown,
Low cuboidal in middle of root,
Flat and spindle close to the apex

Ground substance (jell-like tissue)1) Proteoglycans or acid mucopolysaccharides ( 酸性黏多醣 )2) Glycoproteins ( 醣蛋白 )
Alternation in composition caused by age or disease, interfere with this function, producing metabolic changes, reduced cellular function, and irregularities in mineral deposition
Components of pulp

Fibroblast: stain deeply with basic dyes, and cytoplasm is lighter stained appears homogeneous, typical stellate and extensive processFunction in collagen formation and protein synthesis* Also ingesting and degrading collagen when approximate stimulated
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p112, Fig.9.12

FibroblastsCharacterized by their functional state, young pulp actively
producing matrix and collagen, star shape, have multiple
process with ovoid nucleus
Abundant RER and mitochondria
Old pulp--- fiber increase, smaller
and spindle-shaped with few
organelles
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p112, Fig.9.13

Collagen and fine fibers in pulp
Collagen bundles: cross-sections at 64 nm
intervals, range in length 10-100 m or
more
Fine collagen fibrils: argyrophilic fibers,
originate from pulp fibroblasts formation
of predentin

Both type I and III collagen approximate(55:45) in the pulp remain constant from beginning of tooth development to tooth maturityType I probably produced by odontoblast,type III by pulp fibroblasts

Young pulp fibers are relatively sparse
If pulp is irritated, fibers may accumulate rapidly,
older pulp contain more collagen of both
bundle and diffuse type
* The greatest concentration
of collagen seen in most
apical portion of the pulp
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p114, Fig.9.17

Histiocyte or macrophageirregularly shaped with short blunt
process. Smaller, more rounded, and
darker staining than fibroblast, and
exhibits granular cytoplasm.
* Disclosed by trypan blue (intravital dyes), aggregation of vesicles, phagocytized dense irregular bodies

VascularityVessels arising from external carotids to superior orinferior alveolar arteries. Thin-walled arteries and arterioles enter apical canal and pursue a directroute up to coronal area
Central core Peripheral plexus
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p115, Fig.9.18, 19

Vascularity
Arteriole in coronal portion of pulp they divide and subdivide to form an extensive vascular capillary network, U-looping is seen, this anatomical configuration is thought to be related to regulation of blood flow
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p115, Fig.9.19

* Pulpal blood flow is most rapid than areas of the body Arterioles is 0.3 -1 mm/second Venules is 0.15 mm/second Capillaries about 0.08 mm/second
* Pulpal pressure is among the highest of the body

Blood vessels
Tunica intima --- squamous or cuboid endothelial cells surrounded by closely associated basal lamina
Tunica media --- 1-3 layers of smooth muscle cells, occasionally endothelial cell wall in contact with muscle
cells this is termed a “myoendothelial junction”
Tunica adventitia --- made up of a few collagen fibers forming a loose network around the large arteries

Veins and venules
1. 100-150 m in diameter, larger than arteries2. Tunica adventitia lacking or appear as fibroblast
3. Endothelial cells more flattened
4. In central region of root pulp

Capillary appears as “endothelium - lined”
tubules (8-10 m), nuclei may be lobulated
and cytoplasma projections into luminal
surface
* Fenestrated capillaries may involved in rapid transport of metabolites, for predentinal matrix formation, and calcification of dentin

Nerves1. Most nerves are myelinated
2. Mediate the sensation of pain
caused by external stimuli
3. Non-myelinated nerves closed
to blood vessels, sympathetic
in nature, vasoconstriction
4. Parietal layer of nerve---
plexus of Raschkow
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p116, Fig.9.21

5. Nerve ending close to odontoblast plasma membrane separated only by 200 Å cleft
6. Most of nerve endings in odontoblast are sensory afferents and sympathetic from superior cervical ganglion
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p117, Fig.9.23

Pulp tissue nerve fibers 1. A fibers fast conducting, diameter 1-6 m , f
or early stage of damage in dentin to sense th
e pain, for sharp, localized pain
2. Aβ fibers 1%, 6-12 m
3. C fibers--- nonmyelinated, 0.4-1.2 m, dull a
nd diffuse pain

Most of nerve fibers and endings are found in pulp hornsSensory response in pulp can distinguish among thermal, mechanical and tactile *Raschkows nerve plexus and free nerve ending of unmyelinated axons in predentin and dentin layer

Functions of the pulp
1. Initiative (inductive)
2. Formative
3. Protective
4. Nutritive
5. Reparative

Functions of the pulp
1. Inductive---induce oral epithelium differentiate into dental lamina and enamel organ formation, and becoming a particular type of tooth
2. Formative---odontoblast develop organic matrix
and function in its calcification, dentin is formed

Functions of the pulp
3. Nutritive- nourishes dentin through odontoblast
and their process, and by blood vascular system
4. Protective---sensory nerves responds with pain
to all stimulus
Sympathetic---reflux, control circulation of
blood vessel

Functions of the pulp
5. Defensive or reparative--- producing reparative dentin and mineralizing any affected dentinal tubules Macrophage and PMN aid in the process of repair
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p119, Fig.9.26

Functions of the pulp
Provide vitality to teeth with its cells, bloodvessels, and nerve Endodontic treated tooth function without pain but lost its protective mechanism thatthe pulp nerve provide

Regressive Changes
* Cell changes --- aging pulp are characterized by fewer cells, decrease in size and number of various cytoplasmic organelles, less perinuclear cytoplasma, and possess long, thin cytoplasmic processes

Regressive Changes * Fibrosis -- accumulation of diffuse fibrillar components and bundles of collagen fiber Collagen increase is noted in medial and adventitial layers of blood vessels Any external trauma usually cause localized fibrosis and scarring effect

Regressive Changes* Vascular changes --- outer diameter of vessels
walls becomes greater as collagen fibers increase in the medial and adventitial layers* Calcification in the walls of blood vessels is found in the region near apical foramen
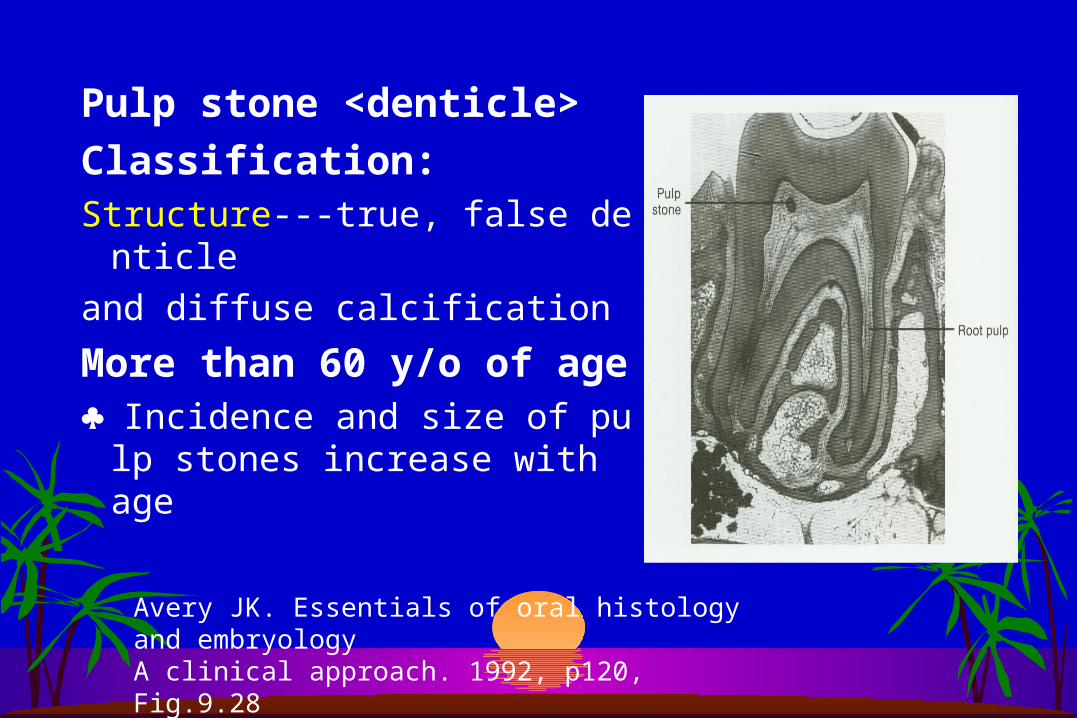
Pulp stone <denticle>
Classification:Structure---true, false denticle
and diffuse calcification
More than 60 y/o of age ♣ Incidence and size of pulp sto
nes increase with age
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p120, Fig.9.28

Pain conduction– three mechanisms 1. Dentin contains nerve ending and directly innervated 2. Odontoblasts acts as a receptor and are coupled to nerve in the pulp3. Receptors are in the pulp and are stimulated by fluid movement through the dentinal tube
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p118, Fig.9.25

Pain conduction--Hydrodynamic theory Stimulation causes odontoblasts and their
processes to move contact with nerve endings
in the predentin and pulp.* It results in mechanoreceptors receiving the impulse that conduct pain response to central nerve system
Avery JK. Essentials of oral histology and embryology A clinical approach. 1992, p118, Fig.9.25

Clinical considerations1. Nonvital tooth becomes brittle and is subject to fractures2. Aging pulp chamber become smaller, due to excessive dentin formation difficult to locate root canal 3. Accessory canals--- deep periodontal pocket may cause inflammation of dental pulp

結論♣ The vitality of dentin-pulp complex plays an important role in maintenance of a functional dentition, and maintaining tooth vitality while focusing particularly on the cell of pulp.
♣ Preservation of the vitality of pulp during operative procedures is the most important challenges to clinical dentist



![醫院牙科經營管理研討會-Lin 20130707.ppt [相容模式] · 2 臺大醫院牙科部基本資料 • 國立臺灣大學醫學院附設醫院 • National Taiwan University](https://img.pdfslide.tips/doc/110x75/5e126537d869aa785e18d15b/eeccccccceoef-lin-c-2-eeeccefoee.jpg)





















![(蝕)[073-083] 05 海外歯科保健医療活動(責)月18日(水)に国立陽明大學牙醫學院キャンパスおよび陽明牙醫診所を訪問し,陽明大學にて](https://img.pdfslide.tips/doc/110x75/5f89e2f44dabbc5fbb0425c3/iei073-083-05-coeciei-oe18iiceceefffeceeeioee.jpg)


